Feb 5, 2026

What makes retatrutide dosing different from other peptides
Most people searching for a retatrutide dose schedule want one thing. A clear, week-by-week plan they can follow without guessing. They want to know exactly when to increase, how much to take at each step, and what to expect along the way. The problem is that most guides out there bury this information under pages of generic background, leaving researchers to piece together their own timelines from scattered clinical trial data and forum posts.
That changes here.
Retatrutide is not like semaglutide or tirzepatide. Those peptides activate one or two receptors. Retatrutide activates three, targeting GLP-1, GIP, and glucagon receptors simultaneously, which is why Eli Lilly calls it a "triple agonist." This triple mechanism is also why the dose schedule matters more than with any other weight loss peptide on the market. Get the escalation wrong, and the gastrointestinal side effects become severe enough that people abandon the protocol entirely. Get it right, and the results speak for themselves, with phase 2 trial participants losing an average of 24.2% of their body weight at the 12mg dose over 48 weeks.
This guide breaks down the complete retatrutide dose schedule into a practical, week-by-week format. You will find the exact titration timeline used in clinical trials, the reasoning behind each escalation step, what to do when side effects force you to slow down, and how to calculate your injection volumes based on common vial sizes. Whether you are following a conservative 4-week escalation or a more cautious 6-week approach, every schedule variation is covered with specific milligram amounts and injection timing.
SeekPeptides has compiled the most comprehensive dose schedule reference available, drawing directly from published research and practical protocol experience.
Understanding retatrutide triple agonist mechanism and why dosing matters
Before diving into the specific dose schedule, understanding why retatrutide requires such careful titration helps explain every decision in the escalation timeline. This is not a peptide you can simply start at the target dose. The triple receptor activation creates a cascade of metabolic effects that your body needs time to adjust to.
The three receptors and what they do
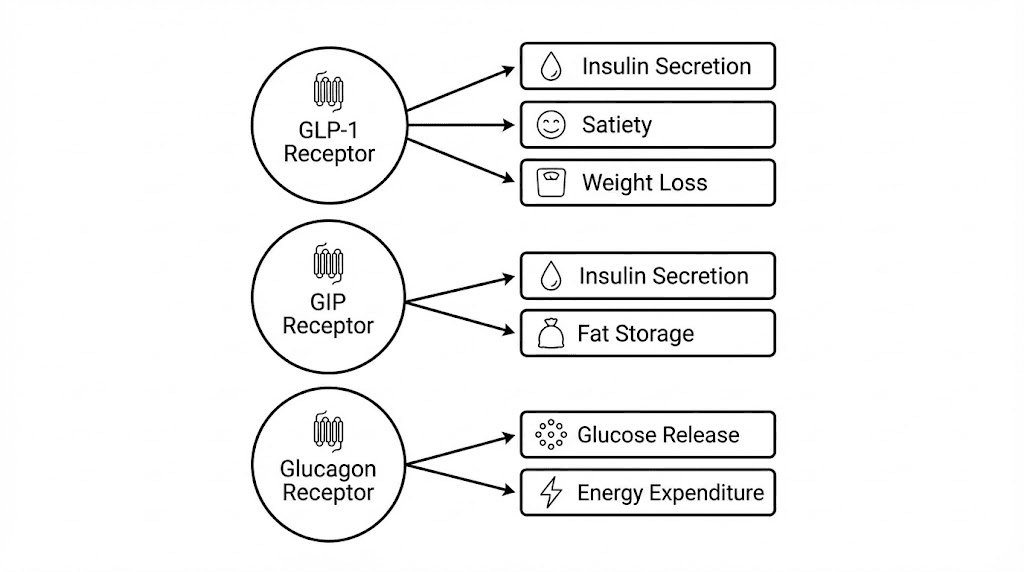
Retatrutide simultaneously activates three distinct hormone receptors. Each one plays a different role in weight management, and each one contributes to the side effect profile that makes proper dose scheduling essential.
GLP-1 receptor activation handles appetite suppression and appetite control. This is the same receptor that semaglutide targets, and it works by slowing gastric emptying, enhancing insulin secretion in response to glucose, and sending satiety signals to the brain. The GLP-1 component is also the primary driver of the gastrointestinal side effects that make gradual dose escalation necessary. When you activate this receptor too aggressively, nausea, vomiting, and diarrhea become significant problems.
GIP receptor activation adds a second layer of metabolic regulation. Glucose-dependent insulinotropic polypeptide, or GIP, works alongside GLP-1 to improve insulin sensitivity and lipid metabolism. This is the same receptor that tirzepatide activates in addition to GLP-1. The dual activation in tirzepatide already showed superior weight loss compared to semaglutide alone. Retatrutide takes this further.
The glucagon receptor is what truly sets retatrutide apart. While it might seem counterintuitive to activate a receptor associated with raising blood sugar, glucagon receptor activation increases energy expenditure through thermogenesis and promotes lipid mobilization. This means your body burns more calories at rest and breaks down stored fat more efficiently. The combination of all three receptors working together produces results that neither single nor dual agonists can match. This triple mechanism is why retatrutide appears prominently in discussions of Ozempic alternatives and top weight loss peptide options.
Why the dose schedule cannot be rushed
Clinical trial data from the phase 2 NEJM study revealed something critical about dose scheduling. Participants who started at 4mg directly experienced nearly double the gastrointestinal side effects compared to those who started at 2mg and titrated upward. The numbers were clear. A lower starting dose of 2mg partially mitigated the severity and frequency of nausea, vomiting, and diarrhea across all dose groups.
This is not a minor difference.
When gastrointestinal symptoms become severe, adherence drops. People miss doses. They reduce their intake without following a structured schedule. They abandon the protocol entirely. The researchers behind the phase 2 trial specifically designed the titration schedule to prevent this, and the data validated their approach. Starting low and escalating gradually over defined 4-week intervals produced the best combination of efficacy and tolerability.
Your body needs approximately 4 weeks at each dose level to adapt. During this period, the GLP-1 mediated slowing of gastric emptying becomes less noticeable as your digestive system adjusts. The appetite suppression stabilizes. The glucagon-driven thermogenesis ramps up without causing excessive metabolic stress. Skip this adaptation period, and you are fighting your own biology instead of working with it. The bioactive peptide precision required for optimal results starts with respecting this adaptation timeline.
The standard retatrutide dose schedule from clinical trials
The phase 2 trial published in the New England Journal of Medicine tested multiple dosing arms, and the data from these arms forms the foundation of every retatrutide dose schedule used today. Understanding exactly what was tested, and what produced the best results, gives you the framework to build your own schedule.
Phase 2 trial dosing groups explained
The trial randomized participants into seven groups. Six received retatrutide at varying doses and starting points, while one received placebo. The groups were assigned in a 2:1:1:1:1:2:2 ratio, meaning the 12mg and placebo groups were larger to improve statistical power at the extremes.
Here is what each group received:
1mg group: 1mg weekly for the full 48 weeks, no escalation
4mg (starting at 2mg): Started at 2mg, escalated to 4mg after 4 weeks
4mg (starting at 4mg): Started directly at 4mg, no escalation
8mg (starting at 2mg): Started at 2mg, escalated through 4mg to reach 8mg
8mg (starting at 4mg): Started at 4mg, escalated to 8mg after 4 weeks
12mg (starting at 2mg): Started at 2mg, escalated through 4mg, 8mg to reach 12mg
The weight loss results at 48 weeks told a clear story. The 1mg group lost 8.7% of body weight. The combined 4mg groups lost 17.1%. The combined 8mg groups lost 22.8%. And the 12mg group lost 24.2%. Placebo lost just 2.1%. The retatrutide dosage chart we published breaks down these numbers in detail.
But the comparison between starting doses within the same maintenance dose was equally important. Groups that started at 2mg and escalated gradually reported fewer and milder GI side effects than groups that started at 4mg, even when both reached the same final dose. This finding directly shaped the recommended dose schedule that most protocols now follow.
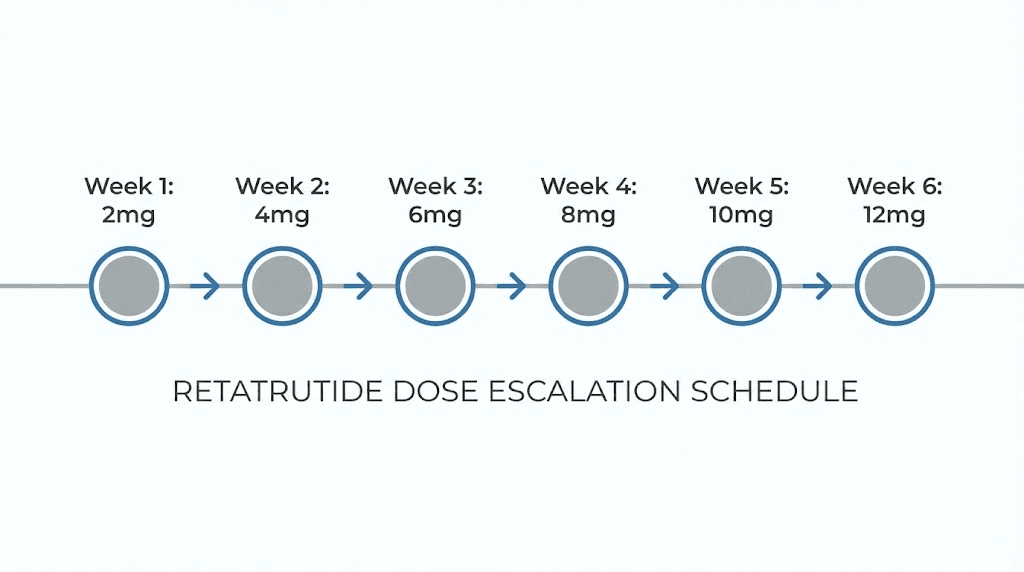
The recommended 4-week escalation schedule
Based on the phase 2 trial data, the standard retatrutide dose schedule follows a 4-week escalation pattern starting at 2mg. This schedule targets a maintenance dose of 12mg, which produced the highest weight loss in clinical testing. Here is the week-by-week breakdown.
Weeks 1 through 4: 2mg weekly
The starting phase. Your body begins adapting to GLP-1, GIP, and glucagon receptor activation simultaneously. Most researchers experience mild appetite suppression starting around days 3 to 5. Nausea, if it occurs, tends to be mild and manageable during this phase. Some people notice no side effects at all at 2mg. This is normal and does not mean the peptide is not working. The receptors are activating, but the dose is deliberately low enough to minimize the initial adjustment period. Understanding common beginner mistakes helps avoid unnecessary changes during this critical adaptation window.
During these first four weeks, pay attention to how your body responds. Notice changes in appetite timing, food preferences, and energy levels. These observations become important later when deciding whether to extend any escalation step. You can track your response patterns using the tools at SeekPeptides.
Weeks 5 through 8: 4mg weekly
The first dose increase doubles the amount. This is typically when appetite suppression becomes more noticeable. Meal sizes naturally decrease. Food cravings, particularly for high-calorie foods, begin to diminish. GI side effects are more common during the first week at 4mg but usually stabilize by week 2 at this dose level. Researchers tracking their before and after results typically notice measurable changes beginning during this phase.
The 4mg dose produced an average weight loss of 17.1% at 48 weeks in the clinical trial. For some researchers, 4mg provides sufficient appetite suppression to achieve their goals without further escalation. This is a legitimate maintenance dose if the side effects at higher levels prove unmanageable or if the weight loss trajectory at 4mg meets your targets.
Weeks 9 through 12: 8mg weekly
This is a significant jump, doubling the dose again from 4mg to 8mg. The retatrutide dosage calculator can help you determine exact injection volumes at this concentration. Many researchers report the most noticeable increase in GI side effects during the first 7 to 10 days at 8mg. Nausea becomes more prominent. Some experience constipation or loose stools. These symptoms typically fade by the end of the second week at this dose.
At 8mg, the glucagon receptor activation becomes more significant. You may notice increased body heat and slightly elevated resting heart rate, both signs of the thermogenic effect. Energy expenditure increases measurably at this dose. The combined 8mg groups in the trial lost 22.8% of body weight at 48 weeks, with 100% of participants achieving at least 5% weight loss and 91% achieving 10% or more.
Weeks 13 through 16: 12mg weekly (full maintenance dose)
The final escalation step brings you to the maximum dose tested in phase 2 trials. The 12mg dose produced the headline results: 24.2% mean body weight reduction at 48 weeks. Every participant in the 12mg group lost at least 5% of body weight. 93% lost 10% or more. And 83% lost 15% or more.
At this dose, all three receptor systems are fully engaged. Appetite suppression is substantial. Thermogenesis is elevated. Lipid mobilization is maximized. The key during the first 2 weeks at 12mg is managing the GI adjustment. After that, most researchers find the side effects stabilize at a tolerable level.
Once you reach 12mg, this becomes your maintenance dose. You continue at 12mg weekly for the duration of your protocol. The phase 2 trial ran for 48 weeks total, and the weight loss curve had not fully plateaued by that point, suggesting continued benefits beyond the trial period.
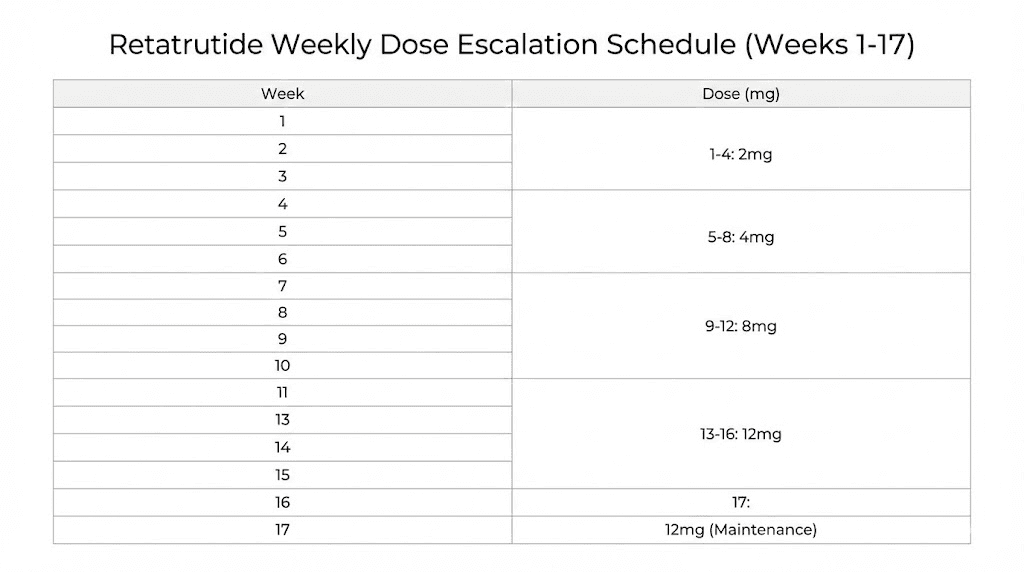
Week-by-week dose schedule table
Week | Dose | Injection frequency | Expected effects | Common side effects |
|---|---|---|---|---|
1-4 | 2mg | Once weekly | Mild appetite suppression, initial receptor adaptation | Mild nausea in some, minimal for most |
5-8 | 4mg | Once weekly | Noticeable appetite reduction, decreased food cravings | Moderate nausea first week, constipation possible |
9-12 | 8mg | Once weekly | Strong appetite suppression, increased thermogenesis | Nausea, possible diarrhea, elevated body heat |
13-16 | 12mg | Once weekly | Maximum appetite suppression, peak fat mobilization | GI symptoms that stabilize after 1-2 weeks |
17+ | 12mg | Once weekly | Steady weight loss, maintained metabolic enhancement | Generally well tolerated at this point |
This table provides the standard schedule. Your actual escalation may need adjustments based on individual tolerance, which the next section covers in detail. For general peptide dosing principles, our comprehensive guide covers the fundamentals that apply across all protocols.
Conservative dose schedule for sensitive individuals
Not everyone tolerates the standard 4-week escalation well. Some researchers experience more pronounced GI side effects, particularly those who are sensitive to GLP-1 receptor agonists or who have a history of digestive issues. For these individuals, a conservative schedule extends each dose step to 6 weeks instead of 4, giving the body additional adaptation time.
The 6-week escalation protocol
This modified schedule takes 24 weeks to reach the full 12mg maintenance dose instead of 16 weeks. The tradeoff is clear. Slower escalation means fewer side effects but a longer time to reach the maximally effective dose. For many people, this tradeoff is worth it. Adherence matters more than speed, and a researcher who completes the full protocol at a slower pace will achieve better long-term results than someone who quits halfway through a faster schedule due to intolerable side effects. Our peptide dosage chart provides visual references for multiple escalation approaches across different peptides.
Weeks 1 through 6: 2mg weekly
Same starting dose as the standard schedule, but with two extra weeks of adaptation. This extended period allows even the most sensitive individuals to fully adjust to the initial receptor activation. By week 6, any GI symptoms from the 2mg dose should have completely resolved.
Weeks 7 through 12: 4mg weekly
The first increase with a full 6 weeks to adapt. Researchers following this protocol often report that the nausea at 4mg peaks during week 7 or 8 and resolves completely by week 10. The extra time at each step does not reduce the eventual effectiveness of higher doses.
Weeks 13 through 18: 8mg weekly
The jump to 8mg is where the conservative schedule provides the most benefit. This dose level causes the most significant GI adjustment, and having 6 weeks instead of 4 makes the transition substantially more comfortable. Many researchers on the conservative schedule report that their 8mg experience is comparable to what standard-schedule users describe at 4mg.
Weeks 19 through 24: 12mg weekly (maintenance begins)
The final step to full maintenance dose. After 6 weeks, the body is fully adapted and ready for long-term use at 12mg. From week 25 onward, the protocol continues at 12mg weekly indefinitely.
When to choose the conservative schedule
Choose the 6-week schedule if any of these apply to you:
Previous strong GI reactions to GLP-1 agonists like semaglutide or tirzepatide
History of IBS, GERD, or other chronic digestive conditions
BMI under 30 (lower body mass can increase sensitivity to fixed doses)
Current use of other medications that affect gastric motility
First-time use of any GLP receptor agonist
The research is clear on this point. Staying at your current dose for an extra 2 to 4 weeks does not reduce long-term weight loss effectiveness. It simply allows your body more time to adjust, which often improves overall adherence and compliance with the full protocol. Researchers who have explored peptide therapy options through clinical settings often find that supervised protocols use similar conservative escalation approaches. The peptide therapy clinics guide covers how medical professionals typically manage dose titration.
Phase 3 TRIUMPH trial dose schedule updates
The phase 3 TRIUMPH program expanded on the phase 2 dosing framework, and the recent results add important context to how dose schedules may evolve. Eli Lilly has been running multiple TRIUMPH studies simultaneously, each targeting different patient populations and conditions.
TRIUMPH-4 results and dosing insights
The TRIUMPH-4 trial focused on adults with obesity and knee osteoarthritis. Participants taking retatrutide 12mg lost an average of 28.7% of their body weight at 68 weeks. That translates to an average of 71.2 pounds lost. These results surpassed even the impressive phase 2 data, and they used a refined titration schedule that incorporated lessons from the earlier trial. For perspective on what these numbers mean in practice, our peptide transformation guide documents real-world body composition changes, and the peptide research overview places these results in the broader context of weight management science.
The phase 3 trials also tested a 4mg maintenance dose in addition to the 9mg and 12mg doses. This is significant because it suggests that lower maintenance doses may be sufficient for some populations, particularly those using retatrutide for conditions other than maximum weight loss. The phase 3 titration schedule follows the same principle of 4-week escalation steps but with slightly adjusted intermediate doses.
Updated phase 3 titration pathway
The phase 3 schedule uses the following escalation:
Weeks 1-4: 2mg weekly
Weeks 5-8: 4mg weekly
Weeks 9-12: 8mg weekly
Week 13+: Maintenance dose (4mg, 9mg, or 12mg depending on assignment)
The introduction of a 9mg dose option is interesting. It sits between the 8mg and 12mg levels tested in phase 2, offering a middle ground for individuals who find 12mg difficult to tolerate but want more effect than 8mg provides. This 9mg option may become the most commonly prescribed dose when retatrutide receives FDA approval, which analysts expect could happen as early as 2027.
Seven additional phase 3 readouts are expected throughout this year, covering a range of conditions including type 2 diabetes, obstructive sleep apnea, chronic low back pain, cardiovascular outcomes, and metabolic dysfunction-associated steatotic liver disease. Each of these trials may produce slightly different dosing recommendations tailored to the specific condition being treated.
Retatrutide dose schedule compared to tirzepatide and semaglutide
Understanding how the retatrutide dose schedule differs from the two currently available GLP-1 agonists helps put the titration timeline in perspective. Each peptide has a different escalation pace, different dose steps, and different maintenance ranges.
Side-by-side titration comparison
Feature | Retatrutide | Tirzepatide | Semaglutide |
|---|---|---|---|
Receptors targeted | GLP-1, GIP, glucagon | GLP-1, GIP | GLP-1 only |
Starting dose | 2mg weekly | 2.5mg weekly | 0.25mg weekly |
Escalation interval | Every 4 weeks | Every 4 weeks | Every 4 weeks |
Maintenance dose range | 8-12mg | 5-15mg | 1.7-2.4mg |
Time to maintenance | 12-16 weeks | 16-20 weeks | 16-20 weeks |
Max weight loss (trials) | 24.2% at 48 weeks | 22.5% at 72 weeks | 14.9% at 68 weeks |
Injection frequency | Once weekly | Once weekly | Once weekly |
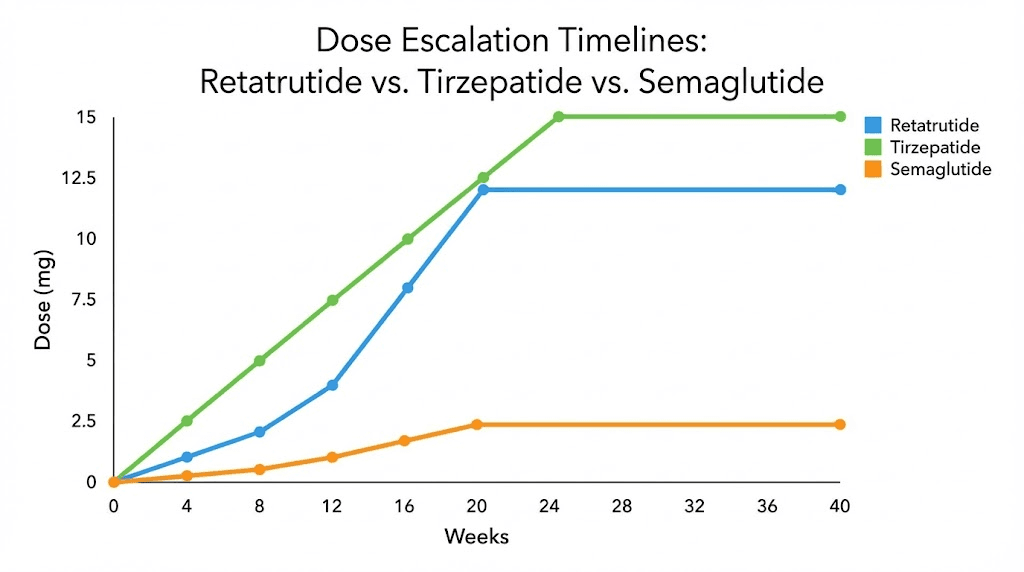
The most striking difference is the efficiency. Retatrutide achieves greater weight loss in less time. The 24.2% reduction at 48 weeks exceeds tirzepatide results that took 72 weeks to achieve 22.5%, and far surpasses semaglutide results of 14.9% at 68 weeks. This accelerated timeline is directly attributable to the glucagon receptor activation, which adds the thermogenic and lipolytic effects that single and dual agonists lack.
For researchers transitioning from semaglutide or tirzepatide to retatrutide, the dose schedule requires a fresh start. You cannot simply cross-taper from one peptide to another. The triple receptor profile means your body needs to adapt to the glucagon receptor activation regardless of your prior experience with GLP-1 or GLP-1/GIP agonists. Always start at 2mg and follow the standard or conservative escalation schedule.
Why retatrutide reaches maintenance faster
Semaglutide takes 16 to 20 weeks to reach its maximum dose of 2.4mg because the escalation uses smaller incremental steps: 0.25mg to 0.5mg to 1mg to 1.7mg to 2.4mg. Each step is roughly a doubling, giving five escalation periods. Semaglutide dosing in units can be confusing because the concentrations vary between formulations.
Tirzepatide follows a similar pattern with steps at 2.5mg, 5mg, 7.5mg, 10mg, 12.5mg, and 15mg, requiring potentially six escalation periods.
Retatrutide uses fewer, larger jumps: 2mg, 4mg, 8mg, 12mg. Three escalation steps instead of four or five. The 4-week interval at each step means you can reach 12mg maintenance by week 13, faster than either alternative peptide. This efficiency reflects the designers understanding that the triple receptor profile provides robust efficacy even at the earlier dose levels, allowing for a more streamlined escalation.
Managing side effects during dose escalation
Gastrointestinal side effects are the primary challenge during retatrutide dose escalation. The phase 2 trial reported that GI events were the most common adverse effects across all dose groups, and they were dose-dependent, meaning they increased in frequency and severity as the dose went up. However, these events were mostly mild to moderate in severity and were partially mitigated by using a lower starting dose.
What to expect at each dose level
At 2mg: Most researchers experience minimal side effects. Some notice mild nausea during the first 2 to 3 days after the initial injection. This typically resolves quickly. A small percentage report decreased appetite, which is actually the desired effect, not a side effect. Understanding peptide safety helps set appropriate expectations before starting any new protocol.
At 4mg: Nausea becomes more common, affecting approximately 20 to 30% of users. This usually peaks on days 1 to 2 after the injection and subsides by day 3 or 4. Constipation may develop as gastric emptying slows more noticeably. Some researchers report mild headaches during the first week at this dose.
At 8mg: This is the dose where side effects are most pronounced during the initial adjustment. Up to 40 to 50% of researchers report nausea during the first week at 8mg. Diarrhea or loose stools may alternate with constipation. Some experience increased heart rate and body warmth from the thermogenic glucagon receptor activation. These symptoms typically normalize within 10 to 14 days.
At 12mg: Similar GI symptoms to the 8mg transition, though the body has already adapted to much of the receptor activation by this point. Most researchers find the 8mg to 12mg transition more manageable than the 4mg to 8mg transition, possibly because the GI system has already adapted to substantial receptor agonism. The key side effect at this level is the sustained thermogenic effect, which some experience as increased sweating or feeling warmer than usual.
Practical side effect management strategies
These strategies are drawn from clinical trial protocols and practical experience. They apply at every dose level but become most important during the 4mg to 8mg and 8mg to 12mg transitions.
Dietary modifications that help:
Eat smaller, more frequent meals instead of large ones
Prioritize protein-forward meals, as protein is easier to digest when gastric emptying is slowed
Avoid high-fat meals, which take longer to digest and can worsen nausea
Eat slowly and stop before you feel full, as the sensation of fullness hits faster on retatrutide
Stay hydrated with slow, steady sipping rather than drinking large amounts at once
Timing strategies:
Take your weekly injection at a consistent time each week
Many researchers prefer evening injections so that the peak nausea period occurs during sleep
Plan your dose increase days on weekends or rest days when GI symptoms are less disruptive
Stay upright for at least 30 minutes after eating, as gravity helps with digestion when gastric emptying is slowed
Natural remedies for mild nausea:
Ginger has demonstrated anti-nausea properties in multiple studies and can help manage mild GI symptoms during dose transitions. Ginger tea, ginger chews, or ginger capsules taken 30 minutes before meals can reduce nausea without interfering with the peptide mechanism. Peppermint oil capsules have also shown benefit for GI discomfort in small studies. These natural approaches complement the gradual dose schedule by making each transition more comfortable. The guide to mixing peptides with water covers proper preparation that also affects GI tolerability, and our overview of peptide benefits and risks frames side effect management within the larger context of expected outcomes.
When to extend a dose step
The standard schedule calls for 4-week intervals between dose increases. But the clinical trial data supports extending any step by 2 to 4 additional weeks if side effects remain problematic. This is not a setback. It is a legitimate modification that does not reduce long-term effectiveness.
Extend your current dose step if:
Nausea persists beyond 10 days at the current dose
You are experiencing vomiting more than twice per week
Diarrhea is disrupting daily activities
You have lost significant amounts of food intake due to GI symptoms
Your quality of life is substantially affected
Stay at the current dose for an additional 2 to 4 weeks, then attempt the escalation again. Most researchers find that the extra adaptation time makes the subsequent increase much more tolerable. If you have tried twice and still cannot tolerate the next dose level, your current dose may be your optimal maintenance dose. The complete retatrutide dose guide covers maintenance dose selection in more detail.
Reconstitution and injection volume calculations for each dose step
Knowing the dose schedule is only half the equation. You also need to know exactly how much liquid to draw for each injection based on your vial concentration. This section provides the practical calculations for the most common vial sizes.
10mg vial reconstitution
A 10mg vial reconstituted with 2ml of bacteriostatic water produces a concentration of 5mg per ml. At this concentration:
Dose | Volume to inject | Insulin syringe units |
|---|---|---|
2mg | 0.40ml | 40 units |
4mg | 0.80ml | 80 units |
8mg | 1.60ml | Not practical from single vial |
12mg | 2.40ml | Not practical from single vial |
The 10mg vial at 5mg/ml concentration works well for the 2mg and 4mg dose steps. For the 8mg and 12mg steps, you would need to either use a higher concentration or draw from two vials. A more practical approach is to add only 1ml of bacteriostatic water, creating a 10mg/ml concentration.
With 10mg/ml concentration from a 10mg vial:
Dose | Volume to inject | Insulin syringe units |
|---|---|---|
2mg | 0.20ml | 20 units |
4mg | 0.40ml | 40 units |
8mg | 0.80ml | 80 units |
12mg | 1.20ml | Not ideal for insulin syringe |
20mg vial reconstitution
A 20mg vial offers more flexibility. Reconstituted with 2ml of bacteriostatic water, it produces 10mg per ml. This is the most practical concentration for the full dose schedule.
Dose | Volume to inject | Insulin syringe units |
|---|---|---|
2mg | 0.20ml | 20 units |
4mg | 0.40ml | 40 units |
8mg | 0.80ml | 80 units |
12mg | 1.20ml | Use 3ml syringe or two draws |
The 20mg vial at 10mg/ml concentration is the most versatile option. It keeps injection volumes manageable across all dose levels. At the 12mg maintenance dose, each vial provides slightly less than two full doses (20mg total divided by 12mg per dose = 1.67 doses). Plan your vial supply accordingly to avoid running short during the maintenance phase.
For precise calculations at any concentration, use the peptide reconstitution calculator available on our site. You can also reference our guide on how to reconstitute peptides for step-by-step instructions on proper mixing technique, and our bacteriostatic water guide covers exactly how much water to use for different vial sizes.
Storage after reconstitution
Once reconstituted, retatrutide should be stored at 2 to 8 degrees Celsius (35.6 to 46.4 degrees Fahrenheit) in the refrigerator. The reconstituted solution remains stable for 2 to 4 weeks under proper refrigeration. Do not freeze reconstituted peptides. Do not leave them at room temperature for extended periods. For a complete breakdown of peptide storage after reconstitution, our dedicated guide covers temperature ranges, shelf life, and stability indicators.
Unreconstituted lyophilized powder can be stored at room temperature, though refrigeration is preferred for long-term storage. The peptide storage guide provides comprehensive storage protocols for all forms and conditions. For specific information on how long peptides last in the fridge and room temperature stability, our dedicated guides cover every storage scenario. The reconstituted peptide shelf life guide is particularly relevant for managing multi-week vial use during the dose schedule.
Injection technique and site rotation on a weekly schedule
Retatrutide is administered subcutaneously once per week. The injection technique is straightforward, but proper site rotation becomes important on a weekly dosing schedule to prevent lipodystrophy and ensure consistent absorption.
Preferred injection sites
The most common subcutaneous injection sites for weekly retatrutide are:
Abdomen: The area around the navel, at least 2 inches away from the belly button. This is the most popular site due to easy access and consistent absorption. Avoid the area directly around the navel. For abdominal fat reduction, injection site does not affect local fat loss.
Thigh: The front or outer portion of the upper thigh. This site works well for those who find abdominal injections uncomfortable.
Upper arm: The back of the upper arm. This site requires either flexibility or assistance from another person. The peptide injection pen guide covers devices that make upper arm self-injection easier.
Rotate between at least two of these sites on a weekly basis. A simple rotation pattern might alternate between left abdomen, right abdomen, left thigh, and right thigh over a 4-week period. This prevents any single area from receiving repeated injections, which can cause tissue changes over time. Our guide on peptide injections covers technique in complete detail, and the peptide injection overview explains the fundamentals for those new to subcutaneous administration.
Timing your weekly injection
Consistency matters more than the specific day or time you choose. Pick a day of the week that works for your schedule and stick with it. If you inject every Tuesday evening, continue that pattern throughout your dose schedule. For those new to peptide protocols, building this weekly habit from day one makes the entire dose schedule easier to follow. Our guide on what peptides are used for provides broader context for researchers beginning their first protocol.
If you miss a dose, take it as soon as you remember, provided it is within 3 days of your scheduled injection. If more than 3 days have passed, skip that dose and resume your regular schedule. Do not double up on doses to make up for a missed injection. Missing a single dose during the dose schedule does not require restarting the titration. Simply continue at your current dose level on your next scheduled injection day.
Retatrutide has a half-life of approximately 6 days, which supports the once-weekly dosing frequency. This long half-life means the drug maintains therapeutic levels between injections, and a single missed dose does not cause dramatic fluctuations in blood levels. For comparison, most injectable peptides have much shorter half-lives requiring more frequent dosing. The legal status of peptides varies by region, so researchers should verify their local regulations before beginning any protocol.
Dose schedule modifications for specific goals
While the standard schedule targets 12mg maintenance, not every researcher aims for the same outcome. Different goals may call for different target maintenance doses, and the escalation schedule should be adjusted accordingly.
Maximum weight loss protocol (12mg target)
Follow the standard or conservative schedule as outlined above. The 12mg dose produced the highest weight loss in clinical trials and is the target for researchers prioritizing maximum fat reduction. This protocol requires the full escalation through 2mg, 4mg, 8mg, and 12mg over 12 to 24 weeks depending on the schedule chosen. For those specifically targeting visceral fat reduction, the 12mg dose provides the strongest metabolic activation. The best fat burning peptide comparison shows how retatrutide stacks up against alternatives at this dose level.
Expected outcomes based on trial data:
Average weight loss of 24.2% at 48 weeks (phase 2)
Average weight loss of 28.7% at 68 weeks (phase 3, TRIUMPH-4)
100% of participants achieved 5% or greater weight loss
93% achieved 10% or greater
83% achieved 15% or greater
Moderate weight loss protocol (8mg target)
For researchers who want significant weight loss but have a lower tolerance for side effects, stopping the escalation at 8mg is a validated approach. The phase 2 trial showed 22.8% average weight loss at 48 weeks with the 8mg dose, only 1.4 percentage points less than the 12mg dose.
The schedule follows the standard pathway through 2mg and 4mg, then maintains at 8mg:
Weeks 1-4: 2mg weekly
Weeks 5-8: 4mg weekly
Week 9+: 8mg weekly (maintenance)
This reaches maintenance 4 weeks sooner than the 12mg protocol and avoids the final dose escalation that many researchers find most challenging. The 8mg dose provides 100% responder rate at the 5% weight loss threshold and 91% at the 10% threshold. For many people, these numbers are more than sufficient.
Lower dose protocol (4mg target)
The 4mg maintenance dose is appropriate for researchers who are particularly sensitive to GLP receptor agonists or who have more modest weight loss goals. At 4mg, the phase 2 trial showed 17.1% average weight loss at 48 weeks, which exceeds the maximum dose of semaglutide (14.9%) in its own trial.
Schedule:
Weeks 1-4: 2mg weekly
Week 5+: 4mg weekly (maintenance)
This protocol reaches maintenance by week 5 and provides clinically meaningful weight loss with the mildest side effect profile. It may be particularly suitable for researchers who have had difficulty tolerating other weight loss peptides or those who are using retatrutide for metabolic benefits beyond weight loss. The safest peptide options for women guide discusses tolerance considerations that often favor lower maintenance doses, and the peptides for men guide covers male-specific factors in dose selection.
Choosing your target maintenance dose
The right maintenance dose depends on several factors:
Factor | Suggests lower dose (4-8mg) | Suggests higher dose (12mg) |
|---|---|---|
Weight loss goal | Less than 15% body weight | 15% or more body weight |
GI tolerance | History of sensitivity | Generally tolerant |
Prior GLP-1 experience | First time using any agonist | Previous experience with semaglutide or tirzepatide |
BMI | 27-32 | 35+ |
Primary goal | Metabolic health improvement | Maximum fat reduction |
Timeline flexibility | No rush, prioritize comfort | Want fastest results possible |
Remember that you can always adjust your target dose based on how you respond. Starting with a 12mg target and settling at 8mg because it provides sufficient results with better tolerability is a perfectly valid approach. The dose schedule is a framework, not a rigid rule. SeekPeptides members access detailed protocol builders that help match the right maintenance dose to individual factors and goals.
Tracking your progress through the dose schedule
A structured tracking system helps you make informed decisions about dose escalation timing and identifies patterns that optimize your protocol. Without tracking, you are making dose schedule decisions based on memory and general impressions rather than data.
What to track weekly
At minimum, track these variables every week throughout your dose schedule. The peptide calculator for weight loss can help quantify your progress, and our free reconstitution calculator ensures your dose measurements remain accurate throughout the protocol:
Body composition metrics:
Body weight (same time, same conditions each week)
Waist circumference
Waist-to-hip ratio
Optional: body fat percentage if you have access to reliable measurement
Side effect monitoring:
Nausea frequency and severity (1-10 scale)
Digestive function (constipation, diarrhea, normal)
Appetite level (1-10 scale, where 10 is strongest appetite)
Energy levels throughout the day
Sleep quality
Any unusual symptoms
Protocol adherence:
Injection date and time
Injection site used
Exact dose and volume injected
Any missed or delayed doses
Using data to modify your schedule
Your tracking data tells you when to proceed with escalation and when to hold. Strong indicators that you are ready for the next dose step include:
GI side effects have fully resolved at the current dose
Appetite suppression has stabilized (not increasing or decreasing week to week)
Weight loss has slowed or plateaued at the current dose
Energy levels are stable and consistent
Sleep quality has returned to baseline
Indicators that you should hold at the current dose for another cycle include:
Persistent nausea beyond the first week at the current dose
Digestive issues that have not resolved
Weight loss is still progressing well (no need to increase if current dose is working)
Energy levels are still adjusting
Any concerning symptoms that need medical evaluation
The tracking data also helps identify your optimal maintenance dose. If you are achieving your weight loss goals at 8mg with minimal side effects, continuing to 12mg may not be necessary. If the data shows a clear response plateau at 4mg, that signals that a higher dose would likely provide additional benefit. For detailed peptide cycle planning, our guide covers how to use tracking data to optimize any peptide protocol.
Common dose schedule mistakes and how to avoid them
Even with a clear dose schedule, researchers commonly make errors that undermine their results. These mistakes range from impatience with the titration process to improper dose calculations. Avoiding them can mean the difference between a successful protocol and an abandoned one.
Mistake 1: skipping the starting dose
Some researchers, particularly those with prior experience on semaglutide or tirzepatide, assume they can skip the 2mg starting dose and begin at 4mg or higher. The clinical trial data specifically warns against this. Even though your body may have adapted to GLP-1 receptor activation from a previous peptide, the glucagon receptor activation in retatrutide is entirely new. Your body has not adapted to this component, and starting too high risks severe GI side effects that can derail the entire protocol.
Always start at 2mg. No exceptions.
Mistake 2: escalating based on calendar rather than response
The 4-week intervals are guidelines, not mandatory deadlines. If you are still experiencing significant side effects at week 4 of a dose step, escalating because the calendar says it is time is a mistake. The schedule should be response-driven, not purely time-driven. Use your tracking data to confirm readiness before each dose increase. The peptide stacking guide covers similar principles about responding to your body rather than following rigid timelines.
Mistake 3: reducing the dose when side effects occur instead of holding steady
When nausea or other GI symptoms appear after a dose increase, some researchers immediately drop back to the previous dose. This is usually unnecessary. Most GI side effects resolve within 7 to 14 days at the new dose level. Dropping back and then re-escalating later means you go through the adjustment period twice. Instead, hold at the current dose, implement the management strategies described earlier, and give your body the full 2 weeks to adapt before deciding to step back. Understanding the relationship between peptides and gut health provides useful context for why these GI adjustments are temporary rather than permanent.
Mistake 4: incorrect reconstitution leading to wrong doses
Math errors during peptide mixing are surprisingly common. If you add the wrong amount of bacteriostatic water, every subsequent injection will be at the wrong dose. A 20mg vial reconstituted with 4ml instead of 2ml gives you 5mg/ml instead of 10mg/ml, meaning you would need to inject double the volume at each dose step. Always verify your concentration calculation before the first injection and mark the vial with the concentration. Use our peptide calculator to double-check your math.
Mistake 5: comparing your results to others too early in the schedule
Weight loss during the dose escalation phase varies enormously between individuals. Some people lose significant weight during the first 4 weeks at 2mg. Others see minimal change until they reach 8mg or 12mg. Comparing your week-4 results to someone elses week-16 results leads to unnecessary discouragement. The phase 2 trial measured outcomes at 24 and 48 weeks for a reason. Short-term comparisons during the escalation phase are not meaningful indicators of eventual outcomes. Understanding how long peptides take to work across different categories provides a realistic framework for setting expectations during the escalation phase.
Mistake 6: not planning vial supply in advance
Running out of retatrutide mid-schedule forces an unplanned break that can disrupt the dose escalation. Calculate your total peptide supply needs before starting. For a standard 48-week protocol at 12mg maintenance, you need substantially more peptide than the starting phase suggests. Plan ahead to ensure continuous supply through the entire schedule. The vendor selection guide helps identify reliable sources, and understanding how long peptides last in powder form informs bulk purchasing decisions. Our peptide expiration guide covers shelf life considerations for long-term supply planning.
Retatrutide dose schedule for combination protocols
Some researchers combine retatrutide with other peptides or compounds. While the clinical trials studied retatrutide as monotherapy, real-world protocols sometimes incorporate complementary agents. Understanding how these combinations affect the dose schedule is important for safety.
Retatrutide with exercise protocols
The dose schedule does not need modification for exercise. However, the appetite suppression at higher doses can make it challenging to consume adequate calories to support intense training. Researchers combining retatrutide with strength training protocols should pay particular attention to protein intake, aiming for 1.0 to 1.2 grams per kilogram of body weight daily to preserve lean mass during weight loss. Those focused on maintaining athletic performance during weight loss will find specific strategies in our dedicated guide, and the muscle growth peptide overview covers complementary approaches to lean mass preservation.
Timing exercise relative to the weekly injection is worth considering. Some researchers prefer to inject on rest days, as the first 24 to 48 hours after injection tend to produce the most pronounced GI effects. Others inject on training days, finding that exercise actually reduces nausea. This is individual and worth experimenting with during the early dose steps. The best peptides for energy guide covers compounds that can support workout performance during aggressive weight loss phases.
Combining with other peptides
Retatrutide should not be combined with other GLP-1 agonists like semaglutide or tirzepatide. The receptor overlap would create unpredictable dose-response relationships and increase the risk of severe GI side effects. The triple receptor profile of retatrutide already covers what dual agonists like tirzepatide provide.
Peptides that target different systems entirely, such as BPC-157 for healing or TB-500 for tissue repair, do not interact with the GLP-1/GIP/glucagon pathways and can theoretically be used alongside retatrutide without modifying the dose schedule. However, any combination protocol should be approached with caution, and our guide on combining multiple peptides covers the principles of safe stacking. The peptide stack calculator can help plan multi-peptide protocols.
Cagrilintide combinations
The emerging research on cagrilintide and semaglutide combinations (CagriSema) has prompted questions about whether cagrilintide could be added to retatrutide. Cagrilintide is an amylin receptor agonist, which operates through a different pathway than any of the three receptors retatrutide targets. While no clinical data exists on this specific combination, the cagrilintide dosing protocols and amylin receptor agonist research suggest it could be complementary. This remains speculative and should not be attempted without appropriate medical guidance.
Long-term maintenance after completing dose escalation
Once you reach your target maintenance dose and complete the initial adaptation period, the dose schedule enters its long-term phase. This phase is less structured than the escalation but still requires attention to specific factors that affect ongoing success.
Duration of maintenance dosing
The phase 2 trial ran for 48 weeks, and the weight loss curve had not fully plateaued by that point. The phase 3 TRIUMPH-4 trial extended to 68 weeks and showed continued weight loss throughout, suggesting that longer maintenance periods produce better outcomes. There is currently no established maximum duration for retatrutide use, as the drug is still in clinical development.
Based on available data, most protocols plan for a minimum of 48 weeks of total treatment, including the escalation phase. Some researchers continue indefinitely, while others cycle off after reaching their weight loss goals. The decision to continue, reduce the dose, or discontinue should be based on individual response and goals. Our peptide cycle planning guide covers general principles for determining optimal protocol duration, and the what are peptides introduction helps researchers understand the broader framework of peptide-based protocols.
Dose reduction for maintenance
Some researchers find that they can maintain their weight loss at a lower dose than what was needed to achieve it. After reaching their goal weight on 12mg, they gradually reduce to 8mg or even 4mg as a maintenance dose. This approach reduces the long-term side effect burden and cost of peptide therapy.
If considering a dose reduction for maintenance:
Wait until weight has stabilized for at least 4 weeks at your current dose
Reduce by one dose step (e.g., 12mg to 8mg), do not jump multiple steps
Monitor weight closely for 8 weeks after the reduction
If weight begins to increase, return to the previous maintenance dose
The phase 3 trials specifically tested 4mg as a maintenance dose, suggesting Lilly sees viability in lower maintenance doses
What happens if you stop
Weight regain after discontinuing GLP-1 agonists is well documented with semaglutide and tirzepatide. The same pattern is expected with retatrutide, though long-term discontinuation data is not yet available. The weight regain patterns observed with other agonists suggest that maintaining lifestyle changes during the treatment period is crucial for sustaining results after discontinuation.
If you plan to discontinue, a gradual taper over 4 to 8 weeks (reducing by one dose step every 2 to 4 weeks) is generally preferred over abrupt cessation. This allows your appetite regulation systems to gradually return to baseline rather than rebounding sharply. The taper follows the escalation schedule in reverse: 12mg to 8mg to 4mg to 2mg, then stop. Some researchers transition to other fat loss peptides or longevity-focused protocols after completing a retatrutide cycle, using the metabolic improvements as a foundation for further optimization.
Nutritional strategies aligned to each dose schedule phase
Your nutrition approach should evolve alongside your dose schedule. The appetite changes at each dose level create different nutritional challenges, and matching your eating strategy to the current phase prevents muscle loss, nutrient deficiencies, and unnecessary discomfort.
Nutrition during the 2mg phase (weeks 1-4)
At 2mg, appetite suppression is mild. This is the easiest phase nutritionally because you can still eat relatively normally. Use this period to establish baseline habits that will serve you during the higher dose phases. Focus on increasing protein intake to 1.0 to 1.2 grams per kilogram of body weight, as this becomes critical later when appetite suppression makes eating more difficult. Start tracking your caloric intake patterns to understand your baseline before the peptide effects intensify.
Hydration habits matter from day one. The GLP-1 mediated slowing of gastric emptying can cause mild dehydration if fluid intake drops. Aim for 2 to 3 liters of water daily. Electrolyte supplementation becomes more important at higher doses, but establishing the habit now prevents problems later.
Nutrition during the 4mg phase (weeks 5-8)
Appetite changes become noticeable at 4mg. Most researchers find that meal portions naturally decrease by 20 to 30%. The key challenge is maintaining adequate nutrition despite reduced appetite. Calorie-dense, nutrient-rich foods become your priority. Think lean proteins with healthy fats, nutrient-dense vegetables, and whole grains in smaller portions.
This is when meal timing starts to matter. Many researchers on the retatrutide dose schedule find that eating 4 to 5 smaller meals works better than 2 to 3 larger ones. The slowed gastric emptying means large meals sit uncomfortably. Smaller, more frequent meals maintain nutrient intake without triggering the nausea that large portions can cause at this dose. Researchers working on muscle preservation goals should distribute protein evenly across all meals rather than concentrating it in one or two sittings.
Nutrition during the 8mg and 12mg phases
At higher doses, appetite suppression becomes substantial. Some researchers report barely feeling hungry at all. While this drives rapid weight loss, it creates a real risk of inadequate protein and micronutrient intake. Protein shakes become a practical tool during these phases, as liquid calories are often easier to consume than solid food when appetite is heavily suppressed.
A practical approach for the 8mg and 12mg phases includes a protein shake in the morning (30 to 40 grams of protein), a small nutrient-dense meal at lunch, a protein-rich snack in the afternoon, and a balanced dinner focused on protein and vegetables. Total daily calories should not drop below 1,200 for women or 1,500 for men, even at peak appetite suppression. Dropping too low risks muscle catabolism and metabolic adaptation that can slow long-term progress. Resources on optimizing fat loss with peptides cover the nutritional balance needed for healthy body composition changes.
Supplements worth considering during the higher dose phases include a quality multivitamin (to cover micronutrient gaps from reduced food intake), vitamin D (often depleted during significant weight loss), B vitamins for energy metabolism, and magnesium for muscle function and sleep quality. The anti-aging benefits of adequate nutrition become particularly relevant during aggressive weight loss protocols, as nutrient deficiencies can accelerate age-related decline.
Understanding the pharmacokinetics behind the dose schedule
The timing of each dose step in the retatrutide schedule is not arbitrary. It reflects the pharmacokinetic properties of the molecule, specifically its half-life, time to steady state, and receptor binding dynamics. Understanding these properties helps explain why 4 weeks works as the standard escalation interval.
Half-life and steady state considerations
Retatrutide has a half-life of approximately 6 days. In pharmacology, steady state is typically reached after 4 to 5 half-lives. For retatrutide, this means approximately 24 to 30 days, or roughly 4 weeks. This is exactly why the dose schedule uses 4-week intervals. At the end of each 4-week period, your blood levels have reached a stable plateau at the current dose. The body has fully adapted to that concentration, and adding more will produce a predictable increase rather than an unpredictable spike.
The acylation of the retatrutide molecule is what gives it this long half-life. A fatty acid chain is attached to the peptide, which allows it to bind to albumin in the blood. This albumin binding creates a reservoir effect, slowly releasing the active molecule over days rather than hours. This is the same pharmacological strategy used in tirzepatide and semaglutide to enable weekly dosing. Understanding how peptides work at the molecular level helps researchers appreciate why the dose schedule follows specific timing.
Why doubling works as an escalation strategy
The dose steps in the retatrutide schedule roughly double at each level: 2mg to 4mg to 8mg, with the final step from 8mg to 12mg being a 50% increase. This doubling approach is deliberate. At each doubling, receptor occupancy increases significantly but not overwhelmingly. The body experiences a meaningful increase in effect without the shock of, say, a tripling or quadrupling of the dose.
The smaller final step from 8mg to 12mg (a 50% increase rather than a 100% doubling) reflects the finding that GI tolerability improves at higher doses once the body has already adapted to substantial receptor activation. By the time you reach 8mg, your GI system has adapted through two previous escalation cycles, and a 50% increase is proportionally less disruptive than the doublings at lower levels.
This escalation math also explains why the 20mg vial is the most practical option for the full dose schedule. It provides enough peptide for the higher dose levels without requiring multiple vials per injection.
Special populations and dose schedule adjustments
Not every researcher fits the standard profile studied in clinical trials. Certain populations may need modifications to the dose schedule based on their unique physiological characteristics.
Dose schedule considerations by body weight
The clinical trials used fixed doses (not weight-based dosing), which means a 200-pound person and a 300-pound person received the same milligram amount. In practice, this means the effective dose-per-kilogram varies significantly between individuals. Lighter individuals may experience stronger effects (and more side effects) at each dose level, while heavier individuals may need the full 12mg maintenance dose to achieve optimal results.
For researchers weighing under 180 pounds (82 kg), the conservative 6-week escalation schedule is often recommended. The fixed doses represent a higher per-kilogram exposure in lighter individuals, increasing the likelihood of significant GI effects at each step. The peptide dosage calculation guide explains weight-based dosing principles for peptides where this approach is available.
For researchers weighing over 300 pounds (136 kg), the standard 4-week escalation is typically well tolerated, and the 12mg maintenance dose is strongly recommended. Higher body mass dilutes the per-kilogram dose, which can reduce both the effects and side effects at lower dose levels. These individuals may not notice significant appetite suppression until reaching 8mg or higher. The weight loss and muscle gain guide covers strategies for larger individuals pursuing body recomposition.
Gender-based considerations
The phase 2 trial included both men and women, and the results did not show statistically significant differences in weight loss between genders at matched doses. However, anecdotal reports suggest that women may experience more pronounced nausea at the 4mg and 8mg dose steps, particularly around menstruation when hormonal fluctuations can amplify GI sensitivity.
Women following the retatrutide dose schedule may benefit from planning dose escalations to avoid the luteal phase of their menstrual cycle, when GI sensitivity tends to be highest. Timing the increase for the follicular phase (days 1 through 14 of the cycle) can reduce the overlap between hormonal GI effects and dose-escalation GI effects. Our guides on peptides for menopause weight loss and peptides for women over 40 cover additional female-specific considerations for weight loss peptide protocols.
Dose schedule with type 2 diabetes
Retatrutide is being studied for type 2 diabetes in separate clinical trials. The dose schedule for diabetic populations may differ from the weight loss schedule because the GLP-1 and GIP receptor activation directly affects blood sugar regulation. Researchers with type 2 diabetes following a retatrutide dose schedule need to monitor blood glucose closely during each escalation step, as the improved insulin sensitivity can cause hypoglycemia if diabetes medications are not adjusted accordingly.
The phase 2 diabetes trial (published in The Lancet) used the same general titration framework but with more intensive metabolic monitoring. If you are using retatrutide alongside diabetes medications, the dose schedule remains the same, but medication adjustments should be anticipated at each step, particularly at the 4mg and 8mg transitions where GLP-1 receptor activation produces the most significant glucose-lowering effects.
Cost planning across the dose schedule
The total cost of a retatrutide protocol varies significantly depending on which phase of the dose schedule you are in. The escalation phase uses less peptide per week than the maintenance phase, so monthly costs increase as you progress through the schedule.
Peptide consumption by schedule phase
Phase | Weekly dose | 4-week consumption | Vials needed (20mg) |
|---|---|---|---|
Weeks 1-4 | 2mg | 8mg | Less than 1 vial |
Weeks 5-8 | 4mg | 16mg | 1 vial |
Weeks 9-12 | 8mg | 32mg | 2 vials |
Weeks 13-16 | 12mg | 48mg | 3 vials |
Each month at maintenance | 12mg | 48mg | 3 vials |
Over a standard 48-week protocol, the total retatrutide consumption breaks down roughly as follows: 8mg for the first month, 16mg for the second, 32mg for the third, and 48mg per month for the remaining 36 weeks. Total consumption is approximately 8 + 16 + 32 + (48 x 9) = 488mg over 48 weeks. The retatrutide cost guide provides detailed pricing analysis based on current market rates, and the peptide cost calculator helps estimate your specific budget needs.
Planning your supply in advance prevents the expensive mistake of ordering emergency shipments mid-protocol. Most researchers find that ordering in bulk at the start provides better value than purchasing month by month. Consider that the overall cost of peptide therapy is more manageable when planned as a complete protocol rather than incremental purchases.
Transitioning between different weight loss peptides and the dose schedule
Researchers who have previously used semaglutide or tirzepatide often want to transition to retatrutide for its superior weight loss efficacy. The transition process requires careful planning because you cannot simply swap one peptide for another mid-protocol.
Transitioning from semaglutide to retatrutide
If you are currently on semaglutide, the transition involves stopping semaglutide and allowing a washout period before starting the retatrutide dose schedule. Semaglutide has a half-life of approximately 7 days, so a washout of 2 to 3 weeks allows blood levels to drop to minimal levels. After the washout, begin the retatrutide dose schedule at 2mg, following the standard escalation.
Some researchers prefer a direct switch without a washout, stopping semaglutide one week and starting retatrutide at 2mg the following week. This approach minimizes the appetite rebound that can occur during a washout but may increase GI side effects during the first 2 weeks of retatrutide as both receptor systems are in flux. The oral tirzepatide guide covers similar transition considerations for that peptide.
Transitioning from tirzepatide to retatrutide
The transition from tirzepatide is similar but involves an important nuance. Tirzepatide already activates GLP-1 and GIP receptors, so your body is adapted to dual receptor activation. The primary new stimulus from retatrutide is the glucagon receptor activation. In theory, this could make the transition smoother for GI effects related to GLP-1 and GIP, while the glucagon-mediated effects (thermogenesis, increased heart rate) would be entirely new.
The recommended approach is still to start retatrutide at 2mg regardless of your previous tirzepatide dose. The 2mg starting dose gives your body time to integrate the new glucagon receptor activation with the familiar GLP-1 and GIP effects. Rushing this process offers no benefit and carries real risk of severe side effects that could compromise the entire protocol. For those tracking their tirzepatide results and comparing them to expected retatrutide outcomes, the transition data from the clinical trials provides useful benchmarks.
Running retatrutide after completing a semaglutide or tirzepatide protocol
If you have completed a full semaglutide or tirzepatide protocol and are starting retatrutide as a new treatment after a break, the standard dose schedule applies without modification. Your body has returned to baseline during the off period, and the full escalation from 2mg upward is necessary regardless of prior experience. The peptide cycle planning guide helps structure transitions between different protocols with appropriate timing.
The future of retatrutide dosing: what clinical trials tell us
The dose schedule is likely to evolve as more phase 3 data becomes available. Several aspects of the current dosing framework may change based on ongoing research, and staying informed about these developments helps researchers plan future protocols.
The 9mg dose option
The phase 3 TRIUMPH trials introduced a 9mg maintenance dose that was not tested in phase 2. This intermediate dose sits between the well-studied 8mg and 12mg levels and may become the most commonly recommended dose when retatrutide reaches the market. The rationale is simple: 8mg provides nearly as much weight loss as 12mg (22.8% vs 24.2%) with a better side effect profile. A 9mg dose could potentially capture the small additional benefit of higher dosing while maintaining most of the tolerability advantage of 8mg. The retatrutide purchase guide will be updated as new dosing recommendations emerge from these trials.
Personalized dose schedules
The one-size-fits-all approach to dose scheduling is a limitation of clinical trial design. In practice, the optimal dose schedule likely varies by body weight, metabolic baseline, genetic factors, and individual receptor sensitivity. Future research may identify biomarkers that predict the ideal maintenance dose and escalation speed for individual patients, allowing personalized peptide protocols that maximize efficacy while minimizing side effects.
SeekPeptides stays current with the latest research developments and updates dosing protocols as new evidence emerges. Members access regularly updated protocol recommendations based on the most recent clinical data, community experience, and expert analysis. For researchers serious about optimizing their retatrutide dose schedule, having access to current, evidence-based guidance makes the difference between a good protocol and a great one.
For researchers serious about getting their dose schedule right, SeekPeptides provides the most comprehensive peptide education platform available, with evidence-based protocols, dosing calculators, community support, and expert guidance that help you navigate every phase of the titration process with confidence.
Frequently asked questions
How long does it take to reach the full 12mg retatrutide dose?
The standard dose schedule takes 12 to 16 weeks to reach the 12mg maintenance dose, following a 4-week escalation pattern through 2mg, 4mg, 8mg, and 12mg. The conservative schedule extends this to 18 to 24 weeks with 6-week intervals between dose increases. Both approaches produce equivalent long-term results, with the conservative schedule offering fewer GI side effects during the escalation period. Use our retatrutide dosage calculator to plan your specific timeline.
Can I skip directly to a higher dose if I have experience with semaglutide?
No. Even with prior semaglutide experience, you must start retatrutide at 2mg. The glucagon receptor activation is entirely new to your body, and the triple receptor profile creates a different physiological response than single or dual agonists. The clinical trial protocol required all participants to start at 2mg regardless of prior GLP-1 experience. Skipping the starting dose significantly increases the risk of severe gastrointestinal side effects.
What should I do if I miss a weekly dose during the dose schedule?
If you remember within 3 days of your scheduled injection, take the dose immediately and resume your regular weekly schedule. If more than 3 days have passed, skip the missed dose and take your next scheduled dose on time. Do not double the dose. A single missed injection does not require restarting the dose escalation. Continue at your current dose level. Retatrutide has a half-life of approximately 6 days, so a brief interruption does not eliminate all therapeutic effect. The peptide dosing guide covers missed dose protocols for other peptides as well.
Is the 4mg maintenance dose effective enough for weight loss?
Yes. The phase 2 trial showed 17.1% average body weight reduction at 48 weeks with the 4mg dose. This exceeds the maximum weight loss seen with semaglutide at its highest dose (14.9% at 68 weeks). The 4mg dose offers a substantially milder side effect profile and may be the optimal choice for researchers with moderate weight loss goals or higher sensitivity to GLP receptor agonists. For those weighing alternatives, the comprehensive weight loss peptide comparison ranks all available options by efficacy and tolerability.
How does the retatrutide dose schedule compare to tirzepatide dosing?
Retatrutide reaches maintenance faster than tirzepatide. Retatrutide uses three escalation steps (2mg to 4mg to 8mg to 12mg) over 12 to 16 weeks, while tirzepatide uses up to six steps (2.5mg through 15mg) over 16 to 24 weeks. Despite the faster escalation, retatrutide achieves greater weight loss (24.2% at 48 weeks versus 22.5% at 72 weeks) due to the additional glucagon receptor activation that increases energy expenditure and fat mobilization.
Can I stay at 8mg and still get good results without going to 12mg?
Absolutely. The 8mg dose produced 22.8% average weight loss at 48 weeks in the phase 2 trial, with 100% of participants losing at least 5% and 91% losing at least 10% of body weight. The difference between 8mg (22.8%) and 12mg (24.2%) is only 1.4 percentage points. For many researchers, the improved tolerability at 8mg makes it the better practical choice. The complete retatrutide dose guide covers the factors that help determine your optimal maintenance dose.
What happens to the dose schedule if I experience severe nausea?
If nausea persists beyond 10 to 14 days at a new dose level, extend your stay at that dose for an additional 2 to 4 weeks before attempting escalation again. Implement dietary modifications (smaller protein-forward meals, avoid high-fat foods), consider evening injections to sleep through peak nausea, and try ginger supplements for mild symptom relief. If you cannot tolerate a dose level after two attempts, your current dose may be your optimal maintenance dose. The dose schedule is designed to be flexible, and staying at a lower maintenance dose is always preferable to abandoning the protocol entirely.
How much weight can I expect to lose during the escalation phase before reaching maintenance?
Weight loss begins during the escalation phase, but the rate varies significantly between individuals. Some researchers lose 3 to 5% of body weight during the first 12 weeks of escalation, while others see minimal change until reaching 8mg or higher. The clinical trial measured results at 24 and 48 weeks, not during individual dose steps, so specific per-step weight loss data is limited. Focus on the long-term trajectory rather than weekly results during the escalation phase. The best weight loss peptide guide provides broader context for comparing weight loss timelines across different compounds.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your dose schedule stay consistent, your titration stay smooth, and your results stay on track.