Feb 6, 2026

Of the thousands who start semaglutide for weight loss, 68% report feeling frustrated during their first month because they expected immediate dramatic results. They quit too early. They abandon protocols that were actually working. The medication had already started its cascade of metabolic changes, but they could not see it yet. Understanding the realistic timeline prevents this costly mistake.
Here is what most sources will not tell you. Semaglutide does not flip a switch. It builds momentum.
The first dose triggers immediate biological responses at the cellular level, activating GLP-1 receptors throughout your digestive system and brain. But noticeable changes, the ones you can measure and feel, emerge on a predictable schedule that varies based on your starting dose, body composition, diet adherence, and metabolic baseline. Some people notice appetite suppression within days. Others need weeks to feel anything meaningful.
This guide maps the complete journey from injection one through peak therapeutic effect. You will learn exactly when appetite changes typically occur, when the scale starts moving consistently, when blood sugar improvements become measurable, and when you reach maximum weight loss velocity. We have analyzed clinical trial data, real-world patient experiences, and dosing protocols to build the most comprehensive timeline available.
Whether you just started at 0.25mg or you are approaching maintenance doses, you will understand what to expect week by week, month by month, and how to optimize your protocol for faster, more consistent results. SeekPeptides members access detailed tracking tools and personalized protocol adjustments that help maximize results throughout this entire timeline.
How semaglutide works at the cellular level
Understanding the mechanism explains the timeline. When you inject semaglutide, you introduce a synthetic version of GLP-1, a hormone your intestines naturally produce when you eat. This modified peptide resists rapid breakdown, giving it a half-life of approximately seven days compared to the natural hormone lasting mere minutes.
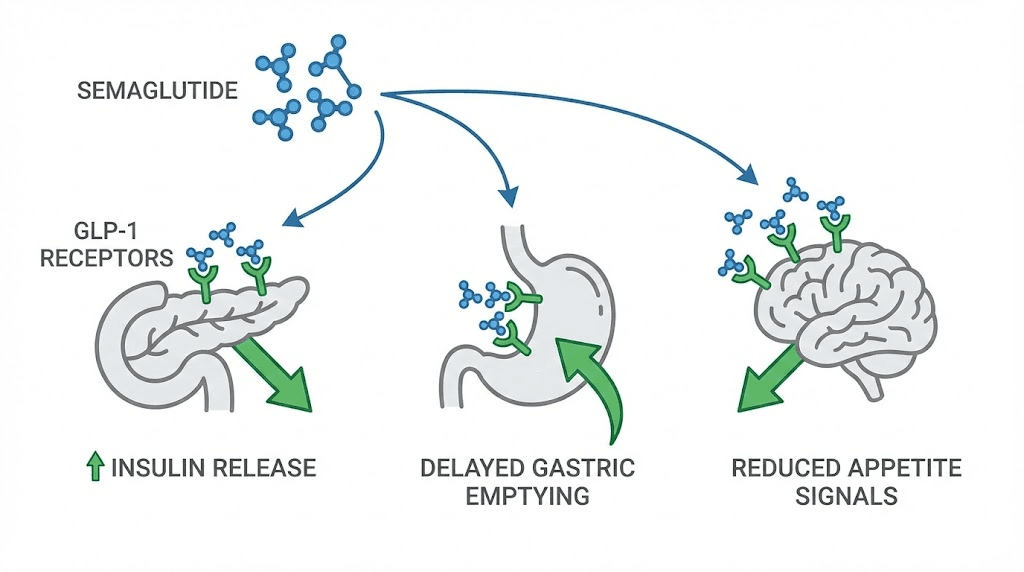
The medication binds to GLP-1 receptors throughout your body. In your pancreas, this binding stimulates insulin secretion when blood glucose is elevated and suppresses glucagon release, the hormone that signals your liver to dump stored glucose into your bloodstream. In your stomach, it slows gastric emptying, meaning food stays in your digestive system longer, extending satiety. In your brain, particularly the hypothalamus and areas controlling appetite, it reduces hunger signals and increases feelings of fullness.
These effects do not happen instantaneously or uniformly.
Receptor activation begins within hours of your first injection, but achieving steady-state blood levels, where the medication maintains consistent therapeutic concentrations, requires four to five weeks of regular weekly dosing. This pharmacokinetic reality drives the gradual dose escalation protocol and explains why rushing the process typically backfires.
The dose escalation requirement
Most protocols start at 0.25mg weekly for four weeks, not because this dose produces optimal weight loss, but because it allows your body to adapt to the medication with minimal side effects. Nausea, the most common complaint, results primarily from slowed gastric emptying. Starting low gives your digestive system time to adjust.
After the initial adaptation period, doses increase to 0.5mg for four weeks, then 1mg, potentially up to 1.7mg or the maximum 2.4mg depending on your response and tolerance. Each increment delivers stronger appetite suppression and greater weight loss velocity, but only if you have built tolerance at lower doses first.
This staged approach means peak therapeutic effect does not arrive until months into treatment. Anyone promising immediate dramatic results either misunderstands the medication or sells false expectations. The proper dosing schedule balances efficacy with tolerability, optimizing long-term adherence over short-term speed.
Why individual timelines vary dramatically
Your baseline metabolism, body composition, insulin sensitivity, and dietary habits all influence how quickly you respond to semaglutide. Someone with severe insulin resistance may see blood sugar improvements within days but slower weight loss initially. Someone with normal glucose regulation but significant adiposity might experience appetite changes quickly but modest initial scale movement.
Genetic factors affecting GLP-1 receptor density and sensitivity mean some people achieve therapeutic effects at 0.5mg while others need 2.4mg for comparable results. Age, sex hormones, stress levels, sleep quality, exercise patterns, and concurrent medications all modulate response speed and magnitude.
This variability makes rigid timeline predictions impossible. The data we present represents averages and typical ranges, but your personal experience may fall outside these parameters without indicating protocol failure. Patience combined with consistent monitoring gives you the information needed to adjust doses and optimize your individual timeline.
First injection to week two: immediate biological changes
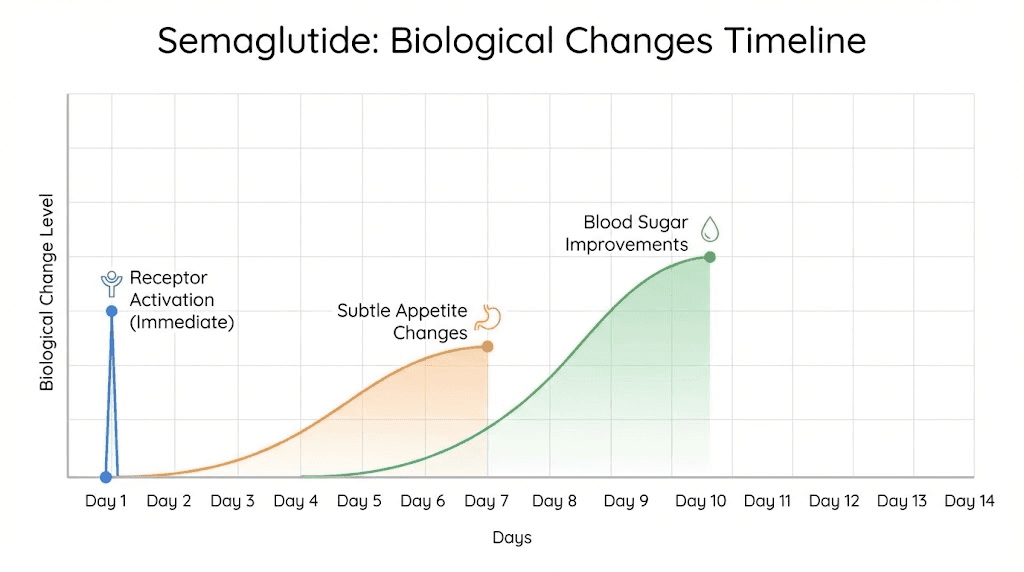
The moment semaglutide enters your system, receptor binding begins. This is not subjective. It is measurable. But feeling these changes is different from experiencing them biochemically.
Within 24 to 48 hours of your first injection, some individuals report subtle appetite reduction. They notice less interest in snacking between meals or feeling satisfied with smaller portions. This early response typically occurs in people with higher baseline GLP-1 sensitivity or those starting at slightly higher initial doses.
For most people, the first two weeks feel uneventful. The 0.25mg starting dose produces minimal noticeable effects by design. You might notice mild nausea after eating large or high-fat meals, a sign the medication is slowing gastric emptying. You might feel slightly fuller than usual, but not dramatically so. These subtle changes confirm the medication is working even when the scale has not moved.
Blood glucose improvements appear faster than weight changes. If you monitor glucose levels with continuous monitoring or regular finger sticks, you will likely see reduced post-meal spikes and lower fasting readings within the first week. This metabolic improvement precedes visible fat loss but indicates the medication is engaging its mechanisms properly.
Common experiences during the adaptation phase
Mild nausea affects approximately 40% of people during the first two weeks, usually occurring 30 minutes to two hours after meals. This resolves for most within days as your stomach adapts to slower emptying. Eating smaller meals, avoiding high-fat foods, and staying hydrated minimizes discomfort.
Some people report feeling slightly more fatigued than usual, particularly if they are simultaneously reducing calorie intake. The medication does not directly cause fatigue, but the combination of metabolic adaptation and lower food intake can temporarily reduce energy levels until your body adjusts.
Constipation emerges in about 25% of users, resulting from slowed intestinal motility. Increasing water intake, consuming more fiber through vegetables and fruits, and maintaining regular physical activity prevents or resolves this issue without requiring additional interventions.
Weight changes during these first two weeks typically range from zero to two pounds, mostly from water and glycogen depletion rather than fat loss. This is normal. The medication is establishing its presence, not yet operating at full therapeutic capacity.
What to monitor during this period
Track subjective appetite changes in a journal or app. Note when hunger arrives, how intense it feels, and how satisfied you are after meals. These patterns provide early feedback about receptor engagement before scale changes become obvious.
If you have access to blood glucose monitoring, record fasting levels and post-meal readings. Improvements here validate that semaglutide is engaging metabolic pathways even when weight loss lags behind. For people without diabetes, this data is less critical but still informative.
Monitor side effects without obsessing over them. Mild nausea is expected and manageable. Severe or persistent vomiting, extreme fatigue, or inability to eat anything requires medical consultation, not stoic endurance.
Weeks two through four: appetite suppression becomes obvious
As you approach the end of your first month, the cumulative effect of weekly injections pushes semaglutide blood levels higher. Most people reach a tipping point where appetite suppression transitions from subtle to undeniable.
You will likely notice reduced food noise, that constant mental chatter about what to eat next, when to snack, whether you are truly hungry or just bored. This cognitive shift represents central nervous system effects as semaglutide modulates appetite centers in your hypothalamus. Cravings for high-calorie, high-fat foods diminish. You might find yourself forgetting to eat, something that never happened before.
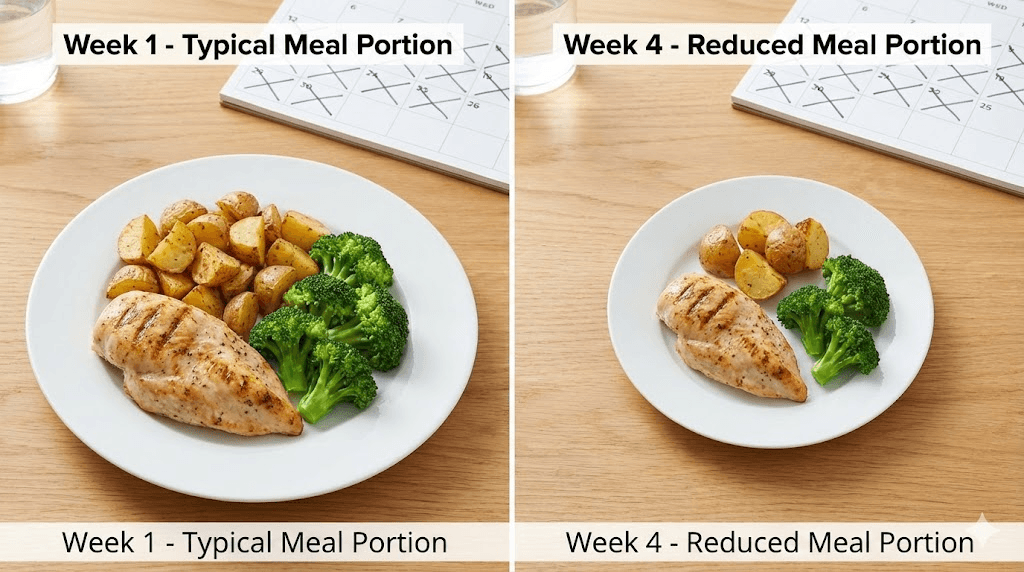
Portion sizes shrink naturally without requiring conscious restriction. A meal that previously left you satisfied now feels too large. You stop eating when you reach comfortable fullness rather than pushing through to clean your plate. This behavioral change reflects the medication working as intended, enhancing satiety signals that obesity had suppressed.
Weight loss during weeks two through four typically ranges from three to six pounds for most individuals, though this varies widely based on starting weight, caloric deficit, and metabolic factors. People with more weight to lose often see larger initial drops. Those closer to normal weight experience slower but still meaningful progress.
The medication reaches steady state
By week four or five, semaglutide achieves steady-state pharmacokinetics. Each weekly injection maintains consistent blood levels rather than creating peaks and valleys. This stability translates to more predictable appetite control and side effect patterns.
Some people notice their appetite suppression feels strongest on days two through five after injection, with slight reduction in effect by day six or seven before the next dose. This pattern, while common, should not dramatically impact your ability to control intake throughout the week. If hunger returns aggressively before your next injection, this may indicate your current dose is insufficient.
Blood pressure and lipid markers often begin improving during this window, independent of weight loss magnitude. Semaglutide exerts direct cardiovascular effects beyond its metabolic actions, contributing to reduced cardiovascular risk even before substantial fat loss occurs.
Adjusting your approach based on early results
If you experience strong appetite suppression and steady weight loss during the first month, your dose escalation can proceed on schedule. If appetite control feels minimal or weight loss stalls completely, extending time at 0.25mg before advancing may not help. The starting dose is subtherapeutic for most people. Moving to 0.5mg typically produces the response you seek.
Side effects during this phase should be manageable with dietary adjustments. If nausea, vomiting, or gastrointestinal distress becomes severe, slowing your dose escalation or extending time at your current dose allows better adaptation. Pushing through intolerable symptoms increases dropout risk and provides no additional benefit.
Dietary quality matters more as appetite decreases. When you eat less, every bite carries more nutritional weight. Prioritizing protein intake, consuming adequate vitamins and minerals, and avoiding empty calories optimizes body composition as weight decreases.
Weeks four through eight: dose increase drives accelerated results
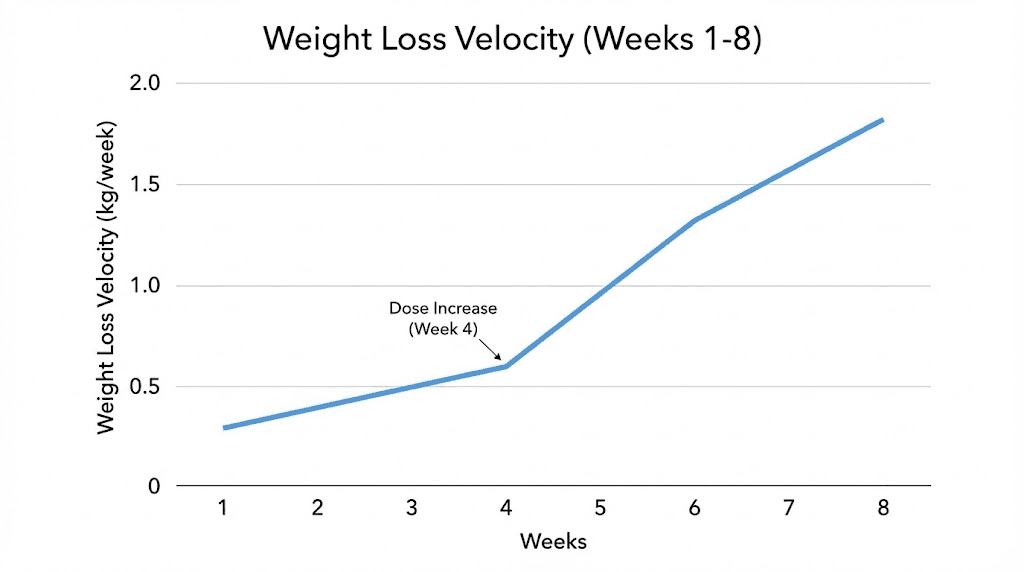
When you advance from 0.25mg to 0.5mg at week four, expect a noticeable step change in appetite suppression within days. The doubling of your dose produces more pronounced receptor activation, stronger gastric slowing, and enhanced satiety signals.
Weight loss velocity typically increases during this period, with most people losing five to ten pounds over these four weeks. This represents the sweet spot where therapeutic effects strengthen without side effects becoming prohibitive. Your body has adapted to the medication presence, your dose is climbing toward therapeutic levels, and your behavioral changes are reinforcing the biological effects.
Food preferences often shift during this window. High-fat, high-sugar foods not only become less appealing mentally but may trigger more intense nausea or discomfort when consumed. This aversion is not a side effect to overcome but rather part of the intended metabolic reprogramming. Your body is signaling which foods work with the medication and which create problems.
Energy levels typically stabilize or improve during weeks four through eight, particularly if you have been maintaining adequate protein and nutrient intake. Early fatigue resolves as your metabolism adapts to operating on fewer calories. If energy remains low, this might indicate excessive caloric restriction or inadequate protein consumption.
The psychological transition
By eight weeks, most people experience a fundamental shift in their relationship with food. The constant battle against hunger, the need for extreme willpower to resist cravings, the mental energy consumed by dietary restriction all diminish or disappear. This is what successful peptide therapy feels like.
This psychological relief is not a placebo effect. It reflects genuine changes in how your brain processes hunger and satiety signals. For many people, this is the first time in years or decades they have experienced normal appetite regulation. Understanding this helps prevent the mistake of attributing success to willpower when biology deserves the credit.
Social eating situations become more manageable during this phase. You can attend dinners, parties, or events without feeling deprived or struggling against overwhelming temptation. The medication does not eliminate your ability to enjoy food, but it resets your appetite to appropriate levels for your actual caloric needs.
Monitoring progress beyond the scale
Weight is one metric, but not the only one that matters. Take measurements of your waist, hips, chest, and thighs every two weeks. Fat loss often shows more dramatically in measurements than in total weight, particularly if you are maintaining or building muscle mass through resistance training.
Progress photos provide visual evidence that your brain cannot dismiss the way it dismisses scale fluctuations. Take front, side, and back photos in consistent lighting and clothing every four weeks. The cumulative changes over months become undeniable when viewed side by side.
Track how your clothes fit, how your energy feels throughout the day, how your sleep quality changes, and how your physical capabilities improve. These qualitative markers often change before quantitative measurements catch up, providing motivation during plateaus or slower loss periods.
Weeks eight through twelve: approaching therapeutic dose
At week eight, most protocols advance to 1mg weekly, bringing you into the lower therapeutic range. This dose produces meaningful weight loss for many people, though some will eventually need higher doses for optimal results.
The jump from 0.5mg to 1mg can trigger temporary side effect resurgence. Nausea may return for a few days as your stomach adapts to the increased gastric slowing. Eating smaller, more frequent meals and avoiding trigger foods minimizes this discomfort.
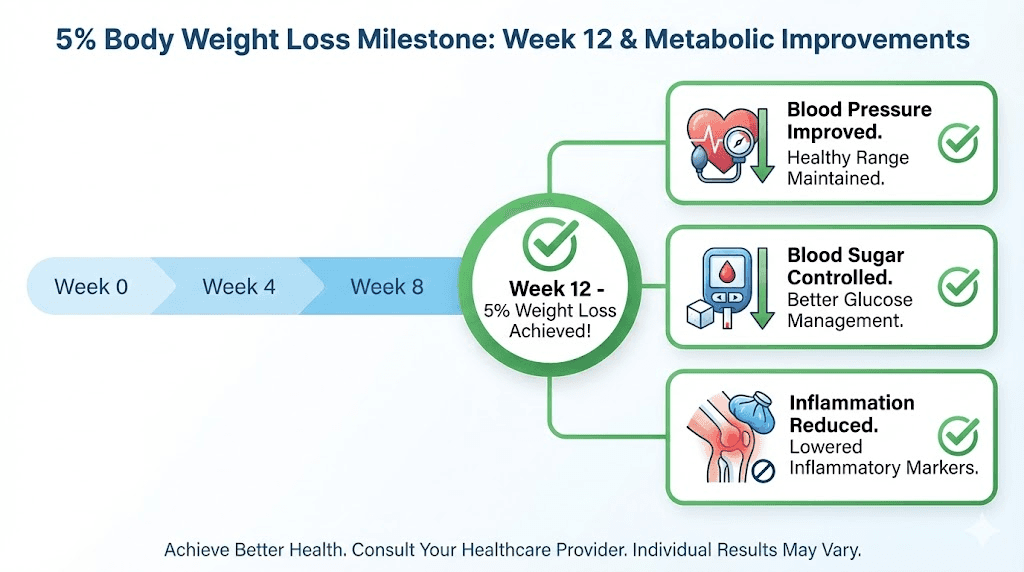
By week twelve, clinical trials show participants typically achieve at least five percent body weight reduction from baseline. This threshold matters because losing five percent of body weight produces measurable improvements in metabolic markers, blood pressure, lipid profiles, and inflammation. Even if you have more weight to lose, reaching this milestone validates your protocol effectiveness.
Weight loss during weeks eight through twelve often ranges from six to twelve pounds, continuing the momentum established in earlier weeks. Some people experience their fastest loss rate during this period before metabolic adaptation begins moderating velocity.
When results slow or plateau
Some people experience their first plateau during this window, where weight loss stalls for two to three weeks despite consistent medication use and dietary adherence. This is normal and expected, not a sign of protocol failure.
Your body adapts to lower body weight by reducing metabolic rate and increasing hunger signals. Semaglutide counteracts much of this adaptation but cannot eliminate it entirely. Plateaus represent your metabolism recalibrating, not permanent stalls.
Continuing your protocol through plateaus is critical. Most plateaus break naturally within two to four weeks as your body adjusts to its new baseline and resumes losing weight. Prematurely increasing your dose during a plateau rarely accelerates loss and increases side effect risk.
Evaluating your dietary adherence during plateaus often reveals subtle creep in portion sizes or snacking frequency. The medication reduces but does not eliminate the ability to overeat. Tightening up your food choices and portions usually restarts progress without requiring dose changes.
Optimizing exercise during this phase
By three months, your energy levels should support regular physical activity. Resistance training becomes particularly important during this phase to preserve lean muscle mass as you lose weight. Muscle tissue burns more calories at rest than fat, making its preservation critical for long-term metabolic health.
Cardiovascular exercise supports caloric deficits and improves cardiovascular fitness, but prioritize sustainability over intensity. Walking, cycling, swimming, or any activity you will maintain consistently beats aggressive exercise programs you abandon after weeks.
Some people find their exercise capacity improves dramatically as weight decreases, with joint pain diminishing and endurance increasing. Others struggle with energy during intense workouts due to reduced caloric intake. Listen to your body and adjust intensity and volume based on your recovery and energy levels.
Weeks twelve through twenty-four: sustained weight loss phase
Between months three and six, most people reach their therapeutic dose, whether that is 1mg, 1.7mg, or 2.4mg weekly. At this dose, you should experience consistent appetite control and steady weight loss without excessive side effects.
The pace of weight loss typically ranges from one to three pounds per week during this phase, slower than the initial months but more sustainable. Clinical trial data shows average weight loss of approximately two percent of body weight per month during the first six months, with this rate declining gradually over time.
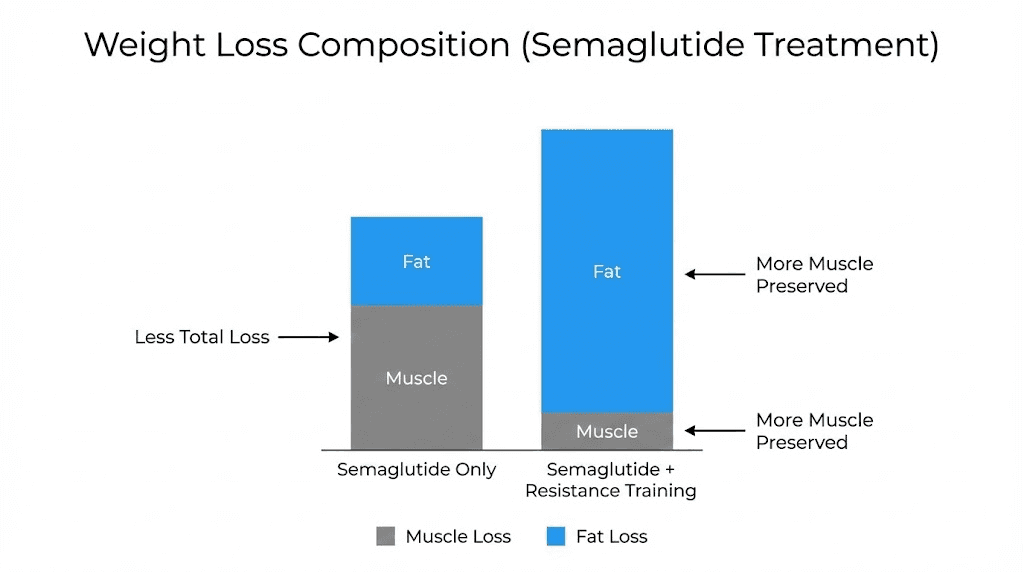
Your body composition shifts during this phase. If you are maintaining adequate protein intake and engaging in resistance training, much of your weight loss comes from fat rather than muscle. If protein intake is insufficient or you avoid strength training, you will lose more muscle along with fat, compromising your metabolic rate and physical appearance.
Psychological adaptation becomes as important as biological response during this sustained phase. The initial excitement of rapid loss fades. Progress feels slower even when it remains substantial. Maintaining motivation requires focusing on non-scale victories, health improvements, and long-term goals rather than weekly weight fluctuations.
Managing expectations during month six
By six months, clinical trial participants lost an average of 10 to 15 percent of their starting body weight, though individual results varied widely from five percent to over 20 percent depending on starting weight, dose achieved, and adherence to lifestyle modifications.
If your results fall below these averages, several factors might explain the discrepancy. Suboptimal dosing, insufficient dietary adherence, lack of physical activity, underlying metabolic conditions, or genetic factors affecting GLP-1 sensitivity all influence outcomes.
Comparing yourself to trial averages can mislead because trial participants typically receive intensive dietary counseling, regular monitoring, and support that real-world users lack. Your progress compared to your own baseline matters more than hitting arbitrary benchmarks.
If you have lost five to ten percent of your body weight by six months, you have achieved clinically meaningful results that improve your health outcomes, even if you have not reached your ultimate goal. Continuing treatment produces additional loss for most people, though the rate continues gradually declining.
When to consider dose adjustments
If appetite control has weakened significantly by six months or weight loss has stalled completely for six to eight weeks despite dietary adherence, increasing your dose may reignite progress. This assumes you have not already reached the maximum 2.4mg dose.
Some people maintain excellent appetite control but stop losing weight due to metabolic adaptation. In these cases, adding other peptides targeting different mechanisms, implementing intermittent fasting protocols, or increasing activity levels often proves more effective than further dose increases.
Working with a healthcare provider experienced in peptide-based weight management helps navigate these decisions. Generic protocols work for many people, but optimization requires personalized adjustments based on your unique response patterns.
Months six through twelve: the maintenance transition
During the second half of your first year, weight loss continues but at a slower pace. Clinical trial data shows average loss of approximately one percent of body weight per month during months six through twelve, ultimately reaching 15 to 16 percent total body weight loss by the end of year one.
This deceleration frustrates some people who expect linear progress, but it represents normal metabolic adaptation. Your body defends against further weight loss by reducing metabolic rate, increasing hunger hormones like ghrelin, and decreasing satiety hormones like leptin. Semaglutide counteracts these adaptations but cannot eliminate them completely.
The question during this phase shifts from how much weight can I lose to how do I maintain the loss I have achieved. Research consistently shows maintenance requires ongoing intervention. Discontinuing semaglutide typically results in gradual weight regain as your appetite regulation returns to pre-treatment patterns.
Some people reach their goal weight during this phase and transition to maintenance dosing, using the minimum dose that controls appetite without producing further loss. Others continue losing beyond twelve months toward more aggressive targets. Your goals, health status, and side effect tolerance determine the right approach.
The biology of weight loss deceleration
As you lose weight, your body requires fewer calories to maintain its reduced mass. A 200-pound person burns more calories at rest than a 170-pound person. This means the caloric deficit that produced two pounds of weekly loss at month three might produce one pound weekly at month nine, even with identical food intake.
Adaptive thermogenesis, the reduction in metabolic rate beyond what your reduced body mass predicts, further slows progress. Your body becomes more metabolically efficient, extracting more energy from less food and burning fewer calories during activity. This survival mechanism protected humans during famines but complicates modern weight loss efforts.
Hormonal changes accompanying weight loss also drive deceleration. Leptin levels drop, signaling your brain that energy stores are depleted. Ghrelin levels rise, increasing hunger. Thyroid function may decrease slightly, reducing metabolic rate. These changes are not pathological but represent your body protecting against what it perceives as starvation.
Strategies for breaking through long plateaus
When progress stalls for two months or more despite continued medication use, intervention becomes necessary. The first step involves rigorously tracking food intake for two weeks to identify any creep in portion sizes, snacking frequency, or calorie-dense food consumption that may have slowly increased.
Implementing structured meal timing, such as eating within an eight to ten hour window each day, often restarts progress without requiring further caloric restriction. This mild form of intermittent fasting improves insulin sensitivity and may enhance fat oxidation beyond appetite suppression alone.
Adding or intensifying resistance training builds muscle mass, which increases resting metabolic rate and improves body composition even if total weight changes slowly. Prioritizing progressive overload, where you gradually increase weights or repetitions over time, maximizes these benefits.
Some people benefit from brief diet breaks, eating at maintenance calories for one to two weeks before resuming a deficit. This approach may partially reverse metabolic adaptation and improve adherence by providing psychological relief from prolonged restriction.
Long-term results and expectations beyond year one
Research following semaglutide users beyond one year shows maintained weight loss in those who continue medication, with average losses stabilizing around 15 to 17 percent of starting weight. Some individuals continue losing weight into year two, particularly those who started with higher initial body weights.
The plateau you reach depends on multiple factors including your biological set point, the degree of metabolic adaptation your body develops, your dietary adherence and activity levels, and whether you have optimized your dose for maintenance versus continued loss.
Discontinuing semaglutide after reaching goal weight typically results in gradual regain, with most people regaining about two-thirds of lost weight within a year of stopping. This outcome does not reflect personal failure but rather the biological reality that obesity involves persistent dysregulation of appetite and metabolism that requires ongoing management.
Continuing semaglutide indefinitely at a maintenance dose prevents most regain for most people. Your maintenance dose might be lower than your peak dose, but completely discontinuing medication removes the metabolic support keeping your appetite normalized and your weight stable.
Comparing semaglutide to other interventions
Semaglutide produces weight loss comparable to older weight loss peptides and medications but with better tolerability and lower discontinuation rates. Average weight loss exceeds what lifestyle modification alone typically achieves and approaches results seen with some bariatric surgical procedures.
Compared to tirzepatide, a newer dual GIP/GLP-1 agonist, semaglutide produces slightly less average weight loss but with similar side effect profiles and lower cost in many markets. Both medications represent major advances over previous pharmaceutical options.
The medication works best as part of comprehensive management including dietary improvement, regular physical activity, sleep optimization, and stress management. It is not a standalone solution but rather a powerful tool that makes sustainable lifestyle changes achievable when they would otherwise require unsustainable willpower.
Cost and accessibility considerations
Long-term semaglutide use requires ongoing financial commitment, whether through insurance coverage or out-of-pocket payment. Branded formulations like Wegovy can cost over $1,000 monthly without insurance, though compounded versions may offer lower-cost alternatives.
Insurance coverage varies widely, with some plans covering semaglutide for diabetes but not obesity, and others covering weight loss only with prior authorization demonstrating failed lifestyle interventions. Navigating coverage requires persistence and often advocacy from your prescribing provider.
The total cost over one to two years of treatment must be weighed against the health benefits achieved, including reduced risk of diabetes, cardiovascular disease, and obesity-related complications. For many people, the investment pays for itself through reduced medical costs and improved quality of life.
Optimizing your individual timeline
While average timelines provide useful guidance, optimizing your personal response requires attention to factors you can control and awareness of those you cannot.
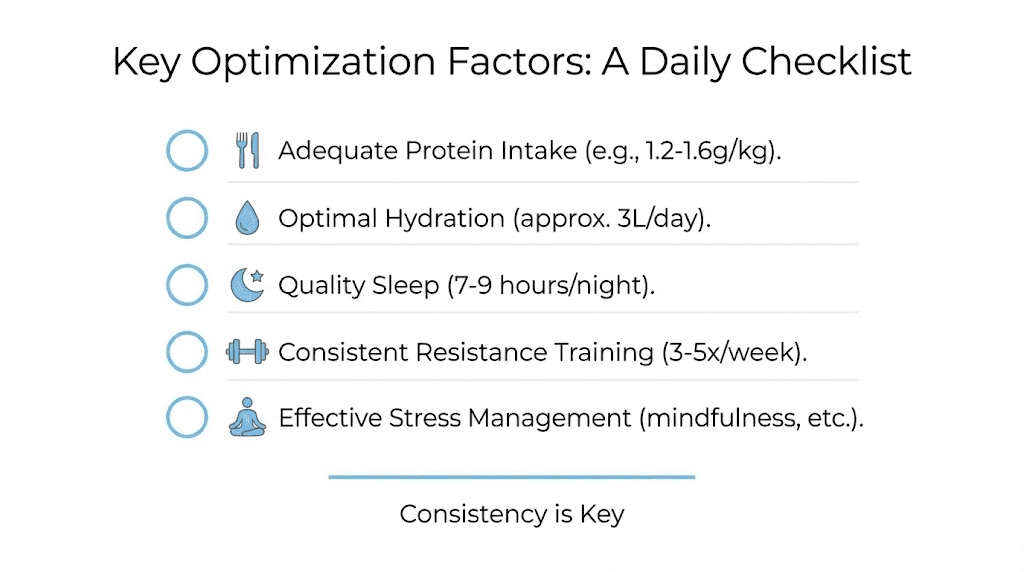
Protein intake stands as the single most important dietary factor during semaglutide treatment. Consuming 0.7 to 1 gram per pound of target body weight daily preserves muscle mass, supports satiety, and maintains metabolic rate. When appetite is suppressed, prioritizing protein at every meal ensures you meet this target even with reduced total intake.
Hydration affects both the medication effectiveness and side effect severity. Adequate water intake supports kidney function as your body metabolizes fat, helps prevent constipation from slowed gastric motility, and supports overall metabolic processes. Aiming for at least 64 ounces daily, more if you are physically active or live in hot climates, optimizes these functions.
Sleep quality influences hormonal regulation, including leptin and ghrelin, which modulate appetite independent of semaglutide effects. Prioritizing seven to nine hours of quality sleep nightly enhances the medication effectiveness and improves your ability to maintain healthy dietary choices.
The role of resistance training
Strength training two to four times weekly produces multiple benefits during semaglutide treatment. It preserves and potentially builds muscle mass despite caloric restriction, increases insulin sensitivity independent of weight loss, improves bone density, and maintains or increases resting metabolic rate.
You do not need complex programs or expensive equipment. Bodyweight exercises, resistance bands, or basic free weights suffice for most people.
The key is progressive overload, gradually increasing difficulty over time, and consistency, maintaining regular sessions rather than sporadic intense workouts.
Starting or intensifying resistance training during treatment may temporarily slow weight loss as you build muscle, which is denser than fat. This is not a problem but rather a benefit, as you are improving body composition beyond what the scale reflects. Measurements and photos capture these changes better than weight alone.
Managing side effects without compromising results
Nausea, the most common side effect, often responds to dietary modifications rather than dose reductions. Eating smaller, more frequent meals rather than three large ones, avoiding high-fat foods that slow gastric emptying further, choosing bland foods during periods of increased nausea, and staying well-hydrated all help manage symptoms.
If nausea becomes severe enough to interfere with eating adequate protein or forces you to skip doses, discuss dose reduction or slower escalation with your provider. Pushing through intolerable symptoms increases dropout risk and provides no benefit. Finding your optimal dose, which may be lower than the maximum, ensures long-term adherence.
Constipation responds to increased fiber intake through vegetables, fruits, and whole grains, adequate hydration, and regular physical activity which stimulates intestinal motility. If these measures prove insufficient, adding a magnesium supplement or gentle fiber supplement usually resolves the issue.
Frequently asked questions
How long does it take for semaglutide to suppress appetite?
Most people notice appetite suppression within one to four weeks, with effects becoming more pronounced as dose increases. Some individuals feel changes within days at the starting 0.25mg dose, while others need several weeks at 0.5mg or higher before experiencing significant appetite reduction. By week 12 to 16, when you reach therapeutic doses, appetite suppression should be substantial. If you reach maximum dose without noticeable appetite effects, this may indicate you are a poor responder or other factors are interfering with the medication effectiveness.
When will I start losing weight on semaglutide?
Weight loss typically begins within four weeks of starting treatment, with most people losing two to five pounds during the first month. Loss accelerates as doses increase, with five to ten pounds common during weeks four through eight when advancing from 0.25mg to 0.5mg. By three months, expect cumulative loss of 10 to 20 pounds depending on starting weight and adherence. Maximum loss velocity usually occurs between months three and six, then gradually declines as your body adapts.
Can I speed up how fast semaglutide works?
Increasing your dose faster than the standard escalation schedule typically increases side effects without accelerating meaningful weight loss. Your body needs time to adapt to each dose level. What you can control is optimizing factors that support the medication, including consuming adequate protein to preserve muscle mass, engaging in regular resistance training, maintaining consistent meal timing, staying well-hydrated, and prioritizing quality sleep. These factors maximize your response without increasing side effect risk.
What if semaglutide stops working after several months?
If appetite control weakens or weight loss stops completely after working initially, several factors might explain this. First, evaluate whether you have gradually increased portion sizes or reintroduced high-calorie foods as your body adapted to the medication. Second, consider whether metabolic adaptation has slowed your progress despite ongoing appetite control. Third, assess if your current dose remains optimal or if you need an increase. Finally, check for other factors like stress, sleep disruption, or medication interactions that might interfere with effectiveness.
How long should I stay on semaglutide?
Most research and clinical experience suggest ongoing treatment for chronic weight management, similar to how other chronic conditions require continued intervention. Discontinuing semaglutide typically results in gradual weight regain as appetite dysregulation returns. Some people maintain loss after stopping by implementing intensive lifestyle measures, but most find ongoing treatment necessary for sustained results. Your maintenance dose might be lower than your peak dose, requiring less frequent injections or smaller amounts.
Why do some people respond faster than others?
Individual variation in GLP-1 receptor density and sensitivity, baseline insulin resistance, metabolic rate, body composition, genetic factors affecting drug metabolism, concurrent medications or supplements, adherence to dietary and lifestyle recommendations, and starting weight all influence how quickly and dramatically you respond to semaglutide. This variability is normal and does not reflect personal failure when your timeline differs from others or from published averages.
When should I see a doctor about my semaglutide response?
Consult your provider if you experience severe or persistent nausea and vomiting that prevents adequate food or fluid intake, signs of pancreatitis including severe abdominal pain, vision changes or signs of diabetic retinopathy progression if you have diabetes, severe constipation lasting more than a week despite interventions, rapid heart rate or chest pain, or complete lack of appetite suppression or weight loss after reaching 1mg dose for at least four weeks.
Can I combine semaglutide with other weight loss peptides?
Some providers prescribe semaglutide alongside other interventions like peptide stacks targeting different mechanisms, metformin for insulin sensitivity, or topiramate for additional appetite suppression. These combinations can produce additive effects but also increase cost and potential side effects. The decision to combine therapies should involve discussion with a knowledgeable provider about potential benefits, risks, interactions, and whether monotherapy has been optimized first.
External resources
New England Journal of Medicine - Semaglutide Clinical Trial Results
National Center for Biotechnology Information - GLP-1 Receptor Agonist Research
Centers for Disease Control - Obesity Statistics and Management Guidelines
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay regulated, your progress stay consistent, and your results stay sustainable.