Mar 18, 2026

Day one feels like nothing. A small injection, barely noticeable. Maybe a slight pinch in the abdomen. You cap the syringe, put it back in the fridge, and wonder if anything actually happened. Day seven brings a surprise. That second slice of pizza? You do not want it. The late-night pantry raids that have been a fixture of your evenings for years? Gone. By day fourteen, your pants fit differently. By day twenty-one, someone at work notices. And by month three, when you look at a photo of yourself from before all this started, you barely recognize the person staring back.
That is the GLP-1 before and after story that thousands of people are living right now.
But here is what the transformation photos do not tell you. They do not show the nausea during week one. They skip over the plateau at month four that made you question everything. They leave out the part where you had to completely rethink your relationship with food, exercise, and your own body. The before and after snapshots are real, but the journey between those two photos is where the actual story lives.
This guide walks through the complete GLP-1 transformation timeline. Week by week. Month by month.
Not just the weight on the scale, but the body composition shifts, the metabolic changes, the side effects that come and go, the mental recalibration that nobody talks about, and the specific strategies that separate average results from extraordinary ones. Whether you are considering starting GLP-1 therapy or you are already months into treatment and wondering what comes next, this is the reference guide you will keep coming back to.
Understanding how GLP-1 medications transform the body
GLP-1 receptor agonists work through a mechanism that most people dramatically underestimate. The common narrative reduces these medications to appetite suppressants. That narrative is wrong. These peptides interact with receptors throughout the entire body, triggering a cascade of metabolic changes that go far beyond simply making you feel less hungry.
The GLP-1 receptor exists in the brain, the gut, the pancreas, the heart, and even muscle tissue. When a synthetic GLP-1 agonist like semaglutide or tirzepatide activates these receptors, the effects ripple through multiple systems simultaneously. Gastric emptying slows. Insulin sensitivity improves. Glucagon secretion decreases. Reward pathways in the brain that previously drove compulsive eating behaviors begin to quiet down.
This multi-system approach explains why GLP-1 before and after results look so different from traditional diet results. When someone loses 30 pounds through caloric restriction alone, they often look deflated. The weight comes off, but body composition does not necessarily improve. Fat loss and muscle loss happen in roughly equal proportions. With GLP-1 therapy, especially when combined with proper resistance training and protein intake, the ratio shifts dramatically toward fat loss while preserving lean mass.
Research from the STEP trials, which studied semaglutide 2.4mg weekly, found that approximately 75% of the weight lost was fat mass rather than lean mass.
That percentage improves further when participants engage in structured exercise. Some clinical data suggests the fat-to-lean loss ratio can reach 85:15 or even 90:10 with optimal training protocols.
The GLP-1 mechanism of action also explains why results accelerate over time rather than plateauing immediately like most diets. As insulin sensitivity improves and inflammatory markers decrease, the body becomes progressively more efficient at mobilizing stored fat. The metabolic environment shifts from one that fights weight loss to one that facilitates it.
Understanding this foundation matters because it sets realistic expectations for your own transformation timeline. The before and after photos you see online represent endpoints. The path to those endpoints follows a predictable pattern that we will map out in detail.
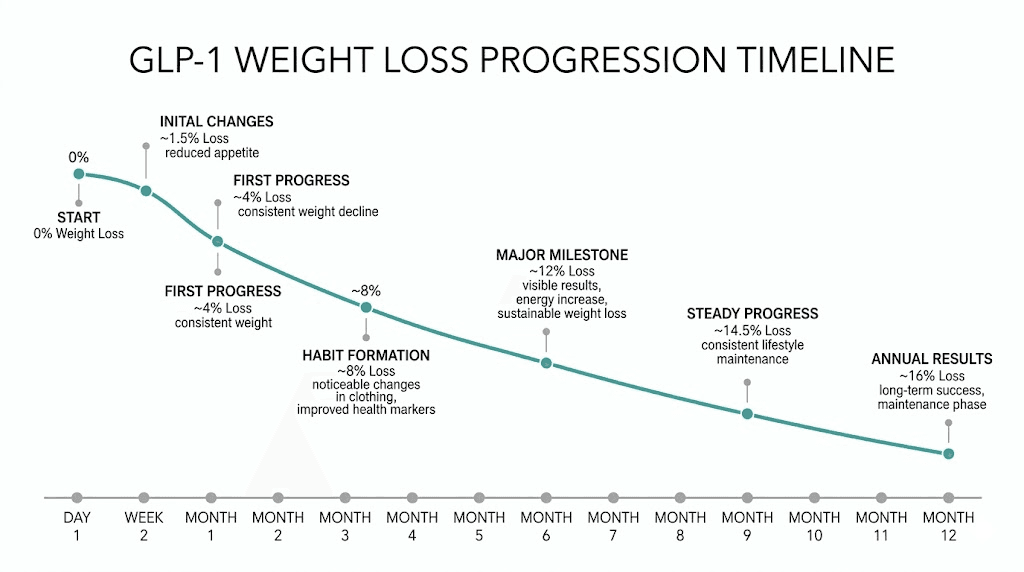
Week 1 through week 4: the initial adjustment phase
The first month on GLP-1 therapy is equal parts exciting and uncomfortable. Your body is meeting a powerful new signaling molecule, and the adjustment period involves real physiological changes that affect everything from appetite to energy levels to digestive function.
Week 1: baseline disruption
Most people begin GLP-1 therapy at the lowest available dose. For semaglutide, that is typically 0.25mg per week. For tirzepatide, the starting dose is usually 2.5mg per week. These starting doses are deliberately low, designed to let your body acclimate before ramping up.
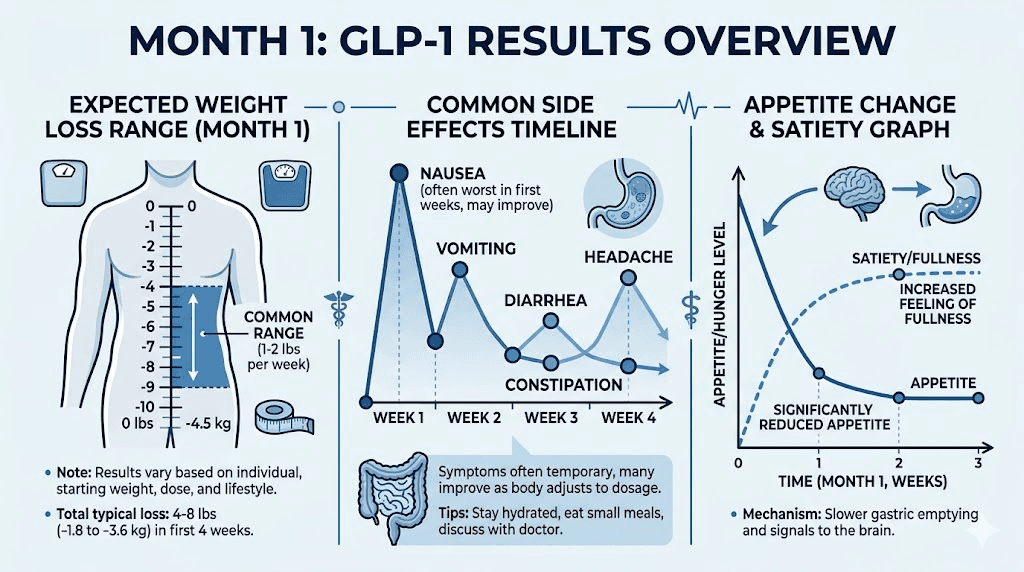
During week one, the most common experience is a noticeable reduction in appetite that feels almost surreal. People describe it as the volume knob on hunger being turned down from 8 to 3. You still feel hunger cues, but they lack the urgency and intensity that previously drove overeating. That voice that used to scream for a snack at 3pm now whispers politely and accepts a glass of water as an answer.
Weight loss during the first week typically ranges from 2 to 5 pounds. Before you get excited, understand that most of this is water weight. GLP-1 agonists reduce insulin levels, and lower insulin triggers the kidneys to release stored sodium and water. This is the same mechanism behind the initial rapid weight loss seen in low-carb diets. It is real weight loss, but it is not representative of the ongoing rate.
Side effects during week one are usually mild but present. The most common include mild nausea (reported by approximately 40% of users), reduced appetite to the point of occasional food aversion, slight fatigue as your body adjusts to lower caloric intake, and occasional digestive changes including softer stools or mild constipation. The nausea typically peaks 24 to 48 hours after injection and improves as the week progresses. Eating smaller meals, avoiding high-fat foods, and staying hydrated significantly reduce this symptom. Understanding GLP-1 side effects before starting helps you prepare for and manage these temporary discomforts.
Week 2: the appetite revolution
By week two, most people have adapted to the initial side effects. Nausea diminishes or disappears entirely. What remains, and what surprises almost everyone, is the profound shift in how you relate to food.
This is not willpower. This is neurochemistry.
The GLP-1 receptors in your hypothalamus are being activated in a way that fundamentally changes satiety signaling. Foods you previously found irresistible now seem merely acceptable. The emotional pull toward comfort eating weakens. You find yourself eating half a meal and feeling genuinely satisfied, not deprived, not fighting urges, just done.
Weight loss in week two typically adds another 1 to 3 pounds of actual fat loss on top of the initial water weight drop. Your clothes may not fit differently yet, but the scale is moving consistently. More importantly, your blood sugar patterns are already improving. Fasting glucose drops. Post-meal glucose spikes flatten. These metabolic changes are happening before the visible transformation begins.
Week 3 and week 4: building momentum
Weeks three and four represent the transition from novelty to routine. The medication becomes a normal part of your weekly schedule. Side effects have largely resolved. Appetite suppression remains strong and consistent.
By the end of month one, most people have lost between 5 and 10 pounds. The range is wide because starting weight, metabolic health, diet quality, and activity level all influence the rate. Someone starting at 300 pounds with significant insulin resistance may lose 12 pounds in the first month. Someone starting at 180 pounds who is already relatively active might lose 5.
The physical changes at this point are subtle. You might notice your face looks slightly leaner. Rings fit more loosely. The bloating that you had accepted as normal has disappeared. These small changes are the earliest visible signs of the transformation that will accelerate dramatically over the coming months.
What matters most during this phase is establishing the habits that will determine your long-term results. Protein intake becomes critical from day one. Aim for 0.7 to 1.0 grams per pound of body weight daily. This is challenging when your appetite is suppressed, which is why protein shakes, high-protein snacks, and strategic meal planning matter enormously. The people who achieve the best GLP-1 before and after transformations are almost universally the ones who prioritize protein from the very beginning.
Month 2 through month 3: the acceleration phase
This is where the GLP-1 transformation becomes visible to everyone around you. The gradual changes from month one compound into noticeable physical differences that friends, family, and coworkers start commenting on. It is also the phase where the medication reaches its therapeutic dose range, amplifying both the benefits and the importance of supporting habits.
Dose titration and its impact
Most GLP-1 protocols involve gradual dose increases during months two and three. Semaglutide typically moves from 0.25mg to 0.5mg at week five, then to 1.0mg at week nine. Some protocols continue increasing to 1.7mg or the maximum 2.4mg dose. Tirzepatide follows a similar escalation from 2.5mg up through 5mg, 7.5mg, 10mg, and potentially 12.5mg or 15mg.
Each dose increase brings a renewed wave of appetite suppression. People who felt their appetite starting to creep back toward the end of month one often find that the first dose increase pushes it right back down. This stepwise approach is intentional. It allows the body to adjust while progressively increasing the metabolic benefits.
The higher doses also bring the possibility of temporary side effect recurrence. Mild nausea may return for a few days after each increase. Gastrointestinal changes are common. These effects are transient, usually resolving within a week of the dose change. The key is expecting them and not panicking when they appear.
What the body looks like at months 2 and 3
By the end of month two, total weight loss typically ranges from 10 to 18 pounds. By month three, the range extends to 15 to 28 pounds. Again, individual variation is enormous. But the pattern is consistent: steady, accelerating fat loss that is visibly changing body shape.
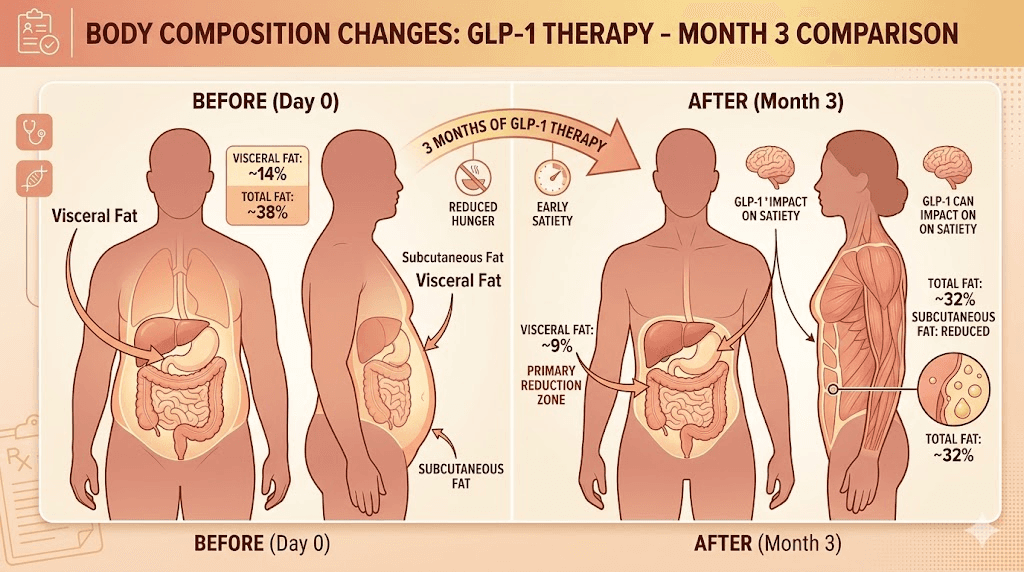
The areas that show change first depend on your body fat distribution pattern. People who carry fat primarily in the midsection often see the most dramatic early changes there. The visceral fat that wraps around organs is actually more metabolically active and responsive to the hormonal changes GLP-1 therapy creates. This means your waist measurement may decrease faster than other measurements, even if the scale seems to slow down at times.
Facial changes become obvious during this phase. The puffiness that accompanies excess weight and chronic inflammation recedes. Jawline definition improves. People often say they look younger, and there is legitimate science behind this. Reduced inflammation decreases facial bloating and improves skin quality.
Body composition analysis during this phase typically shows encouraging ratios. For people following a high-protein diet and engaging in resistance training, fat loss accounts for 80% or more of total weight lost. Lean mass preservation is strong, and some people actually gain muscle during this phase if they are training consistently with progressive overload.
The clothing changes become dramatic. Most people drop one to two full sizes by month three. Belts need new holes. Shirts that were tight now drape loosely. This is often the point where people start needing to shop for transitional clothing, a problem that feels remarkably good to have.
The metabolic transformation beneath the surface
What you cannot see in before and after photos is often more significant than what you can see. By month three, several critical metabolic markers have typically improved substantially.
Fasting blood glucose drops by an average of 15 to 30 mg/dL in people who started with elevated levels. HbA1c, the three-month average of blood sugar, may decrease by 0.5 to 1.5 percentage points. For people with prediabetes, this can mean returning to normal glucose ranges entirely.
Cholesterol panels typically show improvement by month three. Triglycerides decrease, often by 20 to 40%. LDL cholesterol may drop modestly. HDL cholesterol tends to increase slightly. The overall cardiovascular risk profile improves meaningfully.
Blood pressure improvements are common, with systolic pressure dropping by 5 to 10 mmHg on average. For people on blood pressure medications, this sometimes allows dose reductions under medical supervision.
Inflammatory markers like C-reactive protein (CRP) decline significantly. This reduction in systemic inflammation contributes to improved energy levels, better sleep quality, reduced joint pain, and the general sense of vitality that people report during months two and three.
These metabolic improvements matter enormously for long-term health outcomes. The visible transformation motivates you. The invisible transformation protects you. SeekPeptides tracks both dimensions because lasting health requires attention to what the mirror shows and what the bloodwork reveals.
Month 4 through month 6: the transformation deepens
Months four through six represent the heart of the GLP-1 transformation. This is when cumulative fat loss reaches the point where before and after photos become genuinely striking. It is also when the psychological and behavioral changes solidify into something that looks and feels like a new relationship with food and your body.
The plateau that is not really a plateau
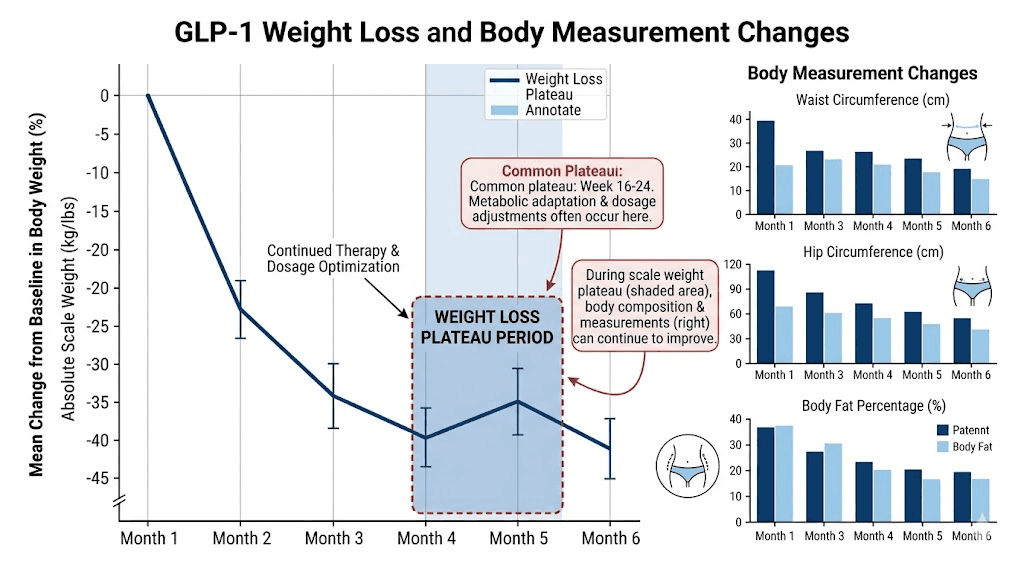
Almost everyone experiences what feels like a stall somewhere between months three and five. The scale, which had been dropping steadily, suddenly stops moving for one to three weeks. This is one of the most psychologically challenging moments in the entire GLP-1 journey, and it is also one of the most misunderstood.
What is actually happening during a plateau is usually a combination of several factors. Water retention increases temporarily, often in response to hormonal shifts or changes in sodium intake. If you are exercising consistently, muscle glycogen stores may be replenishing, which adds water weight. And sometimes the body simply needs time to adjust to its new metabolic setpoint before continuing to lose fat.
The critical insight is that fat loss is often still occurring during a plateau. Body measurements may continue decreasing even when the scale is stuck. Waist circumference drops. Hip measurements shrink. The scale is measuring total body mass, which includes water, glycogen, food volume, and muscle tissue in addition to fat. The scale tells one story. The tape measure tells a more complete one.
People who quit during the plateau, and some do, miss the breakthrough that almost always follows. Within one to three weeks, the scale typically drops several pounds seemingly overnight as the retained water flushes out. This is sometimes called a whoosh effect, and while the mechanism is debated, the pattern is remarkably consistent across thousands of GLP-1 users.
Months 4, 5, and 6: cumulative results
By month four, total weight loss typically ranges from 20 to 35 pounds. Month five pushes that to 25 to 42 pounds. By the six-month mark, the range extends to 30 to 50 pounds for most users, with some people exceeding these numbers significantly.
The SURMOUNT-1 trial for tirzepatide showed average weight loss of 15% of starting body weight at 36 weeks (roughly 8.5 months). The STEP 1 trial for semaglutide 2.4mg showed 14.9% average weight loss at 68 weeks. Extrapolating to the six-month mark, most participants had lost between 12 and 15% of their starting weight.
For a 250-pound person, 12 to 15% represents 30 to 37.5 pounds. For a 200-pound person, it means 24 to 30 pounds. These are averages. The top quartile of responders exceeds these numbers by a wide margin.
The physical transformation at six months is dramatic. Side-by-side photos from day one and month six often show what looks like a different person. Facial features are more defined. The neck area slims considerably. Abdominal fat, which is the most dangerous type metabolically, shows the most dramatic reduction.
Body composition at this point has shifted meaningfully. People who have been exercising consistently throughout their GLP-1 journey often have better muscle definition than they have had in years, not because they gained significant muscle, but because the fat layer covering existing muscle has decreased enough to reveal what was always underneath.
Behavioral and psychological changes at the halfway mark
The six-month mark brings psychological changes that are arguably more important than the physical ones. By this point, you have spent half a year eating differently. The patterns that led to weight gain have been disrupted for long enough that new patterns have taken root.
Portion sizes that felt tiny at month one now feel normal. The amount of food you used to eat seems almost absurd in retrospect. Restaurant meals that you would have finished easily now provide two or three servings. Grocery shopping changes fundamentally because your preferences have shifted toward foods that support your new relationship with hunger and satiety.
The psychological freedom from constant food thoughts is something that GLP-1 users describe as life-changing. People who spent decades thinking about their next meal, planning what they would eat, feeling guilty after eating, and cycling through restriction and overeating find that the mental noise simply quiets down. Food becomes fuel and occasional pleasure rather than an obsession and source of shame.
This mental transformation does not show up in before and after photos. But ask anyone who has experienced it, and they will tell you it matters more than the weight loss itself.
SeekPeptides members frequently discuss these psychological shifts in community forums, sharing strategies for navigating social situations, managing food relationships, and building sustainable habits that will outlast the medication itself.
Month 7 through month 12: long-term transformation and maintenance
The second half of the first year on GLP-1 therapy is where the transformation matures. Weight loss continues but gradually decelerates as the body approaches a new equilibrium. The focus shifts from rapid change to optimization, body recomposition, and building the foundation for lasting results.
The deceleration curve
Weight loss during months seven through twelve follows a predictable deceleration pattern. If you lost 35 pounds in the first six months, you might lose an additional 15 to 25 pounds in the second six months. The rate slows for physiological reasons that have nothing to do with the medication becoming less effective.
As body weight decreases, total daily energy expenditure decreases with it. A 250-pound person burns significantly more calories at rest and during activity than a 200-pound person. This means the caloric deficit that produced rapid weight loss in the early months narrows as you get lighter, even if your eating habits remain exactly the same.
Additionally, metabolic adaptation, sometimes called adaptive thermogenesis, means the body becomes more efficient at lower body weights. Metabolic adaptation during GLP-1 therapy is less severe than with traditional dieting, which is one of the major advantages of GLP-1 medications. But it still occurs to some degree.
The deceleration is not a failure. It is the body reaching a new, healthier equilibrium. The total weight loss at 12 months for most people falls between 15 and 22% of starting body weight. For tirzepatide at the highest dose, the SURMOUNT-1 trial showed an average of 22.5% weight loss at 72 weeks, which represents one of the most significant weight loss results ever achieved with any medication.
Body recomposition in the later months
Months seven through twelve are where body recomposition becomes the primary focus for many people. The scale may move slowly or even stall, but the mirror tells a very different story. This is the phase where people build the physique they actually want, not just a smaller version of their previous body.
With consistent strength training, muscle definition continues to improve even as the scale stabilizes. Body fat percentage continues to drop because muscle gain offsets fat loss on the scale.
A person who weighs the same at month 10 as they did at month 8 but has gained 3 pounds of muscle and lost 3 pounds of fat looks dramatically different.
DEXA scans during this phase often reveal improvements that the scale completely misses. Visceral fat continues to decrease. Bone mineral density stabilizes or improves, particularly important for women. Lean mass percentage increases, which improves metabolic rate and creates a more favorable environment for maintaining weight loss long term.
The 12-month milestone
The one-year GLP-1 before and after comparison is typically the most dramatic. Total weight loss commonly ranges from 40 to 75 pounds, depending on starting weight and individual factors. Some people lose more than 100 pounds in the first year, particularly those who started at higher weights and responded well to the medication.
But weight loss alone does not capture the full scope of the 12-month transformation. Consider the typical changes across all dimensions.
Body measurements tell a comprehensive story. Waist circumference decreases by 4 to 8 inches on average. Hip circumference drops 3 to 6 inches. Chest measurement decreases 2 to 4 inches. Neck circumference drops 1 to 2 inches. These measurement changes often exceed what the raw weight loss would predict, because the shift in body composition means the body is not just smaller but shaped differently.
Metabolic health markers at 12 months are frequently remarkable. Many people who started with prediabetes have normal glucose levels. Cholesterol panels look completely different. Blood pressure has often normalized. Inflammatory markers have dropped to levels associated with significantly reduced disease risk.
Fitness capabilities have transformed. Activities that were difficult or impossible at the starting weight are now routine. Climbing stairs without breathlessness. Walking for miles without joint pain. Playing with children or grandchildren without exhaustion. These functional improvements represent the transformation that matters most for quality of life.
The psychological transformation at one year is profound. Twelve months of changed eating habits, improved body image, and freedom from food obsession have created a fundamentally different relationship with health. People describe feeling like they have their lives back, like a weight has been lifted in every sense of the word.
GLP-1 before and after by specific areas: what changes where
Before and after transformations are not uniform across the body. Understanding where and how changes occur helps set realistic expectations and explains why two people who lose the same amount of weight can look very different in their before and after photos.
Face and neck transformation
Facial changes are often the first thing other people notice, even before overall weight loss becomes obvious. The face loses fat in a specific pattern. Submental fat (the double chin area) typically reduces early, improving jawline definition. Buccal fat (the cheeks) decreases more gradually, creating more angular facial features. Periorbital puffiness, the slight swelling around the eyes that accompanies inflammation and excess weight, resolves as systemic inflammation decreases.
The neck transformation is particularly noticeable. A thinner neck changes the entire appearance of the head and shoulders. Shirt collars fit differently. Necklaces that were tight become loose. The visual impact is dramatic because people see your face and neck in every interaction.
One consideration during facial fat loss is the potential for volume loss that can add years rather than subtract them. People over 40 who lose significant weight sometimes find that facial fat loss creates a slightly aged appearance. This is manageable with proper collagen support, adequate hydration, and in some cases, dermatological interventions. The net effect is still overwhelmingly positive for most people, but it is worth being aware of.
Midsection transformation
The abdominal area undergoes the most medically significant transformation during GLP-1 therapy. Visceral fat, the deep fat surrounding organs, responds particularly well to the metabolic changes GLP-1 medications create. This is not just cosmetically important. Visceral fat is strongly associated with cardiovascular disease, type 2 diabetes, and certain cancers.
Subcutaneous abdominal fat, the layer you can pinch, decreases more slowly than visceral fat. This means that internal health improvements often precede visible midsection changes. CT scans and DEXA scans during the early months frequently show dramatic visceral fat reduction even when the midsection still looks largely unchanged from the outside.
By months four through six, the external changes become obvious. The belly flattens. Love handles shrink. The waistline definition improves. By months eight through twelve, many people achieve a midsection they have not seen since their twenties, or in some cases, ever.
Loose skin in the abdominal area is a legitimate concern for people losing large amounts of weight. The degree of loose skin depends on age, genetics, how long the excess weight was carried, and how much weight is lost. Younger people and those who lose weight more gradually tend to experience less loose skin. Strategies for supporting skin elasticity during weight loss, including adequate protein intake, hydration, and collagen supplementation, can help but do not eliminate the issue entirely for everyone.
Arms, legs, and overall shape
Upper arm fat loss is another early and noticeable change. Sleeves fit more loosely. The upper arm profile becomes more defined, especially for people who combine GLP-1 therapy with resistance training. Arm definition is one of the changes that shows clearly in photos and often generates the most dramatic before and after comparisons.
Leg transformation is significant but often underappreciated. Thigh circumference decreases, reducing chafing and improving comfort. Calf definition improves. The overall leg silhouette changes from cylindrical to more contoured. These changes affect clothing fit dramatically, making fitted pants and shorts more comfortable and flattering.
The overall body shape transformation often involves a shift in proportions rather than just a uniform shrinkage. Someone who carried weight primarily in the midsection may find that weight loss creates a more balanced silhouette. Shoulder-to-waist ratio improves. The body begins to look more athletic and proportioned.
Comparing GLP-1 before and after results: semaglutide vs tirzepatide
Not all GLP-1 medications produce identical before and after results. The two most popular options, semaglutide and tirzepatide, have different mechanisms and produce somewhat different transformation patterns.
Semaglutide results timeline
Semaglutide (brand names Ozempic for diabetes, Wegovy for weight management) is a pure GLP-1 receptor agonist. Clinical trial data from the STEP program provides detailed insight into expected results at each stage.
At 12 weeks (roughly 3 months), average weight loss with semaglutide 2.4mg is approximately 6 to 8% of starting body weight. At 28 weeks (roughly 6.5 months), average weight loss reaches approximately 12 to 14%. At 68 weeks (roughly 16 months), the STEP 1 trial showed average weight loss of 14.9% with semaglutide versus 2.4% with placebo.
The semaglutide transformation tends to be steady and progressive. Weight loss follows a relatively smooth curve with gradual deceleration after the first six months. The medication is well-studied with extensive long-term data supporting both its efficacy and safety profile.
For people interested in semaglutide dosing protocols, the standard titration schedule moves from 0.25mg weekly through 0.5mg, 1.0mg, 1.7mg, and finally 2.4mg, with each dose maintained for approximately four weeks before increasing. This graduated approach minimizes side effects while progressively increasing therapeutic benefit.
Tirzepatide results timeline
Tirzepatide (brand name Mounjaro for diabetes, Zepbound for weight management) is a dual GIP/GLP-1 receptor agonist. This dual mechanism produces notably greater weight loss in clinical trials compared to semaglutide.
The SURMOUNT-1 trial provides the most comprehensive data. At the 5mg dose, average weight loss at 72 weeks was 15%. At 10mg, it was 19.5%. At the maximum 15mg dose, average weight loss reached 22.5%. These numbers represent the highest weight loss ever achieved with any medication in a large-scale clinical trial.
The tirzepatide transformation pattern differs slightly from semaglutide. Weight loss tends to be faster in the early months, likely due to the additional GIP receptor activity. The dual mechanism also appears to provide better preservation of lean mass during weight loss, though head-to-head comparison data is still limited.
Tirzepatide dosing follows a similar escalation pattern from 2.5mg through 5mg, 7.5mg, 10mg, 12.5mg, and 15mg. The dose increases typically occur every four weeks, and many people find their optimal dose somewhere in the middle of the range rather than necessarily at the maximum.
Head-to-head comparison
The SURPASS-2 trial compared tirzepatide directly against semaglutide 1.0mg (not the higher 2.4mg weight management dose). All three tirzepatide doses produced significantly greater weight loss than semaglutide 1.0mg. However, direct comparison against semaglutide 2.4mg is still pending in ongoing trials.
Based on available data, here is a general comparison of expected before and after results.
At 3 months, semaglutide typically produces 6 to 8% weight loss while tirzepatide produces 7 to 10%. At 6 months, semaglutide reaches 10 to 14% while tirzepatide reaches 13 to 18%. At 12 months, semaglutide reaches 13 to 16% while tirzepatide reaches 18 to 23%.
These are averages from clinical trials. Individual results vary enormously based on dose, diet, exercise, metabolic health, genetics, and adherence to the medication protocol. Some people respond better to semaglutide than tirzepatide and vice versa. The choice between them involves factors beyond just weight loss efficacy, including side effect profiles, cost, availability, and individual metabolic considerations.
Factors that determine your personal GLP-1 before and after results
Why do some people lose 20% of their body weight while others on the same medication lose only 8%? The answer involves multiple interacting factors that collectively determine your individual response to GLP-1 therapy.
Starting weight and body composition
People with higher starting weights generally lose more total pounds but a similar or slightly lower percentage of body weight compared to people starting at lower weights. This is partially because higher starting weight means higher daily caloric expenditure, creating a larger absolute deficit when appetite decreases.
Starting body composition also matters. People with higher body fat percentages tend to lose a greater proportion of fat versus lean mass. People who are already relatively lean (under 25% body fat for men or under 32% for women) may find that GLP-1 medications produce less dramatic weight loss but still improve body composition through targeted fat reduction.
Diet quality and protein intake
This is arguably the single most important modifiable factor in determining GLP-1 results. Two people on the same dose of the same medication can achieve dramatically different before and after transformations based on what they eat.
Protein intake is the most critical variable. People who consume adequate protein (0.7 to 1.0 grams per pound of body weight daily) consistently achieve better body composition outcomes. They lose more fat, preserve more muscle, and end up with a more toned, athletic appearance compared to people who eat the same calories but with less protein. Choosing the right protein sources while managing a suppressed appetite requires strategic planning but pays enormous dividends in results.
Overall diet quality matters beyond just protein. Nutrient-dense whole foods support metabolic health, provide essential micronutrients for body processes during rapid weight loss, and help manage the gastrointestinal side effects that sometimes accompany GLP-1 therapy. Processed foods, high-sugar foods, and high-fat foods tend to worsen side effects and provide less nutritional support during transformation.
Exercise and activity level
Exercise is the second most important modifiable factor. GLP-1 therapy creates the deficit. Exercise determines whether the resulting weight loss produces a fit, healthy-looking body or simply a smaller version of the previous body.
Resistance training is particularly important. It signals the body to preserve muscle tissue during caloric deficit, improves insulin sensitivity beyond what the medication achieves alone, increases metabolic rate, and shapes the body in ways that fat loss alone cannot achieve. People who combine GLP-1 therapy with consistent strength training three to four times per week consistently produce the most impressive before and after transformations.
Cardiovascular exercise adds additional caloric burn, improves heart health, and supports mental well-being during the weight loss journey. However, excessive cardio without adequate resistance training can actually lead to greater muscle loss. The optimal approach combines both modalities with an emphasis on strength training.
Daily activity level outside of structured exercise, sometimes called NEAT (non-exercise activity thermogenesis), also significantly impacts results. People who walk regularly, take stairs, stand at their desks, and generally maintain an active lifestyle burn hundreds of additional calories daily compared to sedentary individuals. This difference compounds over months and can represent 10 to 15 additional pounds of fat loss over a year.
Sleep, stress, and recovery
Sleep quality and duration directly affect GLP-1 therapy outcomes. Poor sleep increases cortisol, drives insulin resistance, increases hunger hormones (even partially overriding GLP-1 appetite suppression), and impairs recovery from exercise. People who consistently get 7 to 9 hours of quality sleep achieve measurably better results than those sleeping 5 to 6 hours.
Chronic stress similarly undermines results through cortisol elevation. Elevated cortisol promotes visceral fat storage, increases water retention, impairs muscle recovery, and can trigger emotional eating patterns that the medication only partially counteracts.
Recovery from exercise becomes increasingly important during GLP-1 therapy because the body is operating in a caloric deficit. Adequate rest days, proper stretching, and attention to recovery modalities like BPC-157 for recovery support help maintain training intensity and consistency throughout the transformation.
Medication adherence and timing
Consistent, on-time dosing produces better results than irregular dosing. Missing doses or taking them at inconsistent intervals reduces the steady-state drug levels that produce optimal appetite suppression and metabolic effects. Set a specific day and time for your weekly injection and treat it as non-negotiable.
Injection technique matters more than most people realize. Proper subcutaneous injection ensures consistent absorption. Correct injection technique involves rotating injection sites, using proper needle angle, and following storage and handling guidelines that maintain medication potency.
GLP-1 before and after: realistic expectations by starting BMI
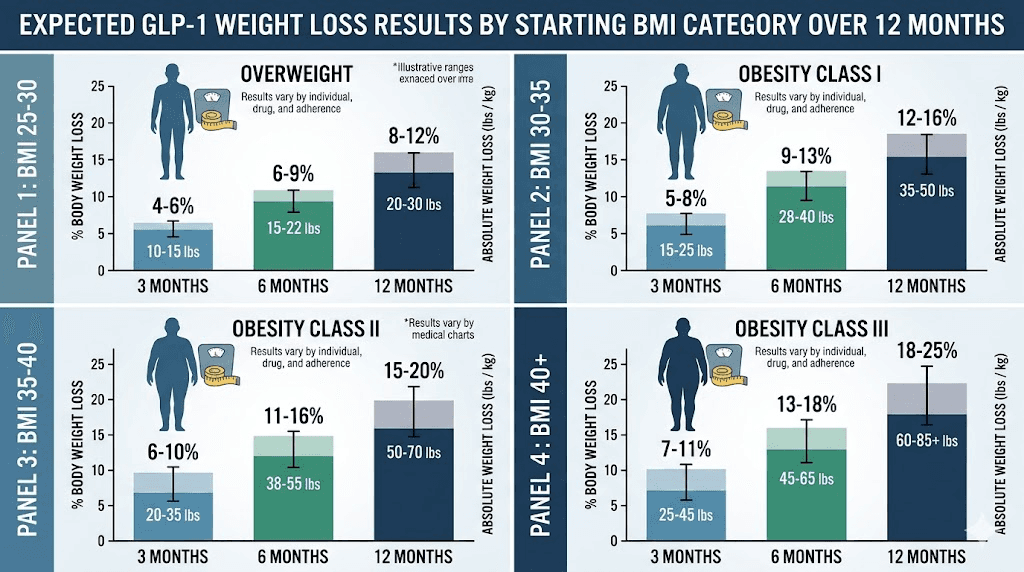
Setting realistic expectations prevents disappointment and helps you recognize genuine progress when it happens. Here is what the clinical data suggests for different starting BMI categories.
BMI 25 to 30 (overweight)
People starting in the overweight range can expect moderate but meaningful weight loss. Typical 12-month results include 10 to 15% body weight loss (20 to 35 pounds for a 200-pound person), 2 to 4 inch waist circumference reduction, noticeable improvement in body composition especially with exercise, and significant improvement in metabolic markers if they were elevated.
The before and after transformation for this group may be less dramatic in photos but often produces the most satisfying results in terms of how people feel. Moving from overweight to normal weight restores energy, eliminates the subtle joint stress that accompanies excess weight, and often resolves early metabolic dysfunction before it progresses to disease.
BMI 30 to 35 (class 1 obesity)
This group typically sees strong responses to GLP-1 therapy. Expected 12-month results include 15 to 20% body weight loss (35 to 55 pounds for a 250-pound person), 4 to 6 inch waist circumference reduction, dramatic improvement in body shape and clothing fit, and substantial improvement in metabolic health markers.
The before and after photos for this BMI range are often the most visually striking because the weight loss is large enough to be obvious but the starting point is not so high that significant loose skin becomes a major factor. Many of the most compelling GLP-1 transformation photos you see online come from people in this starting range.
BMI 35 to 40 (class 2 obesity)
People starting with class 2 obesity often experience the most significant health improvements. Expected 12-month results include 15 to 22% body weight loss (50 to 75 pounds for a 300-pound person), 5 to 8 inch waist circumference reduction, major improvement in mobility and physical function, and often dramatic improvement or resolution of obesity-related health conditions including sleep apnea, fatty liver disease, and joint pain.
The transformation at this BMI range is medically profound. The amount of visceral fat reduction significantly decreases the risk of cardiovascular events, type 2 diabetes, and several cancers. Quality of life improvements are often described as life-changing in a very literal sense.
BMI above 40 (class 3 obesity)
The highest starting BMI group can achieve enormous absolute weight loss with GLP-1 therapy. Expected 12-month results include 15 to 20% body weight loss (65 to 100+ pounds for a 400-pound person), 6 to 10 inch waist circumference reduction, transformative improvement in daily functional capacity, and resolution or significant improvement of multiple obesity-related conditions.
For people in this BMI range, GLP-1 therapy sometimes serves as a bridge to other interventions or as an alternative to bariatric surgery. The weight loss achieved with GLP-1 medications now approaches what was previously only achievable through surgical intervention, though the most severe cases may still benefit from combined approaches.
The side effect timeline: what to expect and when
Every GLP-1 before and after journey involves managing side effects. Understanding the typical timeline helps you prepare, persist through temporary discomfort, and recognize when something requires medical attention versus normal adaptation.
Weeks 1 through 4: the adjustment phase
Gastrointestinal side effects peak during the first month and with each subsequent dose increase. The most common include nausea (affecting 30 to 50% of users), which typically presents as a mild queasy sensation rather than severe nausea. It peaks 24 to 48 hours after injection and improves throughout the week. Eating smaller meals, avoiding fatty foods, and using ginger-based remedies help significantly.
Decreased appetite goes beyond normal satiety. Some people experience genuine food aversion during the first few weeks, where the thought of eating feels unpleasant. This usually normalizes into comfortable reduced appetite within two to three weeks.
Constipation or diarrhea may occur as GLP-1 slows gastric motility, and the change in eating patterns affects gut transit time. Adequate fiber, hydration, and gut health support help manage these symptoms.
Fatigue during the first one to two weeks is common as the body adjusts to significantly lower caloric intake. Energy levels typically improve by week three as the body adapts to its new fuel availability.
Months 2 through 3: dose escalation effects
Each dose increase may bring a mild recurrence of initial side effects, typically lasting three to five days. The pattern is predictable: increase the dose on injection day, experience mild nausea for one to three days, notice renewed appetite suppression, and return to baseline comfort within a week.
Some people develop acid reflux during dose escalation. This responds well to dietary modifications (avoiding acidic foods, not eating close to bedtime, smaller meals) and in some cases, temporary use of over-the-counter antacids. If reflux persists, medical evaluation is warranted.
Injection site reactions occur in approximately 5 to 10% of users. Small red bumps or mild irritation at the injection site are common and usually resolve within a few days. Rotating injection sites between the abdomen, thighs, and upper arms minimizes this issue.
Months 4 through 6: stabilization
By month four, most people have reached their maintenance dose and side effects have largely resolved. The body has adapted to the medication, and the experience settles into a comfortable routine. Appetite suppression remains consistent without the extreme food aversion of the early weeks. Gastrointestinal function normalizes. Energy levels are typically good, often better than before starting the medication due to improved metabolic function and reduced inflammatory burden.
Some people experience hair thinning during months three through six. This is related to the rapid weight loss rather than the medication itself, a phenomenon called telogen effluvium that occurs with any significant weight loss. Hair typically regrows within six to twelve months, and adequate protein intake, biotin supplementation, and peptide support for hair health can minimize the degree of thinning.
Months 7 through 12: long-term adaptation
The second half of the first year is generally smooth from a side effect perspective. The body is fully adapted to the medication. The main consideration during this phase is maintaining adequate nutrition despite continued appetite suppression.
Some people find that appetite suppression decreases somewhat over time. This is not the medication failing. It is the body partially adapting to the GLP-1 signal. The medication remains effective for weight maintenance even if the appetite suppression feels less dramatic than it did initially.
Monitoring for gallbladder issues is important during rapid weight loss. Gallstone formation risk increases during any significant weight loss, and GLP-1 therapy is no exception. Symptoms including right upper abdominal pain, nausea after fatty meals, and pain radiating to the right shoulder should be evaluated promptly.
Regular bloodwork every three to six months helps monitor metabolic improvements and catch any unexpected changes early. Tracking blood sugar levels, liver function, thyroid function, and nutritional markers ensures that the weight loss is occurring safely and sustainably.
Maximizing your GLP-1 before and after transformation: the complete protocol
The difference between average and exceptional GLP-1 results comes down to the supporting protocols you implement alongside the medication. Here is the comprehensive approach that produces the best transformations.
Nutrition protocol for optimal results
Protein first, always. Every meal should start with protein. Target 30 to 50 grams of protein per meal, three to four meals daily. When appetite is severely suppressed (especially during the early weeks and after dose increases), prioritize protein over all other macronutrients. A protein shake counts. Greek yogurt counts. Whatever gets you to your protein target counts.
Total daily protein should reach 0.7 to 1.0 grams per pound of lean body mass, not total body weight. For a 250-pound person with 35% body fat, lean body mass is approximately 162 pounds, making the protein target 113 to 162 grams daily. This is more manageable than targeting based on total weight.
Hydration requires active attention because reduced food intake means less water from food sources. Aim for half your body weight in ounces of water daily, minimum. Dehydration worsens nausea, constipation, fatigue, and can create the illusion of a weight loss plateau through water retention.
Micronutrient supplementation becomes important when caloric intake drops significantly. A comprehensive multivitamin covers basic needs. Additional consideration should be given to vitamin D (most people are deficient regardless of weight), omega-3 fatty acids for inflammation support, magnesium for muscle function and sleep quality, and electrolytes to replace what is lost through the increased water excretion that accompanies early weight loss.
Meal timing affects both results and side effect management. Eating too close to injection time can worsen nausea. Large meals late at night can cause discomfort due to slowed gastric emptying. The optimal pattern for most people involves three moderate meals spaced four to five hours apart, with the last meal finishing at least three hours before bed.
Exercise protocol for the best transformation
The optimal exercise program during GLP-1 therapy prioritizes resistance training while including strategic cardiovascular work.
Resistance training three to four days per week forms the foundation. Focus on compound movements (squats, deadlifts, presses, rows, pull-ups) that engage multiple muscle groups simultaneously. Progressive overload, meaning gradually increasing weight or volume over time, signals the body to maintain and build muscle even during caloric deficit.
A sample weekly schedule might include upper body pushing and pulling on day one, lower body on day two, rest on day three, upper body on day four, lower body on day five, active recovery on day six, and full rest on day seven. This provides enough stimulus for muscle preservation while allowing adequate recovery. A complete strength training program for GLP-1 users details specific exercises, sets, reps, and progression schemes.
Cardiovascular exercise two to three times per week supports heart health and adds caloric expenditure without the muscle-depleting effects of excessive cardio. Walking 30 to 60 minutes daily is the simplest and most sustainable approach. Higher-intensity options like cycling, swimming, or interval training can be incorporated as fitness improves.
The critical rule is this: never let cardio replace resistance training. If you only have time for one type of exercise, choose lifting weights. The body composition benefits of resistance training during GLP-1 therapy are irreplaceable.
Sleep and recovery protocol
Sleep optimization is non-negotiable for best results. Seven to nine hours of quality sleep supports hormone balance, muscle recovery, appetite regulation, and mental health. Practical steps include maintaining a consistent sleep and wake schedule even on weekends, making the bedroom cold (65 to 68 degrees), dark, and quiet, avoiding screens for 60 minutes before bed, and limiting caffeine after noon.
Stress management directly impacts cortisol levels and therefore fat storage patterns. Regular stress reduction practices, whether meditation, deep breathing, time in nature, or social connection, support the metabolic environment that produces the best GLP-1 results.
Tracking and monitoring
What gets measured gets managed. The most successful GLP-1 transformations involve consistent tracking of multiple metrics beyond just body weight.
Weekly weigh-ins at the same time under the same conditions (morning, after bathroom, before eating) provide trend data without the noise of daily fluctuations. Body measurements (waist, hips, chest, arms, thighs) taken every two to four weeks capture body composition changes that the scale misses. Progress photos every two to four weeks create a visual record that is often more motivating than any number. Take them in the same lighting, same clothing, and same poses for meaningful comparison.
Body composition testing via DEXA scan every three to six months provides the most detailed picture of how fat and muscle are changing. If DEXA is not available, bioelectrical impedance scales provide rough estimates that are useful for tracking trends even if the absolute numbers are not perfectly accurate.
Bloodwork every three to six months tracks the metabolic transformation. Key markers include fasting glucose and HbA1c, lipid panel (total cholesterol, LDL, HDL, triglycerides), liver function (ALT, AST), kidney function (creatinine, BUN), thyroid function (TSH, free T4), inflammatory markers (CRP, ESR), and vitamin levels (D, B12, iron panel).
SeekPeptides provides comprehensive guides for interpreting these markers and understanding how they change during GLP-1 therapy, helping members make informed decisions about their health journey.
What happens when you stop GLP-1: before and after discontinuation
No discussion of GLP-1 before and after is complete without addressing what happens when the medication stops. This is arguably the most important topic in the entire GLP-1 conversation, and it is the one that gets the least honest attention.
The weight regain reality
Clinical trial data is clear: most people regain a significant portion of lost weight after discontinuing GLP-1 therapy. The STEP 1 trial extension showed that participants regained approximately two-thirds of their lost weight within one year of stopping semaglutide. Other studies have shown similar patterns.
This is not a personal failure. It is biology. GLP-1 medications work by overriding the body natural weight regulation system, which is powerful and persistent. When the medication is removed, that system gradually reasserts itself. Appetite increases. Metabolic rate adjusts. The biological pressure to return to the previous weight is real and substantial.
However, the framing of this data matters. Regaining two-thirds of lost weight still means retaining one-third. A person who lost 60 pounds and regains 40 after stopping the medication has still lost 20 pounds. Furthermore, many of the metabolic improvements, particularly those related to insulin sensitivity and cardiovascular health, persist partially even with some weight regain.
Strategies for maintaining results after stopping
Some people successfully maintain their results after discontinuing GLP-1 therapy. The common factors among this group include having established strong exercise habits during treatment (particularly resistance training), having completely overhauled eating patterns with a focus on high-protein whole-food diets, gradual tapering rather than abrupt discontinuation, and having lost weight slowly enough for metabolic adaptation to partially recalibrate.
The most successful strategy for maintaining GLP-1 results involves building the behavioral foundation during treatment. The medication provides a window of opportunity where appetite is manageable, motivation is high from visible results, and new habits can take root. People who use this window wisely, who build robust exercise routines, who restructure their food environment, who develop new coping mechanisms for stress that do not involve food, are the ones most likely to maintain results long-term.
Maintaining weight loss after GLP-1 therapy is one of the most actively researched topics in obesity medicine right now. The understanding is evolving rapidly, and new strategies for successful maintenance are emerging from both clinical research and real-world experience.
The case for long-term treatment
An increasing number of medical professionals view GLP-1 therapy as a long-term or permanent treatment for obesity, similar to how statins are used long-term for cholesterol management or blood pressure medications are used indefinitely for hypertension. The argument is straightforward: obesity is a chronic disease with biological drivers that persist regardless of lifestyle changes. Treating it with ongoing medication that effectively manages those drivers is rational medicine.
This perspective is gaining support from insurance companies and medical guidelines. The American Association of Clinical Endocrinology now recommends considering long-term pharmacotherapy for obesity management. The conversation has shifted from when to stop the medication to whether stopping is the right approach for many patients.
For people considering long-term GLP-1 use, the safety data is encouraging. Semaglutide has been used for diabetes management for years, with no emerging safety signals in long-term follow-up.
Tirzepatide data is newer but similarly reassuring so far. The cardiovascular benefits, demonstrated in the SELECT trial showing reduced heart attack and stroke risk with semaglutide, actually argue in favor of continued use for people with cardiovascular risk factors.
Real patterns from GLP-1 transformations: what the data shows
While individual before and after stories are compelling, the aggregate patterns across thousands of GLP-1 users reveal insights that individual stories cannot provide.
The distribution of results
GLP-1 response follows a roughly normal distribution with significant variation. In the STEP 1 trial, about 10% of participants achieved less than 5% weight loss, roughly the same as placebo response. About 50% achieved 15% or greater weight loss. About 30% achieved 20% or greater. And about 10% achieved 25% or greater, representing the super-responders.
This distribution means that while the average result is impressive, individual results vary widely. Some people seem to be particularly responsive to GLP-1 therapy, potentially due to genetic factors affecting GLP-1 receptor density or sensitivity. Others respond less robustly, even with optimal dose, diet, and exercise.
Understanding this distribution helps set appropriate expectations. Hoping for a super-responder outcome while planning for an average one is a psychologically healthy approach. The average outcome is still medically significant and transformative for most people.
Gender differences in transformation
Men and women experience somewhat different GLP-1 transformation patterns. Men tend to lose weight faster in the early months, particularly from the midsection. This is partially because men typically carry more visceral fat, which responds quickly to the metabolic changes GLP-1 creates.
Women may experience more variable results month to month due to hormonal fluctuations across the menstrual cycle. Water retention patterns, appetite changes, and metabolic rate fluctuations tied to the menstrual cycle can create a less smooth weight loss curve. Monthly averages typically even out, but week-to-week variation is often greater in women.
Body composition changes also differ. Men tend to lose proportionally more fat from the trunk and abdomen. Women often see more distributed fat loss, with changes in arms, legs, and hips as well as the midsection. GLP-1 considerations for women include interactions with hormonal contraceptives, effects during perimenopause, and special nutritional considerations.
Age-related patterns
Age influences GLP-1 transformation in several ways. Younger people (under 40) tend to lose weight faster, preserve muscle more easily, experience less loose skin, and achieve more dramatic before and after comparisons. Their metabolic flexibility and skin elasticity support rapid transformation.
People over 50 may lose weight more slowly, require more attention to muscle preservation, and face greater challenges with skin elasticity. However, the health benefits are often even more significant for older individuals because they are at higher baseline risk for obesity-related diseases. A 55-year-old who loses 40 pounds and normalizes their blood pressure, blood sugar, and cholesterol has potentially added years to their life.
The exercise component becomes even more critical for older adults on GLP-1 therapy. Age-related muscle loss (sarcopenia) combined with caloric deficit can create a situation where too much lean mass is lost. Resistance training and adequate protein intake are not optional for this population. They are essential for maintaining functional strength and mobility during weight loss.
GLP-1 before and after: beyond the scale
The most meaningful before and after comparisons go beyond weight and body measurements. The full scope of GLP-1 transformation touches every aspect of daily life.
Physical capabilities transformation
Before GLP-1: struggling to climb two flights of stairs without becoming winded. After: hiking three miles on a weekend without thinking twice about it. Before: avoiding physical activities with friends or family due to embarrassment or inability. After: saying yes to everything from beach vacations to recreational sports.
The functional transformation often brings people to tears when they reflect on it. Things they had given up on, activities they assumed were permanently behind them, suddenly become possible again. This is not hyperbole. It is the lived experience of thousands of people who have undergone significant GLP-1 transformations.
Mental health transformation
The psychological before and after is profound. Clinical data shows significant improvements in depression scores, anxiety measures, and overall quality of life assessments in people who achieve meaningful weight loss with GLP-1 therapy.
The freedom from food obsession deserves emphasis again because it is so transformative. People who spent decades in a cycle of restriction, overeating, guilt, and repeat find that the cycle simply stops. The mental energy previously consumed by food thoughts becomes available for work, relationships, hobbies, and personal growth. This cognitive liberation is consistently rated as one of the most valuable aspects of GLP-1 therapy by people who have experienced it.
Body image improvement follows weight loss but often lags behind. Many people continue to see their pre-weight loss body in the mirror for months after significant transformation. This psychological lag is normal and gradually resolves as the new body becomes the familiar one. Therapy or counseling can be valuable for people who struggle with body dysmorphia or have a long history of weight-related psychological trauma.
Social and relationship transformation
Weight loss changes how people interact with the world, and how the world interacts with them. This is an uncomfortable reality that most GLP-1 discussions avoid. Research consistently shows that people are treated differently based on body size. The social experience of moving from a higher weight to a lower weight often involves receiving more attention, more respect, and more opportunities.
This can be psychologically complex. Some people feel angry that they are treated better now. Others feel grateful. Most feel a mix of emotions that evolves over time. Navigating these social changes is an important but often overlooked aspect of the GLP-1 transformation journey.
Relationships may shift. Partners who are not undergoing their own transformation may feel threatened or left behind. Friends whose social bonds were built around food may feel the dynamic changing. Family members may react with jealousy disguised as concern. Preparing for these relationship dynamics helps navigate them more successfully.
Medical transformation
The medical before and after is often the most objectively impressive aspect of GLP-1 transformation. Consider a typical case: a 45-year-old male starting at 270 pounds with hypertension, prediabetes, elevated cholesterol, and fatty liver disease.
After 12 months of GLP-1 therapy with diet and exercise optimization: weight drops to 205 pounds. Blood pressure normalizes, allowing medication reduction or elimination. HbA1c drops from 6.3% (prediabetes) to 5.2% (normal). Triglycerides drop from 250 to 120 mg/dL. Liver enzymes normalize and imaging shows resolved fatty liver. Sleep apnea resolves, eliminating the need for CPAP.
This type of multi-system medical improvement was previously only achievable through bariatric surgery. The fact that it is now achievable with a weekly injection represents one of the most significant advances in metabolic medicine in decades.
Common mistakes that sabotage GLP-1 before and after results
Understanding what undermines results is as important as understanding what enhances them. These are the most common mistakes that produce disappointing before and after transformations.
Mistake 1: inadequate protein intake
This is the single most common mistake. GLP-1 therapy suppresses appetite indiscriminately. It does not selectively reduce cravings for carbohydrates and fats while preserving protein appetite. Many people on GLP-1 medications end up severely under-eating protein simply because they are not hungry enough to eat adequate amounts of anything.
The consequences are significant: accelerated muscle loss, a soft flabby appearance despite weight loss, reduced metabolic rate, weakened immune function, hair loss, and poor recovery from exercise. Every single one of these problems is preventable with intentional protein prioritization.
The fix: eat protein first at every meal. Use protein supplements (shakes, bars, powders) to fill gaps. Track protein intake for at least the first three months until high-protein habits are automatic. This single change has more impact on the quality of your transformation than any other dietary variable.
Mistake 2: skipping resistance training
Many people view GLP-1 therapy as a weight loss solution and assume that the medication does all the work. It does not. The medication creates the caloric deficit. Without resistance training, that deficit leads to indiscriminate weight loss that includes significant muscle mass. The result is a smaller but still poorly composed body.
The fix: begin a resistance training program as soon as possible after starting GLP-1 therapy. Even two sessions per week provides meaningful muscle preservation benefits. Three to four sessions is optimal. Focus on compound movements with progressive overload. If you are new to lifting, invest in a few sessions with a qualified trainer to learn proper form.
Mistake 3: obsessing over the scale
Daily weigh-ins can be psychologically destructive during GLP-1 therapy. Weight fluctuates by 2 to 5 pounds daily based on water retention, food volume, sodium intake, and hormonal status. These fluctuations are meaningless noise that can trigger anxiety, frustration, and counterproductive behavioral responses.
The fix: weigh yourself once per week under consistent conditions. Better yet, combine weekly weigh-ins with biweekly body measurements and monthly progress photos. The composite picture tells the real story. A week where the scale went up but waist circumference went down is a good week, not a bad one.
Mistake 4: not adjusting expectations for dose escalation periods
Every dose increase brings temporary water retention, digestive changes, and altered eating patterns that can mask ongoing fat loss. People who expect smooth, linear progress are frequently frustrated during these transition periods and may make unnecessary changes to their diet or exercise in response to perceived stalls.
The fix: expect one to two weeks of adjustment after each dose increase. During these periods, focus on how you feel and on maintaining your protein and exercise habits rather than what the scale shows. The fat loss is happening. The scale will catch up once the adjustment period passes.
Mistake 5: using alcohol as a social substitute for food
When food becomes less interesting, some people shift social behaviors toward increased alcohol consumption. This is counterproductive on multiple levels. Alcohol provides empty calories, impairs judgment around food choices, disrupts sleep quality, stresses the liver (which is already working hard during rapid weight loss), and can worsen GLP-1 side effects.
The fix: find non-food, non-alcohol social activities. Physical activities with friends, creative pursuits, or simply adjusting to the reality that social gatherings do not require constant consumption are healthier approaches.
The science behind GLP-1 before and after transformations
Understanding the scientific mechanisms helps explain why GLP-1 transformations look the way they do and why they differ from traditional diet results.
Hormonal changes during GLP-1 therapy
GLP-1 therapy creates a hormonal environment that is distinctly different from caloric restriction alone. During traditional dieting, the body responds to caloric deficit by increasing ghrelin (the hunger hormone), decreasing leptin (the satiety hormone), reducing thyroid hormone output, and increasing cortisol. This hormonal response is why traditional diets feel progressively harder and why weight regain is so common.
GLP-1 therapy partially overrides this response. While some metabolic adaptation still occurs, the direct appetite suppression provided by the medication means that the ghrelin increase is less impactful. Leptin sensitivity improves as fat mass decreases. The cortisol response is blunted because the weight loss does not require the willpower and stress that accompany traditional restriction.
This more favorable hormonal milieu explains why GLP-1 weight loss tends to preserve more muscle mass, produce less hunger and psychological distress, and create a more sustainable long-term trajectory than equivalent weight loss from dieting alone. It also explains why the transformation looks different. People losing weight with GLP-1 therapy often look healthier and more vibrant during the process compared to people losing the same amount of weight through severe caloric restriction.
The inflammation reduction cascade
Excess body fat is an inflammatory condition. Adipose tissue, particularly visceral fat, produces inflammatory cytokines that create systemic inflammation affecting every organ system. This inflammation contributes to insulin resistance, cardiovascular damage, joint deterioration, cognitive impairment, and accelerated aging.
GLP-1 medications reduce inflammation through two pathways. First, the direct anti-inflammatory effects of GLP-1 receptor activation reduce inflammatory signaling independent of weight loss. Second, the reduction in fat mass, particularly visceral fat, removes a major source of inflammatory cytokine production.
The visible results of inflammation reduction include reduced facial puffiness, improved skin quality (clearer, more even tone, reduced redness), decreased joint swelling and pain, improved eye appearance (reduced under-eye bags and redness), and a general appearance of vitality that people describe as looking younger and healthier.
These anti-inflammatory effects are among the reasons why GLP-1 before and after photos often show a person who looks not just thinner but fundamentally healthier. The transformation goes beyond body size. It reflects a shift in the body overall inflammatory state that affects appearance from head to toe.
Neurological changes and food relationship
GLP-1 receptors in the brain are concentrated in areas that regulate appetite, reward, and impulse control. The activation of these receptors by GLP-1 medications creates neurological changes that fundamentally alter the brain relationship with food.
Functional MRI studies have shown that people on GLP-1 therapy show reduced activation in brain reward centers when viewing food images. The neurological pull toward hyperpalatable foods decreases measurably. This is not a subtle effect. People who previously could not walk past a bakery without stopping find that the sight of pastries generates indifference rather than craving.
These neurological changes also appear to extend beyond food for some people. Emerging research suggests that GLP-1 therapy may reduce cravings for alcohol and other addictive substances. While this research is still in early stages, the potential implications for GLP-1 and addiction pathways are significant and actively being studied.
The neurological transformation contributes to the behavioral before and after that underlies the physical transformation. Changed neural pathways lead to changed behaviors lead to changed bodies. The medication initiates this cascade. The resulting behavioral changes sustain it.
Building your personal GLP-1 before and after plan
Every successful GLP-1 transformation begins with a plan. Here is how to build yours for optimal results.
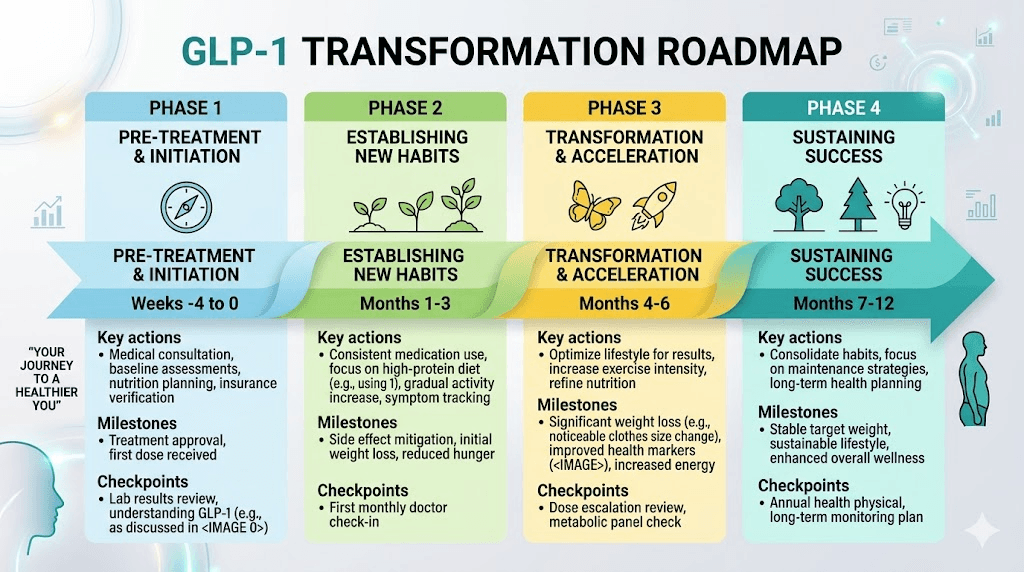
Pre-treatment preparation (weeks 1 through 2 before starting)
Take comprehensive baseline measurements and photos. Weigh yourself. Measure waist, hips, chest, arms, and thighs. Take front, side, and back photos in consistent lighting. Get baseline bloodwork including comprehensive metabolic panel, lipid panel, HbA1c, thyroid panel, and inflammatory markers. This baseline becomes the before in your before and after story.
Establish your nutrition framework before the medication changes your appetite. Calculate your protein target. Stock your kitchen with high-protein foods. Have protein shakes and bars available for the early weeks when appetite may be severely suppressed. Plan your meal structure and timing.
Begin or solidify your exercise routine. Starting a new exercise program simultaneously with a new medication is challenging. If possible, have at least a basic resistance training routine in place before your first injection. If you are completely new to exercise, even establishing a daily walking habit provides a foundation to build upon.
Treatment months 1 through 3: building the foundation
Focus on adapting to the medication while maintaining protein intake and exercise consistency. Do not worry about optimizing every variable. Getting through the adjustment period while keeping protein high and continuing to exercise is a win.
Track your metrics weekly but evaluate progress monthly. The weekly data provides granularity but monthly trends are more meaningful. A month where you lost 6 pounds, reduced your waist by an inch, and improved your lifting numbers is objectively excellent, even if individual weeks within that month felt frustrating.
Schedule a three-month check-in with your healthcare provider. Review bloodwork, assess side effects, discuss dose optimization, and evaluate progress against expectations. This is also a good time for your first body composition assessment (DEXA scan or equivalent).
Treatment months 4 through 6: optimizing results
By this point, you should be comfortable with the medication and have established solid nutrition and exercise habits. Now is the time to optimize.
Evaluate your training program. Are you progressing in strength? If not, consider adjusting volume, intensity, or programming. Progressive overload is essential for continued muscle preservation and development. Consider working with a trainer or following a structured program designed for people in caloric deficit.
Fine-tune your nutrition. Are you consistently hitting your protein target? Are you getting adequate micronutrients? Consider working with a registered dietitian who has experience with GLP-1 patients to optimize your nutrition plan.
Address any persistent side effects. If you are still experiencing significant nausea, constipation, or other issues at this point, discuss dosing adjustments or management strategies with your healthcare provider. Persistent side effects are not normal after the initial adjustment period and may indicate a need for dose modification.
Treatment months 7 through 12: transformation and maintenance
The focus during the second half of the first year shifts toward body recomposition and maintenance planning. Weight loss decelerates naturally, and the emphasis moves toward building the body you want rather than simply losing weight.
Increase exercise intensity and volume if your body is ready. The caloric deficit from the medication plus the increased caloric burn from more intense exercise can continue driving fat loss even as the overall rate slows. Consider adding higher-intensity training methods like interval training or circuit-style resistance work.
Begin planning for long-term maintenance. Whether you plan to continue the medication long-term or eventually taper off, building sustainable habits during this phase is critical. The behaviors you establish while on the medication form the foundation for whatever comes next.
Schedule comprehensive 12-month assessments. Full bloodwork, body composition testing, progress photos, and a thorough review of your transformation to date. This creates the after for your one-year before and after comparison and provides data for planning the next phase of your health journey.
Frequently asked questions about GLP-1 before and after results
How soon will I see visible GLP-1 results?
Most people notice visible changes within four to six weeks of starting GLP-1 therapy. Facial changes and reduced bloating are typically the first visible signs. Significant body shape changes become apparent between months two and three for most users. The timeline varies based on starting weight, dose, and individual response.
What is the average weight loss with GLP-1 medications at 6 months?
Average weight loss at six months is approximately 12 to 15% of starting body weight with semaglutide 2.4mg and 15 to 19% with tirzepatide at higher doses. For a 200-pound person, this translates to 24 to 30 pounds with semaglutide and 30 to 38 pounds with tirzepatide. Individual results vary significantly based on dose, diet, exercise, and metabolic factors.
Will I have loose skin after losing weight on GLP-1?
The degree of loose skin depends on several factors including age, genetics, how much weight you lose, how quickly you lose it, and how long you carried the excess weight. People who lose less than 50 pounds typically experience minimal loose skin issues. Those losing 75 pounds or more may experience noticeable loose skin, particularly in the abdominal area and upper arms. Adequate protein intake, hydration, collagen supplementation, and resistance training help minimize loose skin. In some cases, surgical removal may be considered after weight has stabilized.
Why is my weight loss stalling on GLP-1?
Weight loss plateaus on GLP-1 therapy are normal and typically last one to three weeks. Common causes include water retention (especially after dose increases or during hormonal fluctuations), muscle gain offsetting fat loss (particularly in people who are exercising consistently), metabolic adaptation, and changes in dietary habits that may have gradually increased caloric intake. Continue following your nutrition and exercise plan during plateaus. Measure body dimensions and take photos, as body composition often continues improving even when the scale is static.
Can I build muscle while taking GLP-1 medications?
Yes, though it is more challenging while in caloric deficit. People new to resistance training or returning after a long break can build meaningful muscle while losing fat on GLP-1 therapy. Experienced lifters may primarily maintain rather than gain muscle. The keys are adequate protein intake, consistent progressive resistance training, adequate sleep, and patience. Body recomposition, gaining muscle while losing fat, is achievable and represents the optimal GLP-1 transformation outcome.
How do GLP-1 results compare to bariatric surgery?
Traditional bariatric surgery (gastric bypass or sleeve gastrectomy) produces average weight loss of 25 to 35% of starting body weight. GLP-1 medications at maximum doses produce 15 to 22.5% average weight loss. The gap is narrowing as newer GLP-1 and multi-receptor agonist medications are developed. For many people with BMI 30 to 40, GLP-1 medications now offer a non-surgical alternative with meaningful results. For BMI above 40, comparison between GLP-1 therapy and bariatric surgery involves weighing multiple factors including health status, personal preferences, and long-term management considerations.
What happens to GLP-1 results if I stop the medication?
Clinical data shows that most people regain approximately two-thirds of lost weight within 12 months of stopping GLP-1 therapy. However, people who have established strong exercise habits (particularly resistance training) and high-protein dietary patterns during treatment tend to regain less. Some people maintain most of their results long-term. The decision to continue or discontinue GLP-1 therapy should be made with your healthcare provider based on your individual risk factors, response to treatment, and long-term health goals.
Do GLP-1 before and after results differ between men and women?
Yes, there are some differences. Men tend to lose weight faster initially, particularly from the midsection. Women may experience more week-to-week variation due to menstrual cycle effects on water retention and appetite. However, total weight loss at 12 months is similar between genders when controlling for starting weight. Body fat distribution changes differ, with men seeing more concentrated midsection reduction and women experiencing more distributed fat loss. Both genders achieve significant metabolic health improvements.
Is the weight loss from GLP-1 medications sustainable?
Weight loss is sustainable while continuing the medication. Long-term studies show maintained weight loss with ongoing GLP-1 therapy over two years and beyond. Sustainability after stopping the medication depends heavily on the behavioral and lifestyle changes established during treatment. Strategies for maintaining weight loss after GLP-1 focus on protein-rich nutrition, consistent exercise, and ongoing monitoring.
How much does starting weight affect GLP-1 before and after results?
Starting weight influences absolute pounds lost but percentage of body weight lost is remarkably consistent across starting weights. A person starting at 350 pounds may lose 70 pounds (20%) while a person starting at 200 pounds loses 40 pounds (20%). The visual impact is dramatic for both, though the absolute number differs. People with more weight to lose tend to see faster initial results because their higher metabolic rate creates a larger caloric deficit when appetite decreases.
External resources
GLP-1 Receptor Agonists: Beyond Glycemic Control (Nature Reviews Endocrinology)
Understanding Obesity: Causes, Consequences, and Treatment (The Obesity Society)
And if you have made it this far, in case nobody has told you lately, good morning, and in case I do not see you, good afternoon, good evening, and good night. May your results stay consistent, your protein stay high, and your transformation stay lasting.