Feb 8, 2026

Before you start panicking about finding hair on your pillow, read this first. Retatrutide, the triple-receptor agonist generating massive buzz in weight loss research, has people asking one question that has nothing to do with the scale. Will it make my hair fall out?
It is a fair concern. A real one. Because anyone who has spent time in peptide research communities or read about GLP-1 medications and hair loss has seen the stories. Clumps in the shower drain. Thinning around the temples. Ponytails getting noticeably thinner over weeks. These reports show up with semaglutide, with tirzepatide, and now people want to know whether retatrutide carries the same risk.
The short answer is complicated. The honest answer requires understanding how hair actually grows, why rapid weight loss disrupts it, and what makes retatrutide different from every other peptide in its class. This guide breaks down the clinical trial data, the biological mechanisms behind weight-loss-related hair shedding, the specific nutrients your follicles need during aggressive fat loss, and the practical strategies that researchers and clinicians recommend to minimize shedding while maximizing results on retatrutide protocols.
Whether you are considering retatrutide for the first time, already on a protocol, or just trying to understand the risks before committing, this is the most comprehensive resource available on the topic. SeekPeptides has compiled every relevant study, clinical data point, and practical recommendation into a single guide. No fluff. No speculation. Just what the evidence actually shows.
What retatrutide is and why it matters for this conversation
Retatrutide is not just another GLP-1 medication. It is the first triple-receptor agonist to reach advanced clinical development, simultaneously activating three distinct metabolic receptors that most other weight loss peptides can only dream of targeting.
Those three receptors matter. A lot.
The GLP-1 receptor handles appetite suppression and glucose regulation, the same mechanism that made semaglutide and tirzepatide household names. The GIP receptor enhances insulin secretion and works synergistically with GLP-1 to amplify metabolic effects. And the glucagon receptor, the one that truly sets retatrutide apart, drives energy expenditure, promotes fat burning through lipolysis, and appears to increase thermogenesis in brown adipose tissue.
This triple mechanism produced weight loss results that stunned researchers. In the phase 2 trial published in the New England Journal of Medicine (Jastreboff et al.), participants on the 12mg dose achieved a mean weight reduction of 24.2% at 48 weeks. Let that number sink in for a moment. Nearly a quarter of total body weight, gone in less than a year. At 8mg, the results were still remarkable at 22.8%. Even the lowest dose of 1mg produced an 8.7% reduction.
More recent data from the TRIUMPH-4 trial pushed these numbers even further. Participants taking the 12mg dose for 68 weeks lost an average of 28.7% of their body weight.
And that is precisely where the hair loss conversation begins.
Why more weight loss means more hair risk
Here is the fundamental tension. The very thing that makes retatrutide so effective, its ability to produce rapid, dramatic weight loss, is exactly what creates the conditions for hair shedding. You cannot lose 20-28% of your body weight without sending significant metabolic signals throughout your body. Your hair follicles receive those signals too.
With semaglutide producing roughly 15-17% weight loss and tirzepatide achieving 20-22%, both medications already generate hair loss reports. Retatrutide surpasses both. Simple math suggests that the hair shedding risk with retatrutide could potentially be higher, not because the drug itself is more toxic to follicles, but because the metabolic stress of losing more weight, faster, is simply greater.
Understanding this distinction is critical. The peptide is not poisoning your hair. Your body is redirecting resources during a metabolic emergency. Those are fundamentally different problems with fundamentally different solutions.
What the clinical trials actually say about retatrutide and hair loss
Let us look at the data. Not speculation. Not Reddit anecdotes. The actual published clinical evidence.
The phase 2 trial enrolled 338 adults with obesity but without type 2 diabetes. The most commonly reported adverse events were gastrointestinal. Nausea, diarrhea, vomiting, and constipation dominated the side effect profile, with incidence increasing at higher doses. At the 12mg dose, nausea showed a relative risk of 4.00 compared to placebo, vomiting hit 8.98, and diarrhea reached 2.04.
Hair loss was not listed as a primary or frequently reported adverse event in the published trial data.
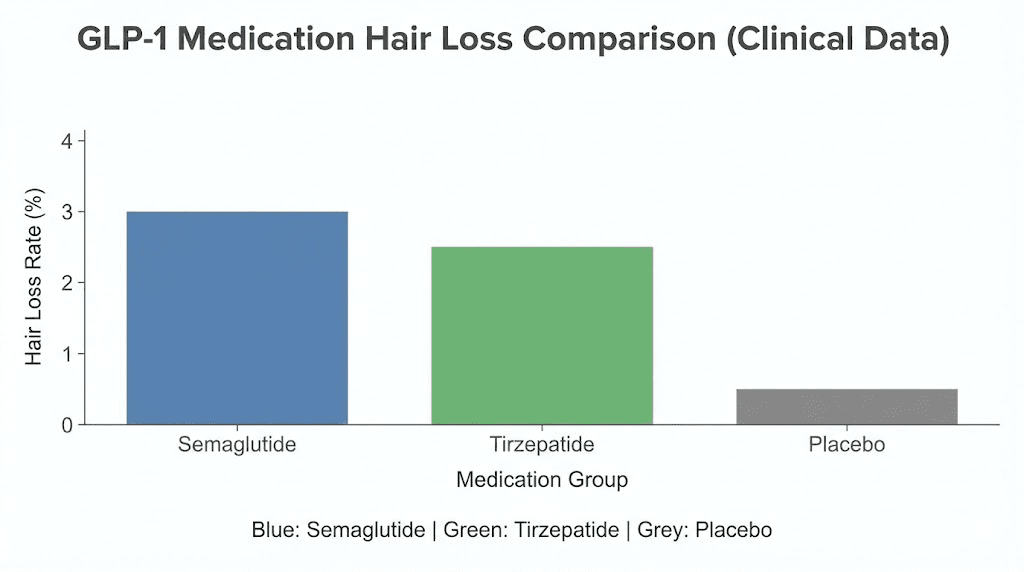
That single sentence deserves emphasis. In the formal clinical trial reports for retatrutide, alopecia did not appear as a common side effect. This stands in contrast to tirzepatide trials, where hair loss was specifically tracked and reported at rates of 4.9-5.3% across dose groups compared to 0.9% with placebo.
Why the absence of data does not mean absence of risk
Before you breathe too deep a sigh of relief, consider this. The phase 2 trial was 48 weeks long with 338 participants. That is a relatively small sample size. Adverse events that occur in 3-5% of users might not reach statistical significance in a group that size. Hair loss often begins 3-6 months after the triggering event, meaning some participants may not have experienced shedding within the study timeframe, particularly those who started on lower doses with gradual titration.
Phase 3 trials, including NCT07232719 and NCT07035093, are currently underway with much larger participant pools. These studies will provide far more definitive data on less common side effects like alopecia. Until those results are published, we must rely on what we know from the broader GLP-1 medication class and the biology of weight-loss-related hair shedding.
What the GLP-1 class data tells us
A systematic review published in PMC (2025), analyzing 5 studies encompassing 2,905 adult patients, found significant associations between GLP-1 receptor agonist use and hair loss. The reporting odds ratios from pharmacovigilance analyses paint a clear picture.
Semaglutide showed a reporting odds ratio of 2.46 (95% CI: 2.14-2.83) for alopecia. Tirzepatide came in at 1.73 (95% CI: 1.42-2.09). In the tirzepatide pivotal trials specifically, hair loss was reported in 4.9-5.3% of treatment groups compared to just 0.9% on placebo, yielding a relative risk of 5.67.
One particularly revealing finding: patients who lost more than 20% of their body weight showed a 5.3% incidence of alopecia, compared to 2.5% in those who lost less than 20%. That dose-response relationship between weight loss magnitude and hair shedding is the single most important data point for anyone considering retatrutide, given that retatrutide routinely produces weight loss exceeding 20%.
Understanding telogen effluvium: the real culprit behind weight loss hair shedding
The medical term you need to know is telogen effluvium. It is not a disease. It is not permanent damage. It is a physiological response, your body reallocating resources during perceived metabolic stress. And understanding it changes everything about how you approach hair protection on retatrutide.
How your hair growth cycle works
Every hair on your head exists in one of three phases at any given time. The numbers matter, so pay attention.
Anagen phase (growth): This is the active growth period, lasting 2-8 years for scalp hair. Under normal conditions, roughly 85% of your hair follicles are in anagen at any given moment. This is where hair gets longer, stronger, and thicker.
Catagen phase (transition): A brief 2-3 week period where the follicle shrinks and detaches from its blood supply. Only about 1-3% of hairs are in catagen at any time.
Telogen phase (resting): The follicle sits dormant for 2-3 months before the hair naturally sheds and a new anagen cycle begins. Normally, 10-14% of your scalp hairs are in telogen.
This is why losing 50-100 hairs per day is completely normal. Those are telogen hairs completing their cycle. You do not notice it because new anagen hairs are simultaneously emerging to replace them.
What happens during telogen effluvium
When your body experiences significant physiological stress, whether from rapid weight loss, caloric restriction, nutritional deficiency, hormonal shifts, surgery, illness, or emotional trauma, it makes a survival calculation. Hair is metabolically expensive to maintain but not essential for survival. So the body prematurely pushes a larger-than-normal percentage of hair follicles from anagen into telogen.
Instead of the normal 10-14% of hairs in telogen, that number can jump to 25-50%. And here is the timing that catches people off guard. The shedding does not happen immediately. It takes 2-4 months for a telogen hair to actually fall out. So you start retatrutide in January, begin losing significant weight by February, and the hair shedding shows up in April or May.
By then, most people have forgotten the timeline. They see hair falling out and blame the drug. The drug did not kill the follicles. The metabolic stress of rapid weight loss shifted the growth cycle months earlier.
Why retatrutide creates a perfect storm for telogen effluvium
Three factors converge with retatrutide that make telogen effluvium particularly likely.
Speed of weight loss. Retatrutide produces faster weight reduction than any other approved or near-approval weight loss medication. The 12mg dose achieved 17.5% reduction at just 24 weeks, progressing to 24.2% at 48 weeks. Some participants in subsequent trials hit 28.7% at 68 weeks. This rate of loss creates significant metabolic stress.
Appetite suppression and caloric deficit. All three receptor pathways in retatrutide suppress appetite. The GLP-1 and GIP receptors reduce hunger signals. The glucagon receptor increases satiety. Combined, these mechanisms can produce dramatic caloric restriction, sometimes to the point where protein and micronutrient intake drops dangerously low.
Hormonal shifts. Adipose tissue is an endocrine organ. Losing 20-28% of body weight reshapes your entire hormonal landscape. Insulin levels change. Leptin levels plummet. Thyroid hormones may shift. Sex hormone binding globulin fluctuates. Each of these hormonal shifts can independently affect the hair growth cycle.
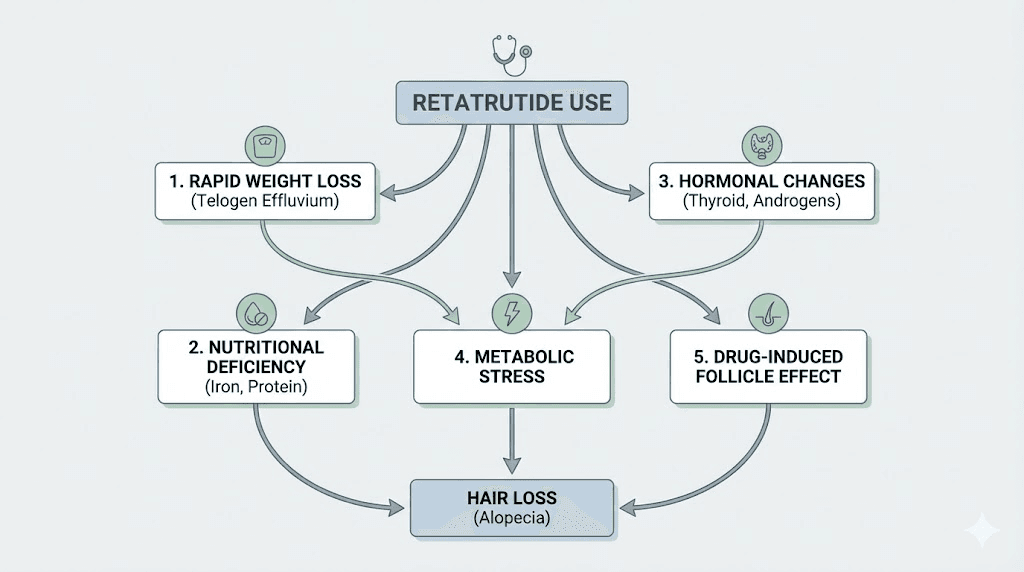
The five mechanisms linking retatrutide to hair shedding
Hair loss on retatrutide does not happen through a single pathway. Five distinct mechanisms can contribute, and understanding each one gives you five distinct intervention points.
Mechanism 1: caloric deficit and metabolic stress
When you eat significantly fewer calories than your body requires, it enters a resource-allocation mode. Vital organs get priority. Immune function gets maintained. Hair growth does not make the cut. Your body literally decides that growing hair is less important than keeping your heart beating and your brain functioning.
Research shows that caloric restriction below 1,200 calories per day significantly increases telogen effluvium risk. With retatrutide suppressing appetite through three simultaneous pathways, many users report eating far less than they realize. Some skip meals entirely without noticing hunger. That caloric deficit accumulates over weeks, and the follicles respond accordingly.
This is why tracking caloric intake matters even when you are not hungry. Your body still needs fuel, and your hair needs that fuel to keep growing.
Mechanism 2: protein deficiency
Hair is made of keratin, a structural protein. Building and maintaining hair requires a steady supply of amino acids, particularly cysteine, methionine, and lysine. When dietary protein drops, the body prioritizes protein for antibodies, enzymes, and muscle maintenance long before it allocates amino acids to hair production.
Studies show that protein intake below 0.8 grams per kilogram of body weight can trigger telogen effluvium independently of any medication. On retatrutide, reduced appetite often means reduced protein consumption, creating a double problem. You are losing weight rapidly (increasing protein requirements for muscle preservation) while simultaneously eating less protein.
The minimum threshold for hair protection during weight loss appears to be around 1.0-1.2 grams of protein per kilogram of body weight daily, with some researchers recommending 1.2-1.6 grams per kilogram for those losing weight aggressively.
Mechanism 3: micronutrient depletion
Four specific micronutrients play outsized roles in hair follicle health, and all four are commonly depleted during rapid weight loss.
Iron: Ferritin levels below 30 ng/mL are strongly associated with telogen effluvium. When you eat less, you consume less dietary iron. When you lose weight rapidly, inflammatory markers can shift, affecting iron absorption. A comprehensive investigation published in the Journal of Cosmetic Dermatology (Durusu Turkoglu, 2024) found significantly lower ferritin levels in telogen effluvium patients compared to controls.
Zinc: Essential for hair follicle cell division and immune function around the follicle. Zinc deficiency is remarkably common during caloric restriction. The body has minimal zinc stores, so even a few weeks of inadequate intake can affect follicle function.
Vitamin D: Supports follicle cycling and immune modulation within the scalp. People losing weight often reduce fat intake, which impairs fat-soluble vitamin absorption. Vitamin D receptors on hair follicle cells are directly involved in the anagen-to-catagen transition.
Biotin (Vitamin B7): While biotin supplementation has not been proven to reverse telogen effluvium specifically, true biotin deficiency does cause hair loss. Individuals on very low calorie diets may develop subclinical biotin deficiency that contributes to hair fragility.
Mechanism 4: hormonal cascade effects
The hormonal changes during rapid weight loss are profound and interconnected. Insulin levels drop, which is metabolically beneficial but also affects insulin-like growth factor (IGF-1), a hormone that directly stimulates hair follicle growth. Leptin, produced by adipose tissue, plummets as fat stores shrink, and leptin receptors on hair follicles play a role in maintaining the anagen phase.
For women, rapid fat loss can shift the estrogen-to-androgen ratio. Fat tissue produces estrone through aromatization. Losing that tissue reduces circulating estrogens while potentially unmasking androgenic effects. This can contribute to female pattern hair thinning in genetically susceptible individuals, a distinct pattern from telogen effluvium that requires different management.
Thyroid function may also shift during significant weight loss, with some individuals developing subclinical hypothyroid patterns that further slow hair growth.
Mechanism 5: psychological stress amplification
This mechanism often gets overlooked. The psychological stress of managing a dramatic body transformation, dealing with GI side effects, adapting to new eating patterns, and the anxiety about potential side effects like hair loss, can itself trigger or worsen telogen effluvium.
Cortisol, the primary stress hormone, has direct effects on hair follicle cycling. Chronic stress pushes follicles into premature catagen. The irony is brutal: worrying about hair loss can actually cause hair loss. This creates a feedback loop where initial shedding causes anxiety, which causes more shedding, which causes more anxiety.
Who is most at risk for hair loss on retatrutide
Not everyone on retatrutide will experience hair shedding. Risk factors stack, and understanding your personal risk profile allows for better prevention strategies.
High-risk factors
Higher doses. The 8mg and 12mg doses of retatrutide produce faster, more dramatic weight loss. The phase 2 trial showed that the 12mg group lost 24.2% of body weight at 48 weeks versus 8.7% in the 1mg group. Greater weight loss velocity correlates with higher telogen effluvium incidence.
Women. Female biology is more susceptible to telogen effluvium for several reasons. Hormonal fluctuations during weight loss disproportionately affect women. Estrogen shifts from fat loss impact hair more in females. Women also tend to have longer anagen phases, meaning more follicles are potentially vulnerable to premature telogen transition.
Pre-existing nutritional deficiencies. If your iron, zinc, vitamin D, or protein levels were already borderline before starting retatrutide, the additional metabolic stress of rapid weight loss will push them over the threshold faster. Many people with obesity have paradoxically low micronutrient levels due to poor dietary quality despite high caloric intake.
Previous history of telogen effluvium. If you have experienced stress-related hair shedding before, whether from pregnancy, surgery, illness, or a previous weight loss attempt, your follicles have demonstrated susceptibility to this pattern. You are more likely to experience it again.
Genetic predisposition to androgenetic alopecia. If you already carry genes for pattern hair loss, the hormonal shifts from rapid weight loss can accelerate and unmask what was previously a slow, barely noticeable process.
The hair loss in this case may have a different distribution pattern, concentrated at the temples and crown rather than diffusely across the scalp.
Thyroid issues. Even subclinical thyroid dysfunction amplifies hair loss risk. If you have borderline thyroid function before starting retatrutide, monitor carefully.
Lower-risk factors
Some characteristics reduce your risk. Being male (paradoxically, except for androgenetic alopecia), starting at lower retatrutide doses with slow titration, maintaining excellent nutrition throughout, having no history of stress-related shedding, and having robust baseline micronutrient levels all lower your likelihood of significant hair loss.
How retatrutide compares to other weight loss peptides for hair loss risk
Understanding where retatrutide sits relative to other medications helps calibrate realistic expectations.
Medication | Type | Avg weight loss (48 wk) | Hair loss ROR | Hair loss risk level |
|---|---|---|---|---|
GLP-1 agonist | 15-17% | 2.46 | Moderate | |
GLP-1/GIP dual agonist | 20-22% | 1.73 | Moderate | |
Retatrutide | GLP-1/GIP/Glucagon triple agonist | 24-29% | Insufficient data | Likely moderate-high |
Amylin analog | Variable (combo) | Limited data | Unknown | |
GLP-1/Glucagon dual agonist | 18-20% | Limited data | Likely moderate |
The pattern is clear. Greater weight loss correlates with greater hair shedding risk. Retatrutide produces the most weight loss. The logical inference, supported by the established relationship between weight loss magnitude and telogen effluvium incidence, is that retatrutide users face a meaningful risk of temporary hair shedding.
But here is what the table does not show: retatrutide may also have some unique characteristics that could theoretically mitigate hair loss risk. The glucagon receptor activation increases energy expenditure, meaning some of the weight loss comes from increased caloric burn rather than purely from caloric restriction. If the caloric deficit is relatively smaller despite larger weight loss, the metabolic stress signal to hair follicles might be somewhat attenuated. This remains speculative and requires direct clinical data to confirm.
The complete hair protection protocol for retatrutide users
Prevention is far more effective than treatment. If you are starting or considering retatrutide, implementing a comprehensive hair protection strategy from day one dramatically reduces your risk of significant shedding.
Strategy 1: nutritional fortification (the foundation)
This is the single most impactful intervention. Most weight-loss-related hair shedding traces directly back to nutritional inadequacy. Fix the nutrition, and you address the primary mechanism.
Protein targets:
Minimum: 1.0 grams per kilogram of body weight daily
Optimal: 1.2-1.6 grams per kilogram daily
Focus on complete proteins containing all essential amino acids
Spread protein intake across 3-4 meals (do not front-load or skip meals)
Prioritize sources rich in cysteine, methionine, and lysine (eggs, fish, poultry, Greek yogurt)
When appetite is severely suppressed on retatrutide, protein shakes, Greek yogurt, and collagen peptide supplements become valuable tools for hitting protein targets without requiring large volume meals.
Iron management:
Get baseline ferritin levels checked before starting retatrutide
Target ferritin above 50 ng/mL (ideally 70+ for optimal hair health)
If levels are below 30 ng/mL, supplement with 18-36mg elemental iron daily
Take iron with vitamin C for enhanced absorption
Avoid taking iron with calcium, coffee, or tea (which inhibit absorption)
Recheck ferritin every 3 months during treatment
Zinc supplementation:
15-30mg of zinc gluconate or zinc picolinate daily
Take with food to prevent nausea
Balance with 1-2mg copper if supplementing above 25mg zinc (zinc competes with copper for absorption)
Zinc is particularly important during the first 3-6 months of rapid weight loss
Vitamin D optimization:
Target blood levels of 40-60 ng/mL
Most people need 2,000-5,000 IU daily, especially during caloric restriction
Take with a fat-containing meal for optimal absorption
Test levels at baseline and every 3-6 months
Biotin and B-vitamins:
5,000mcg biotin daily (standard hair-support dose)
A B-complex supplement covers folate, B12, and B6, all of which support cellular processes in the follicle
Note: high-dose biotin can interfere with certain lab tests, so inform your healthcare provider
Strategy 2: controlled weight loss pacing
The relationship between weight loss speed and hair shedding is well-established. Losing 1-2 pounds per week carries significantly less telogen effluvium risk than losing 3-5 pounds per week, even if the total weight lost over time is the same.
Practical approaches:
Start retatrutide at the lowest dose and titrate slowly
Follow the recommended retatrutide titration schedule rather than jumping to high doses
If weight loss exceeds 3 pounds per week consistently, consider slightly increasing caloric intake
Ensure you are eating at least 1,200 calories daily, preferably 1,400-1,600
Do not skip meals even when appetite is suppressed
The phase 2 trial data showed that starting at 2mg (rather than 4mg) significantly reduced GI side effects. The same gradual approach likely reduces the metabolic shock that triggers telogen effluvium.
Strategy 3: baseline lab work and monitoring
You cannot manage what you do not measure. Before starting retatrutide, and at regular intervals during treatment, check the following:
Pre-treatment labs (essential):
Complete blood count (CBC)
Ferritin and iron studies
Zinc (plasma or serum)
Vitamin D (25-hydroxy)
Thyroid panel (TSH, free T3, free T4)
Complete metabolic panel
Vitamin B12 and folate
Monitoring schedule:
Month 3: Repeat ferritin, zinc, vitamin D, thyroid panel
Month 6: Full panel repeat
Month 9: Full panel repeat
Month 12: Comprehensive reassessment
If any values are trending downward despite supplementation, aggressive correction before clinical hair loss appears is critical. Waiting until hair starts falling out means the telogen shift already happened months ago.
Strategy 4: topical interventions
While addressing the root cause nutritionally is primary, topical interventions can provide additional support for follicles under stress.
Evidence-supported topical options:
Minoxidil (2-5%): The only FDA-approved topical for hair loss. Extends the anagen phase and increases follicle blood supply. Can be used preventively during GLP-1 treatment. Start at 2% to assess tolerance before moving to 5%.
Copper peptides (GHK-Cu): Research shows GHK-Cu promotes follicle size increase and may extend anagen duration. Available in topical formulations and hair serums.
Rosemary oil: Multiple studies show comparable efficacy to 2% minoxidil for stimulating hair growth. Apply diluted in a carrier oil to the scalp 2-3 times weekly.
Low-level laser therapy (LLLT): FDA-cleared devices that stimulate follicle activity through photobiomodulation. Most effective when used consistently (3-4 times per week).
PTD-DBM peptide is another compound gaining attention for its potential to inhibit CXXC5, a protein that suppresses hair follicle neogenesis. While still primarily in research stages, it represents an emerging approach to hair restoration.
Strategy 5: scalp care during shedding
If shedding does begin despite preventive measures, how you treat your hair during the shedding phase matters significantly.
Do:
Use a gentle, sulfate-free shampoo
Condition every wash (hydrated hair is less prone to breakage)
Pat dry gently rather than rubbing vigorously
Use a wide-tooth comb, never a fine-tooth comb on wet hair
Sleep on a silk or satin pillowcase (reduces friction)
Keep up regular washing (skipping washes does not save hair, it just saves the fallen hairs for one dramatic shower)
Do not:
Use tight hairstyles (ponytails, braids, buns) that create traction
Apply heat styling tools frequently
Use harsh chemical treatments (bleaching, perming, relaxing)
Pull or tug at shedding hair (it will fall when ready)
Obsessively count fallen hairs (it amplifies stress, which worsens shedding)
Strategy 6: stress management (seriously)
This strategy sounds soft compared to lab work and supplementation, but the cortisol-hair-loss connection is well-documented. Chronic psychological stress independently pushes follicles into premature catagen.
Practices that measurably reduce cortisol: regular exercise (moderate intensity, not exhausting), adequate sleep (7-9 hours), mindfulness or meditation practice, limiting catastrophic thinking about hair loss, and maintaining social connections.
One practical tip that clinicians report helps enormously: take progress photos of your hair monthly from the same angles under the same lighting. Objective visual evidence prevents the subjective perception that hair loss is worse than it actually is. Many people experiencing telogen effluvium perceive 80% hair loss when the objective reduction is 10-15%.
Timeline: what to expect with hair on retatrutide
Understanding the timeline prevents panic and enables appropriate interventions at each stage.
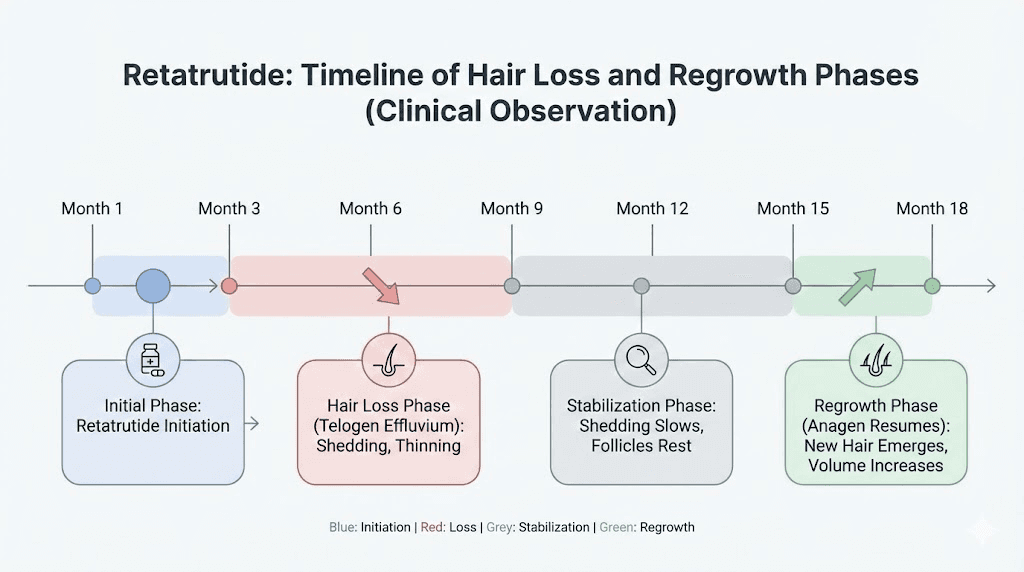
Months 1-2: baseline establishment
Retatrutide titration typically begins at low doses. Weight loss is starting but not yet dramatic. Hair should appear normal during this period. This is your window for getting baseline labs done and establishing nutritional supplementation routines.
Months 3-4: the silent shift
By now, meaningful weight loss has occurred. If follicles are going to shift into telogen, the process begins during this window. But you will not see the results yet. The hair is still attached. This is the most critical prevention window. If you have not started nutritional fortification by this point, start immediately.
Months 4-6: potential shedding onset
If telogen effluvium is going to manifest, this is when most people notice it. Increased hair in the shower drain, on the pillow, in the hairbrush. The shedding can be alarming, but remember: these are hairs that shifted into telogen months ago. They were already destined to fall. The follicles beneath them are not dead.
Do not stop retatrutide solely because of hair shedding. The shedding would continue for weeks even if you stopped immediately, because the telogen shift already occurred. Instead, double down on nutritional optimization and discuss your options with a healthcare provider.
Months 6-9: peak shedding and stabilization
For those who experience telogen effluvium, shedding typically peaks around month 6 and begins to stabilize. If you have been maintaining excellent nutrition, new anagen hairs are already growing beneath the shedding telogen hairs. The density may look thinner, but the follicles are actively cycling back into growth.
Months 9-12: recovery begins
Hair regrowth becomes visible. New hairs emerging from previously affected follicles will be shorter, creating a mix of lengths that some people describe as wispy or fine. This is normal. These hairs will thicken and lengthen over the following months. Hair grows approximately 1-1.25 cm per month, so full visual recovery takes 6-12 months after the shedding phase ends.
Months 12-18: full recovery
Most people who experienced telogen effluvium on GLP-1 medications report near-complete recovery within 12-18 months of onset, provided they maintained adequate nutrition and the shedding was truly telogen effluvium (not androgenetic alopecia or another condition). The hair is back. The volume returns. The panic was, in retrospect, worse than the outcome.
When hair loss on retatrutide is NOT telogen effluvium
Not all hair loss during retatrutide treatment is benign telogen effluvium. Recognizing the difference could save you from mismanaging the situation.
Androgenetic alopecia unmasking
Rapid weight loss and hormonal shifts can unmask or accelerate androgenetic alopecia (pattern hair loss) in genetically susceptible individuals. Unlike telogen effluvium, which causes diffuse thinning all over the scalp, androgenetic alopecia follows specific patterns: receding hairline and crown thinning in men, widening central part in women.
If your hair loss follows a pattern distribution rather than diffuse shedding, consult a dermatologist. Treatment differs significantly, potentially involving finasteride, dutasteride, spironolactone (for women), or other anti-androgen therapies.
Alopecia areata
A case report published in 2025 documented alopecia areata, an autoimmune-mediated patchy hair loss, following semaglutide treatment. This presents as distinct round or oval bald patches rather than diffuse thinning. It is rare, but the immune-modulatory effects of weight loss and hormonal changes could theoretically trigger autoimmune responses in susceptible individuals.
Patchy hair loss requires prompt dermatological evaluation and potentially immunosuppressive treatment.
Thyroid-related hair loss
Significant weight loss can affect thyroid function, and both hypothyroidism and hyperthyroidism cause hair loss with distinct characteristics. If your hair loss is accompanied by fatigue, cold intolerance, dry skin, or unexpected changes in weight loss rate, check thyroid function immediately.
Nutrient deficiency alopecia
Severe iron deficiency, zinc deficiency, or vitamin D deficiency can cause hair loss that looks similar to telogen effluvium but requires specific nutrient correction rather than time. This is why baseline and ongoing lab work is so important. You cannot rely on symptoms alone to distinguish between types of hair loss.
Retatrutide vs semaglutide vs tirzepatide: a hair loss comparison
Let us break down how these three major weight loss peptides compare specifically on the hair loss question.
Semaglutide and hair loss
Semaglutide has the most real-world data on hair loss. With millions of users worldwide, the pharmacovigilance signal is clear: reporting odds ratio of 2.46 for alopecia compared to other medications. Clinical trial data from the STEP program documented hair-related adverse events, though at rates not dramatically different from placebo when controlled for weight loss magnitude.
The semaglutide-specific considerations include its purely GLP-1 mechanism, which creates profound appetite suppression without the energy expenditure increase that retatrutide offers. This means more of the weight loss comes from caloric restriction, potentially creating greater nutritional stress.
Tirzepatide and hair loss
Tirzepatide provides the most directly comparable data because it was the first dual-agonist to track hair loss in pivotal trials. The numbers are specific: 4.9-5.3% across dose groups versus 0.9% placebo. Interestingly, a case report published in PMC documented substantial hair regrowth with tirzepatide in a patient with insulin resistance, suggesting that the metabolic improvements from these medications can sometimes benefit hair rather than harm it.
This finding is fascinating. Treatment of insulin resistance with tirzepatide leading to improvement of hair loss challenges the narrative that all GLP-1-class medications inevitably damage hair. The relationship is more nuanced than simple cause and effect.
Where retatrutide likely falls
Based on the pattern that greater weight loss correlates with greater hair shedding risk, and given that retatrutide produces the most aggressive weight loss of any medication in the class, the logical prediction is that retatrutide will show a hair loss incidence somewhere at or above tirzepatide levels (5% or higher) in large-scale clinical trials.
However, the glucagon receptor component of retatrutide introduces a variable that the other medications lack. Glucagon promotes energy expenditure and thermogenesis. If a meaningful portion of retatrutide weight loss comes from increased metabolic rate rather than purely reduced intake, the nutritional stress on follicles may be somewhat less severe than the raw weight loss numbers would predict.
This remains theoretical until phase 3 data is published. Do not assume protection. Plan for prevention.
Specific protocols for hair protection during retatrutide use
Here are three practical protocols based on risk level. Choose the one that matches your profile.
Protocol A: low risk (preventive maintenance)
For: Men without family history of pattern hair loss, no prior telogen effluvium, starting at low doses, good baseline nutrition.
Approach:
1.0g protein per kg body weight daily
Standard multivitamin with iron (if male, iron-free if ferritin is above 100)
2,000 IU vitamin D daily
Baseline labs before starting, repeat at month 6
Follow standard retatrutide titration
No topical interventions needed unless shedding begins
Expected outcome: Minimal to no noticeable hair changes.
Protocol B: moderate risk (active protection)
For: Women, anyone on 8mg+ doses, those with borderline nutritional status, anyone who has experienced telogen effluvium before.
Approach:
1.2-1.4g protein per kg body weight daily (track with an app)
Iron supplementation to maintain ferritin above 50 ng/mL
30mg zinc daily with 1mg copper
5,000 IU vitamin D daily (adjust based on levels)
5,000mcg biotin daily
B-complex supplement
Collagen peptides 10-15g daily (provides glycine and proline for hair structure)
Baseline labs before starting, repeat at months 3, 6, and 9
Consider starting 2% minoxidil preventively
Monthly hair progress photos
Minimum 1,400 calories daily even when appetite is low
Expected outcome: Mild shedding possible around months 4-6, generally self-limiting with recovery beginning by month 8-9.
Protocol C: high risk (aggressive protection)
For: Women with history of telogen effluvium, anyone with family history of pattern hair loss AND on high-dose retatrutide, individuals with known nutritional deficiencies, those experiencing early signs of shedding.
Approach:
1.4-1.6g protein per kg body weight daily (non-negotiable)
Iron supplementation targeting ferritin above 70 ng/mL
30mg zinc + 2mg copper
5,000 IU vitamin D (adjust to target 50-60 ng/mL serum levels)
5,000mcg biotin + full B-complex
Collagen peptides 15-20g daily
Omega-3 fatty acids 2-3g daily (anti-inflammatory support for scalp)
5% minoxidil applied nightly
GHK-Cu topical applied to scalp 3-4 times weekly
Low-level laser therapy 3-4 times weekly
Baseline labs + repeat every 2-3 months
Dermatologist consultation before starting
Consider slower retatrutide titration (extend each dose step by 1-2 weeks)
Minimum 1,500 calories daily
Stress management protocol (daily meditation, adequate sleep)
Expected outcome: Moderate shedding may still occur but duration and severity should be significantly reduced. Recovery typically begins within 3-4 months of shedding onset.
What to do if hair loss has already started
Maybe you are reading this because it is already happening. Hair is coming out more than usual. Here is your action plan.
Step 1: do not panic (and do not stop retatrutide abruptly)
The hair that is shedding was programmed to shed months ago. Stopping retatrutide today will not stop the shedding tomorrow. Those telogen hairs are already committed to falling. What stopping retatrutide WILL do is eliminate the metabolic benefits you are gaining and potentially lead to weight regain, which creates its own set of hormonal disruptions that can trigger a second wave of shedding.
Talk to your healthcare provider about your options. Dose adjustment might be appropriate. Complete discontinuation rarely is.
Step 2: get lab work immediately
Check ferritin, zinc, vitamin D, thyroid panel, and a complete metabolic panel. Address any deficiencies aggressively. Iron deficiency anemia can mimic and compound telogen effluvium, and correcting it directly accelerates recovery.
Step 3: implement Protocol C
If you were not already on an aggressive hair protection protocol, start Protocol C from the section above immediately. It is never too late to optimize nutrition and support follicle recovery.
Step 4: see a dermatologist
A board-certified dermatologist can perform a pull test, trichoscopy, and potentially a scalp biopsy to determine whether your hair loss is telogen effluvium, androgenetic alopecia, alopecia areata, or something else entirely. The treatment for each is different. Do not self-diagnose.
Step 5: document and monitor
Take consistent photos every 2 weeks. Track the volume of hair shed daily (place a hair catcher in your shower drain and roughly estimate). Note whether shedding is increasing, stable, or decreasing. This data is invaluable for your healthcare provider and for your own reassurance when recovery begins.
The recovery data: does hair grow back after GLP-1-related shedding
The single most reassuring fact about telogen effluvium: it is almost always reversible.
The systematic review data supports this. While the Burke et al. study found that 11.9% of patients experienced worsening, 0.4% saw resolution, and 0.8% stabilized during the study period, the relatively short follow-up means many participants were still in the active shedding phase when assessed. Longer-term data consistently shows recovery.
Case reports documented in the same review showed that some patients on tirzepatide experienced substantial hair regrowth over 9-12 months of treatment. The Desir et al. study of 81 patients (47 responders) demonstrated significant improvement in hair outcomes with extended GLP-1 therapy over a mean of 3.04 years.
The message is clear: for the vast majority of people who experience hair shedding on GLP-1-class medications including retatrutide, the hair grows back. The timeline is measured in months, not years. Recovery is the rule, not the exception.
Hair grows approximately 1-1.25 cm per month. After telogen effluvium resolves and follicles re-enter anagen, visible new growth appears within 3-6 months. Full restoration of pre-shedding volume typically takes 6-12 months after shedding ceases.
Advanced considerations for researchers
For those following the science closely, several emerging research areas may reshape our understanding of retatrutide and hair health.
The GLP-1 receptor on hair follicles
GLP-1 receptors have been identified on dermal papilla cells, the signaling center at the base of each hair follicle. The direct effect of GLP-1 receptor activation on follicle cycling is still being investigated. Some researchers hypothesize that sustained GLP-1 receptor stimulation could directly influence the anagen-to-catagen transition, independent of weight loss effects. If true, this would represent a drug-specific mechanism beyond telogen effluvium.
The glucagon receptor and brown fat thermogenesis
Retatrutide glucagon receptor activation increases energy expenditure through brown adipose tissue thermogenesis. This is metabolically distinct from caloric restriction. If retatrutide achieves significant weight loss through increased expenditure rather than purely decreased intake, the nutritional stress on follicles could be meaningfully different from what semaglutide or tirzepatide produce.
No studies have directly compared the hair-follicle impact of energy-expenditure-driven weight loss versus caloric-restriction-driven weight loss at equal total weight lost. This is a critical gap in the research.
Insulin sensitivity restoration and hair health
The tirzepatide case report showing hair regrowth in an insulin-resistant patient raises an important question. Insulin resistance itself impairs hair follicle function through multiple pathways: reduced IGF-1 signaling, chronic inflammation, and microvascular dysfunction. If retatrutide dramatically improves insulin sensitivity (which the clinical data strongly suggests it does), the long-term net effect on hair might actually be positive for individuals whose prior hair thinning was driven by metabolic dysfunction.
This possibility means that the initial telogen effluvium from rapid weight loss could be followed by improved hair quality once metabolic health normalizes. Early shedding followed by better hair than you started with. Some users of tirzepatide and semaglutide have reported exactly this pattern.
Frequently asked questions
Does retatrutide directly damage hair follicles?
No. Based on all available evidence, retatrutide does not directly damage or destroy hair follicles. The hair shedding associated with GLP-1 class medications, including retatrutide, is primarily caused by the metabolic stress of rapid weight loss, not by direct drug toxicity to follicles. The condition is called telogen effluvium and is temporary and reversible in the vast majority of cases.
How common is hair loss on retatrutide specifically?
The phase 2 clinical trial did not report hair loss as a frequent adverse event. However, with only 338 participants and the known relationship between weight loss magnitude and hair shedding, the true incidence will not be established until larger phase 3 trials report their results. Based on data from similar medications, an incidence of 3-7% is a reasonable estimate.
Will my hair grow back if it falls out during retatrutide treatment?
Yes, in the vast majority of cases. Telogen effluvium is reversible. Once the triggering stress stabilizes, whether from nutritional optimization, weight loss stabilization, or both, follicles re-enter the growth phase. Full visual recovery typically takes 6-12 months after shedding peaks. The follicles remain alive throughout the process.
Should I stop retatrutide if I notice hair loss?
Not necessarily, and not without consulting your healthcare provider. Stopping retatrutide will not immediately stop shedding (the telogen transition already happened) and may lead to weight regain that creates additional metabolic stress. Instead, focus on optimizing nutrition, checking lab values, and consulting a dermatologist for proper diagnosis and management.
Is hair loss worse on retatrutide than on semaglutide or tirzepatide?
No direct comparison data exists. However, retatrutide produces greater weight loss (24-29% vs 15-22%), and greater weight loss correlates with higher telogen effluvium incidence. The glucagon receptor component may partially offset this by increasing energy expenditure rather than relying solely on caloric restriction. Until phase 3 data is available, assume the risk is at least comparable to tirzepatide.
What supplements should I take to prevent hair loss on retatrutide?
The evidence supports iron (targeting ferritin above 50 ng/mL), zinc (15-30mg daily), vitamin D (2,000-5,000 IU daily), biotin (5,000mcg daily), a B-complex, and adequate protein (1.0-1.6g per kg body weight). Collagen peptides (10-15g daily) provide additional amino acid support for hair structure. Get baseline labs and monitor throughout treatment.
Can I use minoxidil while on retatrutide?
Yes. Topical minoxidil (2-5%) can be used safely alongside retatrutide and may help prevent or minimize telogen effluvium. Some clinicians recommend starting minoxidil preventively when beginning GLP-1 class medications, particularly for individuals at higher risk of hair loss.
How long after starting retatrutide does hair loss begin?
If telogen effluvium occurs, it typically becomes noticeable 3-6 months after the onset of rapid weight loss. Since retatrutide involves dose titration, significant weight loss may not begin immediately, potentially delaying the onset of any shedding. Most people who experience it notice increased shedding around months 4-6 of treatment.
Does the dose of retatrutide affect hair loss risk?
Indirectly, yes. Higher retatrutide doses produce faster and more dramatic weight loss, which correlates with higher telogen effluvium risk. The 12mg dose, which produces 24-29% weight loss, carries theoretically higher risk than the 1mg dose at 8.7% weight loss. Slow titration and adequate nutrition at every dose level are your best protection.
Is the hair loss from retatrutide permanent?
Telogen effluvium is not permanent. It is a temporary disruption of the hair growth cycle. However, if the weight loss unmasks underlying androgenetic alopecia (pattern hair loss), that component is progressive and requires separate treatment. A dermatologist can distinguish between these conditions through examination and trichoscopy.
External resources
GLP-1 agonists and hair loss: a call for further investigation (PubMed)
Hair loss associated with GLP-1 receptor agonist use: a systematic review (PMC)
Telogen effluvium: symptoms, causes, treatment (Cleveland Clinic)
For researchers serious about optimizing their peptide protocols while protecting their health, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your follicles stay in anagen, your ferritin stay above fifty, and your results stay worth every strand.