Feb 28, 2026

Some people lose 20% of their body weight in under a year. Others plateau after a few pounds and wonder what went wrong. Same class of medication. Same weekly injection schedule. Wildly different outcomes.
The difference almost never comes down to the drug itself.
GLP-1 fat loss treatment has transformed the landscape of body composition research over the past several years, producing results that were once considered impossible without surgical intervention. Clinical trials show semaglutide and tirzepatide delivering average body weight reductions between 15% and 25%, with some participants in the SURMOUNT-1 trial experiencing a 40% drop in visceral fat alone. These are not modest numbers. These are the kind of results that change how researchers think about peptide-assisted weight management entirely.
But here is what the headlines leave out. The protocol matters more than the peptide. How you eat, how you train, how you manage side effects, and how you titrate your dose all determine whether you land in the 20% body weight reduction camp or the 5% disappointment group. And the gap between those two outcomes is not luck. It is knowledge.
This guide covers everything you need to understand about using GLP-1 receptor agonists for fat loss. You will learn the mechanisms behind how these peptides strip body fat, which compounds produce the best results for different goals, what clinical trials actually demonstrate, and how to build a protocol that maximizes fat reduction while preserving the lean muscle mass you have worked to build. Whether you are considering semaglutide, tirzepatide, or the newer triple-agonist compounds, the principles that drive real fat loss remain the same. SeekPeptides has compiled the research, the protocols, and the practical guidance to help you navigate every step.
How GLP-1 actually strips body fat
Understanding the mechanism matters. Not because it makes you sound smart at dinner parties, but because knowing how GLP-1 drives fat loss helps you optimize every variable in your protocol. Skip this section at your own risk.
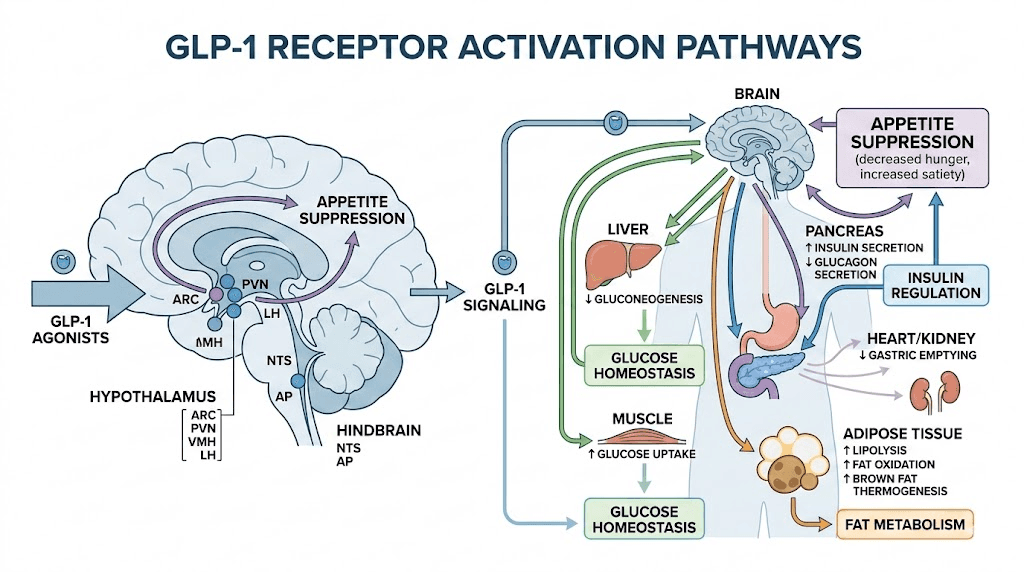
GLP-1 stands for glucagon-like peptide-1. It is a hormone your gut naturally produces after you eat. In a healthy body, GLP-1 signals to the brain that food has arrived, triggers insulin release, slows digestion, and dials down hunger. The problem is that natural GLP-1 breaks down in minutes. Synthetic GLP-1 receptor agonists are engineered to resist that breakdown, staying active for days instead of minutes. That extended activity is what makes them so effective for fat loss.
Central nervous system effects
The most powerful mechanism happens in the brain. GLP-1 receptor agonists cross the blood-brain barrier and bind to receptors in the hypothalamus, the region that controls hunger and satiety. When these receptors activate, something remarkable happens.
Food noise goes quiet.
That constant background hum of thinking about what to eat next, the cravings that hit at 10pm, the inability to walk past a bakery without feeling pulled inside, all of that diminishes significantly. Research from UAB shows that GLP-1 medications blunt the dopamine response to calorie-dense and highly palatable foods. You still enjoy eating. But the obsessive pull toward food weakens dramatically. This is not willpower. This is neurochemistry working in your favor.
The appetite suppression alone accounts for a massive portion of the fat loss these compounds produce. People simply eat less because they genuinely want less food. The appetite suppression typically begins within the first few doses and intensifies as the dose titrates upward.
Peripheral metabolic effects
Below the neck, GLP-1 receptor agonists run a full metabolic optimization program. They enhance insulin secretion in response to meals, which improves how efficiently your body processes glucose. They reduce glucagon release, preventing your liver from dumping excess sugar into the bloodstream. They slow gastric emptying, meaning food moves through the stomach more gradually, keeping you satisfied longer after each meal.
But the fat-specific effects go further. GLP-1 agonists reduce triglycerides and LDL cholesterol. They decrease adipose tissue inflammation, which is critical because inflamed fat tissue resists being mobilized for energy. They minimize ectopic fat deposition, the dangerous fat that accumulates around organs rather than under the skin. Research published in the Journal of Clinical Endocrinology demonstrates that these compounds preferentially target visceral fat, the metabolically active fat wrapped around your organs that drives the highest health risks.
The dual action of eating less and metabolizing fat more efficiently creates a compounding effect. Your caloric intake drops because appetite decreases. Your body simultaneously becomes better at accessing stored fat for energy. The result is fat loss that accelerates over weeks and months rather than stalling out as it typically does with caloric restriction alone.
Why GLP-1 fat loss differs from traditional dieting
Traditional caloric restriction triggers a cascade of hormonal adaptations that fight against continued fat loss. Ghrelin surges. Leptin drops. Metabolic rate slows. Your body treats the calorie deficit as a threat and mounts a full biological defense to get you back to your previous weight. This is why diet-only approaches fail the vast majority of the time long-term.
GLP-1 receptor agonists partially bypass this defense system. By working at the hormonal level rather than the willpower level, they reduce hunger signals at the source rather than asking you to white-knuckle through cravings. The metabolic slowdown that typically accompanies weight loss is partially mitigated because the body experiences less of the stress response associated with severe calorie restriction.
This does not mean the process is effortless. Side effects exist. Plateaus happen. And the compound alone, without proper nutrition and exercise, produces significantly less impressive results. But the fundamental advantage of GLP-1 fat loss treatment is that it works with your biology rather than against it.
Types of GLP-1 treatments for fat loss
Not all GLP-1 treatments are created equal. The landscape has evolved rapidly from single-receptor agonists to dual and even triple-receptor compounds, each offering different fat loss profiles. Understanding which compound does what helps you make an informed decision about which pathway suits your goals. Here is a breakdown of the major GLP-1 peptide options available for fat loss research.
Semaglutide: the established standard
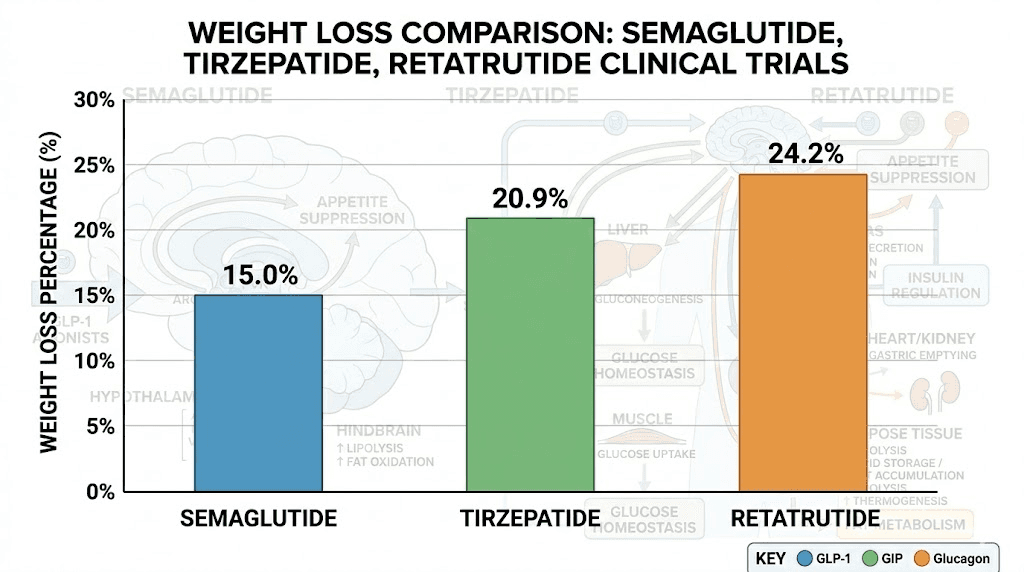
Semaglutide is the compound most people think of when they hear GLP-1. It is a single GLP-1 receptor agonist, meaning it targets one hormonal pathway. Despite targeting only one receptor, its fat loss results are substantial. In the STEP 2 trial, participants receiving 2.4mg semaglutide weekly achieved a mean 9.6% body weight loss from baseline at week 68. The STEP 1 trial showed even more impressive results in participants without diabetes, with average weight loss approaching 15%.
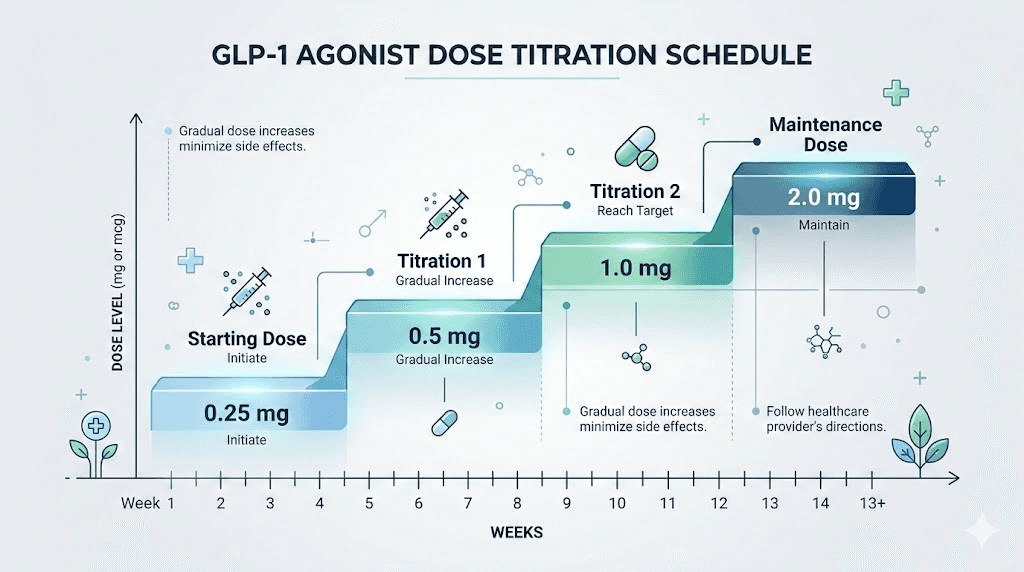
The standard titration protocol for semaglutide starts at 0.25mg weekly, increasing every four weeks through 0.5mg, 1.0mg, and 1.7mg before reaching the maintenance dose of 2.4mg. This gradual escalation minimizes gastrointestinal side effects and allows the body to adapt. You can track your dosing precisely using the semaglutide dosage calculator or review detailed unit-based dosing guides.
Semaglutide is available in both injectable and oral formulations. The FDA approved oral Wegovy in December of the most recent approval cycle, with participants recording a mean body weight reduction of 13.6% after 71 weeks on the 25mg daily tablet. This oral option opens doors for people who prefer not to inject, though the injectable form generally produces slightly superior results due to higher bioavailability.
For those considering compounded semaglutide, additional options exist that combine semaglutide with compounds like B12, glycine, or methylcobalamin to support energy levels and mitigate potential nutrient depletion during extended use.
Tirzepatide: the dual-agonist powerhouse
Tirzepatide changed the game. As a dual GLP-1 and GIP receptor agonist, it targets two hormonal pathways simultaneously. GIP, or glucose-dependent insulinotropic polypeptide, enhances insulin sensitivity and appears to amplify the fat loss effects beyond what GLP-1 alone can achieve. The clinical data speaks for itself.
In the SURMOUNT-1 trial, 50% of participants in the 10mg group and 57% in the 15mg group achieved a body weight reduction of 20% or more. Only 3% of the placebo group hit that mark. The average total fat mass reduction was 34%, with visceral fat dropping by 40% and waist circumference decreasing by an average of 18 centimeters. These numbers place tirzepatide significantly ahead of semaglutide for raw fat loss.
The tirzepatide dosing protocol starts at 2.5mg weekly, escalating through 5mg, 7.5mg, 10mg, 12.5mg, and potentially up to 15mg at the maintenance level. Each dose increase happens at minimum four-week intervals. You can use the tirzepatide dosage calculator to map out your titration schedule precisely.
Tirzepatide also comes in oral formulations and sublingual drops, though the injectable form remains the most studied and widely used. Compounded versions are available with additions like B12, glycine, and niacinamide.
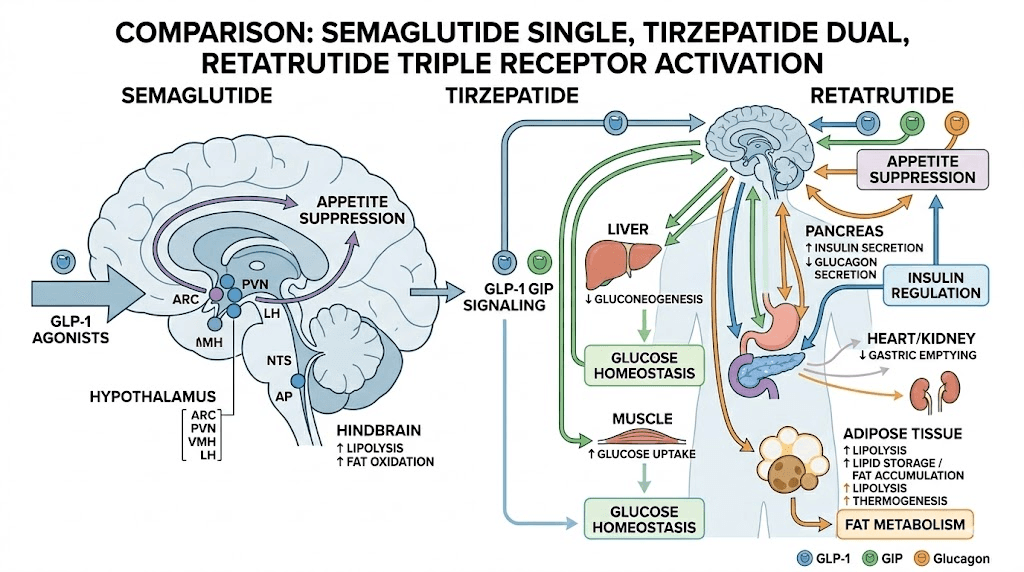
Retatrutide: the triple-agonist frontier
Retatrutide represents the cutting edge. As a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously, it adds a third mechanism that the other compounds lack. Glucagon receptor activation increases energy expenditure directly, promotes thermogenesis, and accelerates the breakdown of stored fat. In research models, body weight reduction reached 24.1% for retatrutide, placing it between semaglutide and tirzepatide in some studies while showing unique advantages in visceral fat reduction and metabolic improvement.
The retatrutide dosing schedule varies by protocol, typically starting at lower doses and titrating upward over several weeks. Current research protocols have explored doses ranging from 1mg to 12mg weekly. Use the retatrutide dosage calculator to plan precise titration. Check the dosage chart for weight-based reference ranges.
It is important to note that retatrutide is not yet FDA-approved and remains available primarily through research channels. The availability landscape is evolving, and the cost considerations differ from established compounds. For those interested in sourcing, review the purchasing guide.
Emerging compounds
The GLP-1 fat loss treatment landscape continues to expand. Survodutide, a dual GLP-1/glucagon receptor agonist, takes a different approach than tirzepatide by pairing GLP-1 with glucagon rather than GIP. Orforglipron, an oral small-molecule GLP-1 agonist from Eli Lilly, delivered weight loss of up to 12.4% in clinical trials, offering a non-peptide oral alternative. Cagrilintide, an amylin analog, is being studied both as a standalone treatment and in combination with semaglutide through CagriSema, which pairs two different appetite-regulating hormones for enhanced effect.
Mazdutide and other dual agonists are also progressing through clinical development, each targeting slightly different receptor combinations. The variety of approaches means that researchers who do not respond optimally to one compound may find better results with another.
Clinical trial results: how much fat can you actually lose
Numbers matter more than marketing. Here is what the clinical evidence actually shows for each major GLP-1 fat loss treatment, broken down by compound, dose, and timeframe. These figures come from controlled trials, not social media testimonials.
Head-to-head weight loss data
Compound | Type | Average weight loss | Top-tier results | Timeline |
|---|---|---|---|---|
Semaglutide 2.4mg | GLP-1 | 15-17% | 20%+ in ~35% of participants | 68-72 weeks |
Tirzepatide 15mg | GLP-1/GIP | 20-22% | 25%+ in ~36% of participants | 72 weeks |
Retatrutide 12mg | GLP-1/GIP/Glucagon | 24% | Not yet fully characterized | 48 weeks |
Oral semaglutide 25mg | GLP-1 (oral) | 13.6% | Not yet fully characterized | 71 weeks |
Orforglipron 36mg | GLP-1 (oral) | 11.2% | Not yet fully characterized | 72 weeks |
Several patterns emerge from this data. Dual and triple agonists consistently outperform single-receptor compounds. Injectable formulations outperform oral versions. And the dose-response relationship is clear: higher maintenance doses produce greater fat loss, though side effects also increase.
Among people without diabetes, the fat loss percentages run even higher. The mean weight loss difference between GLP-1 receptor agonists and placebo sits at 4-6.2% in people with diabetes versus 6.1-17.4% in those without. This gap matters because most people using these compounds for fat loss purposes fall into the non-diabetic category.
What the averages hide
Averages are useful but misleading. Individual response varies by 30-50% based on age, starting BMI, metabolic history, adherence, lifestyle factors, and genetics. Younger participants with higher starting BMI typically lose more weight faster. People with metabolic syndrome or insulin resistance often see dramatic improvements that compound with the fat loss.
Some people are super-responders. They lose 25-30% of body weight on semaglutide alone. Others are non-responders who lose less than 5% regardless of dose. If you find yourself in the non-responder camp after adequate time and dose titration, switching compounds often helps. Moving from one GLP-1 to another can unlock results that the first compound could not produce.
Real-world data paints a more conservative picture than clinical trials. A retrospective cohort study of over 2,400 patients with type 2 diabetes found that GLP-1 agonist initiation without structured behavioral intervention produced approximately 2% weight loss at 72 weeks. This highlights a critical point: the compound is only part of the equation. Diet, exercise, and behavioral modification dramatically amplify the results.
Visceral fat: the hidden victory
Total body weight is one metric. Visceral fat reduction might be the more important one. Visceral fat, the fat surrounding internal organs, drives insulin resistance, systemic inflammation, cardiovascular disease, and metabolic syndrome. You can look relatively lean and still carry dangerous amounts of visceral fat.
The SURMOUNT-1 data on tirzepatide showed a 40% reduction in visceral fat mass over 72 weeks. Retatrutide, with its glucagon receptor activation, directly promotes visceral fat mobilization through enhanced thermogenesis and fat oxidation pathways. Even semaglutide demonstrates significant visceral fat reduction, with imaging studies showing preferential loss from abdominal fat depots.
For people whose primary concern is metabolic health rather than scale weight, the visceral fat data may be more relevant than total body weight reduction. A person who loses 12% of body weight but sheds 35% of visceral fat has achieved a dramatically better health outcome than those numbers alone suggest.
Fat loss versus muscle loss: the body composition question
Here is the concern that keeps researchers up at night. When you lose weight, you do not only lose fat. Lean body mass, including muscle, accounts for a portion of that loss. With GLP-1 treatments, approximately 20-30% of total weight loss may come from lean mass. That percentage is actually similar to what happens with any form of caloric restriction, but when total weight loss is 20% or more, even a proportional lean mass reduction represents significant muscle.
The question is whether this muscle loss is harmful or adaptive.
What the research shows
A paper published in Circulation argues that skeletal muscle changes with GLP-1 receptor agonist treatments appear to be largely adaptive. As body weight decreases, the body needs less muscle mass to support and move a smaller frame. Reductions in muscle volume seem commensurate with what is expected given aging, disease status, and the magnitude of weight loss achieved. Additionally, improvements in insulin sensitivity and reduced muscle fat infiltration likely contribute to improved muscle quality even as total muscle volume decreases.
Think of it this way. A person carrying 300 pounds has more muscle mass than they would at 240 pounds, but much of that extra muscle exists solely to carry the extra weight. Losing it is not the same as a lean athlete losing hard-earned muscle. The muscle that remains often functions better because it is less infiltrated with fat.
That said, the concern is legitimate for people who are already relatively lean or who have specific athletic goals. For these individuals, proactive strategies to preserve lean mass are essential.
Strategies to preserve muscle during GLP-1 fat loss
Research consistently identifies two primary levers for muscle preservation during GLP-1 treatment. The first is protein intake. Studies recommend consuming more than 1.2 grams of protein per kilogram of body weight daily, distributed evenly across meals. Successful cases documented in published literature showed typical protein intakes between 1.6 and 2.3 grams per kilogram of fat-free mass per day. Getting adequate protein can be challenging when appetite is suppressed, which is why protein-dense foods and supplementation become important tools.
The second lever is resistance training. A Medscape review found that resistance training combined with adequate protein intake significantly attenuates lean body mass loss compared to GLP-1 treatment alone. The key word is resistance training specifically, not just exercise in general. Aerobic exercise burns calories but does comparatively little to signal muscle preservation. Lifting weights tells your body that the muscle is needed and should be maintained even during a calorie deficit.
Emerging research on combination therapy offers another approach. A study combining bimagrumab, a myostatin pathway inhibitor, with semaglutide showed that 92.8% of total weight loss came from fat mass, compared to 71.8% with semaglutide alone. While bimagrumab is not widely available, this research points toward a future where GLP-1 treatments are routinely paired with muscle-preserving agents to optimize body composition outcomes.
Patients who engaged in regular exercise from the initiation of GLP-1 treatment and maintained it throughout had the best chances of preserving lean body mass while maximizing fat loss. At six months, one case series documented participants losing approximately 13% of body weight but only about 3% of muscle mass when following a structured exercise protocol.
GLP-1 fat loss treatment protocols
Knowing that GLP-1 treatments cause fat loss is one thing. Knowing how to structure a protocol that maximizes that fat loss is another. This section lays out practical, evidence-based protocols for each major compound.
Semaglutide fat loss protocol
Goal: Maximum fat loss with minimal side effects over 6-12 months
Titration schedule:
Weeks 1-4: 0.25mg weekly (adjustment period)
Weeks 5-8: 0.5mg weekly
Weeks 9-12: 1.0mg weekly
Weeks 13-16: 1.7mg weekly
Week 17+: 2.4mg weekly (maintenance)
Inject once weekly on the same day each week. The best time to inject is typically morning, though the specific time matters less than consistency. Use the recommended injection sites, rotating between abdomen, thigh, and upper arm. If you are reconstituting from powder, follow the reconstitution guide carefully and store according to the shelf life guidelines.
If side effects are intolerable at any dose, stay at the current dose for an additional 2-4 weeks before attempting the next increase. Some researchers find their optimal fat loss dose is lower than the maximum. The plateau troubleshooting guide covers what to do if weight loss stalls.
Tirzepatide fat loss protocol
Goal: Aggressive fat loss with superior visceral fat targeting
Titration schedule:
Weeks 1-4: 2.5mg weekly
Weeks 5-8: 5mg weekly
Weeks 9-12: 7.5mg weekly
Weeks 13-16: 10mg weekly
Weeks 17-20: 12.5mg weekly
Week 21+: 15mg weekly (if tolerated)
Follow the same injection principles as semaglutide. Tirzepatide has specific food considerations and benefits from pairing with a structured diet plan. The meal recommendations focus on lean proteins, complex carbohydrates, and adequate fiber to support the GI tract during treatment.
If you are using reconstituted tirzepatide, precise measurement is critical. Review the unit conversion guides and use a dosage calculator to avoid measurement errors. Store reconstituted product according to refrigeration guidelines.
Retatrutide research protocol
Goal: Maximum fat loss with enhanced thermogenesis and metabolic improvement
Titration schedule (based on clinical trial data):
Weeks 1-4: 1mg weekly
Weeks 5-8: 2mg weekly
Weeks 9-12: 4mg weekly
Weeks 13-16: 8mg weekly
Week 17+: 8-12mg weekly (maintenance, based on tolerance)
Retatrutide protocol management requires attention to the dose schedule and monitoring for glucagon-specific side effects that differ from standard GLP-1 compounds. The injection site selection and injection technique follow similar principles to other subcutaneous peptides. Use the retatrutide dosage calculator for precise measurement from reconstituted vials, and review the reconstitution guide for proper preparation.
Microdosing protocols
Some researchers use microdosing approaches that maintain doses below the standard titration schedule. The theory is that lower doses produce meaningful fat loss with fewer side effects, allowing for longer treatment duration and better adherence. The microdosing guide covers this approach in detail, and the schedule template provides a week-by-week framework.
Microdosing is particularly relevant for people who experience intolerable side effects at standard doses or who want to minimize lean mass loss during a longer, more gradual fat loss phase. The fat loss is slower but often more sustainable, with better body composition outcomes.
Optimizing fat loss on GLP-1: diet, exercise, and supplementation
The compound does the heavy lifting. But everything you do around it determines whether you get 10% results or 25% results. This section is not optional reading. It is the difference between good outcomes and exceptional ones.
Diet optimization
Appetite suppression makes eating less almost automatic. The challenge shifts from willpower to quality. When you eat less food, every bite needs to count. Structured meal plans help ensure you are getting adequate nutrition despite reduced intake.
Protein first. Every meal should prioritize protein. Aim for 1.2-1.6 grams per kilogram of body weight minimum, ideally 1.6-2.3 grams per kilogram of fat-free mass. When appetite is low, protein shakes become a practical tool. Lean meats, fish, eggs, and dairy provide the amino acids your muscles need to resist catabolism during the calorie deficit GLP-1 treatment creates.
Manage fiber and hydration. GLP-1 treatments slow gastric emptying, which can cause constipation and bloating. Adequate fiber from vegetables and whole grains helps maintain digestive regularity. The constipation management guide and tirzepatide-specific approaches address this common issue. Hydration is equally critical, as dehydration worsens nausea and GI symptoms.
Review the recommended food lists, the best foods to eat during treatment, and the foods to avoid. These guides are built from clinical recommendations and real user experience.
Avoid high-fat and spicy foods. High-fat foods take longer to digest. When gastric emptying is already delayed by GLP-1, adding slow-digesting foods creates a backlog in the stomach that triggers nausea and discomfort. Spicy foods irritate the stomach lining. Neither is prohibited forever, but during the initial titration phase when side effects peak, avoidance makes a meaningful difference in tolerability.
Exercise strategy
A published study in Frontiers in Clinical Diabetes and Healthcare found that combining GLP-1 agonists with structured exercise produced additive weight loss effects compared to either strategy alone. But the type of exercise matters enormously.
Resistance training is non-negotiable. Lifting weights 3-4 times per week preserves lean mass, maintains metabolic rate, and improves body composition far beyond what the scale reflects. Compound movements like squats, deadlifts, rows, and presses engage the most muscle mass and send the strongest preservation signals.
Add moderate cardio. Walking 30-60 minutes daily or cycling 3-4 times per week supports cardiovascular health and creates additional calorie expenditure without the cortisol spike of intense cardio. Extreme endurance training during significant caloric deficit can accelerate muscle loss, so moderation is key.
Starting exercise at the same time you begin GLP-1 treatment produces better outcomes than adding it later. The muscle growth support strategies and energy optimization approaches can complement the exercise component of your protocol.
Supplementation support
Extended caloric restriction, even when mediated by GLP-1, can deplete certain nutrients. The most commonly supplemented during GLP-1 treatment include:
Key supplements to consider: B vitamins (especially B12), vitamin D, magnesium, omega-3 fatty acids, and electrolytes. Many compounded formulations already include B12 or glycine and B12 blends to address the most common deficiency risk. The L-carnitine combination is gaining attention for its potential to support fat oxidation alongside GLP-1 treatment.
Managing side effects during GLP-1 fat loss treatment
Side effects are the price of admission. They hit most people, they range from mildly annoying to protocol-disrupting, and managing them properly often determines whether someone sticks with treatment long enough to see transformative results. The good news is that most side effects are transient, mild to moderate in intensity, and manageable with straightforward strategies.
Nausea: the most common hurdle
Nausea affects 15-50% of people taking GLP-1 medications, making it the single most reported side effect. Two distinct mechanisms drive it. The first is delayed gastric emptying, where food sits in the stomach longer than usual, creating that uncomfortable fullness that slides into queasiness. The second is central, with the medication activating GLP-1 receptors in the brain area that controls nausea and vomiting (the area postrema).
Management strategies backed by clinical consensus include eating smaller, more frequent meals rather than large ones. Stop eating the moment you feel full, not five bites later. Avoid high-fat and spicy foods during the initial weeks. Separate fluids from meals by 30-60 minutes. Ginger, whether as tea, chews, or supplements, has clinical support for GLP-1-related nausea relief. Peppermint tea offers additional relief for some.
The critical context: side effects are typically dose-dependent and arise at the start of treatment or when dosage increases. They tend to subside over time as the body adapts. Patience during the first 2-4 weeks of each dose increase usually pays off.
Gastrointestinal issues beyond nausea
Constipation is common. Slowed gastric emptying means slowed everything else in the digestive tract. Adequate fiber, hydration, and gentle physical activity help. For persistent cases, mild laxatives or stool softeners can be appropriate.
Bloating and excessive burping result from the same delayed gastric motility. Eating slowly, chewing thoroughly, and avoiding carbonated beverages reduce the severity. Some people find that digestive enzymes help break down food that sits longer in the stomach.
Diarrhea affects some users, particularly during dose transitions. It typically resolves within the first week of a new dose level. Staying hydrated and maintaining electrolyte balance is essential during episodes.
Fatigue and energy changes
Fatigue during GLP-1 treatment is multifactorial. Reduced caloric intake, adaptation to new hormone levels, and potential nutrient depletion all contribute. The semaglutide fatigue guide details specific strategies for managing energy levels. Some people experience the opposite effect, finding that GLP-1 treatment increases their energy as metabolic function improves and inflammation decreases.
For persistent fatigue, check nutrient levels (B12, iron, vitamin D), ensure adequate caloric intake (extreme restriction backfires), and consider timing exercise to boost energy rather than deplete it.
Other side effects to monitor
Hair thinning can occur during rapid weight loss of any kind, not exclusively with GLP-1 treatment. It typically appears 3-6 months into treatment and often resolves as the body stabilizes. Adequate protein and micronutrient intake reduces the risk.
Headaches, dizziness, insomnia, and muscle pain are less common but documented side effects. Each has specific management approaches covered in their respective guides. The comprehensive safety guide provides an overview of risk management across all peptide treatments.
What to expect: the GLP-1 fat loss timeline
Setting realistic expectations prevents both premature discouragement and unrealistic optimism. Here is what the research and clinical experience tell us about the typical fat loss trajectory on GLP-1 treatment.
Month 1: the adjustment phase
Weight loss in the first month is modest but noticeable. Most people lose 5-10 pounds, primarily from reduced food intake as appetite suppression takes hold. You are on the lowest dose during this period. Side effects are usually at their peak as your body adjusts. The first week experience guide details what to expect day by day.
Do not panic if the scale moves slowly. The first month is about adaptation, not transformation.
Months 2-3: acceleration begins
As the dose titrates upward, appetite suppression intensifies and fat loss accelerates. Many people hit their stride during this period, losing 2-4 pounds per week consistently. The one-month milestone often provides enough encouragement to push through the side effect adjustment period at higher doses.
Body composition changes become visible. Clothes fit differently before the scale reflects the full change, because fat is being redistributed and metabolized even when water weight fluctuations mask the trend.
Months 4-6: the sweet spot
This is where the dramatic results accumulate. You are at or near your maintenance dose. Side effects have largely stabilized. The compounding effect of months of consistent caloric deficit plus metabolic improvement produces visible, measurable change. The tirzepatide weight loss timeline shows typical progression curves during this critical period.
Many people report losing 15-20% of starting weight by month 6 when combining GLP-1 treatment with diet and exercise protocols. Before and after documentation from this timeframe tends to show the most dramatic visual changes.
Months 7-12: optimization and maintenance
Fat loss typically slows during this phase as the body approaches a new equilibrium. This is normal, not a failure. The plateau management guide addresses strategies for pushing through stalls, including dose adjustments, dietary modifications, and exercise changes.
By month 12, clinical trials show average participants reaching the 15-25% total body weight loss range depending on compound and dose. The focus shifts from aggressive fat loss to body composition optimization and long-term maintenance strategy.
Beyond 12 months: the maintenance question
A critical consideration: stopping GLP-1 medication usually leads to regain of 60-70% of lost weight within 12 months. This is not a personal failing. It is biology. The hormonal factors that drove weight gain before treatment reassert themselves when the medication is removed.
Long-term strategies include maintained low-dose GLP-1 treatment, lifestyle modification protocols, or gradual tapering approaches that allow the body to adapt to lower medication levels over time. The treatment duration guide covers the evidence on optimal treatment length.
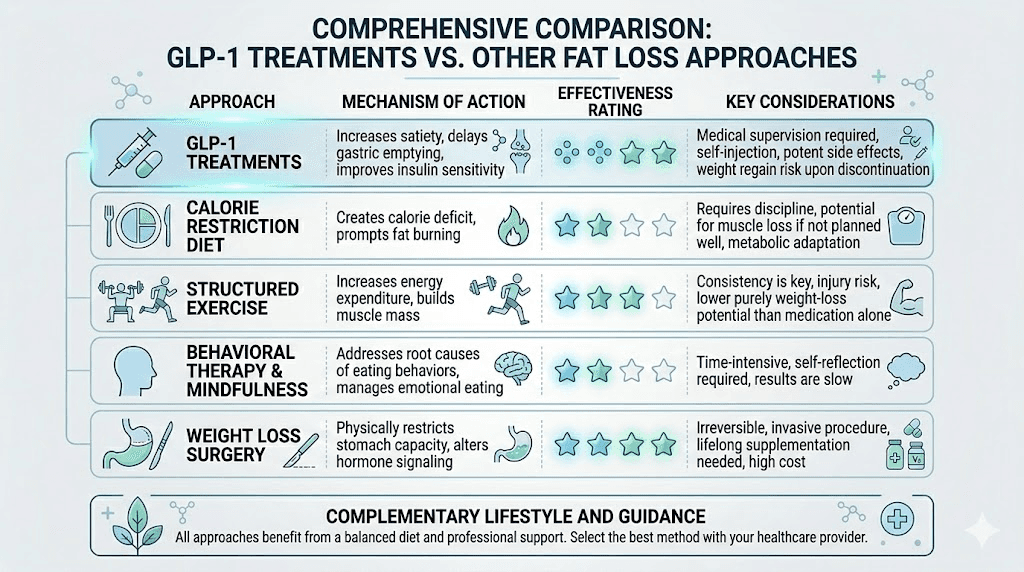
GLP-1 fat loss versus other approaches
GLP-1 treatment does not exist in a vacuum. Understanding how it compares to and combines with other fat loss strategies helps you build the most effective overall approach.
GLP-1 versus phentermine
Phentermine and semaglutide take fundamentally different approaches. Phentermine is a sympathomimetic amine that suppresses appetite through stimulant action. It works fast but is approved only for short-term use (typically 12 weeks) due to side effect and dependence concerns. GLP-1 agonists work through hormonal pathways with approval for long-term use. The fat loss with phentermine averages 5-10% of body weight, significantly less than modern GLP-1 compounds.
Some researchers explore combining phentermine with semaglutide or with tirzepatide for enhanced short-term results, though the evidence base for combination use is still developing. The comprehensive comparison covers all the relevant differences.
GLP-1 versus other fat loss peptides
The peptide landscape for fat loss extends beyond GLP-1. AOD 9604 targets fat metabolism without affecting blood sugar or appetite. FTPP (adipotide) works through a completely different mechanism, targeting blood supply to fat tissue. Lipotropic peptides support fat mobilization and metabolism through various pathways.
None of these alternatives match GLP-1 compounds for raw fat loss magnitude. However, some researchers use them in combination or as maintenance strategies after primary GLP-1 treatment. The best fat burning peptide comparison and weight loss stack guide detail these combination approaches.
For women specifically, the female-specific weight loss peptide guide addresses hormonal considerations that influence compound selection. For those dealing with menopause-related weight gain, GLP-1 compounds offer particularly strong evidence of effectiveness.
GLP-1 plus other peptides
Combination strategies are an area of active research. AOD 9604 alongside tirzepatide is one combination some researchers explore. Cagrilintide with semaglutide (CagriSema) is being developed as a formal combination product. Tesamorelin with retatrutide is explored for synergistic fat loss and growth hormone benefits.
Before combining any compounds, understand the stacking considerations and review the comprehensive stacking guide. The peptide stack calculator helps plan multi-compound protocols. Always prioritize safety when combining multiple active compounds.
Practical considerations for starting GLP-1 fat loss treatment
Before you administer your first dose, several practical factors deserve attention. Getting these right from the beginning saves time, money, and frustration down the line.
Choosing the right compound
Your starting point should consider current health status, fat loss goals, budget, and risk tolerance. For straightforward fat loss with the most established safety data, semaglutide is the most researched option. For more aggressive fat loss with potentially superior body composition outcomes, tirzepatide is the current front-runner. For maximum fat loss potential through triple-receptor activation, retatrutide offers the most advanced mechanism, with the caveat of less long-term safety data.
The three-way comparison guide breaks down every relevant factor, from side effect profiles to dosage equivalencies. For cost considerations, affordable tirzepatide options and retatrutide pricing guides provide current market information.
Injection basics
If you are new to subcutaneous injections, the process is simpler than it sounds. The GLP-1 injection guide covers technique from start to finish. Key points include selecting the best injection site, which is typically the abdomen for optimal absorption. Rotate injection sites to prevent lipodystrophy. Use an injection pen if available, or follow the syringe technique guide for vial-based products.
Injection timing should be consistent. Choose a day of the week and stick with it. The optimal injection timing guide covers morning versus evening administration and how to handle missed doses.
Storage and handling
Proper storage preserves potency. Reconstituted GLP-1 peptides require refrigeration, and each compound has specific shelf life characteristics. Check the tirzepatide storage guide, semaglutide refrigeration guidelines, or retatrutide shelf life depending on your compound.
Temperature excursions happen. If your medication gets warm or leaves the cold chain temporarily, the specific compound and duration determine whether it remains usable. The general peptide storage guide covers best practices across all compounds. For travel, review the travel guide for maintaining cold chain on the go.
Reconstitution and measurement
If working with lyophilized (powder) peptides, reconstitution is a critical skill. The general reconstitution guide teaches the technique, and compound-specific guides for semaglutide and tirzepatide cover exact volumes and procedures. Use the peptide reconstitution calculator to determine precise bacteriostatic water volumes for your specific vial concentration.
Measurement accuracy matters more with GLP-1 compounds than with many other peptides because dose-response curves are steep. A small measurement error at lower doses can mean the difference between therapeutic effect and subtherapeutic dosing. The dosage calculation guide walks through the math, and the peptide calculator handles the conversions automatically.
Monitoring progress
Scale weight alone is an unreliable metric for GLP-1 fat loss treatment. Body composition measurements, waist circumference, progress photos, and how clothing fits provide a more complete picture. The GLP-1 plotter is a useful tool for tracking trends over time.
Key metrics to track weekly:
Body weight (same time, same conditions)
Waist circumference
How clothing fits (more reliable than the scale short-term)
Energy levels and side effect severity
Protein intake (aim for daily targets)
Exercise sessions completed
If weight loss stalls for more than 3-4 weeks at an adequate dose, the semaglutide troubleshooting guide or tirzepatide troubleshooting guide can help identify what is blocking progress. Common culprits include insufficient dose, liquid calories, inadequate protein, insufficient sleep, and excessive stress.
Special populations and considerations
GLP-1 fat loss treatment does not affect everyone identically. Specific populations face unique considerations that warrant additional attention.
Women-specific considerations
GLP-1 compounds can affect menstrual cycles and hormone balance through weight loss-mediated hormonal changes. Rapid fat loss alters estrogen levels because adipose tissue is an endocrine organ that produces estrogen. For women over 40 and those navigating menopause, these hormonal shifts require monitoring.
Fertility is a particular consideration. GLP-1 treatments can increase fertility by improving ovulatory function in women with polycystic ovary syndrome or obesity-related anovulation. If pregnancy is not desired, additional contraceptive measures are important. If pregnancy occurs during treatment, the pregnancy and tirzepatide guide covers immediate steps. For breastfeeding mothers, review the breastfeeding safety information.
Men-specific considerations
Fat loss in men on GLP-1 treatment tends to produce significant improvements in testosterone levels. Visceral fat produces aromatase, the enzyme that converts testosterone to estrogen. As visceral fat decreases, testosterone typically increases naturally. The male-specific results and male peptide guide detail these outcomes.
For men using testosterone replacement therapy alongside peptides, the interaction effects are generally favorable. However, monitoring hormone panels during significant weight loss is advisable to prevent over-supplementation as natural production may increase.
Switching between compounds
Not every compound works equally well for every person. Switching between GLP-1 treatments is common and often productive. The tirzepatide to semaglutide transition, semaglutide to tirzepatide conversion, and tirzepatide to retatrutide transition guides cover dose equivalencies and timing for each switch.
Common reasons to switch include inadequate fat loss on the current compound, intolerable side effects that do not resolve with time, plateau that persists despite optimization, and desire for a different mechanism of action. The conversion is not always straightforward because receptor affinities differ between compounds, so the dosage equivalency charts are essential references.
The role of GLP-1 in comprehensive fat loss
GLP-1 fat loss treatment is best understood as one component of a comprehensive approach. The compound creates the caloric deficit and metabolic environment for fat loss. Everything else you do determines the quality and sustainability of that loss.
SeekPeptides members consistently report that the biggest factor in their results is not which compound they chose, but how well they structured everything around it. Adequate protein, consistent resistance training, proper supplementation, patient dose titration, and realistic timeline expectations separate the success stories from the disappointments.
The evidence is clear: GLP-1 receptor agonists are the most effective pharmacological tools currently available for fat loss. Semaglutide delivers 15-17% average body weight reduction. Tirzepatide pushes that to 20-22%. Retatrutide may exceed both. Combined with proper foundational knowledge, these compounds offer transformative potential.
But potential is not the same as guaranteed results. The people who achieve exceptional outcomes are the ones who treat GLP-1 treatment as the foundation of a comprehensive protocol, not the entirety of one.
Frequently asked questions
How quickly does GLP-1 fat loss treatment start working?
Most people notice reduced appetite within the first week of treatment. Measurable weight loss typically appears within 2-4 weeks, with 5-10 pounds lost in the first month being common. The detailed timeline guide covers what to expect at each stage. Significant visible fat loss usually becomes apparent by months 2-3 as doses reach therapeutic levels.
Which GLP-1 compound is best for fat loss specifically?
Based on current clinical data, tirzepatide produces the most fat loss among FDA-approved compounds, with 40% visceral fat reduction in the SURMOUNT-1 trial. Retatrutide shows promise for even greater results through triple-receptor activation but lacks the long-term safety data of tirzepatide. The comparison guide breaks down all the differences.
Can you maintain fat loss after stopping GLP-1 treatment?
Without continued intervention, most people regain 60-70% of lost weight within 12 months of discontinuation. Strategies to mitigate regain include gradual tapering rather than abrupt cessation, continued dietary and exercise habits, and potential long-term low-dose maintenance. The weight maintenance guide covers evidence-based approaches.
How much muscle do you lose on GLP-1 treatment?
Approximately 20-30% of total weight loss may come from lean mass, similar to any form of caloric restriction. With adequate protein intake (over 1.2g per kg body weight) and consistent resistance training, lean mass loss can be significantly reduced. One case series showed participants losing 13% body weight but only 3% muscle mass when following a structured exercise program.
Is GLP-1 fat loss treatment safe long-term?
Semaglutide and tirzepatide have multi-year safety data from clinical trials and widespread clinical use. The most common side effects are gastrointestinal and typically transient. Rare but serious risks include pancreatitis and potential thyroid concerns (based on animal studies). Regular monitoring and proper medical oversight are recommended for long-term use. The safety and risks guide covers comprehensive risk profiles.
Can you combine GLP-1 with other fat loss peptides?
Combination approaches are being researched. CagriSema (cagrilintide plus semaglutide) is a formal combination product in development. AOD 9604 with tirzepatide is explored by some researchers. Always review the stacking safety guide before combining compounds. The stack calculator helps plan multi-compound protocols.
Do you need to exercise on GLP-1 for fat loss?
GLP-1 compounds produce fat loss without exercise, but the quality of that loss is significantly worse. Without resistance training, a higher proportion of weight lost comes from muscle rather than fat. Exercise also improves insulin sensitivity, cardiovascular health, and long-term weight maintenance. The clinical evidence strongly supports combining GLP-1 treatment with structured exercise for optimal body composition outcomes.
What BMI do you need for GLP-1 treatment?
FDA-approved GLP-1 treatments for weight management are typically indicated for adults with BMI of 30 or higher (obesity), or BMI of 27 or higher (overweight) with at least one weight-related comorbidity. The BMI requirements guide and requesting GLP-1 guide cover qualification criteria in detail.
For researchers serious about optimizing their fat loss protocols, SeekPeptides provides comprehensive, evidence-based resources including dosing guides, calculators, and the most detailed GLP-1 protocol library available. Members access personalized guidance, community support from thousands of experienced researchers, and protocols built from documented outcomes rather than speculation.
External resources
NIH: Weight Reduction with GLP-1 Agonists and Paths for Discontinuation
WHO Guideline on GLP-1 Therapies for Obesity in Adults (JAMA)
In case I do not see you, good afternoon, good evening, and good night. May your fat cells keep shrinking, your muscle mass stay preserved, and your protocols stay optimized.