Feb 28, 2026

What if the problem is not semaglutide itself, but how you are timing it?
That single question drives thousands of people to consider splitting their semaglutide dose into two smaller injections per week instead of one larger shot. The logic sounds reasonable enough. A full weekly dose hits your system all at once, triggers a spike in drug concentration, and sometimes brings nausea, bloating, or fatigue along for the ride. Splitting that same total dose across two injection days, say Monday and Thursday, could theoretically smooth out those peaks and valleys. Less spike. Less crash. Fewer side effects.
But here is where things get complicated.
Semaglutide was designed, tested, and approved for once-weekly use. Every clinical trial from the STEP program to the SUSTAIN trials evaluated the drug on a weekly injection schedule. No randomized controlled study has compared split dosing to standard dosing. That does not mean split dosing cannot work. It means the evidence base is theoretical, anecdotal, and rooted in pharmacokinetic modeling rather than clinical outcomes data. And yet, some healthcare providers are recommending it, compounding pharmacies are filling prescriptions for it, and online communities are full of people who swear by it. This guide breaks down everything you need to know, from the science behind semaglutide dosing to specific protocols, real risks, and smarter alternatives that might solve the same problem without venturing into experimental territory. Whether you are currently dealing with semaglutide bloating, persistent nausea, or just wondering if there is a better way to take this medication, you will find your answers here.
Why people want to split their semaglutide dose
The motivation almost always starts with side effects.
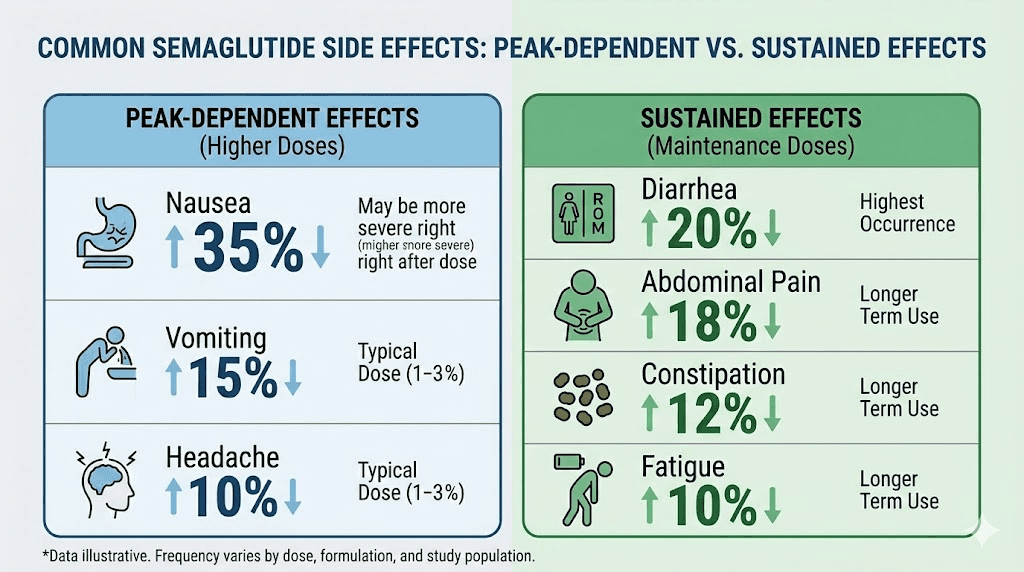
Gastrointestinal problems are the most common reason people abandon semaglutide treatment entirely. Research shows that nausea affects between 15% and 50% of patients during the dose escalation phase, depending on the starting dose and how quickly the titration schedule progresses. For some people, the nausea is mild and passes within a few hours. For others, it persists for days after each injection, making normal eating nearly impossible and turning every week into a cycle of feeling terrible, slowly recovering, and then injecting again.
Constipation is another driver. So is fatigue. The pattern that split dosing advocates describe goes something like this: days one through three after injection are the worst for side effects because drug concentration peaks during this window. Days four through seven feel progressively better as levels drop, but by that point appetite suppression also begins to fade. The result is a rollercoaster where the first half of the week feels awful and the second half feels like the medication is barely working.
Split dosing promises to flatten that curve.
Instead of one big spike followed by a gradual decline, two smaller doses create a more even drug level throughout the week. The peaks are lower, so side effects should theoretically be milder. The troughs are higher, so appetite suppression should remain more consistent. It is an elegant theory. And it is not entirely without pharmacological basis. But the gap between theory and proven clinical practice matters enormously when you are injecting a medication into your body.
Beyond side effects, some people explore split dosing for practical reasons. Those using compounded semaglutide from multi-dose vials sometimes find it easier to draw up two smaller injections than one larger one, particularly at higher doses where injection volume becomes uncomfortable. Others have read about microdosing approaches for related medications like tirzepatide and wonder if the same principle applies to semaglutide.
The question is whether the theoretical benefits actually materialize in practice, and whether the risks of deviating from the studied dosing protocol outweigh those benefits.
How semaglutide works in your body
Understanding why split dosing is even a conversation requires understanding how semaglutide behaves once it enters your system.
Semaglutide is a GLP-1 receptor agonist. It mimics a hormone your body naturally produces called glucagon-like peptide-1. This hormone plays a central role in blood sugar regulation, appetite control, and gastric emptying. When you eat, your gut releases natural GLP-1, which signals your brain to feel satisfied, tells your pancreas to produce insulin, and slows the rate at which food leaves your stomach. The problem is that natural GLP-1 breaks down within minutes. Semaglutide was engineered to last much, much longer.
The half-life of semaglutide is approximately seven days, or about 168 hours. That is the longest half-life of any injectable GLP-1 receptor agonist on the market. For comparison, liraglutide has a half-life of about 13 hours, which is why it requires daily injections. Semaglutide achieves its extended duration through a structural modification that allows it to bind tightly to albumin in your blood. This albumin binding acts like a slow-release mechanism, preventing the drug from being cleared by your kidneys too quickly.
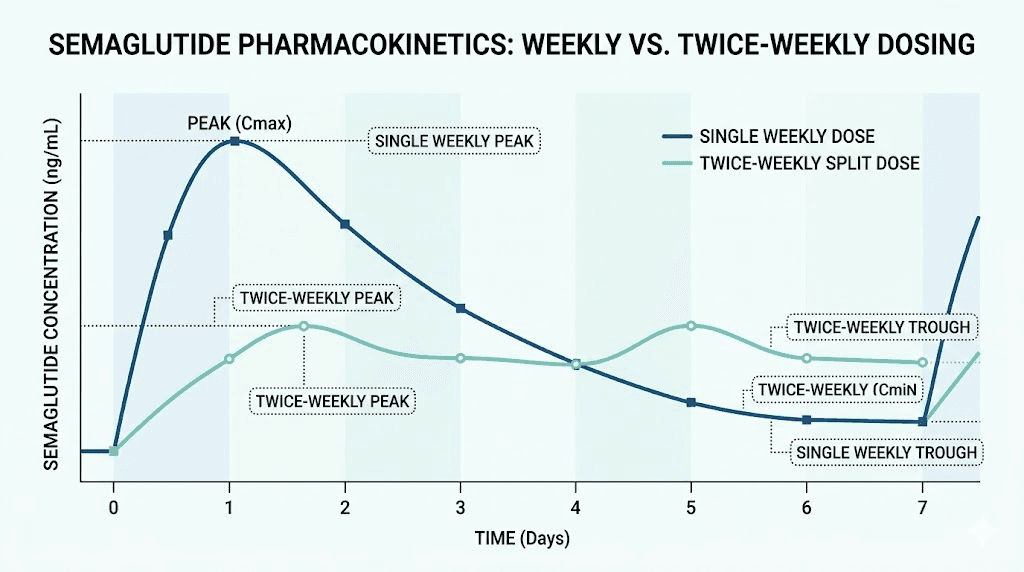
After a subcutaneous injection, semaglutide reaches its peak blood concentration between one and three days. This is the Tmax, the time to maximum concentration. From that peak, levels gradually decline over the remaining four to six days until your next injection. With consistent weekly dosing, the drug reaches what pharmacologists call steady state after approximately four to five weeks. At steady state, the amount entering your system each week roughly equals the amount being eliminated, creating a predictable baseline level with weekly fluctuations around it.
Here is the detail that matters for split dosing. At steady state with weekly injections, the peak-to-trough ratio is approximately 2.7. That means the highest drug concentration during the week is about 2.7 times the lowest concentration. For most people, this fluctuation is well tolerated. The slow release from albumin binding keeps levels relatively stable compared to shorter-acting GLP-1 drugs. But for a subset of patients, those who are particularly sensitive to GLP-1 effects on the gastrointestinal tract, even this modest fluctuation is enough to cause problems during the peak phase.
Bioavailability of subcutaneous semaglutide is approximately 89%, and protein binding exceeds 99%. These numbers tell us that virtually all of the semaglutide you inject reaches your bloodstream and stays bound to albumin for extended periods. The drug distributes slowly, acts slowly, and clears slowly. This pharmacokinetic profile is exactly why semaglutide works so well as a once-weekly medication. It is also why splitting the dose, in theory, creates only modest changes in the overall drug exposure curve rather than dramatic ones.
Understanding your semaglutide concentration and how it relates to your unit measurements becomes important when considering any dosing modification. Whether you are measuring in units for a 0.25 mg dose or calculating milligrams from units, precision matters even more when dividing doses.
The science behind split dosing
Split dosing is not a random idea someone came up with on a forum. It has a pharmacological rationale.
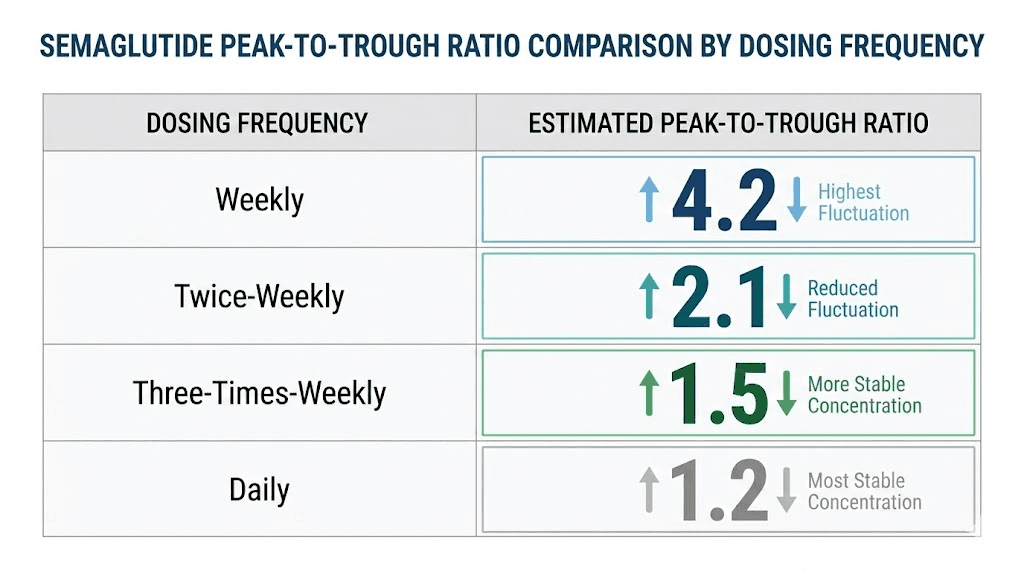
The core principle is straightforward. By dividing a weekly dose into two smaller administrations separated by approximately 72 to 84 hours, you reduce the peak concentration after each injection while maintaining a higher trough concentration before the next one. Mathematical pharmacokinetic models suggest that a twice-weekly split reduces the peak-to-trough ratio from approximately 2.7 to approximately 1.8, representing roughly a 20% reduction in peak drug concentration.
That 20% matters more than it sounds.
Many GLP-1 side effects are concentration-dependent. Nausea, in particular, correlates more strongly with peak concentration than with average drug exposure. Studies on related medications have shown that the sharp rise in drug levels immediately after injection triggers the strongest GI response. If you can lower that peak without significantly changing the total weekly drug exposure, you might reduce the intensity of side effects while preserving the therapeutic benefit.
A study published in the journal Obesity examined alternative dosing regimens for GLP-1 receptor agonists and found that altering dosing frequency does not proportionally reduce efficacy. Specifically, switching from weekly to every-two-weeks dosing maintained approximately 72% of weight loss for semaglutide. The researchers calculated that the relationship between dosing frequency and weight loss is not linear, meaning you lose proportionally less efficacy than you lose in dosing frequency. For split dosing, which maintains the same total weekly dose, mathematical models suggest efficacy maintenance of 80% to 95%.
There are also more aggressive split approaches. A three-times-weekly schedule (Monday, Wednesday, Friday) reduces the peak-to-trough ratio to approximately 1.5, a 28% peak reduction. Daily microdosing pushes it down to approximately 1.2, a 35% reduction. Each step toward more frequent dosing creates a flatter drug concentration curve. But each step also introduces more injection days, more opportunities for measurement error, and more deviation from studied protocols.
If you have explored the concept of microdosing for GLP-1 medications, the principles are similar for semaglutide. The split dosing approach for tirzepatide follows comparable pharmacokinetic logic, though the drugs have different half-lives and receptor profiles. SeekPeptides has covered these approaches extensively because understanding the underlying pharmacology helps researchers make informed decisions rather than guessing.
One critical caveat. All of these models assume perfect dose accuracy. When you split a dose, you need to measure exactly half of your weekly amount for each injection. With pen devices like Ozempic or Wegovy, this is physically difficult or impossible since the pens are designed to deliver fixed doses. Split dosing is primarily feasible with compounded semaglutide vials where you draw up specific volumes using an insulin syringe.
Split dosing protocols explained
If you and your healthcare provider decide to explore split dosing, here is what the various protocols look like in practice.
The standard twice-weekly split
This is the most common approach. You take your total weekly dose and divide it into two equal injections, typically on Monday and Thursday. The Monday-Thursday schedule creates a roughly 72-hour gap between injections, which maintains adequate drug levels while providing enough spacing to avoid excessive accumulation.
For someone on a 1 mg weekly dose, the split would be 0.5 mg on Monday and 0.5 mg on Thursday. For a 2.4 mg weekly dose, you would inject 1.2 mg each day. The total weekly exposure remains identical to standard dosing. Only the distribution pattern changes.
The critical rule is that injections must be separated by at least 48 hours. Injecting too close together defeats the purpose by creating a combined peak that may actually exceed what a single weekly dose would produce. The Monday-Thursday schedule, or a similar Tuesday-Friday pattern, naturally maintains appropriate spacing.
To execute this protocol with compounded semaglutide, you need to know your exact dosage in units. If you are working with a 10 mg vial reconstituted to a known concentration, calculating half-doses requires careful math. Our semaglutide dosage calculator can help determine the exact volume for each injection based on your vial concentration.
The titration split protocol
Some providers recommend starting the split approach from the very beginning of treatment, using it as an alternative titration method. Instead of the standard escalation from 0.25 mg weekly, this protocol starts at 0.125 mg twice weekly and increases gradually.
A typical titration schedule might look like this:
Weeks 1-4: 0.125 mg twice weekly (0.25 mg total)
Weeks 5-8: 0.25 mg twice weekly (0.5 mg total)
Weeks 9-12: 0.5 mg twice weekly (1.0 mg total)
Weeks 13-16: 0.85 mg twice weekly (1.7 mg total)
Weeks 17+: 1.2 mg twice weekly (2.4 mg total)
This approach extends the time at each dose level compared to standard titration. The idea is that slower escalation combined with lower individual peaks creates the gentlest possible introduction to semaglutide. For patients who have struggled with standard titration schedules or abandoned previous attempts due to intolerable side effects, this protocol offers an alternative path forward.
The rescue split protocol
This approach is for people who are already on a stable weekly dose but experiencing unmanageable side effects at that dose. Rather than reducing the total weekly amount, which would diminish therapeutic benefit, the provider splits the existing dose into two injections.
Someone taking 1.7 mg weekly who cannot tolerate the post-injection nausea might switch to 0.85 mg on Monday and 0.85 mg on Thursday. The total weekly exposure stays at 1.7 mg. The goal is purely to reduce peak concentration without sacrificing overall drug levels.
This is perhaps the most defensible application of split dosing from a clinical perspective. The patient has already demonstrated that they respond to the medication at this total dose, and the modification addresses tolerability without changing efficacy expectations.
What about the injection technique?
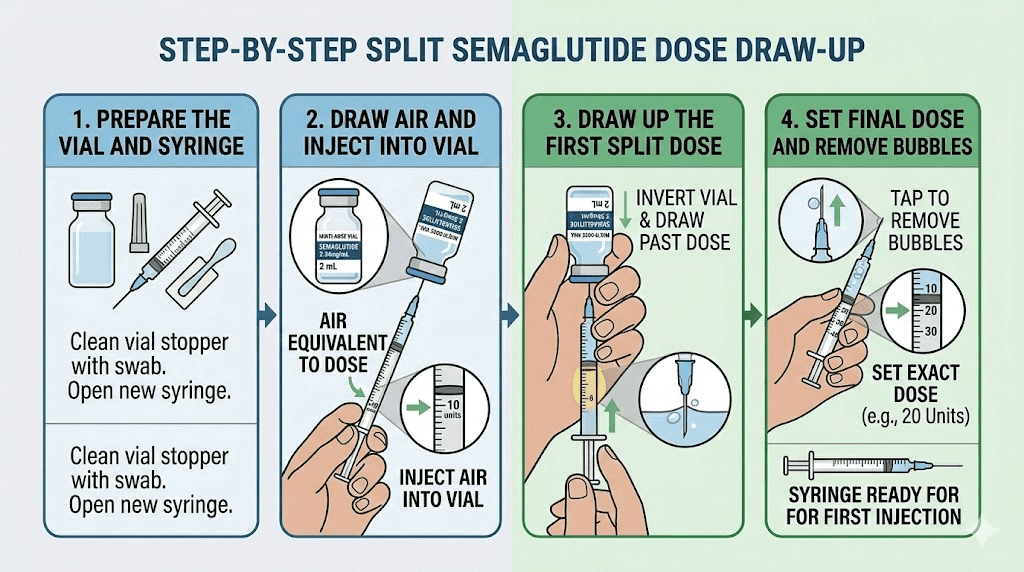
Split dosing does not change where or how you inject. You still use subcutaneous injection sites in the abdomen, thigh, or upper arm. You still rotate sites between injections to prevent lipodystrophy. And you still need to ensure proper reconstitution and storage of your medication, especially since a vial being accessed twice as often increases the risk of contamination if sterile technique is not maintained.
Each injection should follow proper procedure. Clean the vial stopper with an alcohol swab. Use a new, sterile syringe and needle for every injection. Draw up the exact volume needed. Inject at a 90-degree angle into a skin fold. Hold for 5-10 seconds before withdrawing. These steps do not change whether you are injecting once or twice per week.
Does split dosing actually reduce side effects
This is the question everyone wants answered. And the honest answer is: we think so, but we do not know for certain.
No clinical trial has directly compared once-weekly semaglutide to twice-weekly split dosing for side effect outcomes. The evidence supporting reduced side effects comes from three sources: pharmacokinetic modeling, anecdotal reports, and inference from studies on GI tolerability during dose escalation.
The pharmacokinetic argument is the strongest. A 20% reduction in peak concentration is meaningful for concentration-dependent side effects. Studies on semaglutide tolerability have consistently shown that GI side effects are most common and most severe during the first few days after each dose increase, when drug levels are climbing toward a new peak. The STEP 1 trial found that nausea was reported by 44% of participants in the semaglutide group, but the vast majority of nausea episodes were transient and occurred during dose escalation. At maintenance doses, the incidence drops significantly as the body adapts to stable drug levels.
If peak concentration drives the worst of the nausea, and split dosing lowers the peak by 20%, then a meaningful reduction in nausea intensity is pharmacologically plausible. Some semaglutide users report exactly this experience. The nausea becomes manageable. The first two days after injection are no longer completely miserable. They can eat normal meals and maintain energy levels throughout the week.
But plausible is not proven.
Individual variation in GLP-1 receptor sensitivity means that some people will be extremely sensitive to even small changes in drug concentration while others barely notice the difference between peak and trough. For the first group, a 20% peak reduction might be transformative. For the second, it might not matter at all. Without clinical data, there is no way to predict which group you fall into before trying.
Bloating and constipation may respond less predictably to split dosing. These side effects are related to delayed gastric emptying, which is a sustained effect of semaglutide rather than a peak-dependent one. Since split dosing maintains the same average drug levels, these effects might not improve much. Sleep disturbances and fatigue are similarly unpredictable since their relationship to drug concentration peaks versus averages is not well established.
For those considering alternatives, comparing semaglutide side effects to tirzepatide may be worthwhile, as the medications have different GI tolerability profiles.
Does split dosing affect weight loss results
Weight loss efficacy is the other side of the equation. There is no point reducing side effects if you also eliminate the therapeutic benefit.
The good news is that split dosing, when done correctly, should maintain very similar weight loss outcomes to standard weekly dosing. The reason comes back to pharmacology. Weight loss with semaglutide is driven by cumulative drug exposure over time, not by individual peak concentrations. As long as the total weekly dose remains the same, the average drug level throughout the week is nearly identical whether you inject once or twice.
Mathematical efficacy modeling supports this conclusion. Researchers have estimated that twice-weekly split dosing maintains 80% to 95% of the weight loss efficacy of standard weekly dosing at the same total dose. The small potential reduction comes from the theoretical possibility that the lower peaks might produce slightly less aggressive appetite suppression during the first few days after injection. But this effect, if it exists, appears to be minimal and might be offset by the higher trough levels providing more consistent appetite control in the back half of each three-to-four day cycle.
The study on alternative GLP-1 dosing regimens found something remarkable about the relationship between dosing frequency and efficacy. Reducing dosing frequency from weekly to every two weeks, which cuts total drug exposure in half, only reduced weight loss from approximately 17% to approximately 12%. That is a disproportionately small efficacy loss for a 50% reduction in drug exposure. For split dosing, where total exposure stays the same, the implication is that efficacy should be essentially preserved.
There is actually a scenario where split dosing might improve outcomes. If someone is so nauseated by their weekly dose that they cannot eat properly for three days, they are not getting adequate nutrition and may be losing muscle rather than fat. If split dosing allows them to eat normally throughout the week while maintaining adequate appetite suppression, the quality of weight loss might actually improve. This is speculation, not data, but the logic tracks for people experiencing severe side effects.
Understanding your weight loss timeline on semaglutide can help set realistic expectations regardless of your dosing schedule. Most people see initial results within the first week, with significant changes becoming apparent by weeks four to eight as steady state is established. The overall timeline to meaningful results should not change substantially with split dosing since total drug exposure remains equivalent.
If you are not seeing expected results regardless of dosing schedule, our guide on why weight loss stalls on semaglutide covers the most common culprits and solutions.
Compounded semaglutide and split dosing
Split dosing is almost exclusively relevant to people using compounded semaglutide from multi-dose vials. Here is why.
Brand-name semaglutide pens like Ozempic and Wegovy deliver pre-set doses that cannot be easily divided. The Ozempic pen comes in fixed dose options (0.25 mg, 0.5 mg, 1 mg, or 2 mg), and while some pen devices technically allow dose adjustment, they were not designed for half-dose administration. Attempting to deliver exactly half of a fixed pen dose is imprecise at best and dangerous at worst.
Compounded semaglutide, on the other hand, comes in vials with a known concentration, typically expressed in mg/mL. You draw up a specific volume using an insulin syringe, giving you precise control over the dose. This makes splitting straightforward, at least mechanically. If your vial is 5 mg/mL and your weekly dose is 1 mg (0.2 mL), your split dose is 0.5 mg (0.1 mL) on Monday and 0.5 mg (0.1 mL) on Thursday.
The precision of your syringe matters enormously here. Standard insulin syringes come in 0.3 mL, 0.5 mL, and 1 mL sizes with markings every 1 or 2 units. For split dosing at lower concentrations, you may need very small volume measurements. Understanding unit-to-milligram conversions and choosing the right syringe size can mean the difference between accurate dosing and a 20% error that defeats the purpose of splitting in the first place.
If you are reconstituting semaglutide from lyophilized powder, the concentration you create determines how easy or difficult split dosing will be. Reconstituting a 5 mg vial with less bacteriostatic water creates a higher concentration, meaning each dose requires a smaller volume and measurement errors become more significant. Reconstituting with more water creates a lower concentration with larger, easier-to-measure volumes but the vial runs out faster. Our peptide reconstitution calculator can help you find the right balance.
Storage considerations also become more important with split dosing. You are accessing the vial twice as often, which means twice as many needle punctures through the rubber stopper. Each puncture creates a potential pathway for contamination. Proper refrigeration and sterile handling become even more critical. The shelf life of compounded semaglutide may be affected by increased vial access frequency, though this has not been formally studied.
Some compounded semaglutide formulations include additional ingredients like vitamin B12, glycine, L-carnitine, or niacinamide. When splitting these compound formulations, you are also splitting the supplemental ingredients. This is generally not problematic since these additions are included in modest amounts, but it is worth noting that each injection delivers half the intended supplement dose as well.
SeekPeptides members can access detailed reconstitution guides, concentration calculators, and storage protocols specifically designed for multi-dose vial management, which becomes particularly valuable when split dosing requires precise measurements twice per week.
How to discuss split dosing with your provider
You should not split your semaglutide dose on your own. Period. This is a medication change that requires medical supervision, and here is how to have that conversation productively.
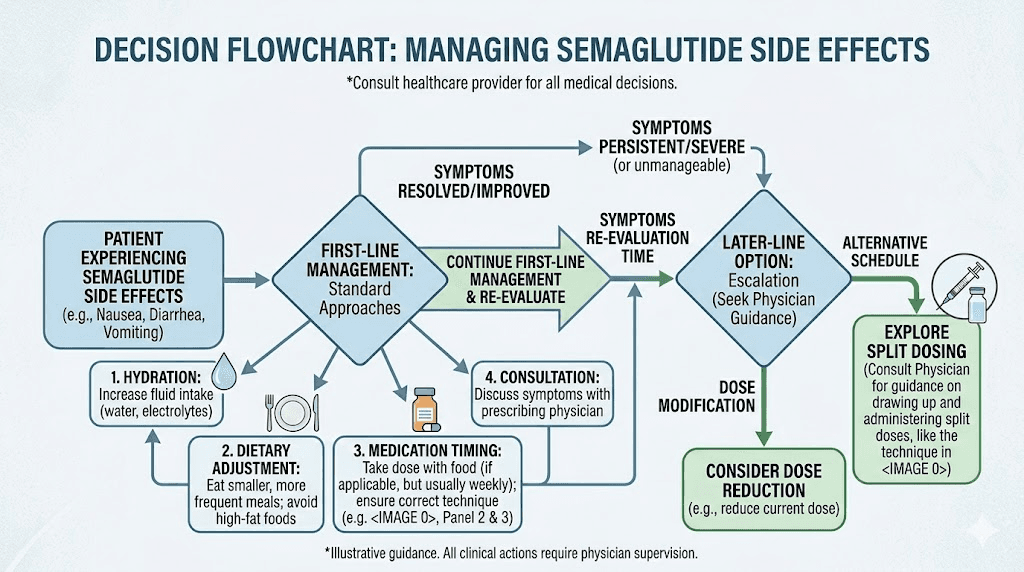
Start with the problem, not the solution. Instead of walking in and asking to split your dose, describe what you are experiencing. Tell your provider which side effects are affecting your quality of life, when they occur relative to your injection day, and how severe they are on a scale they can work with. Quantify things. "I cannot eat solid food for three days after each injection" is more actionable than "I feel nauseated."
Ask about standard approaches first. Your provider may have solutions you have not considered. Extended titration, where you stay at a lower dose for longer before increasing, is the evidence-based approach to managing GI side effects and may solve your problem without any experimental modifications. Switching injection sites, adjusting injection timing relative to meals, or adding anti-nausea medication during the adjustment period are all standard interventions with clinical support.
If standard approaches have been tried and failed, then raise split dosing as a specific question. Frame it as something you have read about and want their medical opinion on. Most providers who are experienced with semaglutide prescribing will have an informed opinion about off-label dosing modifications.
Be prepared for either answer. Some providers are comfortable with split dosing because they have seen it work for other patients. Others strictly adhere to FDA-approved protocols because the liability risk of recommending unstudied dosing regimens is significant. Neither position is wrong. A provider who declines to prescribe split dosing is not being unhelpful. They are following the evidence they have.
If your provider agrees to try split dosing, establish clear expectations upfront. How long will you trial this approach? What metrics determine success or failure? At what point would you return to standard dosing? Having a defined trial period, typically four to eight weeks, prevents the modification from becoming permanent without assessment.
Document everything. Track your injection days, doses, side effects, appetite levels, weight, and any other relevant symptoms. This data helps your provider evaluate whether the split is actually working or if you are experiencing a placebo effect from the novelty of the change. Understanding how to communicate with your provider about GLP-1 medications makes these conversations more productive for everyone.
Alternative strategies for managing semaglutide side effects
Before committing to an experimental dosing modification, exhaust the proven approaches first. There are many evidence-based strategies for managing GLP-1 side effects that do not require deviating from the studied dosing protocol.
Extended dose titration
The single most effective strategy for reducing GI side effects is simply going slower with dose increases. The standard semaglutide titration schedule progresses from 0.25 mg to 0.5 mg to 1 mg to 1.7 mg to 2.4 mg, with four weeks at each level. Many providers now extend this to eight or even twelve weeks per level for patients who are particularly sensitive.
Staying at 0.25 mg for eight weeks instead of four gives your GI system twice as long to adapt before the next increase. Some patients find that they need to stay at lower doses for months before their body tolerates escalation. This is perfectly fine. The destination matters more than the speed of arrival.
Dietary modifications
What you eat significantly affects how well you tolerate semaglutide. Large, high-fat meals are the most common trigger for post-injection nausea because semaglutide slows gastric emptying, and a heavy meal sitting in a slow-moving stomach is a recipe for discomfort. Switching to smaller, more frequent meals with lower fat content can dramatically reduce nausea.
Our complete semaglutide diet plan covers optimal food choices, meal timing, and portion strategies. The foods to eat on semaglutide tend to be high in protein, moderate in complex carbohydrates, and lower in fat, a combination that works with the medication rather than against it. Alcohol consumption also affects tolerability and should be minimized, especially in the first 48 hours after injection.
Injection timing optimization
Choosing the best time of day for your injection can influence side effect severity. Many providers recommend injecting in the evening so that the initial peak, which occurs 24-48 hours later, falls on a day when you can manage symptoms more easily. If your worst day is typically two days after injection, back-calculate your injection day to ensure that peak falls on a weekend or a less demanding day.
Supportive supplements
Certain supplements may help manage GLP-1 side effects. Vitamin B12 addresses the potential for deficiency that long-term GLP-1 use may cause. Methylcobalamin is the most bioavailable form. Glycine may help with nausea management. Some patients report benefits from berberine for blood sugar stability, though this combination should be discussed with your provider.
Switching formulations
If injectable semaglutide is not tolerable regardless of dosing schedule, oral semaglutide offers a different absorption profile that some patients tolerate better. The oral formulation has different pharmacokinetics, with daily dosing and more gradual absorption, which naturally creates the kind of stable blood levels that split dosing attempts to achieve with injectables. Comparing injectable versus oral delivery methods can help you understand the tradeoffs.
Switching medications
Sometimes the answer is not modifying how you take semaglutide but considering a different medication entirely. Tirzepatide is a dual GIP/GLP-1 agonist with a different side effect profile. Some patients who cannot tolerate semaglutide do well on tirzepatide, and vice versa. Our semaglutide to tirzepatide conversion chart and switching guide cover how to transition safely between the two. For those interested in the next generation of GLP-1 medications, retatrutide offers triple-receptor activity, and our three-way comparison breaks down the differences.
Adding complementary medications
Anti-nausea medications like ondansetron can be taken on injection days to blunt the GI response. Proton pump inhibitors may help with acid-related symptoms. Phentermine is sometimes combined with lower-dose semaglutide to achieve appetite suppression from two complementary mechanisms, potentially allowing a lower semaglutide dose with fewer side effects. Discuss these options with your provider before combining medications.
Common mistakes with split dosing
People who attempt split dosing without proper guidance make predictable errors. Avoiding these mistakes is the difference between a potentially helpful modification and a counterproductive one.
Doubling the dose instead of splitting it
This is the most dangerous mistake. Some people misunderstand split dosing and take their full weekly dose twice per week instead of half the dose twice. If your weekly prescription is 1 mg, split dosing means 0.5 mg twice, not 1 mg twice. Taking double your prescribed dose can cause severe nausea, vomiting, and potentially dangerous blood sugar drops if you have diabetes. It also accelerates how quickly you go through your medication.
Inconsistent spacing
Injecting Monday morning and then again Tuesday evening because you forgot is not split dosing. It is two doses crammed into 36 hours, creating an amplified peak that will almost certainly make you feel worse. The minimum spacing between split doses is 48 hours. The ideal spacing for a twice-weekly protocol is 72-84 hours. Pick your days, set reminders, and stick to the schedule religiously.
Measurement errors
Drawing up small volumes from a vial introduces measurement error. At low concentrations, the difference between 10 units and 20 units of semaglutide can be less than the width of a syringe marking line. Use the smallest syringe that accommodates your dose volume for maximum accuracy. A 0.3 mL syringe with half-unit markings is far more precise than a 1 mL syringe for small doses. Our guide on understanding semaglutide units can help clarify what your measurements actually represent.
Splitting without provider knowledge
Modifying your dosing schedule without informing your prescriber is risky for multiple reasons. Your provider cannot properly monitor your response if they do not know what you are actually doing. If something goes wrong, they will be troubleshooting based on incorrect assumptions about your dosing. And if they order blood work or evaluate your progress, they need accurate dosing information to interpret the results correctly.
Abandoning titration principles
Split dosing does not eliminate the need for gradual dose escalation. If you are starting semaglutide for the first time, you still need to begin at the lowest dose and increase slowly, even if each dose level is being split. Jumping straight to a high dose split across two injections will likely produce the same side effects you were trying to avoid.
When split dosing might make sense
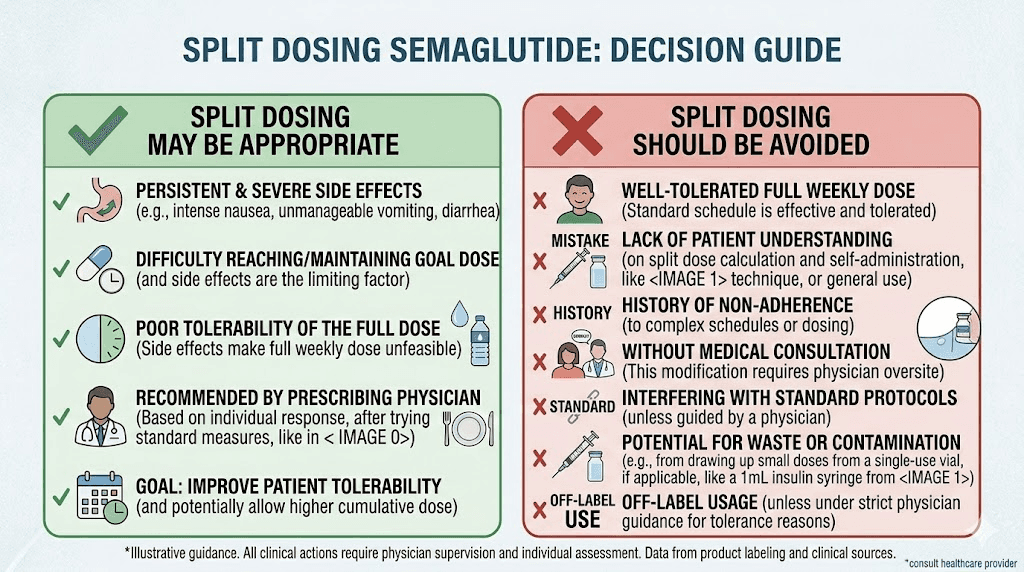
Despite the lack of clinical trial data, there are specific situations where split dosing has a reasonable pharmacological rationale and the benefit-risk calculus favors trying it.
The strongest case is for patients who have failed standard titration at multiple dose levels. If you have spent eight or more weeks at each dose increase, tried dietary modifications, used anti-nausea medications, and still cannot tolerate the weekly injection at a dose that provides therapeutic benefit, split dosing represents a logical next step before abandoning semaglutide entirely. The alternative, dropping to a dose so low that it does not produce meaningful weight loss, is arguably worse than an unstudied but pharmacologically sound modification.
Another reasonable scenario involves patients who experience a pronounced rollercoaster effect, severe symptoms for the first 48-72 hours followed by complete loss of appetite suppression by day six or seven. If the gap between peak and trough is causing both excess side effects and inadequate efficacy, split dosing addresses both problems simultaneously by flattening the curve in both directions.
Patients using compounded semaglutide who have the ability to measure precise doses also represent a better candidate pool than those using pen devices. The practical feasibility of accurate split dosing depends on having the right tools and the right formulation.
And finally, patients whose providers are actively involved in monitoring the transition are far more likely to do this safely than those going it alone based on internet advice. Having medical oversight for an off-label dosing modification is not optional, it is essential.
For researchers serious about understanding dosing modifications, SeekPeptides provides comprehensive protocol databases, dosing calculators, and expert-reviewed guides that cover both standard and alternative dosing approaches for GLP-1 medications.
When split dosing is not recommended
There are equally clear situations where split dosing should not be attempted.
If you are using a pen device (Ozempic or Wegovy), do not try to estimate half-doses by partially pressing the injection button. These devices are engineered for fixed-dose delivery, and partial doses are unreliable. The potential for dosing errors far outweighs any theoretical benefit from splitting.
If your side effects are mild and manageable, split dosing introduces unnecessary complexity. Mild nausea that resolves within 24 hours and does not significantly impair your daily activities is a normal part of semaglutide treatment. It does not warrant modifying a proven dosing protocol.
If you have not tried standard side effect management strategies first, split dosing should not be your first intervention. Extended titration, dietary changes, and timing adjustments are all proven approaches that should be exhausted before moving to experimental modifications.
If you are in the first four weeks of treatment, your body has not had time to adapt to the medication. GI side effects during the initial dose escalation phase are expected and typically improve with continued use. Splitting the dose prematurely may prevent the natural adaptation process from occurring.
If you have type 2 diabetes and semaglutide was prescribed for blood sugar management rather than weight loss, dosing modifications should be approached with extra caution. Blood sugar control is more sensitive to dosing patterns than weight management, and the pharmacokinetic differences between standard and split dosing could affect glycemic outcomes in ways that have not been studied.
If you cannot commit to the discipline of twice-weekly injections with precise measurements, standard weekly dosing is safer. An inconsistent split dosing schedule, with missed doses, variable timing, and imprecise measurements, will produce worse outcomes than consistent weekly dosing.
If you are considering how long to stay on semaglutide or thinking about stopping treatment, focus on those decisions independently rather than complicating them with dosing modifications at the same time.
The role of GLP-1 pharmacology in dosing decisions
Making informed decisions about semaglutide dosing requires understanding where it sits in the broader GLP-1 medication landscape.
Semaglutide is not the only option. The GLP-1 class includes medications with vastly different pharmacokinetic profiles, and sometimes the best solution to dosing problems is not modifying the dose but choosing a medication whose natural profile better matches what you need.
Liraglutide (Saxenda) has a 13-hour half-life and requires daily injections. While this means more frequent needles, it naturally provides the kind of stable blood levels that split dosing attempts to create with semaglutide. If peak-related side effects are your primary concern, daily dosing with a shorter-acting GLP-1 might be a better pharmacological fit than twice-weekly dosing with a longer-acting one.
Tirzepatide has a half-life of approximately five days, shorter than semaglutide but still long enough for weekly dosing. The dosage comparison between the two medications reveals important differences in how they are titrated and maintained. Interestingly, the question of splitting tirzepatide doses comes up just as frequently, and the pharmacokinetic rationale is similar.
Retatrutide is the newest entrant, a triple-receptor agonist targeting GLP-1, GIP, and glucagon receptors simultaneously. Early trials show impressive weight loss results, and the different receptor profile may offer better tolerability for some patients. Comparing the full spectrum of current and emerging GLP-1 medications helps put dosing decisions in perspective.
GLP-1 patches and oral liquid formulations represent additional delivery innovations that naturally provide more stable drug levels through continuous or frequent dosing. As these options become more widely available, the need for split dosing injectable medications may diminish.
Understanding the timeline for GLP-1 medications to take effect is important regardless of which medication or dosing schedule you choose. The underlying biology of GLP-1 receptor activation, metabolic adaptation, and appetite recalibration operates on similar timescales across all formulations.
Tracking your results with split dosing
If you proceed with split dosing under medical supervision, systematic tracking is essential for evaluating whether the modification is actually working.
What to track daily
Record your appetite level on a 1-10 scale at three fixed times: morning, midday, and evening. Note any nausea, its timing relative to your injection, and its severity on the same scale. Track your energy levels, sleep quality, and any other side effects you were experiencing on weekly dosing. This daily log creates a quantitative baseline for comparison.
What to track weekly
Weigh yourself at the same time on the same day each week, ideally first thing in the morning after using the bathroom. Weight fluctuations of 1-3 pounds day to day are normal due to water retention and digestive contents. Weekly averages are more meaningful than any single measurement. Compare your weekly weight trend on split dosing to your trend on standard dosing.
What to assess at four weeks
After four weeks of split dosing, you should have enough data to make a preliminary assessment. Are side effects meaningfully reduced? Is appetite suppression maintained? Is weight loss continuing at a comparable rate? If the answers are yes, the modification appears to be working for you. If side effects persist or weight loss has stalled, the split may not be providing the benefits you hoped for.
Discussing these results with your provider is critical. They may want to see blood work to ensure metabolic markers are responding appropriately, check your energy levels and overall wellbeing, and determine whether to continue, modify, or discontinue the split dosing approach.
Using tools like the semaglutide dosage calculator and maintaining a structured diet plan alongside split dosing ensures you are controlling as many variables as possible and can attribute changes accurately to the dosing modification rather than other factors.
What the medical community says
The medical community is divided on semaglutide split dosing, which reflects the current state of evidence rather than any fundamental disagreement about the pharmacology.
The American Diabetes Association and the Obesity Medicine Association have not issued formal guidance on split dosing. Their current recommendations reference the FDA-approved weekly dosing schedule exclusively. This is not because they have evaluated and rejected split dosing. It is because there are no clinical trial data to inform a recommendation either way.
Novo Nordisk, the manufacturer of Ozempic and Wegovy, explicitly recommends once-weekly dosing and has not studied or endorsed any alternative schedules. From a regulatory and liability perspective, this is the only position a pharmaceutical manufacturer can reasonably take. Their approved labeling reflects what their clinical trials demonstrated.
Individual physicians and obesity medicine specialists hold varying opinions based on their clinical experience. Some have adopted split dosing as a standard tool in their practice for patients who struggle with weekly dosing tolerability. They point to the pharmacokinetic rationale, the consistent anecdotal evidence from patients, and the low theoretical risk when total weekly dose is maintained. Others remain cautious, preferring to work within the studied protocol and use established side effect management strategies before considering experimental modifications.
Compounding pharmacies have, in some cases, actively facilitated split dosing by providing specific concentration formulations designed for twice-weekly measurement. This practical support has made split dosing easier to implement but has also drawn criticism from those who argue that compounding pharmacies should not be encouraging unstudied dosing modifications.
The consensus, if one exists, is this: split dosing is a pharmacologically reasonable modification that has not been clinically validated. It should be reserved for patients who have tried standard approaches, administered under medical supervision, and evaluated systematically.
Resources like SeekPeptides help bridge the gap between emerging dosing strategies and evidence-based practice by providing comprehensive, up-to-date information that helps researchers and patients navigate these evolving conversations with their healthcare providers.
Long-term considerations
If split dosing works for you in the short term, what happens over months and years of continued use?
The honest answer is that nobody knows. Long-term safety data for semaglutide exists only for the approved weekly dosing regimen. The STEP and SUSTAIN clinical trials followed patients for up to two years on standard dosing. No comparable data exists for split dosing.
Theoretically, since the total weekly drug exposure is the same, long-term outcomes should be similar. The difference in concentration patterns (lower peaks, higher troughs) is modest enough that major safety divergence seems unlikely. But "seems unlikely" and "proven safe" are very different standards.
One consideration that may become relevant over time is injection site management. Twice-weekly injections mean 104 injections per year instead of 52. Each injection creates minor tissue trauma at the injection site. Over years, this increased injection frequency could theoretically accelerate the development of subcutaneous nodules, lipodystrophy, or scar tissue at preferred injection sites. Rigorous injection site rotation becomes even more important with twice-weekly dosing.
Another consideration is treatment fatigue. Adding a second weekly injection, even a smaller one, adds complexity and burden to your routine. Some people find that the benefit of reduced side effects outweighs this inconvenience. Others find that the novelty wears off and maintaining a twice-weekly schedule becomes harder to sustain than simply enduring the weekly injection.
If you eventually decide to restart semaglutide after a break or transition your dosing schedule for other reasons, work with your provider to adjust systematically rather than making changes unilaterally.
Frequently asked questions
Can I split my Ozempic pen dose to twice a week?
Technically you should not attempt to split doses with an Ozempic pen. The pen is designed to deliver preset doses and does not reliably deliver exact half-doses. Split dosing is only practical with compounded semaglutide from multi-dose vials where you can draw up precise volumes with an insulin syringe. Attempting to use a pen device for split dosing introduces unacceptable measurement error.
Will I lose less weight if I split my semaglutide dose?
Mathematical models suggest that split dosing maintains 80% to 95% of weight loss efficacy compared to standard weekly dosing, assuming the total weekly dose remains the same. The slight potential reduction comes from lower peak concentrations, but this is partially offset by higher trough levels providing more consistent appetite suppression. Most people who split their dose report similar weight loss timelines to standard dosing.
What is the best schedule for split dosing semaglutide?
The Monday-Thursday schedule is most commonly recommended because it creates approximately 72-hour intervals between doses and is easy to remember. A Tuesday-Friday schedule works equally well. The critical requirement is a minimum of 48 hours between injections to avoid creating amplified drug peaks. Whatever schedule you choose, consistency is more important than the specific days.
How long should I try split dosing before deciding if it works?
Most providers recommend a four-to-eight week trial period. This allows enough time for your body to adjust to the new dosing pattern and provides sufficient data to evaluate whether side effects have genuinely improved. Four weeks is the minimum because it takes approximately that long for semaglutide to reach a new steady state after any dosing change. Track your symptoms systematically throughout this period.
Can I split my dose into more than two injections per week?
Three-times-weekly dosing (Monday, Wednesday, Friday) and even daily microdosing are theoretically possible and would further flatten the drug concentration curve. However, these approaches increase injection burden, multiply opportunities for measurement error, and deviate even further from studied protocols. Most providers who support split dosing recommend starting with the simplest modification, twice weekly, before considering more frequent schedules.
Does split dosing affect how long semaglutide stays in my system?
The total time semaglutide remains active in your body does not change significantly with split dosing. The drug half-life of approximately seven days means that it takes about five weeks to fully clear your system regardless of dosing frequency. What changes is the concentration pattern during each week, with lower peaks and higher troughs creating a more stable level throughout the dosing period.
Is split dosing the same as microdosing semaglutide?
Not exactly. Split dosing divides a standard prescribed dose into multiple smaller injections while maintaining the same total weekly amount. Microdosing typically refers to using a lower total dose than what would be prescribed, sometimes divided into frequent small injections. The terms are often used interchangeably in online forums, but the distinction matters clinically because split dosing preserves total drug exposure while microdosing reduces it.
What if my nausea gets worse with split dosing?
If side effects worsen after switching to split dosing, it may indicate a measurement error resulting in inadvertently higher individual doses, or it may suggest that your side effects are not primarily driven by peak concentration. Return to your standard weekly schedule and discuss the results with your provider. Sometimes understanding how semaglutide suppresses appetite and working with that mechanism through dietary adjustments is more effective than modifying the injection schedule.
Can I switch back to weekly dosing after trying split dosing?
Yes, you can return to standard weekly dosing at any time. Simply take your full weekly dose on your next scheduled injection day and resume the once-weekly schedule from there. No tapering or special transition is needed because the total weekly drug exposure does not change. Some people try split dosing temporarily during dose escalation and then return to weekly dosing once they have adapted to their maintenance dose.
Should I adjust my diet differently with split dosing?
The dietary principles remain the same regardless of dosing schedule. Focus on semaglutide-friendly foods, eat smaller meals, and avoid high-fat foods especially in the 24 hours after each injection. The main difference is that with split dosing, you have two post-injection windows per week where dietary caution is advisable instead of one. Maintaining a structured meal plan helps manage both nutrition and side effects consistently.
External resources
PMC - Alternative dosing regimens of GLP-1 receptor agonists
PMC - Clinical recommendations for GI adverse events with GLP-1 agonists
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, protocol databases, and a community of thousands who have navigated these exact questions about dosing optimization and side effect management.
In case I do not see you, good afternoon, good evening, and good night.