Feb 28, 2026

Before your next injection, stop and read this. Because what nobody tells you about starting semaglutide is that the side effects do not follow a predictable script. Some people feel nauseous within hours of their first dose. Others sail through four weeks without a single symptom, only to get blindsided when the dose goes up. And a small percentage never experience meaningful side effects at all.
The question everyone asks is simple. How long after taking semaglutide do you feel side effects? But the answer involves far more than a single number. It depends on your dose, your body composition, your diet, your hydration levels, and even the time of day you inject. Clinical trials paint one picture. Real-world experience paints another. The gap between the two is where most of the confusion lives.
This guide breaks down exactly what happens in your body after each semaglutide injection, when the most common side effects typically appear, how long they last at each dose level, and what the STEP trial data actually shows about the timeline from first injection to peak side effects. Whether you are on compounded semaglutide or a brand-name formulation, the physiological response follows similar patterns. Understanding those patterns is the difference between panicking at normal symptoms and recognizing when something genuinely needs attention.
SeekPeptides has compiled data from clinical trials, FDA adverse event reports, and thousands of user experiences to build the most comprehensive side effect timeline available anywhere. This is not a generic overview. This is the specific, week-by-week breakdown that researchers and users actually need.
When do semaglutide side effects actually start
The short answer is within hours to days of your first injection. But that oversimplification hides important nuances that determine your actual experience.
Semaglutide reaches peak plasma concentration approximately 1 to 3 days after subcutaneous injection. This means the medication is at its strongest roughly 24 to 72 hours after you inject. For most people, this is when the first side effects appear. Bloating, mild nausea, and reduced appetite are typically the earliest signals that the drug is active in your system.
Not everyone notices something right away, though.
In clinical trials, some participants reported no discernible side effects during the entire first month at the 0.25 mg starting dose. Their bodies processed the medication without triggering the gastrointestinal responses that make headlines. These participants often encountered their first side effects only after the dose escalated to 0.5 mg or higher, which happens around week 5 in the standard semaglutide dosing schedule.
The mechanism behind this is straightforward. Semaglutide is a GLP-1 receptor agonist that slows gastric emptying, reduces appetite through hypothalamic signaling, and increases insulin secretion in a glucose-dependent manner. When your stomach empties more slowly than your brain expects, nausea results. When your gut motility changes, constipation or diarrhea can follow. These are not signs that something is wrong. They are signs that the drug is working exactly as designed.
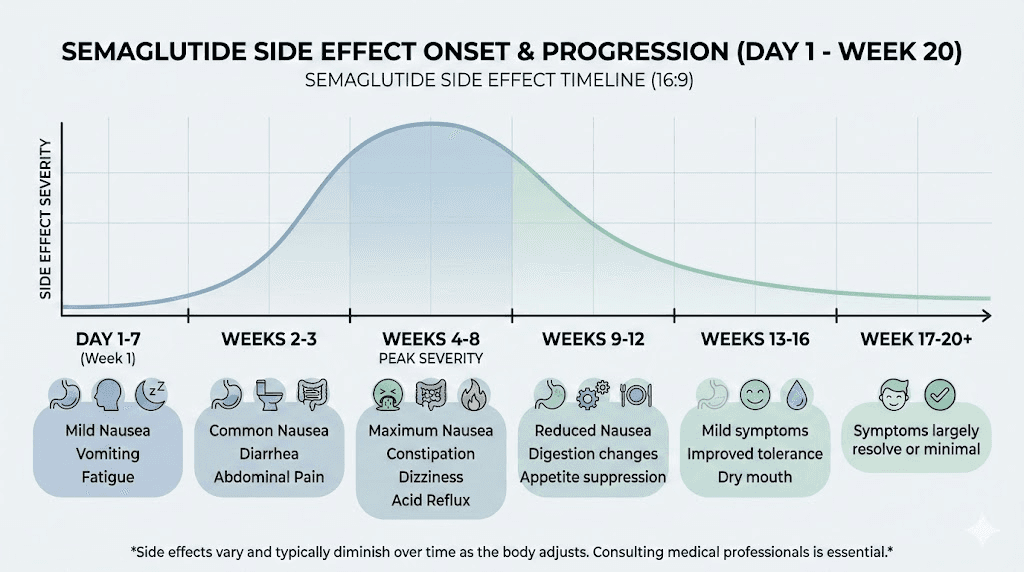
Here is the general timeline that emerges from the research:
Hours 0 to 24: Most people feel nothing. The drug is still being absorbed from the injection site.
Hours 24 to 72: Peak plasma concentration. First symptoms may appear, most commonly mild nausea or decreased appetite.
Days 3 to 7: If side effects are going to occur at this dose, they typically manifest by now. Fatigue and burping are common in this window.
Days 7 to 14: Side effects from the current dose often begin to ease as the body starts adapting to the new GLP-1 levels.
But that timeline resets with every dose increase. And this is where most people get caught off guard.
The complete week-by-week side effect timeline
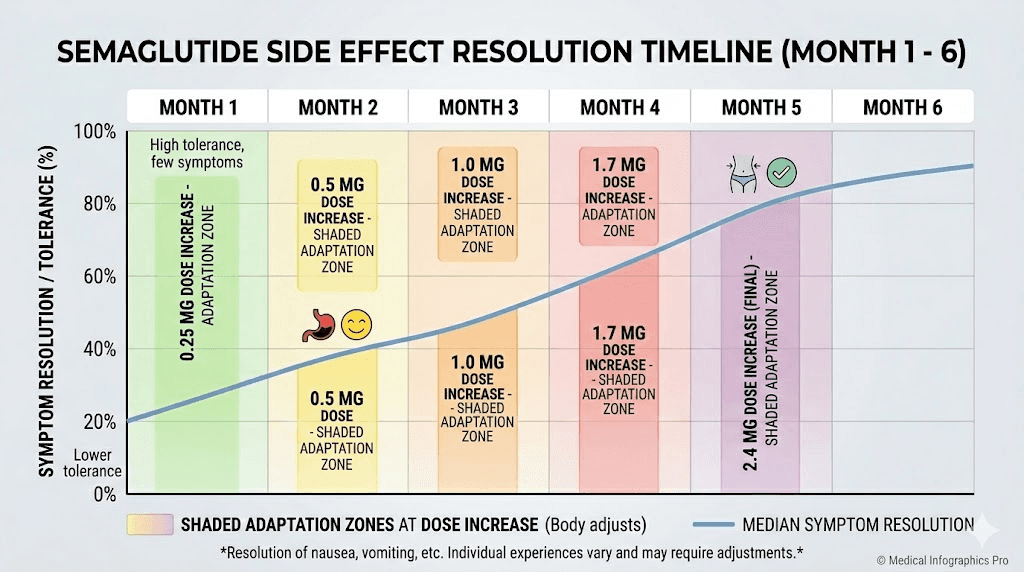
Understanding the full trajectory requires looking at the standard dose escalation schedule and mapping side effects onto each phase. The pattern that emerges from the STEP clinical trials is remarkably consistent across thousands of participants.
Weeks 1 to 4: the 0.25 mg phase
This is the introductory dose. It exists solely to let your body acclimate to semaglutide before therapeutic dosing begins. At 0.25 mg, you are not yet at a dose that produces significant weight loss or glycemic control. You are essentially training your GLP-1 receptors.
Most people experience mild symptoms. Or none at all.
The most common side effect during this phase is subtle appetite reduction. You might notice you are satisfied with smaller meals, that your usual portion size feels like too much, or that you simply forget about snacking. This is the medication beginning to work on hypothalamic appetite signaling before gastric emptying changes become noticeable.
If nausea occurs during weeks 1 to 4, it tends to be mild. A slight queasiness after eating, particularly after large or fatty meals. This usually peaks on days 2 to 3 after each weekly injection and fades by day 5. Some people describe it as the feeling you get when you eat too much at a holiday dinner, that uncomfortably full sensation that sits in your upper abdomen.
Constipation can also begin during this phase, though it is less common at the starting dose. Slower gastric emptying means slower intestinal transit, which means harder stools and less frequent bowel movements. Increasing fiber and water intake during weeks 1 to 4 helps prevent this from escalating when doses go up.
Weeks 5 to 8: the 0.5 mg phase
This is where things get real for most people.
The jump from 0.25 mg to 0.5 mg represents a doubling of your dose. And for many, this is the moment side effects announce themselves with authority. The STEP trials show a clear uptick in reported gastrointestinal events during this period, with nausea being the most frequent complaint.
At 0.5 mg, gastric emptying slows significantly more than at the introductory dose. Meals that sat comfortably before now feel heavy. Bloating increases. Some people experience their first episodes of vomiting, though this remains uncommon at the 0.5 mg level.
The 0.5 mg phase is also when dizziness and headaches tend to appear. Clinical trial data shows headache at approximately 14% incidence and dizziness at around 8%. These are often related to changes in blood sugar regulation and fluid balance rather than direct neurological effects of the medication.
Critical point: the body begins adapting during weeks 5 to 8. Most people who experience nausea at the 0.5 mg dose find that it improves noticeably by week 7 or 8. The gastrointestinal tract is learning to function with slower emptying times, and the nervous system is recalibrating its expectations about how quickly food should move through the digestive system.
Eating smaller, more frequent meals during this phase makes a substantial difference. Clinical guidance consistently recommends reducing portion sizes by 30 to 50% and eating 4 to 6 smaller meals rather than 2 to 3 large ones.
Weeks 9 to 12: the 1.0 mg phase
For those on the Ozempic diabetes protocol, 1.0 mg may be the maintenance dose. For weight loss protocols, it is another stepping stone.
Side effects during weeks 9 to 12 follow a predictable pattern. They intensify briefly after the dose increase, then gradually subside over 2 to 3 weeks as the body adapts. The severity is typically less dramatic than the 0.25 to 0.5 mg jump because the body has already developed some tolerance to GLP-1 receptor activation.
New side effects may emerge at this dose level that were absent at lower doses. Insomnia becomes more commonly reported. Some users notice changes in taste perception, with certain foods tasting different or less appealing. This is not well-studied in clinical trials but appears frequently in user reports and is likely related to altered gut hormone signaling that affects the vagus nerve and taste pathways.
The good news from the data: participants who tolerated the 0.5 mg dose without severe side effects almost always tolerated the 1.0 mg dose as well. The correlation between early tolerance and continued tolerance is strong. If you made it through weeks 5 to 8 without major issues, weeks 9 to 12 will likely be manageable.
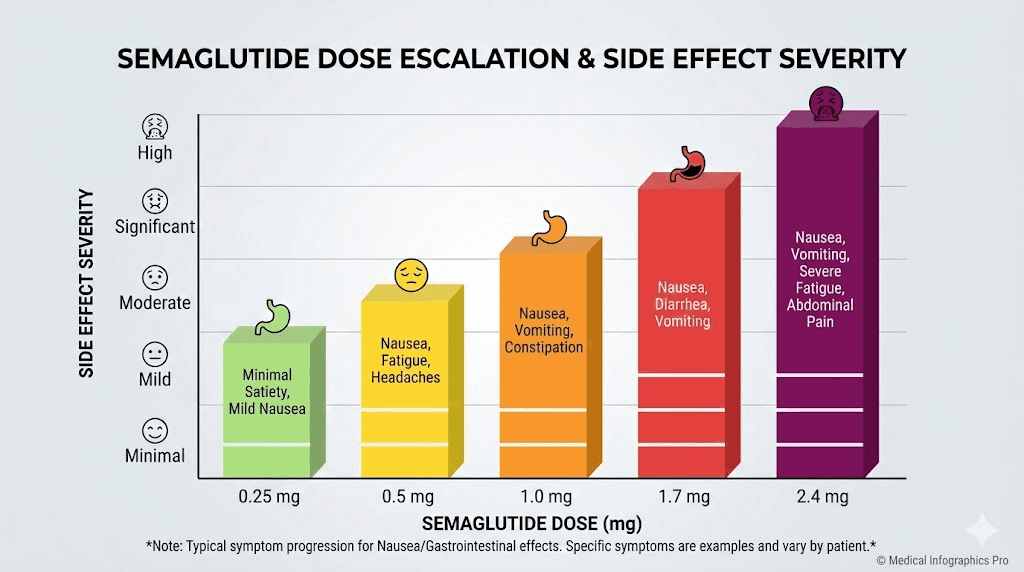
Weeks 13 to 16: the 1.7 mg phase (Wegovy protocol)
If you are following the Wegovy weight loss protocol, the dose continues climbing. The 1.7 mg dose represents a significant increase in GLP-1 receptor activation, and this is where the STEP trial data shows the highest incidence of gastrointestinal side effects.
At 1.7 mg, nausea prevalence reaches its near-peak. The STEP trials reported nausea in approximately 44% of participants receiving the full 2.4 mg dose, and a substantial portion of those cases began or intensified during the 1.7 mg phase.
Vomiting becomes more common. Constipation may shift to diarrhea, or alternate between the two. Fatigue can intensify as caloric intake drops and the body adjusts to operating on less fuel. Some participants report feeling unusually tired for 2 to 3 days after each injection, with energy returning by mid-week.
This is also the dose level where the conversation about whether to continue escalating or hold at the current dose becomes medically relevant. If side effects at 1.7 mg are significant, many providers recommend staying at this dose for an additional 4 weeks before attempting the final escalation to 2.4 mg. The clinical literature supports this approach, as delayed escalation does not appear to compromise long-term weight loss outcomes.
Weeks 17 to 20: the 2.4 mg maintenance phase
The final dose. The destination that the entire dosing schedule has been building toward.
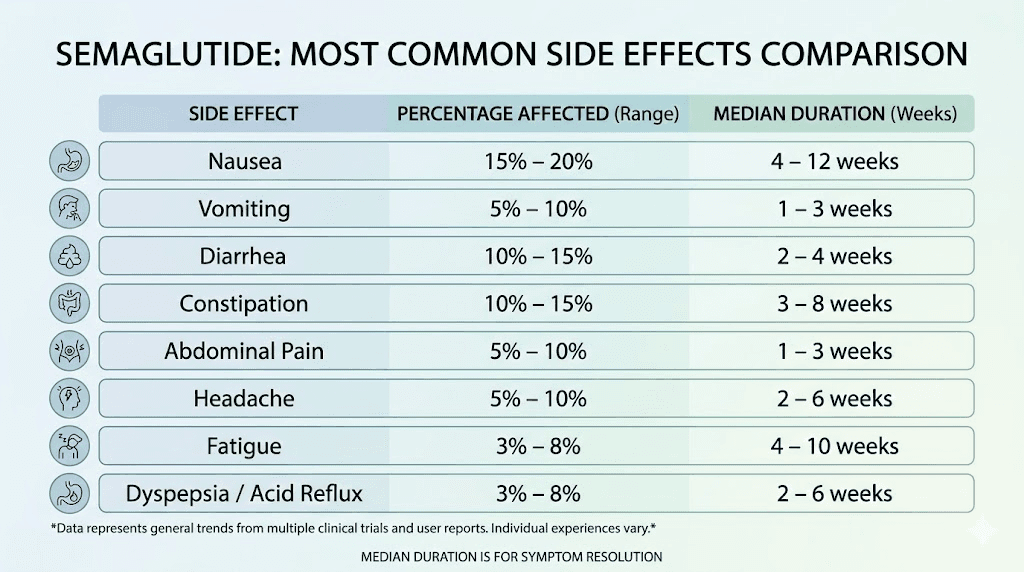
Here is what the STEP trials tell us about side effects at 2.4 mg:
Nausea: 43.9% of participants (vs. 16.1% on placebo)
Diarrhea: 29.7% (vs. 15.9% on placebo)
Vomiting: 24.5% (vs. 6.3% on placebo)
Constipation: 24.2% (vs. 11.1% on placebo)
Headache: approximately 14%
Fatigue: approximately 11%
Dizziness: approximately 8%
Hair thinning: approximately 3% (vs. 1% on placebo)
The crucial detail that gets lost in these numbers: most of these side effects are transient. The median duration of nausea episodes was 8 days. Diarrhea lasted a median of 3 days. Vomiting episodes lasted a median of 2 days. These are not chronic conditions. They are adjustment reactions that come and go.
By week 20, the cumulative incidence of first-time gastrointestinal adverse events plateaus. In other words, if you have not experienced significant GI side effects by week 20, you are unlikely to develop them going forward on a stable dose. The body has either adapted or demonstrated that it handles the medication well.
Only 4.3% of participants discontinued treatment entirely due to gastrointestinal side effects. That means 95.7% of people who started semaglutide were able to continue despite some degree of GI discomfort. The side effects, while common, were overwhelmingly manageable.
The most common side effects and exactly when each one appears
Not all side effects show up at the same time. Each one has its own typical onset window, peak period, and resolution timeline. Understanding these individual patterns helps you identify what is normal and what deserves a conversation with your healthcare provider.
Nausea
This is the side effect that defines the semaglutide experience for most people. It appears earlier, lasts longer, and affects more people than any other symptom.
Typical onset: 24 to 72 hours after the first injection, or 24 to 72 hours after any dose increase.
Peak severity: Usually worst during the first 2 to 3 days after each weekly injection, then fades. The overall peak across the treatment course occurs around weeks 4 to 8, coinciding with the dose escalation phase.
Duration: Individual nausea episodes last a median of 8 days according to pooled STEP trial data. Most participants report significant improvement within 4 to 6 weeks of maintaining a stable dose. Complete resolution typically occurs within 2 to 3 months.
The nausea is directly caused by slowed gastric emptying. Your stomach is holding food longer than your brain expects, creating a mismatch between what your gut signals and what your central nervous system interprets as normal. As your nervous system recalibrates, the nausea subsides.
Eating smaller meals helps enormously. Avoiding high-fat and fried foods reduces the duration of gastric retention and lowers nausea intensity. Some users find that timing their injection in the evening allows them to sleep through the worst of the initial nausea wave.
Constipation
The second most disruptive side effect, and one that can persist longer than nausea if not actively managed.
Typical onset: 1 to 2 weeks after starting or increasing dose.
Peak severity: Weeks 4 to 12, often worsening with each dose increase.
Duration: Can persist throughout treatment if dietary modifications are not made. Responds well to increased fiber, hydration, and if necessary, osmotic laxatives.
The mechanism is simple. GLP-1 receptor activation slows gut motility. Food and waste move through your intestines more slowly. Water is reabsorbed from stool, making it harder and more difficult to pass. This is a direct pharmacological effect, not a side effect in the traditional sense. It is the medication doing what it is designed to do.
Treating semaglutide constipation effectively requires proactive dietary changes. Increasing daily fiber to 25 to 30 grams, drinking at least 2 to 3 liters of water, and incorporating magnesium-rich foods or supplements can prevent constipation from becoming a significant quality-of-life issue.
Diarrhea
Paradoxically, semaglutide can cause both constipation and diarrhea. Sometimes in the same person, during different weeks.
Typical onset: Days 1 to 5 after dose initiation or increase.
Peak severity: First 2 weeks at each new dose level.
Duration: Individual episodes last a median of 3 days. Usually resolves within the first month at a stable dose.
Diarrhea with semaglutide is typically related to changes in bile acid metabolism and altered gut microbiome composition rather than the gastric emptying changes that cause nausea and constipation. The small intestine responds to increased GLP-1 signaling by altering fluid secretion patterns, which can produce loose or watery stools in the adaptation period.
If diarrhea persists beyond 2 to 3 weeks at a stable dose, it deserves medical evaluation. Persistent diarrhea can indicate other conditions unrelated to semaglutide, and attributing all symptoms to the medication is a common mistake.
Vomiting
Typical onset: 24 to 48 hours after injection, most common during dose increases.
Peak severity: First 1 to 2 days after injection during weeks 5 to 20.
Duration: Episodes last a median of 2 days. Usually decreases in frequency after 4 to 6 weeks at a stable dose.
Vomiting is less common than nausea and typically occurs when nausea is not adequately managed. The most frequent trigger is eating too much or eating too quickly after the dose increase. The stomach, already emptying more slowly, simply cannot accommodate the volume of food that felt normal at a lower dose.
Prevention is more effective than treatment. Eating slowly, stopping before feeling full, and avoiding meals within 2 to 3 hours of lying down significantly reduces vomiting episodes. If vomiting occurs more than twice per week despite dietary modifications, dose adjustment may be necessary.
Headache
Typical onset: Days 1 to 3 after injection.
Peak severity: First 4 weeks of treatment.
Duration: Usually resolves within the first month. Individual episodes last 1 to 2 days.
Headache during semaglutide treatment is primarily related to blood sugar fluctuations and dehydration rather than a direct effect of the medication on the central nervous system. When caloric intake drops and insulin dynamics change, the brain can experience relative glucose deprivation that manifests as headache. Staying hydrated and maintaining regular, smaller meals helps prevent this.
Fatigue
Semaglutide fatigue affects approximately 11% of users, and it tends to follow a different pattern than the gastrointestinal symptoms.
Typical onset: Weeks 2 to 4, sometimes not appearing until the second or third dose increase.
Peak severity: Weeks 4 to 12, particularly during caloric deficit periods.
Duration: Can persist as long as the caloric deficit is significant. Improving protein intake and ensuring adequate caloric intake (not extreme restriction) helps resolve it.
Fatigue with semaglutide has multiple causes. Reduced caloric intake means less available energy. Changes in insulin dynamics can cause temporary energy dips. Altered sleep patterns, sometimes related to GI discomfort or insomnia, compound the problem. And rapid weight loss can temporarily reduce metabolic rate, leaving you feeling sluggish.
The distinction between medication-related fatigue and insufficient nutrition is important. If you are eating fewer than 1,200 calories per day (women) or 1,500 calories per day (men) while on semaglutide, the fatigue is likely nutritional, not pharmacological. Consulting with your provider about appropriate dietary planning on semaglutide can address this.
Hair thinning
Hair loss on GLP-1 medications is one of the most distressing side effects, though it affects a relatively small percentage of users.
Typical onset: 3 to 6 months after starting treatment.
Peak severity: Months 4 to 8.
Duration: Usually resolves within 6 to 12 months, even if treatment continues.
The hair loss associated with semaglutide is telogen effluvium, a temporary condition triggered by rapid weight loss rather than the medication itself. When the body loses weight quickly, it diverts nutritional resources away from non-essential functions like hair growth. This pushes more hair follicles into the resting phase simultaneously, resulting in noticeable shedding 3 to 6 months later.
Ensuring adequate protein intake (at least 60 to 80 grams daily), taking a biotin supplement, and maintaining iron and zinc levels can minimize hair thinning. If hair loss is severe or accompanied by other symptoms like extreme fatigue, thyroid function should be evaluated.
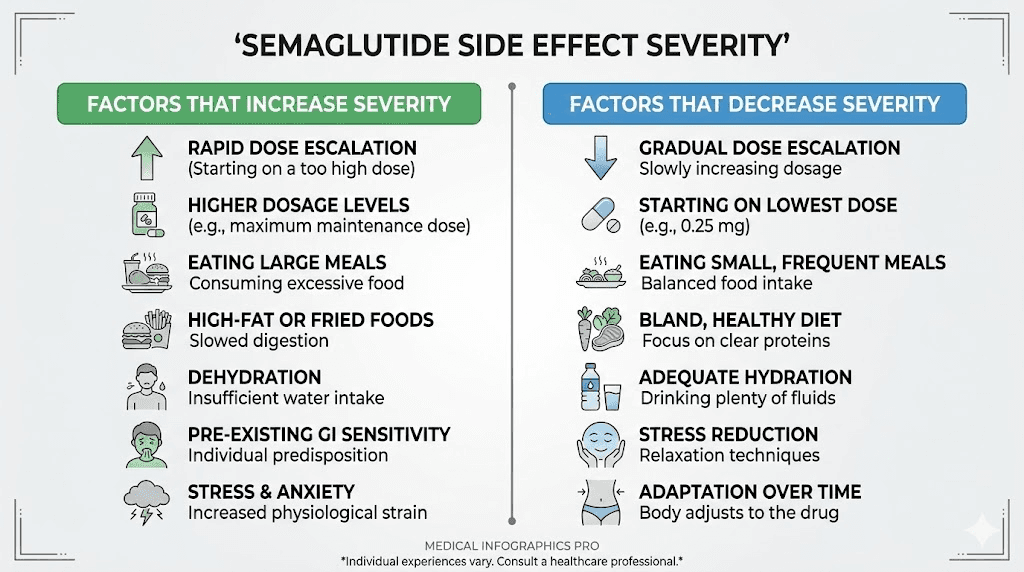
Why some people feel side effects immediately and others do not
The variability in semaglutide side effects is not random. Several factors predict who will experience early, intense side effects and who will have a smoother transition.
Body weight and composition
Semaglutide distributes through body tissues after injection. People with higher body weight may experience a lower effective concentration at the starting dose, which can delay side effect onset. Conversely, those with lower body weight may feel effects more quickly and more intensely because the concentration relative to their body mass is higher.
This is why the semaglutide dosage calculator is valuable. Understanding your dose relative to body weight provides context for what to expect.
Pre-existing gastrointestinal conditions
People with irritable bowel syndrome, gastroparesis, gastroesophageal reflux disease, or chronic constipation are significantly more likely to experience early and intense side effects. The GLP-1 receptor agonist mechanism directly affects gut motility, and systems that are already dysregulated respond more dramatically to further manipulation.
If you have a pre-existing GI condition, discussing a slower dose escalation schedule with your provider is strongly recommended. Extended titration periods, where you spend 6 to 8 weeks at each dose rather than the standard 4 weeks, are supported by the clinical literature and can dramatically improve tolerability.
Concurrent medications
Medications that affect gastrointestinal motility, such as opioids, anticholinergics, certain antidepressants, and proton pump inhibitors, can interact with semaglutide to intensify side effects. Opioids, for instance, already slow gut motility. Add semaglutide on top, and constipation can become severe.
Combining semaglutide with other medications requires careful consideration of how each drug affects GI function. Your provider should review your full medication list before starting semaglutide.
Diet and eating habits
This is the single most controllable factor influencing side effect severity.
People who continue eating large, heavy, high-fat meals after starting semaglutide experience significantly more nausea and vomiting than those who proactively adjust their eating habits. The stomach is emptying more slowly. Putting a large volume of food into a slow-moving stomach is a recipe for discomfort.
The foods you eat while on semaglutide matter enormously. Lean proteins, vegetables, whole grains, and smaller portions are your allies. Fried foods, heavy sauces, large portions, and eating quickly are your enemies during the adjustment period.
Genetics and individual metabolism
There is emerging evidence that genetic variations in GLP-1 receptor expression and sensitivity affect both the therapeutic response to semaglutide and the side effect profile. Some people are naturally more sensitive to GLP-1 receptor agonism, experiencing stronger appetite suppression but also more intense gastrointestinal effects.
This is not something you can test for or control. But it explains why two people of similar weight and health status can have dramatically different experiences on the same dose.
What happens at each dose increase
One of the most common mistakes is assuming that because you tolerated the starting dose well, you will breeze through every dose increase. The reality is that each escalation triggers a new adaptation period, and side effects that had resolved at the previous dose can temporarily return.
The adaptation cycle
Every dose increase follows roughly the same pattern:
Days 1 to 3: New symptoms appear or previous symptoms return. Nausea is the most common recurring symptom. Bloating and fullness increase.
Days 4 to 7: Symptoms peak. This is the most uncomfortable window. Appetite suppression is strongest during this period, which can lead to inadequate caloric intake if you are not careful.
Days 7 to 14: Gradual improvement begins. The body starts adapting to the higher GLP-1 levels. Nausea lessens. Appetite returns partially.
Days 14 to 28: Significant improvement for most people. By the end of the month at the new dose, the side effects have either resolved or reduced to a level that does not interfere with daily function.
This cycle repeats at 0.5 mg, 1.0 mg, 1.7 mg, and 2.4 mg. Each time, the adaptation period tends to be slightly shorter and slightly less intense than the previous one, because the GLP-1 receptors are increasingly accustomed to agonist activity.
When to hold a dose instead of escalating
The standard semaglutide dosing chart calls for monthly dose increases, but this is a guideline, not a mandate. Holding at a dose for an extra 4 weeks before escalating is a medically supported strategy when:
Nausea or vomiting persists beyond 2 weeks at the current dose
You are unable to eat at least 1,000 calories per day comfortably
Dehydration symptoms appear (dark urine, dizziness on standing, dry mouth)
You are losing weight faster than 1 to 2 pounds per week on the current dose (aggressive weight loss increases side effect risk)
In the STEP trials, delayed escalation did not compromise overall weight loss outcomes at 68 weeks. Participants who took longer to reach the full dose achieved similar total weight loss to those who followed the standard schedule. The body simply needs different amounts of time to adapt, and forcing the schedule creates unnecessary discomfort.
How long do semaglutide side effects last
This is the question that matters most to people in the thick of it. When will this end?
The answer depends on which side effect you are experiencing and whether you are still in the dose escalation phase or have reached maintenance dosing.
During dose escalation (weeks 1 to 20)
Side effects are most common and most intense during this period. The STEP trial data shows that the cumulative incidence of gastrointestinal adverse events peaks around week 20 and plateaus thereafter. This means the first 20 weeks are the adjustment period, and anything that shows up after that is increasingly rare.
For specific symptoms during escalation:
Nausea: Individual episodes last 5 to 14 days. Overall prevalence peaks at weeks 8 to 12. Significant improvement by weeks 16 to 20 for most participants.
Constipation: Can persist throughout escalation. Typically worst at weeks 6 to 14. Responds to dietary management and usually improves once dose stabilizes.
Diarrhea: Episodes last 2 to 5 days. Less common than constipation. Usually resolves faster.
Fatigue: Worst during weeks 4 to 12, particularly during rapid caloric reduction. Improves with adequate nutrition.
After reaching maintenance dose
Once you reach your target dose (whether 0.5 mg, 1.0 mg, or 2.4 mg) and stay there, the side effect trajectory improves markedly.
Most participants in the STEP trials reported that gastrointestinal symptoms resolved or became minimal within 4 to 8 weeks of maintaining a stable dose. By 3 months on a stable dose, the vast majority of participants reported no ongoing side effects that interfered with daily life.
However, some people do experience persistent, low-grade symptoms. About 5 to 10% of semaglutide users report ongoing mild nausea or appetite-related discomfort that continues throughout treatment. For most, this is not severe enough to warrant discontinuation, but it is a real experience that should be acknowledged rather than dismissed.
If side effects persist beyond 3 months at a stable dose and are affecting your quality of life, a conversation with your provider about dose adjustment is appropriate. Reducing by one dose level and maintaining there is a valid strategy that preserves most of the weight loss benefit while improving tolerability.
Managing semaglutide side effects effectively
The difference between a miserable semaglutide experience and a manageable one often comes down to proactive management rather than reactive coping. Knowing what is coming and preparing for it changes the equation entirely.
Nausea management protocol
Start implementing these strategies before your first injection, not after nausea hits:
Meal sizing: Cut portions by 30 to 50% from day one. Do not wait until nausea forces you to eat less. Getting ahead of this prevents the worst episodes. Aim for 5 to 6 small meals rather than 3 large ones.
Meal composition: Lean proteins, complex carbohydrates, and cooked vegetables are the easiest foods to tolerate. Raw vegetables, greasy foods, spicy dishes, and highly processed foods are the hardest. Building a semaglutide-friendly meal plan before starting treatment gives you a framework when appetite and nausea make decision-making difficult.
Timing: Many users report less nausea when injecting in the evening, allowing the initial nausea wave to pass during sleep. Others prefer morning injections so they can manage symptoms during waking hours. Experiment with injection timing during the first few weeks to find what works for you.
Ginger: Ginger tea, ginger chews, and ginger supplements have modest anti-nausea effects and are safe to use alongside semaglutide. They will not eliminate nausea, but they can take the edge off.
Over-the-counter remedies: If nausea is moderate, over-the-counter options like bismuth subsalicylate can help. For more significant nausea, your provider can prescribe ondansetron (Zofran) for short-term use during dose transitions.
Constipation management
Semaglutide constipation responds well to a three-pronged approach:
Fiber: Increase intake to 25 to 30 grams daily. Psyllium husk (Metamucil) is particularly effective because it adds bulk and draws water into the stool. Start with a low dose and increase gradually to avoid making bloating worse.
Hydration: Aim for 2.5 to 3 liters of water daily. This is more than most people drink normally, but slower gut transit means more water is reabsorbed from stool. You need to replace what your intestines are taking back.
Magnesium: Magnesium citrate or magnesium oxide at 200 to 400 mg daily has a mild osmotic laxative effect that counteracts semaglutide-induced constipation without harsh stimulant action. Many providers recommend this as a first-line intervention.
Fatigue management
Addressing fatigue on semaglutide requires distinguishing between medication effects and nutritional deficiency:
Protein priority: Aim for at least 60 to 80 grams of protein daily. When appetite is suppressed, protein tends to be the first macronutrient that gets underconsumed. Protein supplementation through shakes or bars can help when whole food intake is limited.
Caloric floors: Do not let daily caloric intake drop below 1,000 to 1,200 calories, even if appetite is minimal. Extreme caloric restriction during the adaptation period compounds fatigue and can trigger muscle loss and metabolic slowdown.
Sleep hygiene: Disrupted sleep from GI discomfort or insomnia amplifies fatigue. Prioritizing 7 to 8 hours of sleep and addressing any sleep-disrupting symptoms early is critical.
Vitamin B12 supplementation: Some evidence suggests that GLP-1 receptor agonists can reduce B12 absorption over time. A B12 supplement or methylcobalamin-containing compound can address potential deficiency-related fatigue.
The STEP trial data in detail
Understanding the clinical trial evidence gives you a realistic baseline for what to expect. The STEP (Semaglutide Treatment Effect in People with Obesity) trials represent the most comprehensive safety data available for semaglutide at the 2.4 mg weight loss dose.
Overall gastrointestinal adverse event rates
Across the STEP trials, 72.9% of participants receiving semaglutide 2.4 mg reported at least one gastrointestinal adverse event, compared to 47.1% on placebo. This means that while GI side effects are common on semaglutide, nearly half of placebo participants also reported them, which tells us that some of the reported symptoms are related to dietary changes and study participation rather than the medication itself.
The net medication-attributable GI event rate is roughly 25 to 30%, meaning about one in four people experience GI symptoms that would not have occurred without the medication.
Severity breakdown
Of all gastrointestinal adverse events reported in the semaglutide arm:
99.5% were non-serious
98.1% were mild to moderate in severity
4.1% experienced severe GI events (vs. 0.9% on placebo)
4.3% discontinued treatment due to GI events
These numbers are reassuring. The overwhelming majority of people who experience side effects are dealing with mild to moderate, transient symptoms that resolve with time and management. Severe events are rare, and treatment discontinuation due to side effects is uncommon.
Timing patterns from pooled data
The STEP trials pooled data reveals several important timing patterns:
The incidence of new-onset nausea was highest during the dose escalation period (weeks 1 to 20) and decreased substantially once participants reached maintenance dosing. After week 20, new cases of nausea were rare.
Diarrhea and vomiting followed similar patterns but with shorter individual episode durations. Abdominal distension and bloating peaked around weeks 8 to 12 and gradually improved.
Constipation was the most persistent symptom, with some participants reporting ongoing issues throughout the 68-week trial period. However, the severity typically decreased over time even when the symptom persisted.
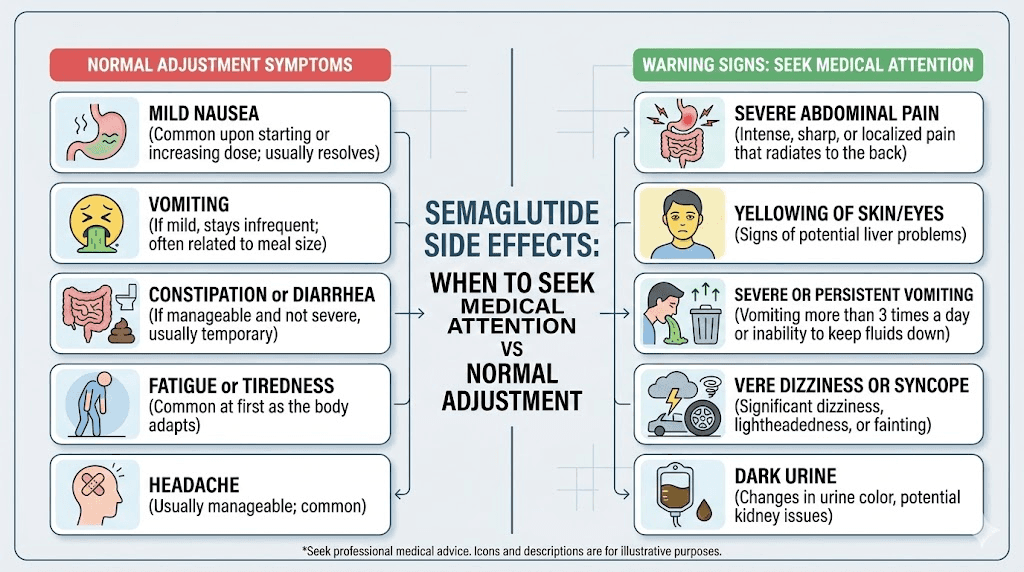
Serious side effects and when to seek medical attention
While the vast majority of semaglutide side effects are mild and self-limiting, certain symptoms require immediate medical evaluation. Knowing the difference between normal adjustment symptoms and red flags could be critically important.
Pancreatitis warning signs
Acute pancreatitis is a rare but serious potential complication. In clinical trials, the incidence was approximately 0.23% (3 out of 1,306 participants). The risk is low, but the condition requires emergency treatment.
Seek immediate medical attention if you experience:
Severe, persistent abdominal pain that radiates to the back
Abdominal pain that does not improve and is accompanied by nausea and vomiting
Pain that worsens after eating, particularly fatty foods
Fever combined with severe abdominal tenderness
If pancreatitis is suspected, semaglutide should be discontinued immediately and not restarted.
Gallbladder complications
GLP-1 receptor agonists are associated with a slightly increased risk of gallbladder disease, including gallstones and cholecystitis. The risk is related to rapid weight loss rather than the medication directly.
Watch for:
Sudden, intense pain in the upper right abdomen
Pain between the shoulder blades
Nausea and vomiting not related to meals
Yellowing of the skin or eyes (jaundice)
Thyroid concerns
Semaglutide carries a boxed warning about thyroid C-cell tumors based on animal studies. While human studies have not confirmed this risk, monitoring is recommended:
New lump or swelling in the neck
Difficulty swallowing or breathing
Persistent hoarseness
People with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should not use semaglutide.
Severe allergic reactions
Rare but possible. Symptoms include:
Swelling of the face, lips, tongue, or throat
Difficulty breathing or swallowing
Severe rash or hives
Rapid heartbeat
These require immediate emergency medical care. Call emergency services if any of these symptoms occur after injection.
Kidney problems
Severe dehydration from persistent vomiting and diarrhea can lead to acute kidney injury. If you are unable to keep fluids down for more than 24 hours, seek medical evaluation. Watch for:
Significantly decreased urine output
Dark-colored urine that does not improve with hydration
Swelling in the ankles or feet
Persistent fatigue with decreased urination
Semaglutide side effects compared to other GLP-1 medications
If you are considering semaglutide versus tirzepatide or evaluating other options, understanding how side effect profiles compare helps inform decision-making.
Side Effect | Semaglutide 2.4mg | Tirzepatide 15mg | Liraglutide 3.0mg |
|---|---|---|---|
Nausea | 43.9% | 24-33% | 39% |
Diarrhea | 29.7% | 18-25% | 21% |
Vomiting | 24.5% | 9-13% | 16% |
Constipation | 24.2% | 9-12% | 19% |
Discontinuation (GI) | 4.3% | 4-7% | 6.4% |
The data shows that semaglutide at the full weight loss dose has somewhat higher rates of nausea and vomiting compared to tirzepatide, though the comparison between semaglutide and tirzepatide side effects involves many variables beyond simple percentage comparisons. Tirzepatide, which acts on both GIP and GLP-1 receptors, appears to have a somewhat more favorable GI tolerability profile, possibly because GIP receptor activation partially counteracts the nausea-inducing effects of GLP-1 agonism.
For people who find semaglutide side effects intolerable, switching from semaglutide to tirzepatide is an option that some providers recommend. The side effect profile may differ enough to improve the experience, though individual responses vary.
Compounded semaglutide and side effect differences
Compounded semaglutide is prescribed by many providers as an alternative to brand-name formulations. The side effect profile is generally similar, but there are some considerations specific to compounded versions.
Compounded formulations may include additional ingredients like vitamin B12, glycine, or niacinamide as stabilizers or added benefits. These additional ingredients can occasionally introduce their own side effects. Niacinamide at higher doses can cause flushing. Glycine may cause mild GI symptoms in some people. B12 injections can occasionally cause injection site reactions.
The reconstitution process for compounded semaglutide also introduces a variable that brand-name formulations do not have. Incorrect reconstitution can lead to inconsistent dosing, which can make side effects unpredictable. Using a reconstitution calculator and following precise preparation protocols minimizes this risk.
Storage matters too. Compounded semaglutide shelf life depends on proper refrigeration and handling. Using degraded medication can alter both efficacy and side effect profile. If your semaglutide changes color or appearance, it may have degraded and should not be used.
What to do when side effects will not go away
For the 5 to 10% of people who experience persistent side effects beyond the typical adaptation period, there are several strategies worth discussing with a healthcare provider.
Dose reduction
Dropping back one dose level and maintaining there is the most common approach. Going from 2.4 mg back to 1.7 mg, for instance, often provides significant side effect relief while maintaining most of the weight loss benefit. Studies show that weight loss outcomes at 1.7 mg, while slightly lower than at 2.4 mg, are still clinically meaningful.
Extended dose intervals
Some providers experiment with extending the injection interval from weekly to every 10 days or even every 2 weeks. This is not part of the standard protocol and lacks robust clinical trial data, but anecdotal reports suggest it can improve tolerability for some patients. The trade-off is potentially reduced efficacy.
Switching medications
If semaglutide side effects remain unmanageable despite dose adjustments, switching to an alternative GLP-1 receptor agonist or to tirzepatide may be appropriate. Different medications in the same class can produce different side effect profiles in the same individual due to variations in receptor binding characteristics, half-life, and metabolism.
Adjunctive medications
For persistent nausea, prescription antiemetics like ondansetron can be used on a scheduled basis rather than as-needed. For persistent constipation, prescription-strength options like linaclotide or lubiprostone may be necessary when over-the-counter solutions are insufficient.
SeekPeptides members gain access to comprehensive troubleshooting guides that cover these scenarios in detail, along with community insights from experienced researchers who have navigated similar challenges.
Oral semaglutide versus injectable: do side effects differ
The oral formulation (Rybelsus) and the injectable formulations (Ozempic, Wegovy) contain the same active molecule, but the delivery method creates some differences in the side effect experience.
Oral semaglutide must be taken on an empty stomach with no more than 4 ounces of water, then you must wait at least 30 minutes before eating, drinking, or taking other medications. This requirement itself can affect side effects, as taking the tablet with food or too much water reduces absorption and can alter the side effect profile.
The onset of side effects with oral semaglutide tends to be slightly more gradual because absorption from the GI tract is less complete than from subcutaneous injection. Bioavailability of oral semaglutide is approximately 1% compared to injectable formulations, which is why oral doses are measured in milligrams (3, 7, 14 mg) rather than the microgram-range doses used for injection.
GI side effects with oral semaglutide are reported at similar rates to injectable formulations, though some users report that nausea is more meal-dependent with the oral form. The stomach-empty requirement means the medication is present in the GI tract during the absorption phase, which can cause localized irritation that injectable forms avoid.
Your first week on semaglutide: what to realistically expect
The first week on semaglutide sets the tone for the entire treatment course. Knowing what is normal prevents unnecessary anxiety.
Day 1 (injection day): You will likely feel nothing different. The injection itself is a small subcutaneous injection, usually in the abdomen or thigh. The injection site may have minor redness or tenderness. That is it.
Day 2: Semaglutide is reaching peak plasma concentration. Some people notice a slight decrease in appetite. Others notice nothing. Mild nausea is possible but not universal.
Day 3: If you are going to experience nausea at the 0.25 mg dose, it usually appears by now. It is typically mild, more of a subtle queasiness than active nausea. Appetite reduction becomes more noticeable.
Days 4 to 5: Nausea, if present, often peaks and then begins to ease. Some people report feeling slightly more tired than usual. Burping or belching may increase as gastric emptying patterns shift.
Days 6 to 7: Symptoms typically stabilize or begin improving. Appetite may feel noticeably different, with less interest in snacking and smaller portions feeling satisfying. This is the medication beginning to establish its effects.
How semaglutide makes you feel in the first week is not necessarily how it will make you feel long-term. The first week is the mildest dose, and many people report that the initial adjustment is surprisingly easy. The bigger test comes with the first dose increase.
The relationship between side effects and weight loss
Here is something the STEP trials revealed that surprises many people: the severity of side effects does not predict the amount of weight loss.
Participants who experienced significant nausea did not lose more weight than those with minimal side effects. The weight loss from semaglutide comes primarily from reduced appetite and altered food preferences through central nervous system pathways, not from feeling too nauseous to eat.
In fact, participants who managed their side effects well and maintained adequate nutrition actually tended to have better long-term outcomes than those whose side effects led to extremely low caloric intake. Severe caloric restriction triggers metabolic adaptation (reduced resting metabolic rate), muscle loss, and nutritional deficiencies that can undermine sustained weight loss.
The take-home message: do not view side effects as the mechanism of weight loss. View them as an adjustment period to get through, not lean into. The goal is to find the dose that provides effective appetite reduction and metabolic benefit with manageable or absent side effects. That is the sustainable path.
If you hit 4 weeks on semaglutide with no weight loss, the solution is almost never to increase the dose until side effects force caloric restriction. The solution is to evaluate dietary patterns, activity levels, and metabolic factors that may be counteracting the medication.
Special populations and side effect considerations
Women
Women report higher rates of nausea and vomiting compared to men in the STEP trials, though the overall weight loss outcomes are similar. Hormonal fluctuations during the menstrual cycle can influence GI symptoms, with some women noticing that semaglutide side effects are worse during certain phases of their cycle. Semaglutide can also affect menstrual patterns, causing irregular or heavier periods in some women, likely related to hormonal changes that accompany significant weight loss.
Older adults
People over 65 may be more susceptible to dehydration from GI side effects, and the consequences of dehydration (falls, kidney injury, confusion) are more serious in older populations. Slower dose escalation and more aggressive hydration monitoring are recommended for older adults starting semaglutide.
People with diabetes
When semaglutide is used alongside other diabetes medications, particularly insulin or sulfonylureas, the risk of hypoglycemia (low blood sugar) increases. Symptoms of hypoglycemia, including dizziness, shakiness, sweating, and confusion, can overlap with semaglutide side effects, making it important to monitor blood glucose regularly during the adjustment period.
What happens to side effects if you stop and restart semaglutide
If you stop semaglutide for any reason, whether due to surgery, supply issues, or personal choice, restarting semaglutide requires going through the dose escalation process again. You cannot resume at your previous dose.
The body loses its GLP-1 receptor adaptation within weeks of discontinuation. Semaglutide withdrawal itself can cause its own set of symptoms, including appetite rebound, temporary weight regain, and changes in GI function as the body readjusts to normal gastric emptying speed.
When restarting, the side effect experience during the second round of dose escalation is usually milder than the first. The body retains some degree of metabolic memory, and adaptation tends to happen faster. Most providers recommend restarting at 0.25 mg and escalating on the standard or slightly accelerated schedule, depending on how long the interruption lasted.
For interruptions of 2 weeks or less at the same dose level, many providers consider it safe to resume at the same dose without re-escalation. For interruptions longer than 2 weeks, restarting from a lower dose is the safer approach.
Long-term side effects: what the extended data shows
The STEP trials ran for 68 weeks, and extension studies have provided data out to 2 years. The long-term safety profile is generally reassuring.
GI side effects: Continue to decrease over time. Most participants who experience GI symptoms during the first 20 weeks report minimal or no symptoms by month 12.
Weight stability: Side effects do not tend to increase over time on a stable dose. Once the body has adapted, it stays adapted.
Nutritional status: Long-term semaglutide use requires attention to nutritional adequacy. Reduced appetite and food intake over months to years can lead to deficiencies in protein, iron, calcium, vitamin D, and B vitamins. Regular nutritional monitoring and supplementation where indicated is recommended for anyone on semaglutide long-term.
Bone health: Rapid weight loss from any cause can reduce bone density. Ensuring adequate calcium and vitamin D intake, along with weight-bearing exercise, helps mitigate this risk.
Muscle mass: Preserving muscle mass during GLP-1 mediated weight loss requires deliberate attention to protein intake and resistance training. The side effect of reduced appetite makes it easy to undereat protein, which accelerates muscle loss during weight reduction.
For researchers serious about optimizing their GLP-1 protocols while managing side effects effectively, SeekPeptides offers evidence-based guides, community support from experienced users, and comprehensive protocol databases that address exactly these long-term considerations.
Frequently asked questions
How quickly do semaglutide side effects start after the first injection?
Most people notice the first side effects within 24 to 72 hours of their initial injection, coinciding with peak plasma concentration. However, at the 0.25 mg starting dose, many people experience no noticeable side effects during the entire first month. The most common early symptom is subtle appetite reduction rather than nausea.
Do side effects get worse with each dose increase?
Side effects typically return briefly with each dose increase but become less intense and shorter in duration with each subsequent escalation. The most challenging transition for most people is the jump from 0.25 mg to 0.5 mg because it is the first time the body encounters a dose that significantly affects gastric emptying. Later dose increases build on existing tolerance.
Can I take semaglutide at a different time to reduce side effects?
Yes. The time of day you inject semaglutide can influence side effect severity. Evening injections allow some people to sleep through the initial nausea peak. The medication is given once weekly on the same day, but you can change the day of the week if needed (by adjusting the interval between doses).
Will drinking alcohol make side effects worse?
Alcohol and semaglutide can be a problematic combination. Alcohol irritates the GI tract and can worsen nausea, and semaglutide-induced changes in gastric emptying may cause alcohol to be absorbed differently. Many users find their alcohol tolerance decreases significantly on semaglutide. Moderation or abstinence during the adjustment period is advisable.
Are compounded semaglutide side effects different from brand-name?
The active molecule is the same, so the core side effect profile is similar. However, compounded formulations may contain different inactive ingredients that can cause additional reactions in some people. Proper reconstitution and storage are essential to consistent dosing and predictable side effect patterns.
Should I eat before or after my semaglutide injection?
For injectable semaglutide, timing relative to meals does not significantly affect absorption or side effects. However, having a light meal a few hours before injecting can provide a baseline of food in the stomach that reduces the intensity of nausea the following day. Avoid large, heavy meals on injection day.
What if I have no side effects at all on semaglutide?
Having no side effects does not mean the medication is not working. Many people experience effective appetite reduction and weight loss without any GI symptoms. The mechanism of weight loss is primarily through central appetite suppression, not through causing nausea. Check typical one-month results to benchmark your progress.
How long should I wait before deciding semaglutide side effects are too much?
Give each dose level at least 3 to 4 weeks before making a decision about tolerability. Side effects that feel overwhelming in the first week often become manageable by week 3. If side effects remain severe after 4 weeks at any dose level, discuss dose adjustment with your provider rather than discontinuing entirely.
External resources
For researchers committed to understanding and managing their GLP-1 protocols with precision, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, personalized protocol tools, and a community of thousands who have navigated these exact questions successfully.
In case I do not see you, good afternoon, good evening, and good night. May your side effects stay mild, your adaptation stay swift, and your protocols stay informed.