Feb 26, 2026

You stopped semaglutide three months ago. Maybe insurance lapsed. Maybe the nausea was unbearable. Maybe life simply got in the way, and those weekly injections slipped off the priority list. Whatever the reason, you are here now, staring at the scale, watching numbers climb, feeling that familiar frustration settle in your chest.
You are not alone in this.
Millions of people stop semaglutide every year, and the vast majority want to restart. The STEP 1 trial extension showed that participants regained two-thirds of their prior weight loss within one year of stopping. That is not a failure of willpower. That is biology doing exactly what biology does when you remove a GLP-1 receptor agonist from the equation. The good news is that restarting is absolutely possible, safe when done correctly, and often just as effective as the first time around. But there is a catch. You cannot simply pick up where you left off. Your body has changed during those three months. The tolerance you built is gone. The appetite suppression you relied on has faded. And if you jump back to your previous dose, you are setting yourself up for the worst gastrointestinal experience of your life. This guide covers everything you need to know about restarting semaglutide after a 3-month break, from the exact dosing protocol to side effect management, dietary strategies, and long-term planning so this restart actually sticks.
What happens to your body during 3 months without semaglutide
Understanding what changed inside your body during those three months is the first step toward a safe restart. Semaglutide is not a vitamin you skip for a while and pick back up without consequence. It is a powerful GLP-1 receptor agonist that fundamentally alters how your brain and gut communicate about hunger, satiety, and food reward.
When you stop, those systems revert.
The pharmacokinetic reality
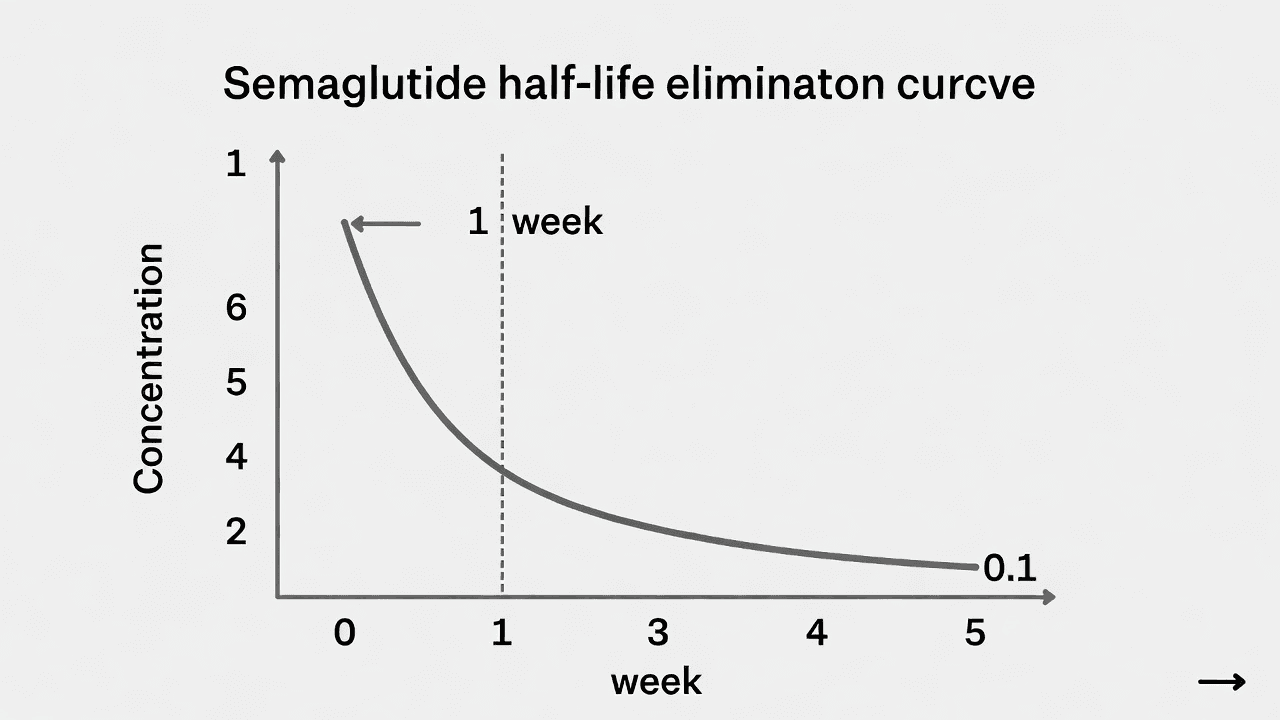
Semaglutide has a half-life of approximately one week. That means after your last injection, half the medication is still circulating seven days later. After two weeks, roughly a quarter remains. By five weeks, the drug has been essentially eliminated from your system entirely.
At the three-month mark, you have been completely without semaglutide for roughly seven weeks. Your GLP-1 receptors, which had adapted to a steady stream of the medication, have returned to baseline functioning. The downstream effects that made weight loss feel almost effortless, the reduced appetite, the slower gastric emptying, the diminished food noise, all of those are gone. Your body is operating as if semaglutide never existed.
Appetite and hunger signals return
This is the change people notice most. That quiet mind, the one that could walk past a bakery without a second thought, gets loud again. The appetite suppression that semaglutide provides works through multiple pathways. It slows gastric emptying so food stays in the stomach longer. It acts on hypothalamic neurons that regulate hunger. It reduces the reward value of highly palatable foods.
All of that reverses within weeks of stopping.
Research shows that hunger hormones rebound relatively quickly after discontinuation. Ghrelin levels, which semaglutide had been keeping low, rise back to pre-treatment levels. Leptin sensitivity, which had improved, begins to deteriorate again. Your brain starts sending the same hunger signals it sent before you ever started treatment, except now you have less body mass, which means your body perceives a caloric deficit and pushes even harder for you to eat.
Gastrointestinal tolerance resets completely
This matters enormously for your restart plan. When you first started semaglutide, your body needed time to adjust to the slower gastric emptying and altered gut motility. That is why the standard protocol begins at 0.25 mg and titrates up gradually over months. Your GI system built tolerance progressively.
Three months off erases all of that tolerance. Your stomach and intestines have returned to normal processing speeds. If you were to inject your previous maintenance dose, say 1.0 mg or 2.4 mg, into a body with zero tolerance, the result would be extreme. Severe nausea. Vomiting that can last days. Diarrhea. Potential dehydration. Some people who skip titration end up in urgent care. It is not worth the risk, and it is entirely preventable by following a proper dosing protocol.
Metabolic adaptation and set point defense
Your body has what researchers call a defended body weight, a range it tries to maintain through metabolic adjustments. When you lost weight on semaglutide, your body was constantly trying to return to its previous set point. The medication overrode those defenses. Without it, your metabolism slows slightly, your hunger increases significantly, and your body becomes remarkably efficient at storing calories as fat. This is not a character flaw. It is an evolutionary survival mechanism that kept our ancestors alive during famines. Understanding this helps remove the shame many people feel about weight regain after stopping treatment.
Weight regain reality: what the clinical data shows
Before diving into restart protocols, you need to understand what the research says about weight regain after stopping semaglutide. Not to discourage you. To prepare you. Knowledge is the difference between panic and a plan.
The STEP 1 trial extension
The most cited data comes from the STEP 1 trial extension, published in Diabetes, Obesity and Metabolism. The original STEP 1 trial randomized 1,961 adults with obesity to receive either semaglutide 2.4 mg or placebo for 68 weeks alongside lifestyle intervention. Participants on semaglutide lost an average of 17.3% of their body weight.
Then they stopped.
The extension followed 327 participants for an additional year after discontinuation. The results were striking. Semaglutide participants regained an average of two-thirds of their prior weight loss during that off-treatment year. Weight regain continued throughout the entire follow-up period without plateauing, and cardiometabolic improvements that had occurred during treatment also reversed partially.
That two-thirds number gets repeated often because it is both alarming and informative. But context matters.
Real-world data tells a more nuanced story
Clinical trials represent controlled environments with specific populations. Real-world data, published by Epic Research, paints a somewhat different picture. Their analysis of actual patients found that two years after stopping GLP-1 treatment, most patients had sustained at least some of their weight loss. Complete weight regain occurred in only 23% of semaglutide users at 24 months. That means 77% of people kept at least some of their results, even without the medication.
Why the difference? Real-world patients often maintain some of the behavioral changes they developed during treatment. They eat smaller portions. They choose different foods. They exercise more consistently. The dietary habits they built while on semaglutide do not vanish overnight, even if the pharmacological appetite suppression does.
The rate of weight regain
A 2025 narrative review in the Journal of Clinical Medicine examined weight regain trajectories across multiple GLP-1 receptor agonist studies. The average rate of regain for semaglutide and tirzepatide was approximately 0.8 kg (about 1.8 pounds) per month after discontinuation. At that rate, projections suggest a return to baseline weight by roughly 18 months, though individual variation is enormous.
A separate study from the University of Oxford, published in early 2026, found that weight regain after stopping GLP-1 medications was approximately 0.3 kg per month faster than weight regain after ending behavioral weight loss programs alone. This suggests that pharmaceutical weight loss creates a somewhat steeper rebound trajectory compared to lifestyle-only approaches, reinforcing the importance of maintaining strong nutritional foundations regardless of medication status.
What this means for your restart
Here is the takeaway. If you stopped semaglutide three months ago and have regained some weight, that is normal. Expected. Predicted by every major clinical trial. The question is not whether regain happens. It does. The question is what you do about it. Restarting semaglutide is a legitimate, evidence-based response to weight regain, and the data suggests you can expect similar efficacy the second time around. Most healthcare providers now view obesity as a chronic condition requiring ongoing management, similar to hypertension or metabolic dysfunction. Restarting treatment is not a failure. It is standard medical practice.
The complete restart dosing protocol
This is the section that matters most. The exact protocol you follow when restarting semaglutide after a 3-month break determines whether your experience is smooth or miserable. There is no ambiguity here. The guidance from manufacturers, clinical pharmacologists, and experienced prescribers all converge on the same recommendation.
The fundamental rule: start from the beginning
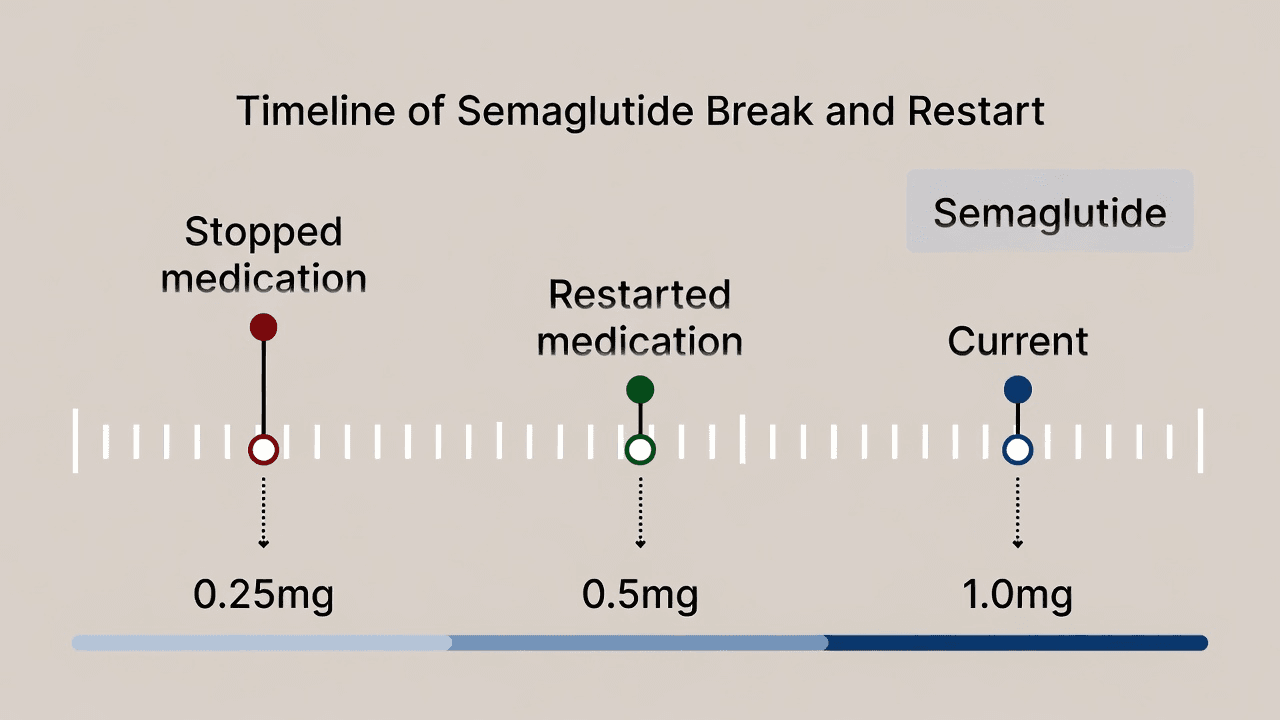
After three months off semaglutide, you must restart at the lowest dose. Period.
For branded Wegovy, that means 0.25 mg weekly. For branded Ozempic, that also means 0.25 mg weekly. For compounded semaglutide, that typically means the lowest available concentration at the starting volume your provider recommends.
This is non-negotiable. Your body has zero tolerance to the drug. The GLP-1 receptors in your gut, brain, and pancreas have fully desensitized. Injecting 1.0 mg or 2.4 mg into a body with no tolerance is like running a marathon with no training. The mechanism still works. But the side effects will be overwhelming.
Duration-based restart guidelines
Different break lengths require different approaches. Here is what clinical practice guidelines suggest based on how long you have been off semaglutide:
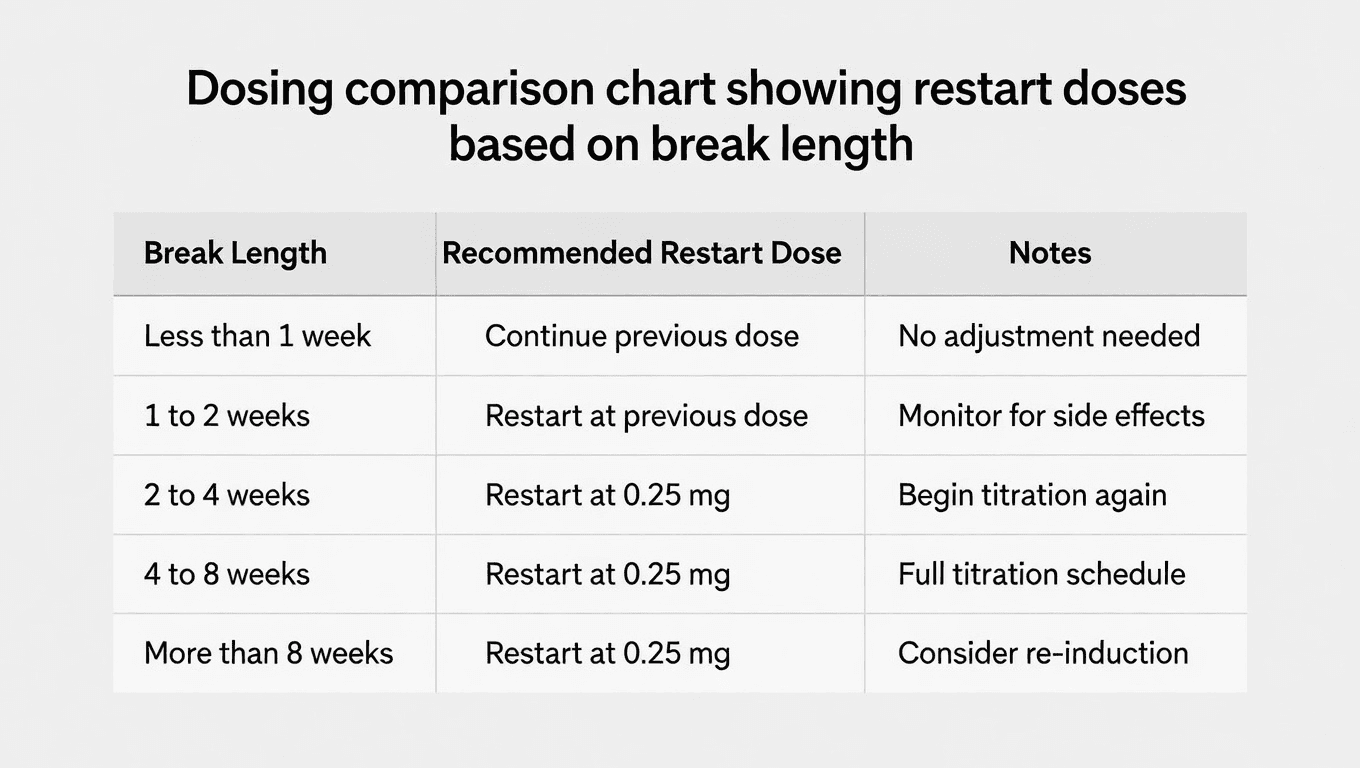
Break of 2 weeks or less: You can generally resume at your previous dose. The drug has not fully cleared, and your tolerance is largely intact. If you missed a dose by fewer than 5 days, simply take it when you remember and resume your regular schedule.
Break of 3 to 4 weeks: Consider dropping one dose level. If you were on 1.0 mg, restart at 0.5 mg. If you were on 0.5 mg, restart at 0.25 mg. Monitor for GI symptoms and titrate back up after 2-4 weeks if tolerated.
Break of 5 weeks or more (including 3 months): Restart at the lowest dose, 0.25 mg weekly. Follow the full titration schedule as if starting for the first time. Your body needs the same gradual adjustment period it needed originally.
Working with your healthcare provider
Before restarting, schedule a visit with the provider who prescribed your semaglutide. They may want to check your current weight, A1C levels if applicable, kidney and liver function, and thyroid markers. They will also review what caused you to stop and help you address those factors so this round of treatment lasts longer.
If you are using compounded semaglutide from a compounding pharmacy, confirm that your product has not expired during your break. Compounded formulations have variable stability depending on the formulation, and proper storage is essential for both safety and efficacy. If you have leftover vials from before your break, check expiration dates carefully. Using expired semaglutide can mean reduced potency at best and safety concerns at worst.
Week-by-week titration schedule for restarting
Here is your complete roadmap from restart to maintenance dose. This schedule follows the standard Wegovy titration protocol, which is the most commonly referenced for weight management. If you are using Ozempic or compounded formulations, the principles are identical even if the specific doses differ slightly.
The standard restart titration
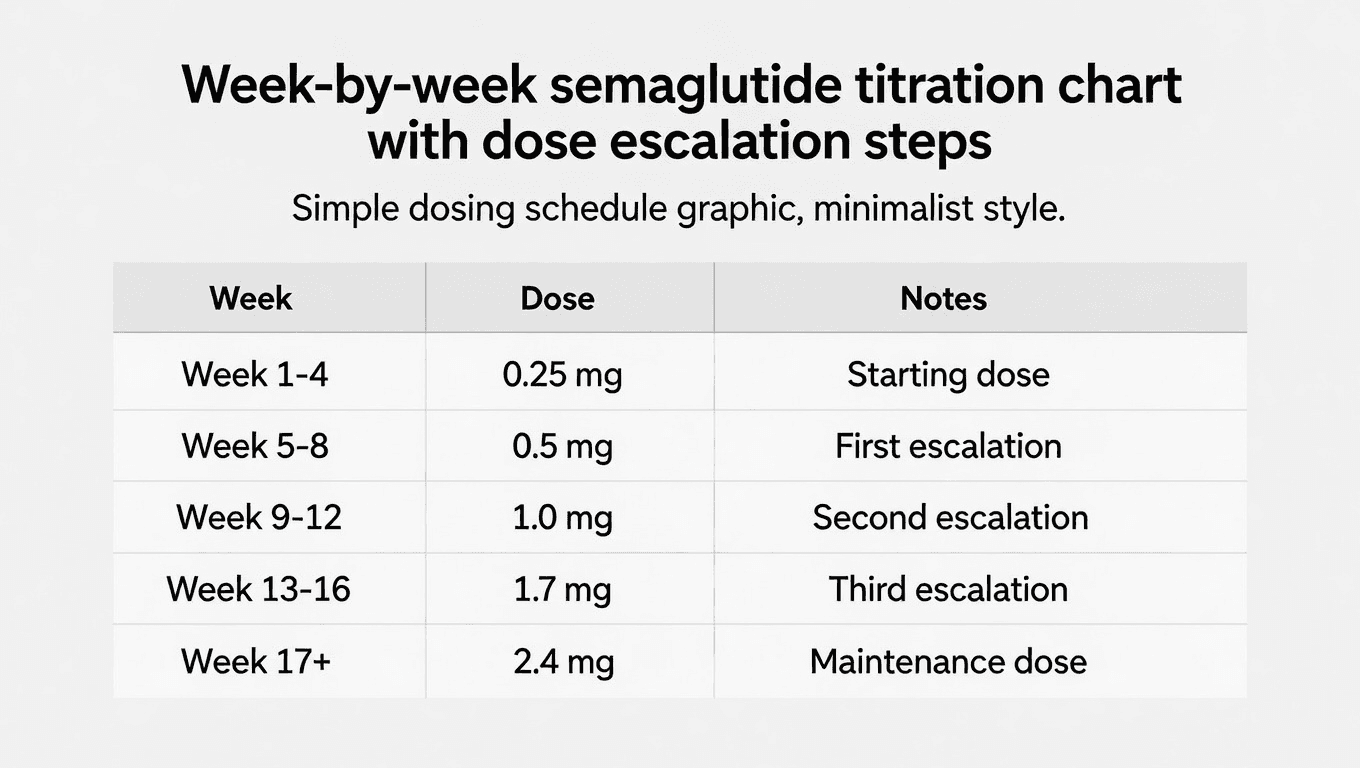
Weeks 1 through 4: 0.25 mg once weekly
This is your re-introduction phase. The dose is intentionally sub-therapeutic for weight loss. Its purpose is to let your GI system readjust to delayed gastric emptying. You may notice mild appetite reduction, but do not expect significant weight changes yet. Some people feel nothing at this dose. That is fine. The 0.25 mg is building the foundation for higher doses. Use our semaglutide dosage calculator to verify your exact units based on concentration.
Weeks 5 through 8: 0.5 mg once weekly
Your first dose increase. This is where most people begin to notice appetite suppression returning. Food noise quiets down. Portions naturally decrease. GI side effects may intensify briefly after the increase, particularly nausea in the first 2-3 days after injection. This typically resolves within the first week at the new dose. If you are using a 5 mg/mL concentration, double-check your unit calculations carefully at this stage.
Weeks 9 through 12: 1.0 mg once weekly
The first truly therapeutic dose for most people. Weight loss typically accelerates during this phase. You should be experiencing consistent appetite reduction, meaningful changes in food preferences, and early scale movement. Monitor for any new side effects and report them to your provider. If GI symptoms are manageable, continue at this dose for the full four weeks before considering the next increase.
Weeks 13 through 16: 1.7 mg once weekly
A significant jump that many people find effective as a maintenance dose. The appetite suppression at 1.7 mg is substantial. If you are tolerating this dose well and losing weight consistently, your provider may recommend staying here rather than pushing to the maximum. There is no rule that says you must reach the highest dose. Effective treatment happens at whatever dose produces results with tolerable side effects.
Weeks 17 and beyond: 2.4 mg once weekly
The maximum approved dose for Wegovy. Not everyone needs to reach this level. If 1.0 mg or 1.7 mg is working, there is no benefit to pushing higher just for the sake of it. Higher doses come with more pronounced GI side effects, and the incremental weight loss benefit diminishes at each step up.
Compounded semaglutide restart considerations
If you are using compounded semaglutide, your titration may look slightly different depending on the concentration of your formulation. Common compounded concentrations include 2.5 mg/mL and 5 mg/mL. The principles remain identical: start low, increase gradually, and let your body adjust before moving up.
Work with your prescriber to determine the equivalent starting dose. If you need to reconstitute your semaglutide, follow sterile technique precisely. Use our peptide reconstitution calculator to get exact measurements based on your vial concentration. Measure carefully using an insulin syringe, and refer to our guides on mixing with bacteriostatic water for proper dilution ratios. If you have a 5 mg vial, the reconstitution math is different from a 10 mg vial, so double-check before drawing your dose.
Signs you are ready to increase your dose
Do not increase simply because four weeks have passed. Increase when all of these conditions are true: your GI symptoms at the current dose have resolved or become minimal, you are not experiencing persistent nausea or vomiting, you feel comfortable with the current level of appetite suppression, and your provider has approved the increase. If you are unsure, stay at your current dose for an additional 1-2 weeks. There is no penalty for a slower titration. There is, however, a real penalty for escalating too quickly.
Can you titrate faster the second time
Some providers allow a slightly compressed titration for patients restarting, particularly if the original titration was well-tolerated. This might mean spending 2-3 weeks at each dose level instead of 4 weeks. However, this should only happen under medical supervision. Self-adjusting your titration speed based on how you feel is risky, because side effects from GLP-1 receptor agonists sometimes appear with a delay. You might feel fine for three days and then get hit with severe nausea on day four.
Managing side effects when you restart
Here is the honest truth about restarting semaglutide: the side effects will probably come back. Not as a punishment. As a predictable, manageable, temporary response to a medication your body is no longer accustomed to. The good news is that you have been through this before, and this time you know what to expect.
What to expect in the first two weeks
The most common side effects upon restarting mirror what you experienced when you first started. Nausea leads the list, affecting 40-44% of patients in clinical trials. It typically peaks in the first 2-3 days after each injection and gradually diminishes over the following days. Most nausea episodes last an average of eight days, though individual experiences vary widely.
Other common GI effects include diarrhea (affecting roughly 30% of patients), constipation (occurring in about 24%), and general abdominal discomfort. Some people experience fatigue in the first few weeks. Others report changes in energy levels that fluctuate before stabilizing. A smaller percentage experience headache, dizziness, or changes in taste. These side effects are almost always temporary and dose-dependent.
Nausea management strategies that actually work
Dietary approaches:
Eat smaller, more frequent meals instead of three large ones. Five to six mini-meals spread throughout the day keep your stomach from overfilling while maintaining steady nutrition. Avoid high-fat, greasy, and heavily seasoned foods during the first few weeks at each new dose level. Fat slows digestion, and when combined with semaglutide-induced delayed gastric emptying, the result is prolonged nausea that can last hours. Focus on bland, easily digestible foods: plain grains, lean proteins, steamed vegetables, and broth-based soups. For a comprehensive approach to eating during treatment, review our guide on foods to eat while on semaglutide.
Timing and behavioral strategies:
Stay upright for at least 30 minutes after eating. Lying down immediately after a meal worsens nausea because gravity is no longer helping move food through your GI tract. Eat slowly. Put your fork down between bites. Stop eating at the first sign of fullness, not when your plate is empty. Some people find that injecting in the evening, rather than the morning, allows them to sleep through the worst of the initial nausea. Experiment with injection timing to find what works for you.
Over-the-counter remedies:
Ginger, in any form, is remarkably effective for GLP-1-related nausea. Ginger tea, ginger chews, ginger capsules, and even flat ginger ale can help. Bismuth subsalicylate (Pepto-Bismol) addresses both nausea and diarrhea. Dimenhydrinate (Dramamine) works for some people, though it can cause drowsiness. Peppermint tea or peppermint oil capsules can also soothe an upset stomach.
Prescription options:
If nausea is severe enough to interfere with daily functioning, ask your provider about ondansetron (Zofran). It is commonly prescribed alongside GLP-1 receptor agonists for patients who struggle with GI symptoms. Metoclopramide is another option, though it carries more potential side effects and is typically reserved for more persistent cases.
Constipation management
Semaglutide slows gut motility, and constipation is one of the most persistent side effects. Stay hydrated aggressively, aiming for at least 64 ounces of water daily. Add fiber gradually through vegetables, chia seeds, and psyllium husk. Magnesium citrate at bedtime (200-400 mg) can help keep things moving. If these measures are insufficient, over-the-counter osmotic laxatives like polyethylene glycol (MiraLAX) are safe for ongoing use and will not create dependence.
When to contact your provider
Most restart side effects are unpleasant but not dangerous. However, contact your healthcare provider immediately if you experience vomiting that persists for more than 24 hours, signs of dehydration (dark urine, dizziness, rapid heartbeat), severe abdominal pain (especially pain that radiates to your back, which could indicate pancreatitis), or any allergic reaction symptoms like swelling, rash, or difficulty breathing.
Diet and nutrition strategies during your restart
What you eat during your restart matters just as much as the medication itself. Your dietary choices during the first 8-12 weeks of retitration directly influence both the severity of your side effects and the speed of your weight loss results. Many people who had success on semaglutide the first time find that being more intentional about nutrition the second time around produces even better outcomes.
The protein-first approach
Protein is your highest priority during a semaglutide restart. Here is why. Semaglutide reduces overall appetite, which means you eat less of everything. Without deliberate effort, protein intake drops along with total calories, and that leads to muscle loss rather than primarily fat loss. During your restart, aim for 0.7-1.0 grams of protein per pound of your goal body weight daily. At every meal, eat protein first before moving to other foods. Lean chicken, fish, eggs, Greek yogurt, cottage cheese, and legumes should form the foundation of every plate.
For a detailed guide on building meals during GLP-1 treatment, review our semaglutide diet plan. Planning meals in advance is critical during the restart phase because reduced appetite can make it tempting to skip meals entirely, which leads to inadequate protein and nutritional deficiencies over time.
Foods that minimize GI distress
During the first weeks at each new dose level, stick to foods that are gentle on the stomach. Oatmeal, bananas, rice, toast, and baked potatoes are easily digestible and unlikely to trigger nausea. Broth-based soups provide hydration and nutrition simultaneously. Scrambled eggs offer high-quality protein without stressing the digestive system. Avoid raw vegetables, high-fiber foods, and large salads until your gut has adjusted to the new dose level. These are healthy foods in general, but during active titration, they can worsen bloating and discomfort.
Foods to avoid during restart
Certain foods are particularly problematic during semaglutide retitration. Fried and high-fat foods top the list because they dramatically slow digestion on top of the medication-induced delay. Carbonated beverages create gas and bloating in a gut that is already processing slowly. Very spicy foods can irritate an already-sensitive stomach lining. Large volumes of raw cruciferous vegetables (broccoli, cauliflower, Brussels sprouts) produce gas that compounds discomfort. Sugary foods and refined carbohydrates can cause blood sugar fluctuations that worsen nausea. For a complete breakdown of what to avoid, see our guide on foods to avoid during GLP-1 treatment, which applies equally to semaglutide.
Hydration is non-negotiable
This cannot be overstated. Semaglutide-related nausea, vomiting, and diarrhea all contribute to fluid loss. Dehydration worsens every single side effect and creates new ones like headache, dizziness, and constipation. Aim for at least 64-80 ounces of water daily. Sip throughout the day rather than drinking large amounts at once. Avoid drinking large volumes during meals, as this fills your stomach and worsens early satiety and nausea. Instead, hydrate between meals.
Supplements worth considering
Several supplements can support your restart. A high-quality multivitamin covers potential nutritional gaps from reduced food intake. Vitamin B12 is especially important, as GLP-1 receptor agonists may reduce B12 absorption over time, and combining semaglutide with B12 supplementation is increasingly recommended by providers. Some formulations even include B12 directly in the compound. Glycine supplementation has gained attention for potential benefits in supporting metabolic health during GLP-1 treatment. Methylcobalamin, the active form of B12, is preferred over cyanocobalamin for better absorption. Magnesium citrate helps with constipation and muscle function. Protein powder can help you meet daily protein targets when solid food is difficult to tolerate.
Exercise and physical activity during your restart
Exercise is the other half of the equation that separates people who maintain their results from people who end up in a cycle of starting and stopping. During your restart, physical activity is not optional. It is essential for preserving muscle mass, supporting metabolic health, and maximizing the effectiveness of the medication.
Resistance training is your top priority
This might surprise people who think cardio is king for weight loss. When semaglutide reduces your caloric intake, your body needs a reason to keep muscle. Resistance training provides that reason. Without it, a significant portion of your weight loss comes from lean mass rather than fat, which slows your metabolism and makes future weight regain even more likely. Aim for at least two to three resistance training sessions per week. Focus on compound movements: squats, deadlifts, bench press, rows, and overhead press. These exercises recruit the most muscle mass per movement and provide the strongest stimulus for muscle preservation. If you are new to resistance training, start with bodyweight exercises or machines and work with a trainer to learn proper form.
Cardio and general activity
Current guidelines recommend at least 150 minutes of moderate-intensity aerobic activity per week. Walking is the most accessible option and can be started immediately regardless of fitness level. Aim for 30 minutes of brisk walking most days. As your fitness improves, consider adding cycling, swimming, or other low-impact activities. High-intensity interval training (HIIT) can be effective but may worsen nausea during the early restart phase. Save intense cardio for after you have settled into a stable dose. Beyond structured exercise, increase your non-exercise activity thermogenesis (NEAT): take the stairs, park farther away, stand while working, and walk during phone calls. These small increases in daily movement add up to significant caloric expenditure over time, supporting the fat loss process without requiring dedicated gym time.
Timing exercise around injections
Many people find that GI side effects peak in the 24-48 hours after injection. Plan your more intense workouts for days 3-7 after your injection, when side effects are typically at their lowest. Lighter activity like walking is fine at any point. If nausea is an issue during exercise, keep the intensity moderate and avoid exercises that involve lying face down or significant abdominal compression.
Common restart mistakes and how to avoid them
Having worked with thousands of people navigating semaglutide treatment, certain mistakes appear over and over. Learn from others so you do not have to learn the hard way.
Mistake 1: jumping straight to your old dose
This is the most dangerous and most common mistake. Someone was on 1.0 mg, stopped for three months, and figures they can just resume at 1.0 mg because that is what they were taking before. The result is predictable and unpleasant: severe nausea, vomiting, diarrhea, and potential dehydration. In some cases, people who did this ended up in urgent care with dehydration so severe they needed IV fluids. Always restart at 0.25 mg regardless of your previous dose. Your body does not remember its tolerance after three months.
Mistake 2: treating the restart like a new beginning instead of a continuation
Some people approach their restart with all-or-nothing thinking. They try to overhaul their entire diet, start an intense exercise program, and restart semaglutide all at once. This creates too many variables and too much stress. Instead, restart the medication first. Let your body adjust for 2-3 weeks. Then gradually reintroduce dietary changes. Then layer in exercise. Sequential changes are sustainable. Simultaneous overhauls are not.
Mistake 3: not addressing why you stopped
If you stopped because of side effects, and you do not have a plan for managing those same side effects this time, you are setting yourself up to stop again. If you stopped because of cost, have you resolved the financial barriers? If you stopped because of supply issues, is your supply chain now reliable? If you are using compounded GLP-1 medications, confirm that your pharmacy has consistent stock. Address the root cause or the cycle repeats.
Mistake 4: comparing the restart to the first time
Your body is different now than it was when you first started semaglutide. You may have more or less body fat. Your hormonal profile may have shifted. Your metabolic rate may be different. Some people find the restart easier because they know what to expect. Others find it harder because the novelty has worn off and the side effects feel more frustrating the second time. Avoid comparing timeline, side effects, or rate of loss to your first round. Treat this as its own experience.
Mistake 5: giving up too soon
The first four weeks at 0.25 mg can feel pointless. You are experiencing side effects but not seeing scale changes. This is where patience becomes critical. The sub-therapeutic starting dose exists for a reason. Trust the process. Results will come once you reach higher doses, but only if you build the GI tolerance foundation first. If you are feeling frustrated by early progress, read about the typical timeline for results to calibrate your expectations properly.
Mistake 6: neglecting protein intake
Reduced appetite means reduced food intake, and most people unconsciously cut protein disproportionately because carbohydrates and fats are easier to consume in small amounts. The consequence is accelerated muscle loss, which reduces your basal metabolic rate and makes future weight management harder. Track your protein for at least the first month of your restart to ensure you are hitting your targets.
Should you restart semaglutide or switch to something else
A 3-month break is a natural inflection point for reconsidering your treatment approach. Maybe semaglutide was not quite right for you the first time. Maybe newer options have become available. Here is how to think through the decision.
When restarting semaglutide makes sense
Restarting the same medication is usually the best choice if semaglutide worked well for you the first time (meaningful weight loss with tolerable side effects), if you stopped for reasons unrelated to the medication itself (cost, supply, scheduling), if your insurance or provider still covers semaglutide, and if you have no new medical contraindications. In these cases, you already know the medication works in your body. That information is valuable. Switching to an unknown introduces uncertainty when you have a proven option available.
When switching to tirzepatide might make sense
Tirzepatide (brand name Mounjaro/Zepbound) is a dual GIP/GLP-1 receptor agonist that has shown greater weight loss than semaglutide in head-to-head trials. Consider switching if semaglutide produced only modest results, if you plateaued at a weight that was far from your goal, if side effects with semaglutide were severe and you are hoping for a different side effect profile, or if your provider recommends it based on your specific metabolic profile.
If you are considering the switch, our semaglutide to tirzepatide conversion chart can help you and your provider determine the appropriate starting dose. Keep in mind that switching medications still requires starting at the lowest dose and titrating up, regardless of your previous semaglutide dose. The side effect profile of tirzepatide is similar but not identical, and some people tolerate one better than the other.
Other options to discuss with your provider
Beyond semaglutide and tirzepatide, the GLP-1 landscape is expanding. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, has shown impressive results in clinical trials with weight loss exceeding 24% in some studies. Oral semaglutide formulations are another option if injections were a barrier. Some people explore combination approaches with other weight management medications, though these should only be pursued under close medical supervision.
There are also newer delivery methods emerging, including GLP-1 patches and various oral formulations that may suit people who struggled with the injection format. Discuss all available options with your healthcare provider before making a decision, and consider using the GLP-1 plotter tool to compare potential outcomes across different medications.
Medical considerations and contraindications
Not everyone should restart semaglutide. Certain medical conditions and situations require caution or complete avoidance. Review this section carefully and discuss any concerns with your healthcare provider before restarting.
Absolute contraindications
Do not restart semaglutide if you have a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2). These are absolute contraindications based on thyroid C-cell tumor findings in rodent studies. Do not restart if you experienced a severe hypersensitivity reaction (anaphylaxis, angioedema) during your previous course of semaglutide. If you developed pancreatitis while on semaglutide, most providers will recommend permanent discontinuation of all GLP-1 receptor agonists.
Situations requiring extra caution
If you are pregnant or planning to become pregnant, semaglutide must be stopped at least two months before conception. The medication is contraindicated during pregnancy due to potential fetal harm. If you are breastfeeding, discuss the risks and benefits with your provider, as data on GLP-1 receptor agonists during lactation is limited.
If you had surgery during your break, the timing of your restart depends on the type of procedure and your recovery status. GLP-1 receptor agonists are typically held for 1-3 weeks before surgery due to aspiration risk from delayed gastric emptying. After surgery, restarting depends on whether you are eating normally and have fully recovered from anesthesia. Consult both your surgeon and prescribing provider.
People with a history of gallbladder disease should be monitored closely, as semaglutide may increase the risk of gallstones and cholecystitis. Those with significant kidney impairment need dose adjustments and more frequent monitoring. If you take other diabetes medications, particularly insulin or sulfonylureas, your provider will need to adjust those medications when restarting semaglutide to avoid hypoglycemia.
Drug interactions to review
Because semaglutide delays gastric emptying, it can affect the absorption of oral medications. This is particularly important for birth control pills, thyroid medications, and any drugs with narrow therapeutic windows. Your provider should review all your current medications before approving a restart. Some combinations require careful timing or dose adjustments. Alcohol consumption should also be discussed, as it can compound GI side effects and interact with the metabolic effects of the medication.
Building a long-term plan so you do not need another break
The best restart is the one you never have to do again. Building sustainability into your treatment plan from the beginning of this restart dramatically increases the probability of long-term success.
Address the original reason for stopping
This is step one. Be brutally honest with yourself about why you stopped. If cost was the issue, explore compounded semaglutide options that may be more affordable, manufacturer savings programs, or insurance appeals. If side effects drove the break, develop a proactive management plan using the strategies outlined earlier in this guide. If adherence was the challenge, set weekly phone reminders, keep your medication visible, and consider enlisting an accountability partner.
Plan for supply interruptions
Drug shortages have been a recurring issue with GLP-1 receptor agonists. Have a contingency plan. Know which pharmacies in your area carry your formulation. If using compounded semaglutide, confirm your pharmacy maintains proper storage and has reliable supply chains. Some people keep a 2-4 week buffer supply, though this should be done within the bounds of your prescription. Understanding how long your medication lasts under various storage conditions helps you plan ahead.
Build habits that survive medication gaps
The behavioral changes you make while on semaglutide should be strong enough to partially sustain you during any future interruption. This means actively practicing portion control even when the medication makes it effortless, developing an exercise routine you enjoy and will maintain independently, learning to cook meals that are healthy and satisfying, and building awareness of emotional eating patterns. The real-world data showing that 77% of people maintain at least some weight loss after stopping GLP-1 medications suggests that lasting behavioral change is possible. It requires intentional effort while the medication is making things easier.
SeekPeptides provides comprehensive resources for building sustainable protocols, including personalized guidance that accounts for individual goals, body composition, and lifestyle factors. Members access detailed protocol builders, community support, and evidence-based strategies that extend far beyond simple medication management.
Monitor your progress systematically
Track more than just weight. Record your measurements, how your clothes fit, your energy levels, sleep quality, mood, and exercise performance. These additional data points provide motivation during periods when the scale is not moving and help your provider make informed decisions about dose adjustments. Weekly weigh-ins at the same time, on the same scale, wearing similar clothing, give the most consistent data. Daily weighing introduces noise that can be psychologically counterproductive, though some people prefer it for the additional data points.
Set realistic expectations for this round
Your restart may not mirror your first experience. Weight loss might be slightly slower if you are starting from a lower weight than your original baseline. Side effects might be different in intensity or duration. The key metric is progress over time, not comparison to your first round. Focus on trends over weeks and months rather than individual data points.
For researchers focused on optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, personalized protocol builders, and a community of thousands who have navigated these exact challenges.
Frequently asked questions
Can I restart semaglutide at 1 mg if that was my previous dose?
No. After a 3-month break, you must restart at 0.25 mg weekly regardless of your previous dose. Your body has completely lost its tolerance to the medication, and jumping to a higher dose will cause severe gastrointestinal symptoms including nausea, vomiting, and potential dehydration. Follow the full titration schedule as if starting for the first time.
How long will it take to get back to my previous dose?
Using the standard titration schedule, reaching 1.0 mg from a 0.25 mg restart takes approximately 8-12 weeks. Reaching 2.4 mg takes approximately 16-20 weeks. Some providers allow slightly compressed titration for patients who previously tolerated the medication well, but this should only be done under medical supervision. Our dosage guide breaks down the exact units for each dose level.
Will the medication work as well the second time?
Yes. There is no evidence that semaglutide becomes less effective with repeated use. Your GLP-1 receptors respond to the medication the same way they did the first time. Some people actually find the second round more effective because they have better strategies for diet, exercise, and side effect management based on their prior experience. Refer to our guide on how long semaglutide takes to work for realistic timeline expectations.
What if my previous semaglutide prescription expired during the break?
Do not use expired medication. Semaglutide is a peptide that degrades over time, and expired semaglutide may have reduced potency or altered composition. Contact your prescribing provider for a new prescription. If you are using compounded semaglutide, check both the expiration date and the beyond-use date (BUD) on the vial.
I regained all the weight I lost. Is it still worth restarting?
Absolutely. Weight regain after stopping GLP-1 medications is well-documented and expected. Restarting is a medically appropriate response to a chronic condition. The fact that your body regained weight confirms that obesity has a strong biological component that requires ongoing management. Most healthcare providers will support restarting without hesitation. If you are not seeing results after your restart, review our troubleshooting guide on why semaglutide might not be working.
Can I use my old semaglutide pens or vials that have been stored in the fridge?
Check the expiration date and storage conditions. Properly refrigerated, unopened semaglutide pens (branded Ozempic or Wegovy) are good until their printed expiration date, typically 18-24 months from manufacture. Once opened, they are good for 56 days (8 weeks) at room temperature or refrigerated. Compounded semaglutide has different stability windows, with refrigerated shelf life varying by formulation and pharmacy. When in doubt, discard old product and get a fresh supply.
Should I do anything differently with my diet before restarting?
Yes. Begin reducing portion sizes and increasing protein intake 1-2 weeks before your first restart injection. This primes your body for the reduced appetite and helps establish healthy eating patterns before the medication takes effect. Review our complete semaglutide diet plan and supplement recommendations to prepare comprehensively.
Is the hair loss associated with GLP-1 medications worse when restarting?
Hair loss (telogen effluvium) associated with GLP-1 medications is primarily caused by rapid weight loss and caloric deficit rather than the medication itself. When restarting, hair loss risk follows the same pattern as initial treatment. It correlates with the rate and amount of weight loss. Ensuring adequate protein intake (at least 60-80 grams daily) and considering biotin supplementation can help minimize this risk.
External resources
STEP 1 Trial Extension: Weight regain after semaglutide withdrawal (PMC)
Mayo Clinic: Semaglutide side effects and dosage information
GI tolerability of semaglutide 2.4 mg in adults with overweight or obesity (PMC)
In case I do not see you, good afternoon, good evening, and good night. May your restart go smoothly, your titration stay on schedule, and your progress hold steady for the long run.