Mar 20, 2026

What if the biggest fear about retatrutide, the worry that keeps researchers hesitating before their first dose, is based on incomplete information? Muscle loss during weight loss treatment is a legitimate concern. Nobody wants to trade body fat for a weaker, less functional physique. And with retatrutide producing some of the most dramatic weight loss results ever seen in clinical trials, up to 24% body weight reduction at the highest doses, the question of what happens to lean tissue deserves a serious answer.
Here is the good news. The phase 2 clinical trial data, published in The Lancet Diabetes and Endocrinology, tells a more nuanced story than the headlines suggest. DEXA scans from 189 participants reveal that 62% to 69% of total weight lost on retatrutide came from fat mass, not muscle. That ratio is consistent with, and in some cases better than, what researchers observe with semaglutide and tirzepatide. The triple-agonist mechanism that makes retatrutide so effective at burning fat may actually offer a metabolic advantage when it comes to preserving lean tissue.
But data alone does not protect your muscles. Strategy does. This guide breaks down every piece of available evidence on retatrutide and body composition, explains exactly how much lean mass you can expect to lose, and provides research-backed protocols for keeping as much muscle as possible while maximizing fat loss. Whether you are considering retatrutide for the first time or already mid-protocol, the information here will change how you approach your entire regimen.
How retatrutide works differently from other weight loss peptides
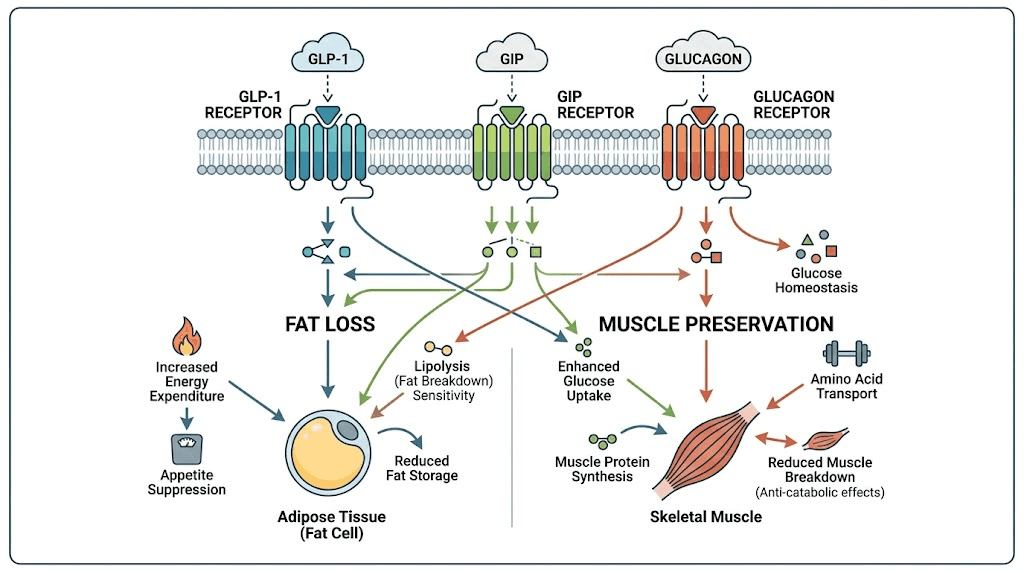
Understanding why retatrutide affects body composition the way it does requires looking at its unique mechanism. Unlike semaglutide, which targets only the GLP-1 receptor, or tirzepatide, which hits both GLP-1 and GIP receptors, retatrutide activates three distinct receptor pathways simultaneously. GLP-1, GIP, and glucagon. That third receptor, the glucagon receptor, is what separates retatrutide from everything else on the market.
Glucagon activation matters for muscle preservation.
When the glucagon receptor is stimulated, the body increases energy expenditure through thermogenesis. It preferentially mobilizes fat stores, particularly visceral fat, for fuel rather than breaking down muscle protein. The phase 2 trial demonstrated this clearly, with android visceral fat mass decreasing by up to 31.4% at the 12mg dose. That level of targeted fat reduction suggests the glucagon component is doing something fundamentally different from simple appetite suppression and caloric restriction.
The GIP receptor activation adds another layer. Research indicates that GIP signaling plays a role in lipid metabolism and may help the body partition nutrients more effectively, directing calories toward lean tissue maintenance rather than fat storage. This dual benefit, enhanced fat burning through glucagon plus improved nutrient partitioning through GIP, creates a metabolic environment that is theoretically more favorable for preserving muscle during weight loss than single-receptor medications.
The GLP-1 component handles appetite suppression and glucose regulation. If you have used semaglutide before, you already know how this receptor works. It slows gastric emptying, reduces hunger signals, and improves insulin sensitivity. Combined with the other two receptors, it creates a comprehensive metabolic reset that addresses fat loss from multiple angles simultaneously. You can explore the full retatrutide dosing guide for detailed protocol information on how these mechanisms translate into practical use.
What the clinical trial data says about retatrutide and muscle loss
Numbers matter more than speculation. The most important data comes from a substudy of the phase 2, double-blind, placebo-controlled trial published in The Lancet Diabetes and Endocrinology. Researchers used dual-energy X-ray absorptiometry (DEXA) scans to measure precise changes in fat mass and lean mass across 189 participants with type 2 diabetes over 36 weeks.
Here is what they found.
Total fat mass decreased significantly across all effective doses. The reductions were dose-dependent: 4.9% with the 0.5mg dose, 15.2% with 4mg, 26.1% with 8mg, and 23.2% with 12mg. Compared to placebo, which showed only a 4.5% reduction, the higher doses delivered statistically significant improvements. The 8mg group showed a 21.6 percentage point difference versus placebo. The 12mg group showed an 18.7 percentage point difference. Both achieved p-values below 0.0001.
Lean mass did decrease. At the 8mg dose, total lean mass dropped by up to 12.5%, with an absolute loss of approximately 6.5kg. That sounds alarming until you put it in context. The fat loss index, which measures the proportion of total weight lost that comes from fat, ranged from 62.0% to 69.3% across the effective doses. In other words, roughly two-thirds of every kilogram lost was fat, not muscle.
This ratio is the critical metric. And it aligns with what researchers observe across virtually all weight loss interventions, whether pharmaceutical, surgical, or dietary. The general scientific consensus is that during significant weight loss, approximately 25% to 40% of total weight lost comes from lean tissue. Retatrutide falls squarely within this expected range, and at the favorable end of it.
The study authors themselves concluded that these findings "provide reassurance that a greater proportion of lean mass is not lost with retatrutide despite the overall increased weight loss."
When researchers who designed the trial reach that conclusion, it carries significant weight. Understanding your retatrutide dosage and titration schedule becomes essential for managing these outcomes effectively.
Android fat versus total body composition
The DEXA data revealed something particularly interesting about where retatrutide removes fat. Android fat, the dangerous visceral fat that surrounds organs and drives metabolic disease, decreased by up to 31.4% at the 12mg dose. Both the android-to-gynoid fat ratio and trunk-to-leg fat ratio were significantly reduced in the 8mg group, indicating that retatrutide preferentially targets the most metabolically harmful fat deposits.
This matters for body composition beyond the scale. A person who loses 15kg total, with 10kg from visceral and subcutaneous fat and 5kg from lean tissue, ends up with a dramatically healthier metabolic profile than someone who loses the same amount but from less targeted locations. The visceral fat reduction alone translates to improved insulin sensitivity, reduced inflammation, and lower cardiovascular risk. These improvements often offset concerns about moderate lean mass changes, especially when combined with the metabolic benefits of improved body composition ratios.
How retatrutide compares to semaglutide and tirzepatide for muscle preservation
Comparison drives clarity. If retatrutide caused disproportionate muscle loss compared to other GLP-1 medications, that would be a genuine concern. But the data suggests the opposite.
Semaglutide studies show that lean mass loss typically accounts for 26% to 40% of total weight lost. The STEP 1 trial, which tested semaglutide 2.4mg in adults with obesity, found that approximately 39% of weight lost was lean mass after 68 weeks. That is actually a higher proportion of muscle loss than what retatrutide showed in its phase 2 data.
Tirzepatide data from the SURMOUNT-1 trial tells a similar story. Body composition analysis revealed lean mass changes comparable to those seen with other obesity treatments. The proportion of lean mass to total weight lost fell within the standard 25-40% range. Since tirzepatide activates two of the same three receptors as retatrutide (GLP-1 and GIP), researchers expected similar body composition outcomes, and that is exactly what they found.
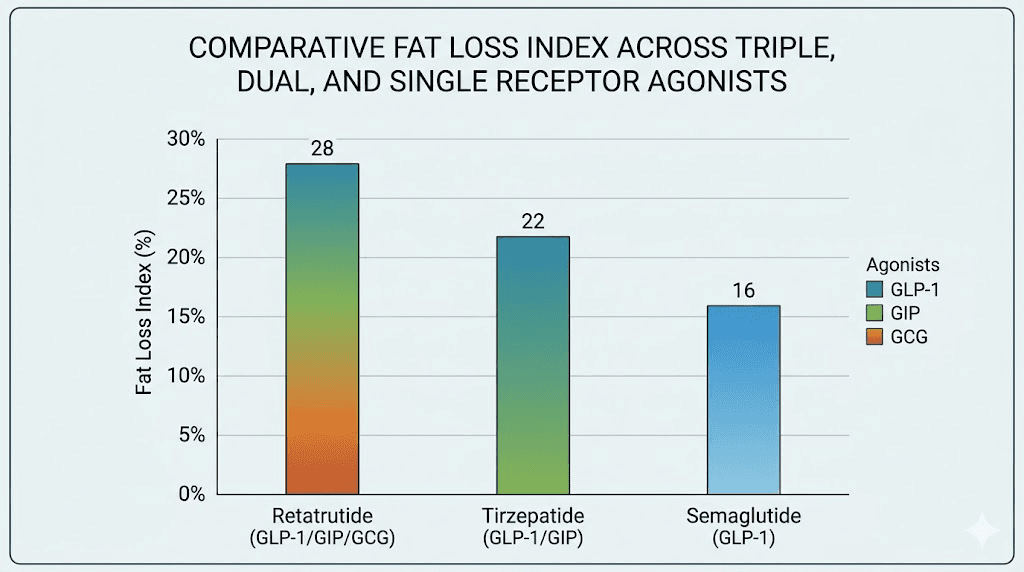
Retatrutide, despite producing greater total weight loss than both semaglutide and tirzepatide in head-to-head comparisons, maintained a fat loss index of 62-69%. That means the additional weight loss driven by the glucagon receptor came predominantly from fat, not muscle. The retatrutide versus semaglutide comparison becomes even more favorable when you consider the absolute amount of fat removed.
Medication | Receptors targeted | Max weight loss | Lean mass loss proportion | Fat loss index |
|---|---|---|---|---|
Retatrutide | GLP-1 + GIP + Glucagon | Up to 24% | 31-38% | 62-69% |
Tirzepatide | GLP-1 + GIP | Up to 22.5% | 33-40% | 60-67% |
Semaglutide | GLP-1 only | Up to 16% | 35-39% | 61-65% |
The data suggests that the glucagon receptor activation in retatrutide may actually provide a modest advantage for fat-selective weight loss. While the differences are not enormous, they are consistent across doses, and they become more meaningful at higher weight loss thresholds where muscle preservation becomes increasingly challenging. For a detailed dose-by-dose comparison, see the retatrutide versus tirzepatide dosage chart and the full comparison guide.
Why some muscle loss happens during any significant weight loss
Before blaming retatrutide specifically, understand that muscle loss during weight loss is a biological reality, not a medication side effect. Your body does not distinguish between intentional fat loss and starvation. When caloric intake drops significantly, it activates survival mechanisms that break down both fat and lean tissue for energy.
Three factors drive this process.
First, reduced caloric intake means less raw material for muscle protein synthesis. Muscles require a constant supply of amino acids to maintain their structure. When total food intake decreases, protein intake almost always decreases proportionally. Fewer amino acids means less muscle maintenance and repair, leading to gradual atrophy. This is true whether the caloric deficit comes from eating less, exercising more, or using any weight loss medication including appetite-suppressing peptides.
Second, the body uses gluconeogenesis to maintain blood sugar during extended caloric deficits. This process converts amino acids from muscle tissue into glucose. The greater the caloric deficit, the more the body relies on this pathway. Retatrutide creates substantial caloric deficits through appetite suppression, but the glucagon receptor activation may actually help mitigate this effect by promoting fat oxidation as the primary alternative fuel source.
Third, reduced physical activity accelerates muscle loss. Many people on GLP-1 medications experience fatigue, nausea, or general malaise during the early weeks of treatment. These side effects can reduce exercise frequency and intensity, removing the mechanical stimulus that tells muscles to maintain their size and strength. Without regular resistance training, the body has no reason to preserve muscle tissue it perceives as metabolically expensive.
The good news is that all three of these factors are modifiable. You cannot eliminate muscle loss entirely during significant weight loss, but you can reduce it dramatically with the right approach. Studies show that adequate protein intake combined with resistance training can reduce lean mass loss by 50% to 95% compared to weight loss without these interventions. That transforms a potentially concerning outcome into a manageable one.
How to prevent muscle loss while taking retatrutide
Prevention requires a multi-pronged strategy. No single intervention is sufficient on its own. The most successful approach combines nutritional optimization, structured resistance training, adequate recovery, and intelligent dose management. Research published in 2025 demonstrates that when all four elements are in place, researchers can lose 13% of body weight while sacrificing only 3% of muscle mass. That is a remarkable ratio.
Think of muscle preservation as a system, not a single tactic.
Each component reinforces the others. Higher protein intake provides the raw materials for muscle maintenance. Resistance training sends the signal to preserve lean tissue. Adequate sleep and recovery allow that preservation to actually happen. And proper dose titration, starting with the recommended starting dose and gradually increasing, ensures the caloric deficit does not become so extreme that the body cannibalizes muscle out of desperation.
The hierarchy of muscle preservation
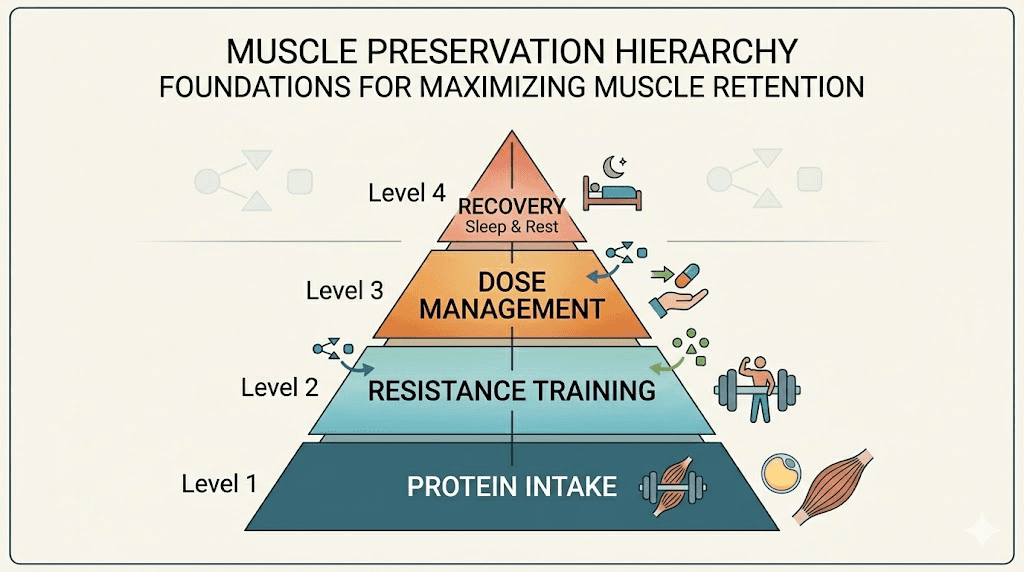
Not all interventions are equally important. Based on the available research, here is the priority order:
Priority 1: Protein intake. This is the single most impactful variable. A 2025 study from the Endocrine Society found that higher protein intake was directly associated with less muscle mass loss in people taking GLP-1 receptor agonists. Aim for 1.2 to 1.6 grams of protein per kilogram of body weight daily. For a 90kg person, that translates to 108 to 144 grams per day. Distribute this across three to four meals for optimal muscle protein synthesis. More on specific strategies in the protein section below.
Priority 2: Resistance training. The mechanical stimulus from resistance exercise is the strongest signal your body receives to maintain muscle mass. A Medscape-reported study showed that combining resistance training with adequate protein reduced muscle loss to just 3% during 13% total weight loss. Two to three sessions per week targeting all major muscle groups provides sufficient stimulus. Progressive overload matters more than volume.
Priority 3: Dose management. Aggressive dose escalation creates extreme caloric deficits that overwhelm the body ability to preserve lean tissue. The retatrutide dosage chart recommends gradual titration starting at 1mg weekly, progressing through 2mg, 4mg, 8mg, and potentially 12mg based on tolerance and response. Rushing this process increases muscle loss risk. Patience with titration pays dividends in body composition.
Priority 4: Recovery and sleep. Muscle protein synthesis occurs primarily during rest, particularly deep sleep. Growth hormone release, which supports lean tissue maintenance, peaks during the first few hours of sleep. If retatrutide causes fatigue or sleep disruption, addressing these side effects directly supports muscle preservation. Seven to nine hours of quality sleep is the target.
Protein intake strategies for retatrutide users
Getting enough protein while on retatrutide presents a unique challenge. The medication dramatically reduces appetite. Food volume capacity drops. Many researchers report struggling to eat enough of anything, let alone hitting specific macronutrient targets. This is where strategic meal planning becomes essential.
The research is clear on targets. A 2025 study published ahead of the Endocrine Society annual meeting found that consuming more protein was directly protective against muscle loss in people taking anti-obesity medications. The minimum effective threshold appears to be 1.2 grams per kilogram of body weight per day. The optimal range extends to 1.6 grams per kilogram. Some researchers push as high as 2.0 grams per kilogram, though diminishing returns set in beyond 1.6 for most people.
Distribution matters as much as total intake. Research shows that distributing protein evenly across meals, approximately 25 to 30 grams per meal across three to four eating occasions, increases muscle protein synthesis by 25% compared to consuming the same total amount in a skewed pattern. Eating 80 grams of protein at dinner and 15 grams at breakfast is significantly less effective than eating 30 grams at each of three meals plus a 10-gram snack.
Practical protein strategies when appetite is suppressed
Protein-first eating. At every meal, eat the protein source before anything else. When your stomach capacity is limited by GLP-1 effects, you need to prioritize the most important macronutrient before filling up on carbohydrates or fiber. Grilled chicken, fish, eggs, or Greek yogurt should hit your plate first. Vegetables and grains fill whatever space remains.
Liquid protein supplements. When solid food feels impossible, protein shakes designed for GLP-1 users can bridge the gap. A 30-gram whey or casein shake takes minimal stomach space and digests easily. Some researchers find that sipping a shake throughout the morning is more tolerable than trying to eat a full breakfast. Casein protein before bed provides sustained amino acid release during sleep, supporting overnight muscle protein synthesis.
High-protein snacks between meals. Cottage cheese, jerky, hard-boiled eggs, and protein bars all deliver significant protein in small volumes. Keeping these accessible throughout the day helps maintain consistent amino acid availability. The goal is never going more than four to five hours without a protein feeding during waking hours.
Leucine-rich sources. Not all proteins are equal for muscle preservation. Leucine is the amino acid that most directly triggers muscle protein synthesis. Whey protein, eggs, chicken breast, and fish are particularly rich in leucine. Aim for at least 2.5 to 3 grams of leucine per meal, which is approximately the amount in 30 grams of whey protein or 150 grams of chicken breast.
Meal timing around training sessions amplifies the effect. Consuming 20 to 40 grams of protein within two hours of resistance training provides the amino acids needed to repair and maintain trained muscle tissue. This post-workout window is not as narrow as bodybuilding culture suggests, but hitting it consistently does produce measurably better outcomes. For complete meal plans optimized for peptide users, explore the GLP-1 breakfast ideas and dinner ideas guides.
Sample daily protein plan for a 90kg researcher on retatrutide
Target: 130g protein daily (1.4g/kg)
Breakfast (7:00 AM): 30g protein. Two eggs plus one scoop whey protein in water. Even on the most suppressed appetite days, this combination takes minimal stomach capacity.
Lunch (12:00 PM): 35g protein. 150g grilled chicken breast with vegetables. Eat the chicken first. If you cannot finish the vegetables, that is acceptable. The protein is non-negotiable.
Afternoon snack (3:00 PM): 15g protein. 200g Greek yogurt or a small portion of cottage cheese. This prevents the long gap between lunch and dinner from depleting amino acid availability.
Dinner (6:30 PM): 35g protein. 200g salmon or lean beef with whatever sides your appetite allows. Fish is often better tolerated on GLP-1 medications than red meat due to its lighter texture and faster digestion.
Evening (9:00 PM): 15g protein. Casein protein shake or a small serving of cottage cheese before bed. This provides sustained amino acid release throughout the night, supporting muscle maintenance during sleep.
Adjust portions based on your specific weight and tolerance. The key principle is that protein intake should be the last thing you compromise when appetite drops. Reduce carbohydrates and fats before reducing protein. Your muscles depend on it. For more dietary guidance while on peptide therapy, see the comprehensive diet strategies that apply across all GLP-1 medications.
Resistance training protocols that protect muscle mass
Exercise is not optional if you care about body composition on retatrutide. A 2025 case series published in PMC demonstrated that supervised resistance training preserved lean soft tissue during GLP-1-induced weight loss. The data is unambiguous. People who lift weights while on these medications keep significantly more muscle than those who do not.
But the approach matters.
You do not need to train like a bodybuilder. You do not need to spend two hours in the gym. You need progressive resistance training that targets all major muscle groups two to three times per week. Consistency trumps intensity. Showing up three times per week at moderate effort beats one heroic session followed by a week of recovery.
The minimum effective program
Frequency: 2-3 sessions per week with at least 48 hours between sessions targeting the same muscle groups.
Exercise selection: Focus on compound movements that work multiple muscle groups simultaneously. Squats, deadlifts, bench press, rows, overhead press, and pull-ups or lat pulldowns form the foundation. These movements provide the maximum muscle-preservation stimulus in the minimum time.
Volume: 2-3 sets of 8-12 repetitions per exercise. This range optimizes the balance between mechanical tension (which preserves muscle) and metabolic stress (which supports fat loss). Higher rep ranges with lighter weights are less effective for muscle preservation, though they still provide some benefit.
Progressive overload: This is the most important principle. You must gradually increase the challenge over time, either by adding weight, performing more repetitions, or adding sets. Without progressive overload, your body has no reason to maintain muscle mass. Even small increases of 1-2kg per week on major lifts signal the body to preserve lean tissue.
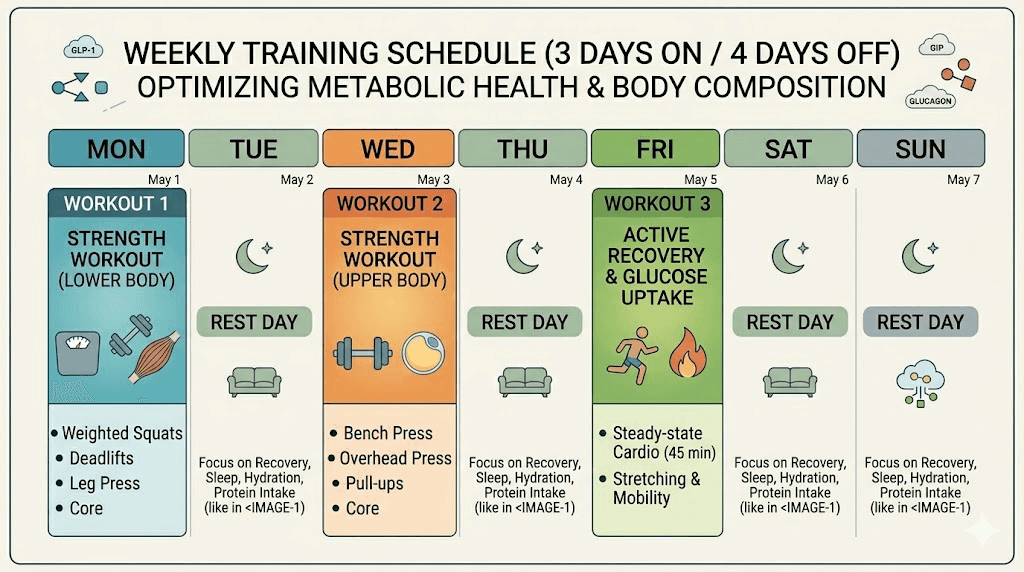
Week-by-week training structure
Session A (Monday):
Squats: 3 sets of 8-10 reps
Bench press: 3 sets of 8-10 reps
Barbell rows: 3 sets of 10-12 reps
Overhead press: 2 sets of 10-12 reps
Plank: 2 sets of 30-60 seconds
Session B (Wednesday):
Deadlifts: 3 sets of 6-8 reps
Incline dumbbell press: 3 sets of 10-12 reps
Pull-ups or lat pulldowns: 3 sets of 8-12 reps
Lunges: 2 sets of 10-12 reps per leg
Face pulls: 2 sets of 15 reps
Session C (Friday):
Leg press: 3 sets of 10-12 reps
Dumbbell rows: 3 sets of 10-12 reps
Dips or chest flyes: 3 sets of 10-12 reps
Romanian deadlifts: 2 sets of 10-12 reps
Bicep curls and tricep pushdowns: 2 sets each of 12-15 reps
Total time commitment: approximately 45-60 minutes per session. That is 2.5 to 3 hours per week, a modest investment that can reduce muscle loss by 50-95%. The return on time invested is extraordinary.
If retatrutide side effects like gastrointestinal discomfort or fatigue make training difficult during the first few weeks, start with just two sessions per week at reduced intensity. Maintaining the habit matters more than maximizing performance during the adjustment period. As your body adapts to the medication and side effects subside, gradually increase both frequency and intensity. The timing of your retatrutide dose relative to your training sessions can also help manage side effects during workouts.
Supplements that support muscle preservation on retatrutide
Supplements play a supporting role. They do not replace protein intake or resistance training, but they can provide an additional edge when the fundamentals are already in place. Several have direct evidence for muscle preservation during weight loss.
Creatine monohydrate is the most well-studied supplement for muscle preservation. It increases intramuscular creatine stores, which improves performance during resistance training and may directly support muscle protein synthesis. A dose of 3-5 grams daily is sufficient. No loading phase is necessary. Creatine is particularly valuable during caloric restriction because it helps maintain training intensity when energy availability is reduced. You can learn more about combining creatine with GLP-1 medications for detailed compatibility information.
HMB (beta-hydroxy beta-methylbutyrate) is a metabolite of leucine that shows promise for reducing muscle breakdown during caloric restriction. Research suggests 3 grams daily may reduce muscle protein breakdown, particularly in people who are not able to maintain optimal protein intake. It is most beneficial during the initial weeks of retatrutide treatment when appetite suppression is most severe and protein intake tends to be lowest.
Vitamin D plays a critical role in muscle function. Deficiency is associated with increased muscle loss during weight loss. Many people starting weight loss protocols are already deficient. Testing your levels and supplementing to maintain 40-60 ng/mL supports both muscle preservation and bone health. The complete GLP-1 supplement guide covers all recommended supplements including vitamin D, magnesium, and B vitamins.
Omega-3 fatty acids from fish oil may enhance muscle protein synthesis response to amino acids. A daily dose of 2-3 grams of combined EPA and DHA supports both muscle preservation and the anti-inflammatory benefits that complement the metabolic improvements from retatrutide. Some researchers report that omega-3 supplementation also helps manage the gastrointestinal side effects common with GLP-1 medications.
Essential amino acids (EAAs) provide a concentrated source of the building blocks muscles need, without requiring the digestion of whole food proteins. On days when appetite is especially suppressed, sipping on an EAA supplement between meals ensures continuous amino acid availability. This is a practical strategy for the first few weeks of treatment when solid food tolerance is at its lowest.
Dose management strategies for better body composition
How you manage your retatrutide dose directly impacts your body composition outcomes. Aggressive dosing creates extreme caloric deficits. Extreme deficits accelerate muscle loss. The relationship is not complicated, but it is frequently overlooked.
The phase 2 trial used a gradual titration schedule. Participants started at lower doses and increased over weeks, allowing the body to adapt at each level. Those who responded well to moderate doses (4-8mg) did not necessarily need to escalate to the maximum 12mg. Use the retatrutide dosage calculator to determine appropriate dosing based on your individual parameters, and review the complete dosing guide for personalized recommendations.
Titration approach for muscle preservation
Weeks 1-4: Start at 1mg weekly. Focus on establishing protein intake habits and beginning or maintaining a resistance training program. Side effects are typically mild at this dose, making it easier to train and eat adequately.
Weeks 5-8: Increase to 2mg weekly if tolerated. Monitor your ability to maintain protein intake targets. If you cannot consistently hit 1.2g/kg protein at this dose, stay here longer before escalating. Your muscles need the amino acids more than they need a larger dose.
Weeks 9-12: Progress to 4mg weekly. This is where significant appetite suppression typically begins. Increase protein supplementation to compensate. Liquid protein sources become more important. Continue resistance training with progressive overload.
Weeks 13-16: Consider 8mg weekly if weight loss has plateaued and protein intake remains adequate. The jump from 4mg to 8mg often produces the most dramatic appetite suppression. Plan your protein strategy in advance of this increase. Have protein shakes, EAA supplements, and high-protein snacks readily available.
Week 17 and beyond: The 12mg dose is available but not always necessary. If you are losing fat at a satisfactory rate on 8mg while maintaining adequate protein and training performance, there is no compelling reason to increase further. The additional appetite suppression from 12mg makes muscle preservation harder, not easier.
Track your body composition over time, not just your scale weight. Before and after comparisons that focus solely on pounds lost miss the critical distinction between fat loss and muscle loss. If available, periodic DEXA scans every 8-12 weeks provide the most accurate assessment of how your body composition is changing. Bioelectrical impedance scales, while less accurate, can track general trends when used consistently under the same conditions.
Signs you are losing too much muscle
Monitoring for excessive muscle loss allows you to adjust your approach before significant damage occurs. Several warning signs indicate that the balance has shifted too far toward lean tissue breakdown.
Strength decline. If your weights in the gym are dropping consistently over weeks, not just a bad day here and there, your body is breaking down muscle faster than it can maintain. A 5-10% strength decrease over the first month of treatment is normal as your body adapts to lower caloric intake. A 20%+ decrease suggests excessive muscle loss that requires intervention.
Rapid weight loss without improved appearance. Losing weight quickly but looking "flat" or "soft" rather than lean suggests a high proportion of the weight lost is muscle. Fat loss improves muscle definition. Muscle loss creates a shapeless, deflated appearance. If the mirror does not match the scale, body composition is shifting in the wrong direction.
Disproportionate fatigue is another signal. Some energy fluctuation is normal on GLP-1 medications. But profound, persistent weakness that worsens over weeks, particularly muscle-specific weakness that makes daily activities difficult, can indicate excessive lean tissue catabolism. This differs from the general malaise of medication adjustment, which typically improves within 2-4 weeks.
Grip strength decline. This is an underappreciated early indicator. Grip strength correlates strongly with overall muscle mass and is easy to track. If you notice difficulty opening jars, carrying groceries, or gripping objects that were previously easy, your overall lean mass is likely declining faster than desired.
Hair loss and nail brittleness. While GLP-1 medications can independently cause hair changes and the broader topic of GLP-1 hair loss is worth exploring, sudden hair shedding combined with the other signs above suggests a severe protein and caloric deficit that is affecting all protein-dependent tissues, not just muscles.
If you notice two or more of these signs, take immediate action. Reduce your retatrutide dose by one step. Increase protein intake aggressively. Ensure you are training at least twice weekly. And consider getting a DEXA scan to objectively assess your body composition. SeekPeptides members have access to detailed protocols for managing exactly these situations, with specific adjustment guidelines based on individual body composition data.
Real-world body composition changes on retatrutide
Clinical trial data provides population averages. Individual outcomes vary. Understanding the range of possible results helps set realistic expectations and guides your personal approach.
The phase 2 trial included 103 participants who completed both treatment and baseline plus week 36 DEXA scans. Among those taking effective doses (4mg, 8mg, or 12mg), body weight decreased by 6.9% to 16.9%. Fat mass decreased by 15.2% to 26.1%. Lean mass decreased by variable amounts, with the 8mg group showing the largest lean mass reduction at approximately 12.5%.
But these averages include participants who did not exercise and did not optimize their protein intake. The 2025 Medscape-reported study on resistance training plus protein shows what is possible when those interventions are in place: 13% total weight loss with only 3% muscle loss. That means the vast majority of weight lost, approximately 77%, was fat. Compare that to the 62-69% fat loss index from the trial where exercise was not controlled.
The message is straightforward. Retatrutide by itself produces acceptable body composition outcomes, with most weight lost coming from fat. Adding protein optimization and resistance training transforms acceptable into excellent.
The difference between losing 30-38% of your weight from muscle versus 20-23% becomes increasingly significant as total weight loss increases.
Expected body composition timeline
Weeks 1-4 (low dose): Minimal weight loss, mostly water and glycogen. Lean mass changes negligible. This is the window to establish training habits and protein intake before the metabolic demand increases. Use this time wisely.
Weeks 5-12 (dose escalation): Fat loss accelerates. Some lean mass reduction begins, primarily from reduced glycogen and water stored in muscle tissue. This initial lean mass drop is partially reversible and should not cause alarm. The retatrutide timeline provides more detail on what to expect during these early weeks.
Weeks 13-24 (therapeutic dose): Peak fat loss period. Lean mass changes stabilize if protein and training are adequate. The body reaches a new equilibrium where fat is being lost at a high rate while muscle tissue is being maintained through sufficient protein and mechanical stimulus. This is the critical window where your habits determine your final body composition outcome.
Weeks 25-36 (maintenance or continued loss): Rate of weight loss naturally slows. Lean mass preservation becomes easier as the body adapts to its new caloric equilibrium. Continuing resistance training during this phase can even result in modest muscle gain, as the reduced fat mass improves insulin sensitivity and nutrient partitioning. Some researchers who maintain excellent protein intake and training consistency report actually gaining strength during this period despite overall weight loss.
For comprehensive tracking guidance, the retatrutide dosage chart can be cross-referenced with the week-by-week results guide to understand typical progression patterns.
Advanced strategies for experienced researchers
If you have already mastered the fundamentals, several advanced approaches can further optimize body composition on retatrutide.
Carb cycling around training days. On resistance training days, increase carbohydrate intake moderately (an additional 30-50 grams) while maintaining protein. Carbohydrates support training performance, drive insulin release that promotes muscle protein synthesis, and replenish glycogen stores in trained muscles. On rest days, reduce carbohydrates and increase dietary fat to maintain a more consistent caloric deficit. This approach maintains the average caloric deficit required for fat loss while providing muscles with the nutrients they need on the days they need them most.
Strategic dose timing. Some researchers time their retatrutide injection on the day after their most important training session, when appetite is naturally lowest from training fatigue anyway. This approach front-loads the strongest appetite suppression to non-training days, allowing slightly higher food intake on training days when nutritional needs are greatest. The injection site guide and injection technique article provide the technical details for optimal administration.
Periodic diet breaks. Every 8-12 weeks, some researchers spend one to two weeks eating at maintenance calories while continuing to take retatrutide at their current dose. This "diet break" allows hormonal markers related to muscle preservation (testosterone, IGF-1, thyroid hormones) to recover from the sustained deficit. Research on intermittent energy restriction suggests this approach may improve long-term body composition outcomes compared to continuous restriction.
Stacking with muscle-supportive peptides. Some advanced researchers combine retatrutide with peptides that specifically support lean tissue, such as growth hormone secretagogues or muscle-building peptides. This area lacks large clinical trials specific to retatrutide combinations, but the theoretical rationale is sound: using one compound for fat loss and another for muscle preservation addresses both sides of the body composition equation simultaneously. Use the peptide stack calculator to evaluate potential combinations.
SeekPeptides provides detailed stacking protocols and body composition optimization guides for members who want to take their retatrutide results to the next level. The platform evidence-based approach ensures that advanced strategies are grounded in research, not speculation.
Comparing muscle loss across different weight loss methods
Perspective helps. Retatrutide is not uniquely problematic for muscle loss. In fact, when compared to other weight loss approaches, it performs quite favorably.
Weight loss method | Average lean mass loss | Fat loss index | Typical rate |
|---|---|---|---|
Retatrutide (with training) | 20-25% of total loss | 75-80% | 1-2 kg/week |
Retatrutide (without training) | 31-38% of total loss | 62-69% | 1-2 kg/week |
Semaglutide (without training) | 35-39% of total loss | 61-65% | 0.5-1 kg/week |
Caloric restriction only | 25-40% of total loss | 60-75% | 0.5-1 kg/week |
Bariatric surgery | 25-35% of total loss | 65-75% | 2-4 kg/week (initial) |
Very low calorie diet | 35-50% of total loss | 50-65% | 1.5-2.5 kg/week |
The data tells a clear story. Retatrutide with resistance training produces the best body composition outcomes of any weight loss method, including approaches that produce less total weight loss. Even without exercise, retatrutide lean mass losses fall within normal ranges. The triple-receptor mechanism does not create a special muscle-wasting effect. It creates more total weight loss while maintaining similar or better fat-to-lean loss ratios.
Very low calorie diets (VLCDs), by contrast, produce the worst body composition outcomes. Up to 50% of weight lost from muscle. This underscores why simply not eating, which is effectively what some people do when they first start retatrutide and let side effects dictate their nutrition, is the worst possible approach. Eating intentionally, with a focus on protein, produces dramatically different results than eating reactively, or not eating at all. The dietary guidance for GLP-1 users applies equally to retatrutide and provides practical frameworks for maintaining adequate nutrition despite reduced appetite.
Common mistakes that accelerate muscle loss on retatrutide
Knowing what to avoid is as important as knowing what to do.
Mistake 1: Treating appetite suppression as permission to not eat. The biggest error researchers make. When retatrutide eliminates hunger, the temptation is to eat as little as possible to maximize weight loss. This approach creates extreme caloric deficits of 1000+ calories per day, which the body compensates for by breaking down muscle at accelerated rates. Even when you are not hungry, you need to eat. Specifically, you need to eat protein. Treat meals as medicine during retatrutide treatment.
Mistake 2: Doing only cardio. Cardio burns calories but does nothing to signal muscle preservation. Running, cycling, and elliptical work are fine for cardiovascular health, but they do not provide the mechanical stimulus that tells your body to maintain lean tissue. Replacing resistance training with cardio during weight loss is a direct path to a "skinny fat" outcome. If you only have time for one form of exercise, choose lifting. Every time.
Mistake 3: Escalating dose too quickly. Rushing from 1mg to 8mg or 12mg over just a few weeks creates an adaptation crisis. The body cannot adjust its metabolic rate, appetite, and energy systems fast enough. The result is excessive caloric restriction that overwhelms muscle-preservation mechanisms. Follow the recommended dose escalation schedule and spend at least 4 weeks at each dose level before increasing.
Mistake 4: Ignoring protein distribution. Eating one large high-protein meal per day and nothing else. Some researchers fall into this pattern, especially during the early weeks when they can only tolerate one meal. While getting any protein is better than none, muscle protein synthesis operates on a meal-by-meal basis. Your muscles cannot store amino acids for later use. Spreading protein across multiple smaller feedings throughout the day is significantly more effective.
Mistake 5: Stopping training during side effects. The first few weeks of retatrutide, particularly during dose increases, often bring nausea, gastrointestinal issues, and fatigue. Many researchers stop exercising entirely during these periods. While reducing training intensity is appropriate, stopping completely sends a strong signal to the body that muscle tissue is no longer needed. Even abbreviated sessions of 20 minutes with lighter weights maintain the preservation signal. Show up. Do something. Consistency matters more than perfection.
Long-term muscle health considerations
Retatrutide is not meant to be taken indefinitely at high doses. Most protocols involve a treatment phase followed by either dose reduction or discontinuation. Understanding the long-term implications for muscle health helps you plan beyond the active weight loss phase.
Muscle lost during retatrutide treatment can be regained. Unlike some forms of tissue loss, skeletal muscle has remarkable regenerative capacity. Research shows that previously trained muscles regain size and strength faster than untrained muscles, a phenomenon called "muscle memory." The myonuclei accumulated during prior training remain even after muscle atrophy, providing a biological foundation for rapid rebuilding.
After completing a retatrutide protocol, transitioning to a maintenance caloric intake while continuing resistance training creates optimal conditions for muscle recovery. Many researchers report gaining back lost lean tissue within 3-6 months of returning to maintenance calories, particularly if they maintained a training program throughout treatment.
The transition between medications is another consideration. If moving from retatrutide to a lower-potency medication for maintenance, the reduced appetite suppression makes it easier to consume adequate protein, which naturally supports lean tissue recovery. The dosage scheduling guide provides detailed protocols for managing these transitions.
Bone density deserves mention alongside muscle. Significant weight loss from any cause can reduce bone mineral density, and muscle mass is directly correlated with bone health. Resistance training addresses both concerns simultaneously by applying mechanical load to both muscles and bones. Adequate calcium and vitamin D intake, which should already be part of your supplement regimen, further supports skeletal health during the weight loss phase.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. The platform detailed body composition guides, dosage calculators, and member-exclusive research updates make it the ideal companion for anyone managing a retatrutide protocol.
Frequently asked questions
Does retatrutide cause more muscle loss than semaglutide?
No. Phase 2 trial data shows retatrutide fat loss index ranges from 62% to 69%, meaning most weight lost is fat. This is comparable to or slightly better than semaglutide, which shows approximately 61-65% fat loss index. The glucagon receptor activation in retatrutide may actually support preferential fat oxidation.
How much muscle will I lose on retatrutide?
Without resistance training and protein optimization, expect approximately 31-38% of total weight lost to come from lean mass. With proper training and protein intake (1.2-1.6g/kg/day), this drops to approximately 20-23%. On a 15kg weight loss, that is the difference between losing 5.4kg of lean mass versus 3.3kg.
Can I build muscle while taking retatrutide?
Building significant new muscle while in a caloric deficit is unlikely for most people. However, maintaining existing muscle mass is very achievable with proper nutrition and training. Some beginners or people returning to training after a break may experience modest strength and muscle gains even during weight loss, a phenomenon called "body recomposition."
What is the best protein source for retatrutide users?
Whey protein isolate provides the highest leucine content per gram, making it the most efficient trigger for muscle protein synthesis. For whole foods, chicken breast, fish, eggs, and Greek yogurt offer the best protein-to-volume ratio, which matters when appetite is suppressed. See the GLP-1 protein shake guide for specific product recommendations.
How soon after starting retatrutide should I begin resistance training?
Ideally, before you start. Establishing a training routine 2-4 weeks before beginning retatrutide means the habit is already in place when appetite suppression and potential side effects begin. If you are already on retatrutide, start training now regardless of where you are in your protocol. Every week without training is a week of unnecessary muscle loss.
Does the 12mg dose cause more muscle loss than the 8mg dose?
The phase 2 data shows variable results. The 8mg dose actually showed the highest lean mass percentage reduction (12.5%), while the 12mg dose showed slightly less. However, absolute lean mass loss tends to increase with dose because total weight loss is greater. Use the retatrutide 10mg guide and 20mg dosing guide for dose-specific body composition information.
Will creatine help preserve muscle on retatrutide?
Yes. Creatine monohydrate (3-5g daily) supports training performance during caloric restriction and may directly support muscle protein synthesis. It also increases intramuscular water retention, which can counteract some of the "flat" appearance that comes from glycogen depletion during dieting. It is one of the most evidence-based supplements for GLP-1 users.
How do I know if I am losing fat versus muscle?
DEXA scans provide the most accurate assessment. Bioelectrical impedance scales offer trending data when used consistently. Practically, monitor your gym performance (strength declining suggests muscle loss), body measurements (waist decreasing while limb measurements hold suggests fat loss), and visual appearance (increased definition suggests favorable body composition changes). Track your weight loss timeline alongside these metrics for the most complete picture.
External resources
The Lancet: Effects of retatrutide on body composition in people with type 2 diabetes
New England Journal of Medicine: Triple-Hormone-Receptor Agonist Retatrutide for Obesity
PMC: Saving muscle while losing weight on GLP-1 related drugs
In case I do not see you, good afternoon, good evening, and good night. May your lean mass stay preserved, your fat loss stay targeted, and your protocols stay evidence-based.