Feb 8, 2026

Tired of conflicting information about semaglutide treatment duration? One article says six months. Another claims you need it forever. Your doctor mentions maintenance doses, but your insurance only approves three months at a time. Meanwhile, you are watching the scale drop and wondering if you will spend the rest of your life with a weekly injection.
Here is what actually works.
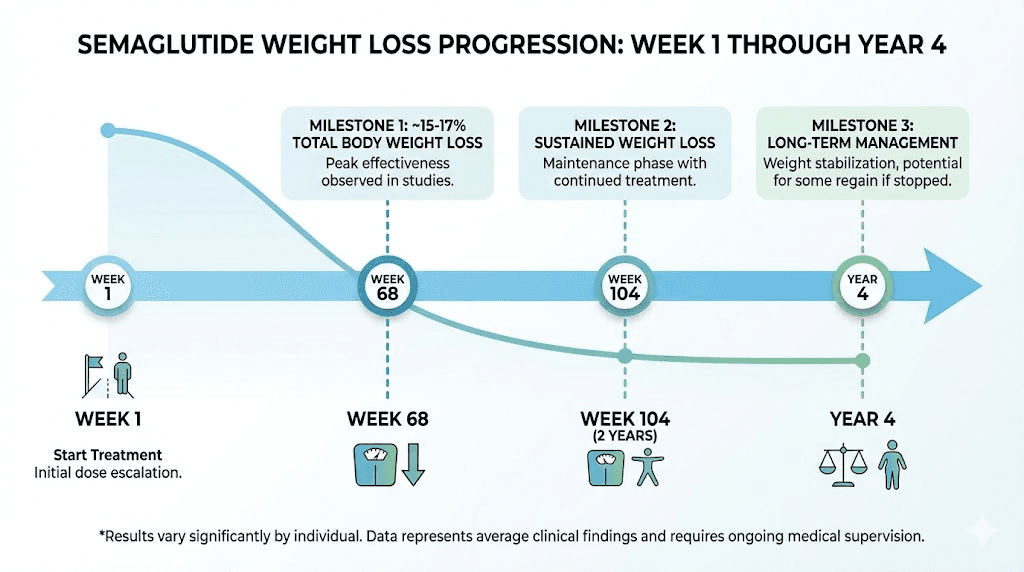
The clinical evidence shows most people stay on semaglutide for at least 68 weeks to achieve significant weight loss. Some continue for years. The real question is not how long you should stay on it, but what happens when you stop, and whether the benefits justify long-term use.
The STEP 1 trial followed 1,961 adults for 68 weeks on semaglutide 2.4mg. Mean weight loss reached 14.9% compared to just 2.4% for placebo. That is nearly 15 pounds for every 100 pounds of starting weight. More importantly, 86.4% of participants achieved at least 5% weight loss, 69.1% hit the 10% mark, and half lost 15% or more.
But the story does not end at 68 weeks.
The STEP 5 trial extended treatment to 104 weeks, two full years. Participants maintained an average weight loss of 15.2% from baseline. Not just maintained, but continued losing weight past the one-year mark. This suggests the medication keeps working as long as you keep taking it, though the rate of loss slows considerably after the initial months.
The SELECT trial took it further. Over 17,604 adults participated for up to four years. Weight loss remained significant at negative 10.2% for the semaglutide group versus negative 1.5% for placebo at the four-year mark. The medication demonstrated not just efficacy but durability over an extended timeline.
Now consider what happens when you stop.
What the weight regain data reveals about stopping treatment
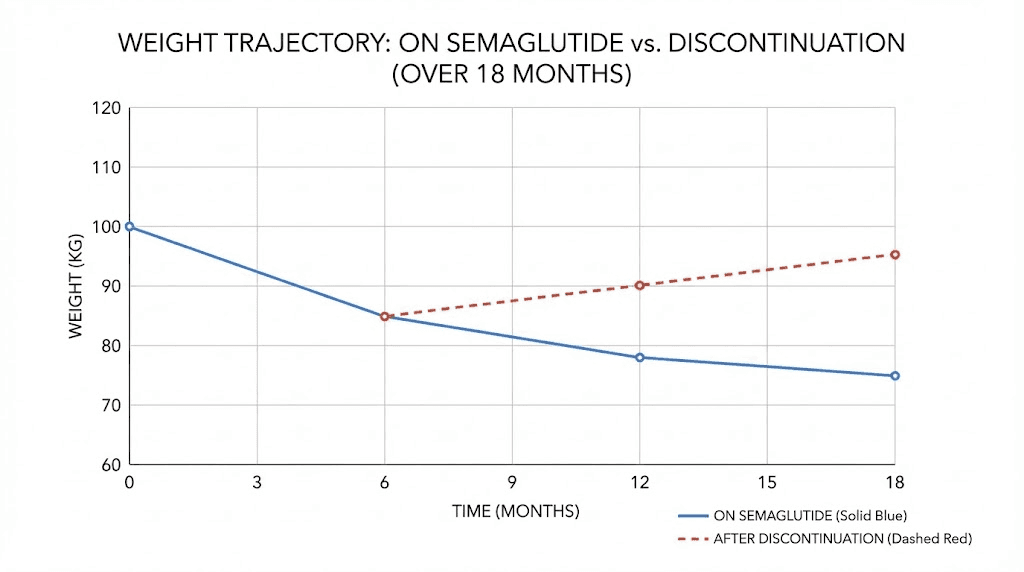
The STEP 1 extension study tracked participants after they discontinued semaglutide. Within one year of stopping, they regained two-thirds of the weight they had lost. The average rate of regain clocked in at 0.8 kilograms per month, roughly 1.8 pounds monthly. Projections suggested a return to baseline weight by approximately 18 months post-treatment.
This is not failure. This is biology.
Semaglutide works by mimicking GLP-1, a hormone that regulates appetite and blood sugar. When you stop injecting synthetic GLP-1, your natural hormone levels resume their previous pattern. The appetite suppression fades. The metabolic adjustments reverse. Your body returns to its prior set point unless you have made substantial lifestyle changes.
Some people view this as evidence that semaglutide is a lifelong commitment. Others see it as a tool for jump-starting weight loss before transitioning to maintenance strategies. Both perspectives have merit depending on your goals, your response to the medication, and your ability to sustain behavioral changes.
The semaglutide withdrawal symptoms add another layer to the stopping equation. Many people experience increased hunger, mood changes, and metabolic shifts when discontinuing treatment. Understanding these effects helps you plan a strategic exit if you choose to stop.
For those comparing options, the semaglutide versus tirzepatide data shows similar weight regain patterns when either medication is discontinued. The issue is not specific to semaglutide but common across GLP-1 receptor agonists.
The semaglutide dosage calculator helps you track your current dose and plan adjustments, but it cannot predict how your body will respond to stopping. That requires understanding your individual metabolic profile and the lifestyle factors that contributed to your initial weight gain.
The dose escalation timeline and what to expect at each phase
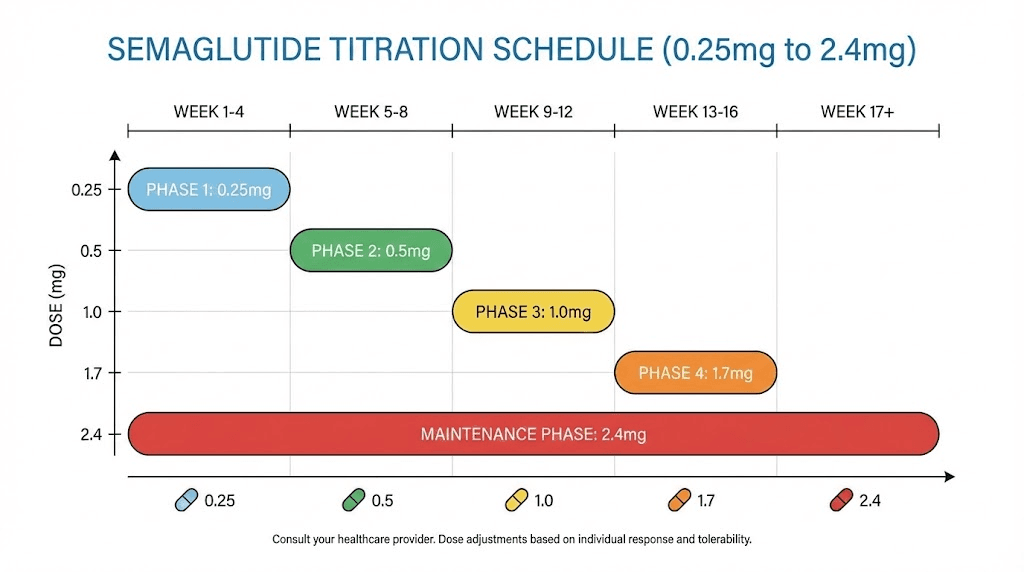
Semaglutide treatment follows a structured escalation schedule designed to minimize side effects while building toward the therapeutic dose. The Wegovy protocol, the FDA-approved formulation for weight loss, uses this progression: 0.25mg for weeks 1 through 4, 0.5mg for weeks 5 through 8, 1.0mg for weeks 9 through 12, 1.7mg for weeks 13 through 16, and finally 2.4mg from week 17 onward.
Each increase challenges your gastrointestinal system. Nausea peaks during the first few days after each dose bump. Some people adapt quickly. Others struggle through the entire four-month ramp-up period.
The 0.25mg starting dose rarely produces significant weight loss. Think of it as priming your system. Your GLP-1 receptors are adjusting to sustained stimulation. Your stomach is learning to empty more slowly. Your pancreas is recalibrating insulin secretion based on this new hormonal signal.
By the time you reach 0.5mg, most people notice reduced appetite. Not dramatic, but noticeable. You might leave food on your plate for the first time in years. Snacking between meals loses its appeal. The constant food thoughts that plagued your waking hours start to quiet down.
The 1.0mg dose is where weight loss accelerates. The how fast does semaglutide work question gets answered here for most people. You are dropping one to two pounds weekly if you are responding well. Your clothes fit differently. People start asking if you have lost weight.
At 1.7mg, some practitioners hold the dose if side effects become problematic. This is the acceptable alternative maintenance dose if you cannot tolerate 2.4mg. Research shows meaningful weight loss occurs at 1.7mg, though not quite as robust as the full dose.
The 2.4mg target dose represents the sweet spot identified through clinical trials. This is where the balance between efficacy and tolerability optimizes for most people. You stay here for the remainder of your treatment, whether that is months or years.
Understanding how many mg is 40 units of semaglutide becomes crucial if you are using compounded medication with insulin syringes instead of pre-filled pens. Dosing errors at higher concentrations can cause severe side effects or waste expensive medication.
The 20 units of semaglutide is how many mg conversion depends on your reconstitution concentration. Most compounding pharmacies use either 2mg per vial or 5mg per vial, dramatically changing the units-to-milligrams ratio.
For those mixing their own medication, how much bacteriostatic water to mix with 10mg semaglutide determines your dosing precision. More dilute solutions offer finer dose adjustments but require larger injection volumes. Concentrated solutions minimize injection volume but increase the risk of dosing errors.
When weight loss peaks and the plateau phenomenon
Most people reach their maximum rate of weight loss between months three and six. The scale drops predictably. Weekly weigh-ins show consistent progress. You start calculating when you will hit your goal weight based on current trends.
Then the plateau hits.
Clinical data shows weight loss typically plateaus around 60 weeks, roughly 14 months into treatment. The rapid losses of the first six months slow to a crawl. Some weeks you lose nothing. Other weeks you gain a pound despite perfect adherence. This is when people panic and assume the medication has stopped working.
It has not stopped working. Your body has adapted.
As you lose weight, your basal metabolic rate decreases. You need fewer calories to maintain your new, lighter body. The caloric deficit that produced rapid initial losses now barely moves the needle. Your body has also upregulated compensatory mechanisms, hunger hormones that try to restore your previous weight.
Semaglutide continues suppressing appetite and regulating blood sugar at the plateau. What changes is the delta between your energy intake and expenditure. The gap narrows as your metabolic rate adjusts downward and your unconscious activity levels may decrease as well.
The why not losing weight on semaglutide question dominates online forums around the one-year mark. People assume they are doing something wrong. Usually, they are simply hitting the physiological wall that all weight loss approaches eventually encounter.
Some practitioners respond by increasing exercise intensity or tightening dietary restrictions. Others add complementary therapies. The best peptides for weight loss include options that target different metabolic pathways, potentially breaking through plateaus when GLP-1 agonism alone stalls.
For those exploring alternatives, switching from tirzepatide to semaglutide or vice versa sometimes restarts progress. The dual GIP and GLP-1 agonism of tirzepatide offers slightly different metabolic effects that may overcome semaglutide resistance.
The plateau does not mean you should stop treatment. STEP 5 trial participants who continued through the plateau maintained their weight loss at 104 weeks. They did not keep losing at the initial rate, but they did not regain weight either. For chronic weight management, maintenance of loss is success.
Why researchers view semaglutide as chronic treatment
The weight regain data changed how endocrinologists think about obesity medication. Before semaglutide, most weight loss drugs were prescribed for short-term use. Take them for six months, lose weight, then stop and maintain through lifestyle changes alone.
That model failed consistently.
Obesity is not a behavior problem. It is a chronic metabolic disease. Your body has regulatory systems that defend a certain weight range, often called the set point. These systems involve dozens of hormones, neural pathways, and feedback loops that resist sustained weight loss.
Semaglutide works by modifying one key component of this regulatory system, the GLP-1 pathway. But it does not reprogram your set point. When you stop the medication, the regulatory system reasserts its original parameters. Your appetite returns. Your metabolic rate stays suppressed from the weight loss. Your body actively works to regain lost weight.
This is why the SELECT trial ran for four years. Researchers wanted to understand long-term outcomes, not just short-term weight loss. The results showed sustained benefit as long as participants continued treatment. Weight loss at four years remained clinically significant. Cardiovascular risk reduction persisted throughout the study period.
The implication is clear. For most people, semaglutide is not a temporary intervention but an ongoing treatment for a chronic condition.
Some patients resist this framing. They view long-term medication use as failure or weakness. This perspective misunderstands the nature of metabolic disease. You would not tell a diabetic to stop insulin after their blood sugar normalized. You would not tell someone with hypertension to discontinue their blood pressure medication once their readings improved.
Obesity follows the same logic. The medication is not a crutch. It is treatment for a physiological condition that will not resolve through willpower alone.
The peptides for weight loss category includes multiple options beyond semaglutide, each with different mechanisms and duration considerations. Some, like AOD 9604 peptide, target fat metabolism directly and may complement GLP-1 therapy for people who plateau.
Understanding how long does it take semaglutide to work helps set realistic expectations for the treatment timeline. Most people see initial effects within two to four weeks, but maximum benefit requires months of consistent use.
For women specifically, peptides for weight loss women considerations include hormonal interactions that may affect treatment duration and efficacy. Estrogen fluctuations can influence GLP-1 sensitivity, potentially requiring dose adjustments over time.
Maintenance dosing strategies after reaching goal weight
You have been on semaglutide for a year. You have lost 60 pounds. Your doctor asks what you want to do next. Continue at 2.4mg indefinitely? Try reducing the dose? Stop completely and see what happens?
This is where clinical practice diverges from clinical trial protocols.
The trials kept participants at their target dose throughout the study period. Real-world practitioners often experiment with dose reduction once patients reach their goal weight. The logic seems sound: you need less appetite suppression to maintain weight loss than to create an ongoing caloric deficit.
Some doctors taper to 1.7mg or even 1.0mg and monitor weight stability. If weight remains stable for several months, they may try further reduction. If weight starts creeping up, they return to the previous effective dose.
No official maintenance dose protocol exists because the research does not support stepping down. The trials that maintained participants at therapeutic doses showed sustained weight loss. The trials that discontinued treatment showed weight regain. No large trials have systematically studied dose reduction for maintenance.
Anecdotal reports suggest some people maintain on lower doses. Others regain weight as soon as the dose drops below 2.4mg. The difference likely relates to individual metabolic factors we do not yet fully understand.
Your natural GLP-1 production matters. Some people have genetic variations that affect GLP-1 secretion and receptor sensitivity. If your baseline GLP-1 function is relatively normal, you might maintain on a lower supplemental dose. If you have significant GLP-1 resistance or deficiency, you probably need the full therapeutic dose indefinitely.
The how long does it take for semaglutide to suppress appetite timeline also varies individually. People who experience rapid appetite suppression might be more sensitive to GLP-1 and potentially able to maintain on lower doses.
Compounded semaglutide introduces additional maintenance considerations. The how long does compounded semaglutide last in the fridge question affects both cost and convenience for long-term users. Most compounded formulations remain stable for 28 to 90 days when refrigerated, requiring regular reorders.
For those concerned about medication longevity, can you use expired semaglutide explores the safety and efficacy trade-offs. While peptides degrade over time, the degradation rate depends on storage conditions and formulation specifics.
Some practitioners combine semaglutide with vitamin B12 for long-term maintenance. The semaglutide with B12 complete guide covers the rationale, which relates to GLP-1 effects on gastric emptying and potential B12 absorption impairment over extended treatment periods.
Long-term safety considerations from four years of data
The SELECT trial provided the longest safety data available for semaglutide at the weight loss dose. No unexpected safety issues emerged over four years of continuous use. This is reassuring but not definitive, as four years is still relatively short for a medication some people may take for decades.
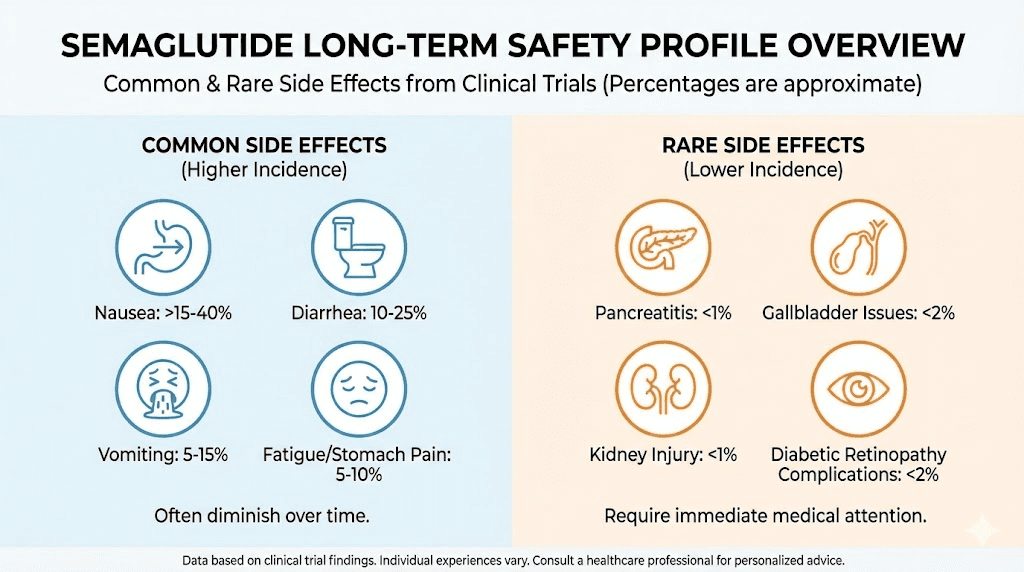
The most common side effects remained gastrointestinal. Nausea, vomiting, diarrhea, and constipation topped the list, particularly during dose escalation. Most participants adapted within weeks of reaching their maintenance dose. Only 16.6% discontinued due to GI symptoms over the entire four-year study period.
Pancreatitis appeared in early animal studies, triggering concerns about long-term pancreatic safety. Human trials showed pancreatitis rates similar to placebo. The theoretical risk exists, but clinical evidence does not support increased incidence with semaglutide use.
Thyroid cancer concerns emerged from rodent studies showing medullary thyroid carcinoma at high doses. Human thyroid cancer incidence in trials remained below 1%, comparable to background rates. The medication carries a black box warning about thyroid C-cell tumors, but no human cases have been definitively linked to GLP-1 agonist use.
Gallbladder issues increase with rapid weight loss regardless of the method used. Semaglutide participants experienced higher rates of gallstones and cholecystitis compared to placebo, but this likely reflects the weight loss itself rather than direct medication toxicity. Any intervention producing 15% weight loss in a year will stress the gallbladder.
Cardiovascular effects proved beneficial in SELECT. The trial demonstrated a 20% reduction in major adverse cardiovascular events, primarily driven by reduced non-fatal heart attacks and strokes. This benefit persisted throughout the four-year study period, suggesting semaglutide does not just help you lose weight but actively protects your cardiovascular system.
Hypoglycemia risk remains low in people without diabetes. Semaglutide enhances glucose-dependent insulin secretion, meaning it only stimulates insulin release when blood sugar is elevated. This mechanism protects against dangerous blood sugar drops that occur with some older diabetes medications.
Bone health data from long-term use remains limited. Rapid weight loss can increase fracture risk through multiple mechanisms, including reduced mechanical loading and potential nutrient deficiencies. No signal for increased fractures appeared in trials, but the participants were relatively young and healthy. Older adults with baseline bone loss might face different risks.
Muscle loss accompanies fat loss with semaglutide, as it does with any caloric deficit. Some estimates suggest 25 to 40% of lost weight comes from lean mass rather than fat. For long-term users, this raises concerns about sarcopenia, particularly in older adults. Resistance training and adequate protein intake become crucial for people staying on semaglutide for years.
The peptides for weight loss and muscle gain article explores strategies for preserving lean mass during GLP-1 therapy. Combining semaglutide with anabolic peptides like ipamorelin or CJC-1295 may help maintain muscle during extended weight loss.
Psychological effects of long-term use deserve consideration. Some people report mood changes, anxiety, or depression when using semaglutide. Whether this stems from the medication itself, the rapid physical changes, or pre-existing conditions remains unclear. Monitoring mental health becomes important for people committing to years of treatment.
The peptide safety and risks overview provides broader context for evaluating long-term peptide therapy. While semaglutide has extensive safety data compared to most peptides, unknowns remain about effects over decades rather than years.
Cost considerations for staying on semaglutide long-term
A one-month supply of branded Wegovy costs between $1,300 and $1,500 without insurance. Multiply that by 12 months and you are looking at $15,600 to $18,000 annually. Extend that over five years and the total exceeds $75,000. Over ten years, you are approaching $150,000.
These numbers stop many people before they start.
Insurance coverage varies dramatically. Some plans cover GLP-1 agonists for weight loss with minimal copays. Others categorize them as cosmetic and refuse coverage entirely. Medicare specifically excludes coverage for weight loss medications, though this may change as cardiovascular benefits become more established.
Compounded semaglutide offers a more affordable alternative. Prices range from $150 to $400 monthly depending on dose and source. Over a year, that is $1,800 to $4,800, still substantial but far less than branded options. Over five years, you are looking at $9,000 to $24,000.
International sourcing presents another cost reduction strategy. Research peptide suppliers sell semaglutide for $50 to $150 per vial, dramatically lower than pharmaceutical pricing. Quality and purity vary widely among suppliers, introducing risk. The best peptide vendors guide helps identify reputable sources, though no research peptide supplier can match pharmaceutical grade manufacturing standards.
Some people start on branded medication, then switch to compounded or research sources once they understand their dose requirements and side effect profile. This approach uses the pharmaceutical product for dose titration when medical support is most critical, then transitions to lower-cost options for maintenance.
The financial calculation changes when you factor in obesity-related health costs. Type 2 diabetes, cardiovascular disease, sleep apnea, and joint problems all carry their own treatment expenses. If semaglutide prevents or delays these conditions, the medication may save money over time despite its high upfront cost.
For those exploring alternatives, tirzepatide before and after results show slightly greater weight loss than semaglutide, potentially offering better value despite similar or higher costs. The cost-effectiveness depends on whether the additional weight loss translates to greater health improvements.
The peptide cost calculator helps estimate long-term expenses based on your specific dosing protocol. Seeing the total cost over one, five, or ten years forces you to confront the financial commitment of chronic treatment.
Some employers now offer GLP-1 coverage as part of wellness programs, recognizing that supporting weight loss may reduce long-term insurance claims. If your employer does not currently cover these medications, advocating for their inclusion could benefit you and coworkers facing similar challenges.
Signs you should adjust your treatment approach
You have been on semaglutide for six months. Your weight loss has stalled for eight weeks. You feel fine, no side effects, but the scale will not budge. Do you stay the course? Increase the dose? Add something else? Stop entirely?
Plateau after initial success is normal, not a signal to change course. But other situations demand adjustments.
Persistent nausea that prevents adequate nutrition means your dose is too high or escalated too quickly. Dropping back to the previous dose for a few weeks often resolves the issue. Some people need eight weeks at each dose level instead of four. There is no prize for reaching 2.4mg quickly if you cannot tolerate it.
Severe constipation lasting more than a week despite fiber, hydration, and exercise interventions may require dose adjustment. While constipation is common with GLP-1 agonists, it should respond to standard remedies. Persistent cases sometimes improve with dose reduction.
Unusual fatigue that interferes with daily function deserves investigation. Semaglutide should not cause significant fatigue, though inadequate caloric intake might. If you are eating so little that your energy crashes, you may need nutritional counseling rather than medication adjustment.
Hair loss affects some people on GLP-1 agonists. The GLP-1 hair loss complete guide explores mechanisms and solutions. Rapid weight loss itself causes telogen effluvium, temporary hair shedding that resolves after weight stabilizes. But ongoing hair loss after reaching maintenance suggests the medication may be contributing.
Mood changes, particularly depression or severe anxiety, require immediate evaluation. While not common, some people experience significant psychological effects on semaglutide. The benefit of weight loss does not justify deteriorating mental health.
Financial strain that affects your ability to pay for housing, food, or other essentials means you need a more affordable approach. Compounded options, international sources, or alternative medications might provide similar benefits at lower cost. The cheap compounded tirzepatide shots guide explores budget-friendly GLP-1 alternatives.
Complete absence of appetite suppression after reaching 2.4mg for at least four weeks suggests you may not respond to semaglutide. Some people have genetic variations affecting GLP-1 receptor sensitivity. For non-responders, tirzepatide may work better due to its dual GIP and GLP-1 mechanism.
Weight loss exceeding two pounds weekly after the first month might seem like good news, but it increases risks. Rapid loss raises gallstone risk, increases muscle loss, and may cause nutrient deficiencies. If you are losing weight too quickly despite reasonable food intake, consider whether your dose is higher than necessary.
Alternative and complementary approaches to extend treatment benefits
Semaglutide works best as part of a comprehensive strategy, not a solo intervention. What you do alongside the medication determines both your success during treatment and your outcome if you eventually stop.
Resistance training preserves muscle mass during weight loss. Two to three sessions weekly targeting major muscle groups can cut muscle loss from 40% of total weight lost down to 20% or less. The peptides for weight loss and muscle gain article details how to combine exercise with peptide therapy for optimal body composition.
Protein intake becomes critical when combining caloric restriction with GLP-1 agonists. Aim for 1.2 to 1.6 grams per kilogram of body weight daily, potentially higher if you are resistance training intensively. The appetite suppression makes hitting protein targets difficult, requiring deliberate meal planning.
Some practitioners add other peptides to address semaglutide limitations. Tesofensine targets norepinephrine, dopamine, and serotonin reuptake, potentially enhancing fat loss through a different mechanism. 5-Amino-1MQ affects cellular energy production and may complement GLP-1 therapy for metabolic enhancement.
For stubborn fat deposits, FTPP peptide adipotide or lemon bottle peptide offer targeted fat reduction approaches. These work locally rather than systemically, addressing areas that resist overall weight loss.
Metabolic rate preservation matters for long-term success. As you lose weight, your metabolic rate drops both from having less body mass and from adaptive thermogenesis, your body actively reducing energy expenditure to defend against further loss. Peptides for energy might help counter this metabolic slowdown.
Behavioral therapy addresses the psychological factors driving overeating. Semaglutide eliminates physical hunger but does not touch emotional eating, stress eating, or habitual eating patterns. Working with a therapist who specializes in weight management helps develop coping strategies that persist after medication stops.
Sleep optimization affects both weight loss success and long-term maintenance. Poor sleep disrupts ghrelin and leptin, hormones regulating appetite and satiety. Seven to nine hours of quality sleep nightly supports semaglutide effectiveness and helps maintain weight loss after treatment ends.
Some people explore Ozempic alternatives if semaglutide becomes unavailable or unaffordable. Options include other GLP-1 agonists, GLP-1/GIP dual agonists, and emerging triple agonists like retatrutide.
For women experiencing menopausal weight gain, peptides for menopause weight loss addresses hormonal factors that may require additional support beyond GLP-1 agonism alone. Estrogen decline affects fat distribution and metabolic rate in ways semaglutide does not fully address.
How to make an informed decision about treatment duration
The decision to stay on semaglutide long-term comes down to individual factors. Your response to the medication matters. Your ability to maintain lifestyle changes matters. Your financial situation matters. Your tolerance for side effects matters. Your underlying health conditions matter.
Start by clarifying your goals. Are you trying to lose weight for a specific reason with a defined timeline? Then a 68-week course might suffice, accepting likely regain afterward. Are you managing obesity as a chronic disease? Then indefinite treatment makes more sense.
Assess your response after six months. Did you lose significant weight? Was the rate of loss acceptable? Did side effects remain manageable? If you answered yes to all three, continuing treatment is reasonable. If you struggled through six months with minimal weight loss and persistent side effects, semaglutide may not be the right medication for you.
Consider your lifestyle change trajectory.
Have you developed sustainable eating habits? Do you exercise regularly? Have you addressed the psychological factors that contributed to weight gain? Strong lifestyle foundations increase the odds you can maintain weight loss after stopping medication.
Factor in cardiovascular considerations. If you have established cardiovascular disease or high risk, the SELECT trial data suggests staying on semaglutide provides ongoing protection. The 20% reduction in major adverse cardiovascular events justifies long-term use even independent of weight loss effects.
Financial sustainability cannot be ignored. Can you afford this medication for years? If the answer is no, plan your exit strategy during treatment. Build habits and metabolic resilience while the medication provides a metabolic advantage.
Discuss dose reduction experiments with your provider once you reach goal weight and maintain it for several months. Trying a lower dose while monitoring weight and appetite gives you data about your minimum effective dose. Some people discover they can maintain on less than the maximum therapeutic dose.
Plan the discontinuation carefully if you choose to stop. Gradual taper reduces rebound effects. Some practitioners step down from 2.4mg to 1.7mg for a month, then to 1.0mg for a month, then to 0.5mg for a month before stopping completely. This gives your body time to adjust at each stage.
The peptide calculator helps plan dosing adjustments whether you are titrating up or tapering down. Precise calculations matter when working with compounded medication and insulin syringes.
Understanding peptide cycle planning provides a framework for strategic treatment periods, breaks, and adjustments. While semaglutide is not typically cycled like some peptides, the principles of intentional dosing strategies apply.
For comprehensive context, getting started with peptides covers foundational concepts that inform long-term treatment decisions across all peptide therapies, not just GLP-1 agonists.
Comparing semaglutide duration to other weight loss peptides
Semaglutide is not the only peptide used for weight loss, and treatment duration expectations vary across different compounds. Understanding these differences helps contextualize the long-term commitment semaglutide typically requires.
Tirzepatide follows a similar chronic treatment model to semaglutide. The SURMOUNT trials ran for 72 weeks with similar weight regain patterns after discontinuation. Switching between tirzepatide and semaglutide does not fundamentally change the duration question, both are long-term therapies.
AOD 9604 represents a different approach. This fragment of growth hormone specifically targets fat metabolism without affecting blood sugar or appetite. Treatment protocols typically run 12 to 16 weeks rather than indefinitely. The mechanism differs enough that comparing treatment duration to GLP-1 agonists is somewhat meaningless.
Tesofensine affects neurotransmitter reuptake and shows promise for weight loss in trials ranging from 24 to 52 weeks. Long-term safety data remains limited compared to semaglutide. Whether it would require indefinite use to maintain weight loss has not been established definitively.
The best peptide stack for weight loss often combines short-acting fat loss compounds with longer-term metabolic modulators. A stack might include semaglutide as the foundation with 8 to 12-week cycles of other peptides layered on top to break through plateaus.
For visceral fat specifically, peptides targeting visceral fat loss include compounds that may require shorter treatment durations than GLP-1 agonists. But visceral fat is metabolically active and quickly regenerates after treatment stops without ongoing intervention.
Lipotropic peptides support fat metabolism and liver function but rarely produce significant weight loss alone. These are typically used as adjuncts to primary weight loss strategies rather than standalone treatments with defined duration protocols.
Growth hormone secretagogues like ipamorelin and sermorelin indirectly support fat loss through enhanced growth hormone production. Treatment typically runs three to six months before taking breaks to prevent desensitization. These are not weight loss medications per se but metabolic optimizers.
The emerging triple agonist retatrutide shows even greater weight loss than semaglutide or tirzepatide in early trials. The retatrutide dose schedule follows a similar escalation pattern, suggesting it will likely require long-term use for sustained benefit. The retatrutide cost remains unclear as it awaits FDA approval, but will likely match or exceed semaglutide pricing.
Combination therapy represents another approach. Cagrilintide and semaglutide together produce greater weight loss than semaglutide alone. The CagriSema dosing protocol will likely follow a chronic treatment model similar to semaglutide alone.
Cagrilintide weight loss results show promise, though cagrilintide side effects include significant nausea that may limit long-term adherence. Cagrilintide dosing when used alone or in combination requires careful titration.
The broader amylin receptor agonist class, which includes cagrilintide, offers another mechanism for long-term weight management. These compounds complement rather than replace GLP-1 agonists, potentially allowing lower doses of each for equivalent efficacy.
Special considerations for different populations
Treatment duration considerations shift based on age, sex, and underlying health conditions. A 65-year-old with type 2 diabetes faces different risks and benefits than a 35-year-old without metabolic disease.
Older adults may benefit most from long-term semaglutide use due to cardiovascular protection. The SELECT trial included participants with established cardiovascular disease, many in their 60s and 70s. The 20% reduction in heart attacks and strokes becomes increasingly valuable as baseline risk rises with age.
But older adults also face greater risks from muscle loss. Sarcopenia, age-related muscle wasting, accelerates during caloric restriction. Combining semaglutide with resistance training becomes critical for older users. Some may need to accept less total weight loss in exchange for preserving functional capacity and independence.
Women face unique considerations. Hormonal fluctuations affect GLP-1 sensitivity across the menstrual cycle. Some women report increased appetite and reduced semaglutide effectiveness during certain cycle phases. This may necessitate dose adjustments or acceptance of more variable weight loss patterns.
The best peptides for women account for these hormonal factors. Peptides for women over 40 specifically address perimenopause and menopause, when metabolic changes often trigger weight gain resistant to diet and exercise alone.
Men typically lose weight faster on semaglutide than women, likely due to higher baseline muscle mass and metabolic rate. The peptides for men complete guide covers male-specific optimization strategies. Men before and after tirzepatide demonstrates typical male response patterns that apply broadly to GLP-1 agonists.
People with type 2 diabetes have the strongest case for indefinite semaglutide use. The medication provides dual benefit, weight loss plus glycemic control. Stopping medication means managing diabetes through other means, often requiring multiple medications with their own side effects and costs.
Practical strategies for staying on treatment long-term
Committing to years of weekly injections requires systems and strategies beyond just filling your prescription. People who succeed long-term develop routines that make adherence automatic rather than requiring constant willpower.
Choose a consistent injection day and time. Most people pick Sunday evening or Monday morning to start the week. The regularity matters more than the specific day. Calendar reminders help until the habit solidifies.
Rotate injection sites to minimize tissue irritation. Abdomen, thighs, and upper arms all work. Some people develop injection site reactions or lipohypertrophy, thickened fat deposits where repeated injections occur. Systematic rotation prevents these issues.
Stock up on supplies during shortages. Semaglutide has experienced multiple supply disruptions. Having a month or two extra on hand protects against forced discontinuation during shortages. The how long does compounded semaglutide last in the fridge information helps you understand storage limits.
Track your doses, weight, and side effects. Simple spreadsheet or app tracking creates accountability and helps identify patterns. You might notice side effects cluster around certain cycle phases or after specific foods. This data informs dose adjustments and lifestyle modifications.
The peptide reconstitution calculator becomes essential if using compounded medication. Correct reconstitution ensures accurate dosing and optimal peptide stability.
Understanding how to reconstitute peptides and how to mix peptides with bac water ensures you prepare your medication correctly every time. The bacteriostatic water for peptides guide covers proper water selection and storage.
Knowing how much bacteriostatic water to add to peptides prevents concentration errors that could lead to under or overdosing.
Plan for travel. Semaglutide requires refrigeration, though it tolerates room temperature for up to 28 days in most formulations. Small insulin cooler bags maintain appropriate temperature during travel.
The peptide storage guide covers optimal storage conditions. How long do peptides last in the fridge and how long do peptides last at room temperature provide specific stability data.
Understand do peptides expire to make informed decisions about medication that approaches expiration dates.
Build a support system. Online communities of long-term users share strategies, troubleshoot problems, and provide encouragement. Regular check-ins help you stay on track.
Work with a knowledgeable healthcare provider. Not all doctors understand long-term semaglutide use. Find someone who views obesity as a chronic disease requiring ongoing management, not a character flaw requiring short-term intervention. The peptide therapy near me guide helps locate practitioners experienced with peptide therapies.
Emerging alternatives that may change duration considerations
The GLP-1 agonist space is evolving rapidly. Compounds in development may offer advantages over semaglutide that change the treatment duration calculus.
Oral semaglutide offers convenience over weekly injections. The oral tirzepatide complete guide explores oral GLP-1 formulations. Daily pills seem easier to maintain long-term than weekly injections for some people, though others prefer the once-weekly approach.
Triple agonists like retatrutide add GIP and glucagon agonism to GLP-1 effects. Early data shows 24% weight loss over 48 weeks, substantially exceeding semaglutide results. Whether this translates to shorter necessary treatment duration or simply greater maximum weight loss remains to be seen.
The mazdutide versus tirzepatide comparison explores another dual agonist. As more compounds reach market, identifying which works best for each individual becomes possible, potentially optimizing both efficacy and duration.
Patches and other delivery systems could change adherence. The Onmorlo GLP-1 patches represent one attempt at needle-free delivery. While current patch technology does not match injection efficacy, improvements may create viable alternatives.
Several proprietary formulations claim enhanced effects. The Thrive GLP-1, Evolv GLP-1, and MMIT GLP-1 products market themselves as optimized formulations. Whether these offer meaningful advantages over standard semaglutide remains unproven.
For general peptide therapy context, what are peptides and how peptides work provide foundational understanding. The longevity peptides article explores broader health optimization strategies that may reduce the need for weight loss medications altogether.
The HGH alternatives category includes peptides that may complement GLP-1 therapy for body composition improvement, potentially allowing lower semaglutide doses or shorter treatment duration by enhancing muscle retention during weight loss.
Frequently asked questions
Can you stay on semaglutide for life?
Current evidence supports safe use for at least four years based on the SELECT trial. No data exists beyond four years, but the safety profile suggests longer use is likely safe for most people. Many endocrinologists view semaglutide as appropriate for lifelong use given obesity is a chronic condition. Individual factors like side effects, cost, and response to treatment determine whether lifelong use makes sense for you specifically.
What happens if you stop semaglutide after one year?
Research shows most people regain two-thirds of lost weight within one year of stopping. The average regain rate is 0.8 kilograms monthly, about 1.8 pounds per month. Without continued treatment or significant lifestyle changes, weight typically returns to near baseline by 18 months post-discontinuation. Understanding semaglutide withdrawal symptoms helps you prepare for what to expect.
Is there a maintenance dose of semaglutide?
No official maintenance dose protocol exists. Clinical trials maintained participants at the full therapeutic dose of 2.4mg weekly. Some practitioners experiment with dose reduction to 1.7mg or 1.0mg after reaching goal weight, but this lacks formal study. Use the semaglutide dosage calculator to track your dosing adjustments.
How long does it take to reach maximum weight loss on semaglutide?
Most people reach peak weight loss between 60 and 68 weeks, roughly 14 to 16 months. Weight loss is most rapid in the first six months, then gradually slows. The STEP 5 trial showed continued loss out to 104 weeks in some participants. Learn more about the semaglutide weight loss timeline.
Can you take breaks from semaglutide?
Taking breaks is not recommended based on current evidence. Weight regain begins within weeks of stopping. No research supports intermittent dosing protocols. If cost or side effects necessitate breaks, expect weight regain during off periods. Some people use lower doses during breaks rather than complete discontinuation, but this strategy lacks clinical validation.
Does semaglutide stop working after a while?
Semaglutide continues working as long as you take it, but the rate of weight loss slows over time. This plateau reflects metabolic adaptation, not medication failure. Your appetite suppression and blood sugar regulation persist. If you feel the medication has completely stopped working, check our guide on why you are not losing weight on semaglutide.
How long should you try semaglutide before deciding it does not work?
Give it at least six months at the full 2.4mg dose before concluding it does not work for you. If you have lost less than 5% of body weight after six months at maximum dose with good adherence, you may be a non-responder. Consider switching to tirzepatide or exploring other weight loss peptide options.
Is it safe to stay on semaglutide while trying to get pregnant?
No. Stop semaglutide at least two months before attempting conception. Animal studies show potential fetal harm, and no human pregnancy data exists. The medication clears your system within weeks, but allowing two months provides a safety margin. Discuss preconception planning with your doctor.
External resources
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed dosing guides, stacking protocols, and research summaries that go far beyond what any single article can cover.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay accurate, your weight loss stay sustained, and your treatment decisions stay informed.