Feb 5, 2026

Some people feel it within 48 hours. Others wait two weeks. A few wonder if the medication is working at all. The timeline for tirzepatide appetite suppression is not one-size-fits-all, and that uncertainty drives a lot of people to search for answers they should have gotten from their provider on day one.
Here is the reality. Tirzepatide is a GLP-1 and GIP dual receptor agonist. It works on two separate pathways in your body, not just one like semaglutide. That dual mechanism means appetite suppression often hits faster and harder, but it also means individual variation plays a bigger role than most guides acknowledge. Your starting dose, your metabolic baseline, your relationship with food, even your sleep quality can shift the timeline by days or weeks.
This guide breaks down exactly what to expect at every stage. Week by week, dose by dose, mechanism by mechanism. You will learn why some people feel full after their very first injection while others need eight weeks and a dose increase before anything clicks. More importantly, you will learn what to do if appetite suppression has not kicked in yet, when to be patient, and when to talk to your provider about adjustments. SeekPeptides has tracked thousands of research protocols, and the patterns are clear once you know what to look for.
How tirzepatide suppresses appetite at the cellular level
Understanding the mechanism matters. Not because you need a biology degree to use tirzepatide, but because understanding how it reduces hunger helps you set realistic expectations for when it will reduce hunger.
Tirzepatide is a synthetic 39-amino acid peptide that activates two receptors simultaneously. The GLP-1 receptor and the GIP receptor. Both are incretin hormones, meaning they are naturally released by your gut after you eat. The medication mimics and amplifies what your body already does, just with greater intensity and duration.
The GLP-1 pathway
GLP-1 receptor activation is the better-understood half of the equation. When tirzepatide binds to GLP-1 receptors in the brain, particularly in the hypothalamus and brainstem, it sends powerful satiety signals. You feel full sooner. You stay full longer. The constant background hum of hunger that drives snacking and overeating gets turned down, sometimes dramatically.
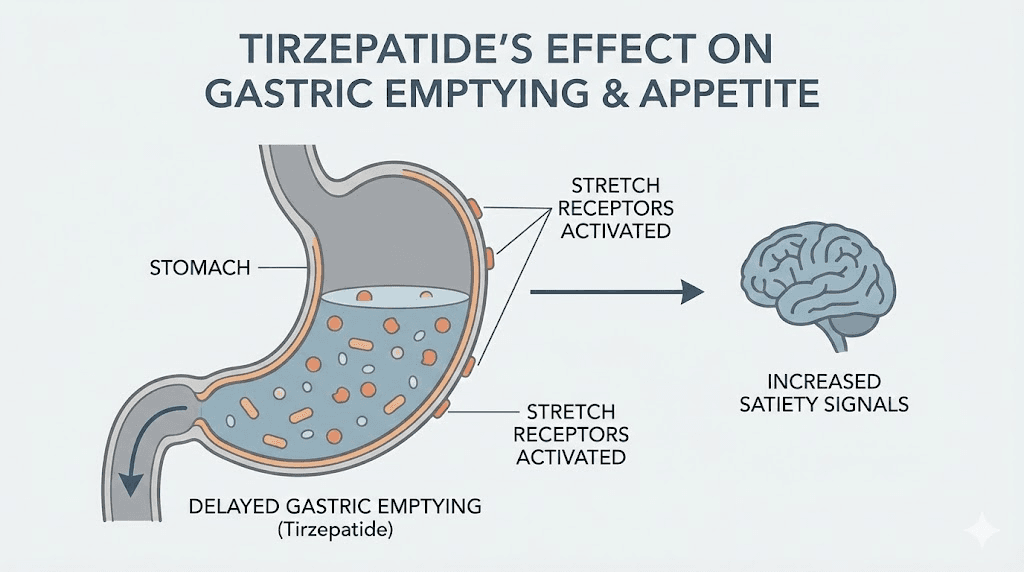
But GLP-1 does more than talk to your brain. It slows gastric emptying, the rate at which food leaves your stomach. When food sits in your stomach longer, stretch receptors keep firing satiety signals. This is why many people on tirzepatide report feeling uncomfortably full from portions that used to feel normal. The stomach is not broken. It is just not emptying as fast as it used to.
Research published in the Journal of Clinical Endocrinology and Metabolism confirmed that gastric emptying delay is most pronounced after the first dose. After that, the body partially adapts through a process called tachyphylaxis. The delay remains clinically meaningful, but it softens. This is actually a good thing. The initial intense fullness often comes with nausea, and the partial adaptation reduces side effects while maintaining enough gastric slowing to support appetite control.
The GIP pathway
This is where tirzepatide separates itself from every GLP-1 only medication on the market. Glucose-dependent insulinotropic polypeptide acts through separate receptors in the brain, gut, and adipose tissue. GIP receptors in the central nervous system influence energy balance, fat metabolism, and food reward processing.
The combination matters. A lot.
In clinical comparisons, tirzepatide produced greater weight loss than semaglutide at comparable doses. The SURPASS trials demonstrated that tirzepatide 15mg achieved up to 22.5% body weight reduction in participants with obesity, compared to approximately 15-17% with semaglutide 2.4mg in the STEP trials. While direct appetite comparisons showed similar subjective hunger scores, the superior weight outcomes suggest GIP adds something beyond what appetite questionnaires capture.
One leading theory is that GIP receptor activation improves fat utilization and lipid clearance. When your body processes dietary fat more efficiently, the metabolic signals that drive hunger are altered even before you consciously register feeling different.
This could explain why some tirzepatide users report that their relationship with food changes before they notice traditional appetite suppression, they just stop thinking about food as much.

The nucleus accumbens and food noise
Recent research from Penn Medicine revealed something fascinating about how tirzepatide affects the brain reward center. The nucleus accumbens, a region strongly linked to impulsiveness, pleasure-seeking, and what patients now call "food noise," shows reduced signaling under tirzepatide treatment.
Food noise is that constant mental chatter about eating. What to eat next. When lunch is. Whether there are snacks in the kitchen. For people with obesity, this noise can be relentless and exhausting. Tirzepatide appears to quiet it by dampening reward-center activity tied to food cues.
But here is the important caveat. The Penn research also found these effects may be temporary. In one case, nucleus accumbens activity returned to pre-treatment patterns after about five months, even while the patient continued medication. The food noise broke through. This does not mean tirzepatide stops working, it means appetite suppression is multifaceted. The gastric emptying effects and hypothalamic signaling continue. But the reward-center component may wax and wane.
Why does this matter for your timeline? Because the type of appetite suppression you experience first, whether it is physical fullness, reduced cravings, or silenced food noise, depends on which mechanism activates most strongly in your individual neurobiology. And that varies person to person.
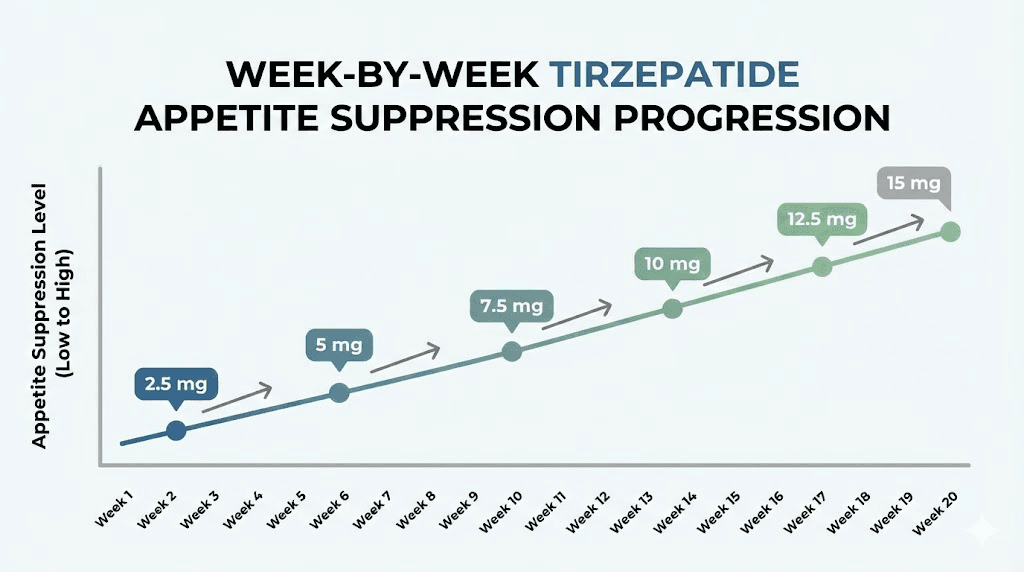
Week-by-week appetite suppression timeline
Let us walk through what most people experience at each stage. Remember, this is a general framework based on clinical data and thousands of reported experiences. Your timeline may be faster or slower, and both are normal.
Days 1-3: the first injection
The starting dose is 2.5mg. This is intentionally subtherapeutic for appetite suppression. Its primary purpose is to let your body adjust to the medication and minimize gastrointestinal side effects.
Some people feel appetite changes within the first 24-48 hours anyway. This early response is driven primarily by gastric emptying delay, which is strongest after the very first dose. You might eat a normal-sized meal and feel uncomfortably full. You might notice that your usual afternoon snack does not sound appealing. Or you might feel absolutely nothing different.
All three responses are normal at this stage.
The people who feel strong effects on day one often have higher baseline sensitivity to incretin hormones. Their receptors respond robustly to even the low 2.5mg dose. The people who feel nothing are not non-responders. They simply need higher doses to reach their threshold.
Week 1: settling in
By the end of the first week, roughly 30-40% of users report some degree of appetite change. It is usually subtle. Not the dramatic "I forgot to eat" experience people describe later, but a gentle nudging. Portions feel slightly more satisfying. The urge to eat between meals softens a little.
Nausea is common during this first week and can confuse the picture. Some people mistake medication-induced nausea for appetite suppression. The distinction matters. True appetite suppression feels like genuine satisfaction with less food. Nausea-related appetite loss feels like you could eat but eating sounds unpleasant. The first is sustainable. The second fades as your body adjusts.
If you are experiencing nausea, eating smaller meals, avoiding high-fat foods, and staying hydrated can help. These are not just comfort measures. They also give tirzepatide a better metabolic environment to work in.
Weeks 2-4: the adjustment period
You are still on 2.5mg during this phase. The FDA-approved dosing protocol keeps you at 2.5mg for the first four weeks before any increase.
During weeks two through four, nausea typically subsides or becomes manageable. As it does, some users notice their appetite creeping back up slightly. This does not mean the medication is failing. The initial gastric emptying delay softens through tachyphylaxis, and 2.5mg is not a therapeutic appetite-suppression dose for most people.
About 50-60% of users report meaningful appetite changes by the end of week four, ranging from mild to moderate. The changes look like this: smaller portions feel satisfying, cravings for hyperpalatable foods decrease, thinking about food becomes less frequent, and the gap between meals stretches naturally without deliberate effort.
The other 40-50% are waiting for a dose increase. And that is completely expected. You are not behind schedule.
Weeks 5-8: the first real dose (5mg)
At week five, the dose increases to 5mg. For many people, this is when appetite suppression truly kicks in. The jump from 2.5mg to 5mg doubles the receptor activation, and the clinical data reflects this.
This is the inflection point.
In the SURMOUNT-1 trial, even the 5mg group, the lowest therapeutic dose, achieved 16% body weight reduction over 72 weeks. That result requires significant and sustained appetite reduction. Most of that appetite effect begins emerging during this 5mg phase.
What people describe at this stage: eating half a plate and feeling done. Walking past the break room without thinking about what is in there. Cooking dinner and not picking at food while preparing it. The food noise getting quieter. Not silent, but quieter.
Physically, gastric emptying delay re-intensifies with the dose increase. You may notice a brief return of nausea for a few days. This is temporary and typically milder than the initial 2.5mg nausea because your body has already partially adapted to the medication class.
By the end of week eight, approximately 70-80% of users report clinically meaningful appetite suppression. If you are in this group, the medication is working. Stay the course.
Weeks 9-12: building momentum (7.5mg)
The optional increase to 7.5mg happens at week nine if your provider determines you need additional appetite control or weight loss. Not everyone moves to this dose. Some people achieve excellent results at 5mg and stay there.
For those who do increase, 7.5mg often deepens the appetite suppression experience. The difference between 5mg and 7.5mg is typically described as going from "I eat less" to "I have to remind myself to eat." Hunger signals become genuinely faint. Meals become functional rather than event-driven.
The SURMOUNT-1 data shows an interesting pattern here. Researchers categorized participants as "early responders" (5% or more weight loss by week 12) and "late responders" (less than 5% by week 12). A full 82% were early responders. But here is the critical finding for late responders: 90% of people who had less than 5% weight loss at week 12 still achieved clinically meaningful weight reduction by week 72.
That means if you are at week 12 and feel like things are moving slowly, the data overwhelmingly supports continuing. Late response does not predict failure.
Weeks 13-20: optimization phase (10mg-12.5mg)
Dose escalation continues through 10mg (week 13) and 12.5mg (week 17) for patients who need it. Each increase follows the same pattern: a brief intensification of appetite suppression and possible mild GI side effects, followed by stabilization at a new, more effective baseline.
At these higher doses, appetite suppression is typically robust. The tirzepatide dosing protocol allows increases only if clinically needed, so not everyone reaches 10mg or higher. Your provider evaluates your response at each step.
The dual mechanism really shines at these mid-to-high doses. GLP-1 mediated satiety is strong. GIP-mediated metabolic improvement is measurable. Food noise, for most people, is significantly reduced. Many patients report that eating has transformed from an emotional activity to a practical one. They eat because they need fuel, not because food is calling to them.
Week 21 and beyond: maximum dose (15mg)
The maximum approved dose of 15mg represents the ceiling of the dose escalation schedule. At this level, appetite suppression is typically at its peak. The SURMOUNT-1 trial showed 22.5% body weight reduction in the 15mg group over 72 weeks.
By this stage, the people who will respond to tirzepatide have responded. Appetite patterns are established. Weight loss is measurable and ongoing, though the rate often slows as you lose more weight and your metabolic rate adjusts downward.
An important note about this phase: appetite suppression is not always constant. Most users experience fluctuations. Some weeks the medication feels incredibly powerful. Other weeks, hunger creeps back a bit. This is normal. Hormonal cycles, stress, sleep disruption, illness, and even seasonal changes can modulate how strongly tirzepatide affects your appetite on any given day.
The medication is still working. The fluctuations happen on top of a baseline that is significantly lower than your pre-treatment hunger level.
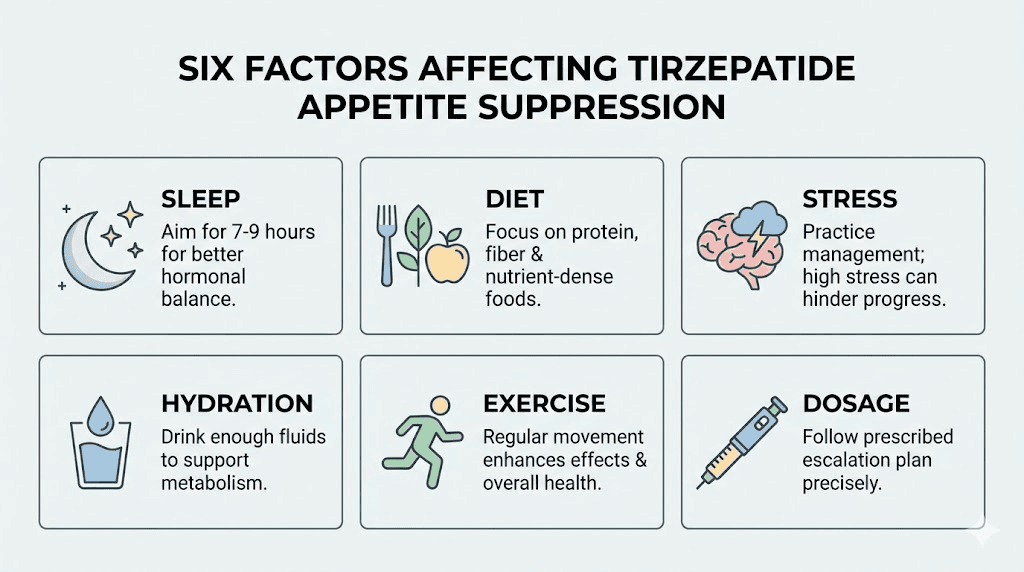
Factors that affect how quickly tirzepatide suppresses your appetite
Not everyone follows the textbook timeline. Here is why.
Starting dose and escalation speed
The standard escalation moves 2.5mg every four weeks. Some providers prescribe faster escalation for patients who tolerate the medication well. Others slow the schedule down for patients with significant GI sensitivity. A slower escalation means slower onset of appetite suppression. A faster escalation can mean quicker results but higher risk of nausea, vomiting, and diarrhea.
The FDA labeling is clear: increases should occur no faster than every four weeks, and only by 2.5mg increments. Providers who deviate from this do so based on clinical judgment.
Body composition and metabolic health
Your starting point matters more than most guides acknowledge. People with higher baseline body fat percentages often have greater insulin resistance, altered incretin signaling, and blunted hormonal responses. This can mean a slower onset of appetite suppression.
Conversely, people with moderate overweight and relatively preserved metabolic function sometimes respond dramatically to even low doses. Their incretin system is closer to normal, so augmenting it with tirzepatide produces quick, noticeable changes.
Underlying conditions play a role too. Hypothyroidism, PCOS, hormonal imbalances, and chronic inflammation can all slow the response. These are not reasons to stop treatment. They are reasons to work with your provider on a comprehensive approach that addresses the underlying condition alongside tirzepatide use.
Sleep quality
This one surprises people. Poor sleep increases ghrelin (the hunger hormone) and decreases leptin (the satiety hormone). These hormonal shifts work directly against tirzepatide mechanism of action. If you are sleeping five hours a night, you are fighting the medication with your lifestyle.
Research consistently shows that sleep-deprived individuals experience more hunger, stronger cravings for high-calorie foods, and greater reward-center activation in response to food cues. Tirzepatide can partially overcome these effects, but it has to work harder. The result: slower onset and weaker appetite suppression.
Seven to nine hours of quality sleep is not optional when using appetite-suppressing medications. It is a force multiplier.
Dietary composition
What you eat affects how well tirzepatide controls your appetite. High-protein meals enhance the medication effects because protein naturally stimulates GLP-1 and GIP release from the gut. You are essentially doubling down on the same pathways tirzepatide activates.
Ultra-processed foods, particularly those high in sugar and refined carbohydrates, can partially counteract appetite suppression. These foods trigger dopamine release in the reward center, the same nucleus accumbens that tirzepatide is trying to quiet. You are pressing the gas and the brake at the same time.
A diet built around lean proteins, vegetables, healthy fats, and whole grains gives tirzepatide the best biochemical environment to suppress appetite effectively.
Hydration status
Dehydration is commonly mistaken for hunger. When tirzepatide slows gastric emptying, adequate hydration becomes even more important. Water helps move food through the digestive tract, reduces constipation (a common side effect), and supports the metabolic processes that tirzepatide enhances.
Aim for at least 64 ounces of water daily. More if you are physically active or live in a hot climate.
Physical activity
Exercise improves insulin sensitivity, which supports tirzepatide mechanism of action. It also influences hunger hormones independently. Moderate exercise tends to reduce appetite in the hours following activity. Intense exercise can temporarily increase hunger but improves overall metabolic health.
The sweet spot for most tirzepatide users is consistent moderate activity: walking, light resistance training, swimming. Enough to support metabolic health without triggering compensatory hunger that the medication then has to fight.
Stress and cortisol
Chronic stress elevates cortisol, which directly stimulates appetite and promotes fat storage, particularly visceral fat. Cortisol-driven hunger is a different beast than normal physiological hunger. It drives cravings for comfort foods, emotional eating, and reward-seeking behavior.
Tirzepatide addresses physiological hunger signals brilliantly. Stress-driven hunger is a different pathway. If chronic stress is a factor in your life, addressing it through stress management, therapy, or lifestyle changes will significantly improve how quickly and effectively tirzepatide suppresses your overall appetite.
Medications and interactions
Certain medications can interfere with tirzepatide appetite-suppressing effects. Corticosteroids increase hunger. Some antidepressants cause weight gain. Insulin and sulfonylureas can cause hypoglycemia that triggers compensatory eating. Antihistamines may increase appetite.
If you are taking medications that promote hunger or weight gain, discuss this with your provider. Tirzepatide can still work, but the timeline to noticeable appetite suppression may be extended, and the degree of suppression may be moderated.
Psychological relationship with food
This is the factor nobody talks about enough. If food has been your primary coping mechanism for stress, boredom, loneliness, or anxiety, tirzepatide will change your physiological hunger but it will not automatically change your behavioral patterns.
You might find that your body is no longer hungry, but your mind still wants to eat. This creates a confusing dissonance. The medication is working. Your appetite IS suppressed. But the habit of reaching for food in response to emotional triggers persists because that is a learned behavior, not a hormonal signal.
People who address the psychological component alongside medication consistently report better outcomes. Whether through therapy, mindful eating practices, or support groups, working on your relationship with food helps the medication work better and faster.
Tirzepatide vs semaglutide: which suppresses appetite faster?
This is one of the most common questions, and the answer is more nuanced than most sources suggest.
Both medications reduce appetite through GLP-1 receptor activation. Clinical trials comparing the two found that subjective appetite scores, how hungry people reported feeling, were similar between tirzepatide and semaglutide. In the SURPASS-2 trial, decreased appetite was reported in 7-9% of tirzepatide patients compared to 5% of semaglutide patients. Statistically comparable.
But weight loss outcomes tell a different story. Tirzepatide consistently produces greater weight loss than semaglutide at maximum doses. In the most recent head-to-head trial published in the New England Journal of Medicine, tirzepatide was superior to semaglutide for reduction in body weight and waist circumference at week 72 in participants with obesity without diabetes.
How do you get more weight loss with similar appetite scores? Two possibilities.
First, the GIP pathway may drive metabolic improvements, improved fat oxidation, better lipid metabolism, enhanced insulin sensitivity, that contribute to weight loss independently of conscious appetite changes. You lose weight through better metabolic efficiency, not just eating less.
Second, appetite questionnaires may not capture the full picture. The way tirzepatide changes your relationship with food might be qualitatively different from semaglutide, even if the intensity of hunger reduction looks similar on a survey. Less food noise, fewer cravings, less hedonic eating, all of these could reduce caloric intake without registering as "feeling less hungry" on a standardized questionnaire.
Onset comparison
Semaglutide (appetite suppression timeline) typically begins affecting appetite within 1-3 weeks, with full effects building over 4-5 months as the dose escalates to the target of 2.4mg.
Tirzepatide follows a similar early timeline (1-2 weeks for initial effects) but has a longer dose escalation period, potentially taking 20+ weeks to reach the maximum 15mg dose. This means the peak appetite suppression with tirzepatide may take longer to achieve, but many users report that the initial onset is at least as fast, sometimes faster, likely due to the dual mechanism engaging more pathways simultaneously.
Neither medication is clearly faster in overall onset. But tirzepatide may have a higher ceiling for appetite control when maximum doses are reached.
Which one is right for you?
This is a clinical decision that depends on your medical history, comorbidities, insurance coverage, and provider recommendation. Both medications work. Both suppress appetite. SeekPeptides members access detailed comparison guides covering mechanisms, dosing, side effects, and real-world outcomes to help inform these conversations with their providers.
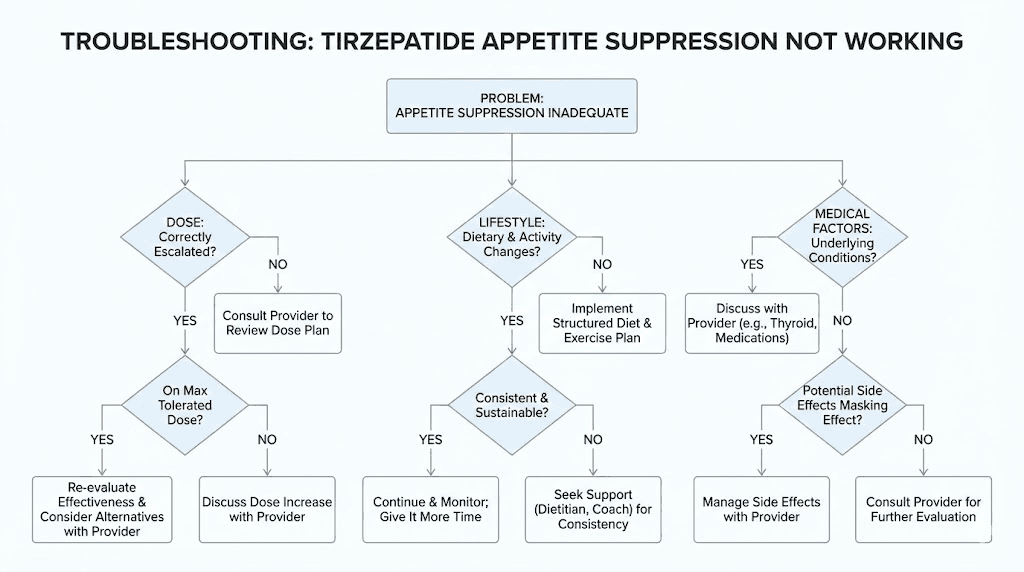
What to do when tirzepatide is not suppressing your appetite
If you are several weeks in and feeling no different, do not panic. But do not just wait and hope, either. Here is a systematic approach.
Check your timeline against the dose schedule
First, where are you in the dose escalation? If you are still on 2.5mg, the lack of appetite suppression is expected. The starting dose is not designed to suppress appetite. It is designed to introduce the medication to your system. True appetite suppression typically begins at 5mg or higher for most people.
If you are on 5mg and into weeks 6-8 with no change, that is worth noting but not alarming. Some people need 7.5mg or 10mg to cross their individual threshold.
If you are on 10mg or higher after 12+ weeks with zero appetite change, that warrants a thorough conversation with your provider.
Evaluate lifestyle factors first
Before assuming the medication is not working, honestly assess the lifestyle factors that can blunt its effects.
Are you sleeping less than seven hours? Are you eating primarily ultra-processed foods? Is your stress level chronically high? Are you dehydrated? Are you taking medications that increase appetite? Any "yes" answer represents a modifiable factor that could be dampening tirzepatide effectiveness.
Address these first. Many people who report "tirzepatide not working" find that fixing sleep, improving diet quality, or managing stress unlocks the appetite suppression they were waiting for.
Distinguish between types of hunger
Tirzepatide is excellent at reducing physiological hunger, the physical sensation of an empty stomach and the hormonal drive to eat. It is less effective against emotional hunger, habitual eating, and environmentally triggered cravings.
Ask yourself: when you eat, are you physically hungry? Does your stomach growl? Do you feel weak or lightheaded? Or are you eating because you are bored, stressed, or because food is available?
If the answer is the latter, the medication may actually be working on your physiological hunger, but habitual eating patterns are masking the effect. The solution is behavioral, not pharmacological.
Consider compounded formulations
Some people using compounded tirzepatide report variable results compared to brand-name Mounjaro or Zepbound. Compounded formulations can differ in potency, stability, and absorption characteristics. If you are using a compounded version and not experiencing expected effects, discuss this with your provider. A switch to brand-name medication, or verification of compounding pharmacy quality, may be warranted.
Request blood work
Underlying metabolic conditions can significantly blunt tirzepatide effectiveness. Ask your provider to check thyroid function (TSH, free T4), fasting insulin and C-peptide, HbA1c, cortisol levels, and sex hormones. Untreated hypothyroidism, severe insulin resistance, or cortisol dysregulation can all reduce tirzepatide appetite-suppressing effects.
Discuss dose adjustment
If lifestyle factors are optimized and no underlying condition explains the lack of response, the next step is dose adjustment. The standard protocol increases by 2.5mg every four weeks. Your provider may recommend continuing to escalate toward higher doses.
Some providers have experimented with more frequent dosing (twice weekly at lower doses) or alternative injection sites in patients with poor subcutaneous absorption.
These are off-label approaches and should only be pursued under direct medical supervision.
The dose escalation schedule explained
Understanding exactly how tirzepatide dosing works helps set realistic expectations for appetite suppression at each level.
Complete FDA-approved schedule
The escalation follows a strict protocol designed to minimize gastrointestinal side effects while building toward therapeutic doses.
Weeks 1-4: 2.5mg once weekly. This is the initiation dose. Its purpose is tolerability, not efficacy. Most people will not experience significant appetite suppression at this level. Think of it as priming your receptors. Your body is meeting tirzepatide for the first time, and this low dose gives your GI tract time to adjust to slower gastric emptying.
Weeks 5-8: 5mg once weekly. The first therapeutic dose. This is where appetite changes typically begin for most users. GLP-1 receptor activation reaches a level that produces measurable satiety. GIP pathway effects start contributing. Many people notice smaller portions, reduced snacking, and less food-focused thinking during this phase.
Weeks 9-12: 7.5mg once weekly (optional). An intermediate step for those who need more effect. Not everyone goes here. Some providers skip directly from 5mg to 10mg. But for patients who had partial response at 5mg, 7.5mg often provides the additional push needed without jumping to a much higher dose.
Weeks 13-16: 10mg once weekly. A maintenance dose for many patients. At this level, appetite suppression is typically robust. The clinical data shows that 10mg produces substantial weight loss in most patients who reach this dose.
Weeks 17-20: 12.5mg once weekly (optional). Another intermediate step. Similar to 7.5mg, this serves as a bridge for patients who need more than 10mg but want to approach the maximum dose gradually.
Week 21+: 15mg once weekly. The maximum approved dose. In SURMOUNT-1, this dose produced 22.5% body weight reduction. Appetite suppression is typically at its strongest, though individual variation exists even at maximum dose.
Key dosing principles
Never increase by more than 2.5mg at a time. Always wait at least four weeks between increases. Your provider decides whether to increase, hold, or (rarely) decrease your dose based on your response and tolerability.
The schedule is a maximum pace, not a required pace. Some patients stay at 5mg for months before increasing. Others move through the escalation steadily. Both approaches are valid depending on individual response.
Understanding this schedule helps explain why "how long does tirzepatide take to suppress appetite" does not have a single answer. A person who responds at 5mg will feel appetite suppression by week 5-6. A person who needs 10mg will not feel it until week 13-16. Both are normal. Both are expected. Neither indicates a problem with the medication or your body.
What real appetite suppression actually feels like
Many people do not recognize appetite suppression when it first arrives because it does not match their expectations.
What it is NOT
Appetite suppression from tirzepatide is not an on-off switch. You will not wake up one morning with zero hunger. You will not suddenly find food repulsive. You will not lose all interest in eating.
If that IS what you are experiencing, particularly if accompanied by severe nausea, vomiting, or abdominal pain, contact your provider. That level of appetite loss may indicate a side effect that needs medical attention, not a therapeutic benefit.
What it IS
Real appetite suppression from tirzepatide is more like a volume dial being turned down than a switch being flipped. Here is what it typically looks like in daily life.
You sit down for dinner and eat half the plate. Then you stop. Not because you are forcing yourself to stop, but because you genuinely do not want more. The desire is gone. The food is fine. You just do not need it.
You drive past a fast food restaurant. Normally, the sign would trigger a craving. Today it does not register. You do not have to resist the urge because there is no urge to resist.
You look at the clock and realize it is 2pm. You have not eaten lunch. Not because you are busy, but because the thought of food simply did not occur to you. When you do eat, a small meal satisfies completely.
You open the fridge and nothing looks particularly appealing. Not in a nauseous way. Everything looks fine. You just do not feel pulled toward any of it. You eat because you know you should, not because your body is demanding it.
The food noise quiets. That constant background mental chatter about meals, snacks, and what to eat next fades into something occasional and manageable.
These changes can be so gradual that you do not notice them until someone points them out, or until you look back and realize your eating patterns have fundamentally shifted. This is why keeping a food journal or tracking progress can be valuable. It captures changes you might otherwise miss.
The role of gastric emptying in appetite suppression timing
Gastric emptying delay is the fastest-acting mechanism in tirzepatide appetite suppression toolkit, and understanding it helps explain the timeline.
How slowed gastric emptying affects hunger
Your stomach has stretch receptors that send fullness signals to your brain. When food sits in the stomach longer, these receptors fire for a longer period. You feel full faster and stay full longer.
Tirzepatide slows gastric emptying significantly, particularly after the first dose. Studies show the delay is most pronounced initially, then partially attenuates through tachyphylaxis, a natural reduction in response to repeated dosing. However, clinically meaningful delay persists throughout treatment.
This mechanism acts fast. It does not require weeks of receptor upregulation or neurological adaptation. Once tirzepatide levels are sufficient in your bloodstream, gastric emptying slows. This is why some people feel appetite changes within 24-48 hours of their first injection.
The trade-offs
Slowed gastric emptying is a double-edged sword. The benefits for appetite control are clear. But the same mechanism causes the most common side effects: nausea, bloating, constipation, acid reflux, and abdominal discomfort.
Managing these side effects is important for sustained appetite suppression. If nausea is so severe that you dread eating, you may inadvertently create an unhealthy relationship with food. The goal is comfortable appetite reduction, not food aversion.
Practical tips for managing gastric emptying-related side effects while maintaining appetite suppression:
Eat smaller, more frequent meals instead of three large ones
Avoid lying down within two to three hours of eating
Prioritize protein-rich foods that support satiety without excessive volume
Limit high-fat meals that take longest to empty from the stomach
Stay well-hydrated between meals, not during meals
Chew food thoroughly to aid digestion
Walk for 10-15 minutes after eating to promote gentle gastric motility
Appetite suppression by the numbers: what the clinical trials show
Let us ground this discussion in the actual data from the major tirzepatide clinical trials.
SURMOUNT-1 results
The landmark obesity trial enrolled 2,539 adults with BMI of 30 or higher (or 27 with at least one weight-related comorbidity) without diabetes. Participants received tirzepatide 5mg, 10mg, or 15mg, or placebo, for 72 weeks.
Weight loss results:
5mg group: 16.0% body weight reduction
10mg group: 21.4% body weight reduction
15mg group: 22.5% body weight reduction
Placebo: 3.1% body weight reduction
These weight losses require sustained, significant appetite reduction. You do not lose 22.5% of your body weight without eating substantially less over an extended period.
The early response analysis is particularly relevant for timeline questions. Of the tirzepatide-treated participants, 82% achieved at least 5% weight loss by week 12, the "early responders." The remaining 18% were "late responders" who had less than 5% weight loss at the 12-week mark.
But the late responders were not non-responders. Ninety percent of them eventually achieved clinically meaningful weight loss by week 72. The appetite suppression came. It just took longer.
Appetite and energy intake data
A dedicated study published in Diabetes Care examined tirzepatide effects on appetite, energy intake, and fat mass in people with type 2 diabetes. The findings:
Tirzepatide 15mg reduced ad libitum lunch intake by approximately 310 calories compared to placebo. That is roughly the equivalent of removing a large snack or a side dish from every lunch. Across three meals a day, the caloric deficit becomes substantial.
Appetite visual analog scale scores showed significant reduction in hunger and increased fullness with tirzepatide compared to placebo. Importantly, tirzepatide reduced food craving scores, not just physical hunger.
SURMOUNT-4 maintenance data
SURMOUNT-4 answered a critical question: what happens when you stop tirzepatide? After 36 weeks of treatment, participants were randomized to continue tirzepatide or switch to placebo for another 52 weeks.
The results were clear. Participants who continued tirzepatide maintained and extended their weight loss. Those who switched to placebo regained weight. The appetite suppression, along with the metabolic benefits, requires ongoing treatment.
This has direct implications for timeline expectations. Tirzepatide is not a short course that permanently resets your appetite. It is an ongoing treatment that maintains appetite suppression as long as you take it. If you are wondering how long the appetite suppression will last, the answer is: as long as you continue the medication at effective doses.
Maximizing tirzepatide appetite suppression: a practical protocol
Based on clinical data and extensive protocol analysis, here is a comprehensive approach to getting the most out of tirzepatide appetite-suppressing effects.
Protocol 1: the first 30 days (foundation building)
Goal: Establish medication tolerance and lay the groundwork for optimal response.
Dosing: 2.5mg once weekly as prescribed.
Nutrition approach:
Focus on protein at every meal (aim for 25-30g per meal minimum)
Reduce ultra-processed food intake by 50% or more
Eat vegetables with every meal to support gut health
Stay hydrated with 64+ ounces of water daily
Sleep optimization:
Target 7-9 hours nightly
Consistent sleep and wake times
No screens 60 minutes before bed
Cool, dark sleeping environment
Movement:
Daily walking, 20-30 minutes minimum
Light resistance training 2-3 times per week
No intense exercise that triggers compensatory hunger
Tracking:
Daily food journal noting hunger levels (1-10 scale) before and after meals
Weekly weight check (same time, same conditions)
Side effect log for provider discussions
Protocol 2: weeks 5-12 (appetite optimization)
Goal: Leverage the first therapeutic dose for maximum appetite control.
Dosing: 5mg, escalating to 7.5mg at week 9 if indicated.
Nutrition refinement:
Increase protein to 0.7-1.0g per pound of goal body weight
Reduce meal frequency if naturally eating less (three meals, no snacking is common)
Prioritize nutrient density, each calorie you eat should deliver maximum nutrition
Consider meal timing, many tirzepatide users find that eating earlier in the day aligns better with the medication appetite-suppressing peak
Behavioral additions:
Practice mindful eating (eat slowly, without screens, paying attention to fullness)
Identify and address emotional eating triggers
Begin to distinguish between physical hunger and habitual eating
Protocol 3: weeks 13+ (sustained optimization)
Goal: Maintain appetite control while maximizing lean mass preservation.
Dosing: 10mg-15mg as prescribed.
Advanced nutrition:
Protein remains priority (even more important as weight loss increases)
Consider working with a registered dietitian familiar with GLP-1 medications
Supplement as needed: fiber, protein supplements, multivitamin if intake drops significantly
Monitor for nutritional deficiencies that can occur with reduced food intake
Exercise progression:
Increase resistance training to preserve muscle mass during weight loss
3-4 strength training sessions per week
Continue daily walking or cardio
Monitor energy levels and adjust intensity if needed
SeekPeptides members access detailed protocol builders, dosing calculators, and expert-reviewed guides that account for individual factors most resources ignore. Whether you are navigating the early weeks or optimizing at higher doses, having evidence-based guidance makes the difference between adequate and exceptional results.
Common mistakes that delay appetite suppression
After reviewing thousands of reported tirzepatide experiences, clear patterns emerge around mistakes that slow down or blunt appetite suppression.
Mistake 1: expecting a light switch
The biggest mistake is expecting appetite suppression to arrive as a dramatic, unmistakable event. For most people, it creeps in gradually. You eat a little less one day. Then a little less the next week. Then you realize your pants are looser and you have not thought about snacking in three days.
If you are waiting for a Hollywood moment where food suddenly becomes irrelevant, you will miss the actual effect happening right in front of you.
Mistake 2: eating through the suppression
Some people feel the appetite suppression but eat anyway. Out of habit. Out of social pressure. Out of fear that skipping a meal is unhealthy. If tirzepatide is telling you that you are full after half a plate, listen to it. That is the medication working. Eating past the fullness signal trains your body to ignore the new set point.
This does not mean you should skip meals or restrict dangerously. It means responding to genuine hunger and fullness cues rather than external cues like the clock, social expectations, or portion sizes.
Mistake 3: poor injection technique
Tirzepatide is a subcutaneous injection. If injected too shallowly (intradermally) or too deeply (intramuscularly), absorption kinetics change. This can affect how quickly the medication reaches therapeutic levels and, consequently, how quickly appetite suppression develops.
Proper technique: inject into the subcutaneous fat of the abdomen, thigh, or upper arm. Rotate injection sites. Follow your provider instructions or the medication guide exactly.
Mistake 4: skipping doses
Tirzepatide is a once-weekly medication with a half-life of approximately 5 days. Consistency is critical. Missing a dose disrupts steady-state blood levels and can cause appetite suppression to fluctuate unpredictably.
If you miss a dose, take it as soon as possible within four days of the missed dose. If more than four days have passed, skip the missed dose and take the next one on schedule. Do not double dose.
Mistake 5: not giving each dose level enough time
Some people feel impatient at 2.5mg and want to jump to higher doses immediately. Others want to abandon the medication entirely after three weeks of "no results." Both reactions are understandable but premature.
The four-week minimum at each dose exists for good reason. Your body needs time to reach steady-state concentration at each dose level. Rushing the escalation increases GI side effects without necessarily producing faster appetite suppression. The medication works on its own schedule. Trust the process.
Mistake 6: ignoring side effects as separate from appetite suppression
Nausea is not appetite suppression. Feeling too sick to eat is not the same as feeling comfortably satisfied with less food. If you are equating severe nausea with "the medication working," you are setting yourself up for a confusing experience when the nausea fades and hunger returns.
True appetite suppression persists even on days when you feel fine. Nausea-based appetite reduction disappears the moment the nausea resolves. Knowing the difference helps you accurately track your response.
Long-term appetite suppression: what happens after months on tirzepatide
Understanding the long-term trajectory is essential for managing expectations.
Months 1-3: building phase
This is the period of dose escalation and initial response. Appetite suppression typically increases with each dose step. Weight loss begins and accelerates. Side effects peak and then improve. Your body is adapting to a new metabolic environment.
Months 3-6: peak effect phase
For most people, months three through six represent peak appetite suppression. The dose has reached a therapeutic level, steady-state blood concentrations are established, and both GLP-1 and GIP pathways are fully engaged. This is when weight loss is often fastest.
Food noise is at its quietest. Portions are at their smallest. The effort required to eat less is minimal because your body genuinely wants less.
Months 6-12: stabilization phase
Around the six-month mark, many users report a slight softening of appetite suppression. Not a loss of effect, but a moderation. The dramatic "I forgot to eat" feeling may settle into a more moderate "I eat less than I used to." This is normal and does not mean the medication is failing.
Several factors contribute to this shift. Partial receptor desensitization. The Penn Medicine research suggesting that reward-center effects may be temporary. And simple metabolic adaptation, as you lose weight, your body requires fewer calories, and the gap between your intake and requirement narrows.
Weight loss typically slows during this phase. Not because you are eating more, but because your smaller body needs less energy. You may need to consciously manage portions and nutrition more actively than you did during the peak phase.
Beyond 12 months: maintenance phase
The SURMOUNT-4 trial clearly showed that ongoing tirzepatide treatment maintains weight loss, while discontinuation leads to regain. Appetite suppression continues as long as you continue the medication, though the intensity may fluctuate.
Long-term users develop a new relationship with food. The initial dramatic appetite changes settle into new habits. Smaller portions become normal. Fewer cravings become the default. The need for the medication to actively suppress appetite becomes less about fighting hunger and more about maintaining a new baseline.
Some long-term users do experience periods where appetite temporarily increases, often correlated with stress, sleep disruption, hormonal changes, or illness. These episodes typically resolve when the underlying trigger is addressed.
Special populations and appetite suppression timing
Different groups may experience different timelines.
People with type 2 diabetes
Tirzepatide was initially approved for type 2 diabetes management (as Mounjaro) before obesity (as Zepbound). People with diabetes often have more severe insulin resistance and altered incretin signaling, which can affect appetite suppression onset.
The SURPASS trials in diabetes populations showed significant weight loss alongside glycemic control, but the weight loss was generally slightly less than in the SURMOUNT obesity trials (participants without diabetes). This may reflect metabolic differences that also affect appetite suppression timing.
If you have type 2 diabetes, you may need higher doses or more time to achieve the same degree of appetite suppression as someone without diabetes. The medication is still effective, the timeline is just shifted.
People on other medications
Concurrent medications interact with tirzepatide in ways that affect appetite. As mentioned earlier, corticosteroids, certain antidepressants, and some diabetes medications can increase hunger. But other medications may also play a role.
Antidepressants that cause weight gain (mirtazapine, certain SSRIs, tricyclics) may counteract some of tirzepatide appetite-suppressing effects. Discuss medication adjustments with your prescriber if you are taking these alongside tirzepatide.
Women vs men
Hormonal differences between men and women can affect tirzepatide response. Women experience cyclical hormonal fluctuations that influence appetite independent of medication. The luteal phase (before menstruation) typically increases hunger and cravings. Some women on tirzepatide notice these monthly cycles pushing through the medication appetite suppression.
Menopause and perimenopause add another layer. Declining estrogen affects body composition, insulin sensitivity, and metabolic rate. Perimenopausal women may need higher doses or more time to achieve the same appetite suppression as premenopausal women.
Men tend to have more stable appetite responses to tirzepatide, reflecting fewer hormonal fluctuations. They also typically have higher lean mass and metabolic rate, which can affect weight loss dynamics even if appetite suppression is similar.
Older adults
People over 65 may metabolize tirzepatide differently. Reduced kidney function, lower metabolic rate, and decreased muscle mass can all affect drug levels and response. Clinical trials included older adults, and the medication was effective, but the timeline to full appetite suppression may be slightly longer.
Older adults also face unique nutritional concerns. Appetite suppression that is too aggressive can lead to sarcopenia (muscle wasting), nutritional deficiencies, and frailty. Close monitoring of protein intake and nutritional status is especially important for this group.
Injection timing and appetite suppression patterns
When you inject tirzepatide within the week can influence when you feel appetite suppression most strongly.
The pharmacokinetic curve
Tirzepatide has a half-life of approximately five days, which is why it works as a once-weekly injection. After injection, blood levels rise over 8-72 hours, peak, and then gradually decline until the next dose.
Many users report that appetite suppression is strongest in the 1-3 days following injection, then gradually softens before the next dose. This pattern is more noticeable at lower doses and less pronounced at higher doses where steady-state levels remain elevated throughout the week.
Strategic injection timing
Some people time their injection to align peak appetite suppression with their most challenging eating days. For example, injecting on Thursday evening so that peak suppression covers the weekend, when social eating and less structured schedules make calorie control harder.
Others prefer injecting on Sunday night so peak effects cover Monday through Wednesday, when work stress and convenience eating are most likely to derail their nutrition.
There is no universally "best" day to inject. The best day is the one that you will remember consistently and that aligns peak medication effects with your highest-risk eating periods.
Injection site and absorption
Tirzepatide can be injected in the abdomen, thigh, or upper arm. Absorption rates may vary slightly between sites. The abdomen typically provides the fastest and most consistent absorption due to rich subcutaneous blood supply.
Rotate sites within each area to prevent lipohypertrophy (thickened fatty tissue at injection sites), which can impair absorption over time. If you notice that appetite suppression varies between injection sites, discuss this with your provider.
Frequently asked questions
Can I feel appetite suppression from the very first dose of tirzepatide?
Yes, some people notice reduced hunger within 24-48 hours of their first 2.5mg injection. This early effect is primarily driven by delayed gastric emptying, which is strongest after the initial dose. However, most people do not experience significant appetite changes until reaching the 5mg dose at week five. Both responses are completely normal.
Why am I still hungry on tirzepatide after four weeks?
At four weeks, you are still on the 2.5mg starting dose, which is not a therapeutic dose for appetite suppression. It is a tolerability dose. Most people need at least 5mg, and many need 7.5mg or 10mg, to achieve meaningful appetite control. Continue the prescribed dose escalation and give each dose level at least four weeks before evaluating its effectiveness.
Does tirzepatide stop suppressing appetite over time?
Appetite suppression typically remains effective as long as you continue taking tirzepatide at therapeutic doses. Some users notice a mild softening of the effect after 6-12 months, but it rarely disappears entirely. The SURMOUNT trials showed sustained weight loss through 72 weeks, which requires ongoing appetite reduction. If you feel appetite suppression weakening, discuss dose adjustment with your provider.
Is tirzepatide or semaglutide better for appetite suppression?
Both medications produce similar subjective appetite scores in clinical trials. However, tirzepatide consistently produces greater weight loss than semaglutide, suggesting additional metabolic benefits beyond appetite reduction alone. The dual GIP/GLP-1 mechanism may provide qualitatively different appetite effects that standard questionnaires do not fully capture. Your provider can help determine which medication is best for your specific situation.
What should I eat to maximize tirzepatide appetite suppression?
High-protein meals enhance tirzepatide effects because protein naturally stimulates GLP-1 and GIP release. Aim for 25-30g of protein per meal, minimize ultra-processed foods, and stay well-hydrated. Avoid large high-fat meals that can worsen gastrointestinal side effects without adding to appetite control. Vegetables and fiber support gut health and satiety.
Can poor sleep affect how well tirzepatide suppresses my appetite?
Absolutely. Sleep deprivation increases ghrelin (hunger hormone) and decreases leptin (satiety hormone), directly counteracting tirzepatide mechanism of action. Research consistently shows that people sleeping fewer than seven hours experience stronger hunger, more cravings, and greater reward-center activity in response to food. Seven to nine hours of quality sleep significantly enhances tirzepatide effectiveness.
What happens to my appetite if I stop taking tirzepatide?
The SURMOUNT-4 trial showed that appetite and body weight return toward baseline after discontinuing tirzepatide. Appetite suppression is maintained by the medication ongoing pharmacological effects, not by permanent metabolic changes. If you stop treatment, expect hunger and eating patterns to gradually return to pre-treatment levels over weeks to months.
Should I track my appetite while on tirzepatide?
Yes. Tracking hunger levels on a simple 1-10 scale before and after meals helps you recognize gradual changes you might otherwise miss. It also provides valuable data for provider conversations about dose adjustments. Many people do not realize their appetite has decreased until they look at their tracking data over several weeks.
External resources
Tirzepatide StatPearls overview, National Library of Medicine
Tirzepatide reduces appetite, energy intake, and fat mass, Diabetes Care
For researchers serious about optimizing their protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay balanced, your doses stay consistent, and your results stay on track.