Feb 15, 2026
Two medications. Completely different mechanisms. And a weight loss gap so wide it changes the entire conversation about which one deserves your attention.
Phentermine has been around since 1959. It is the oldest weight loss medication still in use, a sympathomimetic amine that floods your system with norepinephrine to crush your appetite through sheer stimulant force. Semaglutide arrived decades later, a GLP-1 receptor agonist that mimics a gut hormone your body already produces, working through entirely different pathways to reduce hunger, slow gastric emptying, and rewire how your brain responds to food.
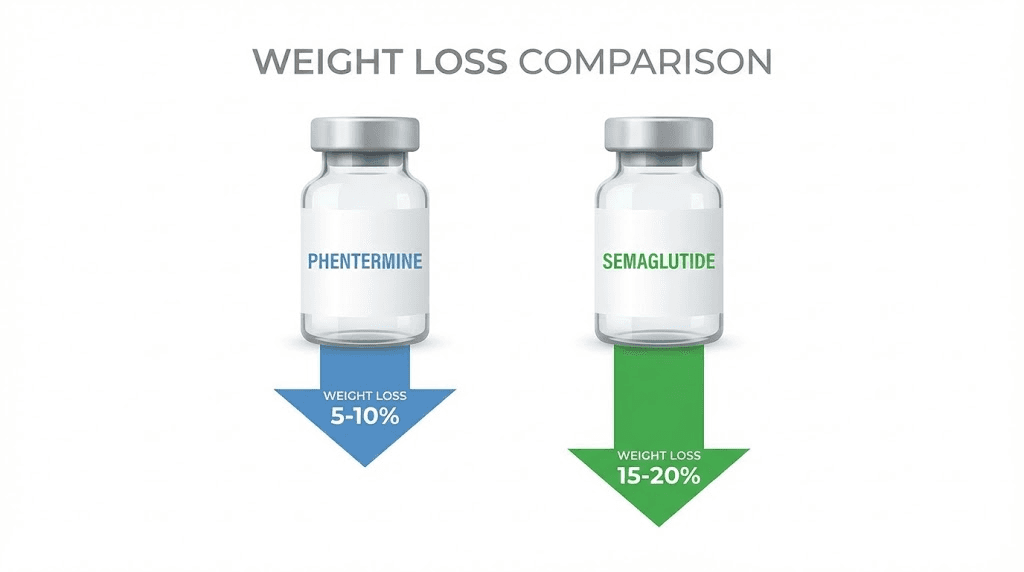
The clinical data tells a story that surprises most people. Semaglutide users in the STEP 1 trial lost an average of 14.9% of their body weight over 68 weeks. Phentermine users typically lose 5 to 10% over just 8 to 12 weeks before the medication must be stopped. But weight loss percentages only tell part of the story. Side effects, cost, accessibility, long-term sustainability, and what happens after you stop, all of these factors matter just as much as the number on the scale. This guide breaks down every meaningful difference between phentermine and semaglutide so you can make an informed decision based on real data, not marketing claims. SeekPeptides has analyzed both medications across every dimension that matters, from molecular mechanisms to monthly costs, to give you the most comprehensive comparison available anywhere.
How phentermine works in your body
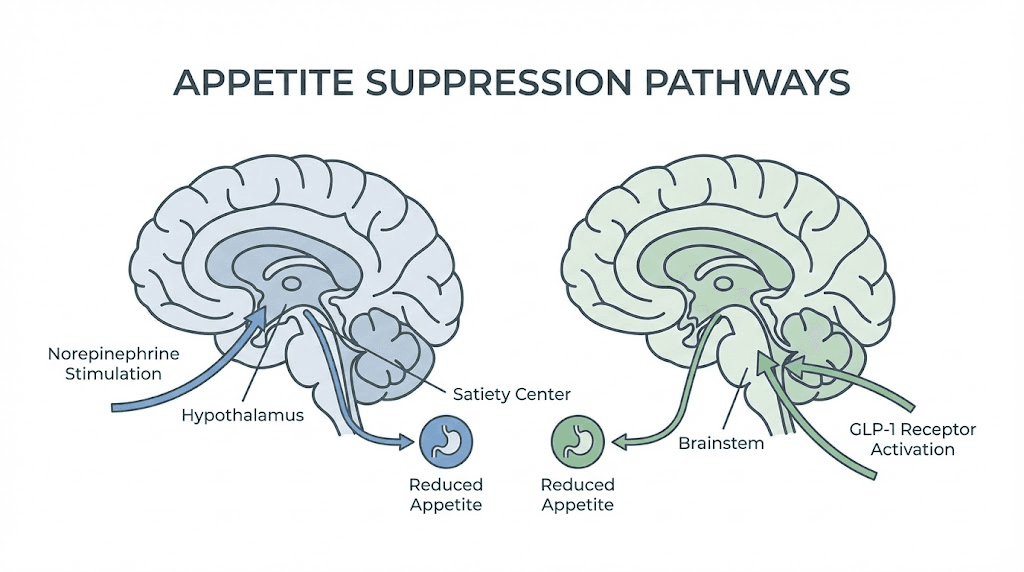
Phentermine is a sympathomimetic amine. That is a clinical way of saying it activates your fight-or-flight response. The drug acts as a potent substrate at the norepinephrine transporter, simultaneously promoting norepinephrine release while blocking its reuptake. This floods your central nervous system with the same chemicals that surge when you face a genuine threat.
Your appetite disappears. Not because your body does not need food, but because your brain has been tricked into thinking survival matters more than eating.
The mechanism is similar to amphetamine, which is why the DEA classifies phentermine as a Schedule IV controlled substance. It is an agonist at the trace amine-associated receptor (TAAR1), stimulating the release of both norepinephrine and epinephrine. The appetite suppression comes from enhanced norepinephrine signaling in hypothalamic satiety centers, the same brain region that semaglutide targets through completely different pathways. Phentermine may also increase resting energy expenditure slightly, though appetite suppression remains the dominant mechanism driving weight loss.
Here is what that looks like in practice. You take the pill in the morning. Within an hour, your heart rate increases. Your blood pressure rises. You feel alert, possibly jittery. Food becomes an afterthought. Some users describe it as having three cups of coffee but without the desire to eat anything. The effect is powerful and immediate, which is both its greatest strength and its fundamental limitation. Your body adapts. Tolerance develops. Studies document approximately 10% tolerance to phentermine effects within the 3 to 6 month window, which is why prescriptions are limited to 12 weeks in most cases.
The classification question comes up often. Phentermine is not a GLP-1 agonist. It is not a peptide. It is a classical stimulant-based appetite suppressant that works through catecholamine release. Understanding this distinction matters because it determines everything about the drug, from its side effect profile to its duration of use to what happens when you stop taking it. Researchers exploring peptide-based weight loss approaches recognize that the mechanism of action shapes the entire treatment experience.
Phentermine dosing and administration
Phentermine comes in oral tablets and capsules. The standard dose is 37.5 mg once daily, taken in the morning before breakfast or 1 to 2 hours after breakfast. Some clinicians prescribe lower doses of 15 mg or 8 mg for patients who experience side effects at the full dose. The medication should never be taken in the evening because the stimulant properties cause insomnia.
Most prescriptions run for 12 weeks. Some practitioners extend treatment to 6 months, though this remains controversial. The FDA approved phentermine for short-term use only, defined as a few weeks. Longer prescriptions happen off-label and carry increased risk of tolerance and dependence.
There is no titration schedule. You start at your prescribed dose and continue until the prescription ends. Compare this to semaglutide, where the dosing protocol involves gradual escalation over 16 to 20 weeks. The simplicity of phentermine dosing is convenient but reflects the drug limitations rather than precision dosing strategies. If you are interested in understanding how dosage calculations work across different weight loss compounds, the differences become even more apparent.
How semaglutide works in your body
Semaglutide mimics GLP-1, a hormone your gut naturally produces after eating. But calling it a simple mimic undersells what happens at the molecular level. The drug binds to GLP-1 receptors across multiple organ systems, triggering a coordinated response that attacks weight gain from several directions simultaneously.
In the brain, semaglutide activates GLP-1 receptors in the hypothalamus and brainstem. Specifically, it stimulates anorexigenic neurons (the ones that create feelings of fullness) while inhibiting orexigenic neurons (the ones that drive hunger). The proopiomelanocortin and cocaine- and amphetamine-regulated transcript neurons get activated. The neuropeptide Y and agouti-related peptide neurons get suppressed. This is not a blunt-force appetite kill like phentermine delivers. It is a recalibration of the hunger and satiety signaling system.
Then there is the gut. Semaglutide slows gastric emptying, meaning food stays in your stomach longer. You feel full sooner. You stay full longer. This delayed gastric emptying creates a prolonged sense of satiety that reduces overall food intake without the stimulant-driven appetite suppression that phentermine relies on.
The appetite suppression timeline with semaglutide unfolds gradually. Most users notice reduced hunger within the first 2 to 4 weeks, with full appetite suppression developing over 8 to 12 weeks as the dose titrates upward. This stands in sharp contrast to phentermine, where the appetite suppression is immediate and intense but fades as tolerance builds.
Semaglutide also improves blood sugar control in several ways. It stimulates insulin release after meals while suppressing glucagon, a hormone that raises blood sugar. It slows digestion to prevent post-meal glucose spikes. For people with type 2 diabetes or prediabetes, these metabolic benefits make semaglutide a dual-purpose medication that addresses multiple health concerns beyond just weight.
Semaglutide dosing and titration
Semaglutide for weight loss (Wegovy) follows a structured titration schedule. You start at 0.25 mg weekly for the first four weeks, then increase to 0.5 mg for weeks 5 through 8, then 1 mg for weeks 9 through 12, then 1.7 mg for weeks 13 through 16, and finally the maintenance dose of 2.4 mg from week 17 onward. This slow escalation minimizes gastrointestinal side effects and gives your body time to adjust.
The injection is subcutaneous, administered once weekly in the abdomen, thigh, or upper arm. Users familiar with GLP-1 injection techniques know that rotating injection sites prevents lipodystrophy and ensures consistent absorption. The semaglutide dosage calculator helps determine exact amounts based on your specific prescription and concentration.
Unlike phentermine, semaglutide is approved for long-term use. The STEP 5 trial demonstrated sustained weight loss over 104 weeks of continuous treatment. There is no arbitrary 12-week cutoff. You continue the medication as long as it remains effective and tolerable. This fundamental difference in treatment duration shapes the entire comparison between these two medications.
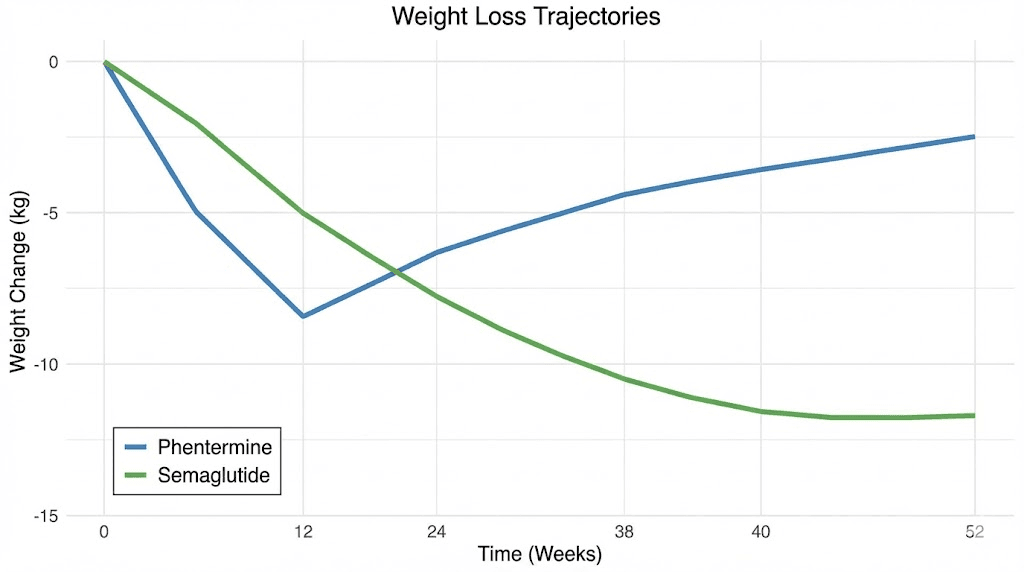
Weight loss results compared head to head
Numbers matter here. Vague claims about which drug works better help nobody. So let us look at what the clinical trials actually show.
Semaglutide (STEP 1 trial): Participants lost an average of 14.9% of body weight over 68 weeks at the 2.4 mg dose, compared to 2.4% with placebo. For a 220-pound person, that translates to roughly 33 pounds of weight loss.
Phentermine studies: Users typically lose 5 to 10% of body weight over 8 to 12 weeks. For that same 220-pound person, that means 11 to 22 pounds, but in a fraction of the time.
A network meta-analysis comparing multiple weight loss approaches found semaglutide achieves 13.7% average weight loss compared to phentermine combined with topiramate at 9.1%. And that comparison uses the enhanced version of phentermine, not phentermine alone, which performs worse.
The rate of weight loss tells an interesting story too. Phentermine works fast. You will see results on the scale within the first week or two. Semaglutide takes longer to ramp up because of the titration schedule, with meaningful weight loss typically beginning around weeks 4 to 8 and continuing to accelerate through week 20.
But here is where it gets complicated.
Phentermine users hit a plateau. The drug stops working as effectively around the 3-month mark due to tolerance. At that point, the prescription ends. Semaglutide users continue losing weight for months beyond that point. The STEP 5 trial showed ongoing weight loss through 104 weeks of treatment, with participants maintaining a 15.2% body weight reduction at the two-year mark.
Weight loss comparison table
Factor | Phentermine | Semaglutide |
|---|---|---|
Average weight loss | 5-10% body weight | 14.9% body weight |
Treatment duration | 8-12 weeks (max) | Ongoing (years) |
Time to notice results | 1-2 weeks | 4-8 weeks |
Peak weight loss | Around week 8-10 | Around week 60-68 |
Weight loss at 6 months | N/A (treatment ended) | 10.9% body weight |
Weight loss at 12 months | N/A (treatment ended) | ~14% body weight |
Weight loss at 24 months | N/A | 15.2% body weight |
The table reveals a fundamental asymmetry. Phentermine delivers rapid results in a short window. Semaglutide delivers greater total results over a much longer period. Which approach is better depends entirely on your situation, goals, and what you plan to do after the medication stops. For context on how long semaglutide takes to show results and the factors that influence individual outcomes, understanding the titration process is essential.
Side effects and safety profiles
Every medication has tradeoffs. The question is never whether side effects exist. It is whether the side effects are manageable, temporary, and worth the benefit.
Phentermine and semaglutide cause completely different types of side effects because they work through completely different mechanisms.
Phentermine side effects
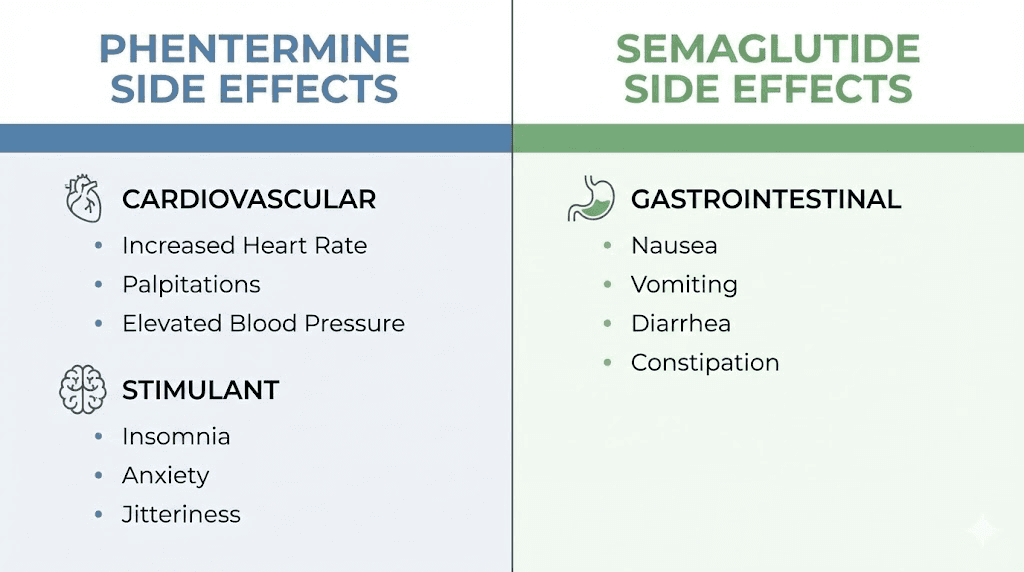
Phentermine is a stimulant. Its side effects reflect that reality.
Common side effects: Dry mouth, insomnia, increased heart rate, elevated blood pressure, headaches, jitteriness, and restlessness. These are not occasional occurrences. They are predictable consequences of flooding the nervous system with norepinephrine.
Serious concerns: Phentermine can trigger cardiovascular events in susceptible individuals. Elevated heart rate and blood pressure place additional strain on the heart. The drug carries risks of dependency because of its amphetamine-like mechanism. Tolerance develops, which means the body requires more stimulation to achieve the same appetite-suppressing effect. Some users experience anxiety, irritability, and mood changes that worsen over the treatment period.
The contraindication list is extensive. Phentermine is not safe for people with heart disease, uncontrolled hypertension, glaucoma, hyperthyroidism, a history of drug abuse, or agitated states. There are 202 known drug interactions, including 43 classified as major. MAO inhibitors must be stopped at least 14 days before starting phentermine. Combining phentermine with antidepressants increases the risk of serotonin syndrome, a potentially life-threatening condition.
Pregnant and breastfeeding women cannot take phentermine. Children under 16 should not use it. People with kidney disease face increased risk because phentermine levels can accumulate. The question of combining phentermine with other medications requires careful evaluation because of these extensive interaction risks.
Semaglutide side effects
Semaglutide side effects are primarily gastrointestinal. Nausea is the most common, affecting roughly 40% of users during the dose escalation phase. Diarrhea, constipation, vomiting, and abdominal discomfort also occur. The good news is that these side effects typically diminish as the body adjusts, especially when the titration schedule is followed properly.
The fatigue question comes up frequently. Some users report tiredness during the first weeks of treatment, likely related to reduced caloric intake rather than a direct drug effect. This usually resolves as the body adapts to new eating patterns. Understanding GLP-1 related fatigue helps set realistic expectations during the adjustment period.
More serious but rare concerns include pancreatitis, gallbladder problems, and potential thyroid tumor risk (observed in rodent studies but not confirmed in humans). Semaglutide should not be used by people with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2.
The overall discontinuation rate due to adverse events is lower with semaglutide than with phentermine. Most users who experience nausea or digestive issues find them manageable and temporary. For those experiencing constipation on semaglutide, several evidence-based strategies can help. The dietary adjustments recommended during treatment can minimize gastrointestinal symptoms significantly.
Side effects comparison table
Side effect category | Phentermine | Semaglutide |
|---|---|---|
Primary type | Cardiovascular/stimulant | Gastrointestinal |
Nausea | Occasional | Common (40%), improves |
Insomnia | Very common | Rare |
Heart rate increase | Yes, significant | Minimal |
Blood pressure | Increases | May decrease |
Anxiety/jitteriness | Common | Rare |
Constipation | Occasional | Common |
Dependency risk | Yes (Schedule IV) | None |
Long-term safety data | Limited (short-term use) | Extensive (2+ year trials) |
What happens when you stop each medication
This is where the conversation shifts from theoretical to deeply practical. Because every weight loss medication is temporary for some users, understanding what happens after stopping matters just as much as what happens during treatment.
The data is sobering for both medications.
After stopping phentermine
Weight regain after discontinuing phentermine is common and well-documented. A survey-based study found that only 42% of responders maintained all the weight they lost while on phentermine. Another 25.2% maintained at least a 10% body weight reduction. But some respondents reported a net weight gain ranging from 2 to 70 pounds after stopping, with a mean net weight gain of 16 pounds.
The pattern makes biological sense. Phentermine suppresses appetite through artificial stimulation. When that stimulation disappears, appetite returns, often with a vengeance. Your body has been running on reduced calories with a chemically suppressed hunger drive. Remove the chemical, and the hunger comes back, sometimes stronger than before because your metabolic rate may have decreased during the calorie restriction period.
This is why practitioners who prescribe phentermine emphasize lifestyle changes during the treatment window. The medication buys you time to establish new eating habits. If those habits take hold, you keep the weight off. If they do not, the weight returns. The challenges of maintaining weight loss apply regardless of which medication you choose, but the timeline and mechanisms differ significantly.
After stopping semaglutide
The STEP 1 trial extension provided the clearest data on semaglutide discontinuation. One year after stopping semaglutide 2.4 mg, participants regained two-thirds of their prior weight loss. They had lost 17.3% of body weight during treatment. After stopping, they regained 11.6 percentage points, leaving a net loss of only 5.6% from baseline.
Weight regain begins approximately 8 weeks after stopping and continues for an average of 20 weeks before plateauing. In the STEP-10 trial, over 40% of lost weight was regained within just 28 weeks of discontinuation. A real-world study of over 20,000 patients found that 17.7% of semaglutide users regained all the weight they had lost, or even exceeded their initial weight, within one year of stopping.
The cardiometabolic improvements achieved during semaglutide treatment also revert toward baseline after stopping. Blood sugar improvements, blood pressure reductions, and lipid changes tend to reverse once the medication is discontinued.
This creates an important clinical reality. Semaglutide works brilliantly while you are taking it. But for many people, it may require indefinite use to maintain results. The withdrawal experience varies between individuals, but appetite rebound is nearly universal. Understanding treatment duration planning is critical for setting realistic expectations.
Weight regain comparison
Factor | Phentermine | Semaglutide |
|---|---|---|
Regain onset | Immediately after stopping | ~8 weeks after stopping |
Regain amount (1 year) | Variable (42% maintain all loss) | Two-thirds regained |
Complete regain risk | Common without lifestyle change | 17.7% regain all or more |
Metabolic effects | Revert upon stopping | Revert upon stopping |
Can resume treatment | Limited by tolerance/DEA scheduling | Yes, can restart |
Cost comparison and accessibility
Money talks. And when it comes to weight loss medications, the cost difference between phentermine and semaglutide is enormous.
Phentermine costs
Generic phentermine costs under $50 per month without insurance. With insurance, the cost drops further. It is one of the most affordable prescription weight loss medications available. Most commercial insurance plans cover phentermine, and about half of Medicaid plans do as well.
The total treatment cost for a standard 12-week course runs between $100 and $150 without insurance. Even without coverage, phentermine remains accessible to most budgets.
Semaglutide costs
Brand-name semaglutide (Wegovy for weight loss, Ozempic for diabetes) costs significantly more. Without insurance, Ozempic runs approximately $1,027 per month and Wegovy approximately $1,400 per month.
Insurance coverage varies widely. Many plans cover Ozempic when prescribed for type 2 diabetes but not for weight loss alone. Wegovy coverage has expanded but remains inconsistent. Medicare does not cover weight loss medications. Some Medicaid plans provide coverage, but restrictions apply.
Manufacturer savings programs can reduce costs to $25 per month for eligible insured patients. Cash-pay discount programs through GoodRx, pharmacy partnerships, and telehealth services bring prices to roughly $300 to $500 per month. Compounded semaglutide offers another pathway for cost savings, though availability and pricing fluctuate. Some patients explore options through pharmacies like Empower Pharmacy or Olympia Pharmacy for more affordable compounded versions.
Because semaglutide treatment is ongoing, the cumulative cost becomes substantial. A year of brand-name Wegovy without insurance costs over $16,000. Even at discounted rates of $400 per month, that is $4,800 annually. Compare that to phentermine at $150 total for a 12-week course.
Cost comparison table
Cost factor | Phentermine | Semaglutide (Wegovy) |
|---|---|---|
Monthly cost (no insurance) | Under $50 | $1,000-$1,400 |
Monthly cost (with insurance) | $10-$30 | $0-$25 (if covered) |
Total 3-month cost | $100-$150 | $3,000-$4,200 |
Annual cost (no insurance) | N/A (short-term only) | $12,000-$16,800 |
Insurance coverage | Most commercial plans | Variable, improving |
Generic available | Yes | Not yet |
The cost-per-pound-lost calculation favors phentermine in absolute terms but shifts when you factor in the amount of weight lost and the duration of results. Someone spending $150 on phentermine and losing 15 pounds is paying $10 per pound lost. Someone spending $4,800 per year on semaglutide and losing 33 pounds is paying roughly $145 per pound lost. But if the semaglutide user maintains that loss long-term and the phentermine user regains, the math changes completely.
Who should consider phentermine
Phentermine is not the inferior choice for everyone. Certain situations make it a reasonable, and sometimes preferable, option.
People who need quick results for a specific event or milestone. A wedding, a surgery that requires weight loss beforehand, a health scare that demands immediate action. Phentermine works fast, and sometimes fast is what you need.
People with limited budgets. If the choice is between phentermine and nothing, phentermine wins every time. Losing 5 to 10% of body weight, even temporarily, provides health benefits, from improved blood sugar to reduced joint strain to better sleep. The affordability question applies across all weight loss medications, and phentermine remains the most budget-friendly prescription option available.
People who are already close to their goal weight. If you only need to lose 10 to 15 pounds, a 12-week course of phentermine paired with solid lifestyle changes can get you there. The short treatment duration becomes a feature rather than a limitation when the weight loss goal is modest.
People who respond poorly to GLP-1 medications. Some individuals experience severe nausea, vomiting, or gastrointestinal distress on semaglutide that does not resolve with dose adjustments. Phentermine offers a completely different mechanism that avoids these GI side effects entirely.
People who want to jumpstart a lifestyle change. The 12-week phentermine window can serve as a catalyst. The rapid weight loss provides motivation. The reduced appetite makes it easier to establish new eating habits. If those habits stick, the phentermine has done its job even after it stops.
Who should consider semaglutide
Semaglutide fits a broader range of situations and generally delivers superior outcomes for most people seeking significant weight loss.
People with substantial weight to lose. If your goal is 30, 50, or 100+ pounds, phentermine simply cannot get you there. The 12-week treatment window and 5 to 10% weight loss ceiling are insufficient for major transformations. Semaglutide sustained use over months to years can achieve the kind of weight loss that changes health trajectories. Understanding real transformation timelines helps calibrate expectations.
People with type 2 diabetes or prediabetes. Semaglutide directly improves glycemic control through multiple mechanisms beyond weight loss alone. The dual benefit makes it a more efficient treatment for people managing both weight and blood sugar.
People with cardiovascular concerns. This one might seem counterintuitive, since semaglutide is a medication that could theoretically affect the heart. But semaglutide actually tends to lower blood pressure and improve cardiovascular markers. Phentermine does the opposite, raising heart rate and blood pressure. For anyone with hypertension or cardiovascular risk, semaglutide is the safer choice by a wide margin.
People who need long-term appetite management. Some individuals have biological hunger drives that lifestyle changes alone cannot overcome. Semaglutide provides sustained appetite reduction that can be maintained for years. This long-term management approach is not available with phentermine.
People who have tried and failed with phentermine. If phentermine provided temporary results followed by complete regain, the switch to a GLP-1 approach often delivers different outcomes because the mechanism is fundamentally different.
Can you take phentermine and semaglutide together
This question comes up constantly. And the answer is more nuanced than a simple yes or no.
Some practitioners do prescribe phentermine alongside GLP-1 receptor agonists. The rationale is that the two medications work through completely different mechanisms, phentermine through norepinephrine release and semaglutide through GLP-1 receptor activation, so they could theoretically complement each other. A study found that phentermine may help certain patients lose more weight after discontinuing GLP-1 medications, suggesting potential utility as a bridge medication.
However, combining these medications is off-label and not supported by large-scale clinical trials. The detailed analysis of combining these medications reveals important considerations about side effect overlap, monitoring requirements, and clinical evidence gaps.
If you are considering combining these medications, this is absolutely a conversation to have with your prescribing physician. The interaction profile, while not dangerous in most cases, requires professional oversight to manage effectively. SeekPeptides provides educational resources to help you ask the right questions during those conversations.
Semaglutide vs phentermine for different health conditions
Weight loss rarely happens in a vacuum. Most people considering these medications have other health conditions that influence which drug makes more sense.
With high blood pressure
Semaglutide wins clearly. It tends to lower blood pressure as a secondary benefit. Phentermine raises blood pressure, sometimes significantly. For anyone with hypertension, even controlled hypertension, phentermine adds cardiovascular risk that semaglutide avoids.
With type 2 diabetes
Again, semaglutide. It was originally developed as a diabetes medication (Ozempic) before the weight loss applications became clear. The blood sugar improvements are substantial and clinically meaningful. Phentermine has no direct effect on blood sugar beyond what weight loss itself provides.
With anxiety or sleep issues
Semaglutide is preferable. Phentermine is a stimulant that commonly causes insomnia, anxiety, and restlessness. These side effects can worsen existing anxiety disorders and disrupt sleep patterns. Semaglutide does not have stimulant properties and rarely causes sleep disruption. Understanding anxiety-related side effects of GLP-1 medications provides additional context for people managing mental health alongside weight loss.
With a history of substance abuse
Semaglutide. Phentermine is a controlled substance with amphetamine-like properties. It is explicitly contraindicated in people with a history of drug abuse. Semaglutide has no abuse potential and no dependency risk.
With kidney disease
Semaglutide. Phentermine levels can accumulate in patients with kidney disease, increasing the risk of adverse effects. Semaglutide dosing does not require adjustment for renal impairment in most cases.
For people over 65
Semaglutide, with caution. Phentermine carries higher cardiovascular risks that become more concerning with age. Semaglutide cardiovascular profile is more favorable, though muscle loss is a concern for older adults on any weight loss medication. The specific considerations for different demographics should inform medication selection.
The oral semaglutide option
One common objection to semaglutide is the injection requirement. Many people prefer the simplicity of swallowing a pill, which is exactly what phentermine offers.
Oral semaglutide (Rybelsus) provides an alternative, though it was originally approved for type 2 diabetes rather than weight loss. Recent studies show oral semaglutide at a dose of 25 mg achieved a mean weight loss of 13.6% from baseline to week 64, comparable to injectable semaglutide. The oral semaglutide guide covers the specific protocols, bioavailability differences, and practical considerations of the pill form.
This changes the comparison somewhat. If needle aversion is the primary barrier to semaglutide, the oral formulation removes that obstacle. However, oral semaglutide requires strict administration protocols, it must be taken on an empty stomach with no more than 4 ounces of water, followed by a 30-minute wait before eating or drinking anything else. Phentermine has no such restrictions.
For those who are comfortable with injections, understanding proper injection technique and injection fundamentals eliminates most concerns about the process.
Diet and lifestyle considerations with each medication
Neither phentermine nor semaglutide works in isolation. What you eat, how you move, and what habits you build during treatment determine whether the results last beyond the prescription.
Eating on phentermine
Phentermine suppresses appetite aggressively. Many users find they can barely eat 800 to 1,000 calories per day without feeling forced. While the rapid calorie restriction drives weight loss, it can also lead to nutritional deficiencies, muscle loss, and metabolic adaptation that makes weight regain more likely after stopping.
The smart approach is to eat structured meals even when appetite is minimal. Protein intake becomes critical because muscle preservation during rapid weight loss depends on adequate protein consumption. Aim for at least 0.7 grams of protein per pound of body weight daily, even if it means forcing meals. Hydration matters more than usual because phentermine causes dry mouth and increased fluid loss.
Eating on semaglutide
Semaglutide reduces appetite more gradually and affects food preferences differently. Many users report decreased interest in high-calorie, high-fat foods specifically. The slowed gastric emptying means smaller portions feel satisfying. The dietary approach with semaglutide focuses on nutrient density because you are eating less overall.
Following a structured semaglutide diet plan optimizes results. The foods to minimize on GLP-1 medications include high-fat items that worsen nausea and high-sugar foods that counteract the blood sugar benefits. Protein remains critical, as with phentermine, because preserving muscle mass during extended weight loss requires deliberate attention to protein intake.
Some users find that meal planning strategies designed for GLP-1 medications help them navigate the reduced appetite without sacrificing nutrition. The key difference from phentermine is time. You have months to years on semaglutide to refine your eating habits, compared to weeks on phentermine.
Supplements and supporting protocols
Both medications benefit from strategic supplementation. Vitamin B12 depletion is a concern with GLP-1 receptor agonists, which is why some formulations now include B12. The semaglutide and B12 combination addresses this directly. Adding glycine supplementation has shown additional benefits for users on GLP-1 medications, supporting muscle preservation and metabolic health during weight loss.
A multivitamin is advisable with either medication because reduced food intake means reduced micronutrient intake. Fiber supplementation helps manage the digestive changes that both medications can cause, though through different mechanisms.
Alternative GLP-1 medications to consider
If this comparison has you leaning toward the GLP-1 approach but semaglutide specifically does not feel right, several alternatives exist within the same drug class.
Tirzepatide (Mounjaro/Zepbound) is a dual GIP/GLP-1 receptor agonist that has shown even greater weight loss than semaglutide in head-to-head trials. The semaglutide vs tirzepatide comparison reveals meaningful differences in weight loss percentages, side effect profiles, and dosing schedules. Tirzepatide users in the SURMOUNT-1 trial lost up to 22.5% of body weight, substantially more than semaglutide STEP trial results.
For those interested in the practical aspects, the tirzepatide dosing guide covers titration schedules and administration. Understanding side effect differences between the two GLP-1 options helps narrow the choice further.
Retatrutide is a triple agonist (GIP/GLP-1/glucagon) currently in clinical trials that has shown weight loss exceeding 24% of body weight. The retatrutide vs semaglutide comparison explores this next-generation option. While not yet commercially available, the retatrutide availability timeline suggests it could enter the market within the next few years.
Cagrilintide works through the amylin pathway, a different mechanism that complements GLP-1 agonists. The cagrilintide and semaglutide combination (known as CagriSema) is being studied as a next-generation obesity treatment. Understanding CagriSema dosing protocols gives perspective on where the field is heading.
The broader landscape of weight loss compounds continues to evolve rapidly, with multiple new mechanisms entering clinical trials. SeekPeptides tracks these developments and provides updated protocols as new data emerges.
Reconstitution, storage, and practical handling
Phentermine requires zero preparation. You open the bottle, take a pill, and close the bottle. Storage is straightforward, room temperature, away from moisture and heat.
Semaglutide, in its injectable form, demands more attention. Unused pens must be refrigerated between 36 and 46 degrees Fahrenheit. Once in use, the pen can be kept at room temperature (up to 86 degrees) for 56 days. The storage duration for compounded semaglutide differs from branded pens and depends on the formulation.
Compounded semaglutide in vial form requires reconstitution with bacteriostatic water before use. This adds a step that some users find intimidating initially but becomes routine quickly. The mixing ratios must be precise to ensure accurate dosing. For those using a 5mg vial, the calculations differ from larger concentrations.
Using a reconstitution calculator eliminates guesswork. The SeekPeptides reconstitution calculator handles the math automatically, reducing the risk of dosing errors that can affect treatment outcomes.
Proper handling extends the life and effectiveness of your medication. The comprehensive storage guide covers temperature management, light exposure, and contamination prevention, topics that are completely irrelevant for phentermine users but critical for semaglutide users.
Understanding the dosage conversion question
Some users transition from phentermine to semaglutide, or from one GLP-1 to another. There is no direct dosage conversion between phentermine and semaglutide because they are fundamentally different drug classes. You cannot say that 37.5 mg of phentermine equals X mg of semaglutide. The mechanisms, pharmacokinetics, and dose-response curves have nothing in common.
When transitioning from phentermine to semaglutide, you start semaglutide at the standard initial dose of 0.25 mg weekly regardless of your phentermine history. Some clinicians overlap the medications briefly during the transition, continuing phentermine while semaglutide titrates up, then discontinuing phentermine once semaglutide reaches therapeutic levels. Others stop phentermine first and start semaglutide after a washout period.
The conversion between different GLP-1 medications is more straightforward because they share receptor targets. But phentermine to semaglutide requires starting fresh with the full titration protocol. Understanding semaglutide dosing in units helps navigate the practical aspects of this transition.
Real-world considerations most guides miss
Clinical trial data tells you what happens under controlled conditions. Real-world experience adds context that trials cannot capture.
Alcohol interactions
Phentermine combined with alcohol increases the risk of cardiovascular side effects and can cause dizziness, impaired judgment, and increased heart rate. The stimulant and depressant combination is inherently unpredictable.
Semaglutide combined with alcohol is generally safer but not without considerations. Many users report decreased alcohol tolerance while on semaglutide. The guide to alcohol and semaglutide covers the specific interactions, including the increased nausea risk and the effect on blood sugar when combining GLP-1 medications with alcohol.
Exercise performance
Phentermine is a stimulant that can enhance short-term exercise performance through increased energy and alertness. Some users appreciate this effect for maintaining workout routines during treatment. However, the elevated heart rate means monitoring becomes important during intense exercise.
Semaglutide does not directly affect exercise performance, but the reduced caloric intake can lead to decreased energy during workouts, especially in the first months. The energy question is common among new users. Adjusting workout timing and intensity during the titration phase helps maintain fitness while the body adapts.
Hair loss
Rapid weight loss from any cause can trigger telogen effluvium, a temporary hair shedding condition. Both phentermine and semaglutide users may experience this. The GLP-1 and hair loss guide explains the mechanism, timeline, and strategies for minimizing this side effect. Adequate protein intake is the single most important preventive measure.
Travel considerations
Phentermine travels easily. A pill bottle fits in a carry-on. No temperature concerns. No sharps disposal issues.
Injectable semaglutide requires a cold pack for extended travel, sharps containers for needle disposal, and understanding of TSA regulations regarding injectable medications. Temperature stability during travel varies by formulation, and planning ahead prevents potency loss.
The future of these medications
The weight loss medication landscape is evolving faster than at any point in pharmaceutical history. Understanding where these two medications stand in that evolving landscape provides important context.
Phentermine has likely reached the end of its development arc. No major pharmaceutical company is investing in improving it. No new formulations are in development. It will remain available as an inexpensive, short-term option, but it will not improve.
Semaglutide, by contrast, sits at the beginning of an era. Next-generation GLP-1 medications like retatrutide and mazdutide build on the foundation semaglutide established. Oral GLP-1 formulations are improving. Higher-dose protocols are being studied. Combination therapies like CagriSema promise even greater efficacy.
Emerging alternatives like the Onmorlo GLP-1 patch could eliminate both the injection requirement and the strict oral dosing protocols, making GLP-1 therapy as simple as applying a patch. And innovations like sublingual GLP-1 drops are expanding the available delivery options.
The pricing picture will also shift. As semaglutide patents expire and generics enter the market, the cost gap between phentermine and semaglutide will narrow. Compounded versions already offer substantial savings, and this trend will accelerate.
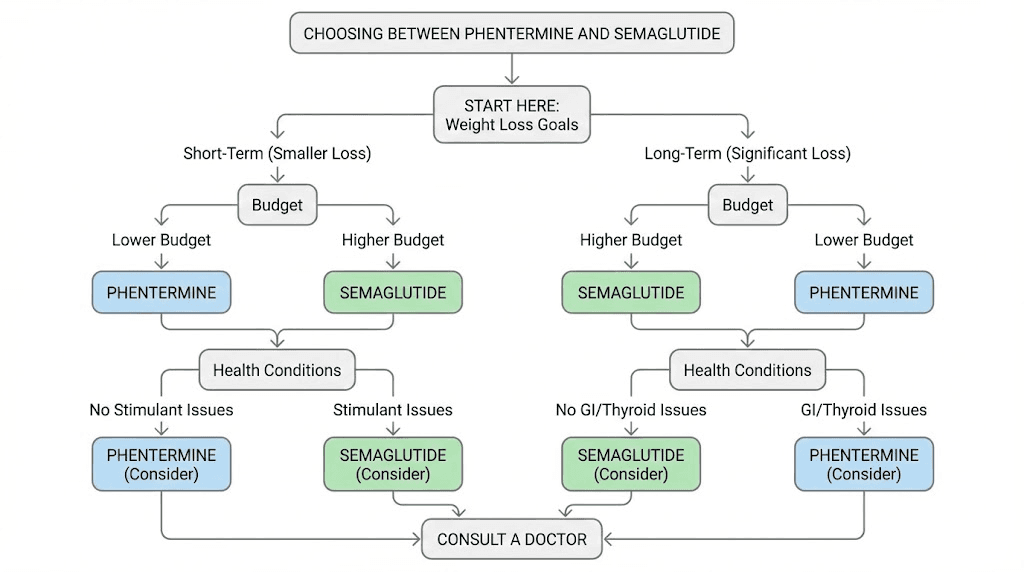
Making your decision
After examining every angle of this comparison, the decision framework becomes clearer. Neither medication is universally superior. But one is almost certainly better for your specific situation.
Choose phentermine if:
You need rapid, short-term weight loss (10-20 pounds)
Budget is a primary constraint
You have no cardiovascular concerns
You are not taking medications that interact with stimulants
You have a solid plan for maintaining results after stopping
You prefer pills over injections and cannot use oral semaglutide
Choose semaglutide if:
You have substantial weight to lose (30+ pounds)
You need long-term appetite management
You have type 2 diabetes or prediabetes
You have cardiovascular risk factors
Previous weight loss attempts have failed
You want the option to continue treatment as long as needed
You value the metabolic benefits beyond weight loss alone
For most people with significant weight loss goals and no budget constraints, semaglutide delivers superior outcomes across nearly every metric. But phentermine fills a legitimate role for people who need a short-term boost, cannot afford GLP-1 medications, or have specific medical situations where stimulant-based appetite suppression is preferable.
The SeekPeptides peptide calculator and semaglutide dosage calculator help with the practical implementation once you have made your choice. And for those exploring the broader landscape of research compounds beyond these two medications, the decision tree expands further.
For researchers serious about optimizing their weight loss protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Frequently asked questions
Is phentermine safer than semaglutide?
No. Phentermine carries higher cardiovascular risks including elevated heart rate, increased blood pressure, and dependency potential as a Schedule IV controlled substance. Semaglutide has a more favorable safety profile with primarily gastrointestinal side effects that typically resolve over time. However, semaglutide does carry rare risks including pancreatitis and gallbladder complications.
Can I switch from phentermine to semaglutide?
Yes. There is no direct dosage conversion, so you start semaglutide at the standard 0.25 mg weekly dose regardless of your phentermine history. Some physicians overlap the medications during transition while others prefer a washout period. The appetite suppression timeline on semaglutide means there may be a gap in coverage during the switch.
Which medication works faster for weight loss?
Phentermine produces visible results within 1 to 2 weeks because of its immediate stimulant-based appetite suppression. Semaglutide takes 4 to 8 weeks to show meaningful results due to the gradual dose titration schedule. However, semaglutide produces greater total weight loss over time, averaging 14.9% versus phentermine 5 to 10%.
Does insurance cover both medications?
Insurance coverage varies significantly. Phentermine is covered by most commercial plans and costs under $50 per month even without insurance. Semaglutide coverage is inconsistent, with many plans covering it for diabetes (Ozempic) but not weight loss (Wegovy). Without insurance, semaglutide costs $1,000 to $1,400 monthly compared to under $50 for phentermine.
Will I regain weight after stopping either medication?
Weight regain is a risk with both medications. After stopping phentermine, about 58% of users experience some weight regain. After stopping semaglutide, participants in the STEP 1 trial extension regained two-thirds of their lost weight within one year. Sustained treatment adherence and lifestyle changes are critical for maintaining results with either medication.
Can phentermine and semaglutide be taken together?
Some physicians prescribe both simultaneously because they work through different mechanisms. This is an off-label combination that requires medical supervision. The detailed combination guide covers the evidence, risks, and monitoring requirements for dual therapy.
Is there a GLP-1 medication better than semaglutide?
Tirzepatide (Mounjaro/Zepbound) has demonstrated greater weight loss than semaglutide in clinical trials, with participants losing up to 22.5% of body weight. The semaglutide vs tirzepatide comparison provides a detailed head-to-head analysis. Newer agents like retatrutide show even greater potential but are not yet commercially available.
External resources
NCBI StatPearls: Topiramate and Phentermine clinical reference
STEP 1 trial extension: Weight regain after semaglutide withdrawal
NEJM: Once-weekly semaglutide in adults with overweight or obesity
Comparative effectiveness systematic review of semaglutide, liraglutide, orlistat, and phentermine
In case I do not see you, good afternoon, good evening, and good night. May your weight loss stay sustainable, your side effects stay manageable, and your choices stay informed.