Feb 5, 2026

Day one, you step on the scale and write down the number. It sits there, stubborn and familiar, the same number that has followed you for months. Maybe years. You have tried calorie counting. You have tried exercise routines that left you sore but no lighter. You have tried willpower, and willpower failed. Now you are holding a tirzepatide pen, wondering if this time will be different.
It will be.
But not in the way most articles describe. The transformation that tirzepatide produces is not a straight line from heavy to thin. It is messy, nonlinear, and deeply personal. Some people lose 15 pounds in the first month. Others barely notice the scale move until week eight, when suddenly everything shifts. The before-and-after photos you see online tell a fraction of the story. They show two snapshots separated by months, stripped of context, stripped of the nausea that hit at week three, the energy surge at week six, the moment you realized your relationship with food had fundamentally changed.
This guide covers the full picture. Not just the weight on the scale, but the body composition changes, the metabolic improvements, the side effects nobody warns you about, and the realistic timeline based on clinical trial data from over 10,000 participants. Whether you are considering tirzepatide, just starting, or months into treatment and wondering if your progress is normal, this is the reference you will keep coming back to.
SeekPeptides members have tracked thousands of tirzepatide journeys, and the patterns that emerge from real data tell a far more useful story than any single before-and-after photo ever could.
What the clinical trials actually show
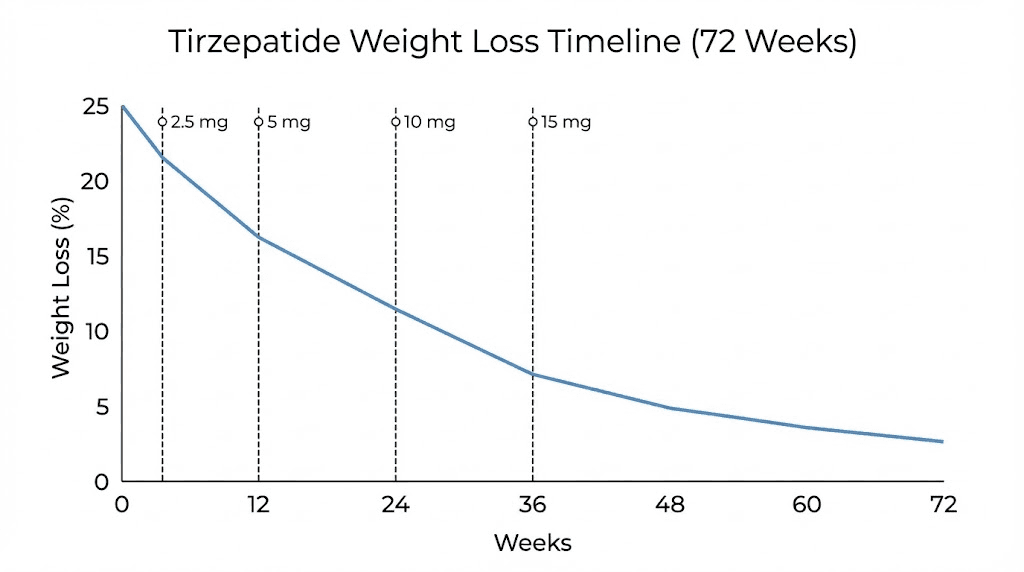
The SURMOUNT-1 trial remains the landmark study for tirzepatide and weight loss. Published in the New England Journal of Medicine, it enrolled 2,539 adults with obesity or overweight across 119 sites in nine countries. Participants received either tirzepatide at 5 mg, 10 mg, or 15 mg, or placebo, injected once weekly for 72 weeks. The results changed the conversation about pharmaceutical weight loss entirely. If you have been exploring bioactive peptides for weight loss, the SURMOUNT data provides the most rigorous evidence base available for any peptide-based treatment.
At 72 weeks, the numbers were striking. Participants on the 5 mg dose lost an average of 16.0% of their body weight, roughly 35 pounds. The 10 mg group lost 21.4%, about 49 pounds. And the highest dose, 15 mg, produced a 22.5% reduction, approximately 52 pounds. The placebo group lost 2.4%.
Those are averages. They matter because they represent what a large, diverse group of people experienced under controlled conditions with proper tirzepatide dosing protocols. But averages also hide the range. Some participants lost more than 25% of their body weight. Others lost less than 10%. Your results will depend on your starting weight, your dose, your adherence, your diet, your activity level, and factors researchers are still working to understand. The latest research continues to identify new variables that influence individual response.
The percentage thresholds that matter
Doctors and researchers track weight loss in percentage thresholds because a 5% reduction in body weight triggers measurable health improvements. At 10%, cardiovascular risk factors improve significantly. At 15% and beyond, metabolic changes approach what bariatric surgery produces. Tracking these thresholds accurately requires understanding your baseline measurements and using consistent methodology.
In SURMOUNT-1, the percentage of participants hitting these thresholds tells the real story. At the 5% threshold, 89% of participants on 5 mg got there. For the 10 mg and 15 mg doses, 96% achieved at least 5% weight loss.
Compare that to 28% in the placebo group.
The higher thresholds are where tirzepatide separates itself from everything else on the market. Between 78% and 84% of those on the 10 mg or 15 mg dose lost at least 10% of their body weight. Between 67% and 71% hit the 15% mark. And between 50% and 57% lost 20% or more. These are weight loss results that were previously only seen with surgical interventions.
How tirzepatide compares to semaglutide
The question everyone asks. The SURMOUNT-5 trial answered it directly, putting tirzepatide head-to-head against semaglutide over 72 weeks. Tirzepatide achieved an average weight loss of 20.2% compared to 13.7% for semaglutide. That is a meaningful difference, roughly 6.5 percentage points, which translates to about 15 additional pounds lost on average.
The mechanism explains the gap. Semaglutide is a GLP-1 receptor agonist, meaning it works on one hormonal pathway. Tirzepatide is a dual GIP and GLP-1 receptor agonist, hitting two pathways simultaneously. The GIP component adds metabolic benefits that amplify the appetite suppression and blood sugar regulation that GLP-1 provides alone. Think of it as stereo versus mono, same basic technology, but with more depth and range.
Both medications cause gastrointestinal side effects. Tirzepatide may cause slightly more nausea during dose escalation, but both settle down as the body adjusts. For a detailed breakdown, see our semaglutide vs tirzepatide comparison. If you are weighing the two options, understanding how these medications differ in practice matters more than the headline numbers. Factors like semaglutide dosing, injection frequency, and individual tolerance all influence which medication is the better fit for your specific goals and medical history.
The week-by-week timeline of tirzepatide results
Before-and-after photos collapse time. They show you where someone started and where they ended. They do not show the weeks where nothing seemed to happen, the plateau at month two, the sudden drop at month three. Understanding the timeline helps you stay the course when progress feels slow.
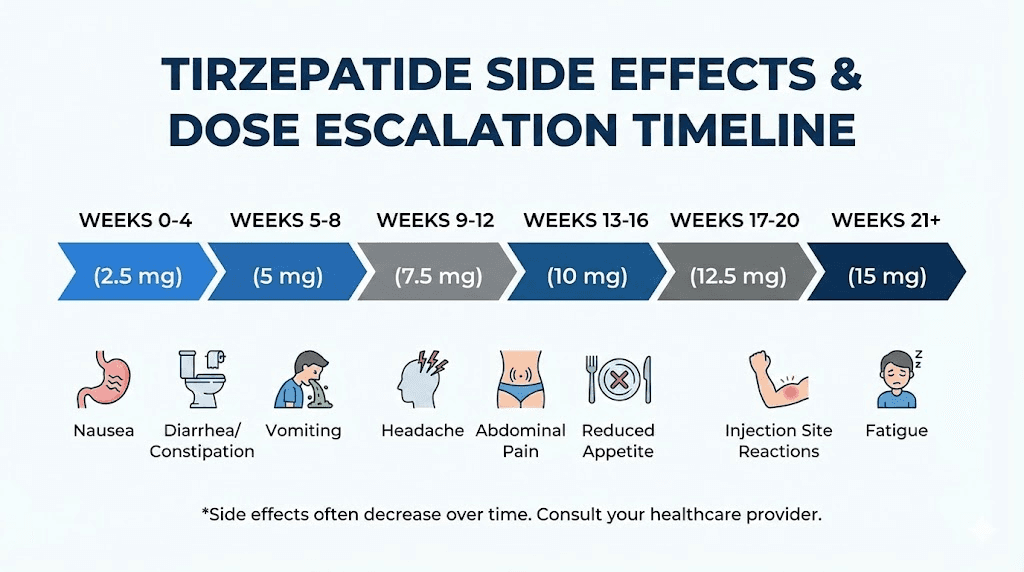
Weeks 1 through 4: the adjustment period
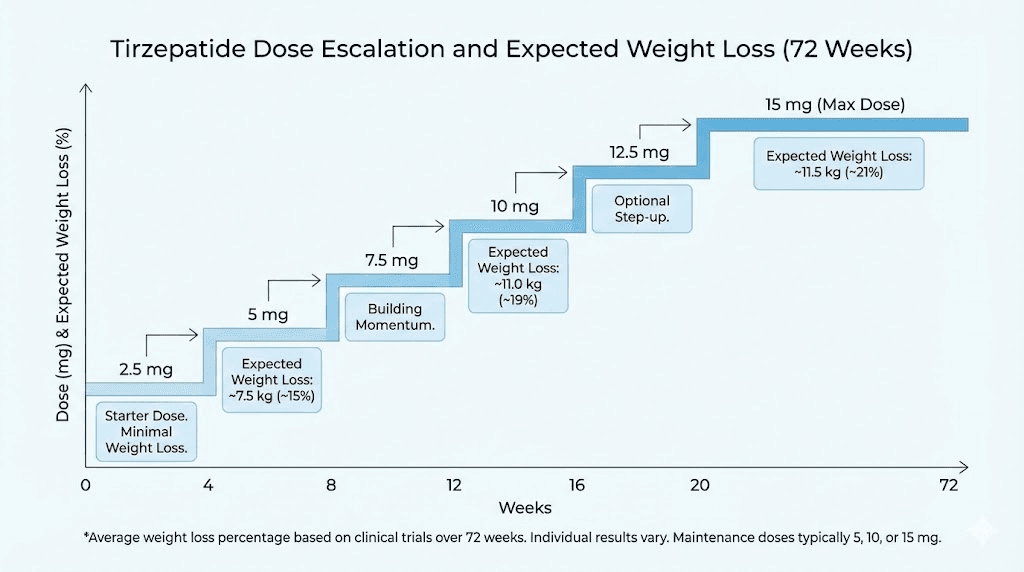
You start at 2.5 mg. This is not a treatment dose. It is a dose designed to let your body adjust to the medication with minimal side effects. The dose escalation schedule exists for good reason. Starting higher increases nausea, vomiting, and diarrhea significantly.
During these first four weeks, most people notice three things. First, appetite changes. You feel full faster. Meals that used to disappear become half-finished plates. Some people describe it as forgetting to eat, something that would have been unthinkable before. Second, subtle digestive changes. Mild nausea is common, especially in the first week. It typically fades. Third, the scale might move 3 to 5 pounds, though some of this is water and food volume reduction rather than fat loss.
Do not judge the medication by month one. The 2.5 mg dose is a handshake, not a full conversation. Many people who later achieve dramatic transformations described month one as unremarkable. Trust the process. If you want to understand the mechanism behind why this gradual approach works, our guide on how peptides work explains the receptor-level science.
Weeks 5 through 8: the dose increases and results begin
At week five, you move to 5 mg. This is where things start to change in ways you can feel. Appetite suppression becomes more pronounced. Cravings, particularly for high-calorie and high-sugar foods, often diminish noticeably. Many people report that food simply becomes less interesting, less of an event and more of a function.
Weight loss accelerates. By week eight, clinical data shows participants losing roughly 6% to 8% of their body weight. For someone starting at 220 pounds, that is 13 to 18 pounds. The rate varies, but the trend becomes unmistakable. Clothes fit differently. The face looks different in photos. People around you start to notice. Many people at this stage begin exploring weight loss strategies specific to their situation to amplify what the medication is already doing.
Side effects may flare briefly with the dose increase. Gastrointestinal symptoms like nausea, diarrhea, or constipation are most common during these transitions. They usually resolve within a week or two. Eating smaller meals more frequently, avoiding high-fat foods, and staying hydrated all help. Some people find that gut health support strategies like probiotics and ginger tea ease the transition. Learning proper injection techniques also reduces local discomfort and makes the weekly routine smoother.
Weeks 9 through 16: the acceleration phase
Depending on your response and your provider's guidance, you may increase to 7.5 mg, 10 mg, or stay at 5 mg if results are strong. Each increase typically comes with a brief adjustment period followed by enhanced effects.
This is the phase where before-and-after becomes visible to everyone. Weight loss rates of 1 to 3 pounds per week are typical. Body composition starts shifting in ways the scale does not fully capture, fat loss outpaces lean mass loss by a ratio of roughly 3 to 1, meaning for every 4 pounds lost, about 3 are fat and 1 is lean tissue. This is a favorable ratio, comparable to what dedicated fat loss protocols and even bariatric surgery produce. Some individuals combine their tirzepatide protocol with AOD-9604 or 5-amino-1MQ for additional metabolic support, though these combinations require careful medical oversight.
Energy levels often improve during this phase. As excess weight decreases, movement becomes easier. Sleep quality frequently improves. Blood pressure and blood sugar markers start normalizing. The changes become systemic, not just cosmetic. People who combine tirzepatide with complementary peptide stacks or supportive supplements often report even more pronounced energy improvements during this period.
For those tracking peptide dosages carefully, this is also the phase where finding your optimal maintenance dose matters most. Some people respond exceptionally well at 10 mg and never need the maximum dose.
Weeks 17 through 32: the transformation window
Months four through eight represent the core transformation period. Most participants in clinical trials reached their 10 mg or 15 mg maintenance dose by this point and sustained consistent weight loss throughout. The SURMOUNT-1 data shows that weight loss continues in a roughly linear fashion through week 40, with the rate slowing gradually after that.
By week 24, the average participant on 15 mg had lost approximately 18% of their starting body weight. At week 32, that number approached 20%. These are the timeframes where the dramatic before-and-after photos are typically taken.
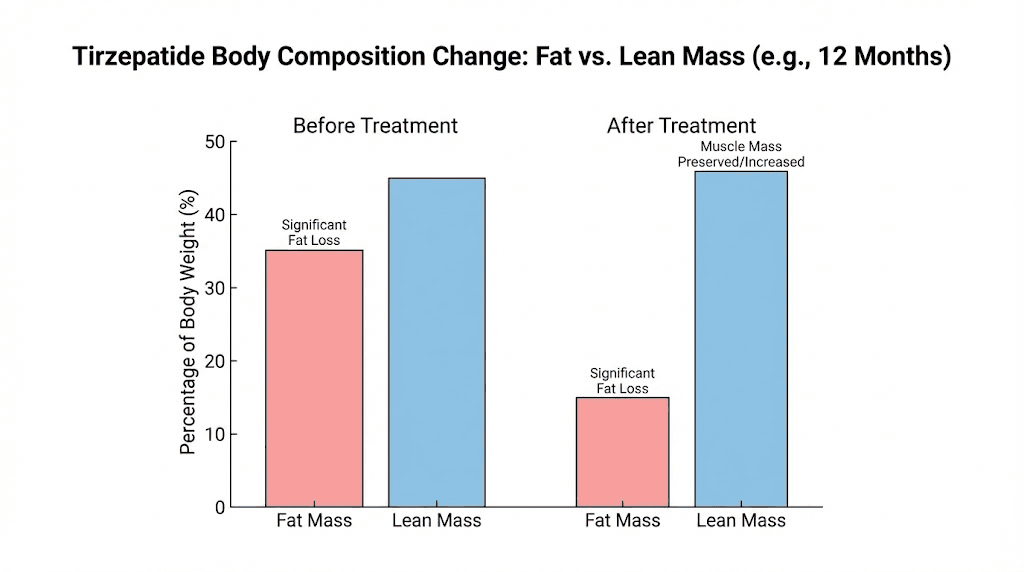
But the transformation is not just visual. Researchers in the SURMOUNT-1 body composition substudy found that tirzepatide-treated participants lost 33.9% of their fat mass compared to 8.2% in the placebo group. Lean mass decreased by 10.9% versus 2.6% with placebo. The key finding was that 75% of weight lost was fat and 25% was lean tissue, a ratio that confirms tirzepatide is not simply causing indiscriminate weight loss but preferentially targeting visceral and subcutaneous fat.
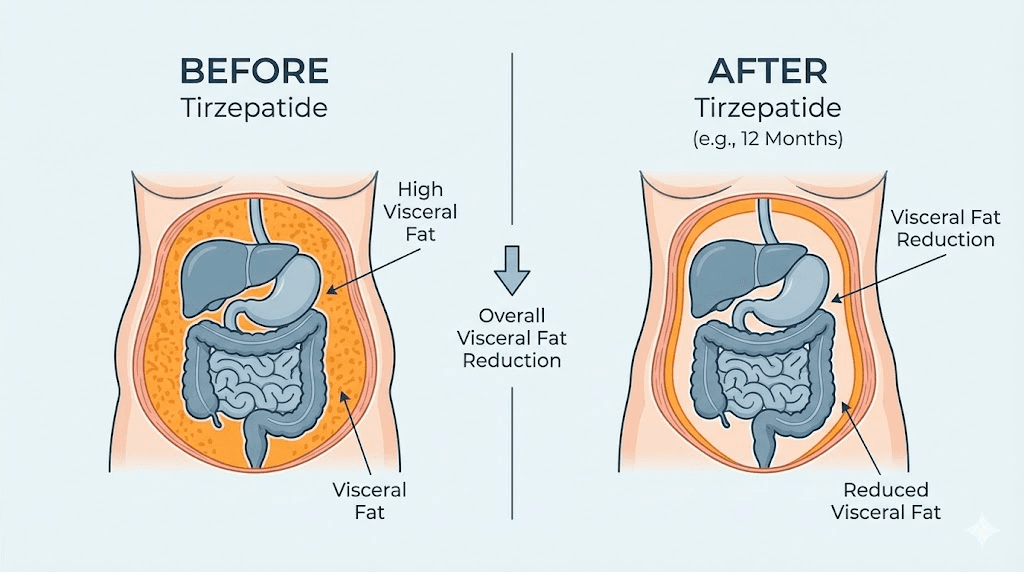
Waist circumference reductions averaged 7 to 10 inches in the higher-dose groups. Visceral adipose tissue, the dangerous fat surrounding organs, decreased substantially. These internal changes carry more health significance than the number on the scale. Understanding the lipotropic mechanisms behind fat mobilization helps explain why tirzepatide targets stored fat so effectively, particularly the abdominal and visceral fat deposits that other interventions struggle to address.
Weeks 33 through 72: the sustained results phase
Weight loss continues but decelerates. By week 40, most participants had achieved 80% or more of their total weight loss. The remaining weeks produced smaller, incremental changes. This is normal. The body reaches a new equilibrium, a lower set point where energy intake and expenditure are balanced at the new weight. Understanding how peptide timelines work helps calibrate expectations for this slower phase.
The SURMOUNT-4 trial specifically examined what happens during this maintenance phase. Participants who continued tirzepatide after initial weight loss maintained their results and lost an additional 5.5% from weeks 36 to 88. Those who switched to placebo regained a significant portion of their lost weight, highlighting that tirzepatide is not a temporary fix but an ongoing treatment for a chronic condition.
At 72 weeks, the full before-and-after picture emerges. Average weight loss of 16% to 22.5% depending on dose. Fat mass reduced by one-third. Waist circumference down by nearly a foot. Blood markers improved across the board. And for many participants, a fundamentally different relationship with food and body composition. The totality of these changes puts tirzepatide in a different category from previous weight loss medications and positions it alongside bariatric surgery for overall efficacy, a comparison that would have seemed absurd just a few years ago.
Body composition changes: beyond the scale
The scale lies. Or rather, it tells an incomplete truth. A person who loses 50 pounds of mostly fat while retaining muscle has achieved something profoundly different from someone who loses 50 pounds of mixed fat and muscle. Tirzepatide research has been unusually thorough in measuring body composition, giving us data that goes far beyond simple weight.
The fat-to-lean mass ratio
In the SURMOUNT-1 body composition substudy, researchers used dual-energy X-ray absorptiometry, the gold standard for measuring body composition, to track exactly what was being lost. The results were reassuring. Tirzepatide-treated participants lost weight in a ratio of 75% fat mass to 25% lean mass. This ratio held consistent across different doses, different starting weights, and different demographic subgroups.
Why does this matter? Because lean mass, which includes muscle, bone, and organ tissue, drives your metabolism. Losing too much lean mass slows your metabolic rate, making weight regain more likely. The 75/25 ratio places tirzepatide in the same category as well-designed exercise and nutrition programs and surgical interventions. It means the weight you lose is primarily the weight you want to lose.
For those concerned about muscle preservation during weight loss, combining tirzepatide with resistance training and adequate protein intake can further improve this ratio. Clinical guidance suggests at least 1.0 to 1.2 grams of protein per kilogram of body weight daily, with higher amounts for those who are physically active. Some researchers explore adding muscle-supportive peptides like BPC-157 or TB-500 alongside tirzepatide to support tissue repair and recovery during intense training, though this combination should only be considered under proper medical supervision. If you are interested in combining multiple peptides, understanding interaction profiles is essential.
Visceral fat reduction
Visceral fat is the fat packed around your liver, pancreas, and intestines. It is the most metabolically dangerous type of fat, driving insulin resistance, inflammation, and cardiovascular disease. You cannot see it in the mirror, but it shows up on imaging studies and in blood markers.
Tirzepatide produces significant reductions in visceral adipose tissue. The systematic review of randomized controlled trials found substantial decreases in waist circumference, which serves as a proxy for visceral fat, across all dose groups. These reductions were evident at intermediate follow-ups and continued through longer treatment periods.
This is one of the most important before-and-after metrics that never appears in photos. A person might lose 30 pounds and look modestly different in clothing, but internally, the reduction in visceral fat has transformed their metabolic health. Blood pressure drops. Insulin sensitivity improves. Inflammatory markers decrease. The fat loss you cannot see is often the fat loss that saves your life. Research on inflammation and peptides shows that reducing visceral fat decreases systemic inflammatory signals, creating a positive feedback loop where lower inflammation further supports metabolic improvements.
Metabolic improvements beyond weight
Weight is one number. The metabolic cascade that tirzepatide triggers produces improvements across dozens of biomarkers. In the SURMOUNT trials, participants experienced significant reductions in fasting insulin, HbA1c (even in non-diabetic participants), triglycerides, and blood pressure. HDL cholesterol increased. LDL cholesterol decreased. C-reactive protein, a marker of systemic inflammation, dropped substantially.
The SURMOUNT-1 three-year follow-up data revealed something even more remarkable. Among participants on tirzepatide, the rate of new-onset type 2 diabetes was dramatically lower: 0.4% for the 15 mg group compared to 13.3% for placebo over three years. Tirzepatide was not just treating existing metabolic dysfunction. It was preventing future disease. For anyone with metabolic health concerns, this is arguably more significant than the weight loss itself. The implications for longevity and healthspan are substantial, as preventing type 2 diabetes eliminates a cascade of downstream complications that would otherwise accumulate over decades.
Men versus women: different starting points, different results
The before-and-after experience is not gender-neutral. Research published in 2024 analyzing SURMOUNT trial data found consistent and significant differences between men and women on tirzepatide.
Weight loss differences by sex
Women lost more weight. Across all doses, female participants achieved greater percentage reductions in body weight compared to males. Women lost between 11.5% and 27.6% of their body weight depending on the dose and trial, while men lost between 8.8% and 18.9%.
Several factors explain this gap. Women typically have a higher starting percentage of body fat, which responds more readily to tirzepatide's metabolic effects. Pharmacokinetic differences mean that men may have lower drug exposure compared to women of the same weight. Hormonal differences in fat storage and mobilization also play a role.
This does not mean tirzepatide works poorly for men. An 18.9% body weight reduction is substantial and clinically meaningful by any standard. The fat loss results for men remain far superior to any other pharmaceutical intervention currently available. It simply means that men should calibrate their expectations accordingly rather than comparing their results to female participants' outcomes. Men looking to maximize results may benefit from exploring peptide protocols designed for men and understanding how testosterone-supporting strategies can complement weight loss efforts.
Cardiometabolic benefits by sex
Women also saw greater improvements in total cholesterol and LDL cholesterol. The cardiometabolic benefits were consistently more pronounced in female participants, with women experiencing about a 5% reduction in total cholesterol versus 3% in men, and a 10% reduction in LDL cholesterol versus 4% in men.
The safety profile was broadly similar between sexes, though women reported a numerically higher incidence of nausea and vomiting. This aligns with the generally higher drug exposure in female participants and echoes patterns seen with other GLP-1 based medications in women. For women navigating these considerations alongside hormonal changes, our guide on peptides for women over 40 and menopause-specific strategies provides additional context on how body composition changes interact with hormonal shifts.
The dose escalation journey: what each level feels like
Understanding what to expect at each dose level helps you interpret your own before-and-after journey. Each increase brings changes, both in results and in how the medication feels.
2.5 mg: the introduction
Expect: mild appetite reduction, possible mild nausea, minimal weight loss. This dose is about acclimation, not results. Your body is meeting tirzepatide for the first time, and the 2.5 mg dose gives your GI system time to adjust. Some people feel almost nothing at this dose. Others notice a distinct reduction in hunger. Both responses are normal. If you are new to peptide injections, this is also the time to establish your injection routine and become comfortable with the process.
Typical weight change: 2 to 5 pounds over 4 weeks. Much of this is reduced food volume and water weight rather than significant fat loss.
5 mg: the therapeutic threshold
This is where tirzepatide begins to work as intended. Appetite suppression becomes more consistent. Cravings diminish. The "food noise," that constant background hum of thinking about your next meal, quiets significantly. Many people describe this as the dose where their relationship with food shifts from emotional to functional.
Weight loss accelerates to roughly 1 to 2 pounds per week. Side effects may briefly intensify with the dose increase but typically resolve within 7 to 14 days. If you are using a dosage calculator to track your progress, this is the dose where the trend line starts pointing clearly downward.
7.5 mg: the middle ground
Not everyone needs this intermediate step, but for those who find 5 mg effective but not sufficient, 7.5 mg provides a meaningful boost without jumping to the higher doses. The appetite-suppressing effects deepen. Some people report that even the sight or smell of previously tempting foods no longer triggers cravings.
Weight loss continues at 1.5 to 2.5 pounds per week for most. GI side effects during transition are typically milder than the jump from 2.5 to 5 mg because the body has already adapted to the medication's mechanism.
10 mg: the sweet spot for many
Clinical data suggests that the 10 mg dose hits a favorable balance between efficacy and tolerability. SURMOUNT-1 participants on 10 mg lost an average of 21.4% of their body weight, only 1.1 percentage points less than the 15 mg group. For many people, the additional side effects of 15 mg do not justify the marginal improvement in results.
At this dose, the full range of tirzepatide's effects is typically apparent. Weight loss is consistent and significant. Metabolic markers improve measurably. Energy levels often increase as the body becomes lighter and more metabolically efficient. The optimal dosing for your situation depends on individual response, and 10 mg is where many people find their balance.
15 mg: the maximum dose
The highest approved dose produces the greatest average weight loss, 22.5% in SURMOUNT-1, but the incremental benefit over 10 mg is modest. Some people need this dose to achieve their goals. Others never progress beyond 10 mg and achieve excellent results.
Side effects at 15 mg are more common and more persistent. Nausea affects up to 29% of participants at higher doses. The decision to increase to 15 mg should be based on whether the 10 mg dose has plateaued and whether the potential additional weight loss justifies the increased side effect burden. Your provider can help you make this calculation using peptide calculators and clinical assessment. Understanding proper dosage calculations ensures accuracy at every dose level. Our reconstitution calculator is particularly useful for those working with compounded formulations where precision matters.
Real-world results versus clinical trial data
Clinical trials are controlled environments. Participants are screened, monitored, coached, and supported in ways that real-world patients often are not. So the question matters: do tirzepatide results hold up outside the trial setting?
The SHAPE study: real-world evidence
The SHAPE study, published in 2025, examined real-world weight loss in patients with overweight or obesity who did not have type 2 diabetes. After one year of treatment, the average weight loss with tirzepatide was 17.2 kg (about 38 pounds), representing 16.5% of body weight. These numbers are slightly lower than the clinical trial averages but remain highly significant and clinically meaningful.
The slight gap between trial and real-world results is expected. Real-world patients face inconsistent insurance coverage, medication interruptions, less dietary support, and variable dose escalation schedules. The fact that real-world results come within a few percentage points of trial data speaks to tirzepatide's robust efficacy even under imperfect conditions.
What separates high responders from moderate responders
Post-hoc analyses of the SURMOUNT trials identified patterns in who responds most strongly to tirzepatide. Early weight loss, defined as losing at least 5% of body weight within the first 12 weeks, predicted greater total weight loss at 72 weeks. This does not mean slow starters are doomed, but it suggests that the body's initial response to tirzepatide may indicate longer-term trajectory.
Factors associated with better outcomes include higher starting BMI (more weight to lose means larger absolute losses), female sex, younger age, absence of type 2 diabetes, and consistent adherence to the prescribed dose. Adding physical activity and dietary modifications amplifies results further.
The SURMOUNT-3 trial demonstrated this clearly. When tirzepatide was combined with intensive lifestyle intervention (structured diet, exercise, and behavioral counseling), participants achieved a total mean weight loss of 26.6%, roughly 64 pounds, over 84 weeks. That is significantly more than medication alone and illustrates why tirzepatide works best as part of a comprehensive approach rather than a standalone solution.
Digital engagement and enhanced outcomes
A 2025 retrospective study found that digital engagement, including app-based tracking, coaching, and community support, significantly enhanced weight loss outcomes in adults treated with tirzepatide. Patients who actively engaged with digital health tools lost more weight and maintained results more consistently than those who relied on medication alone.
This finding aligns with what SeekPeptides members experience. Having access to dosage tracking tools, community support, and structured protocols creates accountability and knowledge that amplify the medication's effects. The before-and-after results you see in engaged communities consistently outperform results from isolated, unsupported use. Whether you are using a cost calculator to plan your budget or a cycle planning guide to structure your protocol, having the right tools makes a measurable difference in outcomes.
The side effects timeline: what nobody shows in before-and-after photos
Every before-and-after photo hides a story about side effects. Understanding what to expect, when to expect it, and how to manage it makes the difference between staying the course and giving up prematurely.
Gastrointestinal effects
The most common side effects are GI-related, and they follow a predictable pattern tied to dose escalation.
Nausea affects 20% to 33% of participants across clinical trials. It is worst during the first two weeks after each dose increase. For most people, it is mild to moderate, feeling like low-grade motion sickness rather than severe illness. It resolves as the body adapts, typically within 7 to 14 days at each new dose level.
Diarrhea occurs in 18% to 23% of participants. Like nausea, it clusters around dose increases and diminishes with time. Staying hydrated is essential during these episodes.
Constipation affects a smaller percentage but can be persistent. Tirzepatide slows gastric emptying, which means food moves through your system more slowly. Fiber supplementation, adequate water intake, and gut health support strategies help manage this.
The critical insight from clinical data is that relatively few participants discontinued tirzepatide due to side effects. Most GI symptoms resolved on their own with time. The adjustment period is real, but it is temporary. If you are concerned about potential side effects, reviewing a comprehensive list of injectable peptides and their side effect profiles puts tirzepatide's tolerability in perspective. It compares favorably to most alternatives.
Fatigue and energy changes
Some people experience fatigue in the early weeks, particularly during dose escalation. This relates partly to reduced caloric intake, as the body adjusts to consuming fewer calories, energy levels can temporarily dip. Ensuring adequate protein and nutrient intake despite reduced appetite is critical.
Paradoxically, many people report increased energy as treatment progresses. As weight decreases and metabolic health improves, physical activity becomes easier and more enjoyable. By months three to four, the energy trajectory typically reverses, and many participants describe feeling more energetic than they have in years. For those wanting to maximize this energy improvement, combining tirzepatide with targeted energy optimization strategies can amplify the effect considerably.
Hair changes
Telogen effluvium, temporary hair shedding associated with rapid weight loss, has been reported by some tirzepatide users. This is not a direct drug effect but rather a consequence of significant caloric deficit and rapid body changes. It typically begins 2 to 4 months after the onset of rapid weight loss and resolves within 6 to 12 months. Adequate protein intake, hair support strategies, and ensuring sufficient micronutrient intake can minimize this effect. Some people explore peptides for hair growth as a supportive measure during this period. GHK-Cu and PTD-DBM are among the most researched options for supporting hair follicle health during periods of metabolic stress.
Injection site reactions
Minor. Redness, swelling, or itching at the injection site affects a small percentage of users. Rotating injection sites between the abdomen, thigh, and upper arm minimizes this. Most people find that injection technique improves with practice and reactions become negligible after the first few weeks.
Setting realistic expectations for your own before and after
The internet is full of extreme transformations. Someone lost 80 pounds in six months. Another person dropped five dress sizes in 12 weeks. These stories are real, but they represent the tail end of the distribution curve, the outliers. Calibrating your expectations to the clinical averages, rather than the viral success stories, protects your motivation and your mental health.
The realistic weight loss range by starting weight
If you start at 200 pounds and achieve the average result for the 10 mg dose (21.4% body weight reduction), you will lose approximately 43 pounds, ending at about 157 pounds. If you start at 250 pounds, that same percentage means losing about 54 pounds, ending at roughly 196 pounds. At 300 pounds, 21.4% is about 64 pounds, bringing you to approximately 236 pounds.
These numbers represent 72-week averages. Your personal result may be higher or lower. But framing your expectations around these ranges, rather than the 30-pounds-in-30-days narratives, keeps you grounded and committed to the process.
When to compare and when not to
Comparing your results to clinical trial averages is useful. Comparing your results to specific individuals on social media is not. Two people can take the same dose of tirzepatide and have vastly different outcomes based on genetics, starting body composition, activity level, diet quality, sleep patterns, stress levels, and dozens of other variables.
The most productive comparison is with yourself. Track your own metrics weekly: weight, waist circumference, how your clothes fit, energy levels, sleep quality, and any biomarkers your provider monitors. The transformation that matters is yours, measured against your own starting point. Using tools like a weight loss calculator to project realistic targets based on your individual data keeps expectations grounded in math rather than aspiration.
The plateau problem
Almost everyone hits a plateau. Weight loss stalls for two, three, sometimes four weeks despite consistent adherence. This happens because the body is recalibrating. Metabolic rate adjusts to a lower body weight. Hormonal signals shift. Water retention fluctuates.
Plateaus are not failure. They are a normal phase of the weight loss process that many people misinterpret as the medication stopping. In most cases, weight loss resumes after the plateau, either spontaneously or with a dose adjustment. The SURMOUNT data shows continuous weight loss through week 40 on average, with slowing but not stopping through week 72.
If you have been on a stable dose for 8 or more weeks with no change, discuss a dose increase with your provider. If you are already at 15 mg and plateaued, the focus shifts to lifestyle optimization, increasing protein, adding complementary strategies, and ensuring your caloric intake has not drifted upward unconsciously.
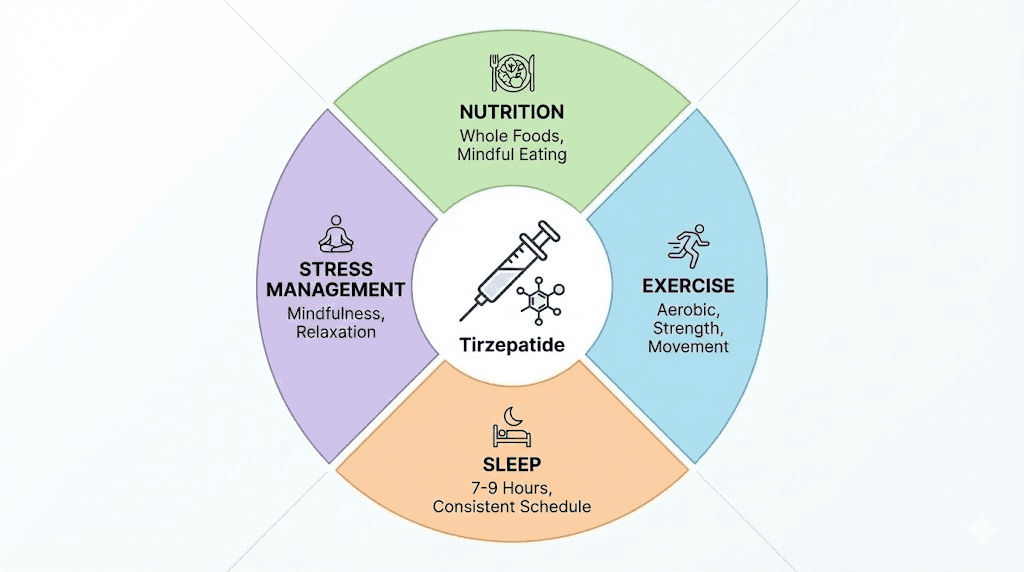
Maximizing your tirzepatide results
Medication creates the conditions for weight loss. What you do with those conditions determines how dramatic your before-and-after will be.
Nutrition strategies that amplify results
Tirzepatide reduces appetite, but it does not choose your food for you. The quality of what you eat during treatment matters enormously. Protein becomes especially critical because reduced caloric intake creates a risk of muscle loss, and adequate protein intake is the primary defense against that risk.
Target at least 1.0 to 1.2 grams of protein per kilogram of body weight daily. For a 200-pound person, that is roughly 90 to 110 grams of protein per day. Lean meats, fish, eggs, Greek yogurt, and legumes are excellent sources. If appetite suppression makes eating difficult, protein shakes and supplements can help you hit your targets without forcing large meals.
Beyond protein, focus on nutrient density. With reduced food intake, every bite matters more. Vegetables, fruits, whole grains, and healthy fats ensure you get the micronutrients your body needs to function well during rapid weight loss. A structured approach to nutrition, just like the structured approach to peptide protocols that produces the best outcomes, requires planning and consistency. Understanding which supplements support weight loss and which are unnecessary helps allocate both budget and stomach capacity toward what actually matters.
Exercise and muscle preservation
Resistance training is the single most important addition to a tirzepatide protocol for optimizing body composition. While the 75/25 fat-to-lean mass ratio is favorable, adding regular strength training can shift it even further toward fat loss while preserving or even building muscle. The science behind muscle growth and preservation during caloric deficit is well-established, and combining it with tirzepatide creates conditions for genuine body recomposition.
You do not need an extreme program. Two to three resistance training sessions per week targeting major muscle groups is sufficient. Start with body weight exercises if you are new to strength training, and progress to weighted movements as capacity allows. The combination of tirzepatide's metabolic effects and resistance training's muscle-preserving effects produces body composition changes that neither achieves as effectively alone.
Cardiovascular exercise supports overall health and can modestly increase caloric expenditure, but it is secondary to resistance training for body composition optimization during pharmaceutical-assisted weight loss. Walking 30 minutes daily is a simple, sustainable baseline. For those already active, understanding how tirzepatide interacts with athletic performance goals helps structure training around the medication's metabolic effects.
Sleep and stress management
Poor sleep undermines weight loss through multiple mechanisms: increased hunger hormones, decreased insulin sensitivity, reduced willpower, and impaired recovery from exercise. Research on GLP-1 medications has found that sleep disturbances can be a side effect for some users, making sleep hygiene even more important.
Aim for 7 to 9 hours per night. Consistent sleep and wake times, a cool and dark bedroom, limiting screens before bed, and avoiding large meals within 3 hours of sleep all contribute. If tirzepatide affects your sleep quality, discuss timing adjustments with your provider. Some people find that injecting in the morning rather than the evening minimizes nighttime GI discomfort.
Chronic stress elevates cortisol, which promotes visceral fat storage and undermines weight loss. Stress management techniques, whether meditation, walking, therapy, or social connection, are not luxuries during a weight loss protocol. They are strategic advantages. The relationship between stress and metabolic health is well-documented and directly relevant to your before-and-after outcome. Some researchers explore anxiolytic peptides like Selank for stress management, while others focus on sleep-supportive peptides to address the cortisol disruption at its root.
What happens when you stop tirzepatide
This is the chapter that every before-and-after article avoids. And it is the most important one.
The SURMOUNT-4 discontinuation data
The SURMOUNT-4 trial specifically studied what happens when you stop tirzepatide after successful weight loss. Participants first lost weight during a 36-week lead-in period on tirzepatide, then were randomized to either continue the medication or switch to placebo for an additional 52 weeks.
The results were sobering but predictable. Those who continued tirzepatide lost an additional 5.5% of their body weight and maintained 89.5% of their initial weight loss. Those who stopped and switched to placebo regained a significant portion, with the majority regaining half or more of their lost weight within a year.
This is not a failure of the medication. It is the nature of obesity as a chronic disease. Just as stopping blood pressure medication leads to blood pressure rising, stopping obesity medication leads to weight returning. The biological drivers, hormonal signals, metabolic adaptations, and neurological pathways, do not disappear because you spent time at a lower weight. They reassert themselves once the pharmacological support is removed.
Strategies for maintaining results
For those who must or choose to discontinue tirzepatide, the research suggests several protective strategies. Building significant muscle mass during treatment provides a metabolic buffer, as muscle burns more calories at rest. Establishing deeply ingrained dietary habits, not just relying on appetite suppression but developing genuine preferences for nutrient-dense foods, helps maintain lower caloric intake.
Transitioning to a lower maintenance dose rather than stopping abruptly may preserve more of the weight loss, though long-term data on this approach is still emerging. Working with a provider who understands peptide mechanisms and weight management can help develop a transition plan tailored to your situation. Our guide to finding qualified providers can help you locate practitioners who specialize in peptide therapy and understand the nuances of long-term management.
The honest answer is that for most people, tirzepatide is a long-term commitment, not a temporary intervention. Your before-and-after results are most likely to endure if the "after" includes continued treatment, continued attention to diet and exercise, and continued medical support. Understanding the proper storage of your medication and maintaining cold chain integrity ensures the tirzepatide you are using retains full potency throughout your treatment course. Compromised medication means compromised results, and many people underestimate how much storage conditions affect efficacy.
Specific before-and-after scenarios by goal
Different people come to tirzepatide with different objectives. The before-and-after picture looks different depending on where you start and what you are trying to achieve.
Scenario 1: significant weight loss (50 or more pounds to lose)
Starting point: BMI 35+, 50 to 100+ pounds above healthy weight range.
This population was the primary focus of the SURMOUNT trials and tends to see the most dramatic absolute weight loss. At the 15 mg dose, losing 22.5% of a 280-pound starting weight means approximately 63 pounds lost, ending near 217 pounds. Over 72 weeks, with lifestyle modifications, losses of 70 to 80 pounds are achievable for high responders.
The before-and-after transformation at this level is profound. Clothing sizes change by 4 to 6 sizes or more. Mobility improves dramatically. Joint pain decreases, and joint health improves as the mechanical load on knees, hips, and ankles reduces substantially. Sleep apnea resolves for many. The metabolic improvements are the most significant, with multiple comorbidity risks decreasing substantially. For those tracking their journey through before-and-after documentation, photos taken at baseline, 12 weeks, 24 weeks, and 48 weeks capture the progression most effectively. If joint pain was limiting exercise before, the weight reduction combined with supportive strategies for tendon and joint repair can create entirely new possibilities for physical activity.
Scenario 2: moderate weight loss (20 to 50 pounds to lose)
Starting point: BMI 27-34, seeking to reduce health risks and improve aesthetics.
This group often sees a faster percentage-based transformation because starting weights are lower. A 200-pound person losing 20% reaches 160 pounds, a change that is visually dramatic on most frames. The before-and-after for this group often centers on body composition rather than total pounds, clothes fitting better, more defined musculature as fat recedes, and a visible transformation in the face, neck, and midsection.
The 5 mg or 10 mg dose is often sufficient for this population, meaning lower side effect burden and lower cost. With strong lifestyle habits, results in the 20% to 25% range are achievable, particularly for those who add structured exercise to their protocol. This group also benefits from skin support strategies during weight loss, as moderate losses sometimes produce mild skin laxity that responds well to targeted care. Understanding how to support skin elasticity and anti-aging during transformation enhances the visual before-and-after outcome significantly.
Scenario 3: metabolic health focus (weight is secondary to biomarkers)
Starting point: prediabetes, insulin resistance, metabolic syndrome, or family history of type 2 diabetes.
For this group, the most important before-and-after data is not visible. It lives in lab results. Fasting glucose dropping from prediabetic ranges to normal. HbA1c normalizing. Triglycerides falling by 30% or more. Blood pressure decreasing enough to reduce or eliminate medications.
The SURMOUNT-1 three-year data showing that tirzepatide at 15 mg reduced new-onset type 2 diabetes to 0.4% versus 13.3% with placebo represents one of the most powerful preventive medicine findings in recent years. For people in this category, the before-and-after is measured in disease prevented, medications avoided, and years of health gained.
Scenario 4: body recomposition (athletes and active individuals)
Starting point: physically active, moderate excess weight, primary goal is improving body composition and performance.
This is the smallest group in clinical trials but a growing population in real-world use. For active individuals, tirzepatide's preferential fat loss with relative muscle preservation aligns well with body recomposition goals. Combined with structured resistance training and high protein intake, it is possible to lose significant fat while maintaining or even gaining muscle.
The before-and-after for this group shows less dramatic scale changes but striking visual transformation. A person might lose only 25 pounds but look like they lost 40 because the weight lost was almost entirely fat. Body composition analysis tools become more valuable than the scale for tracking progress in this population. Active individuals may also explore injury recovery peptides to support the increased training volume that tirzepatide-enhanced body composition enables, and energy-boosting strategies to maintain training intensity during caloric restriction.
Managing expectations month by month
Knowing what to expect month by month prevents the discouragement that leads to premature discontinuation. The pattern below reflects averages from clinical data and real-world observations for someone on a standard dose escalation to 10 mg or 15 mg.
Month 1 (2.5 mg)
Weight loss: 2 to 5 pounds. Appetite: mildly reduced. Side effects: mild nausea possible. Energy: unchanged or slightly reduced. Visible changes: minimal to none.
This month is about adjustment. Do not judge the medication here. Focus on establishing the injection routine, noting how the medication affects your appetite, and making initial dietary improvements. Use this time to increase protein intake, establish a walking routine, and set up tracking systems.
Month 2 (5 mg)
Weight loss: 8 to 15 pounds total. Appetite: noticeably reduced. Side effects: possible GI symptoms during dose transition, resolving by mid-month. Energy: beginning to stabilize. Visible changes: clothes fitting slightly differently, face may look slightly leaner.
This is the month where the medication begins working at therapeutic levels. Lean into the appetite suppression by making smart food choices rather than simply eating less of the same foods. Nutrient density matters more now because you are consuming fewer calories overall.
Month 3 (7.5 mg or 10 mg)
Weight loss: 15 to 25 pounds total. Appetite: significantly reduced. Side effects: brief GI adjustment to new dose. Energy: improving. Visible changes: noticeable to people around you, clothing sizes may change.
The transformation becomes visible. This is typically when people take comparison photos and realize how much has changed. Blood markers improve measurably if checked at this point. The timeline of results starts to feel real rather than theoretical.
Months 4 through 6 (10 mg to 15 mg)
Weight loss: 25 to 45 pounds total. Appetite: well-managed. Side effects: generally resolved. Energy: significantly improved. Visible changes: dramatic, multiple clothing sizes smaller, visible transformation in all photos.
The core transformation phase. Results accumulate rapidly. Health markers continue improving. Physical activity becomes easier and more enjoyable. This period produces the dramatic before-and-after comparisons that populate social media. Remember that this is also the phase where plateaus may occur. Stay the course.
Months 7 through 12 (maintenance dose)
Weight loss: 35 to 55+ pounds total. Appetite: stable. Side effects: rare. Energy: high. Visible changes: complete transformation visible.
Weight loss decelerates but continues. The body is approaching its new equilibrium. Focus shifts from maximizing weight loss to optimizing body composition and establishing sustainable habits for the long term. This is the period where decisions about long-term treatment, dose maintenance, and lifestyle sustainability become most relevant.
Common mistakes that undermine tirzepatide results
Not everyone who starts tirzepatide achieves the results seen in clinical trials. Understanding common pitfalls helps you avoid them.
Mistake 1: insufficient protein intake
Tirzepatide reduces appetite. If you simply eat less of a standard diet, you almost certainly are not getting enough protein. Inadequate protein accelerates lean mass loss, slows metabolism, and sets the stage for regain. Prioritize protein at every meal. Track it for at least the first few months until high-protein eating becomes automatic. Resources like the collagen peptides guide can help you understand whether collagen counts toward your protein goals and how to structure supplementation effectively.
Mistake 2: skipping resistance training
The 75/25 fat-to-lean mass ratio from clinical trials can likely be improved with resistance training. Without it, you lose muscle along with fat. With it, you preserve muscle and sometimes gain it, producing a body composition result that surpasses what medication alone achieves. Even bodyweight exercises performed consistently make a measurable difference in your weight loss and muscle preservation outcomes.
Mistake 3: escalating doses too quickly
Impatience leads some people to push for faster dose escalation. This increases GI side effects without proportionally increasing weight loss. The recommended 4-week minimum at each dose level exists because the body needs time to adjust. Rushing produces more discomfort, more missed doses due to side effects, and paradoxically slower progress.
Mistake 4: ignoring hydration
Reduced food intake means reduced water from food sources. Add GI side effects like diarrhea, and dehydration becomes a real risk. Dehydration causes fatigue, headaches, constipation, and impaired metabolic function. Aim for at least 64 ounces of water daily, more if you exercise or experience GI symptoms. Proper hydration also matters for peptide handling and ensures that any complementary protocols you are running maintain their efficacy.
Mistake 5: expecting linear progress
Weight loss is not linear. It zigzags, plateaus, and sometimes temporarily reverses due to water retention, hormonal fluctuations, or measurement variation. Tracking weekly averages rather than daily weights provides a more accurate picture of the trend. A week without scale movement does not mean the medication has stopped working. Body composition changes can occur even when the scale is static, and understanding normal patterns prevents unnecessary panic.
Mistake 6: not tracking comprehensive metrics
Weight alone is a poor metric. Waist circumference, progress photos, how clothes fit, energy levels, sleep quality, and blood markers all contribute to the full before-and-after picture. Some of the most meaningful transformations show modest scale changes but dramatic improvements in body shape, health markers, and quality of life. Using structured tracking approaches like those outlined in our protocol optimization guide ensures you capture the complete picture rather than fixating on a single number.
The psychological before and after
Physical transformation gets all the attention. The psychological transformation is equally profound and often more impactful on quality of life.
Food noise reduction
The term "food noise" has entered common usage through GLP-1 medication communities, and for good reason. Many people with obesity describe a constant mental preoccupation with food, thinking about the next meal, fighting cravings, negotiating with themselves about portions. Tirzepatide quiets this noise substantially for most users. The mechanism involves both GLP-1 and GIP signaling in brain regions that regulate reward and appetite, creating a fundamental shift in how the brain processes food-related stimuli.
The psychological relief is significant. Mental energy previously consumed by food decisions becomes available for other things. Decision fatigue around eating decreases. The emotional relationship with food shifts from struggle to neutrality. This change often surprises people more than the weight loss itself.
Confidence and self-image
As physical appearance changes, self-perception follows, though not always in a straight line. Some people experience a lag between their physical transformation and their mental self-image. They see the new body in the mirror but still feel like the old body. This adjustment takes time and sometimes benefits from professional support through therapy or counseling.
Others experience a rapid confidence boost that radiates into social relationships, professional life, and personal goals. The freedom from carrying excess weight, both physically and psychologically, opens doors that felt closed before. Some people channel this renewed energy into exploring cognitive enhancement and memory optimization, finding that the metabolic improvements from weight loss create a foundation for broader health optimization goals.
Navigating social dynamics
Significant weight loss changes how others interact with you. Some relationships improve. Others become strained as dynamics shift. Partners, friends, and family may respond with enthusiasm, jealousy, concern, or a complex mix of all three. Preparing for these social changes is as important as preparing for the physical ones.
Online communities, including resources available through SeekPeptides, provide spaces where people navigating these changes can share experiences and support each other. The psychological component of the tirzepatide journey is real, significant, and worthy of attention alongside the physical results. For those dealing with anxiety during their transformation, our guide on managing anxiety offers evidence-based approaches that complement the physical protocol. And for anyone feeling overwhelmed by the emotional dimensions of significant body changes, professional support is always a worthwhile investment.
Tirzepatide and type 2 diabetes: a different before and after
While this article focuses primarily on weight loss in people without diabetes, tirzepatide (as Mounjaro) was first approved for type 2 diabetes management. The before-and-after picture for people with diabetes includes an additional, crucial dimension: glycemic control.
The SURMOUNT-2 results
SURMOUNT-2 enrolled participants with obesity and type 2 diabetes. Weight loss was significant but somewhat lower than in the non-diabetic population: 13.4% at 10 mg and 15.7% at 15 mg. The reduced percentage reflects the metabolic complexity of type 2 diabetes and the fact that many diabetes medications promote weight retention.
But the glycemic improvements were remarkable. HbA1c decreased substantially, with many participants achieving normal or near-normal levels. Fasting glucose normalized. Some participants were able to reduce or eliminate other diabetes medications, including insulin. For this population, the before-and-after comparison includes a disease management dimension that extends well beyond body weight and into overall health outcomes.
Prevention: the most powerful before and after
Perhaps the most underappreciated result from the SURMOUNT program is the diabetes prevention data. Among non-diabetic participants with obesity, only 0.4% of those on tirzepatide 15 mg developed type 2 diabetes over three years, compared to 13.3% on placebo. That is a 97% relative risk reduction.
No before-and-after photo captures the significance of a disease that never develops. But for people with prediabetes, insulin resistance, or strong family histories of type 2 diabetes, this prevention data represents one of the most compelling reasons to consider tirzepatide, even if weight loss alone would not be sufficient motivation. The pancreatic peptide hormones involved in glucose regulation are central to understanding how tirzepatide achieves this prevention effect, and the research opens questions about which other legally available peptides might offer complementary metabolic benefits.
Understanding tirzepatide's mechanism: why it works differently
To fully appreciate the before-and-after transformation, understanding why tirzepatide works the way it does provides context that makes the results less surprising and more predictable.
The dual incretin advantage
Tirzepatide activates two incretin receptors simultaneously: GIP (glucose-dependent insulinotropic polypeptide) and GLP-1 (glucagon-like peptide-1). Most previous peptide medications in this class targeted only GLP-1. The addition of GIP activation is what makes tirzepatide's results consistently superior in head-to-head comparisons.
GLP-1 reduces appetite, slows gastric emptying, and improves insulin secretion. GIP adds complementary effects on fat metabolism, bone health, and potentially neuroprotective benefits. Together, they create a synergistic effect where the whole exceeds the sum of its parts. The mechanism has implications beyond weight loss, touching bone health, brain function, and hormonal balance in ways that single-receptor medications do not.
How appetite suppression evolves over treatment
The appetite suppression you experience on tirzepatide is not static. It evolves. In the first weeks, it feels like external pressure, a force reducing your desire to eat. By months two and three, it feels more natural, integrated into your baseline state. Many long-term users describe reaching a point where they cannot imagine eating the quantities they used to consume. The change feels permanent even though it is pharmacologically mediated.
This evolution matters for the before-and-after narrative because it means the early struggle with portion control and food choices gradually gives way to effortless moderation. The behavioral changes that were initially forced by appetite suppression become habitual, and those habits persist even if the medication is later reduced. Understanding the fundamentals of peptide therapy helps explain why this neurological adaptation occurs and how to work with it rather than against it.
The role of GIP in fat metabolism
GIP receptors are found on adipose tissue, and their activation by tirzepatide promotes healthy fat metabolism. This is partly why the body composition results are so favorable, with preferential fat loss rather than indiscriminate tissue loss. GIP signaling influences how the body stores, mobilizes, and utilizes fat, creating metabolic conditions that favor fat oxidation even outside of exercise.
For those interested in the broader science of peptide mechanisms, tirzepatide represents a new class of molecule that leverages the body's own hormonal systems rather than imposing external metabolic changes. The peptide formula was engineered to optimize binding affinity at both receptor sites, and the resulting pharmacodynamic profile is unlike anything previously available for weight management. The amylin pathway research that preceded tirzepatide laid groundwork for understanding how multiple hormonal signals can be targeted simultaneously for enhanced metabolic control.
How to document your own before and after
If you are starting tirzepatide, documenting your journey serves multiple purposes. It provides motivation during plateaus, helps your provider assess progress, and creates a record you will value in the future.
Photography best practices
Consistency is everything. Take photos at the same time of day, in the same location, with the same lighting, wearing the same or similar clothing. Front, side, and back views. Do this once per week at minimum, or monthly if weekly feels excessive.
Tip: set a recurring reminder on your phone. Take the photos even when you feel like nothing has changed. The comparison between week 1 and week 12 often reveals changes that happened so gradually you did not notice them day to day. If you are documenting a broader peptide transformation journey, having a consistent visual record becomes invaluable for tracking what works and what needs adjustment.
Metrics to track
Beyond weight, track these metrics weekly or biweekly:
Waist circumference at the navel, first thing in the morning
Hip circumference at the widest point
Energy level on a 1 to 10 scale
Sleep quality on a 1 to 10 scale
Appetite level on a 1 to 10 scale
Side effects type and severity
Exercise type and duration
Request blood work from your provider at baseline, 12 weeks, and 24 weeks at minimum. Key markers include fasting glucose, HbA1c, lipid panel, liver function, and inflammatory markers. These invisible before-and-after numbers often tell the most important part of the story, and tracking them through structured protocols ensures nothing gets missed.
Journaling the experience
Brief daily or weekly notes about how you feel, what you ate, what challenges you faced, and what victories you achieved create a narrative that photos and numbers cannot capture. Six months from now, reading about the first week of nausea or the day you fit into old jeans will provide perspective that raw data lacks. This kind of documentation also helps your provider make better dosing decisions based on your response patterns and helps you identify which common mistakes to avoid as you progress through the protocol.
Frequently asked questions
How much weight can I realistically expect to lose on tirzepatide?
Clinical trials show average weight loss of 16% to 22.5% of body weight over 72 weeks, depending on dose. For a 220-pound person, that translates to roughly 35 to 50 pounds. Real-world data shows slightly lower averages around 16.5%, but individual results vary significantly based on dose, lifestyle factors, and adherence. Use our peptide calculator to estimate based on your starting weight.
When will I start seeing visible results?
Most people notice visible changes between weeks 6 and 12, though the timeline depends on starting weight, dose, and individual physiology. The initial 2.5 mg dose produces minimal visible change. Noticeable differences typically appear after transitioning to the 5 mg therapeutic dose and beyond. Facial changes often appear first, followed by midsection reduction.
Is the weight loss from tirzepatide mostly fat or muscle?
Research from the SURMOUNT-1 body composition substudy shows that 75% of weight lost is fat and 25% is lean tissue. This is a favorable ratio comparable to surgical weight loss. Adding resistance training and adequate protein intake can further improve this ratio in favor of fat loss.
Do men and women get different results on tirzepatide?
Yes. Clinical data shows women typically lose a higher percentage of body weight than men, ranging from 11.5% to 27.6% for women versus 8.8% to 18.9% for men. This difference is attributed to pharmacokinetic variations, body composition differences, and hormonal factors. Both sexes achieve clinically significant results.
What happens to weight loss results if I stop taking tirzepatide?
The SURMOUNT-4 trial showed that discontinuing tirzepatide leads to significant weight regain in most participants. Those who continued the medication maintained their results and lost additional weight. Obesity is a chronic condition, and tirzepatide works best as an ongoing treatment rather than a temporary intervention. Strategies for maintaining results without medication include resistance training, high-protein diets, and comprehensive health protocols.
How do tirzepatide results compare to semaglutide?
In the SURMOUNT-5 head-to-head trial, tirzepatide achieved 20.2% average weight loss versus 13.7% for semaglutide over 72 weeks. The 6.5 percentage point advantage reflects tirzepatide's dual GIP/GLP-1 mechanism. See our detailed comparison page for a full breakdown.
Can I improve my tirzepatide results with lifestyle changes?
Significantly. The SURMOUNT-3 trial showed that combining tirzepatide with intensive lifestyle intervention produced 26.6% weight loss versus approximately 21% with medication alone over similar timeframes. Resistance training, high-protein nutrition, adequate sleep, and stress management all amplify results. SeekPeptides members access structured protocols that combine these elements with medication guidance for optimal outcomes.
Are tirzepatide side effects worse at higher doses?
GI side effects are dose-dependent, with nausea affecting up to 29% at the highest doses versus lower percentages at 5 mg. However, most side effects occur during dose escalation rather than at a stable dose. Following the recommended escalation schedule of at least 4 weeks per dose level minimizes discomfort.
External resources
For researchers and health-focused individuals committed to optimizing their tirzepatide journey, SeekPeptides provides the most comprehensive resource available. Members access evidence-based protocols, real community results, progress tracking tools, and expert guidance that transforms a generic prescription into a personalized optimization plan.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay consistent, your progress stay visible, and your health markers stay in the green. Join here.