Feb 9, 2026

Before you attribute that racing heart to anxiety, consider this. The trembling hands, the sudden wave of nervousness, the feeling that something is just not right.
These are real. They are uncomfortable. And for the growing number of people using tirzepatide for weight loss or type 2 diabetes management, they raise a question that demands a thorough answer. Can tirzepatide actually cause anxiety?
The short answer is complicated. Clinical trials involving thousands of participants have not identified anxiety as a common side effect. In fact, post hoc analyses of the SURMOUNT trials suggest that tirzepatide may be associated with lower rates of anxiety compared to placebo. But pharmacovigilance databases tell a different story, one where 144 cases of anxiety have been reported among GLP-1 receptor agonist users. And real-world patients, the ones living with this medication day to day, sometimes describe mood changes that clinical trial data alone cannot explain.
This guide examines every angle. The clinical research, the neurological mechanisms, the psychological factors that masquerade as medication side effects, and the practical strategies for managing anxiety while on tirzepatide. Whether you are starting your first tirzepatide dose, adjusting your protocol, or simply trying to separate real side effects from unrelated symptoms, this comprehensive breakdown will give you the evidence you need to make informed decisions about your health.
What the clinical evidence actually says about tirzepatide and anxiety
Let us start with what matters most. The data.
Tirzepatide has been studied extensively across multiple large-scale clinical trial programs. The SURPASS trials evaluated its efficacy for type 2 diabetes. The SURMOUNT trials examined its role in weight management. Together, these programs enrolled thousands of participants and generated mountains of safety data. And anxiety, as a recognized adverse effect, does not appear in the FDA-approved prescribing information for either Mounjaro or Zepbound.
That is significant.
The SURMOUNT trial findings in detail
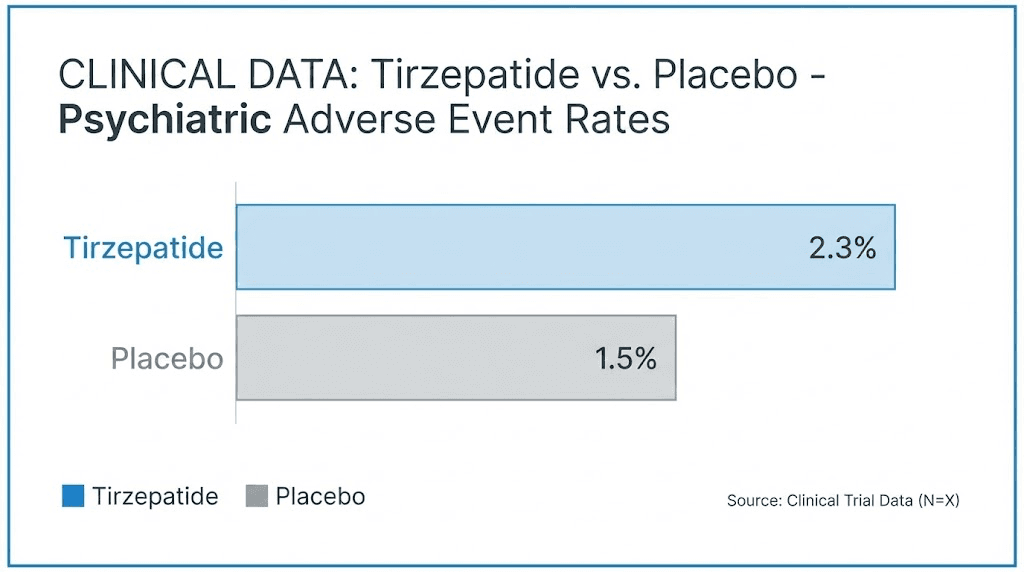
A post hoc analysis of the SURMOUNT program examined psychiatric safety specifically. The researchers analyzed data from 4,056 adults with obesity or overweight but without known major psychopathology. The findings were reassuring. Tirzepatide was not associated with increased depression compared to placebo. More importantly for our discussion, participants taking tirzepatide showed numerically lower occurrence of anxiety symptoms than those on placebo. The rates of treatment-emergent adverse events related to stress, anxiety symptoms, insomnia, and substance-use disorders were low and comparable across all groups. Depression scores, measured using validated instruments, actually improved more in the tirzepatide group than in the placebo group by week 72.
But here is the critical caveat that many articles overlook. Trial participants were screened to exclude anyone with a lifetime history of suicide attempts or serious psychiatric illness. This means the results cannot be extrapolated to everyone. If you have a history of anxiety disorders, depression, or other mental health conditions, the SURMOUNT data does not directly apply to your situation.
EudraVigilance pharmacovigilance data
When we look beyond controlled trials to real-world reporting, the picture gains complexity. An analysis of the EudraVigilance database examined 31,444 total adverse event reports for semaglutide, liraglutide, and tirzepatide combined. Of these, 372 reports involved psychiatric adverse events, representing just 1.18% of all reports.
Within those psychiatric reports, the breakdown is telling. Depression was the most commonly reported event, with 187 cases accounting for 50.3% of psychiatric reports. Anxiety followed with 144 cases, representing 38.7%. Suicidal ideation was reported in 73 cases, or 19.6%. Women accounted for 65% of all psychiatric adverse event reports.
Now, 144 anxiety reports across hundreds of thousands of users might sound alarming in isolation. In context, it represents a fraction of a percentage. But each of those 144 reports represents a real person experiencing real distress, and dismissing their experiences would be irresponsible. The question is not whether anxiety occurs in some tirzepatide users. It clearly does. The question is whether tirzepatide causes it, or whether other factors explain the connection.
The FDA position
In January of a recent evaluation cycle, the FDA conducted a preliminary assessment of GLP-1 receptor agonists and psychiatric side effects. Their conclusion was measured. The evaluation did not find evidence that these medications cause suicidal thoughts or actions. However, the FDA also acknowledged that monitoring continues, and the investigation was not considered final. The safety profile of these medications remains under active surveillance.
Real-world observational studies
Some of the most encouraging data comes from large observational studies. Research examining patients with type 2 diabetes found that those taking tirzepatide were 65% less likely to be diagnosed with depression and 60% less likely to be diagnosed with anxiety compared to patients not taking the medication. For semaglutide, the numbers were also positive but slightly lower, with 45% reduced depression risk and 44% reduced anxiety risk.
These are not small differences. A 60% reduction in anxiety diagnoses suggests that tirzepatide may actually be protective against anxiety in certain populations, not causative. But observational studies carry inherent limitations. Patients who tolerate a medication well enough to continue taking it are a self-selected group. Those who developed anxiety may have stopped treatment and therefore disappeared from the data.
How tirzepatide interacts with the brain and nervous system
Understanding why some people experience anxiety on tirzepatide requires understanding how this medication reaches beyond the gut and pancreas into the brain itself. Tirzepatide is a dual GIP/GLP-1 receptor agonist. That dual mechanism is what makes it so effective for weight loss and blood sugar control. But it also means the medication interacts with neural pathways in ways that single-mechanism drugs do not.
GLP-1 receptors in the brain
GLP-1 receptors are not confined to the pancreas. They exist throughout the central nervous system, concentrated in areas that directly regulate mood, emotion, and stress responses. The prefrontal cortex, which governs decision-making and emotional regulation. The amygdala, the brain fear and anxiety center. The hypothalamus, which orchestrates the stress response. All of these regions express GLP-1 receptors.
When tirzepatide activates these receptors, it modulates the release of several key neurotransmitters. Serotonin, dopamine, GABA, and glutamate all respond to GLP-1 receptor activation. These are the same neurotransmitters targeted by most psychiatric medications for depression and anxiety. The overlap is not coincidental.
The serotonin connection
Serotonin plays a central role in mood regulation, and GLP-1 receptor activation directly influences serotonergic signaling. Research has shown that acute central GLP-1 receptor stimulation alters serotonin signaling in the amygdala, the brain structure most associated with anxiety and fear processing. This alteration can go both ways. For most people, the net effect appears to be positive, contributing to mood improvement. For a minority, particularly those with pre-existing imbalances in serotonergic function, the shift could theoretically contribute to anxiety symptoms.
Think of it this way. If your serotonin system is functioning normally, GLP-1 receptor activation tends to support stable or improved mood. If your serotonin system is already dysregulated, the additional modulation could create temporary instability.
Dopamine and the reward system
Tirzepatide also affects dopaminergic pathways. Stimulation of GLP-1 receptors enhances the activity of dopaminergic neurons in the ventral tegmental area while simultaneously increasing expression of the dopamine transporter in the limbic system and striatum. This combination changes how the brain processes reward and motivation.
For many people, this translates into reduced food cravings and less emotional eating, both positive outcomes. But dopamine does not just regulate food reward. It influences motivation, pleasure, social engagement, and anxiety. Altered dopaminergic transmission could contribute to feelings of anhedonia, reduced motivation, or in some cases, increased anxiety, particularly in individuals whose reward systems were heavily dependent on food-related dopamine release. Understanding how peptides work at the neurological level helps explain why responses vary so dramatically between individuals.
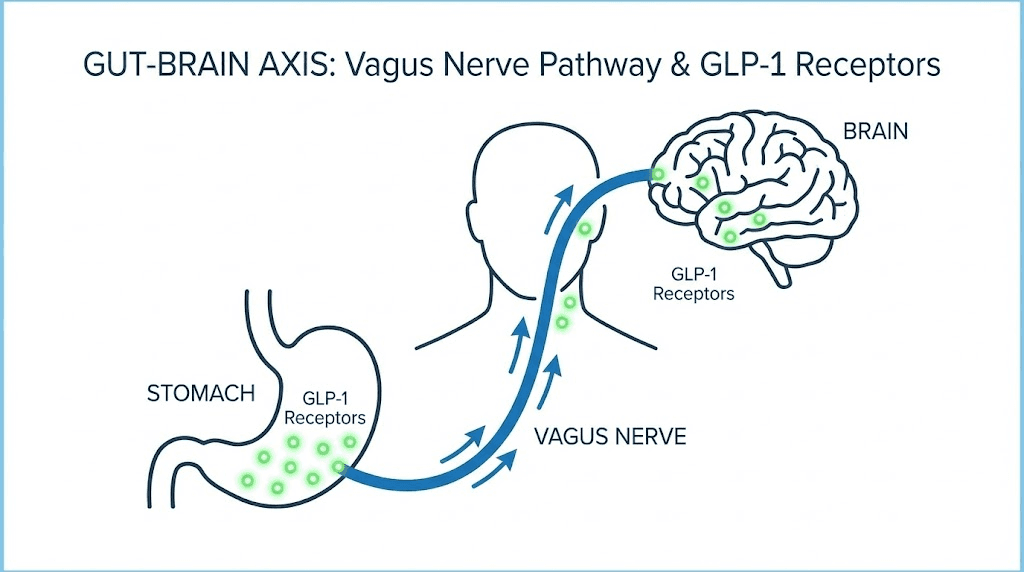
The gut-brain axis and vagus nerve
Much of tirzepatide effect on the brain may not come directly from crossing the blood-brain barrier. Instead, it travels through the gut-brain axis via the vagus nerve. This massive nerve connects the gastrointestinal system to the brainstem, carrying signals in both directions. When tirzepatide alters gut function, slowing gastric emptying, changing nutrient absorption patterns, and modifying the gut microbiome, those changes generate signals that travel up the vagus nerve to the brain.
The vagus nerve is not just a passive cable. It actively modulates the stress response. Vagal tone, the baseline activity level of this nerve, is directly linked to anxiety regulation. Higher vagal tone generally correlates with better stress resilience. Lower vagal tone correlates with anxiety vulnerability. Tirzepatide effects on gut function could, through vagal signaling, influence the brain anxiety thermostat in ways that vary dramatically between individuals.
Anti-inflammatory and neuroprotective effects
Not all of tirzepatide brain effects are potentially anxiety-provoking. GLP-1 receptor activation also demonstrates significant anti-inflammatory and neuroprotective properties. Neuroinflammation is increasingly recognized as a contributor to anxiety and depression. By reducing brain inflammation, tirzepatide may actually be protective against mood disorders in many users. This likely explains why the observational data shows reduced anxiety diagnoses among tirzepatide users overall.
The challenge is that individual responses vary. The same anti-inflammatory cascade that calms one brain may interact differently with another brain already navigating a complex neurochemical landscape.
Rodent research and what it suggests
Animal studies add another layer to this picture. In rodent models, acute activation of GLP-1-producing neurons has been shown to trigger stress-like and anxiety-like behavior. This is an important finding because it suggests that the GLP-1 system does play a direct role in anxiety regulation, not just an indirect one. However, chronic GLP-1 receptor activation, which better mimics what happens with a weekly medication like tirzepatide, did not consistently produce anxiety-like behavior and in some models actually reduced depression-like behavior.
The distinction between acute and chronic GLP-1 signaling matters enormously. A single dose might transiently affect anxiety circuits. But sustained activation, the kind tirzepatide provides week after week, appears to allow the brain to adapt and may ultimately shift mood regulation in a positive direction. This could explain why some people experience anxiety early in treatment that resolves as they continue.
The hypoglycemia-anxiety connection most people miss
Here is where things get practical. And where many people mistake a treatable metabolic event for a psychiatric symptom.
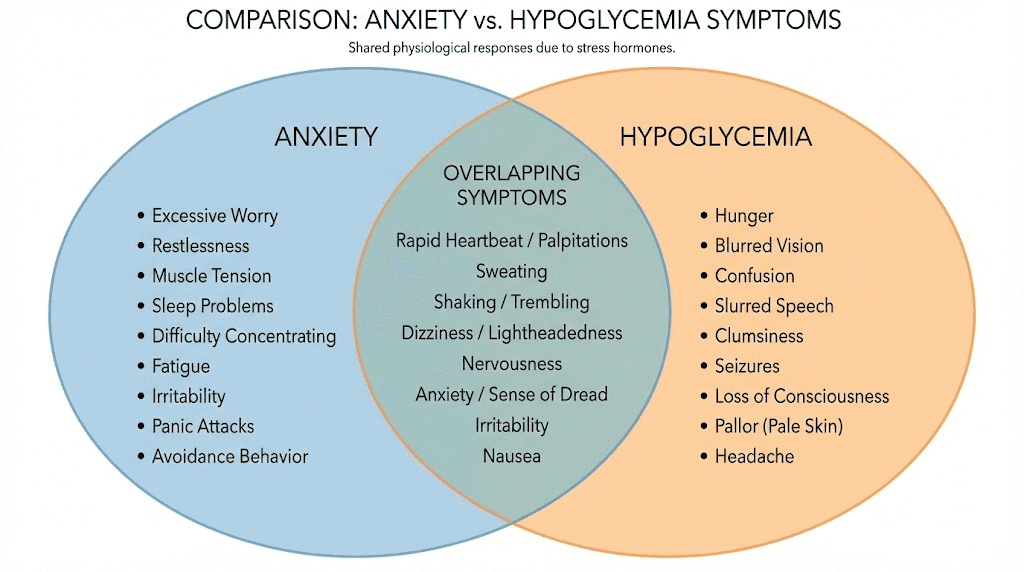
Hypoglycemia, or low blood sugar, produces symptoms that are virtually identical to an anxiety attack. Trembling. Sweating. Rapid heartbeat. Nervousness. Difficulty concentrating. A sense of impending doom. If you did not know your blood sugar was low, you would swear you were having a panic attack.
Does tirzepatide cause hypoglycemia?
Tirzepatide alone does not typically cause hypoglycemia. The medication works by enhancing insulin secretion in a glucose-dependent manner, meaning it stimulates insulin release only when blood sugar is elevated. When blood sugar is normal or low, the insulin-stimulating effect diminishes. This is a built-in safety mechanism that distinguishes GLP-1 receptor agonists from older diabetes medications. The standard dosing protocol accounts for this glucose-dependent mechanism.
But the risk equation changes dramatically when tirzepatide is combined with other medications. If you take tirzepatide alongside insulin or sulfonylureas, the risk of hypoglycemia increases substantially. These combinations can push blood sugar low enough to trigger symptoms that feel exactly like anxiety. Without checking blood glucose at the time of symptoms, distinguishing between anxiety and hypoglycemia becomes nearly impossible.
Symptoms that overlap between anxiety and hypoglycemia
The symptom overlap is striking. Both anxiety and hypoglycemia can cause trembling or shaking in the hands and body. Both produce sweating, sometimes cold sweats that seem to come from nowhere. Both accelerate heart rate and create a pounding sensation in the chest. Both generate feelings of nervousness and unease. Both can cause difficulty thinking clearly and concentrating. Both can produce nausea. Both can create a feeling that something terrible is about to happen.
The similarities are not coincidental. Both conditions activate the sympathetic nervous system, the fight-or-flight response. Hypoglycemia triggers it through a metabolic alarm. Anxiety triggers it through a psychological alarm. But the downstream cascade, the adrenaline release, the cortisol spike, the physical manifestations, are essentially identical.
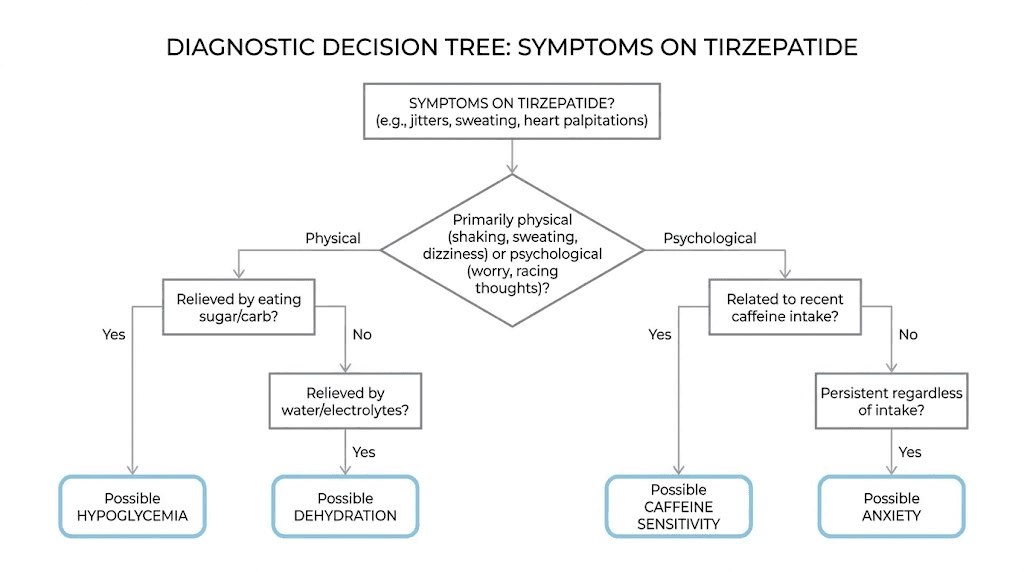
How to tell the difference
Timing offers the best clue. Hypoglycemia-related symptoms tend to emerge 2-4 hours after eating, particularly after high-carbohydrate meals that trigger an exaggerated insulin response. They often improve rapidly after eating. Anxiety symptoms, by contrast, tend to follow psychological triggers, build gradually, and do not resolve immediately after consuming food.
A glucose meter provides the definitive answer. If your blood sugar is below 70 mg/dL when symptoms appear, you are dealing with hypoglycemia, not anxiety. If your blood sugar is normal, the symptoms are more likely anxiety-related. For anyone using tirzepatide who experiences episodes that feel like anxiety, carrying a basic monitoring setup can save enormous amounts of unnecessary worry.
The 15-15 rule for management
If you confirm or suspect hypoglycemia, the 15-15 rule provides a straightforward management protocol. Consume 15 grams of fast-acting carbohydrates, such as 4 glucose tablets, half a cup of juice, or a tablespoon of honey. Wait 15 minutes. Recheck your blood glucose. If it remains below 70 mg/dL, repeat the process. Once blood sugar normalizes, eat a small snack or meal to prevent recurrence.
What you should not do is take an anti-anxiety medication for what is actually a blood sugar problem. Misidentifying hypoglycemia as anxiety leads to inappropriate treatment, continued symptoms, and unnecessary medication. Getting the diagnosis right is essential. If you are tracking your tirzepatide dosing schedule alongside blood glucose readings, patterns will emerge quickly.
Medication combinations that increase risk
Certain medication combinations deserve special attention. Tirzepatide combined with insulin is the highest-risk pairing for hypoglycemia. Tirzepatide combined with sulfonylureas also elevates risk significantly. Even tirzepatide combined with very low calorie diets can occasionally push blood sugar low enough to mimic anxiety. If you take any of these combinations and experience anxiety-like symptoms, hypoglycemia should be ruled out before pursuing psychiatric explanations. Understanding how to calculate proper dosages becomes especially important when multiple medications interact.
Psychological factors that mimic medication side effects
Medication rarely operates in a vacuum. When someone starts tirzepatide, they are not just introducing a chemical compound into their body. They are entering a period of significant physical, emotional, and social change. And those changes can produce anxiety all on their own, without any pharmacological contribution from the medication.
The loss of food as a coping mechanism
This is the factor that most medical discussions completely ignore. And it may be the most important one.
For many people, food serves as more than nutrition. It is comfort after a hard day. It is celebration with friends. It is the reliable pleasure that never disappoints. It is the thing that makes stress bearable. When tirzepatide dramatically reduces appetite and changes the relationship with food, that coping mechanism disappears. Sometimes overnight.
The resulting emotional gap is real. Without food as a buffer, stress that was previously managed through eating suddenly has no outlet. Anxiety that was being numbed by emotional eating surfaces in full force. This is not a side effect of tirzepatide in the pharmacological sense. It is the removal of a coping mechanism that was masking underlying anxiety all along.
Recognizing this distinction matters. If food was your primary stress management tool, the anxiety you feel on tirzepatide may have been there before, hidden behind meals and snacks and the temporary comfort of eating.
Rapid body changes and identity disruption
Significant weight loss changes more than the number on the scale. It changes how you look. How clothes fit. How people treat you. How you see yourself. For some people, these changes are entirely positive. For others, they trigger a complex psychological response that includes anxiety.
Rapid physical transformation can disrupt psychological equilibrium in ways that are poorly understood. Some people report feeling like they do not recognize themselves. Others experience discomfort with increased attention or compliments from others. Some feel guilt about losing weight through medication rather than willpower alone. These feelings are valid. They are also sources of anxiety that have nothing to do with tirzepatide pharmacology. The before and after transformation that looks beautiful in pictures can feel disorienting in real life.
Changed social dynamics around food
Food is social currency. It is how families connect, how cultures express love, how friendships deepen. When tirzepatide changes your appetite and eating patterns, it can create friction in these social connections. Declining food at family gatherings. Eating less at restaurants. Turning down baked goods from well-meaning colleagues. Each of these situations creates social anxiety that is entirely independent of any medication effect.
The anxiety compounds when people start asking questions. Why are you not eating? Are you on one of those weight loss drugs? You are getting too thin. These comments, however well-intentioned, can trigger anxiety in individuals who are already navigating a significant life change. Resources like the peptides for weight loss women guide address some of these social dynamics specific to female users.
Fear of medication side effects
Here is an ironic twist. Reading about whether tirzepatide causes anxiety can itself cause anxiety. The nocebo effect, the negative counterpart to the placebo effect, is well documented. When people expect side effects, they are more likely to experience them. If you have spent hours reading forums, articles, and Reddit threads about tirzepatide and anxiety, you have primed your brain to be hypervigilant for anxiety symptoms. That hypervigilance is itself a form of anxiety.
This does not mean your symptoms are imaginary. It means the human brain is remarkably susceptible to suggestion, particularly regarding symptoms as subjective as anxiety. Staying informed about common mistakes and realistic expectations can help counteract the nocebo effect without leaving you uninformed.
Pre-existing anxiety unmasked
Some people who report anxiety on tirzepatide had anxiety before starting the medication but did not recognize it. Undiagnosed anxiety is remarkably common. When tirzepatide changes daily routines, eating patterns, and coping strategies, previously managed anxiety can surface in ways that feel new and medication-related.
A useful question to ask yourself: did you ever feel anxious before starting tirzepatide? If the answer is yes, the medication may not be creating new anxiety. It may be removing the barriers that were keeping existing anxiety below your awareness threshold.
When anxiety on tirzepatide is actually something else
Not every uncomfortable sensation is anxiety. And on tirzepatide, several other physiological processes can produce symptoms that feel like anxiety but have entirely different causes and solutions.
Dehydration masquerading as anxiety
Tirzepatide can cause nausea, vomiting, and diarrhea, all of which deplete fluids. Dehydration produces symptoms that overlap significantly with anxiety. Rapid heart rate. Lightheadedness. Difficulty concentrating. A vague sense that something is wrong. Before assuming anxiety, assess your hydration status. Are you drinking enough water? Have you had gastrointestinal side effects that might have caused fluid loss? Sometimes the fix is as simple as drinking more water.
Caffeine sensitivity changes
Weight loss changes how your body processes caffeine. As body mass decreases, the same amount of caffeine produces a relatively stronger effect. Two cups of coffee that were fine at 250 pounds might overstimulate at 200 pounds. The resulting jitteriness, increased heart rate, and nervousness feel exactly like anxiety. If you have lost weight on tirzepatide and are experiencing anxiety symptoms, evaluate your caffeine intake before attributing symptoms to the medication. This is a quick and easy variable to test.
Nutrient deficiencies from reduced food intake
Eating significantly less food means consuming fewer micronutrients. Deficiencies in magnesium, B vitamins, iron, and vitamin D all have well-documented connections to anxiety symptoms. Magnesium deficiency alone can produce nervousness, muscle tension, insomnia, and irritability, a constellation that looks identical to generalized anxiety. If your food intake has dropped substantially since starting tirzepatide, nutritional status deserves investigation. A comprehensive blood panel can identify deficiencies that might explain mood symptoms better than the medication itself. Understanding proper dosing and nutritional support protocols helps prevent these deficiencies.
Sleep disruption
Some tirzepatide users report changes in sleep quality, particularly during dose adjustments. Poor sleep is one of the most potent anxiety triggers in existence. Even one or two nights of disrupted sleep can significantly increase anxiety sensitivity, emotional reactivity, and the tendency to interpret neutral situations as threatening. If your anxiety correlates with poor sleep quality rather than with medication timing, addressing sleep hygiene may resolve the anxiety without any changes to your tirzepatide protocol.
The fatigue factor
Tirzepatide causes fatigue in 3-7% of users. When you are tired, everything feels harder. Cognitive resources for managing stress are depleted. Emotional regulation suffers. Minor stressors that you would normally handle without difficulty suddenly feel overwhelming. This increased vulnerability to stress can be misinterpreted as anxiety, when the underlying issue is actually tirzepatide-related fatigue.
Heart rate elevation
Tirzepatide causes a modest average increase in heart rate of 2-4 beats per minute. In most people, this is imperceptible. But in individuals who are body-aware or prone to health anxiety, even a small increase in resting heart rate can trigger anxiety about cardiac health, which produces more anxiety, which further elevates heart rate, creating a self-reinforcing cycle. If you are monitoring your heart rate and noticing a slight increase, know that this is a documented, normal, and generally benign effect of the medication.
Complete management protocol for anxiety while on tirzepatide
Whether your anxiety is related to tirzepatide, unmasked by it, or completely independent of it, you need strategies that work. This section provides a comprehensive management protocol that addresses both the physiological and psychological dimensions of anxiety during treatment.
Physiological stabilization first
Before addressing the psychological components of anxiety, stabilize the physiological variables that can drive anxiety symptoms. Monitor blood glucose during episodes to rule out hypoglycemia. Track hydration by aiming for at least 64 ounces of water daily, more if you are experiencing gastrointestinal side effects. Evaluate caffeine intake and consider reducing it by 25-50% to account for body composition changes. Get a comprehensive blood panel to check magnesium, B12, iron, folate, and vitamin D levels. These steps eliminate the most common non-psychiatric causes of anxiety in tirzepatide users.
Taking these steps before pursuing psychiatric treatment can save months of unnecessary medication trials or therapy focused on the wrong problem. SeekPeptides members access comprehensive protocols that integrate metabolic monitoring with peptide use, helping identify the actual source of symptoms rather than guessing.
Nutritional support strategies
When food intake decreases, nutritional density must increase. Every meal needs to deliver maximum micronutrient value. Prioritize protein at 1.0-1.2 grams per kilogram of body weight daily to support neurotransmitter production. Include omega-3 fatty acids through fish, walnuts, or supplementation, as these directly support brain health and have demonstrated anti-anxiety properties. Ensure adequate magnesium intake through dark leafy greens, nuts, seeds, or supplementation with 200-400mg of magnesium glycinate daily, a form particularly beneficial for anxiety.
B vitamins deserve special attention. B6 is required for serotonin and GABA synthesis. B12 supports nervous system function. Folate works alongside B12 in methylation pathways that influence mood. A high-quality B-complex supplement can address these needs efficiently when food intake is limited. Using the tirzepatide with B12 combination guide provides specific protocols for supplementation alongside this medication.
Movement as medicine
Exercise is the most evidence-based natural anxiety treatment available. It works through multiple mechanisms simultaneously. Acute exercise burns off excess adrenaline and cortisol. Regular exercise increases GABA production, the brain primary calming neurotransmitter. It promotes neuroplasticity, helping the brain adapt to new neurochemical environments. And it provides a sense of accomplishment and control, both of which counter anxiety.
For tirzepatide users experiencing anxiety, aim for 150 minutes of moderate activity per week, broken into manageable sessions. Walking counts. So does swimming, cycling, yoga, and resistance training. The specific activity matters less than consistency. Even 10 minutes of movement during an acute anxiety episode can reduce symptoms significantly. People using peptides for athletic performance often report improved mood as a secondary benefit of their exercise routines.
Breathing techniques for acute episodes
When anxiety strikes acutely, breathing techniques provide the fastest relief available without medication. The physiological sigh, a technique validated by Stanford neuroscience research, involves two quick inhales through the nose followed by a long exhale through the mouth. This pattern activates the parasympathetic nervous system within seconds, countering the fight-or-flight response that drives anxiety symptoms.
Box breathing offers another effective option. Inhale for four seconds. Hold for four seconds. Exhale for four seconds. Hold for four seconds. Repeat for four to six cycles. This structured breathing pattern creates a predictable rhythm that the nervous system interprets as safety, gradually reducing anxiety.
The 4-7-8 technique works especially well at night. Inhale for four seconds. Hold for seven seconds. Exhale for eight seconds. The extended exhale activates the vagus nerve, the same nerve through which tirzepatide communicates with the brain, promoting calm.
Cognitive strategies for reframing
Anxiety feeds on catastrophic thinking. What if this anxiety never goes away? What if the medication is damaging my brain? What if I am developing a serious psychiatric condition? These thoughts are not facts. They are anxiety talking.
Cognitive reframing involves catching these thoughts and examining them objectively. Is there evidence that tirzepatide causes permanent brain changes? No. Is there evidence that medication-related anxiety resolves when the medication is adjusted or discontinued? Yes. Are anxiety symptoms common during major life changes, regardless of medication? Absolutely.
The goal is not to suppress anxious thoughts but to respond to them rationally rather than reactively. Resources on managing anxiety with peptides provide additional cognitive frameworks for navigating this experience.
Sleep optimization protocol
Sleep and anxiety exist in a bidirectional relationship. Poor sleep increases anxiety. Anxiety disrupts sleep. Breaking this cycle requires intentional sleep optimization. Maintain consistent sleep and wake times, even on weekends. Eliminate screens for 60 minutes before bed. Keep the bedroom cool, dark, and quiet. Avoid caffeine after noon. Limit alcohol, which disrupts sleep architecture even in small amounts.
If tirzepatide is affecting your sleep, consider timing your injection to minimize nighttime disruption. Some users find that morning injections produce fewer sleep disturbances than evening injections. Others find the opposite. Individual experimentation, tracked systematically, will reveal your optimal timing. Certain peptides for sleep have been studied for their potential to improve sleep quality alongside other treatments.
Building new coping mechanisms
If food was your primary coping mechanism, you need replacements. Not willpower. Actual replacements. Concrete activities that provide the same emotional relief that eating used to provide.
Physical activity works for some. Creative pursuits work for others. Social connection, journaling, time in nature, meditation, hot baths, music, the specific replacement matters less than having one. The key is identifying what emotional need food was meeting and finding another way to meet it. Was it comfort? Try warmth, softness, physical closeness. Was it stimulation? Try novelty, adventure, challenge. Was it numbing? This one may require professional support, because the urge to numb suggests pain that deserves attention.
Dose titration strategies to minimize mood disruption
If your anxiety correlates with dose changes, the titration schedule itself may be the lever to pull. Not every person needs to follow the standard escalation timeline, and working with your prescriber to customize the approach can make a significant difference.
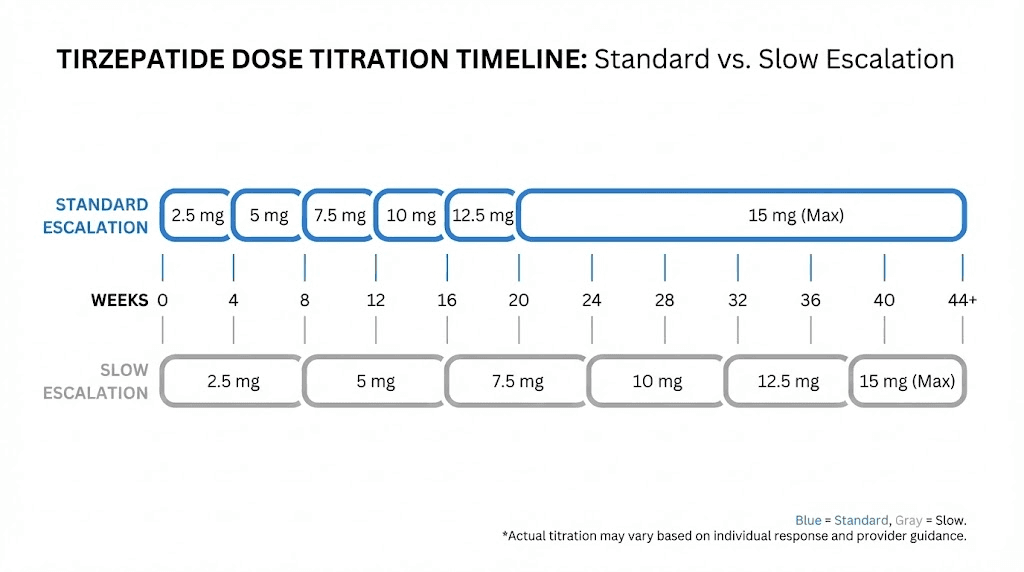
The standard tirzepatide titration schedule
The FDA-approved protocol begins at 2.5mg weekly for four weeks, then increases to 5mg weekly. From there, the dose can be increased by 2.5mg every four weeks, up to a maximum of 15mg weekly. This gradual escalation exists specifically to improve tolerability and allow the body time to adapt. Understanding the complete tirzepatide dosage chart helps contextualize where you are in this process.
For weight management (Zepbound), the same titration applies. For diabetes management (Mounjaro), the maximum dose is also 15mg. The difference lies in the prescribing indication, not the titration approach.
Slower titration for anxiety-prone individuals
If you have a history of anxiety or are experiencing anxiety symptoms during titration, discuss a slower schedule with your prescriber. Instead of increasing every four weeks, some providers extend the titration intervals to six or even eight weeks. This gives the brain more time to adapt to each new dose level before introducing another change.
The trade-off is slower weight loss or slower blood sugar improvement. But if the alternative is intolerable anxiety that leads to discontinuation, a slower approach that keeps you on the medication is far more effective than a fast approach that forces you to stop. Patience here is strategic, not passive.
The microdosing approach
Some practitioners use microdosing tirzepatide strategies, where the dose increases occur in smaller increments. Instead of jumping from 5mg directly to 7.5mg, a provider might prescribe intermediate steps with compounded formulations. This approach is particularly relevant for individuals who are sensitive to medication changes and want to minimize the neurochemical disruption that accompanies each dose increase.
The evidence for microdosing tirzepatide specifically is largely anecdotal and based on clinical experience rather than randomized trials. But the underlying principle, that smaller changes are better tolerated, is well-established in pharmacology. If your response to tirzepatide has been particularly sensitive, this approach deserves discussion with your healthcare provider.
When to step back down
If anxiety symptoms are clearly dose-related, meaning they appear or worsen shortly after a dose increase and do not resolve within two to three weeks, stepping back to the previous dose is a reasonable strategy. This is not failure. It is responsible medication management.
Many people find their optimal dose is not the maximum dose. A dose that provides meaningful weight loss or blood sugar control without intolerable side effects is the right dose, regardless of whether it matches the maximum on the chart. Reviewing the dosing for weight loss in units guide can help you understand what therapeutic range you need to maintain effectiveness without pushing past your tolerance.
Injection timing and anxiety patterns
Some users notice anxiety patterns related to when they inject relative to their weekly cycle. Anxiety may peak 24-48 hours after injection when drug levels are highest, or it may appear at the end of the week when levels are declining. Tracking this pattern provides valuable information for your prescriber.
If anxiety peaks when drug levels are highest, the dose may be too high. If anxiety appears as drug levels decline, it could represent a withdrawal-like phenomenon between doses, though this is poorly studied for tirzepatide. Either pattern points toward dose adjustment as a potential solution. Proper reconstitution and administration technique ensures consistent dosing that minimizes these fluctuations.
When to talk to your doctor versus managing at home
Not every episode of anxiety requires medical attention. But some do. Knowing the difference can prevent both unnecessary emergency visits and dangerous delays in seeking help.
Situations that warrant immediate medical attention
Seek immediate medical evaluation if you experience suicidal thoughts or thoughts of self-harm. This is non-negotiable, regardless of whether you believe the medication is causing these thoughts. The FDA continues to monitor GLP-1 receptor agonists for psychiatric effects, and any emergence of suicidal ideation during treatment should be taken seriously.
Severe panic attacks that include chest pain, difficulty breathing, or a feeling that you are dying also warrant urgent evaluation. While panic attacks are not dangerous in themselves, the symptoms overlap with cardiac events that are dangerous. Let a medical professional make the distinction.
Hallucinations, paranoia, or perceptual disturbances are rare but documented. One published case report described a patient who developed paranoia and visual hallucinations while using compounded tirzepatide. The symptoms resolved completely upon discontinuation. Any perceptual disturbance during tirzepatide use requires immediate medical attention and likely medication discontinuation.
Situations that warrant a scheduled appointment
Schedule an appointment with your prescriber if anxiety symptoms persist for more than two weeks at the same dose level. Persistent anxiety suggests either a dose-related issue that needs adjustment, an underlying condition that needs treatment, or a psychological factor that needs professional support. Your prescriber can evaluate the situation and recommend appropriate next steps.
Also schedule an appointment if anxiety is significantly affecting your daily functioning. Missing work, avoiding social situations, difficulty completing normal tasks, inability to sleep, these are signs that the anxiety has crossed from uncomfortable to impairing. Impairment is the clinical threshold for when anxiety warrants treatment intervention.
If you are considering stopping tirzepatide because of anxiety, talk to your prescriber first rather than discontinuing independently. Abrupt discontinuation can create its own set of problems, and your prescriber may have solutions you have not considered. Understanding the switching between GLP-1 medications process can provide additional options beyond simply stopping treatment.
What you can manage at home
Mild, intermittent anxiety that does not impair your daily functioning can often be managed with the strategies outlined in this guide. This includes anxiety that comes and goes, that responds to breathing techniques or physical activity, that correlates with identifiable triggers like dose changes or stressful events, and that does not include thoughts of self-harm.
Home management is appropriate when you can identify the likely cause, such as caffeine sensitivity, dehydration, or sleep disruption. It is appropriate when symptoms are mild and tolerable. It is appropriate when you have effective coping strategies that bring relief within a reasonable timeframe.
Keep a symptom journal. Track when anxiety occurs, how severe it is on a 1-10 scale, what you were doing when it started, what you ate and drank, how you slept the night before, and where you are in your weekly injection cycle. This data becomes invaluable if you do need to discuss symptoms with your prescriber. It transforms a vague complaint of "I feel anxious" into actionable clinical information.
The role of therapy
Cognitive behavioral therapy, or CBT, is the gold standard for anxiety treatment and works particularly well alongside medication management. A therapist trained in CBT can help you distinguish between medication-related symptoms and psychological responses to the changes in your life. They can provide personalized coping strategies. They can address underlying anxiety that may have been masked by food-related coping. And they can support you through the identity shifts that accompany significant weight loss.
If you are experiencing anxiety on tirzepatide and have never worked with a therapist, this is an excellent time to start. Not because tirzepatide is causing psychiatric problems, but because the changes it facilitates create an optimal window for psychological growth and the development of healthier coping mechanisms.
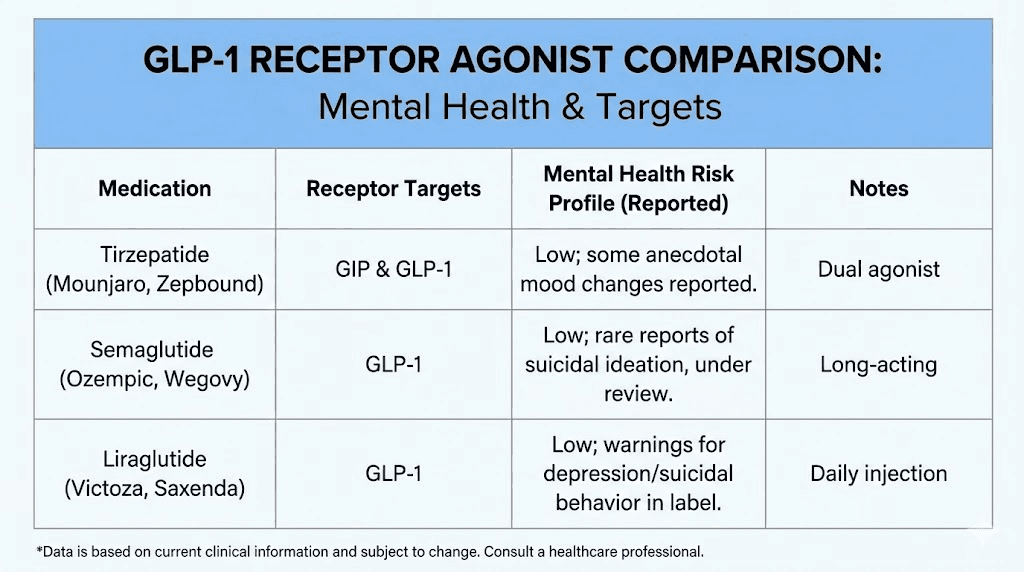
Tirzepatide compared to other GLP-1 medications for mental health
If anxiety is a significant concern, understanding how tirzepatide compares to other medications in its class can help inform treatment decisions. The GLP-1 receptor agonist class includes several medications with varying profiles, and the mental health data differs across them.
Tirzepatide versus semaglutide
The most common comparison is between tirzepatide and semaglutide, the active ingredient in Ozempic and Wegovy. Both medications act on GLP-1 receptors, but tirzepatide also activates GIP receptors, giving it a dual mechanism that semaglutide lacks.
From a mental health perspective, the data actually favors tirzepatide. In the observational study mentioned earlier, tirzepatide users with diabetes showed a 60% reduced risk of anxiety diagnoses compared to 44% for semaglutide users. For depression, tirzepatide showed a 65% reduced risk versus 45% for semaglutide. These are meaningful differences, though the observational design prevents definitive causal conclusions.
Some researchers speculate that the additional GIP receptor activation may provide extra neuroprotective benefits. GIP receptors are also expressed in the brain, and their activation may contribute to mood stabilization in ways that pure GLP-1 agonists do not achieve. The complete semaglutide versus tirzepatide comparison covers efficacy differences across all outcomes, not just mental health.
However, semaglutide has more published research overall, including a larger pharmacovigilance footprint. Some patients who experience anxiety on tirzepatide report improvement after switching to semaglutide, and the reverse is also true. Individual neurochemistry determines which medication is better tolerated, and no amount of population-level data can predict your specific response.
Tirzepatide versus liraglutide
Liraglutide, marketed as Saxenda for weight loss and Victoza for diabetes, was the first GLP-1 receptor agonist widely used for obesity. Its psychiatric profile has been studied for longer, and the data shows a similar pattern to the newer medications. Most users experience no psychiatric side effects. A small minority report mood changes. And population-level data suggests an overall protective effect against depression and anxiety.
The key difference is that liraglutide requires daily injections rather than weekly injections. This means drug levels fluctuate more frequently, which could theoretically influence mood stability. Some patients who experienced mood fluctuations on daily liraglutide report more stable mood on weekly tirzepatide, likely due to the steadier drug levels. Using a dosage calculator can help compare equivalent therapeutic doses across different GLP-1 medications.
Newer options on the horizon
The GLP-1 receptor agonist landscape is expanding rapidly. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, is in clinical trials and will add another option for patients who do not tolerate existing medications. CagriSema, combining cagrilintide with semaglutide, represents another approach. As more options become available, patients who experience anxiety on one medication will have more alternatives to try.
The mental health profiles of these newer medications are not yet well characterized. But the increasing diversity of options is good news for anyone who needs the metabolic benefits of GLP-1 receptor agonists but struggles with psychiatric tolerability on current options. Resources like the best peptides for weight loss comparison help navigate these expanding choices.
The role of compounded versus pharmaceutical formulations
An important distinction exists between FDA-approved tirzepatide products (Mounjaro, Zepbound) and compounded versions. The case report of psychiatric adverse effects, including paranoia and visual hallucinations, involved compounded tirzepatide specifically. While this single case cannot establish a pattern, it raises questions about whether compounded formulations might carry different risk profiles due to variations in purity, concentration, or additional ingredients.
If you are using a compounded tirzepatide product and experiencing anxiety, discussing a switch to the brand-name pharmaceutical version with your prescriber is worth considering. The additional ingredients in some compounded formulations could theoretically contribute to side effects not seen with the pure pharmaceutical product. Understanding the difference between research and pharmaceutical peptides provides essential context for this decision.
Long-term outlook for anxiety and tirzepatide
The long-term psychiatric effects of tirzepatide remain an active area of research. But the existing data, combined with what we know about GLP-1 receptor pharmacology, allows for some reasonable projections about what to expect over extended treatment periods.
Early treatment anxiety often resolves
Many of the anxiety reports associated with tirzepatide occur during the first weeks to months of treatment, particularly during dose titration. This pattern is consistent with a neurochemical adjustment period. The brain is adapting to new signaling patterns, and during that adaptation, mood instability can occur. For most people, this early anxiety diminishes as the brain reaches a new equilibrium.
The timeline varies. Some people feel settled within a few weeks. Others take two to three months. A small number find that anxiety persists beyond the adjustment period, suggesting either a dose issue, a psychological factor, or genuine medication intolerance. If you are in the early weeks and experiencing anxiety, patience combined with the management strategies outlined above is often the best approach. Knowing how long tirzepatide takes to work helps set realistic expectations for both the benefits and the side effect adjustment period.
Dose stabilization and mood improvement
Once you reach your maintenance dose and your body fully adapts, the long-term data is encouraging. The SURMOUNT trials showed continued improvement in depression scores through week 72. Observational studies show sustained reductions in anxiety and depression diagnoses among long-term users. And the anti-inflammatory, neuroprotective properties of GLP-1 receptor activation may provide cumulative benefits over time.
Some researchers have proposed that tirzepatide extended neuroprotective effects could have implications beyond anxiety, potentially benefiting neurodegenerative conditions as well. While this research is in early stages, it suggests that long-term GLP-1 receptor activation may support brain health rather than compromise it. The broader field of peptides for brain function is exploring similar neuroprotective mechanisms across multiple peptide families.
Weight loss and mental health trajectory
The relationship between weight loss and mental health is not linear. Early in treatment, rapid weight loss can be psychologically destabilizing, as discussed earlier. But over time, the benefits of improved health, increased mobility, reduced chronic disease burden, and enhanced self-image tend to accumulate. Most long-term studies show that sustained weight loss is associated with improved mental health outcomes, including reduced anxiety.
The key is getting through the transition period. The first three to six months involve the most dramatic changes, both physical and psychological. After that, a new normal emerges. People who maintain their weight loss typically report stable or improved mental health compared to their pre-treatment baseline. The weight loss results that people see over time are often accompanied by parallel improvements in psychological well-being.
What happens if you stop tirzepatide?
Discontinuation of tirzepatide is associated with weight regain in most studies. From an anxiety perspective, stopping the medication removes both any potential anxiety-causing effects and any potential anxiety-protective effects. One published case report actually described a patient whose psychiatric symptoms worsened after stopping tirzepatide, suggesting that the medication had been providing mood-stabilizing benefits that were only apparent upon discontinuation.
If anxiety is the reason you are considering stopping tirzepatide, work through the complete diagnostic and management process in this guide before making that decision. Dose adjustment, slower titration, management of confounding factors, and therapy can often resolve anxiety without sacrificing the metabolic benefits that brought you to the medication in the first place. Understanding appetite suppression timelines can also help you understand what you might lose by discontinuing and whether a dose reduction could maintain some benefit.
Ongoing monitoring recommendations
For anyone on long-term tirzepatide therapy, periodic mental health check-ins should be part of routine care. This does not require formal psychiatric evaluation for everyone. A simple screening questionnaire at each follow-up visit, such as the PHQ-9 for depression and the GAD-7 for anxiety, provides objective data that can detect changes before they become problematic.
If you are tracking your experience at home, continue the symptom journal described earlier. Over months, patterns emerge that short-term tracking cannot reveal. You may discover that anxiety correlates with specific life stressors rather than medication changes. Or you may identify a dose threshold above which anxiety appears consistently. Either way, the data empowers better decision-making. SeekPeptides provides tracking tools and community support that help members monitor their experience systematically over extended treatment periods.
Frequently asked questions
Does tirzepatide directly cause anxiety?
The clinical trial data does not support a direct causal link between tirzepatide and anxiety. In the SURMOUNT trials, anxiety rates were actually numerically lower in the tirzepatide group compared to placebo. However, individual responses vary, and some people do report anxiety symptoms during treatment. The mechanisms through which this might occur include neurotransmitter modulation, gut-brain axis signaling changes, and psychological responses to rapid weight loss.
How common is anxiety as a side effect of tirzepatide?
Anxiety is not listed as a common side effect in the FDA-approved prescribing information. In pharmacovigilance databases, anxiety comprised 38.7% of psychiatric adverse event reports, but psychiatric reports as a whole represented only 1.18% of total adverse event reports for GLP-1 receptor agonists. The most common side effects are gastrointestinal, including nausea (12-24%), diarrhea (13-17%), and vomiting (6-10%). For perspective, fatigue affects 3-7% of users and is more commonly reported than anxiety.
Will anxiety on tirzepatide go away on its own?
For many people, yes. Anxiety that appears during dose titration often resolves as the body adapts, typically within two to six weeks at a stable dose. If anxiety persists beyond this adjustment period, other factors may be contributing, including underlying mood conditions, nutritional deficiencies, sleep disruption, or psychological responses to weight loss. Persistent anxiety warrants discussion with your prescriber.
Should I stop taking tirzepatide if I feel anxious?
Do not stop tirzepatide without consulting your prescriber. Anxiety during treatment has many possible causes, and several can be addressed without discontinuing the medication. Dose adjustment, slower titration, management of confounding factors, and psychological support often resolve anxiety while maintaining the metabolic benefits of treatment. Your prescriber can help determine the best course of action based on your specific situation. Review the dosing guide to discuss adjustment options with your healthcare team.
Can tirzepatide help with pre-existing anxiety?
Emerging evidence suggests it might. Observational studies show that patients with diabetes taking tirzepatide were 60% less likely to be diagnosed with anxiety compared to non-users. The anti-inflammatory and neuroprotective effects of GLP-1 receptor activation could provide anxiety-reducing benefits in some individuals. However, clinical trials have not specifically studied tirzepatide as an anxiety treatment, and it should not be used for this purpose outside of its approved indications. The broader research on peptides for anxiety explores these emerging connections.
Is anxiety more common at higher tirzepatide doses?
Some users report that anxiety symptoms correlate with dose increases, appearing or worsening when moving to a higher dose and potentially resolving if the dose is reduced. Interestingly, clinical data from the SURMOUNT trials showed that mood improvement was dose-dependent, meaning higher doses were associated with better mood scores overall. Individual responses vary significantly. If you suspect a dose-related pattern, track your symptoms alongside your dose schedule and share this data with your prescriber.
How do I tell the difference between tirzepatide anxiety and hypoglycemia?
Check your blood glucose during symptoms. Hypoglycemia-related symptoms occur when blood sugar drops below 70 mg/dL and resolve quickly after consuming 15 grams of fast-acting carbohydrates. Anxiety symptoms persist regardless of blood sugar levels and do not respond to food intake. If you take tirzepatide alongside insulin or sulfonylureas, hypoglycemia risk increases, making blood glucose monitoring during anxiety-like episodes essential. Understanding how proper dosing in units works can help ensure accurate medication administration.
Does compounded tirzepatide carry a higher anxiety risk?
The published case report describing severe psychiatric symptoms, including paranoia and hallucinations, involved compounded tirzepatide. While a single case cannot establish a pattern, compounded formulations may contain different concentrations, additional ingredients, or quality variations that could theoretically affect tolerability. If you are using compounded tirzepatide and experiencing psychiatric symptoms, discuss switching to an FDA-approved product with your prescriber. The source and quality of tirzepatide matters more than many people realize.
Can other medications I take with tirzepatide increase anxiety risk?
Yes. Certain medication combinations can contribute to anxiety-like symptoms. Insulin and sulfonylureas combined with tirzepatide increase hypoglycemia risk, which mimics anxiety. Stimulant medications, high-dose caffeine, certain asthma medications, and thyroid hormone replacement can all increase anxiety symptoms independently. When combined with tirzepatide neurochemical effects, the cumulative impact may exceed what either would produce alone. A complete medication review with your prescriber can identify potential interactions. The peptide stacking guide discusses interaction principles that apply broadly.
Are women more likely to experience anxiety on tirzepatide?
EudraVigilance data shows that women accounted for 65% of psychiatric adverse event reports for GLP-1 receptor agonists. However, women also use these medications at higher rates than men, particularly for weight loss indications. Whether the higher reporting rate reflects a genuine biological susceptibility or simply higher usage remains unclear. Hormonal factors, including menstrual cycle phase, perimenopause, and menopause, can independently influence both anxiety and medication tolerability. Resources for safe peptide use for women address these gender-specific considerations in detail.
External resources
For researchers and individuals committed to understanding how tirzepatide fits into a broader health strategy, SeekPeptides offers the most comprehensive resource available. Members access evidence-based safety guides, detailed dosing protocols, interaction databases, and a community of thousands who have navigated these exact questions. Whether you are managing anxiety symptoms, optimizing your titration schedule, or simply seeking trustworthy information about peptides and mental health, SeekPeptides provides the support and science you need.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay well-tolerated, your mind stay clear, and your progress stay steady.