Feb 21, 2026

Experienced researchers know something that beginners often miss about compounded tirzepatide formulations. Not all B12 is the same. The form of vitamin B12 paired with your tirzepatide matters more than most people realize, and the difference between methylcobalamin and cyanocobalamin can influence everything from how your body processes energy to how effectively you protect against GLP-1 related fatigue and nerve damage during rapid weight loss.
That distinction is not academic. It is practical. Methylcobalamin is the bioactive form of B12, meaning your body can use it immediately without conversion. Cyanocobalamin, the cheaper and more common form, requires your liver to strip away a cyanide molecule and then attach a methyl group before it becomes useful. For someone already placing metabolic demands on their body through a tirzepatide protocol, that extra conversion step is not trivial.
This guide covers every angle of tirzepatide methylcobalamin compounds. You will learn exactly why compounding pharmacies choose methylcobalamin over other B12 forms, how the two molecules interact in your body, what dosage protocols look like in practice, how to manage side effects, and what the current evidence says about long-term benefits. Whether you are evaluating a new compound or comparing it against tirzepatide glycine B12 formulations, this is the reference you will keep coming back to.
SeekPeptides built this resource because the tirzepatide compounding landscape keeps shifting, and researchers deserve clear answers based on evidence rather than marketing claims. Every protocol, every mechanism, every comparison in this guide comes from published research and documented clinical observations.
What is tirzepatide methylcobalamin?
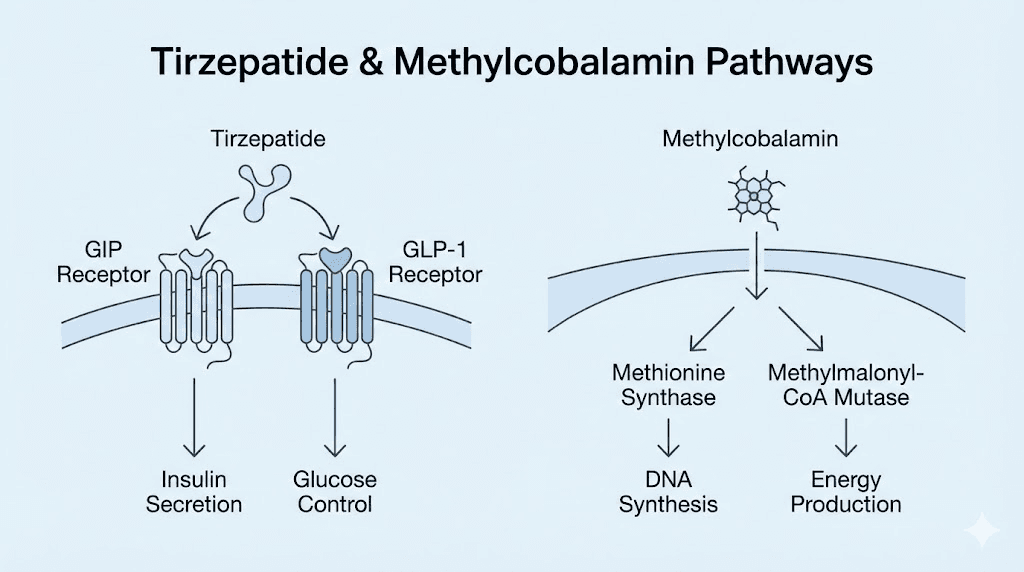
Tirzepatide methylcobalamin is a compounded pharmaceutical formulation that combines two distinct molecules in a single injectable solution. The first component, tirzepatide, is a dual GIP and GLP-1 receptor agonist that works by mimicking two incretin hormones simultaneously. The second component, methylcobalamin, is the most biologically active form of vitamin B12.
Together they serve different but complementary purposes.
Tirzepatide handles the heavy lifting for fat loss and metabolic improvement. It binds to both GIP receptors and GLP-1 receptors in the gut, pancreas, and brain, which triggers a cascade of effects including improved insulin sensitivity, reduced glucagon secretion, delayed gastric emptying, and centrally mediated appetite suppression. Clinical trials have demonstrated weight loss ranging from 15% to 22.5% of body weight depending on dose and duration, making it one of the most effective weight management tools ever studied.
Methylcobalamin plays a supporting but critical role. It is a coenzyme that participates directly in two essential biochemical reactions. The first is the conversion of homocysteine to methionine, which is vital for DNA methylation, protein synthesis, and cellular repair. The second is the conversion of methylmalonyl-CoA to succinyl-CoA in the mitochondria, which feeds directly into the citric acid cycle for energy production.
The reason these two molecules appear together in a single vial is not arbitrary. Compounding pharmacies identified early on that patients using GLP-1 receptor agonists frequently developed B12 deficiencies. The mechanism is straightforward. Tirzepatide slows gastric emptying. Slower gastric emptying reduces stomach acid production. Stomach acid is essential for separating B12 from dietary protein so it can bind to intrinsic factor and be absorbed in the ileum. Less acid means less absorption. Over months of treatment, B12 levels decline.
By including methylcobalamin directly in the injection, the compound bypasses the entire oral absorption pathway. The B12 enters subcutaneous tissue and moves directly into the bloodstream, completely avoiding the gastric absorption problem that tirzepatide itself creates.
How it differs from brand-name tirzepatide
Brand-name tirzepatide, sold as Mounjaro for diabetes and Zepbound for weight management, contains only tirzepatide as the active pharmaceutical ingredient. No B12. No glycine. No niacinamide. The branded versions use specific inactive ingredients as stabilizers and buffers, but the therapeutic molecule is tirzepatide alone.
Compounded versions take a different approach. They can combine tirzepatide with additional active ingredients that address known gaps in the treatment experience. The most common additions include methylcobalamin for B12 support, glycine for nausea reduction and muscle preservation, and niacinamide for cellular energy metabolism. These are not random additions. Each one addresses a specific clinical observation about what happens to patients during extended GLP-1 therapy.
The compounding process
A compounding pharmacy starts with tirzepatide base powder and methylcobalamin powder. Both are pharmaceutical-grade ingredients sourced from FDA-registered suppliers. The pharmacist reconstitutes these into a sterile injectable solution at specific concentrations, typically measured in milligrams per milliliter for tirzepatide and micrograms per milliliter for methylcobalamin.
Common concentration pairings include 5 mg/mL tirzepatide with 1,000 mcg/mL methylcobalamin, 10 mg/mL tirzepatide with 1,000 mcg/mL methylcobalamin, and 15 mg/mL tirzepatide with 2,000 mcg/mL methylcobalamin. The exact ratio varies by pharmacy and prescriber preference. What does not vary is the requirement for sterile compounding conditions, proper beyond-use dating, and stability testing. You can learn more about how different pharmacies approach tirzepatide compounding in our Empower pharmacy tirzepatide guide and Lavender Sky tirzepatide review.
Why methylcobalamin instead of cyanocobalamin?
This is the question that separates informed researchers from everyone else. Both methylcobalamin and cyanocobalamin are forms of vitamin B12. Both can technically correct a B12 deficiency. But the way they work in the body is fundamentally different, and those differences matter when you are already asking your metabolism to do extraordinary things during a tirzepatide weight loss protocol.
Cyanocobalamin is synthetic. It does not exist in nature. Your body has never seen it before in the context of food or natural biological processes. When you inject cyanocobalamin, your liver must first remove the cyanide group, a process that consumes glutathione, your primary cellular antioxidant. Then your liver attaches either a methyl group to create methylcobalamin or an adenosyl group to create adenosylcobalamin. Only then can your cells actually use it.
Methylcobalamin skips those steps entirely.
It arrives ready to work. No conversion necessary. No glutathione depletion. No metabolic overhead. Your cells can immediately put it to use in the methionine synthase reaction and other methylation-dependent pathways.
Bioavailability and retention
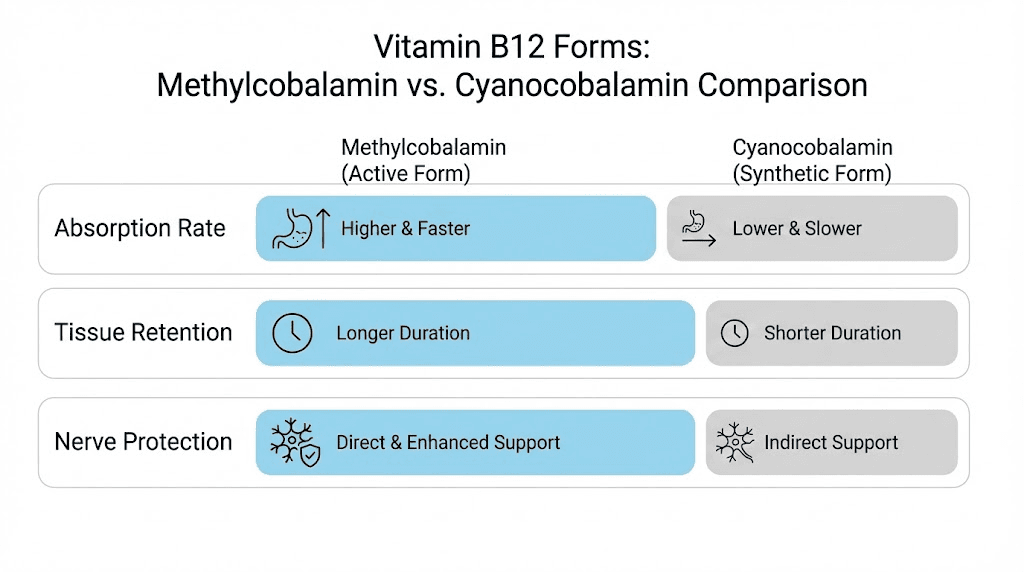
Research on the comparative bioavailability of these two forms reveals an interesting pattern. Cyanocobalamin may have slightly higher initial absorption rates, approximately 49% versus 44% for methylcobalamin at equivalent doses according to published pharmacokinetic data. But here is the critical finding. Cyanocobalamin is excreted in urine at three times the rate of methylcobalamin. Your body absorbs it and then dumps most of it.
Methylcobalamin sticks around. It gets retained in tissues, particularly in the liver and nervous system, at significantly higher rates. For someone on a long-term tirzepatide protocol where sustained B12 levels matter more than a single dose spike, retention is what counts.
The neurological advantage
Methylcobalamin has a direct role in nerve health that cyanocobalamin does not share until it undergoes conversion. Research published in Neural Regeneration Research demonstrates that methylcobalamin promotes nerve regeneration, protects the myelin sheath that insulates nerve fibers, and inhibits abnormal spontaneous firing in damaged sensory neurons. A 12-month randomized controlled trial in patients with diabetic neuropathy found that 1,000 mcg daily of methylcobalamin improved nerve conduction velocity, reduced pain scores, and improved overall quality of life.
This matters for tirzepatide users because body aches, muscle pain, and peripheral tingling are reported side effects during weight loss treatment. Whether these symptoms stem from B12 depletion, rapid metabolic changes, or other factors, having the most neuroprotective form of B12 on board provides a meaningful layer of defense.
Methylation and metabolic support
The methyl group that methylcobalamin carries is not just a structural detail. It is a functional tool. Your body uses methyl groups constantly for a process called methylation, which regulates gene expression, neurotransmitter production, detoxification, and inflammation control. When methyl donors run low, you feel it. Fatigue, brain fog, mood changes, and slow recovery are all signs of impaired methylation.
During tirzepatide therapy, your body is burning through resources faster than normal. You are losing weight rapidly, restructuring metabolic pathways, and adapting to reduced caloric intake. The demand for methyl groups increases. Methylcobalamin delivers those methyl groups directly. Cyanocobalamin makes your body create them, which requires additional folate and enzymatic capacity that may already be strained. For supporting your overall nutritional status during treatment, see our guide on supplements to take with tirzepatide.
How tirzepatide and methylcobalamin work together
Understanding why these two molecules complement each other requires looking at the metabolic picture from multiple angles. Tirzepatide drives weight loss. Methylcobalamin protects the systems that tirzepatide stresses. The partnership is less about synergy and more about balance.
The energy equation
One of the most common complaints during tirzepatide therapy is fatigue. Patients report feeling tired, sluggish, and mentally foggy, especially during the first several weeks and during dose escalations. Multiple factors contribute. Reduced caloric intake drops available glucose. Metabolic adaptation to fat burning takes time. And B12 levels start declining as gastric acid production falls.
Methylcobalamin addresses the B12 component directly. As a coenzyme for methylmalonyl-CoA mutase in the mitochondria, it feeds the citric acid cycle, your primary engine for ATP production. Without adequate B12, this pathway slows down. Cells produce less energy. You feel exhausted despite adequate sleep and nutrition.
Studies show that correcting B12 deficiency in patients with fatigue produces measurable improvements in energy levels, cognitive function, and exercise tolerance within 2-4 weeks. For tirzepatide users who experience energy drops, this is not a minor benefit. It is the difference between maintaining an active lifestyle during treatment and spending evenings on the couch. If fatigue is a persistent concern, our tirzepatide and energy guide covers additional strategies.
Appetite regulation and neurological signaling
Tirzepatide suppresses appetite through central nervous system pathways. It acts on hypothalamic neurons that control hunger and satiety signals. This process depends on healthy neurotransmitter production. Serotonin, dopamine, and norepinephrine all require methylation reactions for their synthesis.
Methylcobalamin supports this machinery. By providing methyl groups for the conversion of homocysteine to methionine, it maintains the supply of S-adenosylmethionine (SAMe), the universal methyl donor. SAMe is required for synthesizing serotonin from tryptophan, dopamine from tyrosine, and melatonin from serotonin. When SAMe levels are adequate, these neurotransmitter pathways function normally.
When SAMe levels drop, things get complicated.
Mood disturbances, anxiety, sleep problems, and even rebound hunger can emerge. These are not tirzepatide side effects per se. They are downstream consequences of inadequate methylation support during a metabolically demanding protocol. Including methylcobalamin in the formulation helps prevent this cascade before it starts.
Homocysteine management
Elevated homocysteine is a cardiovascular risk factor that receives far too little attention in the weight loss community. When B12 is insufficient, homocysteine accumulates because the conversion to methionine stalls. High homocysteine damages blood vessel walls, promotes clotting, and increases inflammation.
Tirzepatide improves several cardiovascular markers on its own, including blood pressure, triglycerides, and HbA1c. But allowing homocysteine to climb during treatment partially undermines those benefits. Methylcobalamin keeps the homocysteine conversion pathway running, maintaining levels in the healthy range below 12 micromoles per liter. This is particularly important for users who are also dealing with metabolic syndrome or type 2 diabetes, conditions where cardiovascular risk is already elevated.
The B12 deficiency problem with GLP-1 medications
The connection between GLP-1 receptor agonists and B12 depletion is not theoretical. It is documented. And the numbers are concerning enough that major medical organizations now recommend B12 monitoring for anyone on long-term GLP-1 therapy.
How GLP-1 medications deplete B12
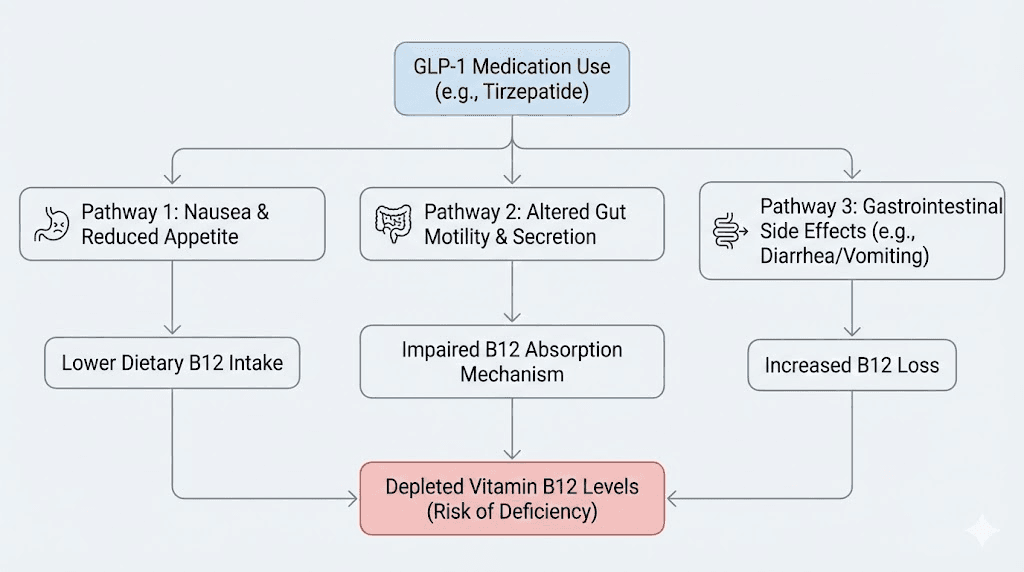
The mechanism operates through three interconnected pathways. First, GLP-1 agonists delay gastric emptying, which is central to how they reduce appetite. Food stays in the stomach longer, which sounds beneficial for satiety but creates a problem for B12 absorption. Prolonged gastric retention alters the pH environment and disrupts the normal sequence of B12 liberation from food proteins.
Second, GLP-1 receptor activation directly reduces parietal cell activity in the stomach lining. Parietal cells produce hydrochloric acid and intrinsic factor, both of which are essential for B12 absorption. Less parietal cell activity means less acid and less intrinsic factor. Less intrinsic factor means less B12 reaching the ileum where absorption occurs.
Third, reduced food intake compounds the problem. People on tirzepatide who experience strong appetite suppression simply eat less. They consume fewer animal products, which are the primary dietary source of B12. Even if absorption capacity were normal, dietary intake alone may be insufficient. Our guide on foods to avoid on tirzepatide and what to eat on tirzepatide can help optimize nutrition during treatment.
The research numbers
A retrospective observational study found that nutritional deficiencies were diagnosed in 12.7% of GLP-1 receptor agonist users within 6 months and 22.4% within 12 months. B12 was among the most commonly depleted nutrients. Another study tracking B12 levels specifically found an average decline of 15% over 12 months of GLP-1 therapy, with approximately 20% of participants falling below the normal B12 range and requiring supplementation.
These are not fringe findings. A joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and the Obesity Society now recommends proactive nutritional monitoring for anyone on GLP-1 medications. B12, vitamin D, calcium, iron, and zinc are all flagged as nutrients of concern. For a broader perspective on how GLP-1 medications affect energy and nutrient status, see our GLP-1 fatigue guide.
Symptoms of B12 deficiency during tirzepatide therapy
B12 deficiency does not announce itself with a single dramatic symptom. It creeps in. The early signs are subtle enough that most people attribute them to the tirzepatide itself or to the stress of caloric restriction.
Fatigue comes first. Not the kind that sleep fixes. A deep, persistent tiredness that settles into your muscles and your thinking. You wake up tired. You stay tired. You assume it is part of the weight loss process.
Then come the neurological symptoms. Tingling in the fingers and toes. Numbness that comes and goes. A feeling like your hands fell asleep except they did not. These symptoms overlap significantly with what some tirzepatide users report as body aches or muscle pain, making it difficult to distinguish between B12 deficiency and direct medication effects without blood testing.
Cognitive changes follow. Difficulty concentrating. Word-finding problems. Memory lapses that feel unusual. Mood shifts toward irritability or low-grade depression.
Advanced B12 deficiency can cause megaloblastic anemia, irreversible nerve damage, and cognitive decline. These severe outcomes are rare in the context of GLP-1 therapy because most people either supplement or discontinue treatment before reaching that point. But the subclinical effects, the fatigue, the brain fog, the tingling, those affect quality of life in ways that can derail an otherwise successful weight loss journey. For users noticing these symptoms, our guide on tirzepatide not working anymore explores how to troubleshoot stalled progress.
Dosage protocols for tirzepatide methylcobalamin compounds
Dosage in compounded tirzepatide methylcobalamin formulations involves two variables. The tirzepatide dose follows established titration schedules. The methylcobalamin dose typically remains fixed. Understanding both is essential for optimizing your protocol.
Standard tirzepatide titration with methylcobalamin
The typical starting point for compounded tirzepatide methylcobalamin mirrors the FDA-approved titration schedule for brand-name tirzepatide, adjusted for the specific concentration of the compound. Most protocols begin at 2.5 mg of tirzepatide per week. If you are new to GLP-1 medications, this starting dose allows your body to adapt to the gastrointestinal effects before increasing. For detailed starting dose guidance, see our compounded tirzepatide starting dose guide.
A typical titration schedule looks like this.
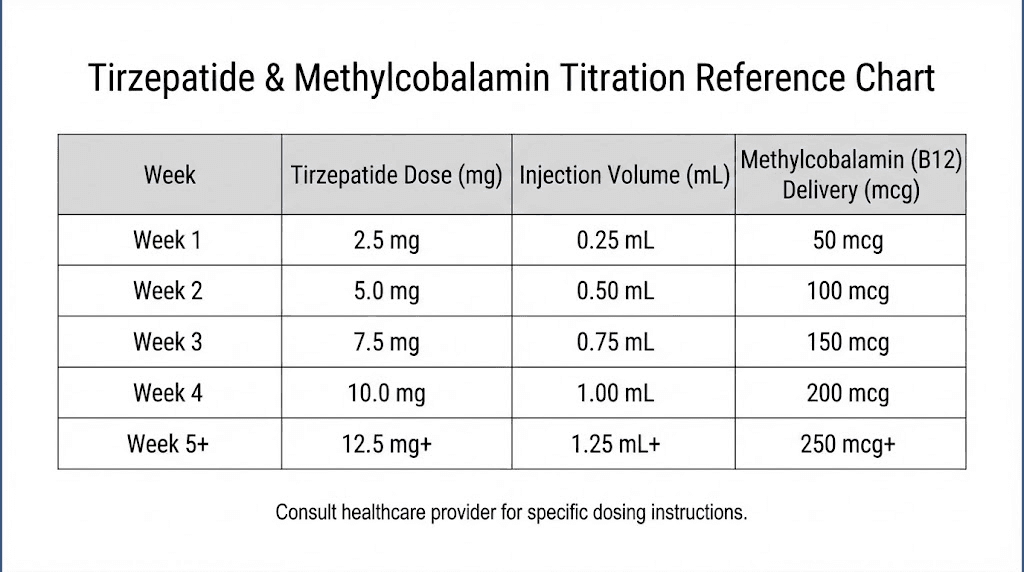
Weeks 1-4: 2.5 mg tirzepatide with 1,000 mcg methylcobalamin weekly. This is the adaptation phase. Expect mild gastrointestinal effects. The methylcobalamin begins building your B12 reserves from the very first injection.
Weeks 5-8: 5 mg tirzepatide with 1,000 mcg methylcobalamin weekly. Weight loss typically becomes noticeable during this phase. Appetite suppression intensifies. The consistent B12 supplementation prevents the early depletion that often occurs with unsupplemented protocols.
Weeks 9-12: 7.5 mg tirzepatide with 1,000-2,000 mcg methylcobalamin weekly. This is where significant results accumulate. Some prescribers increase the methylcobalamin dose at this stage to match the higher metabolic demands.
Weeks 13-16: 10 mg tirzepatide with 1,000-2,000 mcg methylcobalamin weekly. Many patients reach their maintenance dose in this range.
Weeks 17+: Up to 15 mg tirzepatide with 2,000 mcg methylcobalamin weekly for those who need maximum dose. Only escalate under medical supervision. Not everyone needs the highest dose. For comprehensive dosing charts, see our tirzepatide dose chart and tirzepatide compound dosage chart.
Calculating your injection volume
The volume you inject depends on the concentration of your compound. This is where many new users get confused, and getting it wrong means either underdosing or overdosing. Our compounded tirzepatide dosage calculator simplifies this process, but understanding the math is important.
For a 5 mg/mL tirzepatide compound with 1,000 mcg/mL methylcobalamin:
2.5 mg dose = 0.5 mL (500 mcg methylcobalamin delivered)
5 mg dose = 1.0 mL (1,000 mcg methylcobalamin delivered)
7.5 mg dose = 1.5 mL (1,500 mcg methylcobalamin delivered)
For a 10 mg/mL tirzepatide compound with 1,000 mcg/mL methylcobalamin:
2.5 mg dose = 0.25 mL (250 mcg methylcobalamin delivered)
5 mg dose = 0.5 mL (500 mcg methylcobalamin delivered)
10 mg dose = 1.0 mL (1,000 mcg methylcobalamin delivered)
Notice the problem with higher concentration compounds. As the tirzepatide concentration increases, the injection volume decreases, which means less methylcobalamin per dose unless the pharmacy increases the B12 concentration proportionally. Always verify that your compound delivers adequate methylcobalamin at your target tirzepatide dose. For help converting between units and milligrams, see our guides on tirzepatide unit conversions and 50 units of tirzepatide in mg.
Injection technique
Tirzepatide methylcobalamin compounds are administered via subcutaneous injection, typically once weekly. The injection technique is identical to standard tirzepatide. Preferred injection sites include the abdomen (at least 2 inches from the navel), the front of the thigh, and the upper arm. Rotate sites weekly to prevent lipodystrophy and ensure consistent absorption.
One thing to note about methylcobalamin-containing compounds is their color. Methylcobalamin gives the solution a characteristic red or dark pink appearance. This is normal. If your compound is clear and colorless, it likely contains cyanocobalamin rather than methylcobalamin, or it may not contain B12 at all. Always verify with your pharmacy. For detailed injection guidance, see our tirzepatide stomach injection guide and GLP-1 injection guide.
Benefits beyond weight loss
The combination of tirzepatide and methylcobalamin delivers benefits that extend well beyond the number on the scale. Understanding these secondary benefits helps set realistic expectations and provides motivation during the challenging early weeks of treatment.
Energy and cognitive function
Users of tirzepatide methylcobalamin compounds consistently report better energy levels compared to those using tirzepatide alone. This is not a placebo effect. It is a direct consequence of maintaining adequate B12 status while your body adapts to reduced caloric intake and increased fat metabolism. The methylcobalamin feeds the citric acid cycle in your mitochondria, supporting ATP production at the cellular level.
Cognitive benefits follow the same logic. B12 is essential for myelin maintenance, which protects the nerve fibers responsible for fast information processing. It supports neurotransmitter synthesis. It reduces homocysteine, which at elevated levels is neurotoxic. Researchers using methylcobalamin-containing compounds often report clearer thinking and better focus than those on tirzepatide alone, particularly at higher doses where caloric restriction is most severe.
Neuroprotection during rapid weight loss
Rapid weight loss creates metabolic stress. As fat stores mobilize, they release stored toxins, inflammatory mediators, and metabolic byproducts. The nervous system is vulnerable during this period, particularly peripheral nerves that depend on consistent B12 supply for myelin maintenance.
Methylcobalamin provides targeted neuroprotection. Research published in Integrative Medicine Insights found that methylcobalamin at therapeutic doses promoted nerve regeneration and inhibited ectopic spontaneous discharges from damaged sensory neurons. For tirzepatide users experiencing aches or tingling, this neuroprotective effect is directly relevant.
Cardiovascular risk reduction
Tirzepatide alone improves multiple cardiovascular markers. Adding methylcobalamin addresses the homocysteine angle that tirzepatide cannot. By maintaining efficient conversion of homocysteine to methionine, methylcobalamin helps prevent the endothelial damage, increased clotting tendency, and chronic inflammation that elevated homocysteine causes.
This dual approach to cardiovascular protection is particularly relevant for individuals using tirzepatide to manage both weight and type 2 diabetes, where cardiovascular disease is the leading cause of death. The tirzepatide handles blood sugar, triglycerides, and blood pressure. The methylcobalamin handles homocysteine. For a broader comparison of how different formulations affect cardiovascular markers, see our semaglutide vs tirzepatide side effects comparison.
Mood stability and mental health
Weight loss journeys are emotionally turbulent. Caloric restriction affects neurotransmitter production. Hormonal shifts during fat loss alter mood regulation. Sleep disruption from gastrointestinal side effects compounds the problem. Adding anxiety or depression to this mix can derail even the most determined researcher.
Methylcobalamin supports mood stability through its role in SAMe production. SAMe is the primary methyl donor for serotonin, dopamine, and norepinephrine synthesis. Adequate SAMe levels correlate with stable mood, better stress resilience, and healthier sleep patterns. Clinical studies have shown that B12 supplementation improves depression scores in patients with documented deficiency, with some studies suggesting benefits even in those with low-normal B12 levels.
This does not mean methylcobalamin is an antidepressant. It means that preventing B12 deficiency during a metabolically demanding protocol removes one potential contributor to mood disturbance.
Hair and skin preservation
One of the most distressing side effects of rapid weight loss is hair loss. While the primary cause is telogen effluvium triggered by caloric deficit and hormonal changes, B12 deficiency can exacerbate the problem. B12 is involved in DNA synthesis within hair follicle cells, and inadequate levels slow the hair growth cycle.
Methylcobalamin does not prevent telogen effluvium. That requires addressing the caloric deficit and giving the body time to adapt. But it does ensure that B12 deficiency is not an additional contributing factor, and it supports the recovery of normal hair cycling once weight stabilizes.
Side effects and what to expect
The side effect profile of tirzepatide methylcobalamin compounds reflects primarily the tirzepatide component. Methylcobalamin at typical supplemental doses is extremely safe with virtually no adverse effects. Understanding what comes from which molecule helps you manage your experience effectively.
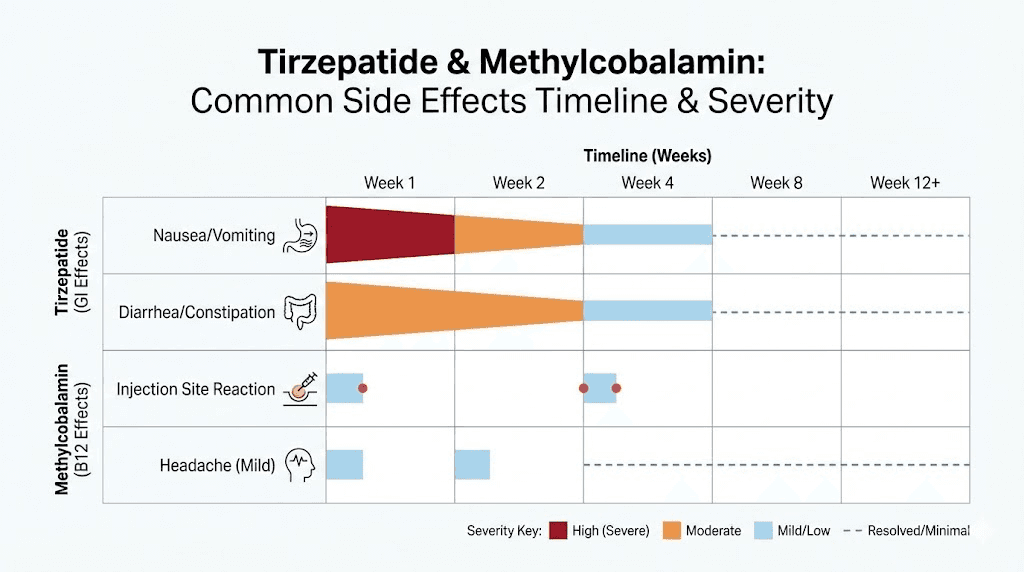
Gastrointestinal effects from tirzepatide
Nausea is the most common side effect, affecting 30-40% of users during the initial weeks. It typically improves as your body adapts. Constipation affects approximately 15-25% of users due to delayed gastric transit. Diarrhea occurs in 10-20% of users, often alternating with constipation as the GI system adjusts. Decreased appetite is technically a therapeutic effect rather than a side effect, but it can be dramatic enough to concern new users.
Interestingly, some evidence suggests that B12 supplementation may help reduce nausea severity during GLP-1 therapy. The mechanism is not fully established, but B12 plays a role in neurological signaling pathways that regulate the vomiting reflex. This is one reason compounding pharmacies began including it in the first place, beyond just preventing deficiency. For comprehensive side effect management, see our guide on tirzepatide headaches and tirzepatide insomnia.
What methylcobalamin does not cause
Methylcobalamin at doses used in compounded tirzepatide (typically 500-2,000 mcg per injection) does not cause significant side effects. B12 is a water-soluble vitamin with no established upper intake level because excess is excreted in urine. Some users notice a slight flushing sensation immediately after injection, which is transient and harmless.
Allergic reactions to methylcobalamin are exceedingly rare but theoretically possible. If you experience hives, swelling, or difficulty breathing after injection, seek medical attention immediately. These reactions are not specifically to methylcobalamin but rather to the injectable formulation as a whole.
The injection site reaction question
Some users report that methylcobalamin-containing compounds cause slightly more injection site redness than standard tirzepatide. This may be due to the red color of methylcobalamin creating the visual impression of more redness, or it may reflect a mild local inflammatory response to the additional component. Either way, injection site reactions are typically mild and resolve within 24-48 hours. Rotating injection sites, as recommended for all subcutaneous injections, minimizes this concern.
Tirzepatide methylcobalamin vs other compounded formulations
Compounding pharmacies offer tirzepatide in several different combinations. Understanding the differences helps you choose the formulation that best matches your needs and work with your prescriber to make an informed decision.
Tirzepatide methylcobalamin vs tirzepatide cyanocobalamin
This is the most direct comparison. Both formulations include B12, but the form differs. Methylcobalamin is the bioactive form that your body uses immediately. It has higher tissue retention and provides direct neuroprotection. It is slightly less stable in solution and sensitive to light. Cyanocobalamin requires liver conversion before your cells can use it. It has lower tissue retention with three times more excreted in urine. It is more stable in solution but consumes glutathione during conversion. For storage guidance, see our articles on tirzepatide refrigeration and tirzepatide fridge storage duration.
Tirzepatide methylcobalamin vs tirzepatide glycine B12
The tirzepatide glycine B12 compound adds glycine as a third active ingredient. Glycine is a nonessential amino acid with several relevant properties for GLP-1 therapy.
Glycine supports muscle preservation during caloric deficit. This matters because rapid weight loss often includes lean mass loss, which slows metabolism and reduces functional strength. Glycine also has documented anti-nausea properties, which can make the tirzepatide experience more tolerable during early titration phases.
If your primary concerns are energy, neuroprotection, and methylation support, tirzepatide methylcobalamin alone may be sufficient. If you are also concerned about muscle loss and nausea management, the triple combination with glycine adds another layer of support. Both are valid approaches, and your prescriber can help determine which better matches your clinical picture.
Tirzepatide methylcobalamin vs tirzepatide niacinamide
Tirzepatide niacinamide compounds take a different approach entirely. Niacinamide, a form of vitamin B3, supports cellular energy production through the NAD+ pathway, reduces inflammation, and may help with skin health during weight loss.
The choice between methylcobalamin and niacinamide depends on your primary concerns. Choose methylcobalamin if B12 deficiency risk is your priority, if you have a history of neurological symptoms or neuropathy, if you want direct methylation support, or if you are on long-term therapy where B12 depletion is cumulative. Choose niacinamide if inflammation management matters most, if skin health during weight loss is a concern, if you already supplement B12 separately, or if your prescriber has identified specific NAD+ pathway needs.
Comparison with semaglutide methylcobalamin
For researchers comparing GLP-1 receptor agonists, the semaglutide methylcobalamin compound offers a useful comparison point. Semaglutide is a pure GLP-1 receptor agonist, while tirzepatide activates both GIP and GLP-1 receptors. The dual mechanism of tirzepatide generally produces greater weight loss and stronger appetite suppression in head-to-head comparisons.
Both compounds benefit equally from methylcobalamin inclusion because the B12 depletion mechanism is common to all GLP-1 medications. The choice between tirzepatide methylcobalamin and semaglutide methylcobalamin should be based on the primary peptide, not the B12 form, since that component is identical. For a full comparison of the two base peptides, see our semaglutide vs tirzepatide comparison page and the dosage comparison chart.
Storage, handling, and reconstitution
Methylcobalamin adds specific storage considerations that standard tirzepatide compounds do not require. Getting this right preserves potency. Getting it wrong wastes money and reduces effectiveness.
Light sensitivity is the primary concern
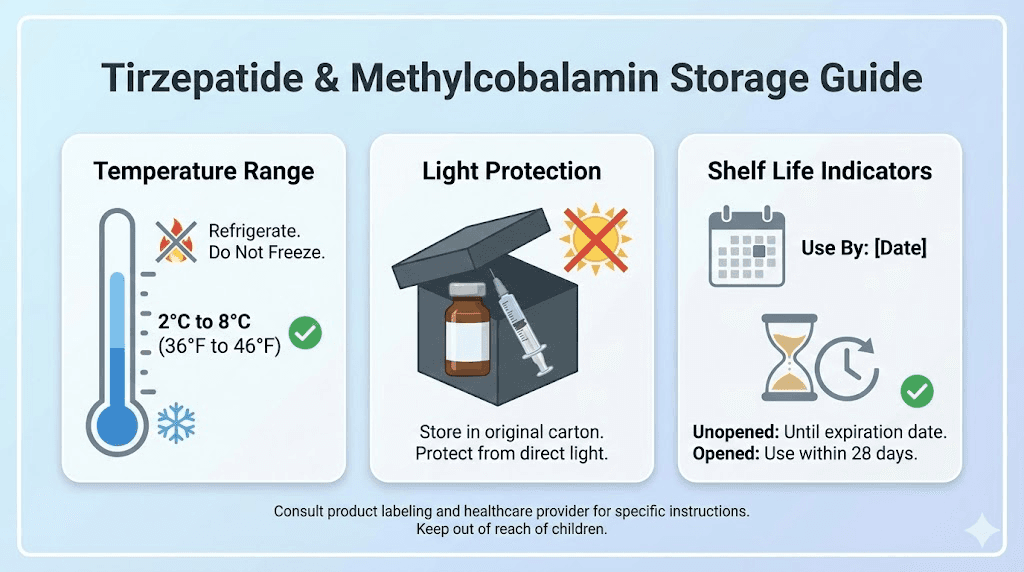
Methylcobalamin degrades when exposed to light. This is the single most important storage difference between methylcobalamin and cyanocobalamin compounds. Ultraviolet and visible light break the carbon-cobalt bond in methylcobalamin, converting it to inactive hydroxocobalamin. A vial left on a counter near a window can lose significant potency within days.
Store your compound in its original amber vial or wrap it in aluminum foil. Keep it in the refrigerator, not on the door shelf where the light hits it every time the door opens, but toward the back where it stays dark and cold. Our guide to tirzepatide out of the fridge covers temperature excursion limits.
Temperature requirements
Compounded tirzepatide methylcobalamin should be stored at 36-46 degrees Fahrenheit (2-8 degrees Celsius). This is standard refrigerator temperature. Freezing damages the peptide structure and can alter the methylcobalamin solution. Room temperature storage is acceptable for short periods, typically up to 24-48 hours, but should not be routine.
If your compound arrives warm from shipping, contact your pharmacy before using it. Temperature excursions during transit can compromise potency, and most reputable pharmacies will replace affected orders. For comprehensive storage information, see our guides on tirzepatide refrigeration requirements and tirzepatide expiration.
Beyond-use dating
Compounded tirzepatide methylcobalamin typically carries a beyond-use date of 30-90 days from compounding, depending on the pharmacy and the specific formulation. This is not the same as an expiration date on a manufactured drug. Beyond-use dates for compounded preparations are more conservative because they are prepared in smaller batches without the extensive stability testing data that large pharmaceutical manufacturers generate.
Mark your vial with the date you receive it. Use it within the pharmacy-specified beyond-use period. If the solution changes color, develops particles, or becomes cloudy, discard it regardless of the date. Methylcobalamin solutions that turn from red to yellow or brown have likely degraded.
Reconstitution considerations
Most compounded tirzepatide methylcobalamin arrives as a ready-to-use solution. Unlike research peptides that come as lyophilized powder requiring reconstitution with bacteriostatic water, compounded formulations from licensed pharmacies are typically pre-mixed.
If you do receive a lyophilized compound requiring reconstitution, follow the pharmacy instructions exactly. Use only the diluent provided or specified. Do not shake the vial, as this can denature the tirzepatide. Gentle swirling is the correct technique. Our tirzepatide reconstitution guide covers the full process, and our peptide reconstitution calculator can help determine volumes for any concentration.
Optimizing your tirzepatide methylcobalamin protocol
Having the right compound is only the beginning. How you use it determines your results. These optimization strategies come from documented clinical observations and community experience.
Timing your injection
Most prescribers recommend a consistent weekly injection schedule. Pick a day and stick with it. The half-life of tirzepatide is approximately 5 days, which means weekly dosing maintains steady-state levels after the first few weeks.
Some researchers report better tolerance when injecting in the evening, as any nausea occurs during sleep rather than during waking hours. Others prefer morning injections to take advantage of the methylcobalamin energy boost during the day. There is no definitive evidence favoring one time over the other. The best time is the time you will be consistent with. For more on timing considerations, see our best time to take a GLP-1 shot guide.
Supporting nutrition
Methylcobalamin addresses B12 needs, but it does not cover all the nutritional bases. During tirzepatide therapy, you should also consider vitamin D (commonly depleted during weight loss), magnesium (supports muscle function and sleep), iron (especially for menstruating women on reduced intake), zinc (important for immune function and wound healing), and omega-3 fatty acids (anti-inflammatory support).
A comprehensive approach to nutrition during GLP-1 therapy involves more than supplements. It requires strategic meal planning that maximizes nutrient density within reduced caloric intake. Our tirzepatide diet plan and tirzepatide meal plan provide structured approaches, while our GLP-1 companion guide covers the full nutritional support framework.
Monitoring your progress
Track more than just weight. The combination of tirzepatide and methylcobalamin affects multiple systems, and monitoring them gives you a complete picture of how you are responding.
Blood tests every 3-4 months should include B12 levels (even with methylcobalamin supplementation, some people need more), methylmalonic acid (a more sensitive marker of functional B12 status than serum B12 alone), homocysteine (should stay below 12 micromoles per liter), complete blood count (to check for anemia), and comprehensive metabolic panel (liver and kidney function).
Body composition measurements complement scale weight. Losing fat while preserving muscle is the goal, and body composition tracking helps confirm you are achieving that ratio. If you notice concerning trends, our guides on why you are not losing weight on tirzepatide and tirzepatide not working anymore provide troubleshooting frameworks.
Dose escalation strategy
The temptation to escalate quickly is real. You want results. But fast titration increases side effect severity without necessarily improving outcomes.
Stay at each dose for a minimum of 4 weeks. Some prescribers recommend 6-8 weeks at each level before escalating. The goal is to find the minimum effective dose, the lowest amount of tirzepatide that produces steady weight loss with tolerable side effects. Higher is not always better. Many researchers achieve excellent results at 5-7.5 mg and never need to reach 10 or 15 mg. For a structured approach to dose management, consult our microdosing tirzepatide chart and microdose tirzepatide schedule.
The regulatory landscape for compounded tirzepatide
The availability of compounded tirzepatide methylcobalamin depends on regulatory decisions that have shifted significantly in recent years. Understanding the current landscape helps researchers make informed decisions about access and legality.
The shortage provision and its evolution
Compounding pharmacies were initially permitted to produce tirzepatide formulations under a provision in federal law that allows compounding when a drug is in shortage. During the period when brand-name tirzepatide faced supply constraints, compounding pharmacies legally produced alternative formulations including those combined with methylcobalamin, glycine, and niacinamide.
When the FDA determined that the tirzepatide shortage had been resolved, the legal basis for compounding changed. The FDA issued guidance restricting the production of compounded tirzepatide, and federal courts upheld these restrictions in several cases. However, the regulatory environment remains dynamic. Some compounding pharmacies continue to operate under state-level regulations or through different legal frameworks, while others have ceased tirzepatide production entirely.
What this means for researchers
If you are currently using or considering a compounded tirzepatide methylcobalamin product, work with a licensed healthcare provider who understands the current regulatory status in your jurisdiction. The legality of compounded tirzepatide varies by state, by pharmacy type (503A vs 503B), and by the specific claims made about the compound.
Regardless of regulatory status, the clinical rationale for combining methylcobalamin with tirzepatide remains valid. If compounded formulations are not available, taking a separate methylcobalamin supplement alongside brand-name tirzepatide achieves the same nutritional goal, though without the convenience of a single injection. For comparing options and finding current sources, see our guides on affordable compounded tirzepatide and affordable tirzepatide options.
Comparing combined compounds to separate supplementation
A reasonable question is whether you need methylcobalamin in your compound at all, or whether taking it separately works just as well. The answer depends on what you prioritize.
Advantages of the combined compound
Convenience is the obvious benefit. One injection handles both the GLP-1 therapy and the B12 supplementation. You do not need to remember a separate supplement. You do not need to worry about oral B12 absorption, which is problematic when tirzepatide is actively suppressing your gastric acid production.
Bypassing oral absorption is the clinical advantage. Injectable methylcobalamin goes directly into subcutaneous tissue and enters the bloodstream without requiring stomach acid, intrinsic factor, or ileal absorption. This is the same reason B12 injections are preferred over oral supplements for patients with pernicious anemia or documented absorption disorders. For tirzepatide users whose medication is actively reducing their ability to absorb oral B12, the injectable route makes physiological sense.
Advantages of separate supplementation
Dose flexibility is the main benefit. When methylcobalamin is built into the compound, your B12 dose is tied to your tirzepatide dose. If you need more B12 than the compound provides, you need an additional supplement anyway. With separate supplementation, you can adjust the B12 dose independently based on blood test results.
Cost may also factor in. Compounded formulations with methylcobalamin cost more than plain tirzepatide compounds. If budget is a concern, using the less expensive compound with a separate sublingual methylcobalamin supplement could provide adequate B12 support at lower cost, though with the absorption limitations noted above. Our peptide cost calculator can help compare total cost scenarios.
The practical recommendation
For most researchers, the combined compound is preferable during active tirzepatide therapy because it ensures consistent B12 delivery through a route that bypasses the absorption barriers that tirzepatide creates. If the combined compound is unavailable, injectable methylcobalamin as a separate weekly injection is the next best option. Oral sublingual methylcobalamin (1,000-5,000 mcg daily) is a reasonable third choice, with the understanding that absorption may be reduced.
SeekPeptides members get access to detailed protocol guides that help determine which supplementation approach best fits individual circumstances, along with tools for tracking B12 levels and adjusting protocols based on lab results.
Who benefits most from tirzepatide methylcobalamin?
Not everyone needs methylcobalamin in their tirzepatide compound. But certain populations benefit significantly more than others. Identifying whether you fall into a high-benefit group helps you make an informed decision about your formulation choice.
High-benefit populations
Individuals over 50 years old benefit substantially because age-related decline in gastric acid production already reduces B12 absorption before tirzepatide further compounds the problem. The combination of age-related and medication-related absorption impairment creates a double risk for deficiency.
People with a history of gastrointestinal surgery, including bariatric procedures, have reduced absorptive capacity that makes injectable B12 particularly important. Vegetarians and vegans who already have lower dietary B12 intake face compounded risk when GLP-1 medications further reduce absorption and appetite.
Individuals with MTHFR gene variants, which affect methylation capacity, benefit from receiving pre-methylated B12 rather than forms requiring additional conversion. Those on long-term GLP-1 therapy (6+ months) face cumulative depletion risk that makes proactive supplementation more important than for short-term users. And anyone who has already experienced muscle pain, fatigue, or neurological symptoms during GLP-1 therapy should strongly consider the methylcobalamin formulation.
Lower-benefit populations
Young, healthy individuals with no digestive issues, no dietary restrictions, and normal B12 levels who plan short-term tirzepatide use (under 3 months) may not need methylcobalamin in their compound. A standard multivitamin may suffice for this group, though monitoring B12 levels remains advisable.
Understanding lab results during treatment
Knowing what to test and how to interpret results ensures you catch problems early and optimize your protocol based on data rather than guesswork.
Serum B12 levels
Normal range is typically 200-900 pg/mL (148-664 pmol/L). However, serum B12 is an imperfect marker. It measures total circulating B12 without distinguishing between active and inactive forms. You can have a normal serum B12 while still having functional deficiency at the tissue level.
Aim for the upper half of the normal range, above 500 pg/mL, during active tirzepatide therapy. If your levels drop below 400 pg/mL despite methylcobalamin supplementation, your prescriber may increase the dose or add an additional B12 source.
Methylmalonic acid
Methylmalonic acid (MMA) is a more sensitive and specific marker of B12 status than serum B12. When B12 is insufficient at the cellular level, MMA accumulates because the B12-dependent enzyme that converts it to succinyl-CoA cannot function properly. Normal MMA is below 0.4 micromol/L. Elevated MMA with a normal serum B12 confirms functional deficiency.
Homocysteine
Target is below 12 micromol/L. Elevated homocysteine in the context of B12 supplementation may indicate either inadequate B12 dosing, folate deficiency (which is a co-factor in the same pathway), or an MTHFR variant that impairs methylation efficiency. If homocysteine remains elevated despite adequate methylcobalamin, adding methylfolate (5-MTHF) often resolves the issue.
Complete blood count
B12 deficiency causes megaloblastic anemia, characterized by elevated mean corpuscular volume (MCV). However, concurrent iron deficiency, which is also common during weight loss, can mask the elevated MCV by pushing it downward. Look at MCV in context with iron studies for a complete picture.
Common mistakes to avoid
Even informed researchers make avoidable errors when using tirzepatide methylcobalamin compounds. These are the most common ones and how to prevent them.
Assuming the compound handles all your B12 needs
If your compound delivers 500 mcg of methylcobalamin per injection and you are significantly deficient, that may not be enough. Some individuals need 2,000-5,000 mcg daily during the repletion phase, far more than a weekly injection provides. Get your levels tested. Adjust accordingly.
Exposing the compound to light
This bears repeating because it is the single most common handling error. Methylcobalamin degrades in light. Every time you draw a dose with the vial sitting on a bright countertop, you are accelerating degradation. Keep the vial in a dark, cold place. Take it out, draw your dose quickly, and return it.
Skipping the titration schedule
Starting at a high dose because you want faster results increases nausea, vomiting, and the likelihood of abandoning treatment. The titration schedule exists because dose-escalation studies show significantly better tolerability with gradual increases. Follow the schedule your prescriber sets. Our starting dose guide explains why patience during early titration pays off.
Not tracking what you eat
Methylcobalamin supports energy metabolism, but it cannot compensate for a diet that is catastrophically low in protein, fiber, and micronutrients. During tirzepatide therapy, every calorie matters more because you are consuming fewer of them. Protein intake should target at least 1.0-1.2 grams per kilogram of goal body weight to preserve lean mass. Our tirzepatide diet plan provides structured approaches.
Changing pharmacies without verifying the formulation
Not all compounding pharmacies use methylcobalamin. Some use cyanocobalamin and call it B12 without specifying the form. If you switch pharmacies, explicitly confirm that your new compound contains methylcobalamin rather than cyanocobalamin if that is your preference.
Tirzepatide methylcobalamin and exercise performance
Researchers who maintain exercise programs during tirzepatide therapy have valid concerns about how the compound affects workout capacity, recovery, and body composition.
Energy for training
The methylcobalamin component supports mitochondrial energy production, which directly impacts exercise capacity. Users who exercise regularly often report that the methylcobalamin-containing compound feels noticeably different from plain tirzepatide in terms of workout energy. While this is anecdotal, the mechanism is biologically plausible. B12 is essential for the citric acid cycle, and any deficiency would reduce ATP availability during exercise.
That said, reduced caloric intake during tirzepatide therapy limits available glucose for high-intensity work. Methylcobalamin improves energy metabolism efficiency, but it does not create energy from nothing. Strategic carbohydrate timing around workouts helps maintain performance. For those interested in combining weight loss with muscle growth or athletic performance, our specialized guides cover peptide strategies for these goals.
Recovery support
B12 supports red blood cell production, nerve function, and protein synthesis, all of which are important for exercise recovery. Adequate B12 ensures that oxygen-carrying capacity remains high, that nerve signals to muscles are transmitted efficiently, and that the muscle protein synthesis signaling pathway has the cofactors it needs.
During rapid weight loss, recovery times tend to increase because the body is already under metabolic stress. Methylcobalamin does not eliminate this effect, but it ensures that B12 deficiency is not adding to the recovery burden. Combined with adequate protein intake and appropriate training volume, the compound supports maintaining fitness progress during the weight loss phase. For recovery from injuries during this period, our healing guide covers additional peptide options.
Special considerations for specific populations
Diabetic users
People with type 2 diabetes using tirzepatide methylcobalamin face unique considerations. Metformin, one of the most commonly prescribed diabetes medications, also depletes B12 through a separate mechanism involving calcium-dependent membrane changes in the ileum. If you are taking both tirzepatide and metformin, your B12 depletion risk is doubled, making the methylcobalamin compound especially valuable.
Blood sugar monitoring becomes more complex when adding tirzepatide to an existing diabetes regimen. The combined effects of tirzepatide on insulin secretion and glucagon suppression alongside methylcobalamin on improved mitochondrial energy metabolism can shift glucose patterns in ways that require medication adjustment. Work closely with your endocrinologist or diabetes specialist.
Women of reproductive age
B12 is essential for fetal neural tube development during early pregnancy. Women who become pregnant while on tirzepatide, which is increasingly documented given the fertility-enhancing effects of weight loss, need adequate B12 reserves. Methylcobalamin supplementation during the pre-conception period and early pregnancy is recommended by most prenatal care guidelines. For specific information about this topic, see our guide on pregnancy on tirzepatide and tirzepatide effects on menstrual cycles.
Tirzepatide is not approved for use during pregnancy. If pregnancy is discovered, tirzepatide should be discontinued. The methylcobalamin component, however, is not a concern during pregnancy and in fact supports fetal development.
Older adults
Age-related changes in gastric acid production, intrinsic factor secretion, and intestinal absorption make older adults particularly vulnerable to B12 deficiency during GLP-1 therapy. The compounded formulation with injectable methylcobalamin bypasses all of these age-related absorption barriers. For adults over 65, the methylcobalamin formulation is arguably the most beneficial variant of compounded tirzepatide available.
Frequently asked questions
What color should tirzepatide methylcobalamin be?
Tirzepatide methylcobalamin solutions typically appear red to dark pink due to the methylcobalamin content. The exact shade depends on concentration. Higher methylcobalamin concentrations produce deeper red colors. If your compound is clear or very light pink, it may contain cyanocobalamin instead of methylcobalamin. Verify with your pharmacy.
Can I take additional methylcobalamin supplements alongside the compound?
Yes. Methylcobalamin is water-soluble with no established upper intake level. If your compound delivers 500-1,000 mcg weekly and your blood tests show inadequate levels, adding a sublingual methylcobalamin supplement (1,000-5,000 mcg daily) is safe and may be necessary. Consult your prescriber for personalized dosing.
Does methylcobalamin help with tirzepatide nausea?
Some clinical observations suggest that B12 supplementation may reduce nausea severity during GLP-1 therapy. The mechanism likely involves B12 role in neurological signaling pathways that modulate the vomiting reflex. However, this has not been established in controlled trials. Glycine is a more established anti-nausea addition to tirzepatide compounds.
How long does tirzepatide methylcobalamin last in the fridge?
Most compounding pharmacies assign a beyond-use date of 30-90 days for tirzepatide methylcobalamin compounds when stored properly at 36-46 degrees Fahrenheit in the dark. Tirzepatide storage duration depends on the specific formulation and compounding method. Always follow the date specified by your pharmacy.
Is tirzepatide methylcobalamin better than brand-name tirzepatide?
They serve different purposes. Brand-name tirzepatide (Mounjaro, Zepbound) has been through rigorous clinical trials and has FDA approval. Compounded tirzepatide methylcobalamin has not undergone the same level of testing but addresses a known nutritional gap in GLP-1 therapy. The B12 component does not enhance the weight loss effect of tirzepatide. It prevents a deficiency that the medication itself tends to cause.
Can I switch between tirzepatide methylcobalamin and regular tirzepatide?
Yes. The tirzepatide component is the same active molecule regardless of whether methylcobalamin is included. If you switch to a formulation without B12, add a separate methylcobalamin supplement to maintain your B12 levels. Our switching guide covers transitions between different GLP-1 formulations.
Do I need a prescription for tirzepatide methylcobalamin?
Yes. Tirzepatide is a prescription medication regardless of the formulation. You need a licensed healthcare provider to prescribe it and a licensed compounding pharmacy to prepare it. Methylcobalamin alone is available over the counter, but the combination product requires a prescription.
What happens if my tirzepatide methylcobalamin compound turns yellow or brown?
Color change from red to yellow or brown indicates methylcobalamin degradation, usually from light exposure or temperature excursion. The tirzepatide may still be active, but the methylcobalamin potency is compromised. Contact your pharmacy for a replacement. Do not use a compound with significant color change.
External resources
PubMed Central: Methylcobalamin as a potential pain management agent
PubMed Central: Comparative bioavailability of B12 supplement forms
PubMed Central: Nutritional deficiencies in GLP-1 receptor agonist users
PubMed: Vitamin B12 supplementation in diabetic neuropathy trial
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your methylcobalamin stay potent, your energy stay high, and your protocols stay optimized.