Feb 26, 2026

Some people breeze through their first tirzepatide injection with nothing more than mild fullness. Others spend three days curled up with nausea so severe they swear off the medication entirely. The difference rarely comes down to biology alone. It almost always comes down to dosing strategy.
Standard tirzepatide protocols start at 2.5 mg per week, then increase every four weeks through 5 mg, 7.5 mg, 10 mg, and up to 15 mg. That works for plenty of people. But for those with GI sensitivity, medication intolerance history, or simply a preference for gentler approaches, the standard ramp feels like jumping into the deep end without learning to swim first. Microdosing offers another path. A slower, more deliberate one that lets the body adapt to GLP-1 receptor activation at a pace it can actually handle.
This guide walks through every step of the microdosing process. Not the theory. Not the debate about whether it works. The actual, practical how-to, from calculating your first sub-therapeutic dose to tracking your response over weeks and months. You will learn exactly how to prepare your vial, draw up precise amounts in a syringe, choose a schedule that matches your goals, and know when to increase. Whether you are brand new to tirzepatide or switching from semaglutide and want a cautious start, this is the reference you will keep coming back to.
One important note before we begin. Microdosing tirzepatide is not an FDA-approved protocol. No large-scale clinical trials have evaluated sub-therapeutic doses specifically. Everything in this guide should be discussed with a licensed healthcare provider who can monitor your individual response and adjust your plan accordingly. Safety comes first. Always.
What tirzepatide microdosing actually means
Tirzepatide microdosing refers to using doses below the standard starting point of 2.5 mg per week. Instead of jumping straight into the clinical protocol, microdosing begins at doses as low as 0.5 mg or even 0.25 mg, then increases gradually over extended timelines. Think of it as a gentler on-ramp to the same highway everyone else is driving on.
The concept is not unique to tirzepatide. Microdosing approaches exist across medicine, from immunotherapy using gradual exposure to psychiatric medications starting below therapeutic doses to assess tolerance. The principle is the same: give the body time to adapt before ramping up to full therapeutic levels. Understanding how peptides work at the receptor level helps explain why this approach makes biological sense.
With tirzepatide specifically, microdosing means different things to different people. For some, it means starting at half the standard dose, roughly 1.0 to 1.5 mg, for the first month instead of 2.5 mg. For others, it means extending the time at each dose level, spending eight to twelve weeks at 2.5 mg before moving to 5 mg instead of the standard four weeks. And for a smaller group, it means maintaining a permanently lower dose as a weight maintenance strategy rather than ever escalating to full therapeutic levels.
The microdosing tirzepatide chart that most providers reference breaks this into weekly increments. But charts alone do not tell you how to actually do it. They do not explain how to calculate syringe units from milligrams, how to reconstitute a vial for precise micro-amounts, or how to know when your body is ready for the next step. That is what this guide covers.
How microdosing differs from standard dosing
Standard tirzepatide dosing follows a rigid schedule. You start at 2.5 mg weekly for four weeks. Then 5 mg for four weeks. Then 7.5 mg, 10 mg, and finally 15 mg, each maintained for at least four weeks before escalation. The clinical dosing protocol was designed for controlled pharmaceutical products with pre-filled pens where the dose is exact.
Microdosing throws out the rigid four-week escalation timeline. Instead, it prioritizes your body response over arbitrary schedules. You might spend six weeks at 1.0 mg before moving to 1.5 mg. You might stay at 2.5 mg for three months because the results satisfy your goals without needing more. The flexibility is the entire point.
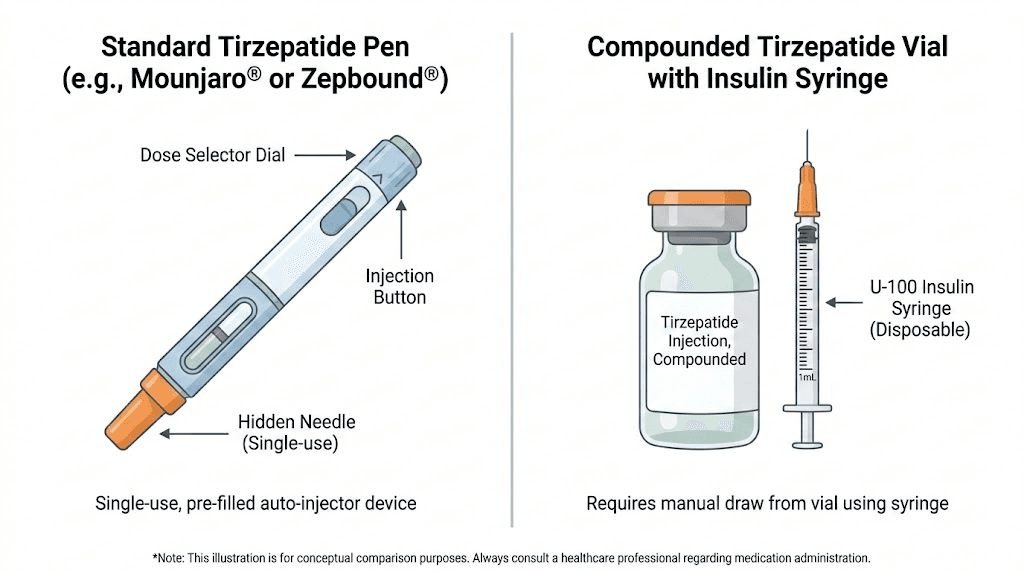
This approach requires compounded tirzepatide in most cases, because brand-name tirzepatide pens come in fixed doses. Compounded vials, on the other hand, allow you to draw any amount with a standard insulin syringe. That precision is what makes true microdosing possible.
How tirzepatide works at lower doses
Understanding what happens inside your body at sub-therapeutic doses helps explain both the potential benefits and limitations of microdosing. Tirzepatide is not like most medications where you either get the effect or you do not. It operates on a sliding scale.
Tirzepatide is a dual GIP/GLP-1 receptor agonist. That dual action is what separates it from semaglutide and other GLP-1-only medications. It binds to both the glucose-dependent insulinotropic polypeptide (GIP) receptor and the glucagon-like peptide-1 (GLP-1) receptor, triggering cascading metabolic effects that influence appetite, insulin sensitivity, fat metabolism, and gastric emptying speed.
Research from the Journal of Clinical Investigation shows tirzepatide binds the GIP receptor with affinity similar to native GIP (Ki of 0.135), while its GLP-1 receptor affinity is roughly five-fold weaker than native GLP-1 (Ki of 4.23). This imbalanced engagement is actually deliberate. It produces a biased signaling pattern that favors cAMP generation over beta-arrestin recruitment at the GLP-1 receptor, which may enhance insulin response while reducing some side effects associated with traditional GLP-1 agonists.
What happens at sub-therapeutic concentrations
At doses below 2.5 mg, the receptor activation is partial. Not absent, but reduced. Think of it like turning the volume knob from zero to three instead of jumping straight to seven. The appetite suppression signals still reach the brain. The gastric emptying still slows somewhat. But the intensity is dialed down, which means both the desired effects and the unwanted side effects tend to be milder.
The GIP receptor responds first at lower concentrations because tirzepatide has stronger affinity for it. This means the earliest metabolic benefits you may notice, improved insulin sensitivity and glucose regulation, can appear before significant appetite suppression kicks in. Some providers frame this as a feature: your metabolism begins improving before the dramatic appetite changes that catch many people off guard.
However, it is important to be honest about the limitations. Ultra-low doses, below 0.5 mg, may not activate the receptors enough to produce predictable or meaningful clinical effects. The receptor activation threshold varies between individuals, which is why some people respond beautifully to 1.0 mg while others feel nothing until they reach 2.5 mg or higher.
The SURMOUNT trial data at lowest doses
The SURMOUNT-1 trial, published in the New England Journal of Medicine, tested tirzepatide at 5 mg, 10 mg, and 15 mg, but not below 5 mg. At the lowest tested dose of 5 mg weekly, participants achieved a mean placebo-adjusted weight reduction of 11.9% from baseline after 72 weeks. That is significant. About 30% of participants on the 5 mg dose reached the 20% weight loss threshold.
The SURMOUNT-4 trial examined weight maintenance, showing that participants who continued tirzepatide after initial weight loss maintained and even extended their results, while those switched to placebo regained 14% of lost weight during the follow-up period. This data supports the idea that even lower maintenance doses may help sustain results, though the specific microdosing ranges have not been formally studied.
The absence of clinical trial data below 2.5 mg is the biggest caveat in the entire microdosing conversation. Everything below that threshold is based on extrapolation, anecdotal reports, and individual provider experience. It is not a reason to avoid microdosing entirely, but it is a reason to approach it with your eyes open and a qualified provider supervising your care.
Step-by-step guide to getting started with tirzepatide microdosing
Theory is useful. But you came here for the how-to. Here is the complete process from your very first day, broken into manageable steps that anyone can follow regardless of prior experience with injectable peptides or GLP-1 medications.
Step 1: Work with a licensed healthcare provider
This is not optional. Tirzepatide is a prescription medication that affects blood sugar levels, gastric function, and metabolic pathways. You need baseline bloodwork before starting, including fasting glucose, HbA1c, a complete metabolic panel, thyroid function tests, and lipid panel. Your provider will also screen for contraindications such as personal or family history of medullary thyroid carcinoma, MEN 2 syndrome, pancreatitis history, or pregnancy.
When discussing microdosing with your provider, be specific about why you want a sub-standard starting dose. Common reasons include previous intolerance to GLP-1 medications, GI sensitivity concerns, desire for gradual weight loss to minimize loose skin, or interest in metabolic benefits before significant appetite suppression. Most experienced providers will support a conservative approach because better adherence leads to better long-term outcomes.
Step 2: Source compounded tirzepatide
Microdosing requires compounded tirzepatide in vial form, not pre-filled pens. Brand-name pens (Mounjaro, Zepbound) deliver fixed doses and cannot be adjusted for microdosing. Compounded vials from a licensed pharmacy allow you to draw any volume, which means any dose, using a standard insulin syringe.
When sourcing your tirzepatide, verify that the compounding pharmacy holds proper accreditation. Look for NABP accreditation, FDA-registered outsourcing facility (503B) status, or state board of pharmacy licensure. Use the FDA BeSafeRx tool to verify online pharmacies. Ask your provider for specific pharmacy recommendations, as many telehealth platforms partner with verified compounding pharmacies. Resources like our affordable tirzepatide guide cover options in more detail.
Your vial will come labeled with a concentration, typically expressed as mg/mL. Common concentrations include 2.5 mg/mL, 5 mg/mL, 10 mg/mL, and 20 mg/mL. Write down your concentration. You will need it for every dose calculation.
Step 3: Gather your supplies
Before your first injection, you need the following items ready:
Insulin syringes (1 mL/100 unit or 0.5 mL/50 unit, with 29-31 gauge needles)
Alcohol swabs (for cleaning vial top and injection site)
Sharps container (for safe needle disposal)
Your compounded tirzepatide vial
Bacteriostatic water (only if your vial requires reconstitution)
A tracking journal or app (for logging doses, side effects, weight, and measurements)
For microdosing specifically, 0.5 mL (50 unit) syringes offer better precision than 1 mL syringes because each unit marking represents a smaller volume. When drawing tiny doses like 5 or 10 units, the smaller syringe makes accurate measurement much easier. The syringe dosage guide explains the differences in detail. If you are new to injectable medications, the peptide injection overview covers the fundamentals of subcutaneous self-injection from start to finish.
Step 4: Reconstitute your vial if needed
Some compounded tirzepatide arrives as a ready-to-inject liquid. Others arrive as lyophilized (freeze-dried) powder that requires reconstitution with bacteriostatic water. Your pharmacy label will indicate which type you have.
If reconstitution is needed:
Clean the tops of both vials (tirzepatide and bacteriostatic water) with alcohol swabs
Draw the specified amount of bacteriostatic water into a syringe
Inject the water into the tirzepatide vial, aiming the stream against the glass wall, not directly onto the powder
Swirl gently. Do not shake. Vigorous shaking can damage the peptide structure
Wait until the solution is completely clear with no visible particles
Label the vial with the reconstitution date and calculated concentration
The amount of bacteriostatic water you add determines your concentration. For example, adding 2 mL of water to a 10 mg vial creates a 5 mg/mL solution. Adding 1 mL creates 10 mg/mL. The bacteriostatic water mixing guide and the reconstitution calculator make this math straightforward.
For microdosing, a lower concentration (like 2.5 mg/mL or 5 mg/mL) is often preferable because it means you draw larger volumes for each dose. Drawing 20 units from a syringe is far more precise than drawing 2 units. Precision matters enormously when you are working with sub-therapeutic amounts. The complete reconstitution chart and printable PDF version are useful references to keep near your preparation area.
Step 5: Calculate your microdose in syringe units
This is where many people get confused. The math is simple once you understand the formula, but getting it wrong means either underdosing or overdosing. Neither is acceptable.
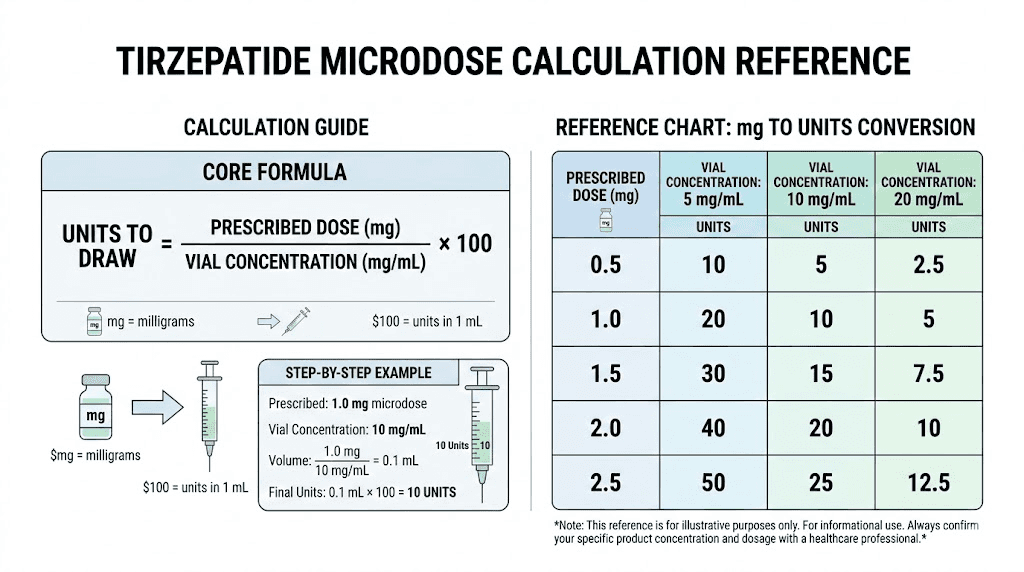
The formula: Units = (Desired dose in mg / Concentration in mg per mL) x 100
For example, if your vial concentration is 5 mg/mL and you want a 1.0 mg microdose:
Units = (1.0 / 5.0) x 100 = 20 units
So you draw 20 units on your insulin syringe. That gives you exactly 1.0 mg of tirzepatide.
Here are common microdose calculations at a 5 mg/mL concentration:
0.5 mg dose: (0.5 / 5.0) x 100 = 10 units
0.75 mg dose: (0.75 / 5.0) x 100 = 15 units
1.0 mg dose: (1.0 / 5.0) x 100 = 20 units
1.25 mg dose: (1.25 / 5.0) x 100 = 25 units
1.5 mg dose: (1.5 / 5.0) x 100 = 30 units
2.0 mg dose: (2.0 / 5.0) x 100 = 40 units
2.5 mg dose: (2.5 / 5.0) x 100 = 50 units
At a 10 mg/mL concentration, those same doses require half the volume. A 1.0 mg dose would be only 10 units. That is still measurable, but less forgiving of small errors. The tirzepatide conversion chart covers every common concentration and dose combination if you want a quick reference. You can also run the numbers through the peptide calculator to double-check your math.
Always verify your calculations before injecting. Have your provider confirm your first calculation. Write it down and keep it visible near your injection supplies.
Step 6: Draw up and inject your microdose
With your calculation confirmed, the injection process follows standard subcutaneous technique. If you have never injected before, do not panic. Millions of people self-inject medications daily. The needle is tiny, the process takes seconds, and most people describe the sensation as a brief pinch or nothing at all.
The injection steps:
Wash your hands thoroughly with soap and water
Clean the top of your tirzepatide vial with a fresh alcohol swab
Remove the cap from your insulin syringe without touching the needle
Pull back the plunger to draw air equal to your dose volume (for example, 20 units of air for a 20-unit dose)
Insert the needle through the vial rubber stopper and push in the air
Invert the vial so the needle tip is submerged in liquid
Pull back slowly to draw your calculated dose
Check for air bubbles. If present, tap the syringe gently and push air out, then redraw to the correct volume
Remove the syringe from the vial
Choose your injection site: abdomen (2 inches from navel), front of thigh, or back of upper arm
Clean the injection site with a fresh alcohol swab and let it dry
Pinch a fold of skin, insert the needle at a 45 to 90 degree angle, and push the plunger steadily
Hold for 5 to 10 seconds before withdrawing the needle
Do not rub the injection site
Dispose of the syringe in your sharps container
Rotate your injection sites with each dose. Using the same spot repeatedly can cause lipohypertrophy (tissue lumps) that affect medication absorption. The stomach injection guide and the broader syringe injection guide provide detailed visual instructions for each site.
Step 7: Track everything from day one
Microdosing only works as a strategy if you are paying attention to how your body responds. Without tracking, you have no basis for knowing when to adjust. Keep a daily log that includes:
Injection date, time, dose, and site
Appetite level on a 1 to 10 scale
Energy level on a 1 to 10 scale
GI symptoms (nausea, bloating, constipation, diarrhea) with severity rating
Weight (same time each morning, same conditions)
Notable observations (food cravings, mood changes, sleep quality)
After two to four weeks at each dose level, review your log for patterns. Are side effects manageable? Is appetite decreasing? Are you losing weight gradually? This data drives your dosing decisions. Without it, you are guessing. SeekPeptides members use structured tracking protocols to monitor their progress systematically, turning subjective feelings into objective data points.
Microdosing tirzepatide dosage schedules
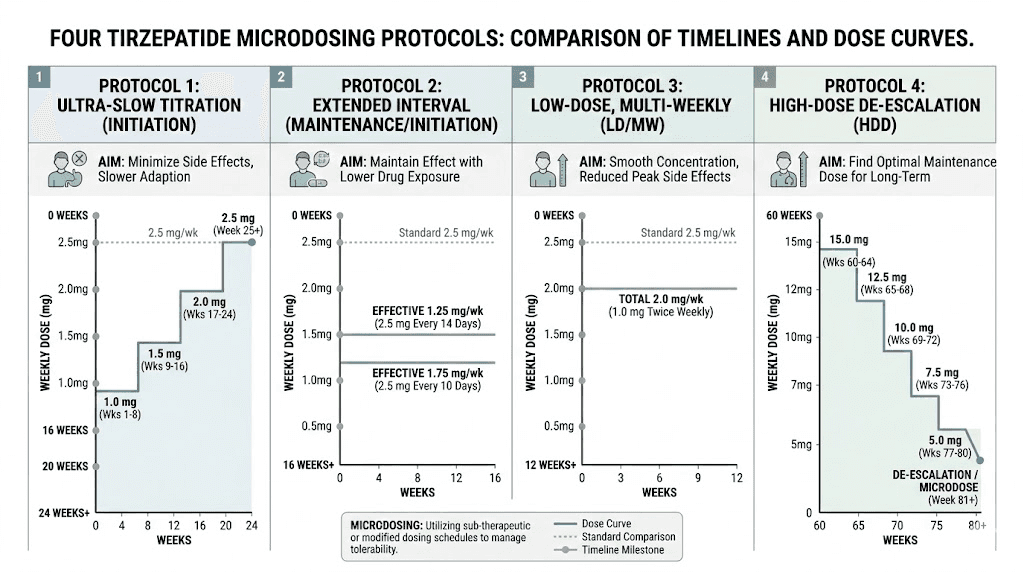
Not everyone microdoses the same way. Your starting point, escalation speed, and target dose depend on your individual goals, sensitivity, and provider guidance. Here are the four most common approaches.
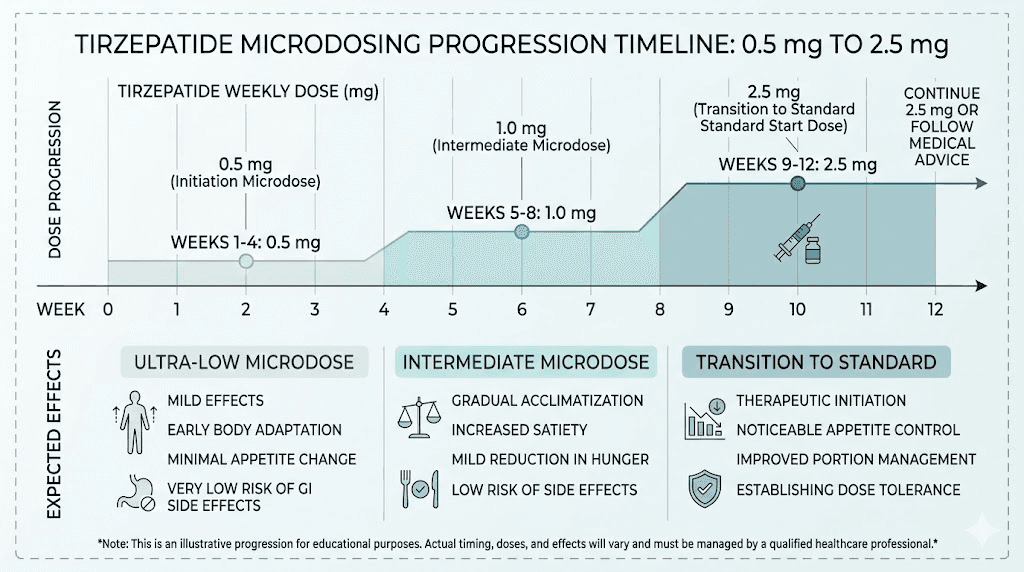
Protocol 1: The conservative slow-start schedule
This protocol is for people who want the gentlest possible introduction. It starts well below the standard dose and increases in small increments over several months.
Weeks | Weekly dose | Purpose |
|---|---|---|
1 to 2 | 0.5 mg | Initial receptor priming |
3 to 4 | 0.75 mg | Gradual adaptation |
5 to 8 | 1.0 mg | Early metabolic effects |
9 to 12 | 1.5 mg | Increasing appetite response |
13 to 16 | 2.0 mg | Approaching therapeutic threshold |
17 and beyond | 2.5 mg | Standard starting dose reached |
This approach takes about four months to reach what most people start at on day one. That sounds slow. It is. But for people with severe GI sensitivity or previous bad experiences with GLP-1 medications, those four months can mean the difference between staying on treatment long-term and quitting in week two.
Protocol 2: The modified standard schedule
This approach starts at or near the standard dose but extends the time between escalations. Instead of increasing every four weeks, you stay at each level for eight to twelve weeks.
Weeks | Weekly dose | Standard comparison |
|---|---|---|
1 to 8 | 2.5 mg | Standard is 4 weeks only |
9 to 20 | 5.0 mg | Standard is 4 weeks only |
21 to 32 | 7.5 mg | Standard is 4 weeks only |
33 and beyond | Assess if higher needed | Standard continues to 15 mg |
Many providers actually prefer this approach because it uses the same doses as the FDA-approved protocol, just at a slower pace. The microdose schedule guide covers this protocol in greater detail. Some people find they reach their goals at 5 mg or 7.5 mg with extended use and never need to escalate to 10 or 15 mg, saving both money and side effect burden.
Protocol 3: The split-dose frequency approach
Instead of reducing the weekly total, this protocol divides the standard dose into smaller, more frequent injections. The weekly total remains the same, but each individual injection is smaller.
Standard approach | Split-dose approach | Weekly total |
|---|---|---|
2.5 mg once weekly | 1.25 mg twice weekly | 2.5 mg |
5.0 mg once weekly | 2.5 mg twice weekly | 5.0 mg |
7.5 mg once weekly | 2.5 mg three times weekly | 7.5 mg |
The rationale is straightforward. Smaller individual doses produce lower peak concentrations in the blood, which correlates with fewer side effects, especially nausea. The trade-off is more frequent injections. The split-dose guide explores whether this approach is right for you, including the pharmacokinetic reasoning behind it. Some users report more stable appetite suppression throughout the week with this method, avoiding the common pattern of strong effects for the first three days followed by waning appetite control before the next injection.
Protocol 4: Low-dose maintenance
This protocol is not for people just starting tirzepatide. It is for those who have already achieved their weight loss goals and want to maintain results without staying on higher doses indefinitely.
After reaching target weight on standard dosing, you gradually reduce back down. Some people maintain on 2.5 mg weekly. Others find 1.0 to 1.5 mg sufficient. The SURMOUNT-4 trial data shows that stopping tirzepatide entirely leads to significant weight regain, so maintaining some level of medication support, even at reduced doses, appears to produce better long-term outcomes than complete cessation.
This is arguably the most practical application of microdosing. Not as a way to start, but as a way to sustain. The weight maintenance guide covers this transition in detail.
How to calculate your tirzepatide microdose in units
Dosing errors are the most dangerous mistake in the microdosing process. Getting this section right is non-negotiable. Read it carefully. Then read it again.
Understanding your vial concentration
Every compounded tirzepatide vial has a concentration listed on the label, expressed as milligrams per milliliter (mg/mL). This number tells you how much active tirzepatide is dissolved in each milliliter of liquid.
Common concentrations and what they mean:
2.5 mg/mL: Each 1 mL of liquid contains 2.5 mg of tirzepatide. Each unit on the syringe equals 0.025 mg
5 mg/mL: Each 1 mL contains 5 mg. Each unit equals 0.05 mg
10 mg/mL: Each 1 mL contains 10 mg. Each unit equals 0.1 mg
20 mg/mL: Each 1 mL contains 20 mg. Each unit equals 0.2 mg
Higher concentrations mean you inject less volume for the same dose. That sounds convenient, but for microdosing, it creates a precision problem. At 20 mg/mL, a 1.0 mg dose requires only 5 units on the syringe. That is a tiny amount, and even a one-unit error means a 20% dosing deviation. For this reason, lower concentrations work better for microdosing. The dosage chart in units provides pre-calculated values for every common combination.
The complete conversion formula
You only need one formula. Memorize it.
Step 1: Volume in mL = Desired dose (mg) divided by Concentration (mg/mL)
Step 2: Syringe units = Volume (mL) multiplied by 100
That is because a standard insulin syringe has 100 units per 1 mL. So 0.2 mL equals 20 units, 0.5 mL equals 50 units, and so on.
Let us work through real examples. If you have a 10 mg/mL vial and want a 1.0 mg microdose: 1.0 divided by 10 equals 0.1 mL, which equals 10 units. If you have that same vial and want 0.5 mg: 0.5 divided by 10 equals 0.05 mL, which equals 5 units.
See the problem? Five units is extremely small. One graduation mark on most syringes. If your concentration forces you into single-digit unit counts, talk to your provider about using a lower-concentration vial or adding more bacteriostatic water during reconstitution (which lowers the concentration). The reconstitution chart helps you figure out the right ratio.
Quick reference: microdose calculations at every concentration
Desired dose | 2.5 mg/mL | 5 mg/mL | 10 mg/mL | 20 mg/mL |
|---|---|---|---|---|
0.25 mg | 10 units | 5 units | 2.5 units | 1.25 units |
0.5 mg | 20 units | 10 units | 5 units | 2.5 units |
0.75 mg | 30 units | 15 units | 7.5 units | 3.75 units |
1.0 mg | 40 units | 20 units | 10 units | 5 units |
1.25 mg | 50 units | 25 units | 12.5 units | 6.25 units |
1.5 mg | 60 units | 30 units | 15 units | 7.5 units |
2.0 mg | 80 units | 40 units | 20 units | 10 units |
2.5 mg | 100 units | 50 units | 25 units | 12.5 units |
Any value with a decimal (like 2.5 units or 6.25 units) is extremely difficult to measure accurately on a standard insulin syringe. Avoid these combinations. Choose a concentration that gives you whole-number unit counts for your target dose. The unit conversion guides walk through each specific dose in detail, including 10 units, 20 units, 30 units, and 40 units.
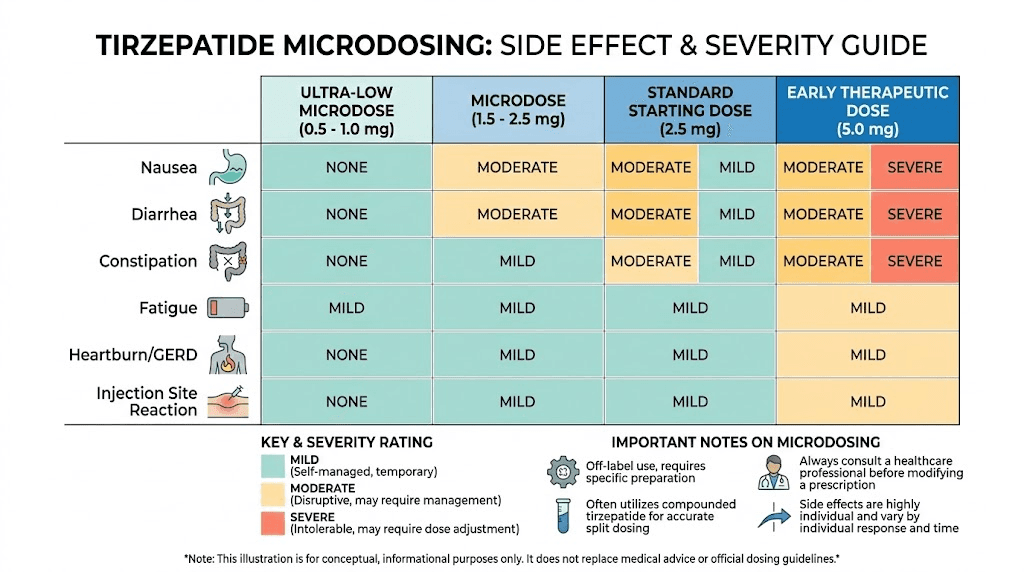
Managing side effects while microdosing tirzepatide
One of the primary reasons people choose microdosing is to reduce side effects. And for most, it works. Lower doses generally mean milder side effects. But "milder" does not always mean "none." Your body is still adjusting to a new medication that fundamentally changes how your digestive system and appetite regulation operate.
Nausea: the most common challenge
Nausea is the hallmark side effect of all GLP-1 and GIP receptor agonists. It occurs because tirzepatide slows gastric emptying, the rate at which food leaves your stomach. Your stomach stays fuller for longer, which is exactly the mechanism that reduces appetite, but it can also trigger queasiness, especially after eating large meals or high-fat foods.
At microdoses, nausea tends to be mild. Most people describe it as a background awareness rather than active sickness. But it can still be uncomfortable, especially during the first week or two at a new dose level.
Strategies that help:
Eat smaller, more frequent meals instead of three large ones
Avoid high-fat and greasy foods for the first few days after each dose increase
Do not eat past fullness. This is counterintuitive for people used to finishing everything on their plate, but with tirzepatide slowing your digestion, overeating causes significantly more discomfort than it did before
Ginger tea, ginger chews, or ginger supplements provide natural anti-nausea relief
Stay hydrated. Dehydration worsens nausea considerably. Aim for at least 64 ounces of water daily
Time your injection so that the first 24 to 48 hours (when side effects peak) fall on days when you can rest. Many people inject on Friday evenings for this reason
If nausea persists beyond the first two weeks at a given dose, or if it is severe enough to prevent eating, contact your provider. They may recommend supportive supplements or a brief hold at the current dose before attempting further increases. Over-the-counter options like vitamin B6 and doxylamine can help, and providers may prescribe ondansetron for more severe cases.
Constipation and other GI symptoms
Slowed gastric motility does not just affect the stomach. It slows the entire digestive tract, which can lead to constipation, bloating, and general abdominal discomfort. Conversely, some people experience loose stools or diarrhea, particularly in the first days after injection.
For constipation:
Increase fiber intake gradually (psyllium husk, vegetables, fruits)
Drink more water than you think you need
Magnesium citrate (200 to 400 mg daily) provides gentle osmotic relief
Stay physically active, as movement promotes gut motility
Consider a daily probiotic to support digestive balance
For bloating, eat slowly. Chew food thoroughly. Avoid carbonated beverages for the first few weeks. And pay attention to which foods trigger the worst symptoms. Many people discover that certain foods they tolerated fine before, like dairy or high-fiber beans, become temporarily problematic on tirzepatide.
Fatigue and energy fluctuations
Fatigue is common in the early weeks. Your body is adjusting to reduced caloric intake and metabolic changes simultaneously. Some people feel more tired than usual, while others report an initial energy boost followed by a mid-afternoon slump.
Adequate protein intake is the single most important factor for managing fatigue. When you are eating less overall, every calorie matters more. Prioritize protein at every meal (30 grams minimum per meal is a good target). Ensure you are getting enough calories overall, as dramatic caloric restriction on top of tirzepatide-induced appetite suppression can crash your energy levels and compromise muscle mass.
Sleep quality also matters enormously. Some people experience insomnia or disrupted sleep on tirzepatide, which compounds daytime fatigue. If this happens, try injecting in the morning instead of evening, as some users find that injection timing affects sleep quality. The injection timing guide covers optimal scheduling in detail.
Headaches, body aches, and other symptoms
Headaches during the first weeks are often related to dehydration or blood sugar fluctuations rather than direct medication effects. Increasing water intake and eating regular small meals usually resolves them. Body aches and muscle pain are less common at microdoses but can occur, particularly if you are also increasing exercise simultaneously.
Injection site reactions, including redness, itching, or small lumps, happen occasionally. These are usually mild and resolve within a few days. The injection site reaction treatment guide covers when to be concerned versus when reactions are normal and expected.
When to contact your provider immediately
Most side effects at microdoses are mild and manageable. But certain symptoms require immediate medical attention:
Severe abdominal pain that does not resolve (possible pancreatitis)
Persistent vomiting that prevents hydration
Signs of allergic reaction (hives, facial swelling, difficulty breathing)
Severe hypoglycemia symptoms (confusion, shakiness, loss of consciousness), especially if you take other diabetes medications
Unexplained lump or swelling in the neck (thyroid concern)
Do not push through severe symptoms hoping they resolve. The entire philosophy of microdosing is built on gentleness and caution. If something feels wrong, stop injecting and call your provider.
Nutrition and diet while microdosing tirzepatide
What you eat matters more on tirzepatide than it did before. Not because the medication restricts certain foods, but because reduced appetite means you eat less overall. When total intake drops, every meal needs to deliver maximum nutritional value. Poor food choices on lower calories lead to nutrient deficiencies, muscle loss, and the kind of weight loss nobody wants, where you lose muscle and keep fat.
Protein as the foundation
Protein is non-negotiable. On any weight loss medication, muscle preservation depends on adequate protein intake combined with resistance training. The general recommendation for people on GLP-1 medications is 0.7 to 1.0 grams of protein per pound of body weight daily. For a 180-pound person, that means 126 to 180 grams per day.
This is challenging when appetite is suppressed. Some strategies that help:
Start every meal with your protein source before eating anything else
Use protein shakes or protein supplements to hit targets on days when solid food is unappealing
Choose protein-dense foods: Greek yogurt, cottage cheese, eggs, lean meats, fish
Spread protein across all meals rather than trying to get it all in one sitting
The tirzepatide eating guide provides a full breakdown of optimal food choices, and the diet plan offers structured daily meal examples specifically designed for people on GLP-1 medications.
Foods to prioritize
Beyond protein, focus on:
Non-starchy vegetables for fiber and micronutrients without caloric density
Healthy fats in moderate amounts (avocado, olive oil, nuts) for satiety and hormone function
Complex carbohydrates in controlled portions (sweet potatoes, quinoa, oats) for sustained energy
Fermented foods (kimchi, sauerkraut, kefir) to support gut health during the digestive adjustment period
Foods to limit or avoid
The foods to avoid guide covers this in detail, but the short version: avoid anything that makes GI symptoms worse. High-fat meals, excessively spicy food, large portions, and alcohol all tend to amplify nausea and digestive discomfort while on tirzepatide. Alcohol deserves special mention because it can worsen blood sugar instability, increase dehydration, and amplify nausea. Many people find their alcohol tolerance drops significantly on GLP-1 medications.
Hydration requirements
Dehydration is a silent problem on tirzepatide. Reduced food intake means reduced water intake from food sources. Add in potential GI side effects like diarrhea, and dehydration can sneak up quickly.
Aim for a minimum of 64 ounces (about 2 liters) of water daily. More if you exercise, live in a hot climate, or experience GI symptoms. Electrolyte supplementation can help, especially during the first few weeks. Look for electrolyte products that provide sodium, potassium, and magnesium without added sugars.
Who should consider microdosing tirzepatide
Microdosing is not for everyone. It has specific applications where it offers genuine advantages over standard protocols. Understanding who benefits most helps you make an informed decision with your provider.
Good candidates for microdosing
People with GI sensitivity or medication intolerance history. If you have a pattern of reacting strongly to new medications, starting below the standard dose makes sense. People with irritable bowel syndrome, gastroparesis, or chronic nausea conditions are particularly good candidates.
Those transitioning from semaglutide. If you are switching from semaglutide to tirzepatide, microdosing allows your body to adjust to the new dual-receptor mechanism without stacking the adjustment on top of an abrupt medication change. The conversion chart helps determine equivalent starting points.
Women with hormonal considerations. Hormonal fluctuations during perimenopause and menopause can amplify GI sensitivity. Some providers specifically recommend microdosing for this population to allow metabolic adjustment without exacerbating hormonal symptoms.
People prioritizing gradual weight loss. Rapid weight loss increases the risk of loose skin, gallstones, and muscle loss. Microdosing produces a slower, more controlled rate of loss that gives skin time to adapt and makes muscle preservation easier.
Individuals seeking weight maintenance. After achieving target weight on standard doses, stepping down to a microdose for long-term maintenance avoids both the cost and side effects of full therapeutic dosing while potentially preventing the regain that occurs with complete cessation.
Who should NOT microdose
People with uncontrolled type 2 diabetes. If your blood sugar is dangerously elevated, you need therapeutic doses under close medical supervision. Microdosing may not provide adequate glycemic control in these situations.
Those unable to commit to careful tracking. Microdosing requires attention to detail, calculating doses, monitoring responses, and adjusting thoughtfully. If you prefer a straightforward "take this dose, increase on this date" approach, the standard starting protocol may be a better fit.
Anyone with contraindications to tirzepatide itself. Microdosing does not eliminate the fundamental risks of the medication. Personal or family history of medullary thyroid carcinoma, MEN 2 syndrome, pregnancy, breastfeeding, or active pancreatitis are absolute contraindications regardless of dose. The breastfeeding safety guide and pregnancy considerations article cover these situations specifically.
Common microdosing mistakes and how to avoid them
After reading through hundreds of community discussions and provider reports, certain mistakes appear again and again. Learning from other people mistakes is far cheaper than making your own.
Mistake 1: Choosing the wrong vial concentration
This is the most impactful error. Buying a 20 mg/mL vial when you plan to microdose at 0.5 mg means drawing 2.5 units, an amount so tiny that accurate measurement is nearly impossible. Before ordering, calculate how many syringe units your target microdose requires at the available concentration. If the answer is below 10 units, choose a lower concentration.
Mistake 2: Not tracking responses systematically
Many people start microdosing with good intentions but stop tracking after a week. Then they cannot remember whether last Wednesday they felt nauseated or fine, whether they ate 1,800 calories or 1,200, whether their energy was better or worse. Without data, dose adjustment decisions become arbitrary. Track daily for at least the first eight weeks.
Mistake 3: Increasing too quickly despite the plan
Impatience is human. You start at 0.5 mg, feel nothing for two weeks, and decide to jump to 2.0 mg. The whole point of microdosing is gradual escalation. If you skip steps, you eliminate the benefit. Stick to your planned schedule for at least two full cycles at each dose before adjusting. If your current dose is not producing effects, increase by one increment, not three. The common mistakes guide covers this pattern across many types of peptide use.
Mistake 4: Neglecting protein and nutrition
When appetite drops, total food intake often drops dramatically. If the food you do eat is calorie-dense but nutrient-poor, you lose muscle while retaining fat. This creates the dreaded "skinny fat" outcome where the scale looks better but body composition deteriorates. Prioritize protein at every meal, take a multivitamin, and track your nutrient intake alongside your weight.
Mistake 5: Improper storage destroying potency
Compounded tirzepatide is a protein that degrades when exposed to heat, light, or contamination. Refrigeration is essential. Store your vial at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Do not freeze. Do not leave it on the counter. Do not store it in a car. A vial left at room temperature for extended periods may look fine but contain degraded peptide that produces inconsistent or absent effects. The refrigerator storage guide explains proper handling in detail.
Mistake 6: Assuming microdosing means no medical supervision
Some people pursue microdosing specifically to avoid involving a healthcare provider, sourcing compounded tirzepatide through informal channels and self-directing their protocol. This is genuinely dangerous. Tirzepatide affects blood sugar, thyroid function, pancreatic activity, and cardiovascular parameters. You need baseline labs, periodic monitoring, and a provider who can intervene if something goes wrong.
Microdosing vs standard dosing: a direct comparison
How do these approaches actually stack up against each other? Here is an honest, side-by-side comparison.
Factor | Microdosing | Standard dosing |
|---|---|---|
Starting dose | 0.25 to 1.5 mg weekly | 2.5 mg weekly |
Escalation speed | Every 4 to 12 weeks | Every 4 weeks |
Time to therapeutic dose | 3 to 6 months | 4 to 8 weeks |
Side effect severity | Generally milder | Moderate, especially early |
Nausea incidence | Lower | Higher at each increase |
Weight loss speed | Slower initially | Faster initially |
Total weight loss potential | Comparable if reaching therapeutic doses | Well-studied at 15 to 22% |
Muscle preservation | Potentially better (slower loss) | Requires active management |
Treatment adherence | Higher (fewer dropouts from side effects) | Lower (more GI-related discontinuation) |
Clinical evidence | Limited/anecdotal | Extensive (SURMOUNT trials) |
Requires compounded product | Usually yes | No (brand pens available) |
Cost | Often lower per month | Higher (full-dose products) |
Neither approach is universally better. Standard dosing has robust clinical evidence and is the medically validated path. Microdosing offers a gentler alternative for specific populations but lacks formal research validation. The right choice depends on your individual circumstances, goals, and risk tolerance. The broader dosage guide covers the full spectrum of dosing approaches for tirzepatide, and the complete dose chart provides a visual reference for every escalation pathway.
What matters most is not which approach you choose, but that you commit to it consistently, track your response carefully, and work with a qualified provider throughout the process. SeekPeptides provides comprehensive dosing protocols, tracking frameworks, and educational resources to support whichever path you take.
What to expect week by week
Timelines vary between individuals, but here is a general framework for what most people experience when microdosing tirzepatide, based on the conservative slow-start protocol.
Weeks 1 to 2 (0.5 mg)
Most people feel nothing significant. Maybe a subtle awareness of fullness after meals. Maybe slightly less interest in snacking. Or maybe nothing at all. This is normal. Remember, 0.5 mg is well below the therapeutic threshold. The purpose of these weeks is receptor priming, not dramatic results.
Possible experiences: mild fullness after large meals, occasional subtle nausea, no measurable weight change. This mirrors what many people describe during their first week on GLP-1 medications, except even more subtle at half the dose.
Weeks 3 to 4 (0.75 mg)
Still subtle. Some people begin noticing slightly reduced appetite, particularly between meals. Cravings for high-sugar or high-fat foods may begin diminishing. Appetite suppression at this stage is gentle, not dramatic.
Possible experiences: mild appetite reduction, some people report improved focus and energy from stabilized blood sugar, very modest weight change (0 to 2 pounds).
Weeks 5 to 8 (1.0 mg)
This is where most people first notice meaningful effects. Appetite reduction becomes more apparent. Portion sizes naturally decrease. Some people report feeling satisfied with less food without conscious effort. Mild GI symptoms may appear, particularly around the injection day.
Possible experiences: noticeable appetite reduction, 2 to 4 pounds of weight loss, occasional mild nausea within 24 hours of injection, reduced food noise (the constant background thoughts about food).
Weeks 9 to 12 (1.5 mg)
Effects become more consistent. Appetite suppression is sustained throughout the week rather than fading after a few days. Weight loss acceleration begins for most people. GI adaptation is usually complete by this point if you have been increasing gradually.
Possible experiences: consistent appetite suppression, 4 to 8 pounds cumulative weight loss, fewer food cravings, improved energy as the body adapts, mild side effects that are manageable. If you plateau at this stage, the plateau troubleshooting guide covers strategies that apply to all GLP-1 medications.
Weeks 13 to 16 (2.0 mg)
Approaching standard therapeutic territory. Most people feel substantial effects. Food noise is significantly reduced. Meal sizes are noticeably smaller. Weight loss is steady and measurable weekly.
Possible experiences: strong appetite regulation, 8 to 12 pounds cumulative weight loss, noticeable clothing fit changes, may experience more pronounced GI effects at this increase.
Week 17 and beyond (2.5 mg and above)
You have now reached the standard starting dose, but your body has had four months to adapt gradually instead of being thrown into the deep end. Many people report that reaching 2.5 mg through microdosing produces noticeably fewer side effects than starting there directly. From this point, you can continue standard escalation (5 mg at week 21, 7.5 mg at week 25, etc.) or maintain at whatever dose produces results that align with your goals.
For a deeper look at results timelines, the before and after guide shows real-world outcomes at various timepoints, and the male-specific results article covers gender-specific patterns.
When and how to adjust your microdose
The entire microdosing philosophy rests on responsive adjustment. You do not increase because the calendar says it is time. You increase because your data tells you that your body is ready.
Signs you are ready to increase
You have spent at least two to four weeks at the current dose with no significant side effects
Appetite suppression has plateaued or is waning
Weight loss has stalled for more than two consecutive weeks
You feel that your body has fully adapted to the current dose
Your provider agrees with escalation based on your tracking data
Signs you should stay at the current dose
Ongoing GI symptoms that have not resolved
Consistent weight loss is still occurring at the current dose
You are still adapting (energy fluctuations, appetite changes in progress)
You have not completed at least two full weeks at this dose
Signs you should decrease or pause
Severe nausea or vomiting lasting more than 48 hours
Weight loss exceeding more than 2 to 3 pounds per week consistently (too fast)
Significant fatigue or weakness that is not improving
Difficulty eating enough to meet basic nutritional needs
New or worsening symptoms that concern you
If you need to pause, do not worry about losing progress. Tirzepatide has a relatively long half-life (approximately five days), which means missing one dose does not reset everything. If you feel like tirzepatide has stopped working, that often signals either plateau (which is normal and temporary) or a need for dose adjustment, not medication failure.
The increase protocol
When you do increase, go up by one increment only. If you are at 1.0 mg, move to 1.25 mg or 1.5 mg. Do not jump to 2.5 mg. Track your response for two full weeks at the new dose before evaluating whether to increase again. Apply the same tracking framework you have been using since day one.
Storage and handling for compounded tirzepatide
Proper storage directly affects whether your medication works as intended. Compounded tirzepatide is a protein. Proteins degrade when exposed to heat, light, repeated temperature fluctuations, or bacterial contamination. Follow these guidelines without exception.
Refrigeration requirements
Store your vial in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Place it in the main body of the refrigerator, not on the door (where temperature fluctuates) and not near the back wall (where it might freeze). A vial that has been frozen should not be used, as ice crystal formation can damage the protein structure.
Unreconstituted (powder) vials have longer shelf lives than reconstituted ones. Once you add bacteriostatic water, the clock starts ticking. Most compounded tirzepatide has a beyond-use date of 30 to 45 days after reconstitution, though some formulations last longer. Check your pharmacy label for the specific timeframe.
What happens if your vial gets warm
Brief exposure to room temperature (under an hour for a single event) is generally not catastrophic. But repeated warm exposure degrades potency. If your vial has been left out of the fridge for extended periods, the medication inside may have partially degraded even though it looks normal. When in doubt, replace the vial. The cost of a new vial is trivial compared to weeks of injecting ineffective medication.
The temperature exposure guide explains exactly how long tirzepatide remains viable at various temperatures, and the broader shelf life article covers long-term storage considerations.
Contamination prevention
Every time you insert a needle through the rubber stopper, you create a potential pathway for bacteria. Minimize contamination risk by:
Always cleaning the vial top with an alcohol swab before each draw
Never touching the needle to anything except the vial stopper and your cleaned skin
Using a new syringe for every injection without exception
Never drawing from a vial that appears cloudy, discolored, or has particles floating in it
The peptide storage guide provides comprehensive handling protocols that apply to all injectable peptides, including compounded tirzepatide.
Combining microdosing with other approaches
Some people use tirzepatide microdosing alongside other strategies to optimize results. A few common combinations and their considerations:
Microdosing with B12 or B6 compounds
Many compounding pharmacies offer tirzepatide combined with vitamin B12, vitamin B6, or methylcobalamin. The B vitamins may help with energy levels and nausea management. B6 in particular has anti-nausea properties that complement the microdosing approach. The glycine and B12 compound guide covers multi-ingredient formulations in detail.
Microdosing with glycine or niacinamide
Glycine is sometimes added to compounded tirzepatide formulations for potential neuroprotective and anti-inflammatory benefits. Niacinamide (vitamin B3) is another common addition that may support metabolic function. These additions are at the discretion of the compounding pharmacy and prescribing provider.
Microdosing with exercise programs
Resistance training is critical during any tirzepatide protocol, but especially during microdosing where the gradual approach gives you more time to establish exercise habits before dramatic appetite suppression makes eating enough to fuel workouts challenging. Start a strength training program in your first few weeks at lower doses, when your appetite and energy are least affected. By the time you reach higher doses, the exercise habit will be established and your muscle preservation strategy will already be in place.
Exercise and physical activity while microdosing
Exercise is not optional when using any weight loss medication. It is the difference between losing fat and muscle (bad) versus losing primarily fat while preserving or even building muscle (good). The gradual nature of microdosing gives you a unique advantage here: you have time to establish an exercise routine before appetite suppression becomes intense enough to compromise workout fueling.
Resistance training priorities
Strength training at least three times per week is the single most important exercise recommendation for anyone on tirzepatide. Muscle preservation during caloric deficit requires a mechanical stimulus that tells the body "these muscles are being used, do not break them down for energy." Without that signal, up to 40% of weight lost can come from lean tissue rather than fat. That ratio is even worse in people who are sedentary.
You do not need a complex program. Compound movements like squats, deadlifts, presses, rows, and lunges performed with progressive overload (gradually increasing weight or reps) provide the stimulus needed. The muscle growth guide and safe muscle preservation strategies cover resistance training principles that apply directly to people on GLP-1 medications.
Cardiovascular exercise
Walking is massively underrated. Thirty to sixty minutes of daily walking improves insulin sensitivity, supports digestive motility (reducing constipation), enhances mood, and burns calories without the recovery demands of intense exercise. For people in their first weeks of microdosing, walking is the perfect complement because it does not require significant caloric fuel.
Higher-intensity cardio is fine if you enjoy it, but monitor your energy levels carefully. As tirzepatide reduces your food intake, intense exercise sessions may leave you more depleted than usual. Listen to your body. If a workout that used to feel easy suddenly feels exhausting, eat more protein and complex carbohydrates around your training sessions. The athletic performance guide covers fueling strategies for active individuals using peptide protocols.
Recovery and rest days
Your body is simultaneously adapting to a new medication and potentially losing weight. Both processes demand recovery resources. Ensure you get seven to nine hours of sleep per night. Take at least two full rest days per week. And do not ramp up exercise intensity at the same time you are increasing your tirzepatide dose. Change one variable at a time so you can attribute any changes in how you feel to the correct cause.
Alternative delivery methods for tirzepatide
While this guide focuses on injectable microdosing (the most common approach), tirzepatide is available in other forms that may interest some readers.
Sublingual drops offer a needle-free alternative, though bioavailability differs from injectable forms. Tablets and orally disintegrating tablets are emerging options with their own dosing considerations. The oral versus injection comparison helps you understand the trade-offs between delivery methods.
For injectable microdosing specifically, subcutaneous injection remains the gold standard because absorption is predictable, dosing is precise, and the clinical evidence base (such as it is) is built on this delivery method. The injectable versus oral comparison page provides a broader framework for understanding why delivery method matters for peptide bioavailability.
How tirzepatide microdosing compares to semaglutide microdosing
If you are weighing semaglutide against tirzepatide, the microdosing comparison adds another dimension. Semaglutide is a pure GLP-1 receptor agonist, while tirzepatide activates both GLP-1 and GIP receptors. At standard therapeutic doses, tirzepatide generally produces greater weight loss than semaglutide in head-to-head comparisons.
At microdose levels, the differences may be less pronounced because neither medication is fully activating its target receptors. However, tirzepatide additional GIP receptor engagement may provide earlier metabolic benefits, particularly improved insulin sensitivity, even at sub-therapeutic GLP-1 doses.
The practical microdosing process is similar for both medications: use compounded vials, calculate units from concentration, start low, increase gradually. If you are currently on semaglutide and considering switching, the conversion chart provides dosage equivalencies to help your provider plan the transition. Some people also wonder about combining both medications, though this is not a standard approach and requires careful medical supervision.
For those interested in other GLP-1 options, emerging medications like survodutide, orforglipron, and CagriSema are in various stages of development, though none currently offer the compounding flexibility needed for microdosing.
The cost angle: does microdosing save money
This comes up frequently, so let us address it directly. When using compounded tirzepatide, microdosing does use less medication per month, which can reduce costs. If a 10 mg vial costs $X and standard dosing uses 2.5 mg per week (the entire vial in a month), microdosing at 1.0 mg per week stretches that same vial to over two months.
However, consider the total timeline. If microdosing takes four months to reach the same dose you would have started at with standard dosing, and if your ultimate target dose is the same either way, the total medication cost over the full treatment period may not differ dramatically. You use less per month but use it for more months.
The real cost savings, if any, come from two scenarios. First, if you find that a lower maintenance dose achieves your goals permanently, you save on every month of ongoing treatment compared to someone maintaining on 10 or 15 mg. Second, if microdosing prevents the side-effect-related dropout that costs some people months of wasted medication plus the need to restart. The affordable tirzepatide guide and the cost calculator help you run the numbers for your specific situation. For those comparing provider options, the budget-friendly compounded tirzepatide guide reviews current pricing across multiple pharmacies.
Frequently asked questions
Can I microdose tirzepatide with brand-name pens like Mounjaro or Zepbound?
No. Brand-name pens deliver fixed doses and cannot be adjusted for microdosing. You need compounded tirzepatide in vial form with insulin syringes to draw custom amounts. The compounded dosage calculator helps you plan doses with vial formulations.
How long should I stay at each microdose level before increasing?
A minimum of two weeks, with four weeks being ideal for most people. The key is response-based advancement, not calendar-based. If side effects are still present or appetite has not stabilized at the current dose, stay longer before increasing.
Is microdosing tirzepatide FDA-approved?
No. The FDA has approved tirzepatide at doses of 2.5 mg through 15 mg. Microdosing below 2.5 mg is an off-label use that lacks clinical trial data. It should only be done under the supervision of a qualified healthcare provider.
What is the lowest effective microdose of tirzepatide?
This varies significantly between individuals. Some people report noticeable effects at 1.0 mg, while others feel nothing below 2.5 mg. Below 0.5 mg, receptor activation is unlikely to produce meaningful clinical effects for most people. Your individual response timeline depends on factors including body weight, metabolic health, and sensitivity to GLP-1 receptor activation.
Can I switch from standard dosing to microdosing?
Yes, this is the maintenance microdosing approach. After reaching your weight loss goals on standard doses, you can work with your provider to gradually taper down to a lower maintenance dose. The maintenance guide covers this transition step by step.
Will I lose weight on a microdose of tirzepatide?
At the lowest microdoses (0.25 to 0.75 mg), weight loss may be minimal or absent. As doses approach 1.0 to 2.0 mg, most people begin seeing gradual weight loss. The rate is slower than standard dosing, which is often the point. For context, the weight loss timeline shows what to expect at various dose levels.
Does microdosing tirzepatide reduce the risk of Ozempic face?
Slower weight loss may help reduce the severity of facial volume loss (sometimes called "Ozempic face" or "GLP-1 face"), because rapid fat loss contributes to skin laxity more than gradual loss. However, this has not been formally studied in the context of microdosing specifically. The hair loss guide and weight loss aesthetics discussions cover these cosmetic concerns in more detail.
Can my provider prescribe a microdose schedule?
Yes. Any licensed provider who prescribes tirzepatide can specify custom doses with compounded formulations. Bring this guide to your appointment as a starting point for discussion, and ask specifically about sub-standard starting doses with extended titration timelines.
How do I travel with compounded tirzepatide while microdosing?
Keep your vial in an insulated cooler bag with ice packs during travel. Carry your prescription documentation in case of TSA or customs questions. The travel guide for GLP-1 medications covers airline regulations, storage tips, and what to do if your vial gets warm during transit. When crossing time zones, maintain your regular injection day and approximate time rather than shifting schedules.
What if I accidentally take too much?
If you accidentally draw more than your planned microdose, do not panic. A single slightly higher dose is unlikely to cause serious harm, though you may experience more pronounced side effects that week, particularly nausea. Contact your provider, monitor your symptoms, and return to your planned dose the following week. Double-check your dose calculation before your next injection to prevent a repeat.
Should I take any supplements while microdosing tirzepatide?
At minimum, consider a daily multivitamin, magnesium (for constipation and sleep), and vitamin D if you are deficient. Electrolyte supplements help with hydration. Omega-3 fatty acids support metabolic health. Some people add glycine for its anti-inflammatory and sleep-promoting properties. Avoid supplements that claim to "boost" GLP-1 without evidence, as they add cost without proven benefit.
How do I know if microdosing is working?
Track three primary indicators: appetite changes (are you naturally eating less?), weight trend over weeks (not daily fluctuations), and side effect severity (are they manageable?). If after eight weeks at progressively increasing microdoses you see no changes in appetite or weight, discuss with your provider whether standard dosing might be more appropriate for your physiology. Some people simply need higher receptor activation to see effects. The troubleshooting guide covers additional factors that can interfere with results.
External resources
New England Journal of Medicine: Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1)
JAMA: SURMOUNT-4 Continued Treatment With Tirzepatide for Maintenance of Weight Reduction
JCI Insight: Tirzepatide Is an Imbalanced and Biased Dual GIP and GLP-1 Receptor Agonist
For researchers serious about optimizing their tirzepatide protocol, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Whether you are microdosing for the first time or stepping down to a maintenance dose after successful weight loss, SeekPeptides members get access to detailed protocol builders, dosing calculators, and expert-reviewed guidance that accounts for the individual factors most resources ignore.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay precise, your side effects stay mild, and your results stay consistent.