Feb 12, 2026

You have the vial in front of you. The syringe is drawn. And now comes the question that stops most people cold: where exactly do you put the needle? It sounds simple. It is not. The injection site you choose for retatrutide affects how quickly the peptide absorbs, how much discomfort you experience, and whether you develop long-term complications like lipodystrophy or injection site reactions. Get the site wrong, and you are wasting peptide. Get the rotation wrong, and you are building scar tissue that reduces absorption over time. Get the technique wrong, and you are creating unnecessary bruising, pain, and inconsistency in your results.
This matters more with retatrutide than with many other peptides for weight loss because of what this molecule actually is. Retatrutide is a triple-receptor agonist, the first of its kind to simultaneously activate GLP-1, GIP, and glucagon receptors. That triple mechanism delivered up to 24.2% mean body weight loss in phase 2 trials and up to 28.7% in the recently completed TRIUMPH-4 phase 3 trial. Those numbers are extraordinary. But they depend on consistent, proper subcutaneous delivery, which starts with knowing where to inject, how to rotate, and what to avoid. SeekPeptides has compiled everything the clinical literature and experienced researchers have learned about retatrutide injection sites into this single, comprehensive guide.
What follows covers the three primary injection sites in detail, the science behind absorption differences between sites, step-by-step injection technique, a complete rotation schedule you can follow week by week, troubleshooting for common injection site problems, and the specific considerations that make retatrutide administration different from other GLP-1 receptor agonists. Whether you are working with a healthcare provider or managing your own retatrutide dosing protocol, this guide ensures you are administering correctly every single time.
Understanding retatrutide and why injection site matters
Before discussing where to place the needle, understanding what retatrutide does in your body explains why injection site selection is not arbitrary. Retatrutide (LY3437943) is a single peptide molecule engineered by Eli Lilly to activate three distinct hormone receptors simultaneously. The retatrutide dosage chart exists because each receptor activation contributes differently to the overall effect, and consistent delivery ensures all three pathways activate as intended.
The GLP-1 receptor activation suppresses appetite, slows gastric emptying, and enhances insulin secretion. The GIP receptor activation amplifies the metabolic signal and may contribute to fat mobilization from adipose tissue. The glucagon receptor activation, the piece that makes retatrutide truly unique, drives energy expenditure upward, promotes lipolysis, and reduces liver fat. In the phase 2 trial published in the New England Journal of Medicine, participants on the 12mg dose saw liver fat reductions of up to 82.4%. Those are numbers that no single-agonist or dual-agonist peptide has achieved.
Why does this connect to injection sites?
Subcutaneous injection delivers the peptide into the fatty tissue layer beneath the skin. From there, it absorbs into the bloodstream at a rate determined by local blood flow, tissue composition, and the depth of the injection. Research on subcutaneous peptide pharmacokinetics demonstrates that absorption from the abdomen is approximately 28% higher in peak concentration compared to thigh injections, with the time to peak concentration occurring more than twice as fast. That difference matters when you are trying to maintain steady weekly drug levels with a peptide that has a specific retatrutide dose schedule.
Different injection sites also carry different risks. The abdomen has more subcutaneous fat in most people, making it easier to inject correctly. The thigh has variable fat distribution and more nerve endings in certain areas. The upper arm requires someone else to inject unless you have exceptional flexibility. Each site has advantages and drawbacks that experienced researchers understand and leverage strategically.
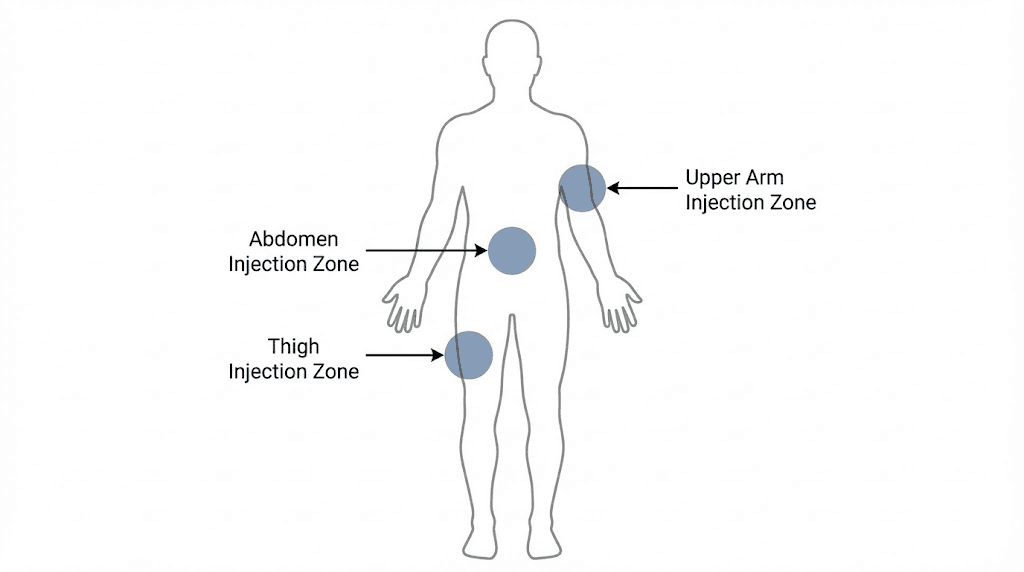
The three primary retatrutide injection sites
Clinical trials for retatrutide specified three approved injection sites: the abdomen, the anterior thigh, and the posterior upper arm. These are the same three sites used for GLP-1 injections generally, and for good reason. All three provide adequate subcutaneous tissue for proper absorption in most body types.
Let us examine each one in detail.
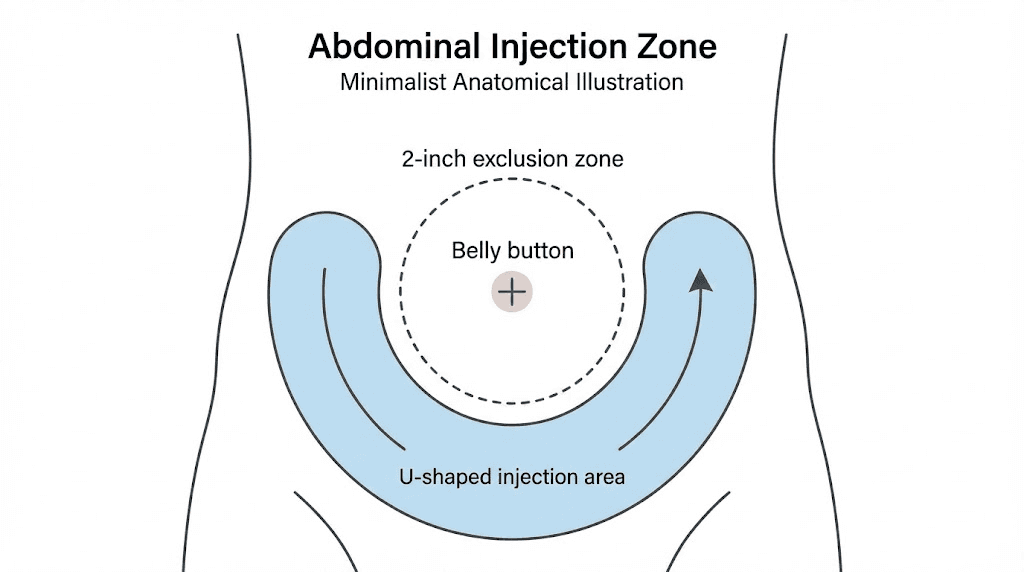
The abdomen: the preferred injection site
Most researchers and clinicians consider the abdomen the gold standard for subcutaneous peptide injection. There is a reason for that. The abdominal subcutaneous tissue has the highest blood flow of any injection site, which translates directly to faster, more consistent absorption.
The specific injection zone on the abdomen is a wide area, but it has boundaries. Stay at least 2 inches away from the navel in all directions. Avoid the waistband area where clothing friction can irritate a fresh injection site. The ideal zone forms a roughly U-shaped region below and to the sides of the navel, extending from the hip bones to the lower rib cage.
Why the abdomen absorbs fastest comes down to physiology. Abdominal subcutaneous adipose tissue blood flow (ATBF) runs consistently higher than femoral (thigh) ATBF, particularly in the post-meal state, where abdominal blood flow exceeds thigh blood flow by more than 30% for at least six hours. For a peptide like retatrutide that you inject once weekly, the initial absorption window sets the pharmacokinetic profile for the entire week. Faster, more complete absorption from the abdomen means more predictable blood levels and more consistent results.
The abdomen also provides the largest total injection area of any site. A typical adult has enough abdominal surface to support 15 to 20 distinct injection points spaced at least 1.5 inches apart. That gives you roughly four to five months of weekly injections without revisiting the same spot, assuming you use the abdomen exclusively. When combined with rotation to other sites, you effectively eliminate the risk of tissue damage from repeated injections.
For people following the standard retatrutide dosage chart for weight loss, the abdomen is the recommended starting site. It is the easiest to access for self-injection. It provides the most forgiving target for proper needle depth. And the absorption characteristics match what the clinical trials used, meaning your results should approximate what the studies demonstrated.
Practical tips for abdominal injection of retatrutide:
Pinch a fold of skin between your thumb and forefinger, pulling the tissue away from the abdominal wall
Insert the needle at a 45 to 90 degree angle depending on the amount of subcutaneous fat (more fat = steeper angle is fine)
Inject slowly over 5 to 10 seconds
Hold the needle in place for 5 seconds after injection before withdrawing
Do not massage the area after injection, this can alter absorption rate
Rotate at least 1.5 inches from the previous injection site
The anterior thigh: the reliable alternative
The front of the thigh provides an excellent alternative injection site, particularly for people who find abdominal injections uncomfortable or who need to rotate away from the abdomen to allow tissue recovery. The injection zone on the thigh runs from about 4 inches above the knee to 4 inches below the groin crease, on the outer front portion of the thigh.
Thigh injections absorb more slowly than abdominal injections. The research on subcutaneous peptide pharmacokinetics confirms that peak concentration (Cmax) from thigh injection is roughly 28% lower than from abdominal injection, and the time to reach that peak is more than twice as long. For some applications, this slower absorption is actually beneficial. With insulin, for example, slower thigh absorption is preferred for basal insulin because it creates a more gradual, sustained effect. With retatrutide, the clinical significance of this absorption difference has not been specifically studied, but experienced researchers note that thigh injections tend to produce a slightly more gradual onset of appetite suppression compared to abdominal injections.
The thigh has some practical advantages. It is visible and accessible for self-injection without needing a mirror. The muscle beneath the fat layer provides a firm base that makes needle insertion straightforward. And the total injection area on both thighs combined is substantial, providing another 10 to 15 distinct injection points per thigh.
One consideration specific to the thigh: exercise affects absorption. Physical activity increases blood flow to the thighs dramatically, which can accelerate absorption beyond what you expect. If you typically inject in the morning and exercise later in the day, this may not matter much. But injecting into the thigh immediately before a leg workout could potentially create a faster-than-intended absorption spike. Researchers who follow careful retatrutide peptide dosage charts account for this by separating injection and exercise by at least 2 hours.
Practical tips for thigh injection of retatrutide:
Sit down with your leg relaxed and slightly extended
Choose the outer front portion of the thigh, avoiding the inner thigh entirely
Pinch the skin if you have less subcutaneous fat in this area
Insert the needle at a 45 degree angle for leaner individuals, 90 degrees for those with more tissue
Alternate between left and right thigh each week at minimum
Avoid injecting within 4 inches of the knee or the groin
The posterior upper arm: the clinical favorite
The back of the upper arm is the third approved injection site for retatrutide. It sits in the triceps area, on the fleshy portion between the shoulder and the elbow. Clinical settings often prefer this site because it is easily accessible by a healthcare provider and typically has adequate subcutaneous tissue even in leaner individuals.
For self-injection, the upper arm presents a practical challenge. You cannot easily see or reach the back of your own arm to inject with proper technique. Some researchers use their non-dominant hand to inject into the dominant arm, but this reduces control over needle angle and depth. Others ask a partner to administer the injection. If you are self-injecting retatrutide and do not have assistance, the upper arm is generally not recommended as a primary site.
Absorption from the upper arm falls between abdominal and thigh rates. Studies on subcutaneous insulin absorption demonstrate that arm injections produce a Cmax that is lower than abdominal but higher than thigh injections. The time to peak concentration is similarly intermediate. This makes the upper arm a reasonable rotation site when the abdomen needs a break and the thighs have been recently used.
The total injection area on each upper arm is smaller than the abdomen or thigh, providing perhaps 4 to 6 distinct injection points per arm. This limits its utility as a primary site but makes it valuable as part of a comprehensive rotation schedule.
Practical tips for upper arm injection of retatrutide:
Have a partner administer the injection if possible
Target the fleshy area on the back of the arm, midway between shoulder and elbow
Avoid the shoulder joint and the bony area near the elbow
If self-injecting, press the back of the arm against a wall to create a stable surface
Use a 45 degree needle angle for most arm injections
Alternate between left and right arms
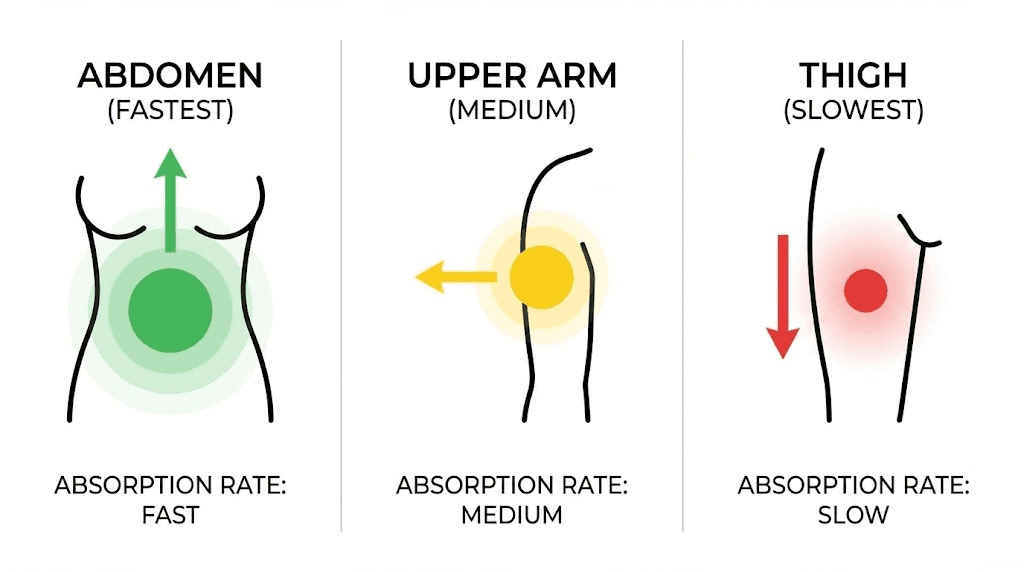
Injection site absorption rates compared
Choosing the right injection site requires understanding the pharmacokinetic differences between sites. The following comparison draws from published research on subcutaneous peptide absorption and represents what experienced researchers consider when planning their retatrutide dose administration.
Injection site | Relative absorption speed | Peak concentration (Cmax) | Time to peak (Tmax) | Best for | Self-injection ease |
|---|---|---|---|---|---|
Abdomen | Fastest | Highest (baseline) | Shortest | Primary site, consistent results | 9/10 |
Upper arm | Intermediate | Moderate (10-15% lower) | Moderate | Rotation site, clinical settings | 4/10 |
Anterior thigh | Slowest | Lowest (up to 28% lower) | Longest (2x abdomen) | Rotation site, sustained release | 8/10 |
These differences are clinically established for insulin and other subcutaneous peptides. While retatrutide-specific absorption comparison data across sites has not been published separately from the clinical trials (which used all three sites), the pharmacokinetic principles that govern subcutaneous absorption apply universally to peptides of similar molecular weight and formulation.
The practical implication is straightforward. If you want the most consistent, predictable retatrutide experience that matches what was studied in clinical trials, use the abdomen as your primary site and rotate to the thigh or arm periodically. If you find abdominal injections uncomfortable or if you are developing tissue irritation at abdominal sites, the thigh provides a reliable alternative with slightly different absorption characteristics.
For researchers comparing retatrutide to other peptides, the absorption principles are the same ones that apply to tirzepatide reconstitution and injection, semaglutide dosing, and other subcutaneous peptide therapies. The site matters. The technique matters. And consistency matters most of all.
Complete site rotation schedule
Site rotation is not optional. Repeated injection at the same location causes lipohypertrophy, a thickening of the subcutaneous fat tissue that creates firm lumps under the skin. These lumps are not just cosmetic. They reduce absorption unpredictably, meaning your carefully calculated retatrutide dosage may not be delivering what you think it is delivering.
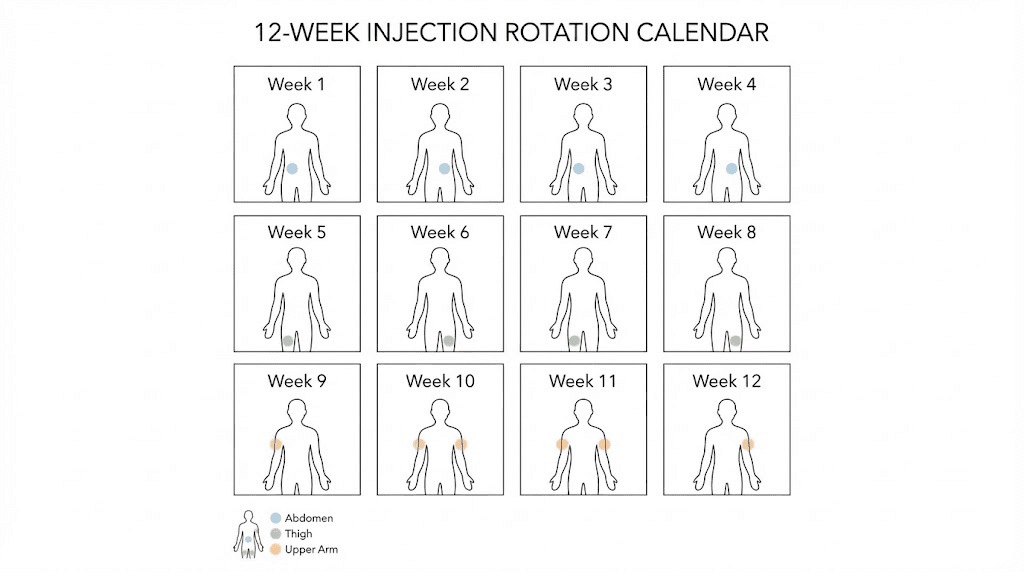
A complete rotation schedule uses all available sites systematically. Here is a proven 12-week rotation that maximizes tissue recovery time while maintaining consistent administration.
The 12-week rotation protocol
Week 1: Right abdomen, upper quadrant (above navel, right side)
Week 2: Left abdomen, upper quadrant (above navel, left side)
Week 3: Right anterior thigh, upper portion
Week 4: Right abdomen, lower quadrant (below navel, right side)
Week 5: Left abdomen, lower quadrant (below navel, left side)
Week 6: Left anterior thigh, upper portion
Week 7: Right abdomen, lateral (right side, toward hip)
Week 8: Left abdomen, lateral (left side, toward hip)
Week 9: Right anterior thigh, lower portion
Week 10: Right upper arm (if partner available) or right abdomen central
Week 11: Left anterior thigh, lower portion
Week 12: Left upper arm (if partner available) or left abdomen central
After week 12, restart the cycle. Each site has had at least 11 weeks of recovery before you return to it, which is more than adequate for complete tissue healing.
Why this rotation works
The schedule front-loads abdominal injections because the abdomen provides the most consistent absorption and the largest injection area. Thigh injections are spaced every 3 to 4 weeks. Upper arm injections appear only twice per cycle and are optional for self-injectors. The pattern ensures no single site receives more than one injection per 12-week cycle while keeping the majority of injections in the highest-absorption zone.
Researchers who use this rotation alongside their retatrutide dose schedule report consistent results without the tissue complications that come from less structured rotation. If you are also reconstituting retatrutide from research vials, maintaining a consistent injection schedule is doubly important because reconstituted peptides have a limited stability window.
Keep a simple log. Write down the date, the site used, and any observations (redness, bruising, pain level). This log becomes invaluable if you develop a site reaction and need to identify which location caused it. SeekPeptides members access tracking tools that make this logging process automatic, but a simple notebook or phone note works fine.
Step-by-step injection technique
Proper technique prevents most injection site problems. Whether you are using a pre-filled pen or drawing from a reconstituted vial with a syringe, the fundamental technique remains the same for subcutaneous delivery. The following applies specifically to retatrutide but mirrors best practices for all subcutaneous peptide injections, including those outlined in our peptide injection guide.
Before the injection
Step 1: Prepare the medication. If your retatrutide requires reconstitution, follow the retatrutide reconstitution chart to mix with bacteriostatic water. If using a pre-filled pen, simply remove the cap. Allow the medication to reach room temperature by removing it from the refrigerator 15 to 30 minutes before injection. Cold injections are more painful and may absorb differently.
Step 2: Gather supplies. You need alcohol wipes, the syringe or pen, a sharps disposal container, and optionally a bandage. Wash your hands thoroughly with soap and water.
Step 3: Select and clean the injection site. Choose your site based on the rotation schedule. Wipe the area with an alcohol swab in a circular motion, moving outward from the center point. Allow the alcohol to dry completely. Injecting through wet alcohol introduces irritation and stinging.
During the injection
Step 4: Prepare the skin. For most people, pinching a fold of skin between the thumb and index finger creates a clear target and ensures the needle reaches subcutaneous tissue rather than muscle. If you have substantial subcutaneous fat at the injection site (more than an inch when pinched), you may not need to pinch, just inject directly at a 90 degree angle.
Step 5: Insert the needle. Hold the syringe like a pencil or dart. Insert smoothly at a 45 to 90 degree angle depending on the amount of subcutaneous tissue. Do not hesitate or insert slowly, a quick, confident insertion is less painful. The needle should pass through the skin and enter the fatty tissue beneath. If using an insulin syringe (29 to 31 gauge), you should feel minimal resistance.
Step 6: Inject the medication. Push the plunger slowly and steadily. A full dose should take 5 to 10 seconds to inject. Injecting too quickly increases pressure on the tissue and causes more post-injection discomfort. If using a pen, hold the injection button for the full recommended time (usually 5 to 10 seconds) after the dose counter reaches zero.
Step 7: Wait and withdraw. After the plunger is fully depressed or the pen has delivered the full dose, count to 5 while keeping the needle in place. This allows the medication to disperse into the tissue and prevents it from leaking back through the needle track. Then withdraw the needle at the same angle you inserted it.
After the injection
Step 8: Apply gentle pressure. Press the alcohol swab or a cotton ball gently against the injection site for 10 to 15 seconds. Do not rub or massage. Rubbing can push medication into different tissue layers and alter absorption.
Step 9: Dispose properly. Place the used needle immediately into a sharps container. Never recap a used needle. Never dispose of needles in regular trash.
Step 10: Log the injection. Record the date, time, site used, dose administered, and any observations. This data helps you maintain your rotation schedule and identify patterns if problems develop.
The entire process takes about 2 to 3 minutes once you are practiced. New researchers often take 5 to 10 minutes as they build confidence with the technique. That is completely normal. Speed comes with repetition. Focus on technique first, efficiency second.
Needle selection for retatrutide injection
The needle you use affects comfort, absorption, and injection accuracy. For subcutaneous retatrutide injection, the ideal needle specifications are:
Gauge: 27 to 31 gauge. Higher gauge numbers mean thinner needles. A 29 or 30 gauge needle is the sweet spot for most people, thin enough to minimize pain but sturdy enough to penetrate skin without bending. Insulin syringes typically come in 29 to 31 gauge and work perfectly for retatrutide.
Length: 1/4 inch to 1/2 inch (6mm to 12.7mm). For subcutaneous injection, you do not want a long needle. The goal is to reach the fatty layer beneath the skin, not the muscle beneath the fat. A 1/2 inch needle at a 45 degree angle deposits medication approximately 8mm deep, which is ideal for most people. Leaner individuals should use shorter needles or shallower angles to avoid intramuscular injection.
Syringe volume: 0.3mL to 1mL syringes work for most retatrutide doses. The smaller the syringe, the easier it is to read precise volumes. If your dose is 0.5mL or less, a 0.5mL syringe provides the best accuracy with clear graduation marks.
For researchers using the peptide calculator to determine their injection volume based on concentration and target dose, matching the syringe volume to the expected injection volume ensures the most accurate measurement.
Common injection site problems and solutions
Even with perfect technique, injection site issues occasionally develop. Knowing what to expect and how to respond prevents minor issues from becoming serious problems. This troubleshooting section covers the most common injection site complications reported with subcutaneous peptide injections, including those specific to retatrutide.
Bruising
Small bruises at injection sites are common and almost always harmless. They occur when the needle nicks a small blood vessel during insertion. Bruising happens more frequently when you inject into areas with visible veins, when you are taking blood-thinning medications or supplements (fish oil, aspirin, vitamin E), or when you apply pressure before the needle is fully withdrawn.
Solution: Apply gentle pressure for 30 to 60 seconds after withdrawing the needle. Avoid the specific spot for future injections until the bruise resolves. If you bruise consistently at one site, adjust your aim by half an inch. No treatment is necessary, bruises resolve on their own within 1 to 2 weeks.
Redness and warmth
Mild redness at the injection site lasting 30 minutes to a few hours is a normal tissue reaction. The alcohol prep, the needle insertion, and the fluid volume all contribute to local irritation. This is different from an allergic or immune reaction, which would involve spreading redness, significant swelling, and possibly hives.
Solution: Redness that stays localized and resolves within 24 hours requires no treatment. A cool compress can reduce discomfort. If redness spreads beyond 2 inches from the injection site, lasts more than 48 hours, or is accompanied by warmth, swelling, or drainage, contact a healthcare provider. These could indicate infection or a significant reaction.
Small lumps or nodules
Occasionally, a small lump forms at the injection site. This is usually a localized accumulation of the injected fluid in the subcutaneous tissue. It resolves as the medication absorbs over the following hours. Persistent lumps that last weeks or months, however, may indicate lipohypertrophy from repeated injection at the same site.
Solution: Temporary lumps need no treatment. If lumps persist, review your rotation schedule. You may be injecting too close to a previous site. Increase the distance between injection points to at least 2 inches. Never inject into a lumpy area, absorption from these sites is unpredictable.
Pain during injection
Some discomfort is expected with any injection. However, significant pain usually indicates a technical problem rather than a medication issue. Common causes include injecting cold medication, using a dull or bent needle, injecting too quickly, hitting a nerve, or injecting into muscle rather than fat.
Solution: Always warm medication to room temperature before injection. Use a new needle for every injection (never reuse). Inject slowly over 5 to 10 seconds. If you feel a sharp, electric pain, you may have contacted a nerve. Withdraw and try a spot half an inch away. If pain persists after every injection regardless of technique, consult a healthcare provider.
Itching at injection site
Mild itching around the injection site is relatively common with GLP-1 receptor agonists. In the retatrutide phase 2 clinical trials, injection site reactions were reported but were not significantly higher than placebo, and the vast majority were classified as mild. Itching typically resolves within a few hours to a day.
Solution: Avoid scratching, which can introduce bacteria. A cool compress or over-the-counter hydrocortisone cream can help. If itching is severe or accompanied by hives away from the injection site, seek medical attention, this could indicate a systemic allergic reaction.
Retatrutide vs. other GLP-1 injections: site considerations
If you have experience injecting semaglutide, tirzepatide, or other GLP-1 receptor agonists, most of that knowledge transfers directly to retatrutide. The injection sites, technique, and rotation principles are identical because all of these medications are delivered subcutaneously. However, there are a few retatrutide-specific considerations worth noting.
First, retatrutide is a larger molecule that activates three receptors instead of one or two. In practical terms, this does not change where you inject. But it does mean that consistent delivery is arguably more important, because inconsistent absorption could affect the balance of receptor activation. If one injection absorbs 28% less efficiently because you used a thigh site instead of the abdomen, the relative activation of GLP-1, GIP, and glucagon receptors might shift slightly. Whether this has clinical significance is unknown, but researchers who track their results closely often notice more consistent appetite suppression and energy levels when they maintain consistent injection sites.
Second, the cost of retatrutide makes waste prevention a priority. Every injection that leaks, absorbs poorly, or hits muscle instead of fat represents lost money and lost results. Proper technique at the right injection site minimizes waste. This is why experienced researchers invest time in learning correct technique rather than rushing through the process.
Third, for researchers who are comparing protocols between different peptides, the injection site considerations discussed here apply equally to retatrutide vs. semaglutide comparisons, retatrutide vs. tirzepatide dosage evaluations, and any other subcutaneous peptide. The pharmacokinetic principles of subcutaneous absorption do not change based on the drug. The injection site, technique, and rotation schedule are universal.
Special situations and considerations
Injecting during weight loss
As you lose weight on retatrutide, your body composition changes. Areas that previously had substantial subcutaneous fat may become leaner, which affects injection technique. The abdomen typically retains adequate subcutaneous tissue longest, but the thighs and arms may require technique adjustments as you progress.
If you can no longer pinch a full inch of tissue at a site, switch to a shallower injection angle (30 to 45 degrees instead of 90 degrees) and use a shorter needle. This prevents the needle from reaching muscle tissue, which changes absorption characteristics and increases pain. Researchers following the retatrutide weight loss protocol should reassess their injection sites every 4 to 6 weeks as their body composition changes.
Injecting with skin conditions
Never inject into areas with active skin conditions, including eczema, psoriasis, sunburn, rash, open wounds, or recent tattoos. These areas have altered blood flow and compromised skin barriers that increase infection risk and unpredictable absorption. If a skin condition develops at a preferred injection site, rotate to an unaffected area and allow the condition to resolve completely before returning.
Injecting in hot vs. cold environments
Temperature affects both the medication and your body. Hot environments increase subcutaneous blood flow, potentially accelerating absorption. Cold environments constrict blood vessels and slow absorption. For the most consistent results, inject in a temperature-controlled environment when possible. If you must inject in extreme temperatures, the abdomen is the most temperature-stable injection site because core body temperature fluctuates less than extremity temperature.
Injection timing within the week
Retatrutide is administered once weekly, and the dose schedule recommends injecting on the same day each week. There is no strong evidence that time of day significantly affects absorption, but many researchers prefer morning injections. Morning administration allows any initial nausea (a common side effect during dose escalation) to occur during waking hours rather than disrupting sleep. Morning injection also means the initial peak absorption coincides with daytime activity levels rather than sedentary sleep hours.
If you miss your scheduled injection day, administer the injection as soon as you remember, as long as the next scheduled dose is at least 3 days away. If the next dose is less than 3 days away, skip the missed dose and resume on schedule. Never double-dose to compensate for a missed injection. This applies to all GLP-1 receptor agonist protocols, not just retatrutide.
Supplies checklist for retatrutide injection
Having the right supplies on hand before your injection ensures a smooth, safe experience. Here is the complete list:
Essential supplies:
Retatrutide medication (stored properly per the peptide storage guidelines)
Insulin syringes (29-31 gauge, 1/2 inch needle) or prescribed pen device
Alcohol prep pads
Sharps disposal container
Clean, flat surface for preparation
Recommended supplies:
Injection log (notebook, app, or spreadsheet)
Cotton balls or gauze pads
Adhesive bandages
Timer or clock (for medication warming and injection timing)
For reconstitution (if applicable):
Mixing syringe (separate from injection syringe)
Alcohol wipes for vial tops
Peptide reconstitution calculator for accurate dilution
Never reuse syringes. Never share needles. Always dispose of sharps properly. These are non-negotiable safety principles that apply to every injection, every time.

What the clinical trials tell us about injection sites
The landmark phase 2 trial for retatrutide, published in the New England Journal of Medicine (Jastreboff et al., 2023), enrolled 338 adults with obesity. Participants received weekly subcutaneous injections of retatrutide at doses of 1mg, 4mg, 8mg, or 12mg, or placebo. The study protocol specified abdomen, thigh, or upper arm as injection sites, with rotation required.
Key findings relevant to injection site safety:
Injection site reactions were not significantly higher in retatrutide groups compared to placebo
The most common injection site reactions were transient redness and mild discomfort
No participants discontinued due to injection site reactions
The overall safety profile was consistent with other GLP-1 receptor agonists
The more recent TRIUMPH-4 phase 3 trial confirmed these safety findings in a larger population. With up to 28.7% mean weight loss and up to 71.2 pounds average weight reduction at the highest dose, retatrutide delivered the most impressive weight loss results of any obesity medication studied to date, and injection site complications remained minimal throughout.
For researchers tracking the retatrutide availability timeline, the compound is currently in multiple phase 3 trials with results expected throughout the coming period. Proper injection technique learned now will serve you well as the compound progresses through the regulatory process.
Advanced injection tips from experienced researchers
Researchers who have administered hundreds of subcutaneous injections develop practical insights that go beyond textbook technique. Here are tips from the experienced community that can make your retatrutide injections more comfortable and effective.
Ice the site first. Applying an ice cube or cold pack to the injection site for 30 to 60 seconds before injecting numbs the area slightly. This is especially helpful for people who are sensitive to needle insertion. The cold constricts local blood vessels, which also reduces bruising risk. Remove the ice, wipe with alcohol, let the alcohol dry, then inject.
Breathe out as you inject. Tensing up during injection tightens the subcutaneous tissue and increases pain. Exhaling slowly during needle insertion relaxes the tissue. Some researchers practice a simple breathing pattern: inhale deeply, begin exhaling, insert needle during the exhale, continue slow breathing while injecting.
Alternate dominant and non-dominant hand. If you always inject with your dominant hand, you limit yourself to sites on the opposite side of your body. Practicing injection with both hands opens up more sites for rotation and prevents you from overusing one area.
Mark your sites. Use a washable marker or small adhesive dot to mark the exact injection point before each injection. This prevents the common mistake of injecting too close to a previous site. Some researchers mark 4 to 6 potential sites at the beginning of each month and rotate through them systematically.
Track absorption consistency. If you notice significant variation in appetite suppression or GI side effects week to week, your injection site rotation might be the variable. Keep notes on which site you used each week alongside how you felt. Over time, patterns emerge that help you optimize your site selection. This is particularly valuable for researchers managing retatrutide side effects during the dose escalation phase.
Warm the medication properly. Never microwave peptides. Never use hot water. Simply remove the vial or pen from the refrigerator and set it on the counter for 15 to 30 minutes. You can roll the vial gently between your palms to warm it slightly faster. Room temperature medication is less viscous, flows more smoothly through the needle, and causes less tissue irritation upon injection.
Building a retatrutide injection routine
Consistency is the backbone of effective peptide administration. Building a routine around your weekly retatrutide injection makes it automatic rather than something you need to think about each time. Here is a framework that experienced researchers use.
Choose your day. Pick a day of the week that works consistently with your schedule. Many researchers choose Sunday evenings or Monday mornings, as these are typically predictable days. Once you pick a day, stick with it. Retatrutide works best with consistent weekly timing.
Choose your time. Morning injections are popular because they align with the daily routine and allow you to monitor for side effects during waking hours. However, evening injections work fine too. The key is consistency, not the specific hour.
Set up your station. Keep all injection supplies in one designated location. A clean drawer, a small case, or a specific shelf in the refrigerator for the medication. When everything is in one place, the injection process flows smoothly and you never find yourself hunting for an alcohol wipe mid-procedure.
Follow the same sequence every time. Remove medication from fridge. Set timer for 15 minutes. Gather supplies. When timer sounds, wash hands, prep site, draw medication, inject, log. The same sequence every week builds muscle memory and reduces errors.
For researchers also using other peptides alongside retatrutide, peptide stacking considerations may affect your injection scheduling and site selection. Different peptides should be injected at different sites to prevent interaction at the tissue level and to allow independent absorption.
Frequently asked questions
Can I inject retatrutide in my buttocks?
The buttocks are not one of the three sites specified in retatrutide clinical trials. While the buttocks have adequate subcutaneous tissue, the difficulty of self-injection in this area and the lack of clinical data supporting this site mean it is not recommended. Stick with the abdomen, thigh, or upper arm for consistency with the studied protocol.
Does the injection site affect how well retatrutide works?
Injection site affects absorption rate and peak concentration but does not fundamentally change how the medication works. The abdomen delivers the fastest, highest peak. The thigh delivers a slower, lower peak. Both sites ultimately deliver the full dose into your bloodstream. The clinical significance of these differences for retatrutide specifically has not been studied, but experienced researchers report the most consistent results with abdominal injections following the standard dosage protocol.
How far apart should injection sites be?
Maintain at least 1.5 inches (approximately 4 centimeters) between injection sites. This distance ensures you are injecting into fresh tissue each time. Some conservative protocols recommend 2 inches between sites. Use whichever standard allows you to maintain adequate rotation across your available injection area.
Can I inject retatrutide and other peptides at the same site?
Different medications should be injected at different sites, separated by at least 2 inches. This prevents local tissue interaction and ensures each medication absorbs independently. If you are taking multiple peptides, plan your rotation schedule to accommodate all of them without overlap.
What if I accidentally inject into muscle?
Intramuscular injection of retatrutide is not dangerous, but it changes the absorption profile. Muscle tissue has higher blood flow than subcutaneous fat, which means the medication absorbs faster and may produce a higher, shorter peak. This can increase side effects like nausea. If you suspect an intramuscular injection (deeper pain, faster onset of effects), do not panic. Simply note it in your log and use a shallower angle or shorter needle at that site next time.
Should I inject retatrutide near my workout injection site for BPC-157 or other healing peptides?
No. Keep different peptide injection sites separated by at least 2 inches. BPC-157 and similar healing peptides are often injected locally near an injury site, while retatrutide should be injected in standard subcutaneous zones regardless of other medications. Mixing injection sites risks altering the absorption of both compounds.
Is it normal for retatrutide to sting during injection?
Mild stinging is common with most subcutaneous injections. Cold medication stings more. Acidic or alkaline solutions sting more. If the sting is brief (a few seconds) and resolves quickly, it is normal. If the stinging is severe or persists for hours, the medication may have degraded, the pH may be off, or you may have a sensitivity. Consult your healthcare provider if persistent stinging occurs.
Can I use an auto-injector or pen for retatrutide?
Eli Lilly is developing a pre-filled pen for retatrutide, similar to the Mounjaro pen for tirzepatide. Pre-filled pens automate much of the injection process, selecting the correct dose and delivering it through a hidden needle at the press of a button. If you have access to a pen device, follow the manufacturer instructions for injection site selection and rotation, which align with the guidelines in this article.
External resources
For researchers serious about optimizing their retatrutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed injection technique videos, personalized dosage calculators, and expert-reviewed protocols that go far beyond what any single article can cover.
In case I do not see you, good afternoon, good evening, and good night. May your injection sites stay rotation-fresh, your absorption stay consistent, and your retatrutide results stay on track.