Jan 9, 2026

Visceral fat is not just stubborn. It is dangerous.
This fat wraps around your liver, pancreas, and intestines. It pumps inflammatory cytokines into your bloodstream. It drives insulin resistance. It elevates cardiovascular disease risk. And it resists the diet and exercise strategies that work on subcutaneous fat.
You can lose weight. You can see the number on the scale drop. But that deep belly fat, the visceral adipose tissue that truly threatens your health, often remains stubbornly in place. This frustrating reality has driven researchers to investigate peptide-based interventions that specifically target visceral fat through mechanisms diet and exercise cannot fully address.
The research is compelling. Certain peptides demonstrate preferential effects on visceral fat stores. Tesamorelin holds FDA approval specifically for reducing visceral adiposity. Growth hormone secretagogues shift body composition toward lean mass. GLP-1 agonists produce dramatic reductions in abdominal fat. The mechanisms are understood well enough to design rational protocols.
This guide examines every peptide with documented research relevant to visceral fat reduction. We cover the molecular mechanisms, review available studies, discuss practical protocols, and help you understand which compounds merit serious investigation for targeting this metabolically dangerous fat depot.
SeekPeptides provides personalized protocols for body composition optimization tailored to individual goals and metabolic profiles.
Understanding visceral fat and why it matters
Before examining specific peptides, understanding what makes visceral fat uniquely problematic explains why targeted interventions matter.
Visceral versus subcutaneous fat
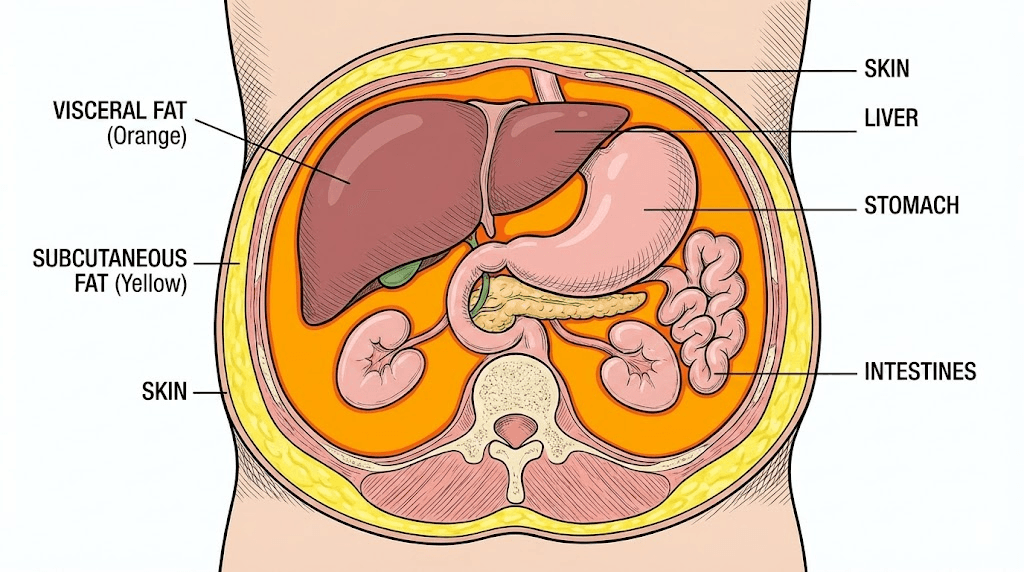
Your body stores fat in two primary locations. Subcutaneous fat sits beneath the skin, the fat you can pinch on your belly, thighs, and arms. Visceral fat accumulates deep within the abdominal cavity, surrounding and infiltrating organs.
These fat depots differ dramatically in their metabolic behavior. Subcutaneous fat functions primarily as energy storage. It releases fatty acids when needed and generally behaves in metabolically benign ways. Many people carry substantial subcutaneous fat without significant metabolic consequences.
Visceral fat behaves differently. This fat depot is metabolically hyperactive, constantly releasing compounds that influence the entire body. The liver receives these compounds directly through the portal circulation, meaning visceral fat has outsized effects on hepatic function.
Understanding this distinction explains why two people at identical weights can have vastly different health profiles. One carries mostly subcutaneous fat and remains metabolically healthy. The other carries substantial visceral fat and shows early signs of metabolic syndrome despite normal BMI.
The inflammatory cascade
Visceral fat functions almost like an endocrine organ, secreting inflammatory cytokines, hormones, and signaling molecules that affect tissues throughout the body.
Key compounds released by visceral fat include interleukin-6, an inflammatory cytokine linked to cardiovascular disease and insulin resistance. Tumor necrosis factor alpha drives inflammation and impairs insulin signaling. Resistin directly promotes insulin resistance. Plasminogen activator inhibitor-1 increases clotting risk. These compounds create a chronic inflammatory state that damages blood vessels, impairs glucose metabolism, and increases disease risk.
The more visceral fat you carry, the more of these harmful compounds enter your circulation. This explains the strong association between visceral adiposity and conditions including type 2 diabetes, cardiovascular disease, fatty liver disease, and certain cancers.
Why visceral fat resists traditional approaches
Diet and exercise reduce total body fat, but visceral fat often proves stubborn for several reasons.
Hormonal factors play a major role. Cortisol, the stress hormone, preferentially promotes visceral fat accumulation. Modern lifestyles characterized by chronic stress, poor sleep, and constant stimulation keep cortisol elevated, encouraging visceral fat deposition even when caloric intake is controlled.
Insulin resistance creates a vicious cycle. Visceral fat causes insulin resistance, and insulin resistance promotes further visceral fat accumulation. Breaking this cycle requires addressing the underlying metabolic dysfunction, not just reducing calories.
Age-related hormonal changes compound the problem. Declining growth hormone, testosterone in men, and estrogen in women all shift fat distribution toward the visceral depot. These changes explain why visceral fat accumulation accelerates after age 40 even in people who maintain stable weight.
Peptides enter this picture because certain compounds address these underlying mechanisms directly. Rather than simply creating caloric deficit, they target the hormonal and metabolic factors that determine where fat is stored and released.
The peptides for fat loss page provides additional context on fat metabolism peptides.
Tesamorelin: the FDA-approved visceral fat reducer
Tesamorelin stands alone among peptides with FDA approval specifically for reducing visceral adipose tissue. Originally approved for HIV-associated lipodystrophy, the peptide's effects on visceral fat have broader implications for metabolic health research.
Mechanism of action
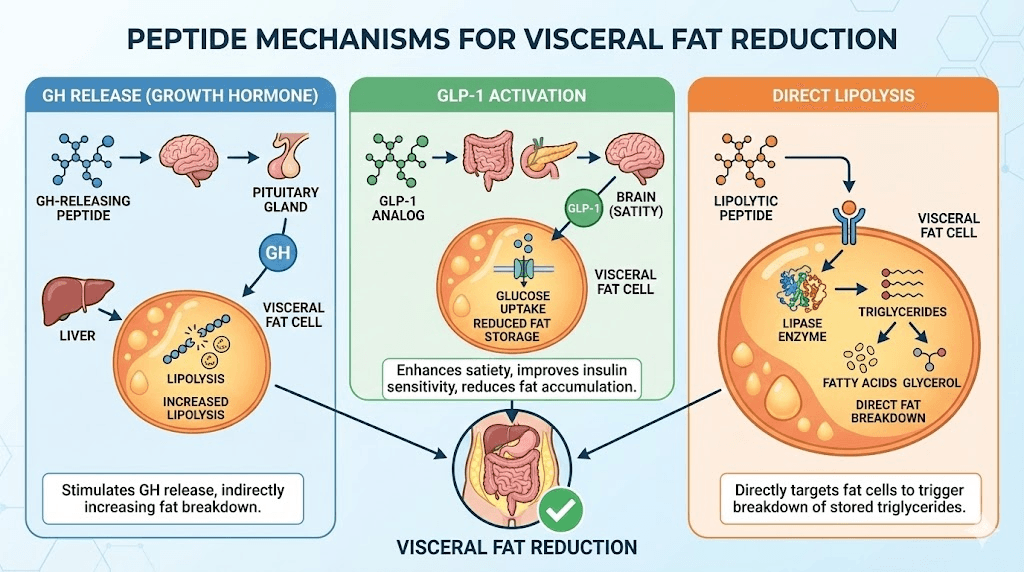
Tesamorelin is a growth hormone releasing hormone analog. It stimulates the pituitary gland to release growth hormone in a physiological pulsatile pattern, mimicking natural GH secretion rather than providing continuous exogenous hormone.
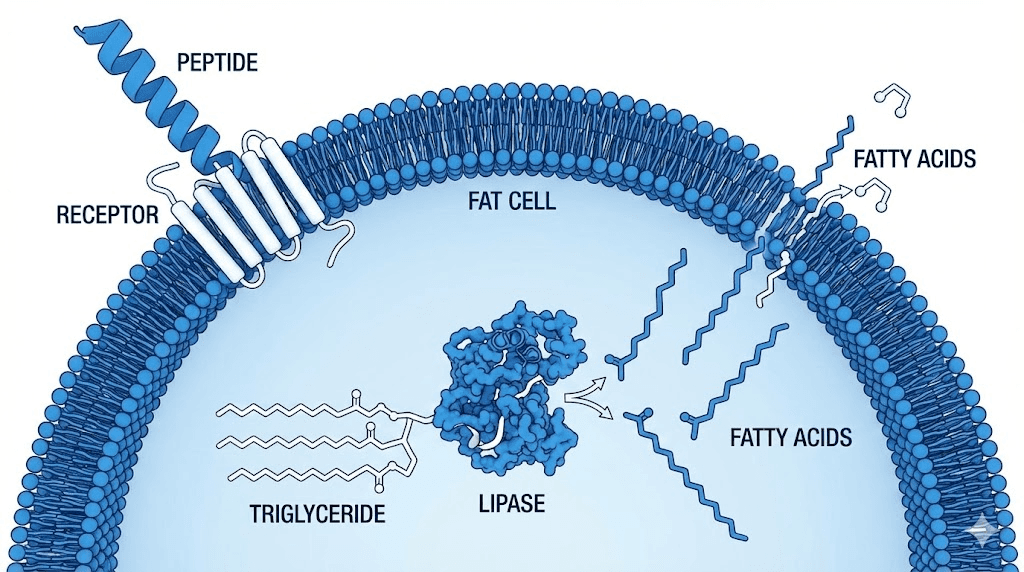
Growth hormone influences fat metabolism through multiple pathways. It promotes lipolysis, the breakdown of stored triglycerides into free fatty acids. It shifts substrate utilization toward fat oxidation. It preserves lean muscle mass during caloric restriction. And crucially, growth hormone appears to preferentially mobilize visceral fat stores.
The preferential effect on visceral fat relates to receptor distribution and local hormone sensitivity. Visceral adipocytes have higher concentrations of growth hormone receptors and greater responsiveness to GH signaling compared to subcutaneous fat cells. When GH levels rise, visceral fat responds more dramatically.
Tesamorelin also influences hepatic function. By reducing visceral fat burden, it decreases the inflammatory and metabolic load on the liver. Studies show improvements in liver fat content and markers of hepatic function alongside visceral fat reduction.
Clinical evidence
Tesamorelin has been evaluated in multiple controlled clinical trials, providing stronger evidence than exists for most peptides.
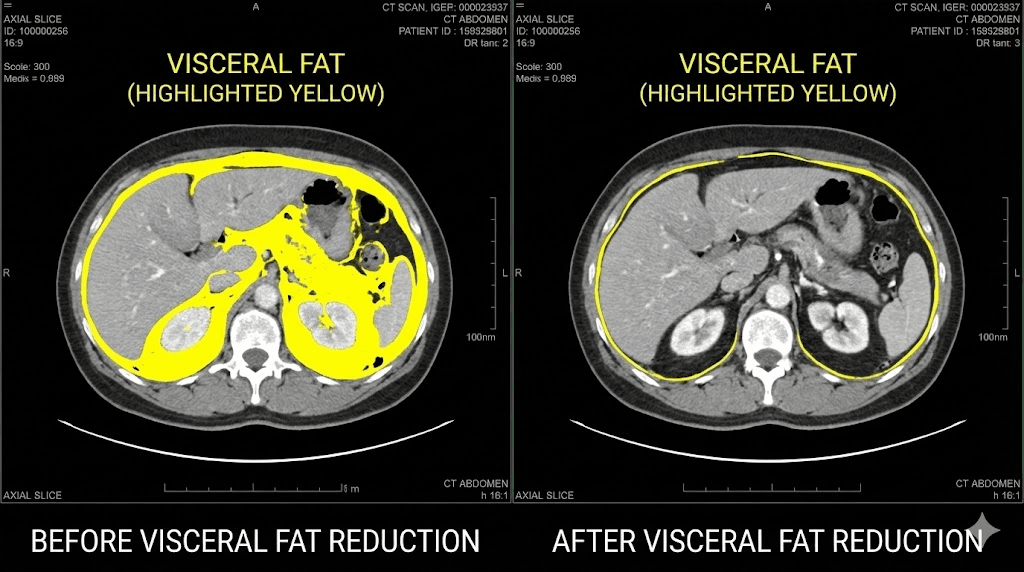
The pivotal trials examined Tesamorelin in HIV patients with excess abdominal fat. After 26 weeks of treatment, subjects receiving Tesamorelin showed significant reductions in visceral adipose tissue compared to placebo. The average reduction exceeded 15 percent of baseline visceral fat volume.
Importantly, the fat loss was specific to the visceral compartment. Subcutaneous fat showed minimal change, and lean body mass was preserved or increased. This selectivity is exactly what makes Tesamorelin valuable for targeting dangerous visceral fat specifically.
Metabolic parameters improved alongside fat reduction. Triglycerides decreased. Some markers of insulin sensitivity improved. These changes suggest the metabolic benefits extend beyond simple fat loss to address the inflammatory and metabolic dysfunction visceral fat causes.
Extension studies following subjects for longer periods showed maintained benefits with continued treatment. Visceral fat reduction persisted as long as Tesamorelin administration continued.
Tesamorelin protocols
Standard research protocol:
2mg subcutaneous injection once daily, typically administered in the evening or before bed. This timing aligns with natural GH secretion patterns and may optimize efficacy.
Duration:
Clinical trials demonstrated significant effects after 26 weeks. Most research protocols plan for at least 3-6 months of continuous use to achieve meaningful visceral fat reduction.
Monitoring:
Periodic assessment of body composition, ideally using DEXA scanning or similar technology that can distinguish visceral from subcutaneous fat. Standard scale weight may not reflect the beneficial changes occurring.
The peptide calculator helps determine appropriate dosing. The peptide reconstitution calculator ensures accurate preparation.
Considerations and limitations
Tesamorelin is not without considerations. The peptide requires daily injection. Cost can be substantial for extended protocols. Some subjects experience injection site reactions or other side effects.
The benefits also require continued treatment. Discontinuing Tesamorelin typically results in gradual visceral fat reaccumulation over subsequent months. This positions the peptide as ongoing therapy rather than one-time treatment.
For researchers considering Tesamorelin, understanding these factors helps set appropriate expectations. The peptide works, but it requires commitment to ongoing administration.
AOD-9604: the targeted fat metabolism fragment
AOD-9604 represents a different approach to fat loss peptides. Rather than stimulating growth hormone release, AOD-9604 is a fragment of the growth hormone molecule itself, specifically designed to capture GH's fat-metabolizing effects without its growth-promoting properties.
Design and mechanism
Growth hormone is a 191 amino acid protein with multiple functional regions. Different portions of the molecule mediate different effects. The section spanning amino acids 176-191 appears particularly important for fat metabolism.
AOD-9604 consists of this fragment plus a tyrosine residue, creating a peptide that activates fat metabolism pathways without stimulating IGF-1 production or affecting blood glucose. This selectivity makes AOD-9604 potentially safer for long-term use than full growth hormone administration.
The mechanism involves beta-3 adrenergic receptor activation and direct effects on adipocyte metabolism. AOD-9604 stimulates lipolysis while inhibiting lipogenesis, essentially telling fat cells to release stored energy rather than accumulate more.
Research suggests AOD-9604 may have some preference for abdominal fat stores, though the selectivity appears less pronounced than with Tesamorelin. The peptide increases overall fat oxidation, which can include visceral fat as part of general fat reduction.
Research evidence
AOD-9604 has been studied in both animal models and human trials, though the human data is more limited than for Tesamorelin.
Animal studies show consistent fat-reducing effects. Obese mice treated with AOD-9604 showed significant weight loss without changes in food intake or lean body mass. The fat loss appeared driven by increased lipolysis rather than reduced energy intake.
Human studies have yielded mixed results. Some trials showed statistically significant fat loss compared to placebo. Others showed trends toward benefit without reaching significance. The variability may relate to dosing, duration, or subject selection.
Importantly, AOD-9604 appears safe. No significant adverse effects on glucose metabolism, IGF-1 levels, or other safety parameters have emerged from clinical trials. This favorable safety profile supports its use in extended research protocols.
The AOD-9604 complete guide provides more detailed coverage of this peptide.
AOD-9604 protocols
Standard dosing:
250-500mcg subcutaneous injection daily, typically administered in the morning on an empty stomach.
Fasted administration:
Like other fat-metabolizing peptides, AOD-9604 appears most effective when administered in a fasted state. Morning administration before eating aligns with this principle.
Duration:
Research protocols typically run 12-24 weeks to allow sufficient time for measurable fat loss.
Stacking:
AOD-9604 is sometimes combined with other fat-loss peptides for enhanced effects. The peptide stack calculator helps design combination protocols.
HGH Fragment 176-191: the classic fat-burning peptide
HGH Fragment 176-191 is closely related to AOD-9604, consisting of the same amino acid sequence without the additional tyrosine. This fragment represents the original fat-metabolizing portion of growth hormone identified by researchers.
Mechanism comparison with AOD-9604
The mechanisms of HGH Fragment 176-191 and AOD-9604 substantially overlap. Both activate lipolysis through similar pathways. Both avoid the IGF-1 elevation and glucose effects of full growth hormone. The practical differences relate mainly to stability and potency.
AOD-9604's additional tyrosine residue may improve stability and receptor binding compared to the naked fragment. However, HGH Fragment 176-191 has a longer research history and more user experience data.
For visceral fat reduction specifically, neither fragment shows the same level of targeted effect as Tesamorelin. Both work by increasing general fat oxidation rather than preferentially mobilizing visceral stores. Visceral fat reduction occurs as part of overall body fat reduction.
Research and practical use
HGH Fragment 176-191 research extends back decades. Studies consistently show lipolytic effects without the side effects of full GH administration. The fragment does not affect blood glucose, does not elevate IGF-1, and does not promote growth of non-fat tissues.
The HGH Fragment 176-191 calculator helps determine appropriate dosing for research protocols.
Typical protocol:
250-500mcg subcutaneous injection, administered 1-2 times daily on an empty stomach. Splitting the dose between morning and afternoon may optimize fat-burning effects throughout the day.
The HGH alternatives article compares various approaches to capturing growth hormone benefits.
Growth hormone secretagogues for visceral fat
Rather than administering GH or its fragments directly, growth hormone secretagogues stimulate natural GH production. This approach maintains physiological pulsatile release patterns and may be more suitable for long-term use.
CJC-1295 and visceral fat
CJC-1295 is a growth hormone releasing hormone analog that extends GH elevation duration. Unlike natural GHRH, CJC-1295 resists enzymatic degradation, producing sustained GH release over days rather than minutes.
The extended GH elevation from CJC-1295 promotes continuous lipolytic signaling. Fat cells receive sustained instructions to release stored energy. Over time, this shifts body composition toward lower fat mass and preserved or increased lean mass.
Research on CJC-1295 body composition effects shows consistent improvements. Subjects experience reduced fat mass alongside maintained or increased lean tissue. The effects on visceral fat specifically depend on overall fat reduction, as CJC-1295 does not appear to specifically target visceral stores.
The CJC-1295 dosage calculator helps determine appropriate protocols. The Ipamorelin vs CJC-1295 comparison explains how these peptides differ and complement each other.
Ipamorelin for body composition
Ipamorelin offers cleaner GH stimulation with minimal effects on cortisol, prolactin, or appetite hormones. This selectivity makes it attractive for body composition research where confounding hormonal effects could complicate results.
The Ipamorelin benefits extend beyond fat loss to include improved sleep, recovery, and overall metabolic function. These systemic benefits support the metabolic health improvements needed to address visceral fat accumulation.
Combination protocol:
Many research protocols combine CJC-1295 (1-2mg weekly) with Ipamorelin (200-300mcg 2-3 times daily) for synergistic GH elevation. This combination provides both sustained baseline elevation and acute pulsatile release.
Hexarelin and cardiac considerations
Hexarelin uniquely combines GH secretion with direct cardiac effects. For subjects with metabolic syndrome, where cardiovascular risk accompanies visceral adiposity, this dual action may provide additional benefit.
Research shows Hexarelin protects cardiac tissue, improves contractility, and supports heart function under stress. These effects occur through cardiac-specific receptors independent of GH release.
For visceral fat reduction in metabolically compromised subjects, Hexarelin's cardiac protection may be particularly relevant. The peptide addresses both the fat accumulation and the cardiovascular consequences simultaneously.
GLP-1 agonists: the metabolic game-changers
GLP-1 receptor agonists have revolutionized obesity treatment and demonstrate remarkable effects on visceral fat specifically. While technically incretin mimetics rather than traditional peptides, their mechanisms and research relevance warrant inclusion.
Semaglutide and visceral fat reduction
Semaglutide produces dramatic weight loss, with clinical trials showing average reductions of 15-20 percent of body weight. Importantly, body composition analysis reveals preferential reduction of fat mass, particularly from the visceral compartment.
Multiple mechanisms contribute to semaglutide's visceral fat effects. Appetite reduction decreases overall caloric intake. Delayed gastric emptying extends satiety. Central nervous system effects modify food preferences and reward signaling. Direct metabolic effects improve insulin sensitivity and substrate utilization.
The visceral fat reduction appears to exceed what caloric restriction alone would predict. Research suggests GLP-1 signaling influences fat distribution directly, shifting the body toward healthier fat deposition patterns even when total fat mass is controlled.
The semaglutide dosage calculator helps determine appropriate protocols. The Ozempic alternatives article compares various GLP-1 approaches.
Tirzepatide: dual mechanism advantage
Tirzepatide combines GLP-1 agonism with GIP (glucose-dependent insulinotropic polypeptide) receptor activation. This dual mechanism produces even greater weight loss and metabolic improvement than GLP-1 agonism alone.
Clinical trials show tirzepatide achieves 20-25 percent body weight reduction in many subjects, with substantial improvements in metabolic parameters including reduced liver fat and improved insulin sensitivity.
The semaglutide vs tirzepatide comparison details how these compounds differ. The tirzepatide dosing guide covers protocol specifics.
Retatrutide: the triple agonist
Retatrutide adds glucagon receptor agonism to GLP-1 and GIP activity, creating a triple agonist with potentially superior fat-reducing effects. Early research shows dramatic weight loss and metabolic improvements exceeding dual agonists.
The glucagon component specifically promotes hepatic fat oxidation and may enhance visceral fat mobilization. Research suggests this mechanism contributes to preferential visceral fat reduction beyond what GLP-1 effects alone produce.
The retatrutide dosage chart provides protocol guidance. The retatrutide buying guide discusses sourcing considerations.
GLP-1 considerations for visceral fat
GLP-1 agonists represent the most powerful pharmacological approach to visceral fat reduction currently available. However, they come with considerations.
Side effects including nausea, vomiting, and gastrointestinal disturbances are common, particularly during dose escalation. Careful titration and appropriate expectations help manage these effects.
The dramatic weight loss can include lean mass if not managed carefully. Adequate protein intake and resistance training help preserve muscle during GLP-1 treatment.
Cost and access remain barriers for some researchers. Generic semaglutide and research-grade compounds offer more accessible options than branded medications.
The peptides to take with Ozempic article discusses how healing peptides can support GLP-1 therapy.
MOTS-c: the mitochondrial metabolic optimizer
MOTS-c represents a different approach, targeting cellular energy production rather than directly promoting fat breakdown. This mitochondrial-derived peptide influences metabolism at the fundamental level of energy production efficiency.
Mitochondrial function and visceral fat
Mitochondrial dysfunction correlates strongly with visceral fat accumulation. People with excess visceral fat typically show impaired mitochondrial function, reduced oxidative capacity, and decreased fat oxidation rates. Whether this dysfunction causes or results from visceral fat accumulation, addressing it may help break the cycle.
MOTS-c activates AMPK, the master metabolic regulator that coordinates cellular energy production. AMPK activation promotes mitochondrial biogenesis, enhances fat oxidation, improves glucose uptake, and shifts metabolism toward a more efficient state.
Research shows MOTS-c administration improves metabolic parameters in both lean and obese subjects. Insulin sensitivity improves. Fat oxidation increases. Exercise capacity enhances. These changes suggest MOTS-c addresses the metabolic dysfunction underlying visceral fat accumulation.
MOTS-c and exercise synergy
MOTS-c is sometimes called an exercise mimetic because it activates many of the same pathways as physical activity. For researchers combining peptides with exercise protocols, MOTS-c may amplify training adaptations.
Exercise remains the most effective intervention for visceral fat reduction. The combination of MOTS-c with structured exercise could produce synergistic effects exceeding either intervention alone.
The best peptide for energy article covers MOTS-c and related compounds in more detail.
MOTS-c protocols
Standard research protocol:
5-10mg subcutaneous injection, administered 3-5 times weekly. Many protocols administer MOTS-c on training days to support metabolic adaptation to exercise.
Combination with other peptides:
MOTS-c combines well with GH secretagogues and fat-loss peptides through complementary mechanisms. The metabolic optimization from MOTS-c enhances the fat-mobilizing effects of other compounds.
5-Amino-1MQ: targeting fat cell formation
5-Amino-1MQ is a small molecule rather than a peptide, but its mechanism is relevant to visceral fat research. This compound inhibits NNMT (nicotinamide N-methyltransferase), an enzyme involved in fat cell formation and energy metabolism.
The NNMT pathway
NNMT activity correlates with adiposity, particularly visceral fat accumulation. Higher NNMT expression promotes fat cell formation and impairs energy expenditure. Inhibiting this enzyme reverses these effects.
Research shows NNMT inhibition reduces fat mass, increases energy expenditure, and improves metabolic parameters in animal models. The effects appear particularly pronounced in visceral fat depots where NNMT expression is highest.
Research applications
5-Amino-1MQ research is earlier stage than established peptides, but the mechanism is compelling for visceral fat specifically. By targeting an enzyme preferentially expressed in visceral fat, this compound may offer the targeted approach that most peptides lack.
Typical protocol:
50-150mg daily, typically administered orally. The compound's oral bioavailability makes it more convenient than injectable peptides.
Tesofensine: the appetite and metabolism modulator
Tesofensine is a triple monoamine reuptake inhibitor that affects dopamine, norepinephrine, and serotonin. Originally developed for neurological conditions, it was found to produce substantial weight loss through appetite reduction and increased energy expenditure.
Mechanism and effects
Tesofensine reduces appetite centrally while increasing metabolic rate. The combined effects produce significant caloric deficit without the typical hunger associated with dieting. Clinical trials showed weight loss averaging 10-12 percent over 6 months.
Body composition analysis from tesofensine trials shows preferential fat mass reduction with lean mass preservation, similar to growth hormone-based approaches. The increased norepinephrine signaling likely contributes to fat mobilization.
The tesofensine peptide article provides comprehensive coverage of this compound.
Considerations
Tesofensine's mechanism involving central monoamine systems means potential for cardiovascular and psychiatric effects. Heart rate and blood pressure monitoring are important during tesofensine protocols. The compound is not appropriate for subjects with cardiovascular conditions or mood disorders.
Comparing peptides for visceral fat reduction
Different peptides suit different situations and goals.
This comparison helps match compounds to specific research objectives.
Peptide | Primary Mechanism | Visceral Specificity | Evidence Level | Administration |
|---|---|---|---|---|
Tesamorelin | GH release via GHRH | High (FDA approved) | Strong clinical | SC daily |
Semaglutide | GLP-1 agonism | High | Strong clinical | SC weekly |
Tirzepatide | GLP-1/GIP dual agonism | High | Strong clinical | SC weekly |
AOD-9604 | Direct lipolysis | Moderate | Moderate clinical | SC daily |
HGH Frag 176-191 | Direct lipolysis | Moderate | Moderate preclinical | SC 1-2x daily |
CJC-1295/Ipamorelin | GH secretion | Moderate | Moderate clinical | SC daily |
MOTS-c | Mitochondrial function | Moderate | Moderate preclinical | SC 3-5x weekly |
Retatrutide | Triple agonism | Very high | Emerging clinical | SC weekly |
Selection guidance
Maximum visceral fat reduction with strong evidence:
Tesamorelin remains the gold standard for proven visceral fat reduction. GLP-1 agonists like semaglutide and tirzepatide offer comparable or superior effects with additional metabolic benefits.
Budget-conscious research:
AOD-9604 and HGH Fragment 176-191 offer fat-reducing effects at lower cost points than branded peptides. Effects are less dramatic but still meaningful.
Long-term metabolic optimization:
CJC-1295/Ipamorelin combinations support sustained body composition improvement through natural GH elevation. MOTS-c addresses underlying mitochondrial dysfunction.
Comprehensive metabolic syndrome:
GLP-1 agonists address multiple aspects of metabolic syndrome simultaneously, including glucose control, lipid profiles, and cardiovascular markers alongside visceral fat.
Stacking strategies for visceral fat
Combining peptides with complementary mechanisms can produce effects exceeding any single compound. Careful stack design addresses multiple pathways simultaneously.
Comprehensive visceral fat stack
For maximum visceral fat reduction:
Tesamorelin: 2mg daily for targeted visceral fat mobilization via GH
BPC-157: 250mcg twice daily for metabolic support and inflammation reduction
MOTS-c: 10mg three times weekly for mitochondrial optimization
Rationale: Tesamorelin provides proven visceral fat reduction. BPC-157 supports metabolic health and reduces inflammation that accompanies visceral adiposity. MOTS-c optimizes cellular energy production to enhance fat oxidation.
The BPC-157 article covers this peptide's metabolic and anti-inflammatory effects.
GLP-1 enhanced stack
For those using GLP-1 agonists as the foundation:
Semaglutide: Titrated to appropriate weekly dose
Ipamorelin: 200mcg twice daily to preserve lean mass
BPC-157: 250mcg twice daily for GI support and healing
Rationale: GLP-1 agonists produce substantial weight loss but can affect lean mass. Ipamorelin's GH elevation helps preserve muscle. BPC-157 supports gastrointestinal health, which GLP-1 agonists can challenge.
Budget-optimized stack
For cost-conscious research:
AOD-9604: 300mcg daily for direct lipolysis
CJC-1295: 1mg twice weekly for sustained GH elevation
Ipamorelin: 200mcg once daily for pulsatile GH release
Rationale: This combination provides fat-mobilizing effects through multiple mechanisms at accessible cost points. Effects may be less dramatic than premium compounds but still meaningful.
The how many peptides can you take at once article discusses safe combination limits.
Practical protocols for visceral fat research
Implementing research requires attention to practical details beyond peptide selection.
Protocol 1: Tesamorelin-focused approach
Goal: Maximum evidence-based visceral fat reduction
Primary peptide: Tesamorelin 2mg subcutaneous daily, evening administration
Support: Ipamorelin 200mcg morning for additional GH pulsatility
Duration: 6 months minimum for meaningful visceral fat assessment
Monitoring: DEXA scans at baseline, 3 months, and 6 months
This protocol provides the strongest evidence-based approach specifically targeting visceral fat. The combination of sustained GHRH stimulation (Tesamorelin) with pulsatile GHRP effects (Ipamorelin) optimizes GH dynamics.
Protocol 2: GLP-1 centered approach
Goal: Comprehensive metabolic improvement including visceral fat
Primary compound: Semaglutide or tirzepatide, titrated per standard schedules
Muscle preservation: CJC-1295 1mg twice weekly
GI support: BPC-157 250mcg twice daily
Duration: 6-12 months for full metabolic remodeling
This approach addresses the broader metabolic syndrome often accompanying visceral adiposity while targeting fat specifically.
Protocol 3: Endogenous optimization
Goal: Sustainable body composition improvement through enhanced natural hormones
GH axis: CJC-1295 1mg + Ipamorelin 300mcg, both administered evening
Metabolic support: MOTS-c 10mg three times weekly
Recovery: BPC-157 250mcg twice daily
Duration: 4-6 months cycles with assessment between
This protocol avoids exogenous hormones while optimizing the body's own GH production and metabolic efficiency.
Administration fundamentals
Successful protocols require proper peptide handling:
The how to reconstitute peptides guide covers preparation basics.
The peptide injection sites article details proper subcutaneous administration.
The how to store peptides guide ensures peptide stability throughout protocols.
The bacteriostatic water guide covers proper reconstitution solutions.
Supporting interventions for visceral fat
Peptides work best alongside lifestyle interventions that address visceral fat through complementary mechanisms.
Exercise specificity
Different exercise modalities affect visceral fat differently. High-intensity interval training shows particular efficacy for visceral fat reduction, likely through AMPK activation and enhanced fat oxidation that persists post-exercise.
Resistance training preserves lean mass during weight loss, which is especially important when using peptides or GLP-1 agonists that can affect body composition. Maintaining muscle mass supports metabolic rate and long-term weight maintenance.
Combining both modalities provides optimal results. HIIT addresses visceral fat directly while resistance training protects metabolically active lean tissue.
Sleep and circadian factors
Sleep deprivation promotes visceral fat accumulation through multiple pathways. Cortisol elevation from poor sleep preferentially drives visceral fat storage. Disrupted growth hormone secretion, which normally peaks during deep sleep, impairs fat metabolism.
Optimizing sleep quality and duration may be as important as any peptide intervention. Address sleep disorders, maintain consistent schedules, and prioritize 7-9 hours nightly.
Stress management
Chronic stress elevates cortisol, which strongly promotes visceral fat accumulation. No peptide fully compensates for chronically elevated cortisol. Addressing stress through behavioral interventions, adaptogenic compounds, or lifestyle changes supports peptide efficacy.
The peptides for anxiety article discusses compounds that may help manage stress responses.
Dietary considerations
Visceral fat responds particularly to metabolic factors beyond simple calories. Reducing refined carbohydrates and increasing protein intake shifts metabolism away from visceral fat accumulation. Time-restricted eating may enhance visceral fat mobilization through extended fasting periods that promote fat oxidation.
Protein adequacy becomes especially important during peptide protocols. At least 1.6g per kilogram bodyweight supports lean mass preservation during fat loss phases.
Monitoring and assessment
Tracking visceral fat specifically requires appropriate measurement methods.
DEXA scanning
Dual-energy X-ray absorptiometry provides the most accessible accurate assessment of body composition including visceral fat estimation. Many protocols use DEXA at baseline and every 3 months to track changes.
Waist circumference
Simple waist measurement correlates reasonably with visceral fat and provides easy tracking between formal assessments. Measure at the same point consistently, typically at the umbilicus or narrowest point.
Metabolic markers
Improvements in visceral fat should manifest in metabolic markers:
Fasting glucose and insulin (improving insulin sensitivity)
Triglycerides (typically decrease with visceral fat reduction)
Liver enzymes (improvement indicates reduced hepatic fat)
Inflammatory markers like CRP (decrease with reduced visceral adiposity)
Tracking these markers alongside body composition provides a more complete picture of metabolic improvement.
FAQs
Which peptide is most effective for visceral fat specifically?
Tesamorelin has the strongest evidence for preferentially reducing visceral fat, with FDA approval specifically for this indication. GLP-1 agonists like semaglutide and tirzepatide also show substantial visceral fat reduction with broader metabolic benefits. For pure visceral fat targeting with the best evidence, Tesamorelin remains the standard.
How long until visceral fat reduction becomes measurable?
Meaningful visceral fat reduction typically requires 3-6 months of consistent intervention. Earlier changes may occur but may not register on standard assessments. Planning for at least 6-month protocols allows sufficient time for significant visceral fat reduction to manifest.
Can peptides reduce visceral fat without diet and exercise?
Peptides can produce some visceral fat reduction independently, as demonstrated in clinical trials where subjects were not required to modify lifestyle. However, combining peptides with appropriate diet and exercise produces substantially greater effects. Peptides work best as part of comprehensive metabolic optimization rather than standalone interventions.
Are visceral fat peptides safe for long-term use?
Safety varies by compound. Tesamorelin has been studied for extended periods with acceptable safety profiles. GLP-1 agonists have years of clinical use data. Newer peptides have less long-term data. Working with knowledgeable clinicians and monitoring appropriate parameters supports safe extended use.
Will visceral fat return after stopping peptides?
Without continued intervention or lifestyle changes, visceral fat typically reaccumulates after discontinuing peptides. Tesamorelin studies show gradual fat regain after cessation. This positions visceral fat peptides as ongoing therapy or as part of transitioning to sustainable lifestyle maintenance.
Can I combine multiple visceral fat peptides?
Yes, combining peptides with complementary mechanisms often produces enhanced effects. However, more is not always better. Carefully designed stacks targeting different pathways make sense. Simply adding multiple peptides targeting similar mechanisms may not provide proportional benefit and increases complexity and cost.
How do I know if I have excess visceral fat?
Waist circumference provides a rough indicator. In men, waist measurements above 40 inches suggest excess visceral fat. In women, above 35 inches indicates concern. DEXA scanning or CT imaging provides more accurate assessment. Metabolic markers like elevated triglycerides, fasting glucose, or liver enzymes may indicate visceral adiposity even when BMI is normal.
How SeekPeptides supports your visceral fat goals
Targeting visceral fat effectively requires matching the right peptides to individual metabolic profiles and goals. SeekPeptides provides personalized protocols designed for your specific situation.
The platform offers customized peptide recommendations based on your metabolic status, goals, and preferences. Rather than generic one-size-fits-all approaches, you receive protocols tailored to address your specific visceral fat challenges.
Access to comprehensive research helps you understand the science behind recommendations. The AI peptide advisor provides 24/7 support for questions during your protocol. Progress tracking tools help assess what works and guide protocol refinement over time.
Visceral fat threatens health in ways subcutaneous fat does not. Addressing it effectively requires the right tools and guidance. Get personalized support for your visceral fat reduction goals with SeekPeptides.
Helpful resources and tools
These tools support visceral fat peptide protocols:
Peptide calculator for general dosing guidance
Peptide reconstitution calculator for accurate preparation
Related guides for further exploration
These articles provide deeper context on specific topics:
Peptides for fat loss covers fat metabolism broadly
Best peptides for weight loss reviews top compounds
Best peptide stack for weight loss discusses combinations
Peptides for weight loss provides comprehensive overview
AOD-9604 complete guide covers this fragment in detail

Final thoughts
Visceral fat is not just an aesthetic concern. It is a metabolic threat that drives inflammation, insulin resistance, and disease risk. Diet and exercise help, but the hormonal and metabolic factors underlying visceral fat accumulation often require additional intervention.
Peptides provide tools specifically suited to this challenge. Tesamorelin offers FDA-approved, evidence-based visceral fat reduction. GLP-1 agonists produce dramatic metabolic improvements. Growth hormone secretagogues shift body composition toward health. Emerging compounds target visceral fat through novel mechanisms.
The research supports real effects. Clinical trials demonstrate measurable visceral fat reduction. Metabolic parameters improve alongside body composition changes. The mechanisms are understood well enough to design rational protocols.
Start with compounds having the strongest evidence for your specific goals. Build protocols around proven peptides before adding experimental compounds. Support peptide interventions with lifestyle factors that address visceral fat through complementary mechanisms.
Visceral fat accumulation is not inevitable. With appropriate tools and consistent intervention, this dangerous fat depot can be reduced. The opportunity exists to address one of the most significant metabolic health challenges through peptide-based approaches.
Your next step: use the calculators to design your protocol, review the related guides for specific compounds, and consider how personalized peptide protocols through SeekPeptides might support your visceral fat reduction goals.