Mar 23, 2026

Some researchers draw 50 units and barely feel a thing. Others draw the same 50 units and spend the next three days on the couch, nauseated and exhausted, wondering what went wrong. Same number on the syringe. Wildly different outcomes. How is that possible? The answer comes down to one critical variable that too many people overlook when they start their tirzepatide dosing journey, and that variable is concentration. Fifty units on an insulin syringe always equals 0.5 mL of liquid. That part never changes. But the amount of actual tirzepatide dissolved in that liquid, measured in milligrams, can range from a gentle 2.5 mg starting dose all the way up to a maximum 15 mg therapeutic dose. That is a six-fold difference.
One could be perfect for your first week. The other could send you straight to the emergency room. The question "is 50 units of tirzepatide a lot?" simply cannot be answered without first asking another question: what is the concentration of your vial? This guide will walk you through every concentration scenario, show you exactly what 50 units delivers in milligrams, explain where each dose falls on the standard tirzepatide dose escalation schedule, and help you understand whether your specific 50-unit draw is too much, too little, or exactly right.
Whether you are using compounded tirzepatide from a pharmacy or brand-name Mounjaro, the math matters. And getting it wrong is not something you want to experience firsthand.
Why 50 units means nothing without knowing concentration
This is the single most important concept in this entire article. Read it twice if you need to.
Units on a syringe measure volume, not potency. When you draw your syringe to the 50-unit mark, you are pulling exactly 0.5 mL of liquid into that syringe. Every time. Regardless of what is dissolved in that liquid. An insulin syringe is calibrated so that 100 units equals 1 mL, which means 50 units always equals half a milliliter. This is a fixed physical measurement, like filling a cup halfway. The cup does not care whether you fill it with water or honey. It holds the same volume either way.
Concentration changes everything.
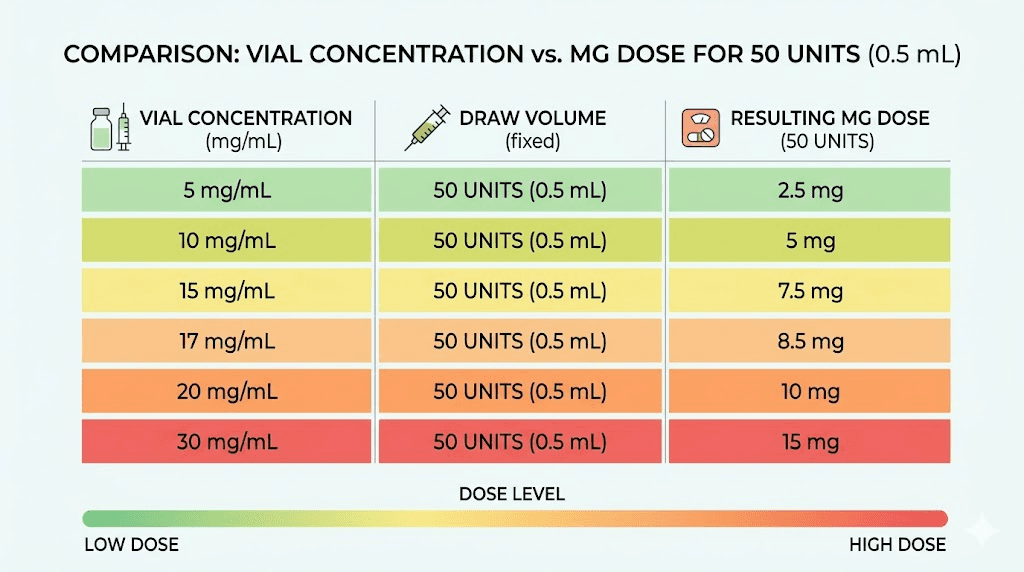
If your vial contains tirzepatide at 5 mg/mL, then that 0.5 mL draw contains 2.5 mg of active peptide. That is the lowest therapeutic dose, the one most providers start patients on during weeks one through four. However, if your vial contains tirzepatide at 30 mg/mL, that same 0.5 mL draw contains 15 mg of active peptide. That is the maximum prescribed dose, typically reserved for patients who have been on tirzepatide for five months or longer and have gradually worked their way up through the entire tirzepatide dosing chart. Same syringe. Same line. Same 50 units. But one delivers a gentle starting dose while the other delivers the absolute ceiling of the medication. The difference between these two scenarios is not trivial. It is potentially dangerous, which is why understanding your vial concentration is not optional. It is essential.
Think about it this way. You would never ask "is half a cup of liquid a lot to drink?" without knowing what liquid you are talking about. Half a cup of water is nothing. Half a cup of espresso would have you climbing the walls. The volume is identical. The contents make it a completely different experience. Tirzepatide works the same way, and the compounded tirzepatide dosage calculator exists specifically to help you navigate this math.
The conversion formula you need to memorize
Here is the formula. It is simple, and it will save you from dosing errors every single time:
mg = (units / 100) x concentration in mg/mL
That is it. Three numbers and one multiplication. For 50 units, the formula simplifies even further because 50 divided by 100 is always 0.5. So for 50 units specifically:
mg = 0.5 x concentration in mg/mL
If you need to work backwards, figuring out how many units to draw for a specific milligram dose, flip the formula:
units = (desired mg / concentration in mg/mL) x 100
The peptide calculator at SeekPeptides automates this math for you, but understanding the formula yourself adds a critical safety layer. Calculators can have input errors. Your own understanding cannot be mistyped. Let us walk through what 50 units actually delivers at every common concentration you are likely to encounter.
What 50 units equals at every common concentration
Compounding pharmacies produce tirzepatide at several different concentrations. Brand-name Mounjaro uses pre-filled pens with fixed doses, so unit conversions do not apply to brand-name products. But if you are using lyophilized compounded tirzepatide that requires reconstitution, or liquid compounded tirzepatide from a pharmacy, you need to know your concentration. Here is what 50 units delivers at each one.
At 5 mg/mL: 50 units = 2.5 mg
This is the lowest concentration commonly available. At this concentration, drawing 50 units gives you 2.5 mg of tirzepatide. That is the standard initiation dose, the one the FDA-approved dosing schedule for weight loss recommends for your first four weeks. If your vial is 5 mg/mL and you draw 50 units, you are at the absolute starting line. This is not a lot. It is the minimum effective dose, designed to let your body acclimate to the medication before increasing.
At 2.5 mg, most people experience mild appetite suppression. Some notice mild fatigue or light nausea. Many feel almost nothing at all and wonder if the medication is working. That is normal and expected at this introductory level.
At 10 mg/mL: 50 units = 5 mg
Now we are getting into the therapeutic range. A 10 mg/mL concentration is one of the most common you will encounter from compounding pharmacies, and at this concentration, 50 units delivers exactly 5 mg. This is the second step on the dose escalation ladder, typically prescribed during weeks five through eight.
Five milligrams is where most people start to feel tirzepatide working. Appetite suppression becomes noticeable. Food thoughts quiet down. You might find yourself forgetting to eat, which is a strange but common experience reported in clinical trials. Side effects at this level can include mild to moderate nausea, some constipation, and occasional headaches. For many individuals, 5 mg is the sweet spot where benefits are meaningful and side effects remain manageable.
Is 50 units a lot at this concentration? No. It is a moderate, standard therapeutic dose. Nothing extreme.
At 15 mg/mL: 50 units = 7.5 mg
At 15 mg/mL, drawing 50 units delivers 7.5 mg. This sits right in the middle of the escalation schedule, prescribed during weeks nine through twelve for patients following the standard protocol. You should not be at this dose unless you have already completed at least two months on lower doses and your provider has approved the increase.
Seven and a half milligrams brings more pronounced appetite suppression. Weight loss typically accelerates at this level. But side effects can intensify too. Gastrointestinal symptoms become more common, and some people experience significant nausea during the first week at this dose before it settles. If you are someone who has never used tirzepatide before and you draw 50 units from a 15 mg/mL vial, you would be taking three times the recommended starting dose. That would absolutely be too much.
At 17 mg/mL: 50 units = 8.5 mg
The 17 mg/mL concentration deserves special attention because it is the format commonly associated with tirzepatide compounded with niacinamide, a formulation popularized by certain compounding pharmacies. At this concentration, 50 units gives you 8.5 mg.
This falls between the standard 7.5 mg and 10 mg dose tiers. It is not a standard escalation step, which means your provider likely calculated this dose intentionally based on your response to previous doses. Eight and a half milligrams is a moderate-to-high dose. For someone properly titrated to this level, it is reasonable. For a beginner, it would be far too much.
At 20 mg/mL: 50 units = 10 mg
Higher concentration vials become more common as patients progress through the dosing schedule, because they allow larger doses in smaller injection volumes. At 20 mg/mL, drawing 50 units delivers a full 10 mg dose. This corresponds to the weeks thirteen through sixteen range on the standard escalation.
Ten milligrams is a significant dose. Clinical trial data shows substantial weight loss at this level, with the SURMOUNT-1 trial reporting average weight loss of 19.5% of body weight at 10 mg over 72 weeks. Side effects are also more prominent. Body aches, fatigue, and GI symptoms are well-documented at this dose tier. If you draw 50 units from a 20 mg/mL vial and this is your first dose, you would be taking four times the recommended starting amount. That is dangerous and could result in severe adverse effects.
At 30 mg/mL: 50 units = 15 mg
This is the ceiling. At 30 mg/mL, which is a rare but available concentration, 50 units delivers the maximum FDA-studied dose of 15 mg. This is as high as the approved dosing schedule goes, typically reached only after twenty or more weeks of gradual escalation.
Fifteen milligrams produces the most powerful appetite suppression and the highest average weight loss in clinical trials. But it also carries the highest side effect burden. Drawing 50 units from a 30 mg/mL vial when you should be at 2.5 mg would mean taking six times your intended dose. The consequences of that kind of error can include severe vomiting, dangerous dehydration, acute anxiety, and potentially hypoglycemia requiring emergency medical attention.
Complete 50-unit conversion reference table
For quick reference, here is every scenario in one place. Bookmark this. Screenshot it. Keep it next to your supplies. The compound dosage chart on SeekPeptides has an interactive version, but having a static reference adds another layer of safety.
5 mg/mL concentration: 50 units = 2.5 mg (starting dose, weeks 1-4)
10 mg/mL concentration: 50 units = 5 mg (moderate dose, weeks 5-8)
15 mg/mL concentration: 50 units = 7.5 mg (mid-range dose, weeks 9-12)
17 mg/mL concentration: 50 units = 8.5 mg (between standard tiers)
20 mg/mL concentration: 50 units = 10 mg (high dose, weeks 13-16)
30 mg/mL concentration: 50 units = 15 mg (maximum dose, week 21+)
Notice the pattern. Every time the concentration doubles, the milligram dose delivered by 50 units also doubles. A 10 mg/mL vial delivers twice what a 5 mg/mL vial does at the same draw volume. A 20 mg/mL vial delivers four times what a 5 mg/mL vial does. This is exactly why concentration awareness is not a nice-to-have. It is a safety requirement.
Where does your 50-unit dose fall on the escalation schedule?
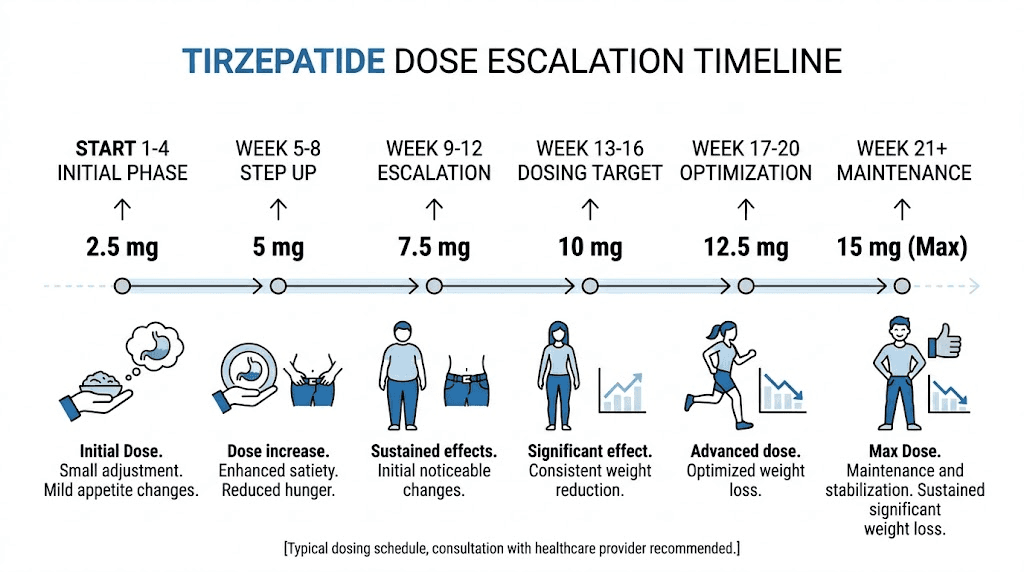
Now that you know how to convert 50 units into milligrams, the next step is understanding where that milligram dose sits on the standard dose escalation. The FDA-approved titration schedule for tirzepatide follows a careful stepwise approach designed to minimize side effects while allowing the body to adapt to the medication gradually. Here is the complete schedule with context for each tier.
Weeks 1-4: 2.5 mg (initiation only)
This is not a therapeutic dose. Let that sink in. The first four weeks at 2.5 mg exist purely to let your GI system adjust. What to expect after your first dose varies from person to person, but meaningful weight loss is not the goal at this stage. The goal is tolerance. If 50 units from your vial equals 2.5 mg, you are at this initiation tier, and it is absolutely not a lot. It is the minimum.
Weeks 5-8: 5 mg
The first true therapeutic dose. This is where the medication begins doing its job. Appetite suppression activates more noticeably. How fast tirzepatide works depends partly on this transition from the initiation dose to the first therapeutic tier. If your 50 units equals 5 mg, you are in standard therapeutic territory. Not high. Not low. Right where many people find meaningful results.
Weeks 9-12: 7.5 mg
Mid-range dosing. The clinical trials showed increasing weight loss with each dose tier, and 7.5 mg represents the middle of the escalation. If 50 units from your vial delivers 7.5 mg, you are at a moderate dose that most providers consider safe for patients who have already proven tolerance at 5 mg. Not a lot in the grand scheme, but not a starting dose either.
Weeks 13-16: 10 mg
Higher therapeutic dosing. This is where some patients choose to stay rather than continuing to escalate. The weight loss timeline often shows strong results at 10 mg without needing to push higher. If your 50 units delivers 10 mg, you are on a higher dose that requires established tolerance and provider oversight.
Weeks 17-20: 12.5 mg
Approaching the upper end. You should only reach 12.5 mg after four months of gradual escalation at minimum. Fifty units does not directly correspond to 12.5 mg at any common whole-number concentration, but at a 25 mg/mL vial (less common), 50 units would deliver exactly 12.5 mg. Most people reaching this dose will be using different unit measurements with their specific vial concentration.
Week 21 and beyond: 15 mg (maximum)
The ceiling. The highest studied and approved dose. If 50 units from your vial equals 15 mg, you are at the absolute maximum, and this should only happen after five or more months of careful titration under medical supervision. Is 50 units a lot at this concentration? Yes. It is the maximum recommended dose of the medication.
How to read your vial label correctly
Misreading a vial label is one of the most common causes of dosing errors with compounded tirzepatide. Brand-name Mounjaro comes in pre-filled pens where the dose is set for you, but compounded tirzepatide requires you to understand what you are looking at. Here is what to look for.
The concentration will be listed in one of several formats. Most commonly, you will see something like "Tirzepatide 10 mg/mL" printed on the label. This tells you that every milliliter of liquid in the vial contains 10 milligrams of active tirzepatide. Some labels express total content instead, such as "Tirzepatide 30 mg / 3 mL." In this case, you need to divide the total milligrams by the total milliliters to get the concentration: 30 divided by 3 equals 10 mg/mL.
Watch for this common mistake.
Some people confuse total vial content with concentration. A vial labeled "30 mg" might contain 30 mg total in 3 mL (concentration: 10 mg/mL) or 30 mg total in 1 mL (concentration: 30 mg/mL). The total milligrams on the label tells you what is in the entire vial. The concentration in mg/mL tells you what is in each milliliter, and that is the number you need for your dose calculation. If you are ever unsure, use the compounded tirzepatide dosage calculator or call your pharmacy directly. Guessing is not an option when the difference could be a 2.5 mg dose versus a 15 mg dose.
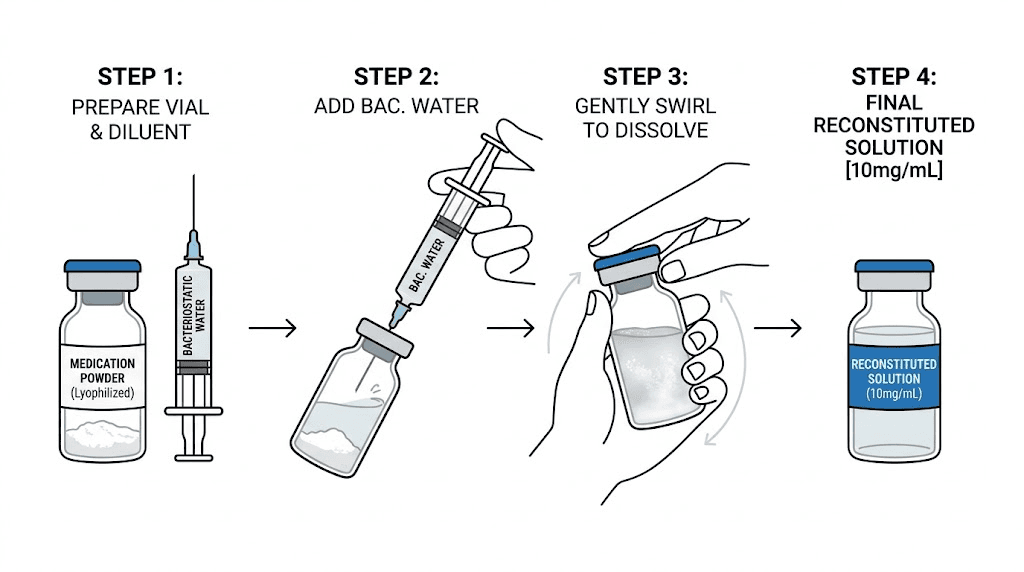
Lyophilized powder versus pre-mixed liquid
The format of your tirzepatide also determines concentration, but in a different way. If you received a vial of lyophilized (freeze-dried) tirzepatide, the concentration depends on how much bacteriostatic water you add during reconstitution. A 10 mg vial of lyophilized powder becomes 10 mg/mL if you add 1 mL of water, 5 mg/mL if you add 2 mL, or 3.33 mg/mL if you add 3 mL. The amount of water you use directly determines your concentration and therefore what 50 units will deliver.
This is why knowing how much bacteriostatic water to use with your vial is not a minor detail. It is a dosing decision. If your provider prescribed a specific concentration, you must add the exact amount of water specified. Adding more water makes the solution weaker. Adding less makes it stronger. Either deviation changes your dose.
For a 30 mg vial, the same principle applies. The amount of bacteriostatic water you mix with 30 mg of tirzepatide creates the concentration you will work with for the life of that vial. The peptide reconstitution calculator helps you determine exactly how much water to add for your target concentration.
Common compounding pharmacy concentrations explained
Not all pharmacies compound tirzepatide at the same concentrations. Understanding what different pharmacies typically offer helps you interpret your prescription correctly and calculate your compounded dose accurately.
5 mg/mL (low concentration)
This concentration is ideal for patients in the early stages of their titration who need small, precise doses. At 5 mg/mL, the unit draws are relatively large for each milligram of medication, which makes it easier to measure small dose increments accurately. The downside is that higher doses require drawing more liquid. To get 15 mg from a 5 mg/mL vial, you would need to draw 300 units, which equals 3 mL. That is a large injection volume that can cause more discomfort at the injection site.
10 mg/mL (most common)
This is arguably the most versatile concentration. It balances precision for lower doses with reasonable injection volumes for higher doses. At 10 mg/mL, 50 units gives you 5 mg, which is a clean, standard dose. The math stays straightforward: 25 units for 2.5 mg, 50 units for 5 mg, 75 units for 7.5 mg, 100 units for 10 mg. Simple round numbers. Fewer chances for errors.
15 mg/mL
A mid-range concentration that works well for patients in the 5-10 mg dosing range who want smaller injection volumes. At 15 mg/mL, reaching common doses requires slightly less intuitive math. For 5 mg, you would draw approximately 33 units. For 7.5 mg, exactly 50 units. For 10 mg, approximately 67 units. The numbers are less round, which increases the importance of careful syringe reading and double-checking with a peptide calculator.
17 mg/mL (niacinamide compound format)
This specific concentration is frequently associated with tirzepatide and niacinamide compound formulations. The 17 mg/mL format requires careful math because the numbers do not land on round milligram doses at common unit draws. Fifty units at this concentration delivers 8.5 mg, which falls between standard escalation tiers. If your provider prescribed a 17 mg/mL compound, they have likely calculated your specific unit draw for a target milligram dose. Follow their instructions precisely.
20 mg/mL (higher concentration)
Higher concentration vials are popular among patients at established, higher doses because they reduce injection volume. At 20 mg/mL, getting 10 mg requires only 50 units (0.5 mL), while getting 15 mg requires 75 units (0.75 mL). The reduced volume means less discomfort during injection and less liquid pooling at the stomach injection site or thigh injection site. However, because each unit contains more medication, small measurement errors have bigger consequences.
30 mg/mL (very concentrated, rare)
The highest concentration you are likely to encounter. At 30 mg/mL, tiny volumes deliver large doses. Just 10 units delivers 3 mg, and 50 units delivers the full 15 mg maximum. This concentration demands extreme precision. Drawing even five units too many means an extra 1.5 mg of medication, which could be the difference between a tolerable dose and a miserable week of side effects.
Signs you are on too high a dose
Regardless of whether you drew 50 units or any other amount, your body will tell you if the dose is too high. Learning to recognize overdose symptoms is not just helpful. It could be medically necessary.
Severe nausea that does not resolve within the first 48 hours after injection is the most common indicator. Mild nausea during the first day or two after a dose increase is normal as your body adjusts. But if you find yourself unable to keep water down, if the nausea is constant rather than intermittent, or if it persists for three or more days, your dose may be too high.
Vomiting is a more serious sign. Occasional mild nausea is expected. Active vomiting is not part of a well-calibrated dosing protocol. If you are vomiting after your injection, especially if it happens repeatedly, contact your provider immediately. Persistent diarrhea alongside nausea compounds the dehydration risk and should not be ignored.
Other high-dose warning signs include:
Severe abdominal pain or cramping that goes beyond mild discomfort
Dizziness or lightheadedness, especially when standing
Excessive fatigue beyond what is normal during dose adjustments, which is distinct from the manageable fatigue that some people experience
Signs of dehydration: dark urine, dry mouth, decreased urination, headache
Hypoglycemia symptoms: shakiness, cold sweats, confusion, rapid heartbeat (especially concerning for individuals on diabetes medications)
Severe sleep disruption that was not present at lower doses
Complete inability to eat anything for more than 24 hours
If you experience any combination of these symptoms after drawing 50 units, check your math immediately. Verify your vial concentration. Calculate the actual milligram dose you administered. And contact your healthcare provider with that information. The more specific you can be about what you actually took, the more effectively they can help you.
Signs you are on too low a dose
The opposite problem also exists. If 50 units from your vial delivers a dose that is too low for your current stage in the titration, you will notice a different set of indicators.
No appetite suppression is the clearest signal. Tirzepatide works primarily through appetite modulation via GIP and GLP-1 receptor agonism. If you feel no change in hunger or food cravings after several weeks at your current dose, the dose may be insufficient. Some people mistake a properly working dose for "not working" because the effect is subtle at lower levels, but after weeks with no noticeable change, the dose likely needs adjustment.
Other indicators of insufficient dosing include:
No change in body weight after four or more weeks at the same dose
Hunger returning well before your next weekly injection, especially if it returns within two to three days
No change in blood sugar levels for individuals using tirzepatide for type 2 diabetes
Food noise remaining as loud as it was before starting the medication
If you are reading this because you drew 50 units from a 5 mg/mL vial and are wondering why you are not losing weight on tirzepatide, the answer may simply be that 2.5 mg is the initiation dose, not a weight-loss dose. Patience and proper titration are the path forward, not increasing your draw without medical guidance.
What to do if you drew too much or too little
Mistakes happen. Even experienced nurses occasionally misdraw medication. What matters is how you respond.
If you already injected too much
You cannot un-inject medication. Once it is administered subcutaneously, the tirzepatide will be absorbed. Here is what to do:
First, calculate exactly how much you took. Use the conversion formula. Write down the concentration and the units you drew, then determine the milligram dose. This information is critical for your healthcare provider.
Contact your prescribing provider immediately, especially if the overdose is significant (double or more of your intended dose). They may recommend monitoring at home for mild overdoses or emergency evaluation for severe ones. In the meantime, stay hydrated. Overdose symptoms, particularly nausea and vomiting, can cause dehydration quickly. Sip electrolyte solutions rather than plain water. Have bland, easily digestible foods available in case you can eat small amounts. Do not attempt to compensate by skipping your next dose without provider guidance. And do not induce vomiting, as the medication is injected subcutaneously, not taken orally, so vomiting will not remove it from your system.
If you already injected too little
This situation is less dangerous but still worth addressing properly. If you realized immediately after injecting that you drew too few units, do not administer a second injection to make up the difference unless your provider specifically instructs you to. Splitting tirzepatide doses can affect absorption patterns and is a decision that should involve medical guidance.
If the under-dose was minor (a few units off), it is generally safe to continue with your regular schedule and simply draw the correct amount next time. If you accidentally took a significantly lower dose, contact your provider to discuss whether to supplement the dose or wait until your next scheduled injection.
If you caught the error before injecting
This is the best-case scenario. If you notice the syringe draw is wrong before the needle goes in, simply push the solution back into the vial (maintaining sterile technique) and redraw to the correct measurement. Check the tirzepatide syringe dosage guide to confirm you are reading the markings correctly. Air bubbles can distort your reading, so tap the syringe to move bubbles to the top and push them out before measuring.
How compounded tirzepatide differs from brand-name Mounjaro
Understanding this distinction matters because the "is 50 units a lot" question almost exclusively applies to compounded tirzepatide users. Brand-name Mounjaro users do not measure in units at all.
Mounjaro comes in single-use, pre-filled auto-injector pens. Each pen contains a fixed dose: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, or 15 mg. You press the pen against your skin, click the button, and the full dose is delivered. There is no syringe. There are no units to measure. There is no concentration to calculate. The pen does the math for you.
Compounded tirzepatide is different. It arrives as either a liquid solution in a multi-use vial or as lyophilized powder that you reconstitute yourself with bacteriostatic water. You draw doses from the vial using an insulin syringe, which means you are responsible for measuring the correct number of units based on your vial concentration and prescribed milligram dose. This additional responsibility comes with additional risk of error, which is why resources like SeekPeptides are valuable. They provide the calculators, charts, and guides that help you navigate the math safely.
Compounded tirzepatide may also contain additional ingredients that brand-name does not. Formulations with vitamin B12, glycine, levocarnitine, or vitamin B6 are common from compounding pharmacies. These additions do not change the tirzepatide concentration listed on the label, but they are worth noting because they may affect the overall appearance of the solution. Knowing what color your tirzepatide should be, and particularly what color tirzepatide with B12 looks like, helps you verify that your vial is what it should be.
Common mistakes people make with unit conversions
After reviewing hundreds of forum posts, community questions, and patient reports, these are the most frequent dosing errors. Every single one is preventable.
Mistake 1: Assuming units equal milligrams
This is the most dangerous mistake. Someone reads their prescription for "5 mg" and draws the syringe to the 5-unit mark. At a 10 mg/mL concentration, 5 units delivers only 0.5 mg, which is one-tenth of the intended dose. At a 30 mg/mL concentration, 5 units delivers 1.5 mg. Neither is the correct 5 mg dose. The correct draw for 5 mg depends entirely on concentration. At 10 mg/mL, you need 50 units. At 5 mg/mL, you need 100 units. Never assume that the milligram number on your prescription matches the unit number on your syringe.
Mistake 2: Confusing total vial content with concentration
A vial labeled "30 mg" could be 30 mg in 1 mL (concentration: 30 mg/mL) or 30 mg in 3 mL (concentration: 10 mg/mL). If you treat a 10 mg/mL vial as if it were 30 mg/mL, you will take only one-third of your intended dose. If you treat a 30 mg/mL vial as if it were 10 mg/mL, you will take three times your intended dose. Always look for the per-milliliter concentration, not just the total content.
Mistake 3: Using the wrong syringe type
Not all syringes are calibrated the same way. Standard insulin syringes are U-100, meaning 100 units equals 1 mL. But U-40 syringes (sometimes used in veterinary medicine) calibrate 40 units to 1 mL. Using a U-40 syringe when your dosing instructions assume a U-100 syringe would deliver 2.5 times the intended dose. Always confirm you are using a U-100 insulin syringe unless specifically instructed otherwise, and review the proper syringe injection technique.
Mistake 4: Not accounting for reconstitution volume
When reconstituting lyophilized tirzepatide, the amount of bacteriostatic water you add determines your concentration. If the instructions say to add 2 mL to a 10 mg vial (creating 5 mg/mL), but you only add 1 mL (creating 10 mg/mL), every single dose you draw from that vial will be double what you intended. This error compounds over the entire life of the vial, affecting every dose, not just one. The reconstitution calculator prevents this error by showing you exactly how much water to add.
Mistake 5: Rounding carelessly
At high concentrations, small rounding errors matter. If your target dose is 7.5 mg from a 20 mg/mL vial, the correct draw is 37.5 units. Some people round to 40 units for convenience, but that changes the dose from 7.5 mg to 8 mg. A half-milligram difference might seem trivial, but over weeks of treatment, consistently taking slightly more than prescribed can affect side effects and tolerance. Use precise measurements whenever possible.
Mistake 6: Changing vials without recalculating
This happens more often than you might expect. A patient finishes a 10 mg/mL vial and starts a new 20 mg/mL vial from a different pharmacy or prescription. They draw the same 50 units out of habit, not realizing they just doubled their dose from 5 mg to 10 mg. Every time you open a new vial, verify the concentration and recalculate your draw. Every time.
Practical dosing scenarios with 50 units
Let us walk through some real-world scenarios that people actually encounter. These examples will help solidify the math and give you context for your own situation.
Scenario 1: New patient, first injection
Sarah just received her first vial of compounded tirzepatide at 10 mg/mL. Her provider prescribed 2.5 mg weekly as a starting dose. She draws 50 units. Is this right?
No. At 10 mg/mL, 50 units delivers 5 mg, which is double her prescribed starting dose. For 2.5 mg at 10 mg/mL, she needs 25 units. This is exactly the kind of error that sends people searching for "is 50 units of tirzepatide a lot" after a rough first week.
Scenario 2: Established patient, routine dose
Michael has been on tirzepatide for three months. He has successfully titrated from 2.5 mg through 5 mg and is now at 7.5 mg weekly. His vial is 15 mg/mL. He draws 50 units. Is this correct?
Yes. At 15 mg/mL, 50 units delivers exactly 7.5 mg. His draw is perfect for his current dose tier.
Scenario 3: Patient switching vials
Jessica was using a 10 mg/mL vial and drawing 50 units for her 5 mg dose. She ran out and her pharmacy sent a 20 mg/mL vial this time. She draws 50 units out of habit. What happens?
She just took 10 mg instead of 5 mg. Double her established dose. She skipped two entire dose escalation steps. This will likely result in significant nausea, possibly vomiting, and an unpleasant several days while the excess medication processes through her system. For 5 mg from a 20 mg/mL vial, she should draw only 25 units.
Scenario 4: Reconstitution error
David received a 10 mg vial of lyophilized tirzepatide. His instructions said to add 2 mL of bacteriostatic water for a 5 mg/mL concentration. He misread and added only 1 mL, creating a 10 mg/mL concentration. He then draws 50 units for what he thinks is his 2.5 mg starting dose. What did he actually take?
He took 5 mg. Double his intended dose. The reconstitution error cascaded into a dosing error, which is why careful attention during reconstitution is just as important as careful syringe measurement.
Building a double-check habit: the three-second verification
The fastest way to prevent every dosing error in this article is a three-second routine before every injection. It sounds almost too simple. It is simple. And that is why it works.
Before you push the plunger, look at three things. First, the vial label. Confirm the concentration in mg/mL. Second, the syringe. Confirm the number of units you drew. Third, the math. Multiply 0.5 (for 50 units) by the concentration. Does the result match your prescribed milligram dose? If all three check out, inject. If any one does not match, stop and recalculate.
This habit takes literal seconds. It costs nothing. And it catches errors that could otherwise ruin your entire week or, in extreme cases, land you in the emergency room. Experienced nurses do a version of this check with every single medication they administer in clinical settings. There is no reason you should hold yourself to a lower standard when self-injecting at home.
Some people write their calculation on a sticky note and keep it with their supplies. Others set a recurring phone reminder that includes the specific draw volume: "Tuesday 8 PM, tirzepatide, 50 units from 10 mg/mL vial = 5 mg." Whatever system works for you, make it automatic. The time to discover a dosing error is before the needle goes in, not three days later when you are wondering why you feel terrible.
How body weight and composition affect dose response
Two people can inject the same milligram dose and experience very different results. Body weight plays a role in this variation, though it is not the only factor. A 150-pound person and a 300-pound person receiving the same 5 mg dose are getting the same absolute amount of medication, but the per-kilogram dose is quite different. The larger individual is receiving roughly half the weight-adjusted dose.
Clinical trials for tirzepatide used fixed doses (not weight-based dosing), and the medication proved effective across a wide range of body weights. However, some researchers and clinicians note that heavier individuals may need to progress through the dose escalation more quickly to achieve the same level of receptor saturation as lighter individuals. This does not mean you should self-adjust your 50-unit draw. It means your provider may recommend a different escalation timeline based on your starting weight, and that recommendation should be followed.
Body composition matters too. Subcutaneous fat distribution affects absorption rates. Someone with more adipose tissue at the injection site may absorb the medication slightly differently than someone with less. This is one reason the stomach injection technique involves pinching a fold of skin, which ensures consistent subcutaneous delivery regardless of body fat percentage.
Muscle mass also plays a role in overall metabolic response. People with higher muscle mass tend to have higher basal metabolic rates, which can influence how the weight loss effects of tirzepatide manifest.
The muscle-related side effects some users report may also correlate with body composition, though research on this specific connection is still emerging.
Tracking your response to 50 units over time
Documentation transforms guesswork into data. And data is what helps you and your provider make smart dosing decisions.
Keep a simple log. It does not need to be complicated. After each injection, record the date, the number of units drawn, the vial concentration, the resulting milligram dose, and any side effects you notice over the following 48-72 hours. Also record your weight, ideally at the same time of day each week, and any subjective notes about appetite, energy, and mood.
This record serves multiple purposes. It helps your provider identify patterns, like whether your nausea peaks on day two post-injection or whether a specific concentration from a specific pharmacy seems to affect you differently. It also protects you from memory errors. After eight weeks of injections, it becomes difficult to remember exactly what happened during week three. Your log remembers for you.
Some people use smartphone apps to track their GLP-1 journey. Others prefer a simple notebook. The format does not matter nearly as much as the consistency. The before-and-after documentation that many users share started as exactly this kind of weekly tracking, accumulated over months into a visible transformation story.
Pay particular attention to weeks when something changes. Did you switch vial concentrations? Start a new vial from a different lot? Change your injection day or time? Miss a dose? These variables can all affect your experience with the same 50-unit draw, and noting them helps isolate what is actually causing any changes you observe.
50 units compared to other common draws
To give you more context for whether 50 units is a lot, it helps to see how it compares to other common unit draws that people use with tirzepatide.
10 units is a small draw. At most concentrations, this delivers between 0.5 mg and 3 mg. People using microdosing protocols or microdose schedules often work with draws in this range.
20 units delivers 1-6 mg depending on concentration. This is a common draw for starting doses at higher concentrations.
30 units delivers 1.5-9 mg. Mid-range territory that covers several dose tiers depending on concentration.
50 units, as we have established, delivers 2.5-15 mg. This is the widest practical range because it spans from the minimum starting dose to the maximum therapeutic dose.
75 units delivers 3.75-22.5 mg. At higher concentrations, this exceeds the maximum recommended dose and should only be drawn at lower concentrations for mid-range to high doses.
25 units delivers 1.25-7.5 mg. A common draw for people on lower to moderate doses with higher concentration vials.
The point of these comparisons is simple: the number of units drawn is meaningless without concentration context. Fifty units is neither inherently large nor small. It is just a volume measurement.
How the semaglutide comparison adds perspective
Many people searching about tirzepatide dosing have either switched from semaglutide or are comparing the two medications. If you previously used semaglutide, your unit-drawing experience does not transfer directly because the two medications have different potency profiles and concentration standards.
The question "is 50 units of semaglutide a lot" has a completely different answer than the same question about tirzepatide. Semaglutide is typically compounded at different concentrations, and its dose escalation schedule differs from tirzepatide. You can compare the two medications using the semaglutide vs. tirzepatide comparison tool, and the semaglutide to tirzepatide conversion chart provides specific equivalencies.
If you are switching between the two medications, your provider will determine the appropriate starting dose of the new medication. Do not attempt to calculate an equivalent dose yourself, as the two drugs work through different receptor pathways (semaglutide is a GLP-1 agonist; tirzepatide is a dual GIP/GLP-1 agonist) and their side effect profiles differ. The dosage comparison chart shows how the escalation schedules line up.
For semaglutide-specific dosing math, the semaglutide dosage calculator handles unit-to-mg conversions for that medication. And if you want to understand the broader landscape of next-generation options, guides on semaglutide versus tirzepatide versus retatrutide cover the differences in depth.
The role of injection technique in dose effectiveness
Even if you draw exactly 50 units and your math is perfect, injection technique can affect how much of that dose your body actually absorbs. This is a factor that many dosing guides overlook.
Subcutaneous injection depth matters. Tirzepatide is designed for subcutaneous (under the skin) injection, not intramuscular. Injecting too deeply, into muscle tissue, can alter absorption rates and peak concentration timing. Injecting too shallowly, into the dermal layer, can cause pooling at the surface and injection site reactions including redness, swelling, and itching.
The recommended injection sites include the abdomen (at least two inches from the navel), the front of the thigh, and the back of the upper arm. Rotating between sites reduces the risk of lipodystrophy and improves consistent absorption. The best injection site for weight loss results is often debated, but proper technique at any approved site is more important than the specific location.
For detailed step-by-step guidance, the GLP-1 injection guide and injection site overview cover proper technique comprehensively. The injection site reaction treatment guide helps if you experience localized side effects.
Timing your injection for best results
Does when you inject your 50 units matter? Yes, somewhat.
Tirzepatide is a once-weekly injection. The best time to take your tirzepatide shot depends on your personal routine and side effect patterns, but most providers recommend injecting at the same time on the same day each week. Consistency helps maintain stable blood levels.
Many users prefer injecting in the evening or before bed, especially during dose escalation phases where nausea is more likely. The logic is straightforward: if you sleep through the initial wave of side effects, they bother you less. Others prefer morning injections so they can monitor their response during waking hours. Neither approach is medically superior, and the best time for your GLP-1 shot is ultimately whatever time you will consistently remember.
Some people ask whether taking tirzepatide a day early is acceptable. The answer is generally yes, as long as you maintain approximately weekly spacing going forward. Taking it two days early or two days late is more concerning and should be discussed with your provider.
Storage and handling after drawing your dose
Once you draw 50 units from your vial, inject it promptly. Do not draw and then wait hours to inject, as the peptide can degrade when exposed to air and room temperature inside a syringe. If you must pre-draw doses (some people do this for travel), keep the prepared syringes refrigerated and use them within 24 hours.
Your vial itself requires proper storage. Tirzepatide needs refrigeration, typically between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius). How long it lasts in the fridge depends on whether it is reconstituted or pre-mixed, but most compounded formulations remain stable for 28 to 90 days when properly refrigerated.
What happens if your tirzepatide gets warm depends on the temperature and duration of exposure. Brief excursions to room temperature (during preparation and injection) are fine. Extended exposure to heat degrades the peptide, reducing potency and potentially making your carefully measured 50 units less effective than intended. Understanding how long compounded tirzepatide can be out of the fridge helps you plan around travel and daily routines.
Always check the expiration date on your vial. Using expired tirzepatide means your 50 units might contain significantly less active peptide than expected, and expired medication can also pose safety risks from degradation products. The shelf life of tirzepatide varies by formulation, so always defer to the date on your specific vial.
Microdosing: when less than 50 units might be the right approach
Not everyone follows the standard escalation schedule. Some providers and patients are exploring microdosing protocols, where smaller, more frequent doses replace the traditional weekly injection. In a microdosing framework, 50 units might actually be more than an entire week worth of medication distributed across multiple administrations.
The microdosing tirzepatide chart breaks down common protocols, while the microdose schedule guide explains the rationale and implementation. Some people use microdosing during initial titration to minimize side effects. Others use it for inflammation management at sub-therapeutic weight-loss doses.
If you are considering splitting your dose, the article on splitting tirzepatide into twice-weekly injections covers the practicalities and considerations. This approach means your individual draws would be less than 50 units (if 50 units is your total weekly dose), which some people find reduces gastrointestinal side effects while maintaining the same total weekly exposure.
Diet and lifestyle factors that affect your dose response
Two people can take exactly the same 50-unit draw from the same concentration vial and have very different experiences. Part of this comes from individual biology. Part comes from diet and lifestyle choices.
Foods to avoid while on tirzepatide include high-fat meals, greasy foods, and large portions that can amplify nausea. If you inject your 50 units and then eat a heavy meal, the GI side effects will feel significantly worse than if you eat the right foods on tirzepatide. Following a structured tirzepatide diet plan maximizes your results and minimizes discomfort regardless of your dose level.
Alcohol is another factor. Drinking on tirzepatide can intensify both the medication side effects and alcohol intoxication. If you do choose to drink, the guide on the best alcohol choices while on tirzepatide helps minimize negative interactions.
Certain supplements can support your tirzepatide protocol, particularly electrolytes, fiber, and nutrients that address common deficiencies during rapid weight loss. These do not change how much medication your 50 units delivers, but they can improve how well you tolerate and benefit from that dose.
Some users combine tirzepatide with other medications. Whether phentermine and tirzepatide together is appropriate depends on your medical situation and provider guidance. These combinations should always be discussed with a healthcare professional rather than self-directed.
What to expect at each dose level over time
Understanding the trajectory helps contextualize whether your 50-unit dose is appropriate for where you are in your journey.
First month (2.5 mg equivalent)
If your 50 units equals 2.5 mg, you are in the onboarding phase. After your first dose, you may notice subtle changes: slightly less hunger, feeling full sooner at meals, maybe some mild GI symptoms. Some people feel almost nothing at 2.5 mg and worry the medication is not working. That is normal. This dose is about adaptation, not results. Weight loss at this stage is modest, typically 2-4 pounds over four weeks, and some of that may be water weight.
Months 2-3 (5-7.5 mg equivalent)
If your 50 units delivers 5 mg or 7.5 mg, you are in the active therapeutic phase where tirzepatide starts working noticeably. The weight loss timeline typically shows more significant results during this period. Appetite suppression is more pronounced. Food noise (the constant background thinking about food) often diminishes significantly. Some people find that their relationship with food fundamentally shifts during these months.
Side effects may intensify temporarily with each dose increase. Dry mouth, constipation, and fatigue are common complaints at these mid-range doses. Most people find that symptoms peak in the first week after each escalation and then improve.
Months 4-5 (10-12.5 mg equivalent)
If your 50 units corresponds to 10 mg, you are on a higher dose that delivers more potent effects. Before-and-after results at this dose tier often show dramatic changes. Many clinical trial participants experienced 15-20% body weight reduction by this stage.
At higher doses, monitoring becomes more important. Joint pain, muscle pain, and hair thinning can emerge at these higher doses and should be discussed with your provider. Some people experience plateau effects where weight loss stalls temporarily. This does not necessarily mean the dose is insufficient. It may mean your body is adjusting.
Month 6 and beyond (15 mg equivalent)
If your 50 units equals 15 mg, you are at the maximum. This is where long-term maintenance planning becomes relevant. How to maintain weight loss after tirzepatide is a question you should start considering well before you decide to discontinue. And if you do decide to stop, understanding how to wean off tirzepatide properly can help prevent rapid weight regain.
Tirzepatide beyond weight loss: other benefits of your dose
Whether your 50 units delivers 2.5 mg or 15 mg, tirzepatide does more than suppress appetite. The benefits of tirzepatide beyond weight loss include improvements in blood sugar control, cardiovascular markers, blood pressure, and potentially anti-inflammatory effects.
Some people wonder whether tirzepatide gives you energy. The answer is nuanced. Early in treatment, fatigue is more common as your body adjusts. But as weight decreases and metabolic health improves, many people report increased energy levels. Others ask whether tirzepatide increases metabolism, and research suggests it may improve metabolic efficiency through multiple pathways beyond simple caloric restriction.
These broader benefits apply regardless of whether you are at the starting dose or the maximum. Lower doses may produce more subtle metabolic improvements, while higher doses tend to produce more dramatic changes across all measured parameters.
When to contact your healthcare provider about dosing
Self-education about dosing is valuable. But certain situations require professional medical guidance. Contact your provider if:
You are unsure about your vial concentration. Never guess. If the label is unclear, if you lost the pharmacy paperwork, or if you simply cannot determine the mg/mL, call the pharmacy or your provider before drawing any dose.
You experience severe side effects after any injection. Severe nausea lasting more than 72 hours, vomiting that prevents hydration, signs of pancreatitis (severe abdominal pain radiating to the back), or hypoglycemia symptoms all warrant immediate medical attention. These could indicate a dose that is too high for your current tolerance, whether you drew 50 units or any other amount.
You accidentally took a significantly wrong dose. If you realize after injecting that you drew from the wrong concentration or measured the wrong number of units, call your provider with the specifics: what concentration, how many units, and therefore how many milligrams you actually administered. This information helps them decide whether monitoring at home is sufficient or whether you need clinical evaluation.
Your hunger is not responding to your current dose after adequate time at that level. If you have been at the same dose for four or more weeks and feel no appetite suppression whatsoever, your provider may recommend advancing to the next dose tier. Do not increase your dose independently.
You want to discontinue or reduce your dose. Stopping tirzepatide abruptly can lead to rapid appetite return and weight regain. A supervised taper is generally recommended.
You are experiencing unexpected symptoms like weight gain while on tirzepatide, changes in menstrual patterns, or significant headaches that concern you.
The cost perspective: 50 units and your budget
Concentration affects cost efficiency as well as dosing. Higher concentration vials typically offer better per-milligram value because you get more doses from each vial. If your 50 units delivers 15 mg from a 30 mg/mL vial, you are getting the maximum dose from relatively little liquid, stretching your vial further than someone who needs 300 units (3 mL) of a 5 mg/mL solution for the same 15 mg dose.
For those researching cost options, the peptide cost calculator helps compare per-dose costs across different concentrations and suppliers. Articles on finding affordable tirzepatide and cost-effective compounded options cover the financial landscape in detail.
Emerging alternatives to traditional dosing
The GLP-1 and GIP agonist space is evolving rapidly. While understanding your current 50-unit tirzepatide dose is immediately practical, knowing about emerging options helps you have informed conversations with your provider about future possibilities.
Oral tirzepatide is in development, which would eliminate unit conversions entirely since the dose would be taken as a pill. The oral versus injection comparison covers the trade-offs between the two delivery methods.
Next-generation compounds are also entering clinical trials. Retatrutide is a triple receptor agonist (GIP, GLP-1, and glucagon) showing even more dramatic weight loss in early trials. Comparisons with mazdutide, survodutide, and CagriSema provide context on how the field is advancing. The duration of action for tirzepatide and these newer compounds varies, which could eventually change dosing frequency and unit calculations.
A complete safety checklist before drawing 50 units
Use this checklist every time you prepare a dose. It takes 30 seconds and could prevent a serious error.
Step 1: Check your vial label for the concentration (mg/mL). Read it twice.
Step 2: Calculate the milligram dose you will receive: 50 units = 0.5 mL x concentration. Compare this to your prescribed dose.
Step 3: Confirm you are using a U-100 insulin syringe.
Step 4: Check the vial for signs of degradation: particulate matter, unusual color, cloudiness (unless the formulation is normally not crystal clear, such as certain colored compounds).
Step 5: Verify the vial has not expired. Check the expiration date.
Step 6: Ensure the vial has been stored properly, refrigerated and protected from light.
Step 7: Draw to the 50-unit mark carefully. Remove air bubbles. Verify the measurement.
Step 8: Inject promptly using proper subcutaneous injection technique.
The complete guide to how many mg is 50 units on SeekPeptides provides additional conversion tables and calculation tools that complement this checklist.
Understanding your results with 50 units
After several weeks at your dose, assess your progress thoughtfully. Results vary enormously between individuals, and comparing your experience to online success stories can be misleading.
Weight loss averages from clinical trials provide useful benchmarks, but they are averages. Some people lose significantly more than average. Others lose less. The before-and-after weight loss results showcase the range of outcomes, while male-specific results address the different patterns men typically experience. How long it takes for tirzepatide to work also varies by individual, dose level, and what "working" means to you.
If your 50 units delivers a starting dose and you are not seeing dramatic results, patience is the answer, not drawing more units. If your 50 units delivers a high dose and you are still not progressing, the answer is a conversation with your provider, not an even higher draw. Self-directed dose escalation is one of the most dangerous things you can do with any injectable medication.
Stacking and combination considerations
Some people use tirzepatide as part of a broader peptide protocol. While this article focuses specifically on whether 50 units is a lot, understanding how tirzepatide fits into combination approaches provides useful context.
Compounded formulations may include additional compounds like glycine and B12 together or methylcobalamin. These additions do not change your tirzepatide dose calculation. If the label says 10 mg/mL tirzepatide, then 50 units still delivers 5 mg of tirzepatide regardless of what other compounds are in the solution. The other ingredients have their own dosing considerations, but they do not alter the tirzepatide math.
The peptide stack calculator at SeekPeptides can help you understand how different compounds interact, and the tirzepatide with glycine guide explains the rationale behind this particular combination.
Special populations and 50-unit dosing considerations
Certain groups need extra attention when it comes to tirzepatide dosing.
People with type 2 diabetes using tirzepatide alongside other diabetes medications face hypoglycemia risks that those using it for weight loss alone do not. If you take insulin or sulfonylureas, a 50-unit draw of tirzepatide that delivers a higher dose can compound the blood-sugar-lowering effects and create dangerously low glucose levels.
Women who are breastfeeding should know that tirzepatide during breastfeeding is not recommended due to insufficient safety data. If you are in this situation and have tirzepatide on hand, do not use it without explicit provider approval.
People with menstrual cycle considerations may notice that their dose response varies with their cycle. Some women report increased nausea during certain phases. This does not mean the dose is wrong. It means the body processes the medication differently depending on hormonal fluctuations.
For patients taking additional medications like phentermine alongside tirzepatide, the combined effects can make a standard dose feel stronger. Always disclose all medications to your provider so they can adjust your tirzepatide dose accordingly.
What healthcare providers wish patients understood about units
After speaking with healthcare professionals who prescribe compounded tirzepatide regularly, several themes emerge about what they wish every patient understood before their first injection.
The number one concern is that patients treat units as if they are a universal dosing language. They are not. A provider who says "take 50 units" without specifying the concentration is giving incomplete instructions, and unfortunately, this happens more often than it should, especially in telehealth settings where communication can be compressed. If your prescription says a milligram dose but your pharmacy labeled the vial in mg/mL, and nobody explicitly told you how many units to draw, you have a gap that needs filling before you inject anything.
Providers also emphasize that dose escalation is not a race. Some patients view the escalation schedule as a countdown to their "real" dose and rush through the lower tiers. They draw more units to get more milligrams because they feel the starting dose is not producing dramatic enough results. This impatience is understandable but counterproductive.
The GI adaptation that happens at each dose tier is what allows you to tolerate higher doses later. Skipping steps does not get you to results faster. It gets you to nausea and vomiting faster.
Another common concern: patients who share dosing information with friends or online communities without accounting for concentration differences. Someone might post "I take 50 units and feel great" without mentioning their vial concentration. Another person reads that, draws 50 units from their different-concentration vial, and has a completely different experience. Context-free dosing advice is one of the most dangerous things circulating in online GLP-1 communities. Always verify that any dosing information you receive specifies both units AND concentration, or ideally, the milligram dose directly.
Finally, providers stress the importance of follow-up appointments. Your 50-unit dose should be re-evaluated periodically. As you lose weight, your dose-to-body-weight ratio changes. As your metabolism adapts, the same dose may produce different effects. Regular check-ins allow your provider to adjust your protocol based on current data rather than the assumptions made when you first started.
The psychology of dose anxiety
Searching "is 50 units of tirzepatide a lot" often reflects something deeper than a simple math question. It reflects anxiety about getting the dose right, about making a mistake, about taking too much or too little of a medication that feels consequential. That anxiety is valid. And it is worth addressing directly.
Many people starting injectable medications experience significant nervousness. The act of self-injection itself is unfamiliar and can feel intimidating. Adding dose calculation on top of that amplifies the stress. Some people check and recheck their syringe five or six times before injecting, caught in a loop of doubt about whether they measured correctly.
Here is what helps. Education reduces anxiety. The fact that you are reading this article, learning the conversion formula, understanding the relationship between units and milligrams, that is the single best thing you can do for your confidence. Knowledge replaces fear. When you understand that 50 units always equals 0.5 mL, and that multiplying by your concentration gives you the milligram dose, the mystery dissolves. You are left with simple, verifiable math.
Practice also helps. Your third injection will feel less stressful than your first. Your tenth will feel routine. The mechanical skills of drawing from a vial, clearing air bubbles, and reading syringe markings improve quickly with repetition. If you are on your first or second injection and feeling overwhelmed, know that this feeling is temporary. It gets easier.
And if the anxiety persists despite education and practice, tell your provider. Some offices offer in-person injection training where a nurse walks you through the entire process, from reconstitution to injection, while you do it under supervision. That hands-on experience often resolves residual doubt in ways that articles and calculators cannot.
Frequently asked questions
Is 50 units of tirzepatide the same as 50 mg?
No. This is the most critical distinction in tirzepatide dosing. Fifty units is a volume measurement (0.5 mL on a U-100 insulin syringe), not a milligram measurement. The actual milligram dose depends on your vial concentration. At 10 mg/mL, 50 units equals 5 mg. At 20 mg/mL, 50 units equals 10 mg. The complete 50 units to mg conversion guide covers every concentration scenario.
Can 50 units of tirzepatide be dangerous?
It depends entirely on concentration and your current dose tier. If your vial is 30 mg/mL, 50 units delivers 15 mg, which is the maximum therapeutic dose and would be dangerous for anyone who has not spent months gradually titrating to that level. If your vial is 5 mg/mL, 50 units delivers only 2.5 mg, which is the standard starting dose and is generally well-tolerated even by first-time users.
How do I know what concentration my vial is?
Check the label on your vial. It should list the concentration in mg/mL (milligrams per milliliter). If it lists total content (e.g., "30 mg total"), divide by the total volume to calculate concentration. If you reconstituted a lyophilized vial yourself, the concentration depends on how much bacteriostatic water you added. If you are still uncertain, call the pharmacy that dispensed it.
Should I draw 50 units if my provider said to take 5 mg?
Only if your vial concentration makes 50 units equal to 5 mg. At 10 mg/mL, 50 units equals 5 mg, so yes. At 5 mg/mL, you would need 100 units for 5 mg. At 20 mg/mL, you would need only 25 units for 5 mg. Always calculate based on your specific concentration, and confirm with the dosage calculator if you are unsure.
What happens if I accidentally inject 50 units when I should have injected 25?
You have taken double your intended dose. Do not panic, but do contact your provider. They will advise based on what milligram dose you actually received and your history with the medication. Expect increased side effects, particularly nausea and reduced appetite, over the following 3-5 days. Stay well hydrated, eat bland foods when possible, and monitor for severe symptoms that would require medical attention.
Is 50 units a normal amount to draw from a syringe?
Fifty units (0.5 mL) is a very common draw volume for subcutaneous injections. It is half the capacity of a standard 1 mL insulin syringe. The volume itself is not unusual. What makes it "normal" or "abnormal" for tirzepatide is whether the resulting milligram dose matches your prescription and current escalation stage.
Can I use the same 50-unit measurement if I switch to semaglutide?
No. Semaglutide has different concentrations and a different dose escalation schedule. Fifty units of semaglutide at various concentrations delivers different milligram amounts than tirzepatide, and the therapeutic ranges are different. If you are switching between medications, your provider will prescribe a specific starting dose for the new medication. Use the semaglutide dosage calculator for semaglutide-specific conversions, and review the semaglutide dosing in units guide.
How many weeks should I stay at my current 50-unit dose before increasing?
The standard protocol recommends at least four weeks at each dose tier before escalating. Some providers extend this to six or eight weeks, especially if side effects are still prominent. Do not increase your dose faster than your provider recommends, even if you feel you are tolerating it well. The four-week minimum exists to allow full physiological adaptation before adding more medication.
External resources
Mayo Clinic: Tirzepatide drug information, comprehensive overview of usage, precautions, and side effects from one of the most trusted medical institutions.
FDA prescribing information for Mounjaro (tirzepatide), the official label containing approved dosing, contraindications, and clinical trial data.
NIH MedlinePlus: Tirzepatide injection, patient-friendly information on proper use, storage, and side effects from the National Institutes of Health.
PubMed: Tirzepatide weight loss research, searchable database of peer-reviewed studies on tirzepatide efficacy and safety.
SURMOUNT-1 trial (NEJM), the landmark clinical trial demonstrating tirzepatide weight loss outcomes at 5 mg, 10 mg, and 15 mg doses.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay accurate, your concentrations stay clear, and your results stay consistent.