Feb 22, 2026
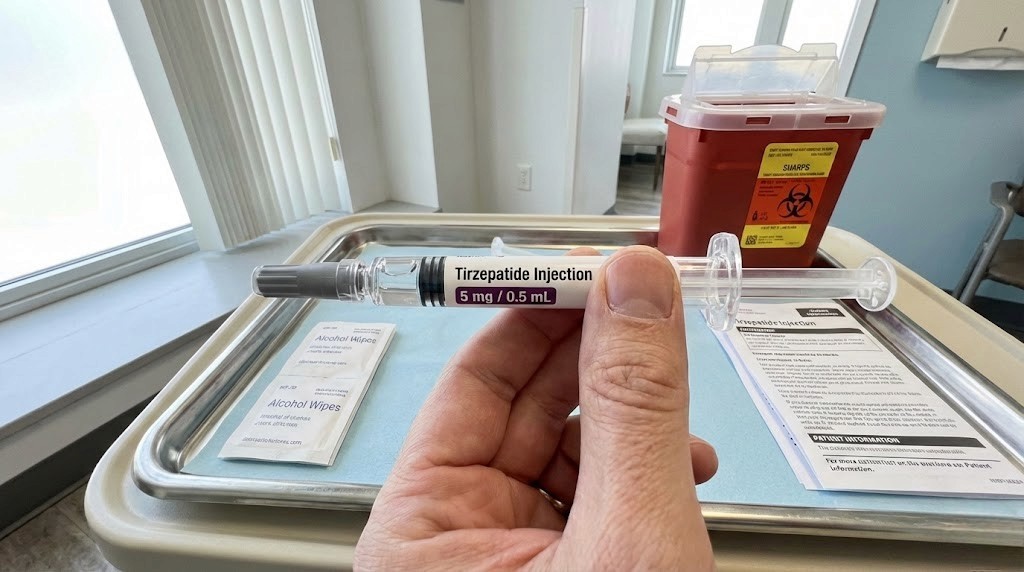
What if the problem is not your tirzepatide? What if the real issue sits in your hand, right now, every time you draw a dose? The syringe you choose, how you read it, and whether you understand what those tiny lines actually mean determines whether you get 2.5 mg or 5 mg from the same vial.
That is not a rounding error. That is a doubled dose. Or a halved one. And the syringe itself will never warn you.
Most guides jump straight to conversion charts. Milligrams to units. Units to milliliters. Helpful, sure. But they skip the part that actually causes the mistakes: the physical syringe in your hand. Which size to grab. Which markings to trust. How to read the liquid level without introducing a 10% error from a bad angle. The practical, tactile knowledge that separates accurate dosing from expensive guesswork.
This guide covers everything about tirzepatide syringe dosage that the conversion charts leave out. You will learn which syringe size matches your dose tier, how to read markings on each syringe type, the critical difference between insulin and tuberculin syringes, and the step-by-step technique for drawing from a vial without wasting a drop. SeekPeptides created this resource because dosing accuracy starts with the right tool, not just the right math.
Why the syringe matters more than most researchers realize
A syringe is not a syringe is not a syringe. Not when fractions of a milliliter separate a therapeutic dose from a problematic one.
Consider this scenario. You have a 20 mg/mL vial of compounded tirzepatide. Your target dose is 2.5 mg. That requires 12.5 units on the syringe. Now look at the syringe in your hand. If you are holding a 1.0 mL syringe where each tick mark represents 2 units, you literally cannot measure 12.5 units. You are forced to round to 12 or 14 units. At 20 mg/mL, that rounding error means you inject either 2.4 mg or 2.8 mg. Every single week.
But grab a 0.3 mL syringe with half-unit markings. Now 12.5 units falls on an actual line. No rounding. No guessing. No accumulated error over months of injections.
The right syringe eliminates the problem before it starts. The wrong syringe guarantees imprecision that compounds with every injection. Understanding tirzepatide dosing in units means nothing if the tool measuring those units cannot hit the mark.
The three insulin syringe sizes and when to use each
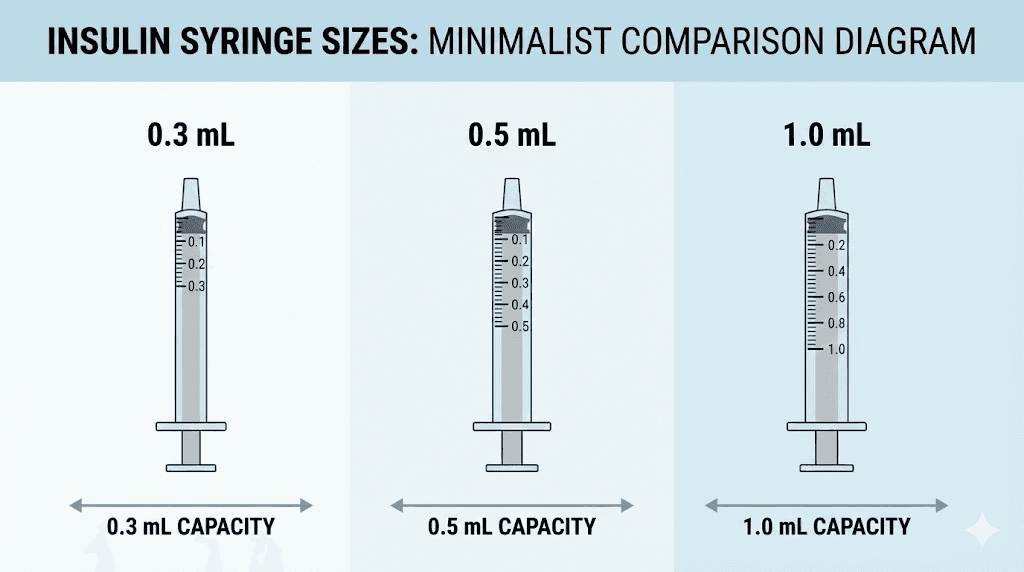
All standard insulin syringes sold in the United States follow the U-100 calibration. That means 100 units equals 1 mL. Always. This ratio does not change across syringe sizes. What changes is the maximum capacity, the spacing between tick marks, and the precision of your measurement.
0.3 mL syringe (30 units maximum)
This is the precision instrument of the three. It holds up to 30 units (0.30 mL) and typically features half-unit markings. Each full tick mark represents 1 unit. Each half tick represents 0.5 units. The barrel is narrow, which means even small volume changes produce visible plunger movement.
Use the 0.3 mL syringe when:
Your dose falls below 30 units
You are working with high-concentration vials (15 mg/mL, 20 mg/mL, or above) where small unit differences create large milligram swings
You are microdosing tirzepatide at sub-2.5 mg amounts
Precision matters more than convenience
The 0.3 mL syringe shines during early titration. A starting dose of 2.5 mg from a 10 mg/mL vial requires 25 units. That fits comfortably within the 30-unit capacity, and the half-unit markings let you adjust by as little as 0.05 mg at that concentration. For researchers who track their tirzepatide dose progression carefully, this level of control matters.
0.5 mL syringe (50 units maximum)
The workhorse. It holds up to 50 units (0.50 mL) with markings at every 1-unit increment. Some versions include half-unit markings, though this is less common than with the 0.3 mL size. The barrel width falls between the other two sizes, offering a reasonable balance of capacity and readability.
Use the 0.5 mL syringe when:
Your dose falls between 25 and 50 units
You are in mid-titration at 5 mg per week from a 10 mg/mL vial (exactly 50 units)
You want a built-in safety ceiling that prevents drawing more than 0.5 mL accidentally
At 10 mg/mL concentration, which is the most common compounded tirzepatide concentration, the 0.5 mL syringe covers the 2.5 mg through 5.0 mg dose range cleanly. That maps to the first two titration tiers in standard protocols, which is where most researchers spend their first eight weeks.
1.0 mL syringe (100 units maximum)
The large-capacity option. It holds a full 100 units (1.00 mL). Tick marks typically appear at every 2-unit increment, though some brands mark every unit. The wider barrel means small volume changes produce less visible plunger movement, making precise measurement slightly harder at low volumes.
Use the 1.0 mL syringe when:
Your dose exceeds 50 units
You are at higher titration tiers (7.5 mg or above from a 10 mg/mL vial)
You are working with lower concentration vials (5 mg/mL) where a 5 mg dose requires 100 units
A word of caution. Many researchers default to the 1.0 mL syringe because it is the most commonly available and they figure bigger is more versatile. That logic backfires at low doses. Drawing 12 units on a 1.0 mL syringe with 2-unit markings means eyeballing a spot between the 12 and 14 lines. On a 0.3 mL syringe, 12 units sits on a clearly marked line with half-unit precision available. For standard 2.5 mg starting doses, the smaller syringe is almost always the better choice.
Syringe size | Maximum capacity | Typical tick marks | Best concentration range | Best dose range |
|---|---|---|---|---|
0.3 mL (30 units) | 0.30 mL | Every 0.5 or 1 unit | 10-40 mg/mL | 0.5-3.0 mg (at 10 mg/mL) |
0.5 mL (50 units) | 0.50 mL | Every 1 unit | 5-20 mg/mL | 2.5-5.0 mg (at 10 mg/mL) |
1.0 mL (100 units) | 1.00 mL | Every 1 or 2 units | 5-10 mg/mL | 5.0-10.0 mg (at 10 mg/mL) |
The right syringe for your situation depends on two numbers: your dose in units and your vial concentration. Once you know both, the table above tells you which syringe delivers the best precision for your specific scenario.
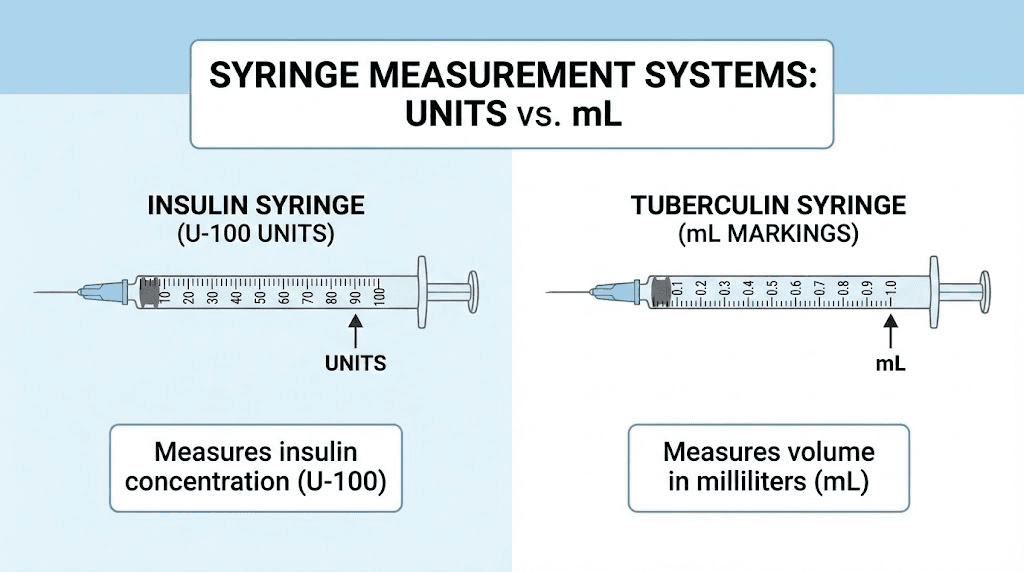
Insulin syringe versus tuberculin syringe: a critical distinction
This is where dangerous mistakes happen. Insulin syringes and tuberculin syringes look almost identical. Same general shape. Same small barrel. Same fine needle. But their markings mean completely different things.
An insulin syringe (U-100) marks volume in units. One hundred units equals 1 mL.
A tuberculin syringe marks volume in milliliters directly. The numbers on the barrel represent milliliters and tenths of a milliliter.
Here is where it gets dangerous. If you pick up a tuberculin syringe by mistake and draw to the "50" mark thinking you are drawing 50 units (0.50 mL), you are actually drawing 5.0 mL, which is ten times the intended volume. At a 10 mg/mL concentration, that would be 50 mg of tirzepatide instead of 5 mg. Ten times your dose.
This is not a hypothetical scenario. Medical literature documents cases of significant dosing errors from syringe-type confusion. The consequences with tirzepatide include severe nausea, vomiting, and gastrointestinal distress that can last days. Understanding the difference between these syringe types is as important as understanding tirzepatide side effects at normal doses.
How to tell them apart
Check the label on the syringe packaging. Insulin syringes are marked "U-100" and display unit measurements. Tuberculin syringes display "mL" markings. If you cannot find a label, look at the barrel itself. Insulin syringes show numbers like 10, 20, 30, 40, 50 (units). Tuberculin syringes show numbers like 0.1, 0.2, 0.3, 0.4, 0.5 (milliliters).
When in doubt, do not inject. Verify first. A moment of checking beats hours of headaches and nausea from a dosing error.
Can you use a tuberculin syringe intentionally?
Yes. Some researchers prefer tuberculin syringes because the milliliter markings eliminate the extra mental step of converting units to volume. If your dose requires 0.25 mL, you simply draw to 0.25 on a tuberculin syringe. No division by 100 needed.
The official Mounjaro product monograph states that patients may use either a tuberculin or insulin syringe with a 28 to 31 gauge needle appropriate for subcutaneous injection. Both types work. The danger exists only when you confuse one for the other.
If you choose to use a tuberculin syringe, convert your dose to milliliters first using this formula:
mL = desired mg / concentration in mg/mL
For 5 mg from a 10 mg/mL vial: 5 / 10 = 0.50 mL
Then draw to 0.50 on the tuberculin syringe. The SeekPeptides peptide calculator handles this conversion instantly if you prefer not to do manual math.
How to read an insulin syringe accurately
Reading a syringe sounds simple. It is not. Researchers who have been injecting for months still make reading errors that shift their dose by 5-10%. The errors are small enough to go unnoticed, large enough to affect results over time.
The meniscus rule
When liquid sits in a syringe barrel, the surface curves upward at the edges where it contacts the barrel wall. This curve is called the meniscus. The correct reading comes from the flat bottom of the curve, not the raised edges.
Hold the syringe at eye level with the needle pointing up (or to the side, with the markings facing you). Find the bottom of the liquid curve. That is your volume. Reading from the top of the meniscus adds approximately 1-2 units of false volume to your measurement.
At low concentrations, a 2-unit error might mean only 0.1 mg difference. Insignificant. At higher concentrations like 20 mg/mL, that same 2-unit error translates to 0.4 mg. Over 12 weeks of weekly injections, that accumulated error equals an entire extra dose worth of tirzepatide. Researchers tracking their tirzepatide results should know whether inconsistent measurements might explain inconsistent outcomes.
Parallax error
Look at your syringe from above and the plunger appears higher than it really is. Look from below and it appears lower. Only a straight-on, eye-level reading gives an accurate result.
The fix is simple. Hold the syringe horizontally at eye level. Let your eyes align with the target unit marking. Read the bottom of the meniscus at that marking. Do this every single time.
Reading different syringe sizes
On a 0.3 mL syringe with half-unit markings, each long line represents 1 unit and each short line represents 0.5 units. If your target is 12.5 units, you draw to the short line between 12 and 13. Precise.
On a 0.5 mL syringe with single-unit markings, each line represents 1 unit. Drawing 25 units means aligning the plunger with the 25 line. The numbers might appear every 5 or 10 units (5, 10, 15, 20, 25...) with unmarked lines between them. Count carefully from the nearest labeled number.
On a 1.0 mL syringe with 2-unit markings, each line represents 2 units. Drawing 50 units means aligning with the 50 line. But drawing 25 units means estimating the midpoint between the 24 and 26 lines. This is where the 1.0 mL syringe loses precision compared to smaller sizes.
Understanding these differences matters whether you are working with 5 mg tirzepatide doses or 7.5 mg doses. The syringe determines your precision ceiling regardless of how well you understand the math.
Tirzepatide dose conversion by syringe and concentration
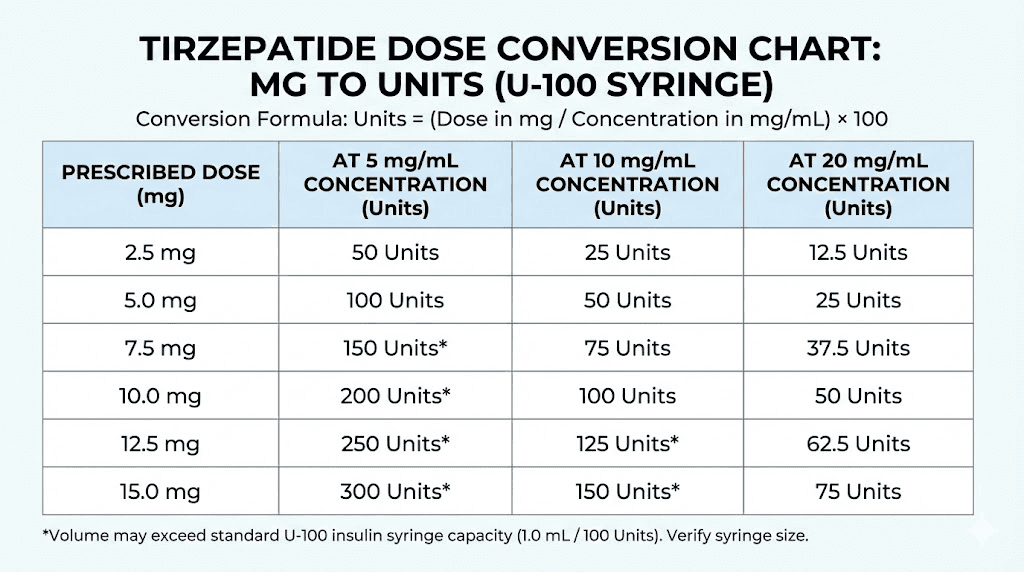
Every dose conversion starts with two numbers: your vial concentration (mg/mL) and your target dose (mg). The formula that connects them is the same regardless of syringe size:
units = (desired mg / concentration in mg/mL) x 100
The syringe size determines whether you can measure that calculated number of units accurately. Here are the complete reference charts organized by the most common concentrations, showing exactly where each dose falls on each syringe type.
At 5 mg/mL concentration
Target dose | Units needed | mL volume | Best syringe | Precision notes |
|---|---|---|---|---|
1.25 mg | 25 units | 0.25 mL | 0.3 mL or 0.5 mL | Falls on a line on both |
2.5 mg | 50 units | 0.50 mL | 0.5 mL (exactly full) | Maxes out the 0.5 mL syringe |
5.0 mg | 100 units | 1.00 mL | 1.0 mL (exactly full) | Full syringe, no room for error |
7.5 mg | 150 units | 1.50 mL | N/A (exceeds all syringes) | Need higher concentration vial |
Notice the limitation. At 5 mg/mL, anything above 5.0 mg per dose exceeds the 1.0 mL syringe capacity. Researchers on higher tirzepatide weight loss doses need a more concentrated vial to keep injection volumes manageable.
At 10 mg/mL concentration (most common)
Target dose | Units needed | mL volume | Best syringe | Precision notes |
|---|---|---|---|---|
1.0 mg | 10 units | 0.10 mL | 0.3 mL | Half-unit precision available |
2.5 mg | 25 units | 0.25 mL | 0.3 mL or 0.5 mL | Clean line on both |
5.0 mg | 50 units | 0.50 mL | 0.5 mL | Exactly full capacity |
7.5 mg | 75 units | 0.75 mL | 1.0 mL | Falls on a line on most 1.0 mL syringes |
10.0 mg | 100 units | 1.00 mL | 1.0 mL | Full syringe |
At 10 mg/mL, the math stays clean across all standard dose tiers. This is exactly why most compounding pharmacies default to this concentration. The tirzepatide dosage chart in units aligns neatly with syringe markings, reducing the chance of measurement errors at every dose tier.
At 20 mg/mL concentration
Target dose | Units needed | mL volume | Best syringe | Precision notes |
|---|---|---|---|---|
2.5 mg | 12.5 units | 0.125 mL | 0.3 mL (half-unit markings required) | Only measurable with half-unit syringe |
5.0 mg | 25 units | 0.3 mL or 0.5 mL | Clean line on both | |
7.5 mg | 37.5 units | 0.375 mL | 0.5 mL (with half-unit markings) | Requires precision |
10.0 mg | 50 units | 0.50 mL | 0.5 mL | Exactly full capacity |
15.0 mg | 75 units | 0.75 mL | 1.0 mL | Falls on a line |
Higher concentrations squeeze more tirzepatide into less volume. That means smaller injection volumes and better comfort, but it also means each unit on your syringe carries more weight. A 2-unit error at 10 mg/mL costs you 0.2 mg. That same 2-unit error at 20 mg/mL costs 0.4 mg. At 40 mg/mL, it costs 0.8 mg. The higher the concentration, the more precision matters, and the more you need the right syringe for the job.
For detailed conversion math at every concentration, the 50 units of tirzepatide conversion guide walks through the formula step by step.
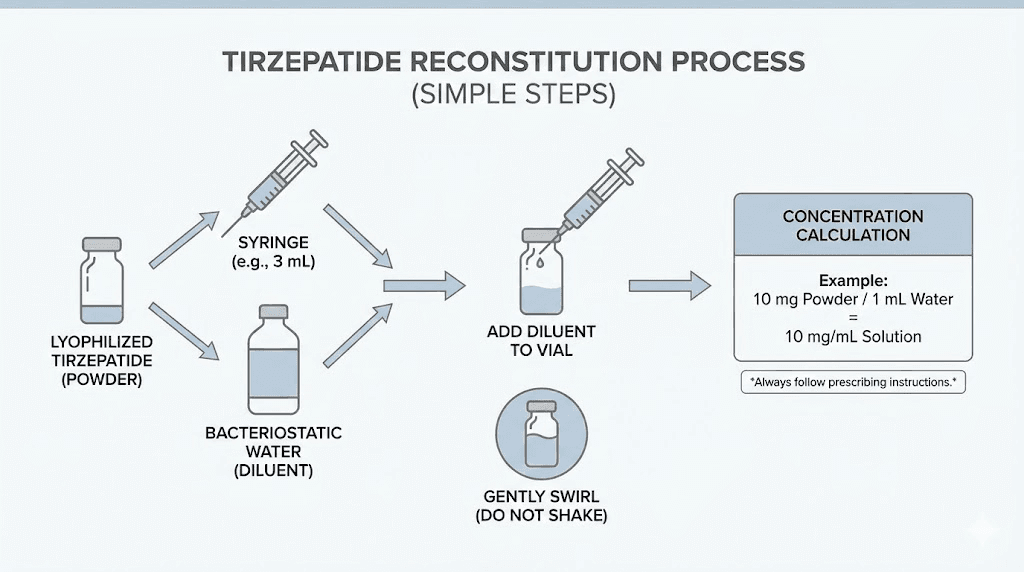
Step-by-step guide to drawing tirzepatide from a vial
Knowing which syringe to use is half the equation. Using it correctly is the other half. This process applies whether you are drawing from a compounded multi-dose vial or a vial you reconstituted yourself from lyophilized powder.
What you need
Gather everything before you start. Interruptions mid-draw lead to contamination and measurement errors.
Your tirzepatide vial (check the concentration on the label)
The correct syringe (based on your dose calculation)
Alcohol swabs (for the vial stopper and injection site)
A sharps disposal container
A flat, clean surface with good lighting
Step 1: verify your dose calculation
Before touching the syringe, confirm your numbers. Read the concentration on the vial. Calculate your units using the formula: units = (desired mg / concentration) x 100. Verify with the peptide calculator or a second manual calculation. Two methods. One answer. If they disagree, figure out why before proceeding.
Step 2: clean the vial stopper
Wipe the rubber stopper with an alcohol swab. Let it dry for a few seconds. This step matters more than you think. Every needle puncture introduces a potential contamination pathway. Alcohol reduces surface bacteria to near zero when given a moment to evaporate.
Step 3: draw air into the syringe
Pull the plunger back to the number matching your target units. This draws room air into the barrel. You will inject this air into the vial to equalize pressure, making it easier to draw liquid out. Without this step, the vacuum inside the vial fights against your draw, making precise measurement harder.
Step 4: inject air into the vial
Insert the needle through the rubber stopper. Push the plunger to inject the air. Keep the needle in the vial.
Step 5: invert the vial and draw your dose
Turn the vial upside down so the stopper faces the floor and the syringe points upward. Pull the plunger slowly past your target volume by 5-10 extra units. You will remove the excess after dealing with air bubbles.
Step 6: remove air bubbles
With the vial still inverted, tap the syringe barrel gently with your fingernail. Air bubbles rise to the top (toward the needle, which is now pointing upward into the vial). Keep tapping until all visible bubbles collect near the needle tip.
Push the plunger slowly to push the air (and any excess liquid) back into the vial. Stop when the plunger reaches your exact target unit marking. The liquid surface should sit flat at your target line with no visible bubbles below it.
Step 7: verify the measurement
With the needle still in the inverted vial, check your reading. Eye level. Bottom of the meniscus. Exact line. If you are over, push a tiny bit back into the vial. If you are under, pull a tiny bit more. Take the time to get this right. Rushing this step is the single biggest source of dosing inconsistency.
Step 8: withdraw the needle
Once your measurement is confirmed, pull the needle straight out of the vial stopper. Do not twist or bend. Set the vial upright. Cap the needle if you are not injecting immediately, using the one-handed scoop technique to avoid needle sticks.
This technique applies identically whether you are working with tirzepatide, semaglutide, or any other injectable GLP-1 peptide. The mechanics of drawing from a vial are universal. What changes is the math that determines how far you pull the plunger.
Needle gauge selection for tirzepatide injections
The needle attached to your syringe affects comfort, flow rate, and depth of injection. Getting this right makes the difference between a barely noticeable injection and one that leaves a bruise.
Understanding gauge numbers
Gauge measures needle thickness. Higher numbers mean thinner needles. A 31-gauge needle is thinner than a 27-gauge needle. Thinner needles hurt less going in but draw liquid more slowly. Thicker needles draw faster but cause more sensation at the injection site.
Needle gauge | Thickness | Comfort level | Draw speed | Best for |
|---|---|---|---|---|
27 gauge | Thickest common option | Moderate | Fast | Viscous solutions, large volumes |
29 gauge | Medium | Good | Moderate | Most tirzepatide formulations |
30 gauge | Fine | Very good | Slower | Standard aqueous solutions |
31 gauge | Finest common option | Excellent | Slowest | Low-volume injections, sensitive individuals |
For most compounded tirzepatide formulations, a 29 or 30 gauge needle works well. The solution is typically aqueous (water-based) and flows easily through fine needles. Some compounded formulations that include additional compounds like glycine and B12 or niacinamide may be slightly more viscous. If drawing takes noticeably long with a 31-gauge needle, stepping down to 29 gauge eliminates the issue without significantly increasing discomfort.
Needle length and subcutaneous depth
Tirzepatide is a subcutaneous injection. The needle must reach the fatty tissue layer beneath the skin but not penetrate into muscle. For most adults, needle lengths between 4 mm and 8 mm achieve this reliably.
The most common insulin syringe needle lengths:
4-5 mm: Suitable for lean individuals. Insert at 90 degrees without pinching skin.
6 mm: Works for most body types at 90 degrees.
8 mm: May require a skin pinch or 45-degree angle to avoid intramuscular injection in leaner individuals.
12.7 mm (1/2 inch): Always requires a skin pinch. Common on older syringe designs but largely replaced by shorter options.
For GLP-1 injection sites including the abdomen, thigh, and upper arm, a 5-6 mm needle at 90 degrees covers the vast majority of body compositions. If you can pinch at least 2 inches of skin at your injection site, a 6 mm needle at 90 degrees will reliably deposit the medication in the subcutaneous layer.
Dead space, wasted peptide, and syringe efficiency
Every syringe wastes a small amount of medication. Understanding this waste helps you calculate the true cost per dose and choose syringes that minimize losses.
What is dead space
Dead space is the volume of liquid that remains trapped in the needle hub and the gap between the bottom of the plunger and the needle opening after injection. You push the plunger all the way down. You think you injected everything. But a tiny amount of liquid never leaves the syringe.
In standard insulin syringes, dead space ranges from 0.5 to 7 microliters depending on the design. That sounds trivial. Over the life of a vial, it adds up.
The math on wasted tirzepatide
Suppose your syringe has 5 microliters (0.005 mL) of dead space. At 10 mg/mL, each injection wastes 0.05 mg of tirzepatide. Over 10 injections from a multi-dose vial, you lose 0.5 mg total. That is a meaningful fraction of a dose.
At 20 mg/mL, the same dead space wastes 0.1 mg per injection, or 1.0 mg over 10 draws. At higher concentrations, dead space becomes a real cost factor worth addressing.
Low dead space syringes
Low dead space (LDS) syringes are engineered to minimize the volume trapped after injection. They achieve this through a modified plunger tip that fits more tightly against the needle hub, reducing dead space to as little as 0.5-1 microliter.
LDS syringes cost slightly more than standard insulin syringes. Whether the premium is worth it depends on your concentration and vial size. For researchers using small, expensive vials of high-concentration tirzepatide, LDS syringes recover enough peptide to justify the extra cost. For researchers using large vials at lower concentrations, the savings are marginal.
The calculation is straightforward. Multiply your dead space volume by your concentration by the number of draws per vial. If the resulting milligram loss bothers you or exceeds the price difference of LDS syringes, make the switch. If not, standard syringes serve just fine.
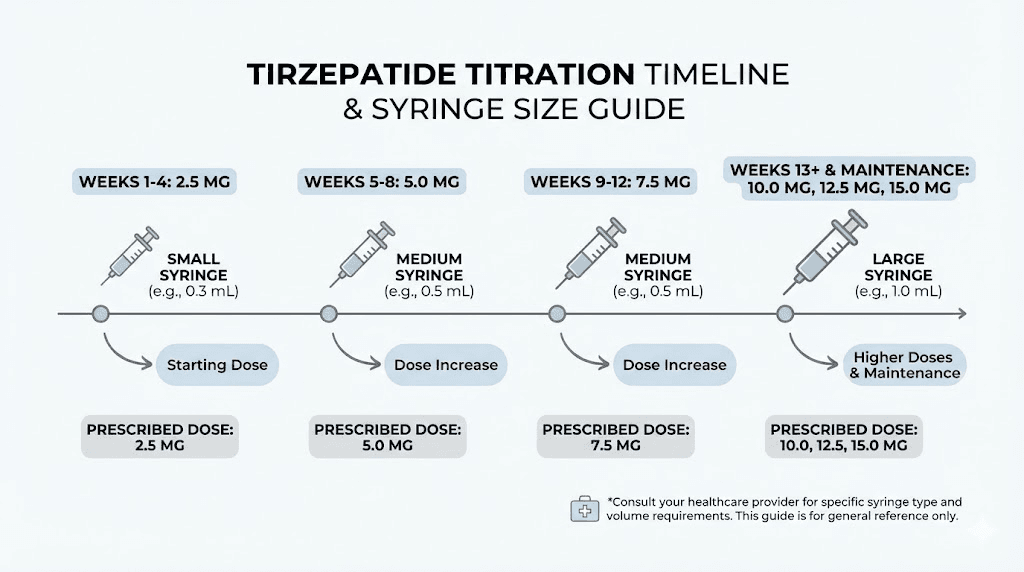
Matching your syringe to your tirzepatide dose tier
As you progress through tirzepatide titration, your optimal syringe changes. Sticking with the same syringe from week 1 through week 20 means either starting with too much capacity or ending with too little. Smart researchers keep two syringe sizes on hand and switch as their dose evolves.
Starting dose: 2.5 mg (weeks 1-4)
At 10 mg/mL, the starting dose requires 25 units. Both the 0.3 mL and 0.5 mL syringes handle this cleanly. The 0.3 mL syringe offers superior precision if you anticipate any dose adjustments below 2.5 mg. Some researchers start even lower with microdosing approaches, where the 0.3 mL syringe is essential.
At 20 mg/mL, the starting dose requires only 12.5 units. You absolutely need the 0.3 mL syringe with half-unit markings here. Trying to eyeball 12.5 units on a 1.0 mL syringe with 2-unit markings is a recipe for inconsistent dosing.
Second tier: 5.0 mg (weeks 5-8)
At 10 mg/mL, 5.0 mg requires 50 units. The 0.5 mL syringe is ideal here, drawing right to its maximum capacity. The 1.0 mL syringe works but offers less precision at this volume. The 0.3 mL syringe cannot hold enough.
This is typically the dose tier where researchers begin to notice significant appetite suppression and where tirzepatide appetite effects become most pronounced. Getting the dose exactly right at this phase matters because it establishes your baseline response before deciding whether to increase further.
Third tier: 7.5 mg (weeks 9-12)
At 10 mg/mL, 7.5 mg requires 75 units. You need the 1.0 mL syringe. Neither smaller size has enough capacity. At 20 mg/mL, the same dose requires only 37.5 units, which fits in a 0.5 mL syringe. This is one practical advantage of higher-concentration vials as your dose increases.
Higher tiers: 10-15 mg (weeks 13+)
At 10 mg/mL, 10 mg requires 100 units (a full 1.0 mL syringe) and 15 mg would require 150 units (exceeds all standard syringe sizes). Researchers on these higher doses typically use 20 mg/mL or higher concentrations to keep volumes manageable. At 20 mg/mL, 10 mg needs only 50 units and 15 mg needs 75 units, both of which fit standard syringes.
The tirzepatide versus semaglutide dosage comparison shows why concentration management becomes critical at higher doses. Tirzepatide dose ranges (2.5-15 mg) are significantly higher than semaglutide dose ranges (0.25-2.4 mg), which means syringe capacity becomes a limiting factor much earlier with tirzepatide.
Drawing from multi-dose vials safely
Compounded tirzepatide typically comes in multi-dose vials containing enough medication for several weeks of injections. Each time you puncture the rubber stopper, you introduce a small contamination risk that the bacteriostatic water in the solution helps manage. But bacteriostatic water has limits.
Sterile technique fundamentals
Clean the vial stopper with alcohol before every single draw. Not just the first time. Every time. Use a new syringe and needle for every injection. Never reuse needles, even on the same vial. A used needle carries bacteria from your skin and potentially from the subcutaneous tissue back into the vial.
Work on a clean, flat surface with good lighting. Avoid drawing your dose in a rush, in the car, or in other environments where contamination risk increases. A dedicated space for injection preparation, even just a clean bathroom counter, reduces the chance of introducing bacteria.
Tracking doses per vial
Know how many doses your vial contains. This prevents the frustration of running out mid-protocol and helps you time refill orders.
Vial size (total mg) | Concentration | Total volume | Doses at 2.5 mg | Doses at 5.0 mg | Doses at 10.0 mg |
|---|---|---|---|---|---|
10 mg | 10 mg/mL | 1.0 mL | 4 | 2 | 1 |
20 mg | 10 mg/mL | 2.0 mL | 8 | 4 | 2 |
30 mg | 10 mg/mL | 3.0 mL | 12 | 6 | 3 |
60 mg | 10 mg/mL | 6.0 mL | 24 | 12 | 6 |
Write the first-use date on the vial with a permanent marker. Most compounding pharmacies recommend discarding multi-dose vials after 28-30 days regardless of remaining contents. The bacteriostatic water preserves the solution, but its protective capacity diminishes over time and repeated needle punctures. For detailed storage guidance, check our guide on how long tirzepatide lasts in the fridge.
When to discard a vial
Discard immediately if:
The solution turns cloudy or develops visible particles
You notice any color change from the original appearance
The vial has been at room temperature for an extended period (check the pharmacy guidelines for your specific formulation)
More than 28-30 days have passed since first puncture
You suspect any contamination
Tirzepatide is a large peptide molecule that degrades with heat, light, and bacterial contamination. Injecting degraded peptide means injecting an unknown amount of active compound. Your dose might be significantly less than intended, and the degradation products may cause unexpected reactions. Understanding tirzepatide expiration and refrigeration requirements protects both your health and your investment.
The seven most common syringe mistakes with tirzepatide
These errors account for the vast majority of dosing problems in the peptide research community. Each one is preventable.
Mistake 1: using the wrong syringe type
Confusing tuberculin and insulin syringes creates 10x dosing errors. Always verify U-100 markings on the syringe barrel and packaging before use. This mistake happens most often when researchers order syringes online and receive a mixed shipment, or when a household member places a tuberculin syringe in the same drawer as insulin syringes.
Mistake 2: ignoring vial concentration changes
Your pharmacy switches from 10 mg/mL to 20 mg/mL. You keep drawing 50 units out of habit. Your dose just doubled from 5.0 mg to 10.0 mg. Check the concentration label on every new vial. Recalculate before the first draw. Write the new unit amount directly on the vial.
This scenario is especially common with compounded tirzepatide from larger pharmacies that may change their standard concentrations due to supply chain shifts.
Mistake 3: reading the syringe at an angle
Parallax error adds or subtracts 1-3 units depending on the viewing angle. At 20 mg/mL, a 3-unit error equals 0.6 mg. Always read at eye level, using the bottom of the meniscus as your reference point.
Mistake 4: not removing air bubbles
Air bubbles displace liquid volume. A 5-unit air bubble trapped in the barrel means 5 fewer units of actual tirzepatide in your syringe, even though the plunger reads correctly. Tap, float, and expel bubbles before every injection. This step takes ten seconds and prevents dose shortfalls that accumulate over weeks.
Mistake 5: choosing the wrong syringe size
Using a 1.0 mL syringe for a 12-unit dose, or trying to draw 80 units from a 0.5 mL syringe. Match your syringe to your dose tier. Keep multiple sizes available if your protocol spans different volume ranges during titration.
Mistake 6: reusing syringes
Some researchers reuse syringes to save money. Every reuse dulls the needle tip, increases injection pain, and raises contamination risk. A new 29-gauge needle glides through skin. A reused needle tears. The cost savings are minimal compared to the risks. Fresh syringe, every time.
Mistake 7: not accounting for reconstitution math
If you reconstitute your own tirzepatide, your chosen water volume determines the concentration. Adding 2 mL of bacteriostatic water to a 10 mg vial creates 5 mg/mL. Adding 1 mL creates 10 mg/mL. Your syringe dosing changes accordingly. Researchers who reconstitute one vial at 10 mg/mL and the next at 5 mg/mL without adjusting their draw volume will get inconsistent doses. The peptide reconstitution calculator makes this math automatic.
Syringe best practices for long-term tirzepatide protocols
Tirzepatide protocols typically run for months. Some researchers maintain their protocols for a year or longer. Over that timeframe, small habits compound into significant differences in outcomes, comfort, and safety.
Injection site rotation
Rotate between at least three injection sites: the abdomen (2 or more inches from the navel), the front of the thigh, and the back of the upper arm. Within each region, vary the exact spot by at least 1 inch between injections. This prevents lipohypertrophy, a condition where repeated injections in the same spot cause fatty tissue to thicken and harden, which then alters absorption unpredictably.
Our detailed guide on where to inject GLP-1 medications covers site selection, rotation patterns, and what to do if you notice tissue changes at injection sites.
Proper syringe disposal
Used syringes go in a puncture-resistant sharps container. Not the regular trash. Not a plastic bag. Not loose in a box. FDA-cleared sharps containers are available at most pharmacies for a few dollars. When full, follow your local guidelines for disposal. Many pharmacies and hospitals accept full sharps containers at no charge.
Improper syringe disposal creates a genuine safety hazard for anyone who handles your trash. It also violates regulations in most jurisdictions. Handle it correctly.
Traveling with syringes and tirzepatide
When traveling, keep your tirzepatide in an insulated cooling case with gel packs. Avoid direct ice contact, which can freeze the solution and destroy the peptide. The vial should stay upright to minimize stopper contact with the solution.
For air travel, carry syringes and medication in your carry-on bag. Bring your prescription documentation or pharmacy label. TSA and most international security agencies permit medical syringes with documentation. Check how long compounded tirzepatide can stay out of the fridge to plan your cooling strategy for your specific travel duration.
Tracking your injections
A simple log prevents two common problems: forgetting whether you already injected this week and losing track of where you are in your titration schedule. Record the date, injection site, units drawn, vial concentration, and any side effects. This data becomes invaluable when making titration decisions with your healthcare provider.
SeekPeptides members access protocol tracking tools that simplify this process, combining dose logging with progress tracking and titration reminders that keep your protocol on schedule.
How concentration affects your syringe choice
Your vial concentration and your syringe choice are linked decisions. Making them independently leads to suboptimal outcomes. Here is how to think about them together.
Low concentration (5 mg/mL): larger volumes, easier measurement
At 5 mg/mL, doses require more liquid. A 2.5 mg dose needs 50 units. A 5 mg dose needs 100 units. The advantage is that larger volumes are easier to measure precisely because each unit on the syringe carries less drug. The disadvantage is larger injection volumes, which some researchers find uncomfortable. This concentration pairs best with 0.5 mL and 1.0 mL syringes.
Medium concentration (10 mg/mL): the sweet spot
This is the most common compounded concentration for good reason. Doses produce manageable volumes (25-100 units for the standard 2.5-10 mg range) and the math stays clean. All three syringe sizes find useful application at this concentration. The compounded peptide industry has largely standardized around 10 mg/mL for both tirzepatide and semaglutide because it balances precision, volume, and vial economy.
High concentration (20+ mg/mL): small volumes, precision critical
High-concentration vials pack more drug into less liquid. A 2.5 mg dose from a 20 mg/mL vial requires only 12.5 units, just 0.125 mL. Injection volumes are tiny and comfortable, but measurement precision becomes critical. The 0.3 mL syringe with half-unit markings is essential at these concentrations, especially for starting doses. Without half-unit precision, you are forced to round, and rounding errors at high concentrations translate to meaningful dose variations.
Researchers transitioning between concentrations, perhaps because their pharmacy changed suppliers, must recalculate their draw volume. The guides on 20 units of tirzepatide and 40 units of tirzepatide demonstrate how the same unit marking delivers different milligram amounts at different concentrations.
Self-reconstitution and syringe dosing
Researchers who reconstitute lyophilized tirzepatide powder have an advantage: they choose their own concentration by controlling the water volume. This choice should be made with your syringe in mind.
Choosing your water volume based on your syringe
The goal is to make your weekly dose fall on a round, easy-to-measure number of units on your preferred syringe. Work backward from the syringe to the water volume.
Example 1: You have a 10 mg vial and want your 2.5 mg weekly dose to equal 50 units on a 0.5 mL syringe. What concentration do you need?
concentration = desired mg / (units / 100) = 2.5 / 0.5 = 5 mg/mL
So add 2.0 mL of bacteriostatic water (10 mg / 5 mg/mL = 2.0 mL).
Example 2: You have a 30 mg vial and want your 5.0 mg dose to equal 50 units. What concentration?
concentration = 5.0 / 0.5 = 10 mg/mL
Add 3.0 mL of bacteriostatic water (30 mg / 10 mg/mL = 3.0 mL).
Example 3: You have a 10 mg vial and want to use a 0.3 mL syringe for maximum precision. You want your 2.5 mg dose at 25 units (mid-range on the 0.3 mL syringe).
concentration = 2.5 / 0.25 = 10 mg/mL
Add 1.0 mL of bacteriostatic water.
The reconstitution calculator handles this optimization automatically, letting you input your target units and vial size to get the optimal water volume. For step-by-step reconstitution instructions, see our guides on reconstituting tirzepatide and reconstituting semaglutide.
Bacteriostatic water measurement
Ironically, the syringe you use to measure bacteriostatic water during reconstitution also affects your final concentration. If you intend to add 2.0 mL and accidentally add 2.3 mL, your concentration drops from 5 mg/mL to 4.35 mg/mL. Every subsequent dose from that vial will be about 13% lower than intended.
Use a separate 3 mL or 5 mL syringe for measuring bacteriostatic water. These larger syringes provide clear milliliter markings that make precise water measurement easier. Never use your tiny insulin syringe to measure water volumes above 1 mL, as you would need multiple draws and the cumulative error from each draw adds up.
Tirzepatide syringe dosing compared to other GLP-1 peptides
The syringe mechanics are identical for all injectable peptides. The differences lie in the dose ranges and typical concentrations.
Semaglutide comparison
Semaglutide versus tirzepatide dosing differs substantially. Semaglutide therapeutic doses range from 0.25 mg to 2.4 mg weekly. Tirzepatide ranges from 2.5 mg to 15 mg. This means semaglutide requires much smaller syringe volumes at comparable concentrations.
At 5 mg/mL, a 1.0 mg semaglutide dose requires only 20 units. At the same concentration, a 5.0 mg tirzepatide dose requires 100 units. Researchers who use both peptides, either concurrently or when switching from tirzepatide to semaglutide, need to recalibrate their syringe expectations. The unit amounts that felt normal for tirzepatide will seem enormous for semaglutide, and vice versa.
For semaglutide-specific unit conversions, see how many mg is 50 units of semaglutide and 20 units of semaglutide conversions.
Retatrutide and newer GLP-1 compounds
Emerging compounds like retatrutide follow the same syringe dosing principles. Units measure volume. Concentration determines drug content. The conversion formula is universal. What changes with each peptide is the dose range, the titration schedule, and the clinical effects.
If you already understand tirzepatide syringe dosing, you understand the mechanics for any injectable peptide. The specific numbers change. The technique does not.
When prefilled pens eliminate the syringe question entirely
Brand-name tirzepatide (Mounjaro for diabetes, Zepbound for weight management) comes in prefilled autoinjector pens at fixed doses: 2.5, 5.0, 7.5, 10.0, 12.5, and 15.0 mg. No syringe selection. No unit conversion. No drawing from vials. You press a button and the pen delivers the pre-measured dose.
The syringe dosing information in this guide applies specifically to compounded tirzepatide from multi-dose vials and self-reconstituted preparations. If you use a prefilled pen, you can skip syringe selection entirely, though understanding the underlying math helps you verify what the pen delivers and makes informed conversations with your prescriber easier.
For researchers considering other delivery methods, the comparison between oral and injectable tirzepatide offers additional context on how administration route affects dosing and bioavailability.
Building a complete syringe dosing kit
Having the right supplies organized and accessible makes weekly injections faster, safer, and less stressful. Here is what a complete tirzepatide dosing kit looks like.
Essential items:
0.3 mL insulin syringes (for doses under 30 units or precision needs)
0.5 mL insulin syringes (for doses between 25-50 units)
1.0 mL insulin syringes (for doses above 50 units)
Alcohol swabs (individually wrapped)
Sharps disposal container
Permanent marker (for writing dates and concentrations on vials)
Helpful additions:
A 3 mL syringe with a blunt-tip needle for measuring bacteriostatic water during reconstitution
A printed dose conversion chart for your specific concentration (tape it to your refrigerator)
A simple injection log (notebook, spreadsheet, or app)
Keeping all items in a dedicated pouch or container prevents the common problem of searching for supplies at injection time and settling for a suboptimal syringe because the right one is buried in a drawer.
Advanced tip: the air lock technique
Some experienced researchers use the air lock technique to ensure every drop of tirzepatide exits the syringe during injection.
After drawing your dose, pull back the plunger slightly to draw a small air bubble (about 2-3 units of air) into the syringe. Do not expel this bubble. When you inject, push the plunger until the air bubble follows the medication out of the needle. The air pushes the remaining liquid through the dead space, delivering slightly more of your measured dose.
This technique is standard practice in some medical settings. It does not affect your measured volume (the air was drawn after measurement) and it reduces dead space waste by pushing the last bit of solution through the needle. At high concentrations where dead space losses are meaningful, this simple technique recovers drug that would otherwise stay trapped in the hub.
The technique is optional. It helps most at higher concentrations where even tiny amounts of wasted peptide represent measurable milligrams of tirzepatide.
Frequently asked questions
Can I use the same syringe to draw from the vial and inject?
Yes, and this is the standard approach. Most insulin syringes are designed for single use: draw from the vial, inject, dispose. Drawing and injecting with the same syringe minimizes waste, requires only one needle puncture of the vial stopper, and keeps the process simple. Never reuse a syringe for a second injection session.
My tirzepatide dose falls between two syringe markings. What do I do?
Three options. First, switch to a syringe with finer markings (a 0.3 mL syringe with half-unit marks). Second, adjust your reconstitution volume to create a concentration where your dose lands on an exact marking. Third, round to the nearest measurable unit and accept a small variation. The first two options eliminate the problem. The third manages it.
Do syringe brands matter for tirzepatide dosing?
All U-100 insulin syringes follow the same calibration standard. A 50-unit mark on a BD syringe equals a 50-unit mark on an Easy Touch syringe. Brand differences exist in needle sharpness, plunger smoothness, dead space volume, and marking clarity, but the volume measurement is standardized. Choose a brand you find comfortable and consistent, then stick with it.
How do I know if my syringe has half-unit markings?
Look at the barrel closely, ideally with magnification. Between each numbered unit line, half-unit syringes show an additional shorter line at the midpoint. Standard syringes show only the numbered lines. Half-unit markings are most common on 0.3 mL syringes and less common on 0.5 mL or 1.0 mL sizes. The packaging should specify "half-unit" markings if present.
Is it normal for a tiny amount of liquid to remain in the syringe after injection?
Yes. This is the dead space volume discussed earlier. A small amount of liquid in the needle hub and plunger gap is normal and unavoidable with standard syringes. Low dead space syringes minimize this but do not eliminate it entirely. The air lock technique described above can push most of this residual liquid through the needle during injection.
What happens if I accidentally inject an air bubble?
Small air bubbles injected subcutaneously are harmless. The air absorbs into surrounding tissue within minutes. This is different from intravenous injection, where large air volumes can cause serious complications. For subcutaneous tirzepatide injections, a small bubble causes no medical concern. However, the bubble means you received slightly less tirzepatide than intended because the air occupied space that should have contained medication.
Should I inject fast or slow?
Slow and steady. A moderate injection speed (about 5-10 seconds for a 50-unit dose) allows the subcutaneous tissue to accommodate the incoming fluid without creating excessive pressure. Fast injection forces liquid into tissue rapidly, which can cause stinging, welting, and increased post-injection discomfort. After the plunger reaches the bottom, hold the needle in place for 5-10 seconds to allow the last of the medication to exit the needle tip before withdrawing.
Can I draw from a vial that has been punctured multiple times?
Yes, within limits. Multi-dose vials are designed for repeated puncture. The bacteriostatic water preservative protects against bacterial growth. However, most guidelines recommend discarding vials 28-30 days after first puncture. Check your specific pharmacy instructions. Some compounded formulations have different recommended use periods. If the solution looks cloudy, discolored, or contains particles, discard it immediately regardless of date. For specifics, see our guide on tirzepatide expiration and stability.
My pharmacy sent me a different concentration than last time. Do I need different syringes?
Maybe. Recalculate your dose in units using the new concentration. If the new unit amount fits within your current syringe capacity with adequate precision, keep using the same syringe. If it falls outside the capacity or requires finer measurement than your syringe provides, switch sizes. The compounded tirzepatide dosage calculator shows you the exact units for any concentration change.
External resources
For researchers serious about mastering their tirzepatide protocols, SeekPeptides provides comprehensive dosing guides, precision calculators, and a community of experienced researchers who navigate these exact syringe and dosing questions daily. Accurate dosing starts with the right syringe, the right technique, and the right resources.
In case I do not see you, good afternoon, good evening, and good night. May your syringes stay precise, your measurements stay accurate, and your protocols stay consistent.