Feb 4, 2026
You are wasting tirzepatide.
Not because you want to. But because you drew 15 units when you needed 25. Or 50 units when you needed 12.5. Or you used the wrong syringe entirely and ended up with a dose that was not even close to 2.5 mg.
The question seems simple: how many units is 2.5 mg of tirzepatide? The answer depends entirely on your vial concentration. At 10 mg/mL, it is 25 units. At 20 mg/mL, it is 12.5 units. At 5 mg/mL, it is 50 units. Get this wrong and you are either underdosing and wasting weeks of progress, or overdosing and inviting side effects you did not need to experience.
Tirzepatide is not cheap. A single vial can cost hundreds of dollars, especially if you are using compounded sources or grey market peptides. Every microgram counts. Every unit drawn matters. When you are starting at the 2.5 mg dose, which is the standard entry point for tirzepatide therapy, you need absolute precision.
This guide gives you the exact unit conversions for every common tirzepatide concentration. You will get charts, syringe selection advice, reconstitution protocols, and the full escalation schedule in units so you never have to guess again. We will cover what to expect at the 2.5 mg starting dose, how to avoid the most common measurement mistakes, and how this dose compares to other GLP-1 therapies. By the time you finish reading this, you will know exactly how many units to draw for 2.5 mg of tirzepatide, no matter what vial is in your hand.
The quick answer: how many units is 2.5 mg of tirzepatide
The conversion depends on the concentration of your tirzepatide vial. Here is the direct answer for the most common concentrations.
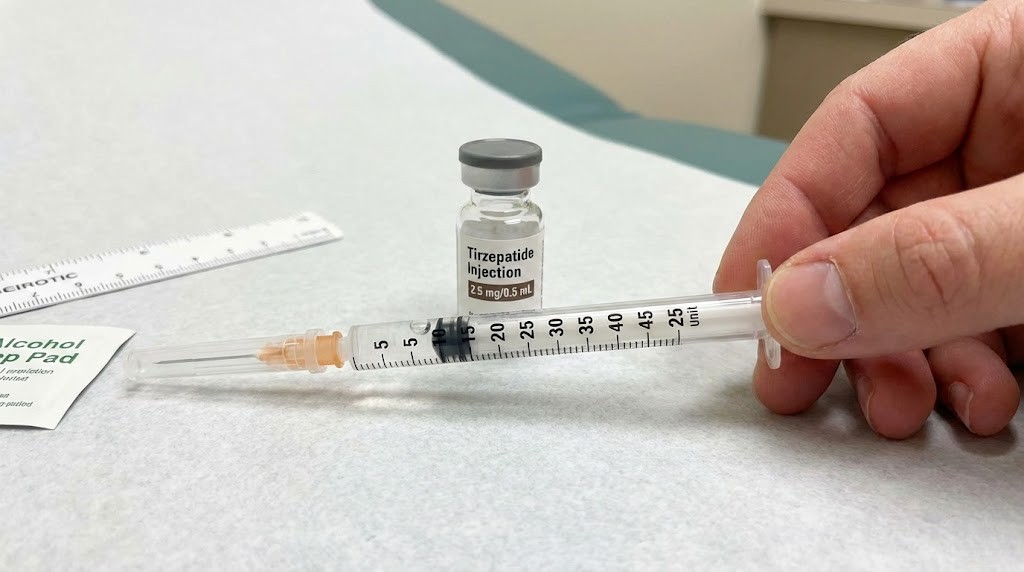
At 10 mg/mL, which is the most frequently compounded concentration, 2.5 mg of tirzepatide equals 25 units (0.25 mL). This is the standard starting dose. You draw to the 25-unit mark on a U-100 insulin syringe.
At 20 mg/mL, which is a more concentrated formulation often used to reduce injection volume, 2.5 mg equals 12.5 units (0.125 mL). You draw to the 12.5-unit mark, which sits between 10 and 15 on most syringes.
At 5 mg/mL, a lower concentration sometimes used for peptide injections with more volume, 2.5 mg equals 50 units (0.50 mL). This is half a milliliter, which fills exactly half of a standard 100-unit syringe.
At 15 mg/mL, an intermediate concentration used by some compounding pharmacies, 2.5 mg equals approximately 16.67 units (0.167 mL). You would round to 17 units on a syringe.
If you are using pharmaceutical tirzepatide such as Mounjaro or Zepbound, the pens are pre-filled and pre-measured. You do not need to calculate units. The pen delivers 2.5 mg automatically when you dial the dose. But if you are working with compounded tirzepatide, you are responsible for the conversion.
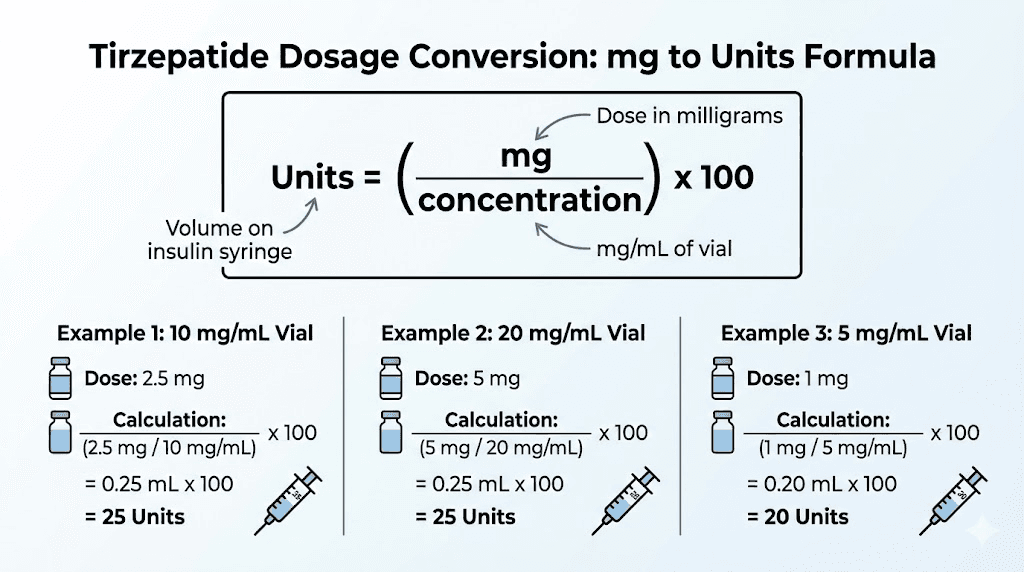
The formula is straightforward. Units equal the dose in milligrams divided by the concentration in milligrams per milliliter, multiplied by 100. For 2.5 mg at 10 mg/mL: (2.5 / 10) x 100 = 25 units. For 2.5 mg at 20 mg/mL: (2.5 / 20) x 100 = 12.5 units. For 2.5 mg at 5 mg/mL: (2.5 / 5) x 100 = 50 units.
This formula works because insulin syringes are calibrated as U-100, meaning 100 units per 1 mL. Each unit is 0.01 mL. When you know your concentration and your target dose, you can calculate the exact volume in milliliters, then multiply by 100 to get units. The peptide calculator at SeekPeptides does this instantly, but understanding the math ensures you never draw the wrong dose.
Most tirzepatide users start at 2.5 mg for four weeks before escalating to 5 mg, then 7.5 mg, then 10 mg, and potentially up to 15 mg depending on tolerance and results. The tirzepatide dosing for weight loss in units guide covers the full escalation schedule, but the 2.5 mg starting dose is where everyone begins. Clinical trials, including SURMOUNT-1, used this dose as the entry point to assess tolerability before increasing.
Why does concentration matter so much? Because tirzepatide vials are not standardized. Compounding pharmacies reconstitute lyophilized powder with varying amounts of bacteriostatic water for peptides, resulting in different concentrations. A 10 mg vial reconstituted with 1 mL of water yields 10 mg/mL. The same 10 mg vial reconstituted with 2 mL yields 5 mg/mL. If you assume the concentration without checking the label, you could easily inject double or half the intended dose.
Some users prefer higher concentrations like 20 mg/mL because they reduce injection volume. Smaller volumes mean less discomfort and faster injections. Others prefer lower concentrations like 5 mg/mL because they find it easier to measure small incremental doses with less risk of drawing too much. There is no universal right answer, but you must know your concentration before calculating units.
If you are unsure of your vial concentration, check the label. Compounded vials should state the total milligrams and the total volume. Divide total milligrams by total volume to get mg/mL. A 40 mg vial in 4 mL is 10 mg/mL. A 50 mg vial in 2.5 mL is 20 mg/mL. If your vial has no label or unclear labeling, do not inject it. Contact your pharmacy or supplier immediately.
The 2.5 mg dose is not therapeutic for most people. It is a priming dose designed to let your body adjust to GLP-1 and GIP receptor activation. You may notice mild appetite suppression, slight nausea, or no effects at all. That is expected. The goal is tolerability, not weight loss. Full therapeutic effects begin at 5 mg and above, which is why the tirzepatide dosing guide emphasizes patience during the escalation period.
Now that you know the quick answer, let us break down the conversion formula, chart every possible concentration scenario, discuss syringe selection, and walk through reconstitution protocols so you can dose with absolute confidence.
Understanding the conversion formula
The relationship between milligrams, milliliters, and units is the foundation of accurate peptide dosing. Milligrams measure the mass of active ingredient. Milliliters measure the volume of liquid. Units are a standardized measurement used by insulin syringes to simplify dosing.
Insulin syringes are calibrated as U-100. This means 100 units equal 1 mL. Each unit is therefore 0.01 mL. When you draw 25 units, you are drawing 0.25 mL. When you draw 50 units, you are drawing 0.50 mL. When you draw 12.5 units, you are drawing 0.125 mL.
Concentration ties mass to volume. A concentration of 10 mg/mL means there are 10 milligrams of tirzepatide in every milliliter of solution. A concentration of 20 mg/mL means there are 20 milligrams per milliliter. The higher the concentration, the less volume you need to inject to achieve the same dose.
The formula for converting dose to units is: Units = (Dose in mg / Concentration in mg/mL) x 100.
Let us work through examples. You want 2.5 mg of tirzepatide. Your vial is 10 mg/mL. First, calculate the volume in milliliters: 2.5 mg / 10 mg/mL = 0.25 mL. Then convert to units: 0.25 mL x 100 = 25 units.
Same dose, different concentration. You want 2.5 mg. Your vial is 20 mg/mL. Volume: 2.5 mg / 20 mg/mL = 0.125 mL. Units: 0.125 mL x 100 = 12.5 units.
Same dose, lower concentration. You want 2.5 mg. Your vial is 5 mg/mL. Volume: 2.5 mg / 5 mg/mL = 0.50 mL. Units: 0.50 mL x 100 = 50 units.
The formula applies to any dose and any concentration. If you are escalating to 5 mg at 10 mg/mL: 5 mg / 10 mg/mL = 0.50 mL = 50 units. If you are at 7.5 mg with 15 mg/mL: 7.5 mg / 15 mg/mL = 0.50 mL = 50 units. If you are at 10 mg with 20 mg/mL: 10 mg / 20 mg/mL = 0.50 mL = 50 units.
Notice how different combinations of dose and concentration can yield the same volume. This is why using the peptide reconstitution calculator is critical when you are planning your peptide reconstitution protocol. You can target a specific injection volume by adjusting the amount of bacteriostatic water you add.
Why do we multiply by 100 in the formula? Because U-100 syringes have 100 units per mL. The multiplication converts milliliters into the unit scale marked on the syringe. Without this step, you would be working in decimals that are harder to visualize. It is easier to draw to the 25-unit mark than to measure 0.25 mL on a syringe with no unit markings.
Some users work with tuberculin syringes instead of insulin syringes. Tuberculin syringes are marked in milliliters, not units. They typically hold 1 mL and are divided into 0.01 mL increments. If you use a tuberculin syringe, you skip the unit conversion entirely. For 2.5 mg at 10 mg/mL, you simply draw to 0.25 mL. For 2.5 mg at 20 mg/mL, draw to 0.125 mL. For 2.5 mg at 5 mg/mL, draw to 0.50 mL.
The advantage of tuberculin syringes is precision in milliliter measurements. The disadvantage is that most peptide protocols and online communities discuss doses in units, not milliliters. Using units makes communication easier and reduces errors when sharing protocols.
Concentration is not arbitrary. It is determined during reconstitution. When you buy lyophilized tirzepatide, it arrives as a powder in a vial. The vial label states the total milligrams of peptide. To use it, you add bacteriostatic water. The amount of water you add determines the final concentration. If you add 1 mL of water to a 10 mg vial, you get 10 mg/mL. If you add 2 mL, you get 5 mg/mL. If you add 0.5 mL, you get 20 mg/mL.
This is why the how much bacteriostatic water to add to peptides guide is so important. The water volume you choose affects every dose you draw for the life of that vial. Choose too much water and you may not have enough volume in your syringe for higher doses. Choose too little and you may struggle to measure small doses accurately.
Most users aim for concentrations between 5 mg/mL and 20 mg/mL. Lower than 5 mg/mL requires large injection volumes, which can be uncomfortable. Higher than 20 mg/mL risks precipitation or incomplete dissolution, especially with peptides that have limited solubility. Tirzepatide is relatively soluble, but extremely high concentrations should be avoided unless you have experience with peptide reconstitution.
Once you reconstitute a vial, the concentration is fixed. You cannot change it without transferring the peptide to a new vial and adding more water, which introduces contamination risks and degrades the peptide. This is why planning your concentration before reconstitution is essential. Use the semaglutide dosage calculator or the peptide calculator to model different reconstitution scenarios before you add water.
The formula works for any peptide, not just tirzepatide. BPC-157, TB-500, CJC-1295, and other research peptides follow the same math. If you understand the formula for tirzepatide, you understand it for everything. The only variable is concentration.
Understanding the formula protects you from dosing errors. If someone tells you to draw 25 units without specifying concentration, they are giving you incomplete information. 25 units at 10 mg/mL is 2.5 mg. 25 units at 20 mg/mL is 5 mg. 25 units at 5 mg/mL is 1.25 mg. Same units, wildly different doses. Always confirm concentration before drawing.
Complete 2.5 mg conversion chart for every concentration
Here is every common tirzepatide concentration with the exact unit conversion for a 2.5 mg dose. Save this chart. Reference it before every injection.
Concentration (mg/mL) | Volume for 2.5 mg (mL) | Units for 2.5 mg | Syringe type |
|---|---|---|---|
5 mg/mL | 0.50 mL | 50 units | 100-unit insulin syringe |
10 mg/mL | 0.25 mL | 25 units | 30-unit or 50-unit insulin syringe |
12.5 mg/mL | 0.20 mL | 20 units | 30-unit or 50-unit insulin syringe |
15 mg/mL | 0.167 mL | 16.7 units (round to 17) | 30-unit or 50-unit insulin syringe |
20 mg/mL | 0.125 mL | 12.5 units | 30-unit or 50-unit insulin syringe |
25 mg/mL | 0.10 mL | 10 units | 30-unit insulin syringe |
The 10 mg/mL concentration is standard. Most compounding pharmacies default to this because it balances ease of measurement with reasonable injection volumes across the dose escalation range. At 10 mg/mL, the starting dose of 2.5 mg is 25 units, the 5 mg dose is 50 units, the 7.5 mg dose is 75 units, and the 10 mg dose is 100 units. This progression is intuitive and uses standard syringe sizes efficiently.
The 20 mg/mL concentration is popular among users who want to minimize injection volume. At 20 mg/mL, 2.5 mg is only 12.5 units. The trade-off is that measuring small doses requires a precise syringe with fine graduations. A 30-unit syringe works well here because each unit is clearly marked.
The 5 mg/mL concentration is less common but useful if you are titrating slowly. At 5 mg/mL, 2.5 mg is 50 units, which is half a 100-unit syringe. Easy to see and measure. The downside is that higher doses require large volumes. The 10 mg therapeutic dose would be 200 units, or 2 mL, exceeding the capacity of a standard insulin syringe.
Let us look at reconstitution scenarios. Suppose you have a 10 mg vial of lyophilized tirzepatide. Here is how different bacteriostatic water volumes change the concentration and the resulting unit measurements for 2.5 mg.
Vial size (mg) | Bac water added (mL) | Final concentration (mg/mL) | Units for 2.5 mg |
|---|---|---|---|
10 mg | 1 mL | 10 mg/mL | 25 units |
10 mg | 2 mL | 5 mg/mL | 50 units |
10 mg | 0.5 mL | 20 mg/mL | 12.5 units |
10 mg | 0.67 mL | 15 mg/mL | 17 units |
10 mg | 0.8 mL | 12.5 mg/mL | 20 units |
Now suppose you have a 20 mg vial.
Vial size (mg) | Bac water added (mL) | Final concentration (mg/mL) | Units for 2.5 mg |
|---|---|---|---|
20 mg | 2 mL | 10 mg/mL | 25 units |
20 mg | 4 mL | 5 mg/mL | 50 units |
20 mg | 1 mL | 20 mg/mL | 12.5 units |
20 mg | 1.33 mL | 15 mg/mL | 17 units |
20 mg | 1.6 mL | 12.5 mg/mL | 20 units |
And a 50 mg vial, common for long-term users who want to reduce vial changes.
Vial size (mg) | Bac water added (mL) | Final concentration (mg/mL) | Units for 2.5 mg |
|---|---|---|---|
50 mg | 5 mL | 10 mg/mL | 25 units |
50 mg | 10 mL | 5 mg/mL | 50 units |
50 mg | 2.5 mL | 20 mg/mL | 12.5 units |
50 mg | 3.33 mL | 15 mg/mL | 17 units |
50 mg | 4 mL | 12.5 mg/mL | 20 units |
These charts assume complete dissolution and no peptide loss. In practice, a small amount of peptide may adhere to the vial walls or remain undissolved. This is why mixing peptides with bac water requires gentle swirling and time. Never shake tirzepatide vials. Shaking can denature the peptide and reduce potency. Swirl gently until the solution is clear.
If you are using pre-mixed tirzepatide from a compounding pharmacy, the concentration is printed on the label. Do not assume. Always check. Some pharmacies ship 10 mg/mL, others ship 20 mg/mL, and a few use custom concentrations based on your prescription.
If you are reconstituting yourself, measure the bacteriostatic water precisely. Use a syringe to draw the exact volume. Do not estimate by eyeballing the vial. A 10 percent error in water volume translates to a 10 percent error in concentration, which compounds over every dose you take. The free peptide reconstitution calculator at SeekPeptides helps you plan reconstitution with precision.
The charts above cover every realistic scenario. If your concentration is not listed, use the formula: Units = (2.5 / Concentration) x 100. For 8 mg/mL: (2.5 / 8) x 100 = 31.25 units. For 30 mg/mL: (2.5 / 30) x 100 = 8.33 units. The formula never fails.
Choosing the right syringe for your 2.5 mg dose
Syringe selection determines measurement accuracy. The wrong syringe makes precise dosing nearly impossible. The right syringe makes it effortless.
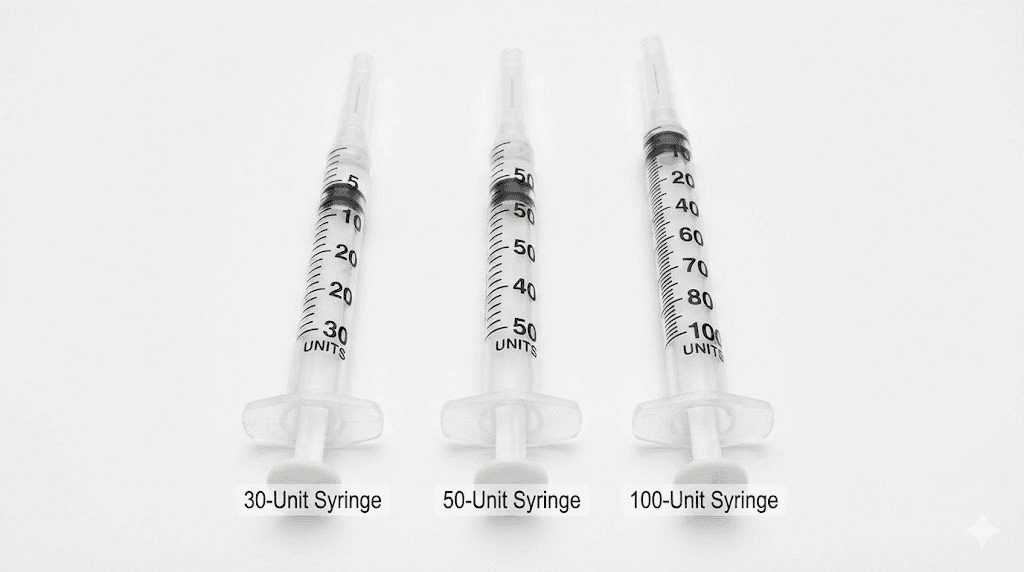
Insulin syringes are the standard for peptide injections. They come in three common sizes: 30-unit, 50-unit, and 100-unit. All are U-100 syringes, meaning 100 units per mL. The difference is total capacity and the precision of graduations.
A 30-unit syringe holds 0.3 mL total. Each unit is individually marked. This is the most precise syringe for small volumes. If you are injecting 12.5 units (2.5 mg at 20 mg/mL) or 17 units (2.5 mg at 15 mg/mL), a 30-unit syringe is ideal. The markings are clear, the increments are fine, and there is little room for error.
A 50-unit syringe holds 0.5 mL total. Each unit is individually marked, but the graduations are slightly closer together than on a 30-unit syringe. This syringe works well for doses up to 50 units. If you are injecting 25 units (2.5 mg at 10 mg/mL) or 50 units (2.5 mg at 5 mg/mL), a 50-unit syringe offers a good balance of precision and capacity.
A 100-unit syringe holds 1 mL total. Units are marked every 2 units, not individually. This means you can measure 10, 12, 14, 16, 18, 20 units precisely, but not 11, 13, 15, 17, 19, or 21 units. If your dose is 12.5 units or 17 units, the markings are not precise enough on a 100-unit syringe. You would need to estimate between lines.
For the 2.5 mg starting dose, here is the optimal syringe for each concentration.
Concentration | Units for 2.5 mg | Best syringe | Why |
|---|---|---|---|
5 mg/mL | 50 units | 50-unit or 100-unit | 50 units is easy to read on both |
10 mg/mL | 25 units | 30-unit or 50-unit | 25 units is clearly marked on both |
12.5 mg/mL | 20 units | 30-unit or 50-unit | 20 units is an even marking |
15 mg/mL | 17 units | 30-unit | 17 units requires individual markings |
20 mg/mL | 12.5 units | 30-unit | 12.5 units needs fine graduations |
25 mg/mL | 10 units | 30-unit | 10 units is a very small volume |
Needle gauge affects injection comfort. Insulin syringes typically come in 28G, 29G, 30G, or 31G. The higher the gauge number, the thinner the needle. For most users, 29G or 30G needles offer the best balance. The what is a peptide injection guide covers needle selection in more detail.
Some users prefer tuberculin syringes, which are marked in milliliters instead of units. Tuberculin syringes hold 1 mL and are divided into 0.01 mL increments. If you use a tuberculin syringe, you skip the unit conversion and draw directly to the milliliter mark. For 2.5 mg at 10 mg/mL, draw to 0.25 mL. For 2.5 mg at 20 mg/mL, draw to 0.125 mL.
Do not reuse syringes. Single-use syringes are sterile and designed for one injection. Reusing dulls the needle, increases infection risk, and introduces contamination into your vial. Syringes cost pennies each. Dispose of used syringes in a sharps container, not in household trash.
How to reconstitute tirzepatide to get the concentration you want
Reconstitution is where you control concentration. If you are working with lyophilized tirzepatide powder, you decide how much bacteriostatic water to add. This determines the final mg/mL concentration and, by extension, the unit measurements for every dose you take from that vial.
The formula for reconstitution is: Concentration (mg/mL) = Total mg in vial / mL of bac water added.
If you have a 10 mg vial and you add 1 mL of bacteriostatic water, you get 10 mg/mL. Add 2 mL, you get 5 mg/mL. Add 0.5 mL, you get 20 mg/mL. The amount of water is your control variable.
Before you add water, plan your dose escalation. Tirzepatide therapy starts at 2.5 mg and escalates to 5 mg, 7.5 mg, 10 mg, 12.5 mg, and sometimes 15 mg depending on response and tolerance. Your concentration should accommodate this entire range without requiring excessively large or small injection volumes.
Let us model the full escalation schedule at different concentrations.
At 10 mg/mL:
2.5 mg = 25 units (0.25 mL)
5 mg = 50 units (0.50 mL)
7.5 mg = 75 units (0.75 mL)
10 mg = 100 units (1.0 mL)
12.5 mg = 125 units (requires two injections)
15 mg = 150 units (requires two injections)
At 20 mg/mL:
2.5 mg = 12.5 units (0.125 mL)
5 mg = 25 units (0.25 mL)
7.5 mg = 37.5 units (0.375 mL)
10 mg = 50 units (0.50 mL)
12.5 mg = 62.5 units (0.625 mL)
15 mg = 75 units (0.75 mL)
Notice how 20 mg/mL keeps all doses under 1 mL, fitting comfortably in standard syringes. This is why many experienced users prefer 20 mg/mL once they are past the starting dose.
Here is the reconstitution process step by step.
Step 1: Gather supplies. You need your lyophilized tirzepatide vial, bacteriostatic water, a syringe for drawing water, alcohol wipes, and a sharps container.
Step 2: Calculate the target volume of bacteriostatic water. Use the formula: mL of water = Total mg in vial / Desired concentration. For a 10 mg vial targeting 10 mg/mL: 10 mg / 10 mg/mL = 1 mL.
Step 3: Wipe the rubber stoppers of both the peptide vial and the bacteriostatic water vial with alcohol. Let them dry for a few seconds.
Step 4: Draw the calculated volume of bacteriostatic water into your syringe. Be precise.
Step 5: Insert the syringe needle into the peptide vial. Tilt the vial at an angle so the needle tip is near the vial wall, not aimed directly at the lyophilized powder. Slowly inject the bacteriostatic water down the side of the vial.
Step 6: Withdraw the needle and gently swirl the vial. Do not shake. Swirl gently in a circular motion until the powder dissolves completely. The solution should be clear with no visible particles.
Step 7: Label the vial with the concentration, reconstitution date, and your initials. Once reconstituted, tirzepatide should be stored in the refrigerator and used within 28 days. The how long reconstituted peptides last in the fridge guide covers storage timelines in detail.
Step 8: Let the vial sit in the refrigerator for 10 to 15 minutes before your first injection. This ensures complete dissolution and allows any bubbles to dissipate.
The peptide reconstitution calculator simplifies this planning. Enter your vial size, target concentration, and dose schedule, and it outputs the exact water volume to add and the unit measurements for every dose.
What to expect at the 2.5 mg starting dose
The 2.5 mg dose is not therapeutic. It is a priming dose. Clinical trials, including the SURMOUNT-1 study, used 2.5 mg as the entry point to assess tolerability and minimize side effects before escalating to therapeutic doses.
Tirzepatide is a dual GIP and GLP-1 receptor agonist. At 2.5 mg, receptor activation is mild. You may notice subtle appetite suppression, slight nausea after meals, or no effects at all. This is expected and does not indicate the peptide is ineffective.
Some users report mild appetite reduction even at 2.5 mg. You might feel full sooner during meals or have less interest in snacking between meals. Cravings for high-calorie foods may decrease slightly. These effects depend on your baseline metabolism, body composition, and sensitivity to GLP-1 and GIP receptor activation.
Nausea is the most common side effect at the starting dose. It typically occurs one to two hours after injection and lasts a few hours. For most people, nausea is mild and does not interfere with daily activities. Eating smaller meals, avoiding high-fat foods, and staying hydrated can reduce nausea. Anyone new to what peptides are and what peptides are used for will find this introductory dose reassuringly gentle.
Weight loss at 2.5 mg is minimal. Clinical data shows an average weight loss of 1 to 2 kg (2 to 4 pounds) during the first four weeks on 2.5 mg. Most of this is water weight and glycogen depletion, not fat loss. Do not judge tirzepatide effectiveness based on the starting dose. The real results come at 5 mg, 7.5 mg, and 10 mg. For perspective on what higher doses produce, the peptides for weight loss guide covers expected outcomes across the full escalation.
Gastrointestinal effects beyond nausea can include bloating, constipation, or diarrhea. These are less common at 2.5 mg but do occur. The common peptide mistakes beginners make article covers how ignoring early side effect signals leads to worse outcomes.
The 2.5 mg dose lasts four weeks. Do not escalate sooner unless directed by your healthcare provider. The four-week period allows your body to adapt to the peptide, reduces the risk of side effects at higher doses, and establishes a baseline for evaluating response.
Some users see no effects at 2.5 mg. This does not mean the peptide is inactive. It means the dose is too low to produce noticeable effects in your body. Therapeutic effects begin at 5 mg for most people. Patience is essential. The how long peptides take to work guide explains why realistic timelines matter more than dose maximization.
Blood sugar changes are common even at 2.5 mg, especially if you have insulin resistance or prediabetes. Tirzepatide improves insulin sensitivity and lowers fasting glucose. You may see a 5 to 10 mg/dL reduction in fasting glucose during the first four weeks.
Do not combine tirzepatide with other GLP-1 agonists like semaglutide unless directed by a physician. The semaglutide versus tirzepatide comparison covers the differences and why stacking GLP-1 agonists is generally not recommended.
Hydration is critical. Tirzepatide can reduce thirst perception, leading some users to drink less water without realizing it. Dehydration worsens nausea, headaches, and fatigue. Aim for at least 2 to 3 liters of water daily.
The complete tirzepatide dose escalation schedule in units
Tirzepatide follows a structured escalation protocol. Each dose stays constant for at least four weeks before increasing. Here is the full schedule in units for the three most common concentrations.
At 10 mg/mL:
Dose (mg) | Volume (mL) | Units | Duration |
|---|---|---|---|
2.5 mg | 0.25 mL | 25 units | Weeks 1-4 |
5 mg | 0.50 mL | 50 units | Weeks 5-8 |
7.5 mg | 0.75 mL | 75 units | Weeks 9-12 |
10 mg | 1.0 mL | 100 units | Weeks 13-16 |
12.5 mg | 1.25 mL | 125 units (two injections) | Weeks 17-20 |
15 mg | 1.5 mL | 150 units (two injections) | Weeks 21+ |
At 20 mg/mL:
Dose (mg) | Volume (mL) | Units | Duration |
|---|---|---|---|
2.5 mg | 0.125 mL | 12.5 units | Weeks 1-4 |
5 mg | 0.25 mL | 25 units | Weeks 5-8 |
7.5 mg | 0.375 mL | 37.5 units | Weeks 9-12 |
10 mg | 0.50 mL | 50 units | Weeks 13-16 |
12.5 mg | 0.625 mL | 62.5 units | Weeks 17-20 |
15 mg | 0.75 mL | 75 units | Weeks 21+ |
At 5 mg/mL:
Dose (mg) | Volume (mL) | Units | Duration |
|---|---|---|---|
2.5 mg | 0.50 mL | 50 units | Weeks 1-4 |
5 mg | 1.0 mL | 100 units | Weeks 5-8 |
7.5 mg | 1.5 mL | 150 units (two injections) | Weeks 9-12 |
10 mg | 2.0 mL | 200 units (two injections) | Weeks 13-16 |
12.5 mg | 2.5 mL | 250 units (three injections) | Weeks 17-20 |
15 mg | 3.0 mL | 300 units (three injections) | Weeks 21+ |
The 5 mg/mL concentration becomes impractical at higher doses. This is why most users switch to 10 mg/mL or 20 mg/mL. If you are planning long-term tirzepatide use, reconstitute at 20 mg/mL to keep all doses under 1 mL.
The escalation schedule is not rigid. Some users stay at 5 mg or 7.5 mg indefinitely if they achieve their weight loss goals. Others escalate to 15 mg. Work with your healthcare provider to determine your optimal dose. The peptide cycle planning guide can help structure a long-term approach.
Each dose should be administered once per week, on the same day and roughly the same time. Tirzepatide has a half-life of approximately five days, so once-weekly dosing maintains stable blood levels. The how peptides work guide explains why consistent timing matters for maintaining stable receptor activation.
If you miss a dose, take it as soon as you remember, as long as it is within four days of the scheduled dose. If more than four days have passed, skip the missed dose and resume your regular schedule. Do not double up.
Side effects tend to peak during the first week at a new dose, then diminish. If you experience significant nausea when escalating, extend the previous dose for an additional two to four weeks before trying again. The peptide safety and risks resource covers when side effects cross from expected into concerning territory.
Some users add intermediate doses between standard escalation steps. For example, 6.25 mg between 5 mg and 7.5 mg. This can reduce side effects but extends the overall timeline. Use the peptide calculator to determine unit measurements for custom doses.
When you reach your goal weight, some users reduce the dose to a lower maintenance level. This maintains appetite suppression while reducing side effects and cost. The peptides before and after results page showcases what sustained commitment to a protocol looks like over months of consistent use.
Common mistakes when measuring 2.5 mg of tirzepatide
Dosing errors are common. Most are avoidable.
Mistake 1: Assuming concentration without checking the label. Users assume their vial is 10 mg/mL because that is the standard, then draw 25 units, only to discover the vial is 20 mg/mL. They just injected 5 mg instead of 2.5 mg. Always check the vial label. Always confirm concentration before calculating units.
Mistake 2: Using the wrong syringe type. Users try to measure 12.5 units with a 100-unit syringe, which only has markings every 2 units. They guess between the lines and inject 10 or 15 units instead. Use a 30-unit or 50-unit syringe for small doses.
Mistake 3: Not removing air bubbles. Air bubbles take up space in the syringe, reducing the actual dose. If you draw 25 units but there is a 2-unit air bubble, you are only injecting 23 units. Hold the syringe vertically, tap the side, then push the plunger slightly to expel the air.
Mistake 4: Drawing from a nearly empty vial. Users do not track how many doses remain. They draw 25 units from a vial that only has 15 units left. Always calculate how many doses a vial contains. Mark the vial with remaining doses after each injection.
Mistake 5: Storing the vial at room temperature. Reconstituted tirzepatide should be refrigerated at 2 to 8 degrees Celsius. Storing at room temperature degrades the peptide. Users leave the vial on the counter, then wonder why the peptide stops working. The how to store peptides after reconstitution guide covers best practices, and understanding how long peptides last at room temperature prevents waste.
Mistake 6: Reusing syringes. Reusing dulls the needle and introduces contamination. Use a fresh syringe for every injection.
Mistake 7: Injecting too quickly. Pushing the plunger too fast increases discomfort and can cause leakage. Inject slowly over 5 to 10 seconds. After injecting, hold the needle in place for 5 seconds before withdrawing.
Mistake 8: Not rotating injection sites. Injecting in the same spot repeatedly causes lipohypertrophy. Rotate between the abdomen, thighs, and upper arms. The peptide injections guide explains proper site rotation.
Mistake 9: Shaking the vial. Shaking creates bubbles and can denature the peptide. Always swirl gently. If you see bubbles in the vial, let it sit in the refrigerator for 10 minutes before drawing a dose.
Mistake 10: Using expired bacteriostatic water. Once opened, bacteriostatic water is good for 28 days. Using expired water introduces bacterial contamination. Always check the expiration date. The water to mix with peptides guide covers bacteriostatic water handling.
Mistake 11: Mixing peptides in the same vial. Some users try to mix tirzepatide with other peptides like BPC-157 or CJC-1295 to reduce injections. Peptides can interact, precipitate, or degrade when mixed. Each peptide should be in its own vial. The peptide stacks guide explains how to combine peptides safely.
Mistake 12: Switching vial concentrations without recalculating. A person who drew 25 units from a 10 mg/mL vial (2.5 mg) receives a new 20 mg/mL vial. Out of habit, they draw 25 units again, but now that delivers 5 mg. Every time you open a new vial, verify the concentration and recalculate. The how to calculate peptide dosages guide walks through this process.
Tirzepatide 2.5 mg versus other starting doses
Comparing starting doses across different peptides helps contextualize why 2.5 mg is the standard entry point for tirzepatide.
Semaglutide starts at 0.25 mg per week. This is one tenth of tirzepatide starting dose by weight, but not by receptor activation. Semaglutide is more potent per milligram at the GLP-1 receptor. The escalation schedule for semaglutide is 0.25 mg for 4 weeks, 0.5 mg for 4 weeks, 1 mg for 4 weeks, 1.7 mg for 4 weeks, and up to 2.4 mg. The semaglutide versus tirzepatide comparison explains the pharmacological differences, and the semaglutide dosage calculator handles unit conversions for that compound.
Why does tirzepatide start higher? Because it is a dual agonist. It activates both GLP-1 and GIP receptors. GIP receptor activation adds metabolic benefits but requires a higher starting dose. The 2.5 mg entry point was chosen in clinical trials to balance tolerability with receptor coverage.
Retatrutide, a triple agonist that activates GLP-1, GIP, and glucagon receptors, starts at 2 mg per week. Slightly lower than tirzepatide because glucagon receptor activation adds additional metabolic pathways. The retatrutide dosage chart provides detailed escalation protocols, and the retatrutide 20mg dosing guide covers higher dose ranges.
Cagrilintide, an amylin analog, starts at 0.6 mg per week. Amylin slows gastric emptying through different mechanisms than GLP-1 or GIP. The cagrilintide dosing guide covers the full protocol. Some researchers combine cagrilintide with tirzepatide. The cagrilintide dosage with tirzepatide guide addresses combination protocols.
Older peptides like AOD-9604 typically start at 300 mcg daily (about 2.1 mg per week). 5-Amino-1MQ starts at 50 mg daily sublingually. Tesofensine offers yet another approach to appetite control. These work through entirely different mechanisms and are not directly comparable to tirzepatide. The broader conversation about bioactive precision peptides for weight loss continues to evolve as new compounds enter clinical trials.
Some users ask if they can start tirzepatide at 5 mg to accelerate results. This is strongly discouraged. Starting higher dramatically increases the risk of severe nausea, vomiting, and gastrointestinal distress. Clinical trials used 2.5 mg for a reason. The peptide dosing guide emphasizes gradual escalation for exactly this reason.
Transitioning from semaglutide to tirzepatide requires a bridging protocol. If you are currently on semaglutide, your GLP-1 receptors are already primed. Some providers start tirzepatide at 5 mg instead of 2.5 mg when transitioning. These transitions should be supervised by a healthcare provider. For those considering alternatives, the Ozempic alternatives overview covers available options.
Some users stack tirzepatide with other peptides like BPC-157 for gut health, ipamorelin for growth hormone support, or sermorelin for recovery. When stacking, start each peptide at its recommended starting dose. The how many peptides you can take at once guide and the cycling different peptides resource provide essential context for multi-compound protocols. The peptide stack calculator helps plan these combinations.
Frequently asked questions
Can I draw 2.5 mg of tirzepatide with a tuberculin syringe instead of an insulin syringe?
Yes. Tuberculin syringes are marked in milliliters, not units. For 2.5 mg at 10 mg/mL, draw to 0.25 mL. For 2.5 mg at 20 mg/mL, draw to 0.125 mL. For 2.5 mg at 5 mg/mL, draw to 0.50 mL. The how to calculate peptide dosages guide covers both unit and milliliter systems.
What happens if I accidentally inject 5 mg instead of 2.5 mg on my first dose?
You will likely experience increased nausea, possible vomiting, and stronger appetite suppression. Stay hydrated, eat small bland meals, and avoid high-fat foods. The effects will peak 12 to 24 hours after injection and gradually diminish. Do not inject again until your next scheduled dose. Resume at 2.5 mg to re-establish tolerance. If vomiting is severe or persistent, contact your healthcare provider.
How long does a 10 mg vial last if I am injecting 2.5 mg per week?
A 10 mg vial contains four doses of 2.5 mg, lasting four weeks with once-weekly injection. A 20 mg vial gives eight doses (eight weeks). A 50 mg vial gives twenty doses (twenty weeks). Once reconstituted, tirzepatide should be used within 28 to 60 days, so do not buy vials so large that you cannot finish them within the stability window. The how long peptides last in the fridge and do peptides expire guides explain storage limits.
Can I split my 2.5 mg dose into two smaller injections during the week?
This is not recommended. Tirzepatide is designed for once-weekly administration based on its pharmacokinetics. The long half-life (approximately five days) maintains stable blood levels with weekly dosing. Splitting into two doses does not improve results and may increase side effects. Stick to once-weekly injections as prescribed.
Do I need to inject 2.5 mg at the same time of day each week?
Not necessarily. The long half-life means timing flexibility is high. Most users pick a consistent day and time for convenience and adherence. If you inject Monday morning one week and Monday evening the next, it will not affect results. Consistency helps with habit formation. The tirzepatide dosing guide recommends choosing a day and time that fits your routine.
How do I know if my tirzepatide vial is 10 mg/mL or 20 mg/mL if the label is unclear?
If the label states total milligrams and total volume, divide milligrams by volume. For example, 40 mg in 4 mL is 10 mg/mL. If the label only states total milligrams, you cannot determine concentration without knowing how much bacteriostatic water was added. Contact your pharmacy or supplier immediately. Do not inject from a vial with unclear concentration.
Can I increase from 2.5 mg to 5 mg after two weeks instead of four if I feel no effects?
Not recommended. The four-week period is about establishing a safety baseline, not just about effects. Even if you feel nothing at 2.5 mg, your body is adapting metabolically. Escalating early increases the risk of side effects at higher doses. Stick to the schedule unless your healthcare provider advises otherwise.
Is tirzepatide safe to use long-term?
Clinical trials running up to 72 weeks have shown a manageable safety profile with primarily GI-related side effects. Long-term data beyond trial periods is still being collected. The most common concerns involve gallbladder events, pancreatitis risk, and potential thyroid effects, all of which occur at low rates but warrant monitoring. The peptide research and studies section tracks ongoing safety data. Understanding the legal landscape of peptides and peptide regulation developments also helps inform sourcing decisions.
Can I use tirzepatide with other peptides?
Some researchers combine tirzepatide with peptides targeting different pathways, such as BPC-157 for gut health or TB-500 for recovery. Combining multiple GLP-1 agonists simultaneously is not recommended. The peptide stacks guide and the cagrilintide and semaglutide resource provide context for combination approaches.
External resources
SURMOUNT-1 Trial Publication, New England Journal of Medicine - Landmark clinical trial data for tirzepatide in obesity treatment
FDA Prescribing Information for Mounjaro (tirzepatide) - Official FDA label with complete dosing and safety information
Mayo Clinic: Tirzepatide Side Effects and Dosage - Patient-focused overview of side effects and proper use
StatPearls: Tirzepatide - Comprehensive pharmacology reference from the National Library of Medicine
CDC Adult Obesity Facts - Background on obesity prevalence and health implications
By now, you know exactly how many units is 2.5 mg of tirzepatide for every common concentration. You understand the formula, the syringe selection, the reconstitution process, and the escalation schedule. You have the charts, the common mistakes, and the comparison to other peptides. Most importantly, you have the tools to dose accurately and safely.
The 2.5 mg starting dose is not about dramatic weight loss. It is about establishing tolerance, priming your receptors, and setting the foundation for therapeutic doses. Check your vial label every single time before drawing. Use the right syringe for your concentration. Remove air bubbles. Inject slowly. Rotate sites. Track your doses. Follow the escalation schedule. Be patient.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, protocol tracking tools, and a community of thousands who have navigated these exact questions. Whether you are working with tirzepatide, exploring peptides for fat loss, building lean mass with peptides for muscle growth, or diving into peptide stacks, the platform provides everything you need to succeed safely.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your doses stay precise, and your progress stay consistent.