Feb 18, 2026

You have a syringe in your hand. The vial is in front of you. Your protocol says 30 units. But how many milligrams is that, exactly? The answer is not as simple as you might think, and getting it wrong means either wasting your tirzepatide or dealing with side effects that could have been completely avoided.
This is the question that trips up more people than almost any other dosing question in the peptide research community. Thirty units on an insulin syringe represents a volume of liquid, not a fixed amount of medication. The actual milligrams you receive depend entirely on the concentration of your specific vial. A 30-unit draw from a 5 mg/mL vial delivers a very different dose than 30 units from a 20 mg/mL vial. And that difference matters enormously for your results, your side effects, and your safety.
SeekPeptides members frequently ask about this exact conversion, and for good reason. The stakes are real. Underdose and you waste weeks waiting for results that never come. Overdose and you spend days dealing with nausea that could have been prevented with a simple calculation. This guide breaks down every concentration, gives you the exact math, and makes sure you never second-guess your tirzepatide dosing again.
We will cover the universal conversion formula, provide complete charts for every common concentration, walk through real-world examples, explain why 30 units is such a common dosing landmark, and give you the tools to convert any unit measurement to milligrams in seconds. Whether you are using a compounded vial from a pharmacy or reconstituting lyophilized tirzepatide yourself, the math works the same way.
Why units and milligrams are not the same thing
Here is where most confusion starts. People assume that units on a syringe correspond directly to milligrams of medication. They do not. Units on an insulin syringe measure volume, not drug potency.
Think of it this way.
A standard U-100 insulin syringe is calibrated so that 100 units equals exactly 1 mL of liquid. That is it. That is the only thing the unit markings tell you. They tell you how much liquid you are drawing into the syringe. They say nothing about how much active medication is dissolved in that liquid.
The concentration of your vial determines everything. If your vial contains 5 mg of tirzepatide dissolved in every milliliter of solution, then each unit on your syringe delivers 0.05 mg. But if your vial contains 20 mg per milliliter, each unit delivers 0.2 mg. Same syringe. Same markings. Four times the dose. This is why knowing your tirzepatide dosage in units requires knowing your concentration first.
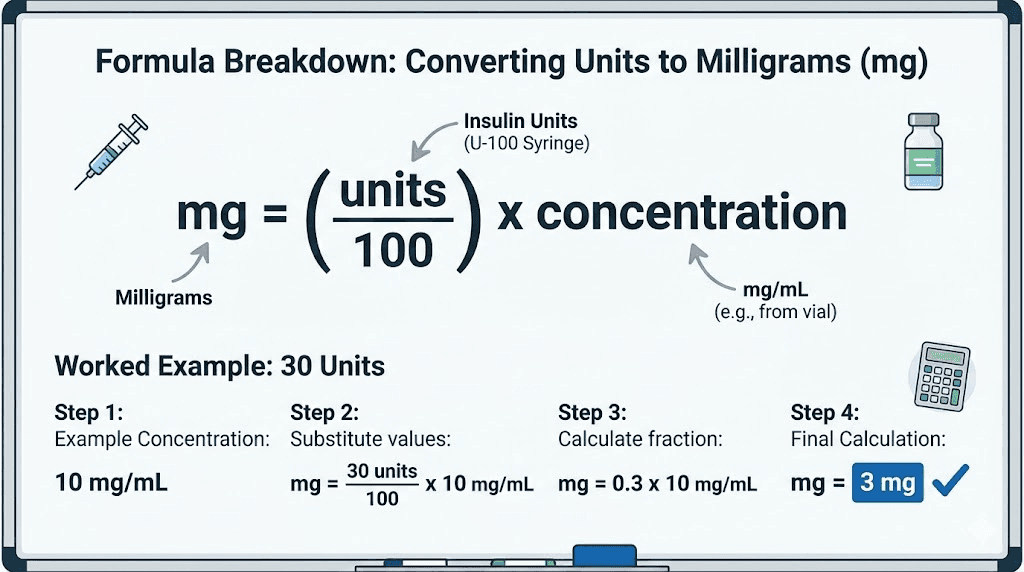
The relationship looks like this: milligrams equals units divided by 100, then multiplied by concentration in mg/mL. Or stated differently, mg = (units / 100) x concentration. This single formula is the key to every conversion in this guide, and once you understand it, you will never struggle with dosing math again.
The universal conversion formula
Every single unit-to-milligram conversion uses the same three-step process. Master this and you can convert any dose at any concentration.
Step 1: Convert units to milliliters. Since 100 units equals 1 mL on a U-100 syringe, you divide your units by 100. For 30 units: 30 / 100 = 0.3 mL.
Step 2: Multiply by your vial concentration. Take that 0.3 mL and multiply it by whatever concentration is listed on your vial label. If your vial says 10 mg/mL: 0.3 mL x 10 mg/mL = 3 mg.
Step 3: Verify against your target dose. Compare the result to what your protocol calls for. If your protocol says 3 mg and you calculated 3 mg at 30 units, you are set. If the numbers do not match, recalculate before drawing.
That is the entire process. Three steps. One formula. Works every time regardless of the vial, the concentration, or the peptide. The same math applies to semaglutide dosage conversions, reconstituted peptides, and every other injectable you will ever work with.
Why concentration varies so much
Compounded tirzepatide comes in a dizzying array of concentrations. Some pharmacies send 5 mg/mL vials. Others use 10 mg/mL. Still others compound at 20 mg/mL or even higher. Why such variation?
Several factors drive the differences. Vial size plays a role. A pharmacy working with 2 mL vials needs higher concentrations to fit enough medication for a full dosing cycle. Cost efficiency matters too. Higher concentrations mean smaller injection volumes, which means less bacteriostatic water, fewer vials, and lower shipping costs. Patient comfort is another consideration. Injecting 0.15 mL is more comfortable than injecting 0.5 mL, so some pharmacies deliberately compound at higher concentrations to reduce injection volume.
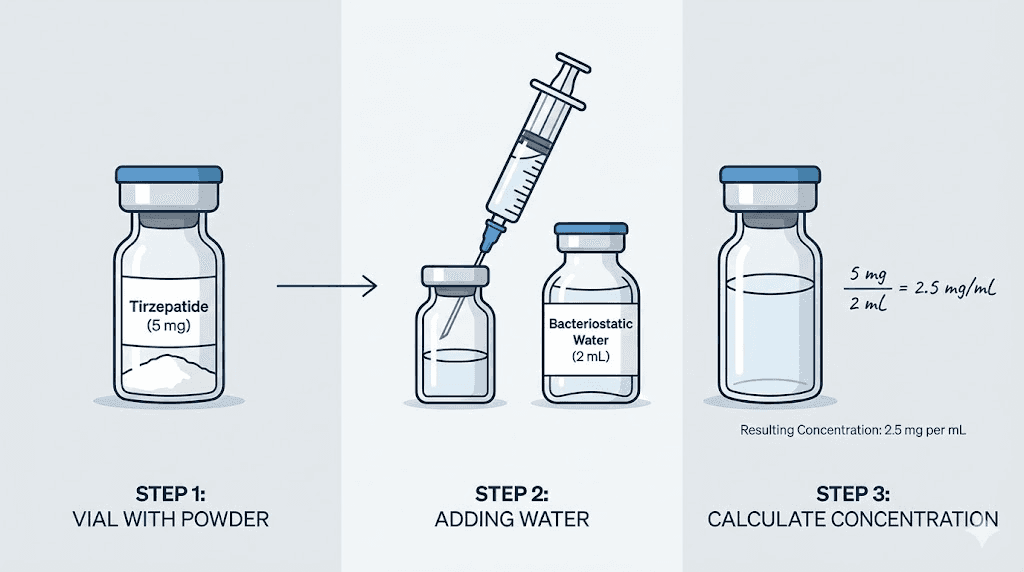
For researchers reconstituting their own lyophilized tirzepatide, the concentration depends entirely on how much bacteriostatic water they add to the vial. Add 1 mL to a 10 mg vial and you get 10 mg/mL. Add 2 mL to that same vial and you get 5 mg/mL. The choice is yours, and it directly affects how many units you need to draw for your target dose. Our peptide reconstitution calculator makes this math effortless.
30 units of tirzepatide at every common concentration
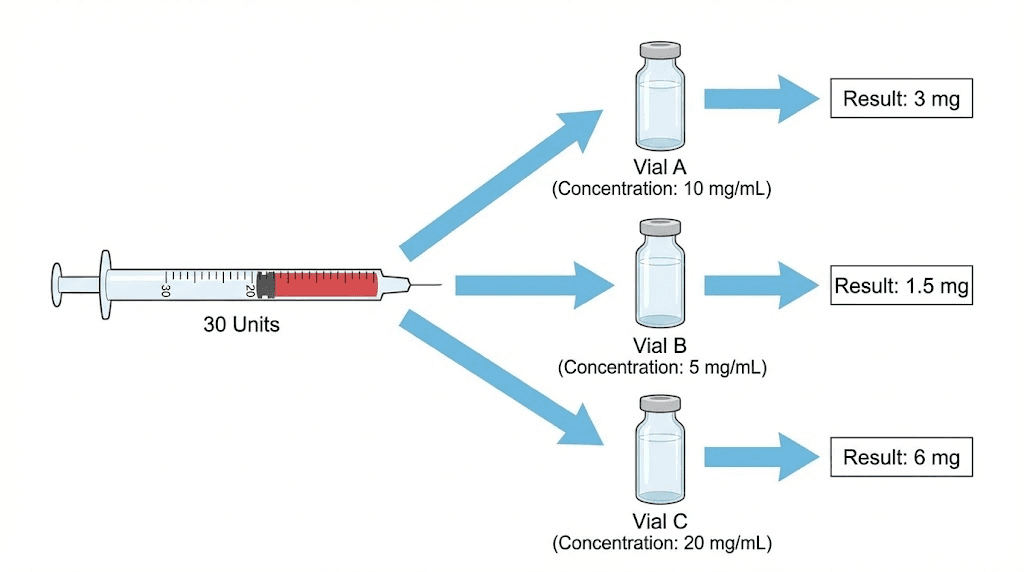
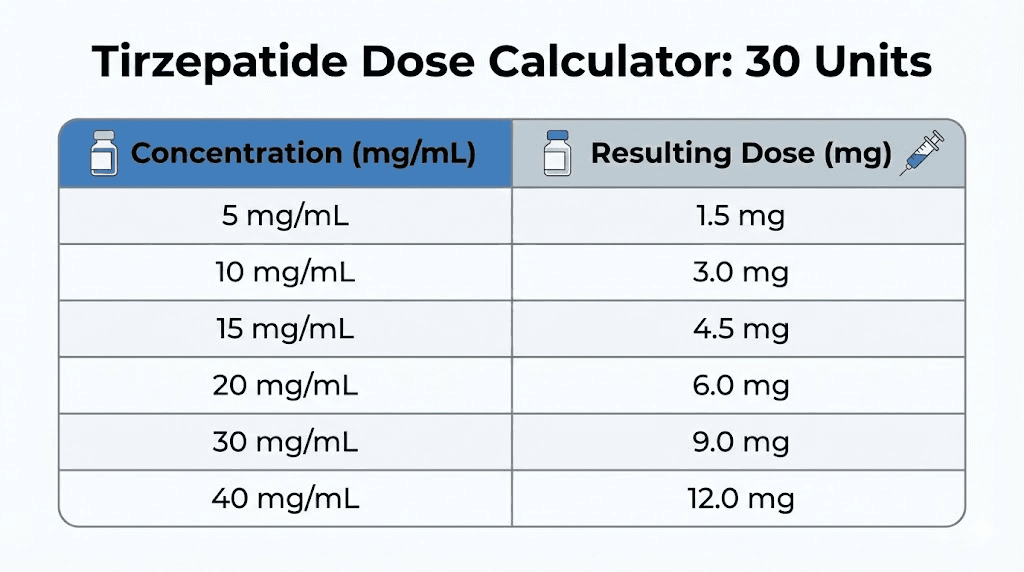
Here is the answer you came for. The number of milligrams in 30 units depends entirely on your vial concentration. Below is the complete breakdown for every concentration you are likely to encounter.
At 5 mg/mL: 30 units = 1.5 mg
This is the lowest common concentration for compounded tirzepatide. At 5 mg/mL, each unit on your syringe delivers 0.05 mg. Drawing 30 units gives you exactly 1.5 mg of tirzepatide.
A dose of 1.5 mg sits below the standard FDA starting dose of 2.5 mg. This means 30 units at this concentration is effectively a microdose of tirzepatide. Some researchers use this as a gentle introduction to assess tolerance before moving to standard doses. Others use it as a maintenance micro-protocol after reaching their goals.
To reach the standard 2.5 mg starting dose at this concentration, you would need 50 units. For 5 mg, you would need 100 units, which is a full 1 mL draw. That is a large injection volume, which is one reason many pharmacies have moved to higher concentrations.
At 10 mg/mL: 30 units = 3 mg
This is perhaps the most common concentration for compounded tirzepatide vials. At 10 mg/mL, each unit delivers 0.1 mg. Thirty units gives you precisely 3 mg.
Three milligrams falls between the FDA-approved starting dose of 2.5 mg and the second-tier dose of 5 mg. For researchers following a compounded tirzepatide dosage chart, 3 mg often represents a common intermediate step during titration. It provides slightly more appetite suppression and metabolic activity than the 2.5 mg dose while remaining well below the 5 mg threshold where side effects tend to increase.
This concentration makes the math clean and memorable. Ten units equals 1 mg. Twenty units equals 2 mg. Thirty units equals 3 mg. Simple patterns like these reduce dosing errors significantly. If your pharmacy offers a choice, 10 mg/mL is often the most user-friendly concentration for this reason.
At 15 mg/mL: 30 units = 4.5 mg
At 15 mg/mL, 30 units delivers 4.5 mg. This sits just below the second standard FDA dose tier of 5 mg. Each unit provides 0.15 mg of tirzepatide at this concentration.
Researchers using this concentration often find that 30 units serves as a natural stepping stone between the 2.5 mg and 5 mg dose levels. The 4.5 mg dose provides a more gradual escalation for those who experience side effects from tirzepatide when jumping directly from 2.5 mg to 5 mg. It is close enough to 5 mg to deliver meaningful clinical effects while being gentle enough to minimize gastrointestinal disturbances.
At 20 mg/mL: 30 units = 6 mg
Higher concentration vials are increasingly common, and 20 mg/mL is popular among pharmacies that prioritize smaller injection volumes. At this concentration, 30 units delivers 6 mg of tirzepatide.
Six milligrams falls between the 5 mg and 7.5 mg FDA dose tiers. For researchers following tirzepatide dosing for weight loss in units, this can serve as a useful intermediate step during dose escalation. Rather than jumping from 5 mg to 7.5 mg (a 50% increase), stepping through 6 mg first provides a smoother transition that the body tolerates better.
A word of caution here. At 20 mg/mL, the margin for error shrinks dramatically. Drawing just 5 extra units (35 instead of 30) means an additional 1 mg of tirzepatide. At lower concentrations, that same 5-unit error would add only 0.25 mg. Precision matters more as concentration increases.
At 30 mg/mL: 30 units = 9 mg
Some compounding pharmacies and research-grade vials come at 30 mg/mL. This is a high concentration that demands careful measurement. Thirty units at this concentration delivers a full 9 mg of tirzepatide.
Nine milligrams sits between the 7.5 mg and 10 mg dose tiers. This is a substantial dose that most researchers reach only after weeks or months of careful titration. At this concentration, every single unit on the syringe represents 0.3 mg. An error of just 10 units means a 3 mg dosing discrepancy, which is significant enough to cause meaningful side effects or undermined results.
If you are working with 30 mg/mL concentrations, using a 0.3 mL (30-unit) syringe with half-unit markings provides the most accurate measurements. The smaller syringe gives you finer gradations and makes it easier to draw precisely the amount you need. Many researchers who use higher concentrations also benefit from our peptide calculator to double-check their math before every draw.
At 40 mg/mL: 30 units = 12 mg
While less common, some vials are compounded at 40 mg/mL for researchers on higher maintenance doses. Thirty units at this concentration delivers 12 mg, which falls between the 10 mg and 12.5 mg FDA dose tiers.
At this concentration, measurement precision is absolutely critical. Each unit represents 0.4 mg. A 5-unit error means a 2 mg dosing difference. Use the smallest appropriate syringe, take your time reading the markings, and always verify your math twice before injection. This is not a concentration for beginners. If you are new to tirzepatide, start with lower concentrations where small measurement errors have smaller consequences.
Complete conversion table: 30 units at every concentration
For quick reference, here is the complete table showing exactly how many milligrams 30 units delivers at each common tirzepatide concentration:
Vial concentration | 30 units equals | Volume drawn | Nearest FDA dose tier |
|---|---|---|---|
5 mg/mL | 1.5 mg | 0.3 mL | Below 2.5 mg (microdose) |
8 mg/mL | 2.4 mg | 0.3 mL | Near 2.5 mg |
10 mg/mL | 3 mg | 0.3 mL | Between 2.5 and 5 mg |
12 mg/mL | 3.6 mg | 0.3 mL | Between 2.5 and 5 mg |
15 mg/mL | 4.5 mg | 0.3 mL | Near 5 mg |
17 mg/mL | 5.1 mg | 0.3 mL | At 5 mg |
20 mg/mL | 6 mg | 0.3 mL | Between 5 and 7.5 mg |
25 mg/mL | 7.5 mg | 0.3 mL | At 7.5 mg |
30 mg/mL | 9 mg | 0.3 mL | Between 7.5 and 10 mg |
40 mg/mL | 12 mg | 0.3 mL | Between 10 and 12.5 mg |
50 mg/mL | 15 mg | 0.3 mL | At 15 mg (maximum) |
Notice that the volume is always the same: 0.3 mL. That is because 30 units always equals 0.3 mL regardless of concentration. The concentration is what changes the milligram dose. This is the single most important concept in peptide dosing. Volume stays constant for a given number of units. Milligrams change based on what is dissolved in that volume.
Understanding the math behind unit-to-milligram conversions
Some people prefer to just look at charts. Others want to understand the math so they never need a chart again. This section is for the second group.
The core formula explained
The formula is elegant in its simplicity:
Milligrams = (Units / 100) x Concentration (mg/mL)
Let us break down why this works. An insulin syringe labeled U-100 means it is calibrated for a solution where 100 units equals 1 mL. So dividing your units by 100 converts them to milliliters. Once you know how many milliliters you are drawing, you multiply by the concentration (milligrams per milliliter) to get the total milligrams.
For 30 units at 10 mg/mL: (30 / 100) x 10 = 0.3 x 10 = 3 mg.
For 30 units at 20 mg/mL: (30 / 100) x 20 = 0.3 x 20 = 6 mg.
For 30 units at 5 mg/mL: (30 / 100) x 5 = 0.3 x 5 = 1.5 mg.
See the pattern? The volume (0.3 mL) stays the same. Only the multiplication factor changes based on concentration. You can do this math in your head for any unit count at any concentration. The complete peptide dosage calculation guide covers this formula in even greater depth.
Working the formula backwards: mg to units
Sometimes you know your target dose in milligrams and need to figure out how many units to draw. The reverse formula is just as simple:
Units = (Desired mg / Concentration) x 100
Say your protocol calls for 5 mg and your vial is 10 mg/mL. Units = (5 / 10) x 100 = 50 units. Need 2.5 mg from a 20 mg/mL vial? Units = (2.5 / 20) x 100 = 12.5 units. For the 2.5 mg calculation on different concentrations, check our guide on how many units is 2.5 mg of tirzepatide.
This bidirectional understanding is crucial. Protocols from clinics often specify milligrams, while your syringe shows units. Being able to convert in both directions without hesitation means you always know exactly what you are drawing.
Quick mental math shortcuts
Here are some shortcuts that experienced researchers use to convert doses quickly without pulling up a calculator:
For 10 mg/mL concentrations: The unit count equals 10 times the mg dose. Want 3 mg? Draw 30 units. Want 5 mg? Draw 50 units. Want 7.5 mg? Draw 75 units. This is the easiest concentration to work with and why many researchers prefer it.
For 20 mg/mL concentrations: The unit count equals 5 times the mg dose. Want 4 mg? Draw 20 units. Want 6 mg? Draw 30 units. Want 10 mg? Draw 50 units.
For 5 mg/mL concentrations: The unit count equals 20 times the mg dose. Want 2.5 mg? Draw 50 units. Want 5 mg? Draw 100 units. This concentration requires larger draws, which is why it has fallen out of favor at higher dose levels.
How 30 units fits into standard tirzepatide dosing protocols
Now that you know the math, let us talk about where 30 units actually falls in real-world dosing protocols. This is important context because the dose you are taking matters as much as getting the measurement right.
FDA-approved tirzepatide dose escalation
The FDA approved tirzepatide (as Mounjaro for type 2 diabetes and Zepbound for weight management) with the following escalation schedule:
Starting dose: 2.5 mg once weekly for 4 weeks
Second tier: 5 mg once weekly for at least 4 weeks
Third tier: 7.5 mg once weekly for at least 4 weeks
Fourth tier: 10 mg once weekly for at least 4 weeks
Fifth tier: 12.5 mg once weekly for at least 4 weeks
Maximum dose: 15 mg once weekly
Dose increases happen in 2.5 mg increments, and each tier requires a minimum of 4 weeks before escalating. This gradual approach gives the body time to adjust and minimizes gastrointestinal side effects like nausea, which are most common during dose transitions.
Where does 30 units fall in this schedule? It depends entirely on your concentration. At 10 mg/mL, 30 units is 3 mg, placing you slightly above the starting dose. At 20 mg/mL, 30 units is 6 mg, placing you between the second and third tiers. At 30 mg/mL, 30 units is 9 mg, placing you between the third and fourth tiers. Each of these is a valid dose, but they represent very different stages of a tirzepatide protocol.
For detailed dose escalation charts at every concentration, our tirzepatide dose chart provides a complete visual reference.
Why 30 units is a common dosing landmark
Thirty units comes up frequently for several practical reasons. First, it is a clean fraction of the syringe. On a 100-unit syringe, 30 units is easy to locate and measure. No squinting at tiny markings between lines. No guessing at half-unit increments. Just draw to the 30 line and inject.
Second, 0.3 mL is a comfortable injection volume. It is small enough to minimize discomfort at the injection site but large enough to measure accurately. Compare this to a 5-unit draw (0.05 mL), where a tiny measurement error represents a huge percentage of the dose, or a 100-unit draw (1 mL), where the sheer volume can cause injection site soreness.
Third, at the most popular 10 mg/mL concentration, 30 units delivers 3 mg. This happens to be an excellent intermediate dose between the 2.5 mg starting dose and the 5 mg second tier. Many clinics actually prescribe 3 mg as a stepping stone for patients who tolerate 2.5 mg well but want a gentler transition to 5 mg than jumping straight up.
Microdosing and sub-therapeutic uses of 30 units
At lower concentrations, 30 units enters microdosing territory. The microdosing tirzepatide chart shows that doses below 2.5 mg are increasingly popular among researchers exploring sub-therapeutic protocols.
At 5 mg/mL, 30 units is 1.5 mg. This is well below the standard starting dose. Some researchers use this as a very gentle introduction to assess basic tolerance before committing to standard protocols. Others use micro-protocols for maintenance after reaching their goals with higher doses, taking advantage of the metabolic benefits of tirzepatide at a fraction of the standard dose.
The research on sub-therapeutic tirzepatide dosing is still emerging, but early community reports suggest that even doses below 2.5 mg can provide some appetite modulation and metabolic support. Whether these effects are clinically meaningful at such low doses remains an active area of investigation.
Choosing the right syringe for 30 units
The syringe you use affects the accuracy of your measurement. This is not just a preference issue. It is a precision issue that directly impacts your dose.
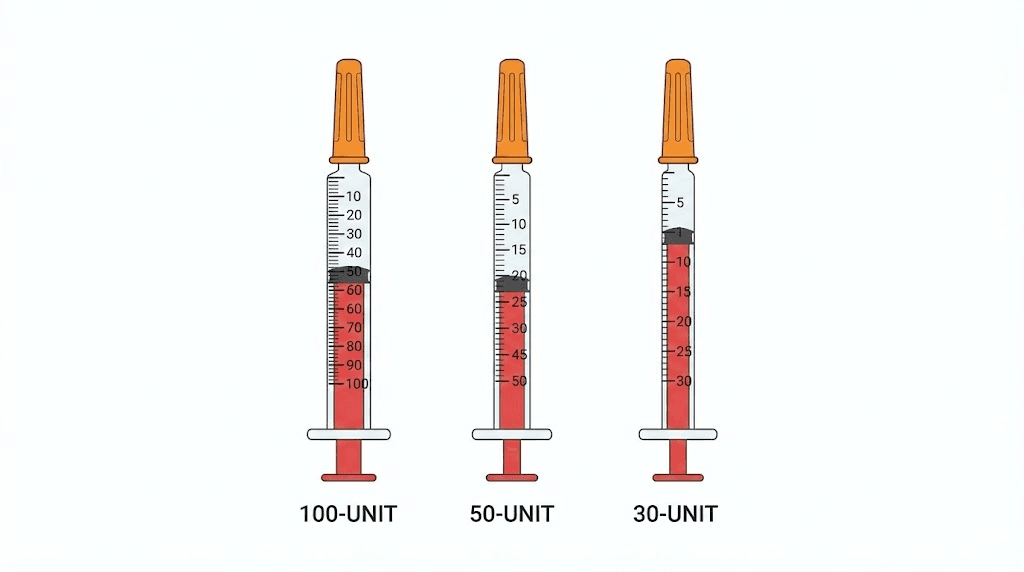
Standard 1 mL (100-unit) syringes
The most common insulin syringe holds 100 units (1 mL). On this syringe, the markings typically appear every 2 units, with numbered lines at every 10 units. Drawing to 30 units means lining up the plunger with the line marked "30."
This syringe works perfectly fine for 30-unit draws. The markings are clear enough, and the volume is well within the readable range. However, if you need to draw something like 27 or 33 units (for partial-unit adjustments), the 2-unit markings can make precision tricky. You would need to estimate the position between lines.
Half-mL (50-unit) syringes
A 50-unit syringe (0.5 mL) offers finer gradations for the same measurement range. Markings typically appear every unit, with numbered lines every 5 units. Drawing 30 units on this syringe is even more precise than on a 100-unit syringe because the scale is expanded.
The 50-unit syringe is arguably the best choice for 30-unit draws. It provides unit-level precision without the extreme scale compression of the 100-unit syringe, and 30 units falls comfortably within its range without maxing it out.
0.3 mL (30-unit) syringes
The smallest standard insulin syringe holds just 30 units (0.3 mL). This syringe provides markings every half-unit, giving you the finest possible gradation. Drawing 30 units means filling the syringe completely to its maximum capacity.
While this syringe offers the best precision for doses at or below 30 units, filling it all the way to the top leaves zero margin. You cannot overdraw. If you need to adjust to 31 or 32 units, you need a larger syringe. For exactly 30 units, though, this syringe gives you the most readable, most accurate measurement possible.
For a deeper dive into syringe selection and accurate drawing technique, our guide on how to inject GLP-1 medications covers proper technique from syringe selection through injection.
Reading your syringe correctly: avoiding the most common errors
Drawing 30 units sounds straightforward. Put the needle in the vial, pull the plunger to 30, inject. But the details matter, and small reading errors compound into significant dosing mistakes over time.
The meniscus problem
Liquid in a syringe forms a curved surface called a meniscus. The edges of the liquid ride slightly up the barrel walls while the center dips lower. When reading your syringe, always read from the flat bottom of the meniscus, not the curved edges. Reading from the top edge adds approximately 1-2 units of extra volume to your measurement.
Over weeks of dosing, that 1-2 unit error adds up. If you consistently overdraw by 2 units from a 20 mg/mL vial, that is an extra 0.4 mg per injection. Over 4 weekly injections, you have taken 1.6 mg more than intended. Not catastrophic, but enough to affect side effects and potentially throw off your titration schedule.
The plunger reading point
Another common error involves reading the wrong part of the plunger. The rubber stopper at the tip of the plunger has a domed shape. The correct reading point is the flat front edge of the stopper, where it meets the barrel wall. Not the top of the dome. Not the bottom of the rubber. The flat edge.
Many people read from the wrong part of the plunger and do not even realize their doses are slightly off. When dealing with tirzepatide dosage in syringe units, precision at the plunger level matters.
Air bubbles and their effect on dosing
Air bubbles in your syringe displace liquid and reduce your actual dose. A bubble that takes up 3 units of space means you are only getting 27 units of tirzepatide instead of 30. That is a 10% underdose.
To remove bubbles, hold the syringe needle-up and tap the barrel gently. The bubbles will float to the top near the needle. Push the plunger slowly until the bubbles are expelled and a tiny droplet of liquid appears at the needle tip. Then re-draw to your target of 30 units if the expulsion pushed liquid below that mark.
This step takes seconds but makes a meaningful difference in dosing accuracy. Researchers who skip the bubble-removal step often wonder why their results seem inconsistent from week to week. Inconsistent bubble volumes create inconsistent doses, even when you draw to the same line every time.
Parallax errors
How you hold the syringe while reading affects what you see. Hold it at eye level and look straight at the markings. If you look down at the syringe from above, you will read a number lower than the actual volume. If you look up from below, you will read higher than actual. This optical illusion is called parallax error, and it affects every measurement involving graduated markings.
The fix is simple. Hold the syringe horizontally at eye level. Turn it so the markings face you directly. Read the flat bottom of the meniscus at the exact point where it intersects the graduated line. Do this consistently and your doses will be accurate every time.
Real-world dosing scenarios with 30 units
Theory is useful. But seeing how 30 units plays out in actual protocols makes the conversion concrete and actionable. Let us walk through several real-world scenarios that researchers commonly encounter.
Scenario 1: starting dose with a 10 mg/mL vial
A researcher receives a compounded tirzepatide vial labeled 10 mg/mL, total volume 5 mL (50 mg total). Their clinic instructions say to start at 2.5 mg weekly and increase to 5 mg after 4 weeks.
At 10 mg/mL, 2.5 mg requires 25 units. After 4 successful weeks with minimal side effects, they want to move to 5 mg, which requires 50 units. But rather than jumping straight from 25 to 50 units, they decide to try 30 units (3 mg) for two weeks as an intermediate step.
This is a smart approach. The 0.5 mg increase from 2.5 to 3 mg is gentle enough to avoid triggering severe nausea while still providing a test of how their body handles a higher dose. If 3 mg goes well, they can increase to 37.5 units (3.75 mg) or jump to 50 units (5 mg) with confidence.
This gradual titration approach is covered in detail in our tirzepatide dosing guide, which outlines both standard and slow titration schedules.
Scenario 2: higher dose with a 20 mg/mL vial
A researcher has been on tirzepatide for 12 weeks and has titrated up to 6 mg. Their new vial is 20 mg/mL. They calculate: (6 / 20) x 100 = 30 units.
Here, 30 units is the correct draw for their 6 mg target dose. But there is a critical step they must not skip. Their previous vial may have been a different concentration. If their old vial was 10 mg/mL, they were drawing 60 units for 6 mg. The new vial requires only 30 units for the same dose. If they draw 60 units from the new 20 mg/mL vial out of habit, they would inject 12 mg instead of 6 mg. Double the intended dose.
This exact mistake happens more often than you might think. When switching between medications or between vials of different concentrations, always recalculate from scratch. Never assume the same number of units delivers the same dose across different vials.
Scenario 3: reconstituting a lyophilized vial
A researcher purchases a 10 mg lyophilized tirzepatide vial and needs to decide how much bacteriostatic water to add. They want their standard dose to land at an easy-to-measure unit count.
If they add 1 mL (100 units worth) of bacteriostatic water: concentration = 10 mg / 1 mL = 10 mg/mL. Drawing 30 units gives 3 mg.
If they add 2 mL (200 units worth): concentration = 10 mg / 2 mL = 5 mg/mL. Drawing 30 units gives 1.5 mg.
If they add 0.5 mL (50 units worth): concentration = 10 mg / 0.5 mL = 20 mg/mL. Drawing 30 units gives 6 mg.
The choice of water volume determines the concentration, which determines what 30 units means in milligrams. Researchers who want 30 units to equal a specific dose can work the formula backwards to determine exactly how much water to add. Our guide to reconstituting tirzepatide walks through this process step by step, and the reconstitution calculator automates it completely.
Scenario 4: switching from brand-name to compounded
A researcher was previously using brand-name Mounjaro auto-injector pens at 5 mg per dose. They switch to compounded tirzepatide at 20 mg/mL and need to figure out how many units to draw for the same 5 mg dose.
The math: (5 / 20) x 100 = 25 units. Not 30. This is an important distinction. If someone told them "draw about 30 units," they would be getting 6 mg instead of 5 mg, a 20% overdose. Always calculate. Never approximate. The difference between 25 and 30 units at this concentration is a full 1 mg of tirzepatide.
The brand-name pens handled all this dosing complexity automatically. The pen delivered exactly 5 mg with each click. Switching to vials means taking personal responsibility for the math. Our compounded tirzepatide dosage calculator helps bridge this gap.
How 30 units compares to other common unit draws
Context helps. Understanding where 30 units sits relative to other commonly prescribed unit amounts helps you gauge whether your dose is appropriate for your stage of treatment.
Common unit amounts at 10 mg/mL
Units drawn | Volume (mL) | Dose (mg) | FDA dose tier |
|---|---|---|---|
12.5 | 0.125 | 1.25 | Below starting dose |
25 | 0.25 | 2.5 | Starting dose |
30 | 0.3 | 3.0 | Between tiers 1 and 2 |
37.5 | 0.375 | 3.75 | Between tiers 1 and 2 |
50 | 0.5 | 5.0 | Second dose tier |
75 | 0.75 | 7.5 | Third dose tier |
100 | 1.0 | 10.0 | Fourth dose tier |
At 10 mg/mL, 30 units puts you 0.5 mg above the starting dose. This table makes it easy to see how 30 units relates to the standard dose tiers that the FDA established based on clinical trials.
Common unit amounts at 20 mg/mL
Units drawn | Volume (mL) | Dose (mg) | FDA dose tier |
|---|---|---|---|
12.5 | 0.125 | 2.5 | Starting dose |
25 | 0.25 | 5.0 | Second dose tier |
30 | 0.3 | 6.0 | Between tiers 2 and 3 |
37.5 | 0.375 | 7.5 | Third dose tier |
50 | 0.5 | 10.0 | Fourth dose tier |
62.5 | 0.625 | 12.5 | Fifth dose tier |
75 | 0.75 | 15.0 | Maximum dose |
At 20 mg/mL, the same 30 units delivers 6 mg, placing you squarely between the second and third dose tiers. Notice how 20 mg/mL requires half the units of 10 mg/mL for any given dose. This makes higher concentrations more practical for researchers on larger doses, as they avoid the need for large-volume draws.
For similar conversion guides covering other unit amounts, check our articles on how many mg is 20 units of tirzepatide, how many mg is 40 units of tirzepatide, and how many mg is 50 units of tirzepatide.
Tirzepatide storage and its impact on dose accuracy
You might not think storage affects dosing, but it does. Improper storage changes the concentration of your vial over time, which means the same 30 units could deliver a different dose from a degraded vial compared to a fresh one.
Temperature requirements
Compounded tirzepatide should be stored in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). At these temperatures, the peptide remains stable and the concentration stays consistent throughout the life of the vial.
Leaving tirzepatide at room temperature accelerates degradation. The peptide breaks down, the effective concentration drops, and your 30 units delivers fewer active milligrams than the label would suggest. How quickly this happens depends on the temperature, the formulation, and the storage duration. Our guide on how long tirzepatide lasts in the fridge covers stability timelines in detail.
What happens when tirzepatide degrades
Degraded tirzepatide does not suddenly become dangerous. It becomes less effective. The peptide chains break apart, and the fragments no longer activate the GIP and GLP-1 receptors with the same potency. You might draw your usual 30 units and wonder why the appetite suppression feels weaker this week. The answer could be that your vial sat on the counter for too long.
Signs that your tirzepatide may be degraded include cloudiness or particulate matter in the solution, reduced efficacy at your usual dose, a sudden need for higher doses to achieve the same effect, and an unexpected color change in the solution. If you notice any of these, it is time for a new vial. For more on tirzepatide expiration, see our article on does tirzepatide expire.
Proper vial handling between doses
Every time you puncture the vial stopper with a needle, you introduce a tiny pathway for contamination. Using bacteriostatic water (which contains 0.9% benzyl alcohol as a preservative) helps prevent bacterial growth, but proper technique still matters. Wipe the stopper with an alcohol swab before every draw. Use a new needle each time. And never touch the stopper with your fingers after cleaning it.
For the full rundown on maintaining vial integrity, our peptide storage guide covers everything from initial preparation through the last draw of the vial.
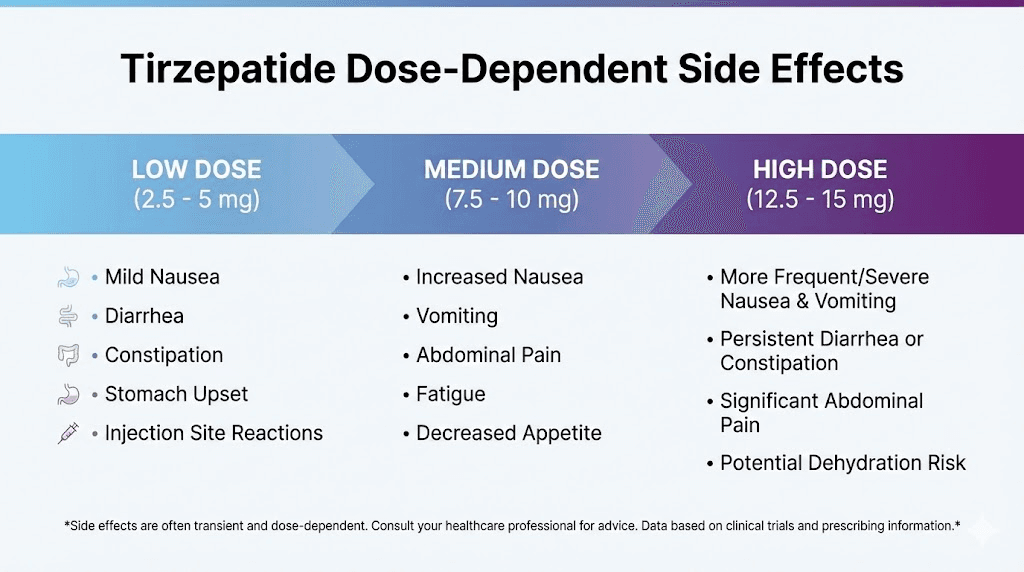
Side effects at different mg doses from 30 units
The side effect profile of tirzepatide is dose-dependent. This means that 30 units from a 5 mg/mL vial (1.5 mg) produces a very different side effect experience compared to 30 units from a 30 mg/mL vial (9 mg). Understanding this relationship helps you anticipate what to expect at your specific dose.
Lower doses (1.5 to 3 mg from 30 units)
At 30 units from a 5 mg/mL vial (1.5 mg) or a 10 mg/mL vial (3 mg), side effects tend to be mild or absent entirely. Common experiences at these doses include mild appetite reduction that starts 24 to 48 hours after injection, occasional mild nausea that resolves within a few hours, subtle changes in food preferences (less craving for calorie-dense foods), and slightly slower gastric emptying that may cause early fullness at meals.
Most researchers tolerate these lower doses well. The 2.5 to 3 mg range is specifically designed as the initiation phase, giving the body time to adjust to the medication before moving to higher, more therapeutically active doses. If you are experiencing significant side effects at 3 mg or below, that is worth discussing with your healthcare provider, as it could indicate unusual sensitivity. Our article on whether tirzepatide can cause anxiety addresses one of the less commonly discussed low-dose side effects.
Moderate doses (4.5 to 6 mg from 30 units)
At 30 units from a 15 mg/mL vial (4.5 mg) or a 20 mg/mL vial (6 mg), side effects become more noticeable. This is the dose range where tirzepatide begins producing significant metabolic effects, and the body is adjusting to GIP and GLP-1 receptor activation at meaningful levels.
Common experiences include more pronounced appetite suppression lasting several days per injection, nausea that peaks 12 to 24 hours after injection and gradually fades, possible constipation as gastric motility changes, occasional fatigue or reduced energy in the first 24 to 48 hours, and mild injection site reactions. Managing these side effects is an important part of a successful protocol. Eating smaller, more frequent meals helps with nausea. Adequate hydration addresses much of the constipation from tirzepatide. And taking the injection before bed allows some researchers to sleep through the peak nausea period.
Higher doses (9 to 12 mg from 30 units)
At 30 units from a 30 mg/mL vial (9 mg) or a 40 mg/mL vial (12 mg), you are in the higher dose range where both efficacy and side effects are amplified. These doses should only be reached through careful, gradual titration over weeks or months.
At these levels, appetite suppression is substantial and persistent. Weight loss tends to be more rapid. But side effects can include significant nausea lasting 24 to 72 hours after injection, constipation requiring active management, fatigue and tiredness that impacts daily activities, reduced enjoyment of food beyond simple appetite suppression, and possible injection site pain or induration.
Researchers at these dose levels need robust side effect management protocols. Proper nutrition becomes critical because the combination of reduced appetite and caloric restriction can lead to muscle loss, nutrient deficiencies, and metabolic slowdown if not managed carefully. Our guide to eating on tirzepatide and supplements to take with tirzepatide address these nutritional challenges.
Comparing 30 units of tirzepatide to 30 units of semaglutide
If you have experience with semaglutide (Ozempic, Wegovy), you might assume that 30 units of tirzepatide and 30 units of semaglutide deliver comparable doses. They do not. These are different medications with different potencies, different concentrations, and different dosing schedules.
Different medications, different concentrations
Semaglutide and tirzepatide have completely different concentration standards. Compounded semaglutide commonly comes in concentrations ranging from 1 mg/mL to 5 mg/mL, while compounded tirzepatide concentrations typically range from 5 mg/mL to 40 mg/mL.
Thirty units (0.3 mL) of semaglutide at 5 mg/mL delivers 1.5 mg. Thirty units of tirzepatide at 10 mg/mL delivers 3 mg. These are not equivalent doses. Tirzepatide and semaglutide have entirely different dose-response curves, different receptor binding profiles, and different clinical efficacy ranges.
For a detailed comparison of how doses translate between the two medications, our tirzepatide vs semaglutide dosage chart provides side-by-side conversion tables. And for the broader comparison of efficacy and side effects, see our semaglutide vs tirzepatide side effects comparison.
Why dose equivalence between medications does not work simply
Even if you calculate milligram amounts perfectly, you cannot directly translate a semaglutide dose to a tirzepatide dose based on milligrams alone. The clinical trial data shows different response curves, and the medications work through different receptor mechanisms.
Tirzepatide is a dual GIP and GLP-1 receptor agonist, while semaglutide targets only the GLP-1 receptor. This means tirzepatide often achieves similar or greater effects at milligram-for-milligram lower doses for some endpoints, but higher doses for others. The semaglutide to tirzepatide conversion chart helps researchers understand approximate equivalencies, but the transition should always be done under medical supervision.
If you are switching between tirzepatide and semaglutide, start conservatively with the new medication regardless of what you were taking before. The receptor binding profiles are different enough that tolerance to one does not fully predict tolerance to the other.
Tracking your doses: building a dosing log
Accurate dosing is not just about getting the right number in the syringe once. It is about consistency over weeks and months. A dosing log helps you track patterns, spot issues, and make informed decisions about dose adjustments.
What to record for each injection
Every injection entry should capture these key data points: the date and time of injection, the vial concentration (check every time, especially with new vials), the number of units drawn, the calculated milligram dose, the injection site location (abdomen, thigh, or upper arm), and any immediate reactions or unusual experiences during injection.
This seems like a lot of detail for a weekly injection. It is not. It takes 30 seconds to jot down and provides invaluable data when you need to troubleshoot issues like inconsistent results, unexpected side effects, or questions about whether your current dose is optimal.
Why injection site matters for your 30-unit dose
The absorption rate of subcutaneous tirzepatide varies by injection site. The abdomen generally provides the most consistent absorption. The thigh is slightly slower. The upper arm falls somewhere between. These differences are small for most people, but they can contribute to the week-to-week variability that some researchers experience.
Rotating injection sites is important to prevent lipodystrophy (changes in the fat tissue at the injection site). But try to use the same general area for your dosing assessment. If you always inject in the abdomen and then switch to the thigh, the slightly different absorption rate might make it seem like your dose changed when it did not.
For detailed injection technique guidance, our guide to GLP-1 injection sites covers optimal placement, rotation patterns, and technique tips.
When to consider changing from 30 units
Your 30-unit dose is not meant to be permanent. Most tirzepatide protocols involve gradual dose escalation based on response and tolerance. Consider adjusting your dose when you have been at 30 units for at least 4 weeks with good tolerance, your weight loss or metabolic improvements have plateaued for 2 or more consecutive weeks, side effects at your current dose are minimal and manageable, and your healthcare provider recommends an increase based on your progress.
Conversely, consider reducing from 30 units if side effects are persistent and significantly impacting quality of life, nausea or vomiting lasts more than 48 hours after injection consistently, you have reached your target goals and want to find a maintenance dose, or you experience any concerning symptoms that warrant medical evaluation.
Tracking all of this in a log makes the decision process clearer and more objective. Patterns become visible over time that are impossible to spot from memory alone. If your results plateau, you might wonder why tirzepatide stopped working, and a dosing log helps identify whether the issue is dose-related, tolerance-related, or something else entirely.
Special considerations for compounded tirzepatide
Compounded tirzepatide introduces variables that brand-name auto-injectors eliminate automatically. Understanding these variables is essential for anyone drawing 30 units from a multi-dose vial.
Verifying your vial concentration
The concentration should be clearly printed on the vial label. Check it. Every single time you receive a new vial, check it. Pharmacies can change formulations, concentrations, or suppliers without advance notice. If your previous vial was 10 mg/mL and your new one is 20 mg/mL, your standard 30-unit draw now delivers double the dose.
Write the concentration on the vial with a permanent marker if the label is hard to read. Some researchers also write the unit count for their target dose directly on the vial so they do not need to recalculate each week. Anything that reduces the chance of a dosing error is worth the extra seconds.
Tirzepatide with additives
Some compounded tirzepatide vials include additives like niacinamide (vitamin B3), glycine, or methylcobalamin (vitamin B12). These additives do not change the tirzepatide concentration or the unit-to-milligram conversion. If your vial says 10 mg/mL tirzepatide with 2 mg/mL niacinamide, you still calculate based on the tirzepatide concentration alone.
However, additives can change the total solution volume and may slightly affect how the medication feels at the injection site. For more on these formulations, see our guides on tirzepatide with niacinamide, tirzepatide with glycine, and tirzepatide with B12.
Multi-dose vial management
A single compounded vial typically contains multiple doses. A 5 mL vial at 10 mg/mL contains 50 mg total, enough for 16 weekly draws at 30 units (3 mg per dose) plus a small amount left over.
As you draw from the vial over weeks, the volume decreases. The last few draws can be tricky because the reduced liquid level makes it harder to get a clean draw without pulling in air. Tilt the vial at an angle to pool the remaining liquid near the needle. If you cannot get a full 30-unit draw without significant air, switch to a new vial rather than trying to estimate a partial dose.
The storage requirements for tirzepatide also become more important with multi-dose vials because the vial is in use for weeks rather than being consumed in a single dose.
Using tools and calculators for verification
Mental math and charts are helpful, but having a calculator to double-check your work adds an extra layer of safety. This is especially important when changing vials, adjusting doses, or working with less common concentrations.
Peptide dosage calculators
The SeekPeptides peptide calculator lets you input your vial concentration, desired dose in milligrams, and syringe type to get the exact number of units to draw. It works in reverse too, meaning you can input units and get milligrams. It handles all the math described in this guide instantly and without error.
Using a calculator does not mean you are bad at math. It means you are serious about accuracy. Even pharmacists use calculators for routine dispensing calculations. The stakes are too high and the math too important to leave to mental arithmetic alone.
Reconstitution calculators
If you are reconstituting lyophilized tirzepatide and want 30 units to equal a specific milligram dose, the reconstitution calculator tells you exactly how much bacteriostatic water to add. Input the total peptide in the vial, your desired concentration, and it provides the water volume.
For example, if you want 30 units to equal 5 mg from a 10 mg vial, you need a concentration of 16.67 mg/mL. The calculator tells you to add 0.6 mL of water. Without the calculator, that math requires division with decimals, which is where errors creep in. The bacteriostatic water guide covers the mechanics of accurate water addition.
The SeekPeptides advantage
SeekPeptides members get access to comprehensive dosing calculators, detailed protocol guides, and a community of experienced researchers who have navigated these exact questions. When you are staring at a vial wondering whether your math is right, having verified tools and expert support makes all the difference. The platform provides personalized protocol builders, weight-based calculation tools, and expert-reviewed dosing guides that account for individual factors most resources ignore.
Frequently asked questions about 30 units of tirzepatide
Is 30 units always 0.3 mL?
Yes. On a standard U-100 insulin syringe, 30 units always equals exactly 0.3 mL of liquid. This volume measurement never changes regardless of the medication or concentration in the vial. The milligram dose changes based on concentration, but the volume stays constant at 0.3 mL.
Can 30 units of tirzepatide be a starting dose?
It depends on your concentration. At 10 mg/mL, 30 units is 3 mg, which is slightly above the FDA-recommended starting dose of 2.5 mg. At 5 mg/mL, 30 units is 1.5 mg, well below the starting dose. Check your concentration and compare the resulting milligrams to the standard tirzepatide dosing schedule to see where 30 units falls for your specific vial.
What if I accidentally drew 30 units instead of 20 units?
If you have not injected yet, simply push the plunger back to your correct measurement and proceed. If you have already injected, the extra dose depends on your concentration. At 10 mg/mL, the difference between 20 and 30 units is 1 mg. At 20 mg/mL, it is 2 mg. Monitor for increased side effects like nausea or fatigue and continue your normal schedule the following week. Do not skip a dose or reduce the next dose to compensate. One slightly higher dose is unlikely to cause serious issues, but contact your healthcare provider if you experience severe or unusual symptoms.
Should I use a TB syringe or insulin syringe for 30 units?
Either works, but they are calibrated differently and you must know which one you have. An insulin syringe (U-100) shows units where 100 units = 1 mL. A tuberculin (TB) syringe shows milliliters directly. On a TB syringe, you would draw to the 0.3 mL mark rather than the 30 unit mark. The result is the same volume, but misreading one type of syringe with the other type's markings can cause dramatic dosing errors. Stick with one type consistently.
How long does a vial last at 30 units per week?
Divide the total volume of your vial by 0.3 mL to get the number of 30-unit draws. A 3 mL vial gives you 10 weekly draws. A 5 mL vial gives you about 16 draws (accounting for a small amount of waste from air bubbles and dead space in the needle). Check our guide on tirzepatide storage duration to make sure your vial stays effective through its entire use period.
Does drawing 30 units multiple times degrade the vial?
Each needle puncture creates a microscopic pathway through the rubber stopper. Over dozens of draws, this can theoretically compromise sterility. In practice, most multi-dose vials with bacteriostatic water remain safe for 28 to 30 days after first puncture, regardless of how many draws you take. Using a new needle for each draw, wiping the stopper with alcohol before every puncture, and keeping the vial refrigerated between uses all help maintain sterility and potency.
Is 30 units the same as 30 IU?
In the context of insulin syringes and peptide dosing, yes, 30 units and 30 IU (international units) refer to the same volume measurement on a U-100 syringe, which is 0.3 mL. However, IU can also refer to a biological potency measurement used for some medications like insulin and hCG, where one IU represents a standardized amount of biological activity. For tirzepatide, we measure doses in milligrams, and the "units" on your syringe are strictly a volume measurement, not IU of biological potency.
Can I split a 30-unit dose into two injections?
Some researchers split their weekly dose into two smaller injections to reduce side effects. If your protocol calls for 30 units once weekly, splitting it into 15 units twice weekly delivers the same total milligrams over the same time period. Some community reports suggest this approach reduces nausea peaks while maintaining efficacy, though clinical trial data specifically on split dosing is limited. Discuss this approach with your healthcare provider before modifying your protocol.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your calculations stay accurate, your concentrations stay clear, and your doses stay precise.