Feb 21, 2026

Some people draw 50 units for their 10 mg tirzepatide dose. Others draw 100 units. A few draw 25. And every single one of them could be correct. That sounds impossible, but it is not. The number of units on your insulin syringe that equals 10 mg of tirzepatide depends entirely on one variable: the concentration of your reconstituted or compounded solution. Get that variable wrong, and you could inject half your intended dose. Or double it.
This is the question that trips up more people than almost any other in the tirzepatide dosing world. And it makes sense. Milligrams measure mass. Units measure volume. They are not the same thing. Converting between them requires knowing your concentration, and concentration changes based on how the solution was prepared. A 10 mg dosage chart that does not specify concentration is worse than useless. It is dangerous.
This guide covers everything you need to measure 10 mg of tirzepatide accurately. The universal conversion formula. Quick reference tables for every common concentration. Step-by-step math you can verify yourself. Reconstitution instructions for 10 mg vials. What to expect when you reach the 10 mg dose tier. Side effects, management strategies, and the mistakes that send people to forums asking why their results disappeared. SeekPeptides members rely on guides exactly like this one to navigate the conversion math that generic dosing charts leave out.
Whether you are working with a compounded tirzepatide vial or pre-mixed solution, the math is the same. And by the end of this article, you will never second-guess your syringe readings again.
The quick answer: how many units is 10 mg of tirzepatide
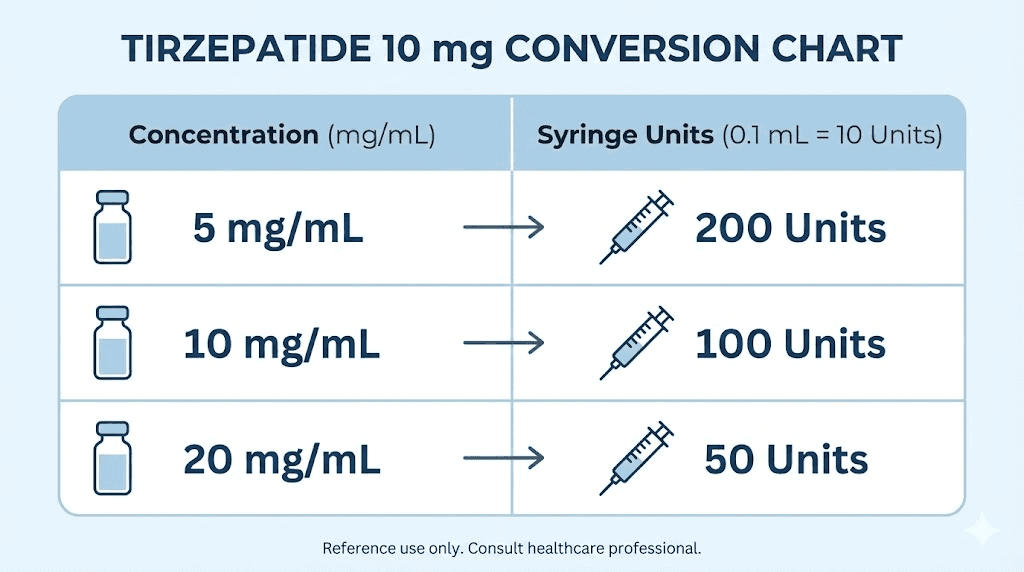
Here is the direct answer. For a 10 mg dose of tirzepatide, the number of units you draw depends on your concentration:
Concentration | Units for 10 mg | Volume (mL) |
|---|---|---|
5 mg/mL | 200 units (2 full syringes) | 2.0 mL |
10 mg/mL | 100 units (1 full syringe) | 1.0 mL |
20 mg/mL | 50 units | 0.50 mL |
30 mg/mL | 33 units | 0.33 mL |
40 mg/mL | 25 units | 0.25 mL |
60 mg/mL | 16.7 units | 0.167 mL |
That is it. Find your concentration on the left. Read across to the right. Draw that many units.
But if you do not know your concentration, or you want to understand why these numbers are what they are, keep reading. The math matters here. One wrong assumption about concentration, and you could be injecting 5 mg thinking it is 10 mg, or 20 mg when you only wanted 10 mg. Both scenarios happen more often than anyone in the tirzepatide dosage community would like to admit.
Why concentration changes everything
Units on an insulin syringe do not measure milligrams. They measure volume. Specifically, on a standard U-100 insulin syringe, 100 units equals 1 mL of liquid. That is all. The syringe has no idea whether you filled it with saline, tirzepatide at 10 mg/mL, or tirzepatide at 60 mg/mL. It just measures how much liquid you drew.
This is where people get confused. They see "units" and assume it is a standardized measurement of tirzepatide. It is not. The only standardized measurement of tirzepatide is milligrams. Units are just a convenient way to measure volume on the type of syringe most commonly used for GLP-1 injections.
Think of it this way. A shot glass holds about 44 mL. If you fill it with water, you have 44 mL of water. Fill it with olive oil, still 44 mL, but the weight is different because the density is different. Same volume, different mass. Concentration works the same way with tirzepatide. The syringe measures volume. The concentration determines how much actual tirzepatide sits inside that volume.
Common concentrations and where they come from
Different concentrations come from different sources. Understanding where yours came from helps you verify the number on the label.
5 mg/mL typically results from reconstituting a 10 mg vial with 2 mL of bacteriostatic water. Some compounding pharmacies also prepare solutions at this concentration. It is the most dilute common option, which means larger injection volumes but easier dose adjustments in small increments. For a 10 mg dose at this concentration, you would need 200 units, which exceeds a single 1 mL insulin syringe. That makes it impractical for this dose level. Most people who start at 5 mg/mL concentration move to higher concentrations before reaching the 10 mg dose tier.
10 mg/mL comes from reconstituting a 10 mg vial with 1 mL of bacteriostatic water, or a 30 mg vial with 3 mL. This is one of the most common concentrations from compounding pharmacies. At this concentration, 10 mg equals exactly 100 units, which is one full standard insulin syringe. Clean. Simple. No math required. You can verify your reconstitution calculations easily because the numbers are round.
20 mg/mL is popular among compounding pharmacies because it keeps injection volumes small even at higher doses. At this concentration, 10 mg equals 50 units, exactly half a syringe. Many pharmacy-specific charts like the Empower tirzepatide dosage chart and the Olympia tirzepatide dosage chart use this concentration. It is also what you get when you reconstitute a 10 mg vial with 0.5 mL of bacteriostatic water.
30 mg/mL, 40 mg/mL, and 60 mg/mL come from higher-concentration compounded preparations. These are less common for lyophilized (powder) vials because they require very small reconstitution volumes that are difficult to measure precisely. You will mostly encounter these from pharmacies that ship pre-mixed solutions. The 20 mg/mL dosing chart and 30 mg dosage chart resources cover these higher concentrations in detail.
The universal conversion formula
Every conversion in this article uses one formula. Learn it once, and you can calculate the units for any dose at any concentration.
Units = (Dose in mg / Concentration in mg per mL) x 100
That is it. Three numbers. One division. One multiplication. Let us walk through it for 10 mg at every common concentration so you can see exactly how it works.
10 mg at 5 mg/mL
Start with the dose: 10 mg. Divide by the concentration: 5 mg/mL. That gives you 2.0 mL. Multiply by 100 to convert milliliters to insulin syringe units: 200 units.
This is impractical for a single injection. A standard insulin syringe holds 100 units (1 mL). You would need two full syringes to deliver 10 mg at this concentration. Most researchers working at the 10 mg dose for weight loss use a higher concentration to keep the injection volume manageable. If you are still using a 5 mg/mL solution and have reached the 10 mg dose tier, it is time to consider a more concentrated preparation. The compounded tirzepatide dosage calculator can help you determine the best concentration for your dose level.
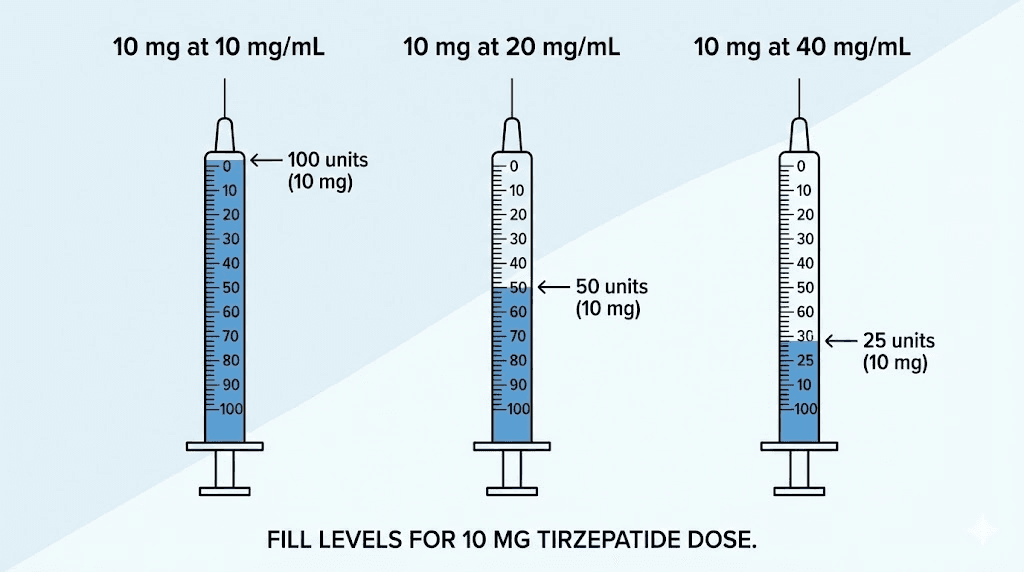
10 mg at 10 mg/mL
Dose: 10 mg. Concentration: 10 mg/mL. Division: 10 / 10 = 1.0 mL. Multiply by 100: 100 units.
One full syringe. This concentration makes the math effortless. You draw the entire syringe for your 10 mg dose. No partial measurements. No estimating between hash marks. The simplicity is why many compounding pharmacies default to this concentration for their compound tirzepatide dosage charts.
There is one downside. A full 1 mL injection is a relatively large volume for a subcutaneous injection. Some people experience more injection site discomfort at this volume compared to the smaller volumes that come with higher concentrations. If injection site reactions are a concern, a 20 mg/mL concentration cuts the volume in half.
10 mg at 20 mg/mL
Dose: 10 mg. Concentration: 20 mg/mL. Division: 10 / 20 = 0.5 mL. Multiply by 100: 50 units.
Half a syringe. This is the sweet spot for many people at the 10 mg dose. The volume is small enough to minimize injection discomfort but large enough to measure accurately on a standard syringe. You can see exactly where the 50-unit mark sits. No squinting. No guessing. The Empower tirzepatide dosing chart and many other pharmacy-specific references use this concentration as their standard.
10 mg at 30 mg/mL
Dose: 10 mg. Concentration: 30 mg/mL. Division: 10 / 30 = 0.333 mL. Multiply by 100: 33.3 units.
Now the math gets less clean. You need to draw to approximately the 33-unit mark, which falls between the 30 and 35 hash marks on most syringes. This requires careful attention. Round to the nearest whole unit. At this concentration, each unit on your syringe represents 0.3 mg of tirzepatide, so being off by one unit only changes your dose by 0.3 mg. That is within an acceptable margin for most tirzepatide dosing protocols.
10 mg at 40 mg/mL
Dose: 10 mg. Concentration: 40 mg/mL. Division: 10 / 40 = 0.25 mL. Multiply by 100: 25 units.
A quarter syringe. Clean number. Easy to measure. At this concentration, the injection volume is small, which most people prefer. The 25 units of tirzepatide dosage chart provides additional reference for this exact measurement. The tradeoff is that each unit on your syringe now represents 0.4 mg, so accuracy in your draw matters more than it does at lower concentrations.
10 mg at 60 mg/mL
Dose: 10 mg. Concentration: 60 mg/mL. Division: 10 / 60 = 0.167 mL. Multiply by 100: 16.7 units.
Very small volume. Draw to approximately 17 units. At this concentration, each unit represents 0.6 mg of tirzepatide. Being off by even 2 units means a 1.2 mg difference in your dose. That is not negligible. If you are using a 60 mg/mL solution, consider using a syringe with finer graduation marks (0.3 mL or 0.5 mL syringes with half-unit markings) for better precision. The peptide dosage calculation guide explains why precision matters more at higher concentrations.
Reconstituting a 10 mg vial for accurate dosing
If you have a lyophilized (freeze-dried) 10 mg vial of tirzepatide, you need to reconstitute it before you can draw any units at all. The amount of bacteriostatic water you add determines the concentration, which determines how many units equal 10 mg.
Here is a quick reference for a 10 mg vial:
BAC water added | Resulting concentration | Units for 10 mg (full vial) |
|---|---|---|
0.5 mL | 20 mg/mL | 50 units |
1.0 mL | 10 mg/mL | 100 units |
2.0 mL | 5 mg/mL | 200 units |
Notice something important. If you have a 10 mg vial and you need a full 10 mg dose, you are using the entire vial in one injection. That means you either reconstitute with a small volume to keep the injection manageable, or you accept a large injection volume. Most people at the 10 mg dose level use vials larger than 10 mg (such as 30 mg or 60 mg vials) and draw the appropriate portion for each weekly dose.
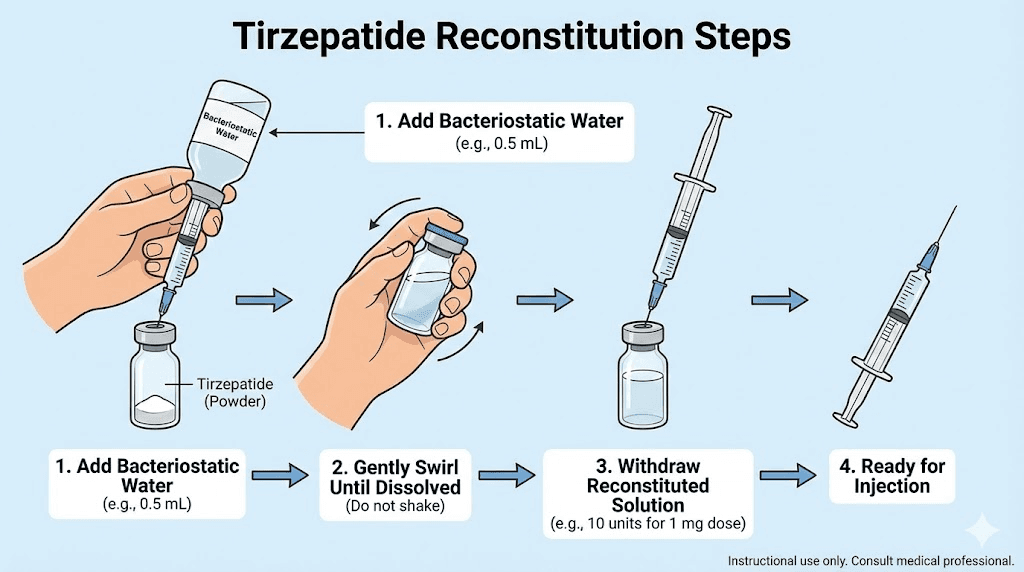
Step-by-step reconstitution process
The reconstitution process itself is straightforward, but each step matters for accuracy and sterility. Before you begin, gather your vial, bacteriostatic water, alcohol swabs, and a fresh syringe.
First, wipe the top of the tirzepatide vial and the bacteriostatic water vial with alcohol swabs. Let them air dry for a few seconds. This prevents contamination from the rubber stoppers.
Second, draw the desired amount of bacteriostatic water into a clean syringe. For a 10 mg vial, 1 mL is the most practical choice because it creates a 10 mg/mL concentration where the math is simple.
Third, insert the needle into the tirzepatide vial at an angle. Aim the stream of water at the glass wall, not directly onto the powder. Direct impact can cause foaming, which damages the peptide and makes it harder to see when the powder has fully dissolved. The tirzepatide reconstitution chart provides visual references for this technique.
Fourth, let the water run slowly down the side of the vial. Do not push the plunger quickly.
Fifth, once all the water is in the vial, remove the syringe. Gently swirl the vial by rolling it between your palms. Do not shake it. Shaking creates bubbles and can denature the peptide, reducing its effectiveness. The reconstitution chart PDF has detailed visual instructions for this step.
The solution should be clear and colorless once fully dissolved. If it is cloudy or has particles floating in it, something went wrong. Do not use a cloudy solution.
After reconstitution, label the vial with the date and concentration. Store it in the refrigerator at 2-8 degrees Celsius (36-46 degrees Fahrenheit). Reconstituted tirzepatide stays stable in the fridge for approximately 28-30 days. After that, potency drops and the solution should be discarded. Understanding tirzepatide expiration is critical for maintaining dose accuracy over time.
Where 10 mg fits in the tirzepatide dosing schedule
The 10 mg dose is not where anyone starts. It is the fourth tier in the standard tirzepatide escalation schedule, and reaching it means you have already spent at least 12 weeks building tolerance through lower doses. Understanding where 10 mg sits in the full tirzepatide dose schedule gives important context for what to expect.
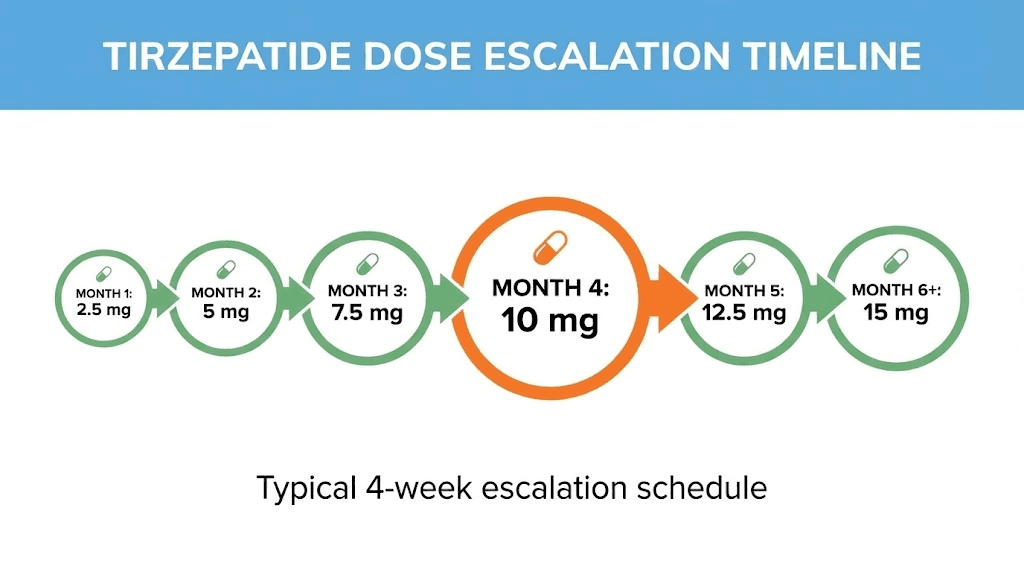
The standard escalation timeline
The FDA-approved tirzepatide dosing schedule follows a slow escalation pattern designed to minimize gastrointestinal side effects:
Weeks 1-4: 2.5 mg weekly (starting dose, not therapeutic)
Weeks 5-8: 5 mg weekly (first therapeutic dose)
Weeks 9-12: 7.5 mg weekly
Weeks 13-16: 10 mg weekly
Weeks 17-20: 12.5 mg weekly
Weeks 21+: 15 mg weekly (maximum dose)
Some protocols extend the time at each dose beyond four weeks, and that is perfectly acceptable. The four-week minimum exists because it takes approximately that long for side effects to stabilize at each new dose level. Rushing the escalation is one of the most common mistakes covered in the tirzepatide not working troubleshooting guide.
Not everyone needs to reach 10 mg. Some people achieve excellent results at 5 mg or 7.5 mg and stay there. The decision to increase should be based on whether the current dose is still producing adequate appetite suppression and weight loss, not on a predetermined schedule. The tirzepatide dosing for weight loss conversion chart helps evaluate whether escalation makes sense for your situation.
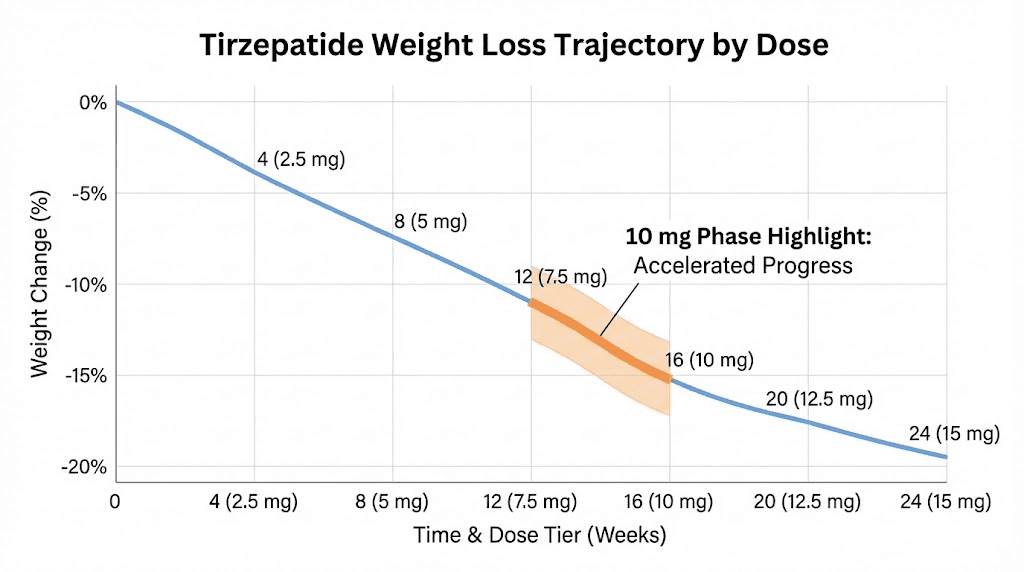
Clinical results at the 10 mg dose
The SURMOUNT-1 clinical trial provides the best data on what the 10 mg dose can achieve. In that 72-week trial, participants on the 10 mg weekly dose experienced remarkable results.
Average weight loss was 19.5% of starting body weight. For someone who started at 220 pounds, that is approximately 43 pounds. For a 250-pound starting weight, nearly 49 pounds. The numbers are significant by any standard.
Looking deeper, 89% of participants on the 10 mg dose lost at least 5% of their body weight. That threshold matters because even modest weight loss of 5-10% produces measurable improvements in blood pressure, blood sugar, cholesterol, and metabolic health markers. Perhaps more impressively, 50% of participants on 10 mg lost 20% or more of their starting weight. Half the group. That kind of result was nearly unheard of with previous weight loss medications.
These results are not guaranteed for every individual. Genetics, diet, activity level, and adherence all play roles. But they establish 10 mg as a highly effective dose tier that sits right in the middle of the available range. Many people find their maintenance dose somewhere between 7.5 mg and 12.5 mg, making 10 mg one of the most commonly used long-term doses. To see real-world outcomes, the tirzepatide before and after collection shows what consistent use at various doses looks like over time.
How 10 mg compares to other GLP-1 options
If you are comparing tirzepatide 10 mg to semaglutide, the semaglutide vs tirzepatide comparison is essential reading. In the SURMOUNT trials, tirzepatide 10 mg outperformed the maximum dose of semaglutide (2.4 mg) for weight loss. Tirzepatide works through dual GIP and GLP-1 receptor agonism, while semaglutide targets only GLP-1. That dual mechanism is believed to contribute to the enhanced efficacy.
For those considering a switch between the two, the semaglutide to tirzepatide conversion chart provides dose equivalency guidance. And if you are curious about newer alternatives, the survodutide vs tirzepatide and orforglipron vs tirzepatide comparisons cover the next generation of GLP-1 therapies.
Detailed conversion tables by concentration
The master table earlier in this article gave you the quick answer for 10 mg specifically. But if you are at the 10 mg dose tier, you probably also need to know conversions for nearby doses, since you may have recently stepped up from 7.5 mg or might be considering moving to 12.5 mg soon. Here are complete conversion tables for every common concentration, covering the full dose range.
5 mg/mL concentration
Dose (mg) | Units | Volume (mL) |
|---|---|---|
2.5 mg | 50 units | 0.50 mL |
5.0 mg | 100 units | 1.00 mL |
7.5 mg | 150 units | 1.50 mL |
10.0 mg | 200 units | 2.00 mL |
12.5 mg | 250 units | 2.50 mL |
15.0 mg | 300 units | 3.00 mL |
As the table makes clear, 5 mg/mL is not practical for doses of 10 mg and above. You would need multiple syringes or a larger non-insulin syringe. This concentration works best for lower doses early in the tirzepatide injection dosage schedule.
10 mg/mL concentration
Dose (mg) | Units | Volume (mL) |
|---|---|---|
2.5 mg | 25 units | 0.25 mL |
5.0 mg | 50 units | 0.50 mL |
7.5 mg | 75 units | 0.75 mL |
10.0 mg | 100 units | 1.00 mL |
12.5 mg | 125 units | 1.25 mL |
15.0 mg | 150 units | 1.50 mL |
The 10 mg/mL concentration is the Goldilocks option for the 10 mg dose. Exactly 100 units. Exactly 1 mL. Nothing to round. Nothing to estimate. If you are reconstituting your own vials, choosing this concentration eliminates measurement ambiguity entirely at the 10 mg dose level. The compound tirzepatide dosing chart often defaults to this concentration for exactly this reason.
20 mg/mL concentration
Dose (mg) | Units | Volume (mL) |
|---|---|---|
2.5 mg | 12.5 units | 0.125 mL |
5.0 mg | 25 units | 0.25 mL |
7.5 mg | 37.5 units | 0.375 mL |
10.0 mg | 50 units | 0.50 mL |
12.5 mg | 62.5 units | 0.625 mL |
15.0 mg | 75 units | 0.75 mL |
This is the most popular concentration from compounding pharmacies. At 10 mg, you draw exactly 50 units. That is a clean, easy-to-read mark on any insulin syringe. The Southend pharmacy tirzepatide dosage chart and Mochi tirzepatide dosage chart both reference this concentration frequently.
One thing to watch: the lower doses (2.5 mg and 7.5 mg) produce half-unit readings at this concentration. Drawing exactly 12.5 or 37.5 units requires a syringe with half-unit markings or very careful estimation. This is typically not an issue at the 10 mg dose level, but it matters if you are also drawing doses for the earlier escalation phase from the same vial.
30 mg/mL concentration
Dose (mg) | Units | Volume (mL) |
|---|---|---|
2.5 mg | 8.3 units | 0.083 mL |
5.0 mg | 16.7 units | 0.167 mL |
7.5 mg | 25 units | 0.25 mL |
10.0 mg | 33.3 units | 0.333 mL |
12.5 mg | 41.7 units | 0.417 mL |
15.0 mg | 50 units | 0.50 mL |
The 30 mg/mL concentration produces decimal readings for 10 mg. Draw to 33 units and accept the minor rounding. At this concentration, the difference between 33 and 34 units is 0.3 mg, which will not meaningfully affect your results. Consistency matters more than perfection. Draw the same amount each week, and your body adjusts to whatever small variation exists. Your dosage chart in mL can help you cross-reference these numbers.
40 mg/mL concentration
Dose (mg) | Units | Volume (mL) |
|---|---|---|
2.5 mg | 6.25 units | 0.0625 mL |
5.0 mg | 12.5 units | 0.125 mL |
7.5 mg | 18.75 units | 0.1875 mL |
10.0 mg | 25 units | 0.25 mL |
12.5 mg | 31.25 units | 0.3125 mL |
15.0 mg | 37.5 units | 0.375 mL |
At 40 mg/mL, 10 mg equals exactly 25 units. Clean number. Easy read. The injection volume of 0.25 mL is small, which means less discomfort at the injection site. The tradeoff is that lower doses become extremely small volumes that are harder to measure precisely, which matters if you are sharing a vial with someone at a different dose tier or using the same vial across your entire escalation.
60 mg/mL concentration
Dose (mg) | Units | Volume (mL) |
|---|---|---|
2.5 mg | 4.2 units | 0.042 mL |
5.0 mg | 8.3 units | 0.083 mL |
7.5 mg | 12.5 units | 0.125 mL |
10.0 mg | 16.7 units | 0.167 mL |
12.5 mg | 20.8 units | 0.208 mL |
15.0 mg | 25 units | 0.25 mL |
Very concentrated. Very small volumes. The 10 mg dose at this concentration is under 17 units, which is a tiny amount of liquid. Precision is critical here. A half-unit syringe (0.3 mL or 0.5 mL with half-unit graduation marks) provides much better accuracy than a standard 1 mL syringe at these volumes. The peptide dosage chart discusses syringe selection based on the volume you need to measure.
What to expect when you reach the 10 mg dose
Reaching 10 mg is a milestone. You have been on tirzepatide for at least three months at this point, likely longer if you spent extra time at any dose tier. Your body has adapted to the GLP-1 and GIP receptor agonism, but the jump from 7.5 mg to 10 mg still brings noticeable changes for most people.
Appetite suppression
Most people report the strongest wave of appetite suppression during the first two weeks at a new dose. At 10 mg, this can be quite pronounced. Food simply does not sound appealing. Some people have to set reminders to eat because their natural hunger signals go quiet. This is the mechanism working as intended, but it is important to still consume adequate protein and nutrients even when you do not feel hungry.
The tirzepatide appetite suppression timeline explains how this effect develops and stabilizes. After the initial surge, appetite suppression typically settles into a steady, manageable level by weeks 3-4 at the new dose. If you experienced strong appetite suppression at 7.5 mg that faded before your dose increase, 10 mg typically restores and exceeds that level of control.
Weight loss trajectory
Weight loss at the 10 mg dose tends to be steady rather than dramatic. The largest drops usually happen earlier in treatment, during the transition from no medication to the first therapeutic dose. By the time you reach 10 mg, your body has established a new metabolic baseline, and weight comes off at a consistent but slightly slower rate. That is normal and expected.
In the SURMOUNT-1 trial, participants on 10 mg lost an average of about 0.5-1% of their body weight per week during the active loss phase. That translates to roughly 1-2 pounds per week for most people. It adds up. Week after week, month after month, those steady losses compound into the dramatic before and after results you see in forums and research reports.
If weight loss has stalled before you reached 10 mg, the dose increase often breaks through the plateau. The troubleshooting guide for tirzepatide weight loss covers strategies beyond just increasing the dose, including dietary adjustments and timing considerations.
Energy and mood changes
Some people report increased energy at the 10 mg dose compared to lower doses. This may seem counterintuitive since you are eating less, but tirzepatide affects more than just appetite. The dual GIP/GLP-1 mechanism influences glucose metabolism, insulin sensitivity, and inflammatory markers, all of which can affect how you feel day to day. The tirzepatide and energy article digs into the mechanisms behind this effect.
Others report the opposite. Reduced caloric intake at this dose can cause fatigue, especially during the first two weeks. The body needs time to adapt to running on fewer calories. If tiredness persists beyond the adjustment period, it usually signals insufficient protein or calorie intake rather than a medication issue. The GLP-1 fatigue guide offers targeted strategies for managing this.
Side effects at the 10 mg dose and how to manage them
Side effects at 10 mg follow the same general pattern as lower doses: gastrointestinal symptoms dominate the first two weeks, then fade. But the intensity can increase compared to what you experienced at 7.5 mg. Your body is processing 33% more medication, and that difference is noticeable for some people.
Nausea
The most common side effect at any dose. At 10 mg, nausea typically appears 1-3 days after your first injection at the new dose. It peaks around days 2-5, then gradually improves. Most people find it manageable by week two. By week three to four, it is usually gone or reduced to mild, intermittent discomfort.
Management strategies that work: eat smaller, more frequent meals. Avoid high-fat foods during the first week at the new dose. Stay hydrated. Ginger tea or ginger chews can help. Some people find that taking their injection in the evening rather than the morning reduces daytime nausea. The best time to take your GLP-1 shot guide covers timing strategies in detail.
If nausea is severe enough to prevent eating for more than 48 hours, that warrants medical attention. Dehydration from persistent vomiting is the most serious risk associated with dose escalation.
Constipation and digestive slowdown
Tirzepatide slows gastric emptying. That is part of how it reduces appetite. But slower gastric emptying also means slower transit through the entire digestive system, which can cause constipation. At 10 mg, this effect intensifies.
The tirzepatide constipation treatment guide covers evidence-based approaches: adequate fiber intake (25-30 grams daily), sufficient water consumption (aim for half your body weight in ounces), magnesium supplementation (particularly magnesium citrate, which has a mild osmotic laxative effect), and regular physical activity. If dietary measures fail, a gentle over-the-counter stool softener can help during the transition period.
Headaches
Less common than nausea but still reported by a meaningful percentage of users at the 10 mg dose. Tirzepatide-related headaches are usually mild and often linked to dehydration or blood sugar fluctuations rather than a direct effect of the medication. Eating regular meals, staying hydrated, and monitoring blood sugar (if applicable) usually resolves them. The broader GLP-1 headache guide explores this topic further.
Injection site reactions
At 10 mg, the injection volume is larger than at lower doses (assuming the same concentration). Larger volumes can cause more noticeable redness, swelling, or itching at the injection site. Rotating injection sites between the abdomen, thigh, and upper arm minimizes this. The stomach injection technique guide and injection site selection guide provide specific guidance on rotation patterns and proper technique.
Let the solution reach room temperature before injecting. Cold injections sting more and cause more local irritation. Fifteen to twenty minutes outside the refrigerator is usually sufficient. Just do not leave reconstituted tirzepatide at room temperature for extended periods, as the storage stability guidelines explain.
Muscle and joint discomfort
Some users report muscle pain, body aches, or joint discomfort at the 10 mg dose. These are less common than GI symptoms but worth knowing about. They are typically mild, transient, and resolve within the first few weeks. Adequate protein intake (at least 0.7-1.0 grams per pound of body weight) helps preserve muscle mass and may reduce these symptoms. The supplements to take with tirzepatide guide covers nutritional support strategies.
Sleep disruption
Tirzepatide and sleep is a topic that does not get enough attention. Some users find their sleep quality changes, either improving or worsening, when they step up to 10 mg. Changes in eating patterns, blood sugar levels, and body composition all affect sleep. If insomnia develops at the new dose, it usually stabilizes within two to three weeks.
Hair thinning
This is not a direct side effect of tirzepatide itself but rather a consequence of rapid weight loss, a condition called telogen effluvium. When the body loses weight quickly, it can shift hair follicles from the growth phase to the resting phase, causing increased shedding roughly three to six months after significant weight loss begins. The GLP-1 hair loss guide explains the mechanism and evidence-based strategies for prevention and management. Ensuring adequate protein, biotin, iron, and zinc intake helps minimize this effect.
When to contact your healthcare provider
Most side effects at the 10 mg dose are mild and self-limiting. However, contact a healthcare provider if you experience severe abdominal pain that does not resolve, persistent vomiting lasting more than 48 hours, signs of pancreatitis (severe upper abdominal pain radiating to the back), signs of allergic reaction (difficulty breathing, severe rash, swelling), or vision changes. These are rare but serious. The side effects comparison between semaglutide and tirzepatide provides additional context on the safety profile of both medications.
Common mistakes when measuring 10 mg of tirzepatide
Mistakes happen. Some are harmless. Others can significantly affect your results or safety. Here are the ones that come up repeatedly in tirzepatide dosing discussions.
Mistake 1: assuming all vials have the same concentration
This is the most dangerous mistake. Someone has been drawing 50 units from a 20 mg/mL vial for their 10 mg dose. They get a new vial. Same pharmacy. Same label design. But this time the concentration is 10 mg/mL. They draw 50 units out of habit. Instead of 10 mg, they just injected 5 mg. Half the intended dose.
The reverse is worse. Going from 10 mg/mL to 20 mg/mL and drawing the same 100 units means injecting 20 mg instead of 10 mg. Double the dose. That can trigger severe nausea, vomiting, and other gastrointestinal distress that could require medical attention.
Prevention is simple: read the vial label before every single injection. Even if you think you know the concentration. Even if the vial looks the same. Verify the concentration and recalculate. The tirzepatide conversion chart should be your constant reference when switching between vials.
Mistake 2: confusing units with milligrams
Units and milligrams are not the same thing. Drawing 10 units does not give you 10 mg unless your concentration happens to be 100 mg/mL (which would be extremely unusual). At the most common concentration of 20 mg/mL, 10 units equals only 2 mg, not 10 mg. Understanding this distinction is fundamental, and the peptide dosage calculation guide explains it thoroughly.
Mistake 3: not accounting for dead space
Every syringe has dead space, the small amount of liquid that remains in the needle hub and syringe tip after you push the plunger all the way down. On a standard insulin syringe, dead space is typically 0.5-2 units. At low concentrations, this is negligible. But at high concentrations like 60 mg/mL, 2 units of dead space equals 1.2 mg of tirzepatide. Over time, that adds up.
Low dead space syringes are available and worth using if you are working with highly concentrated solutions. They minimize waste and improve dose accuracy. The peptide dosing guide covers syringe selection in detail.
Mistake 4: not purging air bubbles properly
Air bubbles take up space in the syringe that should be occupied by your tirzepatide solution. A visible air bubble of 5 units means you are 5 units short on your dose. At 20 mg/mL, that is 1 mg less tirzepatide than intended.
After drawing your dose, hold the syringe needle-up and tap the barrel gently to move bubbles to the top. Push the plunger slightly to expel the air, then verify your volume is correct. Pull a tiny bit more solution if you expelled too much. This takes 10 seconds and ensures accurate dosing every time.
Mistake 5: rushing the escalation to reach 10 mg
Impatience kills results. Skipping from 5 mg straight to 10 mg, or shortening the four-week minimum at 7.5 mg, dramatically increases the risk of severe side effects. The escalation schedule exists for a reason. Each dose tier gives your GI system time to adapt. Rushing it does not produce faster weight loss. It produces more nausea, more vomiting, and sometimes causes people to abandon tirzepatide entirely. The tirzepatide not working guide frequently traces stalled results back to improper escalation.
Tips for accurate syringe measurements
Getting the right number of units into your syringe requires technique, not just math. These tips come from experienced researchers who measure tirzepatide doses weekly and have refined their process over months of practice.
Choose the right syringe size
Match your syringe to your injection volume. If you need 50 units, a 1 mL (100 unit) syringe works fine. The 50-unit mark is clearly visible and easy to hit. But if you need 17 units (as with a 60 mg/mL concentration), a 0.3 mL syringe with half-unit markings gives you much better precision. The graduation marks are closer together, making it easier to land exactly where you need to be.
For most people at the 10 mg dose with a 20 mg/mL concentration (50 units), a standard 1 mL insulin syringe is perfectly adequate. Use the SeekPeptides peptide calculator to verify your numbers before drawing.
Read at eye level
Hold the syringe at eye level when reading the measurement. Looking down at the syringe from above creates parallax error, making the liquid level appear higher than it actually is. Looking up from below has the opposite effect. Eye level gives you the true reading.
Read the bottom of the meniscus
Liquid in a syringe curves slightly at the surface. This curve is called the meniscus. Read the measurement at the bottom of the curve, where the liquid meets the flat part of the surface. Reading the top of the curve overestimates your volume.
Use consistent technique
The exact number matters less than consistency. If you consistently draw to 50 units the same way each week, your dose is consistent each week, even if the true volume varies by a fraction of a unit due to reading angle or bubble size. Consistency is what creates predictable results over the course of a tirzepatide weight loss protocol.
Double-check with the formula
Before your first injection at any new concentration, run the formula: (Dose in mg / Concentration in mg per mL) x 100 = Units. Write the answer down. Tape it to your refrigerator if you need to. Do not rely on memory or habit, especially when switching between concentrations or pharmacies.
Switching concentrations safely
At some point, most people switch between concentrations. Maybe your pharmacy changes their formulation. Maybe you switch pharmacies. Maybe you reconstituted your own vial at a different concentration than your previous one. Whatever the reason, switching concentrations is the single highest-risk moment for dosing errors.
The critical recalculation step
When you receive a vial at a new concentration, recalculate everything from scratch. Do not adjust your old number by a ratio. Do not try to do the math in your head. Sit down with the formula and calculate your new units.
Example: You have been drawing 50 units from a 20 mg/mL vial for your 10 mg dose. Your new vial is 10 mg/mL.
New calculation: (10 mg / 10 mg per mL) x 100 = 100 units.
You now need to draw 100 units, double what you were drawing before. If you had drawn 50 units from the new vial out of habit, you would have only gotten 5 mg. Half your dose. Your appetite suppression would fade, your weight loss progress would stall, and you might think tirzepatide stopped working.
The switching dosage charts are designed for exactly this scenario. Use them every time you change vials, even if you think the concentration is the same. A five-second label check prevents a week of suboptimal dosing or a dangerous overdose.
Keeping a dosing journal
Simple but effective. Write down the date, your vial concentration, your dose in milligrams, and the number of units you drew. This creates a record you can reference if something seems off. It also helps track your progress over time, which is valuable for making informed decisions about dose escalation or maintenance.
Nutrition and lifestyle at the 10 mg dose
The 10 mg dose suppresses appetite significantly. That is the whole point. But it also means you need to be more intentional about what you eat, because you will be eating less of it. The tirzepatide diet plan and meal plan guide provide structured approaches, but here are the key principles.
Protein is non-negotiable
At minimum, aim for 0.7 grams of protein per pound of body weight daily. Ideally, closer to 1 gram per pound if you are exercising. Protein preserves muscle mass during weight loss, supports metabolic rate, and helps prevent the muscle wasting that can occur with rapid caloric restriction. Protein shakes designed for GLP-1 users make hitting this target easier when appetite is low.
Since you may only feel like eating one or two meals per day at the 10 mg dose, those meals need to be protein-dense. Chicken, fish, eggs, Greek yogurt, cottage cheese. Protein first, then vegetables, then everything else. If you are not hungry for a full meal, a protein shake between meals can bridge the gap.
Foods to prioritize and avoid
The what to eat on tirzepatide guide goes deep on this, but the short version: prioritize lean proteins, vegetables, fruits, and whole grains. Avoid greasy or high-fat foods, which can worsen nausea. Avoid carbonated beverages, which can increase bloating. And the foods to avoid on tirzepatide article lists specific items that commonly trigger GI distress at higher doses.
Hydration
Dehydration is sneaky at the 10 mg dose. You are eating less, which means you are getting less water from food. Tirzepatide can also cause nausea and diarrhea, both of which deplete fluids. Aim for at least half your body weight in ounces of water per day. A 200-pound person should drink at least 100 ounces daily. More if you exercise.
Alcohol
The interaction between tirzepatide and alcohol is worth understanding before you reach the 10 mg dose. Many users report lower alcohol tolerance, faster intoxication, and worse hangovers. The tirzepatide and alcohol guide covers the mechanisms and provides practical guidelines. The short answer: if you drink, reduce your intake and expect stronger effects.
Supplements
Certain supplements pair well with tirzepatide at the 10 mg dose. Magnesium citrate for constipation prevention. Vitamin B12 for energy, especially if you are on a tirzepatide with B12 compound. A good multivitamin to cover potential gaps from reduced food intake. Electrolytes if you are exercising or experiencing any GI-related fluid losses.
Some compounds combine tirzepatide with additional ingredients. The tirzepatide glycine B12 compound and tirzepatide niacinamide combinations are increasingly popular. These added ingredients may provide complementary benefits, though they also mean different concentrations and conversion math, so always verify your specific formulation.
Using calculators to verify your math
SeekPeptides offers several free tools that eliminate guesswork from tirzepatide dosing calculations.
The peptide calculator handles the basic conversion: enter your vial size, the amount of water you added (or the pre-mixed concentration), and your desired dose. It tells you exactly how many units to draw. No formula required. No mental math. Just verified numbers you can trust.
The peptide reconstitution calculator works backward, helping you determine how much bacteriostatic water to add to achieve your desired concentration. If you want 10 mg to equal exactly 50 units (requiring a 20 mg/mL concentration), the calculator tells you precisely how much water to add to your specific vial size.
The semaglutide dosage calculator is also worth knowing about if you are comparing or considering switching from tirzepatide to semaglutide or running the medications in sequence.
These tools exist because conversion errors happen, even to experienced researchers. A calculator does not get tired, does not confuse concentrations, and does not make arithmetic mistakes. Use it every time you reconstitute a new vial or receive a new shipment. SeekPeptides members find that building the calculator into their weekly routine eliminates the anxiety that comes with manual dosing math.
Tirzepatide delivery methods beyond injection
While injection remains the standard delivery method, alternative forms of tirzepatide are gaining attention. If syringes and units are not your preferred approach, it is worth knowing what else exists.
Oral tirzepatide is in advanced clinical trials and shows promising bioavailability. The conversion from injection to oral dosing is different because absorption rates vary, so direct mg-to-mg comparison does not apply. The oral vs injection comparison covers the current state of research.
Tirzepatide drops (sublingual formulations) and tablet formulations are also being explored. These bypass the syringe entirely, which eliminates the unit conversion question altogether. However, they come with their own dosing considerations that the sublingual dosage chart addresses.
For now, subcutaneous injection remains the most reliable and well-studied delivery method for tirzepatide. The GLP-1 injection technique guide ensures you are getting the most out of each dose regardless of which concentration you use.
Planning ahead: what comes after 10 mg
If 10 mg is working well and you are satisfied with your results, you can stay at this dose indefinitely. Not everyone needs to reach 15 mg. Many people find their optimal balance between effectiveness and tolerability somewhere in the 7.5-12.5 mg range.
But if your weight loss has plateaued at 10 mg and you want to increase, the next step is 12.5 mg. At your current concentration, that means recalculating your units. For reference:
Concentration | Units for 12.5 mg |
|---|---|
10 mg/mL | 125 units |
20 mg/mL | 62.5 units |
30 mg/mL | 41.7 units |
40 mg/mL | 31.25 units |
60 mg/mL | 20.8 units |
Notice that 12.5 mg at 10 mg/mL requires 125 units, which exceeds a single 1 mL insulin syringe. If you plan to go above 10 mg and your concentration is 10 mg/mL, you will either need a larger syringe or a more concentrated solution. Planning ahead for this is wise. The complete tirzepatide dosage chart in units covers every dose and concentration combination through the maximum 15 mg dose.
The decision to increase, maintain, or decrease your dose should be based on your results, your tolerance of side effects, and your overall health goals. The tirzepatide timeline guide helps set realistic expectations for each dose tier.
Storage and handling for dose accuracy
Even perfect dosing math becomes meaningless if the tirzepatide in your vial has degraded due to improper storage. The tirzepatide refrigeration guide covers the full details, but here is the summary relevant to maintaining accurate 10 mg doses.
Reconstituted tirzepatide should be stored at 2-8 degrees Celsius (36-46 degrees Fahrenheit). That is the main body of your refrigerator, not the door (too much temperature fluctuation) and not near the back wall (risk of freezing). Freezing destroys the peptide.
The vial is good for approximately 28-30 days after reconstitution. Mark the reconstitution date clearly on the vial. If you are using a 30 mg vial and drawing 10 mg weekly, that gives you exactly three weeks of doses per vial, well within the stability window.
Pre-mixed solutions from compounding pharmacies may have different stability periods depending on their formulation and preservatives. Follow the pharmacy-specific storage instructions. The room temperature stability guide covers what happens when tirzepatide is left unrefrigerated and how long it remains usable.
If your solution changes color, becomes cloudy, or develops visible particles, do not use it. These are signs of degradation or contamination. Using a degraded solution means your actual dose could be lower than what you calculated, leading to inconsistent results. The peptide storage guide provides comprehensive stability information.
Comparing 10 mg across different pharmacy charts
Different compounding pharmacies ship tirzepatide at different concentrations and provide their own dosing charts. If you have switched pharmacies and the new chart looks different, do not panic. The same dose of tirzepatide produces the same effect regardless of the concentration it was dissolved in. The only thing that changes is the volume (and therefore the units) you draw.
Here is how 10 mg looks across popular pharmacy-specific charts:
Pharmacy/Chart | Typical concentration | Units for 10 mg |
|---|---|---|
20 mg/mL | 50 units | |
20 mg/mL | 50 units | |
Varies | Check label | |
Varies | Check label |
The pattern is clear: always check the label. Always verify the concentration. Always recalculate if anything has changed. The compounded tirzepatide dosage calculator handles the math for any pharmacy formulation.
Microdosing considerations relative to 10 mg
Some researchers use microdosing protocols where they split their weekly 10 mg dose into multiple smaller injections throughout the week. Instead of one injection of 10 mg (50 units at 20 mg/mL), they might inject 5 mg twice per week (25 units each time) or even smaller amounts more frequently.
The tirzepatide microdose chart provides conversion tables for split dosing at every common concentration. Splitting the dose can reduce side effects by maintaining more stable drug levels, but it also means more injections per week and more opportunities for measurement error.
If microdosing interests you, the math is the same. Just divide your total weekly dose by the number of injections and apply the formula to each smaller dose. For example, 10 mg split into two doses means 5 mg per injection. At 20 mg/mL, that is 25 units per injection, twice per week.
Combining tirzepatide with other compounds
At the 10 mg dose level, some researchers add complementary compounds to their protocol. Common additions include:
Vitamin B12 is the most common addition, often compounded directly into the tirzepatide solution. Some pharmacies offer pre-mixed tirzepatide with B12. B12 supports energy levels and may help offset the fatigue that some users experience at higher doses.
Glycine is another popular addition. It may support liver function and improve sleep quality. The tirzepatide with glycine combination is available from certain compounding pharmacies.
AOD-9604 is sometimes stacked with tirzepatide for enhanced fat loss. This is a separate injection with its own dosing protocol.
Important: when tirzepatide is compounded with additional ingredients (B12, glycine, niacinamide), the concentration and therefore the unit conversion can be different from plain tirzepatide solutions. Always verify the tirzepatide concentration specifically, not the total solution volume. The glycine B12 compound guide provides detailed dosing instructions for these multi-ingredient formulations.
When timing matters for your 10 mg injection
Tirzepatide is a once-weekly injection. Pick a day. Stick with it. Consistency matters more than the specific day. But timing within the day can make a difference for some people.
Some find that injecting in the morning leads to stronger nausea during the day. They switch to evening injections and tolerate the dose better because the peak nausea window occurs overnight while they sleep. Others prefer morning injections because they want the appetite suppression strongest during waking hours when food is accessible.
The best time to take your GLP-1 shot article covers the timing debate in depth. There is no universally correct answer. Experiment with morning versus evening and note how you feel. The 10 mg dose is strong enough that timing can make the difference between tolerable and miserable side effects during the first few days after each injection.
On the question of taking tirzepatide early, you have some flexibility. A day early or a day late is generally fine. The half-life of tirzepatide is approximately 5 days, which means the drug remains active well beyond the 7-day dosing interval. That pharmacokinetic buffer means minor scheduling shifts do not significantly affect your blood levels or results.
Understanding related conversion questions
If you arrived at this article looking for 10 mg specifically, you might also need conversion information for adjacent doses. Here are the most commonly searched dose-specific conversion guides from SeekPeptides:
How many units is 2.5 mg of tirzepatide (starting dose)
How many units is 5 mg of tirzepatide (first therapeutic dose)
How many units is 7.5 mg of tirzepatide (third dose tier)
How many mg is 20 units of tirzepatide (reverse conversion)
How many mg is 30 units of tirzepatide (reverse conversion)
How many mg is 40 units of tirzepatide (reverse conversion)
How many mg is 50 units of tirzepatide (reverse conversion)
And for the complete picture across all doses and concentrations, the tirzepatide dosage chart in units is the definitive reference.
Special considerations for women
The 10 mg dose affects men and women differently in some respects. Women generally experience stronger appetite suppression at lower doses and may find 10 mg very potent. The clinical trials showed slightly different weight loss percentages by sex, though both groups achieved significant results.
For women of reproductive age, tirzepatide carries specific considerations. The tirzepatide and menstrual cycle article covers how weight loss and GLP-1 agonism can affect periods. The pregnancy on tirzepatide and breastfeeding while on tirzepatide guides address the safety considerations that matter for women at this dose level.
For a broader look at how peptides, including tirzepatide, apply specifically to women, the safe peptides for women guide and the peptides for women over 40 article provide gender-specific guidance. Understanding how the 10 mg dose interacts with female physiology helps set appropriate expectations for results and side effect management.
Frequently asked questions
Is 10 mg of tirzepatide a high dose?
It is a moderate dose. The approved range goes from 2.5 mg to 15 mg. At 10 mg, you are past the starting phase and into the therapeutic range, but you still have room to increase if needed. Many people find their maintenance dose at 10 mg, making it one of the most commonly used long-term doses according to the tirzepatide dose chart.
Can I draw 10 mg in one injection?
Yes, as long as your concentration allows it. At 20 mg/mL (50 units) and above, 10 mg fits easily in a single 1 mL insulin syringe. At 10 mg/mL (100 units), it fills the entire syringe. At 5 mg/mL (200 units), you would need two syringes, which is impractical and should be avoided by using a higher concentration.
How do I know if my concentration is mg/mL or something else?
The vial label will state the concentration. It is almost always expressed in mg/mL. If it says "10 mg/mL" that means each milliliter of solution contains 10 milligrams of tirzepatide. If you reconstituted the vial yourself, divide the total milligrams of powder by the milliliters of water you added. The peptide dosage calculation guide covers this in detail.
What if I accidentally draw too much or too little?
If you drew too much, push the excess back into the vial before injecting. If you drew too little, pull more solution until you reach the correct mark. If you already injected an incorrect amount, do not take a corrective injection. Accept the slightly off dose for this week and be more careful next time. A single slightly high or low dose is not dangerous. Consistency over time is what matters.
How long until I see results at the 10 mg dose?
If you are stepping up from 7.5 mg, most people notice increased appetite suppression within the first week. Weight loss typically becomes apparent within 2-3 weeks. Full effects stabilize by week 4. The tirzepatide results timeline provides week-by-week expectations.
Should I stay at 10 mg or keep increasing?
Stay at 10 mg if you are still losing weight at a satisfactory rate (0.5-1% of body weight per week), your appetite is well-controlled, side effects are manageable, and you are progressing toward your goal. Increase only if weight loss has genuinely plateaued despite proper diet and exercise adherence. The troubleshooting guide helps distinguish between a true plateau and a temporary stall.
Can I use a tuberculin syringe instead of an insulin syringe?
Yes. A 1 mL tuberculin syringe measures in milliliters rather than units, but the conversion is straightforward: 1 mL = 100 units. So for 10 mg at 20 mg/mL, you would draw to the 0.50 mL mark on a tuberculin syringe, which equals 50 units on an insulin syringe. Some people actually prefer tuberculin syringes for higher-concentration solutions because the mL markings can be easier to read at small volumes.
Does the needle gauge affect the dose?
No. Needle gauge (thickness) affects comfort and injection speed but not the amount of medication delivered. Common gauges for subcutaneous tirzepatide injection are 27-31 gauge. Thinner needles (higher gauge numbers) hurt less but take longer to draw and inject. The injection technique guide covers needle selection in detail.
External resources
For researchers serious about getting every dose right, SeekPeptides provides the most comprehensive tirzepatide resource available, with evidence-based dosing guides, verified calculators, and a community of thousands who have navigated these exact conversion questions.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay verified, your measurements stay precise, and your results stay consistent.