Feb 25, 2026
Experienced researchers understand something about tirzepatide that most beginners overlook completely. The question is not simply how long a single injection lasts. It is how the drug builds in your system over weeks, how it interacts with your body unique chemistry, and how long its effects truly persist after you stop injecting. These are fundamentally different questions, and confusing them leads to wrong expectations, poor timing, and frustrating results.
Tirzepatide, the dual GIP/GLP-1 receptor agonist behind brand names like Mounjaro and Zepbound, has pharmacokinetics that surprise most people. A single injection does not simply peak and vanish. It lingers. It accumulates. And its effects ripple through your metabolism for weeks, sometimes months, after your final dose. Understanding these timelines changes how you approach tirzepatide dosing for weight loss, how you handle plateaus, and how you plan for the future.
This guide breaks down every aspect of tirzepatide duration, from molecular half-life to real-world effects, using clinical trial data and pharmacokinetic research. Whether you want to know how long tirzepatide takes to work, what happens between weekly injections, or what the weight loss timeline looks like after stopping, every answer is here. SeekPeptides members get even deeper protocol guidance, but the science belongs to everyone.
How long tirzepatide stays in your system
The short answer is approximately 25 to 30 days after your last injection. But the short answer misses everything important about how tirzepatide actually behaves inside your body.
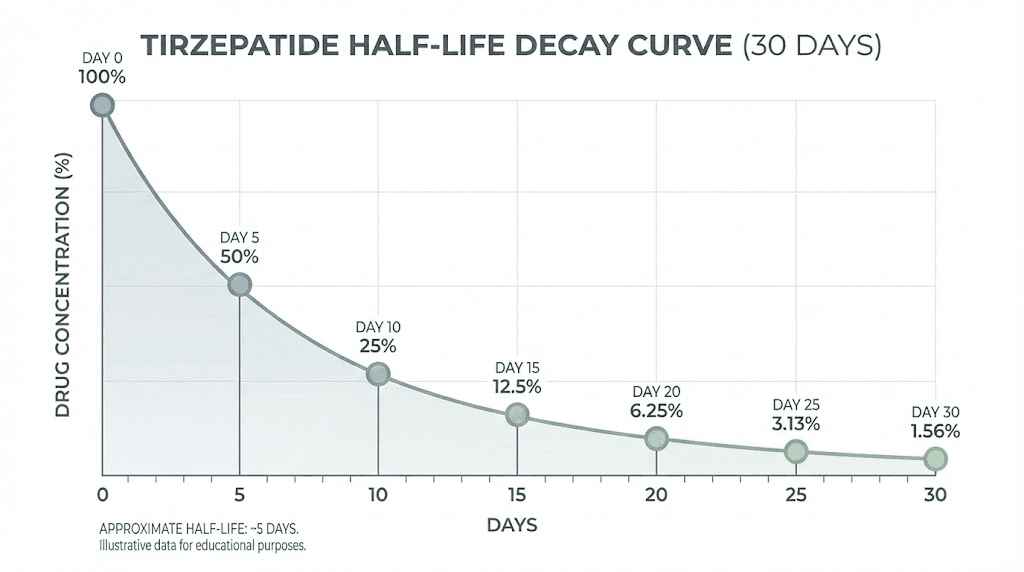
Tirzepatide has an elimination half-life of approximately 5 days, or 120 hours. That means every 5 days, the concentration of tirzepatide in your bloodstream drops by half. After one half-life, 50% remains. After two half-lives, 25%. After three, 12.5%. After four, about 6%. And after five half-lives, roughly 25 to 30 days, less than 3% of the original dose remains in circulation.
For most practical purposes, five half-lives represents complete clearance. Trace amounts might linger slightly longer, but they fall below the threshold needed to produce meaningful physiological effects.
Here is how the decline looks after a single dose:
Days after last injection | Approximate drug remaining | What you feel |
|---|---|---|
Day 0 (injection day) | 100% | Full dose administered |
Day 5 | 50% | Strong appetite suppression continues |
Day 7 (next injection due) | ~40% | Effects still present, may notice slight hunger increase |
Day 10 | 25% | Noticeable reduction in appetite suppression |
Day 15 | 12.5% | Appetite returning closer to baseline |
Day 20 | ~6% | Minimal drug effect remaining |
Day 25-30 | Less than 3% | Functionally cleared from system |
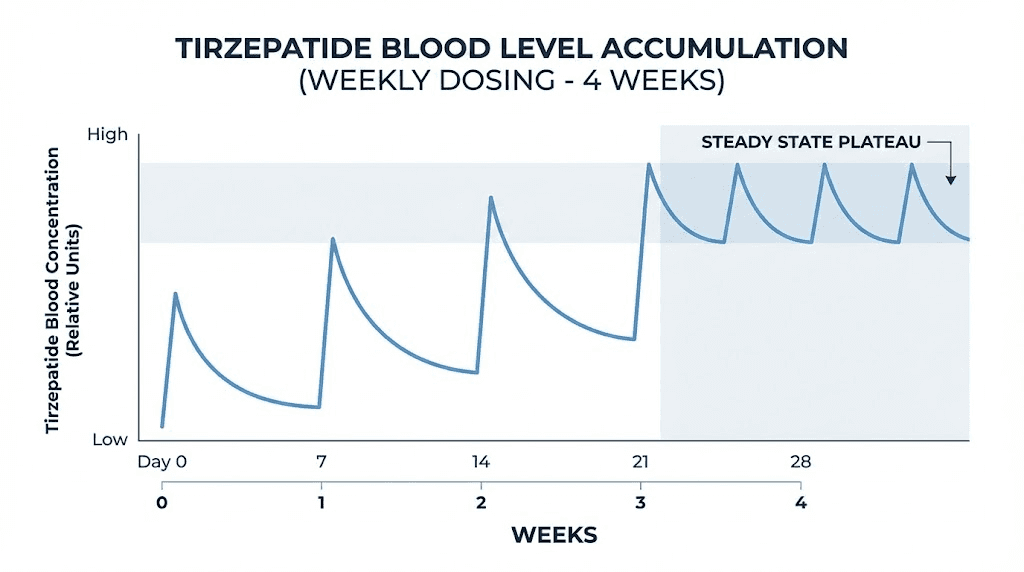
This table represents a single dose in isolation. But here is what makes tirzepatide different from a medication you take once. With weekly dosing, the drug accumulates. Each new injection adds to whatever remains from previous weeks. After about four weeks of consistent injections, you reach what pharmacologists call steady state, a consistent baseline level that the weekly dose maintains.
At steady state, the picture changes dramatically. You are not starting from zero each week. You are maintaining a reservoir. The trough level, the lowest point just before your next injection, stays high enough to maintain therapeutic effects throughout the entire dosing interval. This is why tirzepatide works faster in week four than in week one, even at the same dose.
Understanding this accumulation pattern matters for anyone wondering about starting doses, dose escalation, or why effects seem to build gradually rather than hitting full force from the first injection.
Understanding the 5-day half-life in practical terms
Half-life sounds simple. Cut the amount in half, wait five days, repeat. But the practical implications run deeper than basic math.
Tirzepatide pharmacokinetics follow a two-compartment model with first-order absorption and elimination. In plain language, this means the drug distributes between your blood (the central compartment) and your tissues (the peripheral compartment), and it moves between these spaces at predictable rates.
The central compartment volume is approximately 2.47 liters per 70 kilograms of body weight. The peripheral compartment adds another 3.98 liters. Together, the mean apparent steady-state volume of distribution comes to about 10.3 liters. For a peptide-based medication, this is relatively contained, meaning tirzepatide stays concentrated rather than spreading thin across all body tissues.
One reason tirzepatide lingers so long is its binding behavior. The peptide binds to plasma albumin at a rate of 99%. That is not a rounding up. Virtually every molecule of tirzepatide in your bloodstream attaches to albumin, the most abundant protein in your blood. This creates a slow-release effect. Instead of floating freely and getting cleared quickly, tirzepatide rides albumin through your circulation, gradually releasing from its carrier and interacting with GIP and GLP-1 receptors over days rather than hours.
This albumin binding also explains why tirzepatide clearance is remarkably slow. Population pharmacokinetic studies involving over 5,800 participants across 19 clinical trials found a clearance rate of just 0.0329 liters per hour per 70 kilograms of body weight. For comparison, that is roughly equivalent to filtering about 790 milliliters per day, less than a liter of plasma fully cleared of tirzepatide each day.
The 5-day half-life enables once-weekly dosing. This is a significant practical advantage. Unlike liraglutide, which requires daily injections due to its 13-hour half-life, tirzepatide maintains therapeutic levels with a single weekly shot. The injection process is straightforward, and the long half-life means you have flexibility in timing without losing effectiveness.
For those managing their own protocols, dosage calculators and syringe dosage guides become essential tools. The pharmacokinetics are predictable enough that consistent weekly dosing produces reliable results, but only when you understand what is happening beneath the surface.
Peak levels and how tirzepatide absorbs after injection
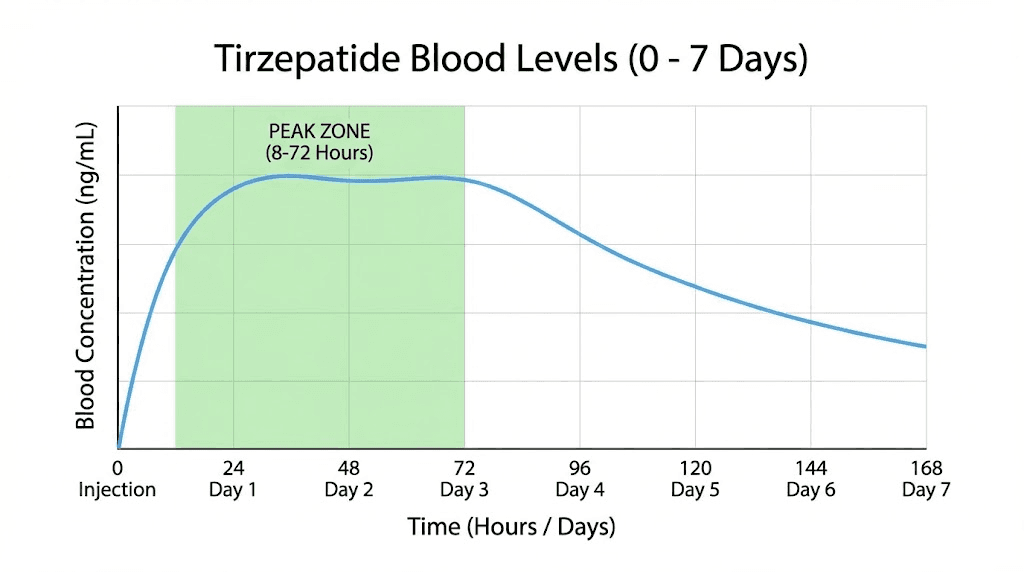
After a subcutaneous injection, tirzepatide does not hit peak levels instantly. The absorption window ranges from 8 to 72 hours, with most people reaching maximum plasma concentration somewhere between 24 and 48 hours post-injection.
That range might seem wide. It is.
Multiple factors influence absorption speed. Injection site matters. The abdomen typically offers faster absorption than the thigh, which absorbs faster than the upper arm. Blood flow to the injection area plays a role. Physical activity after injection can accelerate absorption. Temperature at the injection site can alter it too, which is one reason some people notice injection site reactions that correlate with absorption patterns.
Bioavailability sits at approximately 80%. This means that 80% of the injected dose reaches systemic circulation. The remaining 20% degrades at the injection site or gets cleared locally before entering the bloodstream. This is actually quite good for a subcutaneous peptide. Many peptide therapeutics have significantly lower bioavailability.
The practical takeaway is this: if you inject tirzepatide on Monday morning, peak blood levels arrive sometime between Monday evening and Wednesday morning. Effects on appetite and blood sugar regulation follow these peaks, though the relationship is not perfectly linear. Receptor binding and downstream signaling create effects that lag behind and persist beyond simple drug concentration curves.
For those exploring alternative delivery methods, oral tirzepatide and tirzepatide drops are emerging options with different absorption profiles. The comparison between oral and injectable forms reveals significant differences in bioavailability and peak timing. Orally disintegrating tablets represent another delivery pathway, though injectable remains the gold standard for consistent pharmacokinetics.
When preparing compounded formulations, proper reconstitution technique directly affects what you inject and how it absorbs. Using the correct amount of bacteriostatic water ensures proper concentration, and choosing the right injection site helps optimize absorption consistency from week to week.
How long tirzepatide effects last between weekly doses
Here is where theory meets daily experience. The pharmacokinetic half-life tells you how long the drug molecule persists. But what people actually care about is how long the effects last. When does appetite suppression fade? When does blood sugar regulation weaken? When do you start feeling different?
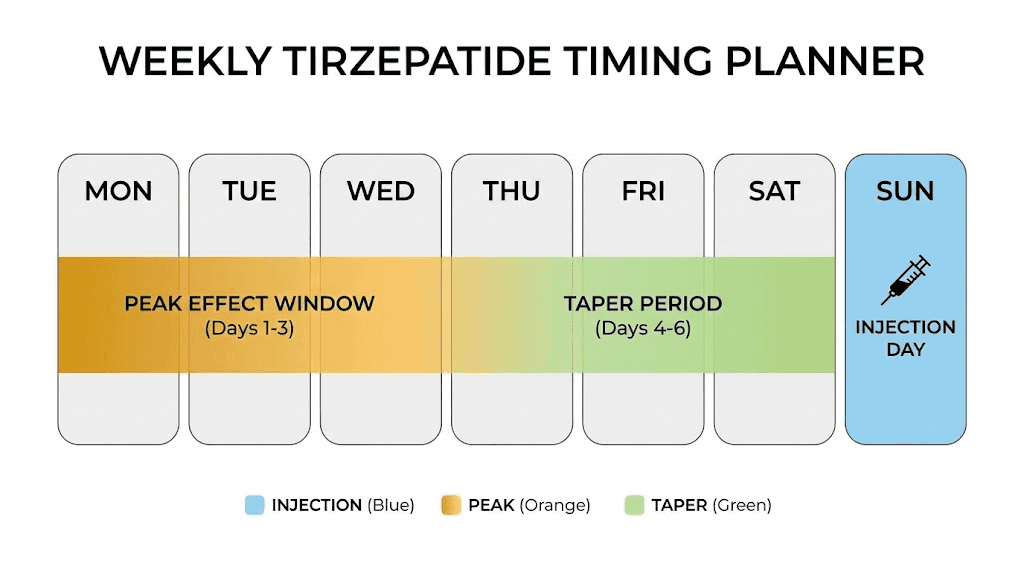
Most people on stable weekly dosing report a recognizable pattern throughout their injection cycle.
Days 1-2 after injection: Effects build as tirzepatide absorbs and reaches peak levels. Appetite suppression strengthens. Some people experience the most pronounced gastrointestinal side effects during this window, including nausea and diarrhea. These tend to moderate as the body adjusts over weeks.
Days 2-5: Peak therapeutic window. Appetite suppression is strongest. Blood sugar regulation is most effective. Many people report feeling a notable metabolic boost during this period. Cravings diminish. Satiety comes faster during meals. The foods to avoid become easier to skip when appetite suppression is at its peak.
Days 5-7: Effects begin tapering. The drug level is now roughly 40% of what it was at peak. Most people on well-titrated doses still feel meaningful appetite suppression through day seven, but some notice a subtle return of hunger or cravings in the 24 to 48 hours before their next injection. Following a structured diet plan and meal plan helps maintain consistency even as drug levels dip.
This end-of-cycle dip is normal. It does not mean your dose is too low. It reflects the natural pharmacokinetic curve of a drug with a 5-day half-life dosed every 7 days. At steady state, your trough level remains high enough to maintain the core effects, though they may feel slightly less intense compared to day two or three.
Some people wonder about splitting the dose into twice-weekly injections to flatten this curve. The idea has pharmacokinetic logic. Two smaller doses maintain more consistent blood levels with less peak-to-trough variation. However, this approach comes with trade-offs in injection frequency and is not standard protocol.
What about missed doses?
The prescribing information allows a 96-hour window, four full days, to administer a missed dose. If your injection is due on Monday and you miss it, you have until Friday to inject and stay on schedule. After that window, skip the missed dose entirely and inject on the next regular day. For those who want more detail, our guide on taking tirzepatide early covers timing flexibility from the other direction.
Taking the right supplements with tirzepatide can also support your experience between doses. Many researchers add B12, glycine, or other compounds to their protocols. Formulations like tirzepatide with B12, tirzepatide with glycine, and triple compound formulations aim to enhance the overall experience and reduce certain side effects.
Reaching steady state and what it means for your results
Steady state is where the real transformation begins. And most people do not understand what it actually means.
After approximately four weeks of consistent weekly dosing, the amount of tirzepatide entering your body each week roughly equals the amount being cleared. Your baseline drug level stabilizes. Instead of starting near zero each week, you maintain a consistent reservoir that each new injection tops up.
The accumulation ratio at steady state is approximately 1.6 to 1.7 fold. This means your average drug level at steady state is about 60 to 70 percent higher than what you would get from a single isolated dose. This is not a small difference. It explains why week four often feels dramatically different from week one, even when the dose has not changed.
Think of it like filling a bathtub with the drain partially open. The first few pours raise the water level quickly. But as the level rises, more water drains out. Eventually, the inflow and outflow equalize. Your water level, your drug level, stabilizes at a consistent height.
This steady-state concept has several practical implications.
First, appetite suppression timelines make more sense in this context. People who report minimal effects in weeks one and two are not failing. They have not reached steady state yet. The protocol calls for four weeks at each dose level before escalating, and this is precisely why. You need steady state to judge whether a dose is adequate.
Second, dose escalation resets the clock. When you move from 2.5 mg to 5 mg, you are building toward a new, higher steady state. It takes another four weeks to fully reach it. The dosage chart reflects this with its recommended four-week intervals between increases.
Third, abrupt discontinuation from steady state means the drug clears more slowly than you might expect. Your starting point is that elevated 1.6x reservoir, not a single-dose level. Total clearance from steady state takes closer to 30 to 35 days rather than the 25 days calculated from a single dose.
Understanding steady state also helps explain why microdosing protocols work differently than standard escalation. Lower doses reach lower steady states, which may be sufficient for some goals while inadequate for others. The microdose schedule relies on the same accumulation principles but targets a different therapeutic window.
What happens when you stop taking tirzepatide
This section matters more than any other in this guide. Because eventually, most people face this question. What happens when you stop?
The clinical data is sobering. And it is important to understand it clearly.
The SURMOUNT-4 trial specifically studied what happens when tirzepatide treatment stops after significant weight loss. The trial design was elegant. Participants took tirzepatide for 36 weeks during an open-label lead-in period, achieving substantial weight loss. Then they were randomized. Half continued tirzepatide. Half switched to placebo. Researchers tracked both groups for another 52 weeks.
The results were stark.
Participants who continued tirzepatide maintained and even extended their weight loss, ultimately losing an average of 25.3% of body weight by the end of the study. Those who stopped? They regained weight. Significantly. By week 88, 82.5% of participants who discontinued tirzepatide had regained at least 25% of their lost weight. They still remained below their original starting weight on average, having lost about 9.9% total, but the trajectory was clearly heading back toward baseline.
The weight regain did not happen overnight. It followed a predictable pattern tied directly to tirzepatide clearance from the body.
Weeks 1-2 after stopping: Most people report increased hunger within one to two weeks. The appetite-suppressing effects do not vanish instantly because the drug is still clearing. But the reduction in circulating tirzepatide allows hunger signals to strengthen. Meals that felt satisfying on treatment start feeling insufficient.
Weeks 2-4: Appetite approaches pre-treatment levels for most people. Gastric emptying speeds back up. The sensation of early fullness that made smaller portions easy begins to fade. This is when the discipline challenge intensifies, because the pharmacological support is disappearing while the behavioral habits may not be fully cemented.
Months 2-6: Weight regain accelerates for most people who do not implement strong lifestyle interventions. The metabolic adaptations that tirzepatide supported, improved insulin sensitivity, reduced lipogenesis, enhanced satiety signaling, gradually revert toward pre-treatment baselines.
Months 6-12: The SURMOUNT-4 data shows the most significant regain occurring during this period. Cardiometabolic markers, including blood pressure, cholesterol, and glycemic parameters, worsen in proportion to weight regain.
There is an important nuance, however. Participants who managed to keep their weight regain below 25% of lost weight showed a different pattern. Their waist circumference, triglycerides, non-HDL cholesterol, and fasting insulin did not deteriorate significantly. This suggests a threshold effect. Maintaining most of your weight loss preserves the metabolic benefits, even without the drug.
What does this mean practically? Stopping tirzepatide is not an automatic return to square one. But it does require a plan. Diet planning, nutrition strategies, exercise habits, and potentially transitioning to a lower maintenance dose are all strategies that researchers and clinicians discuss. Understanding GLP-1 withdrawal patterns from related medications like semaglutide provides additional context for what to expect.
For those considering switching rather than stopping entirely, comparing options like switching from tirzepatide to semaglutide or using conversion charts to move between medications helps maintain continuity of care during transitions.
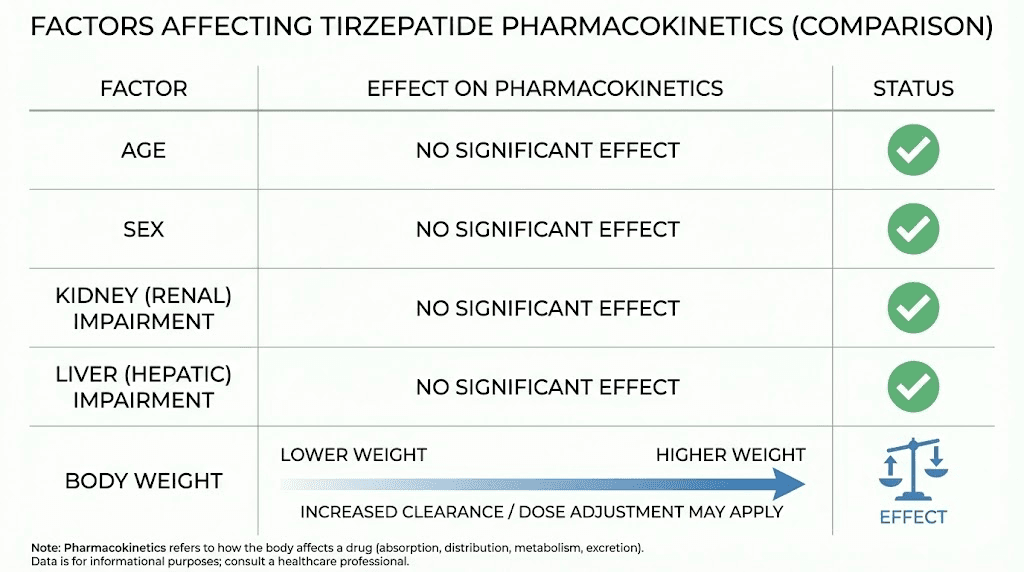
Factors that affect how long tirzepatide lasts in your body
One of the most reassuring findings from pharmacokinetic research is how consistent tirzepatide behaves across different populations. Many factors that dramatically alter other medications have minimal impact on tirzepatide duration.
Let me walk through each factor individually.
Body weight: This is the one factor that does meaningfully affect tirzepatide exposure. Population pharmacokinetic modeling shows that exposure changes approximately 1.1% per kilogram of body weight difference from the 70 kg reference. A person weighing 90 kg would have about 22% lower exposure than someone at 70 kg on the same dose. At 120 kg, exposure drops by roughly 33%. This is one reason dose escalation exists. Larger individuals may need higher doses to achieve equivalent therapeutic effects. The peptide calculator can help estimate weight-adjusted dosing.
Fat mass specifically contributes about 48% to the volume of distribution calculations. This means body composition, not just total weight, influences how tirzepatide distributes and persists. Two people at the same weight but different body fat percentages may experience slightly different pharmacokinetic profiles.
Kidney function: No clinically significant effect. Studies specifically evaluating tirzepatide in people with various degrees of renal impairment found similar drug exposure across all groups, including those with severe kidney impairment. No dose adjustment is needed based on kidney function. This is a significant advantage for a medication often used in populations where kidney disease is common, such as those with type 2 diabetes.
Liver function: No clinically significant effect for mild to moderate hepatic impairment. Tirzepatide is not metabolized through the cytochrome P450 (CYP) enzyme system, which is the primary drug metabolism pathway in the liver. Instead, it undergoes proteolytic cleavage in the blood, with the resulting amino acids recycled through normal protein metabolism. Data on severe hepatic impairment remains limited.
Age: No clinically relevant effect. Tirzepatide pharmacokinetics remain consistent between younger and older adults. This is important because BMI thresholds for GLP-1 treatment do not vary by age, and neither does the drug behavior.
Sex: No clinically relevant differences between males and females. The before and after results for men and weight loss results overall vary by individual factors, not by sex-based pharmacokinetic differences.
Race and ethnicity: No clinically relevant effect on pharmacokinetics.
Anti-tirzepatide antibodies: Some people develop antibodies against tirzepatide during treatment. The pharmacokinetic analyses found no statistically significant effect of these antibodies on drug levels or clearance. However, this does not mean antibodies never cause issues. In rare cases, injection site reactions and reaction management may relate to immune responses.
The bottom line: tirzepatide duration is remarkably predictable across populations. The 5-day half-life and 25-30 day clearance timeline apply to almost everyone, with body weight being the primary variable that shifts exposure levels. This consistency is one reason why standardized dosing guides work reliably across diverse patient populations.
Tirzepatide duration at each dose level
A common misconception is that higher doses of tirzepatide last longer in your system. They do not. Not exactly.
The half-life remains approximately 5 days regardless of whether you inject 2.5 mg or 15 mg. What changes is the peak concentration and the absolute amount of drug present at any given time. A 15 mg dose reaches a higher peak and maintains higher levels throughout the week compared to a 2.5 mg dose, but both decline at the same proportional rate.
Tirzepatide exposure increases proportionally across the entire dose range from 0.25 mg to 15 mg. Double the dose, double the exposure. Triple the dose, triple the exposure. This linear dose-proportionality simplifies dose adjustments and makes pharmacokinetic predictions straightforward.
The standard dose escalation schedule reflects this predictability:
Dose level | Duration at this level | Purpose | Typical effects |
|---|---|---|---|
2.5 mg | 4 weeks minimum | Initiation and tolerability | Mild appetite reduction, GI adjustment |
5 mg | 4 weeks minimum | First therapeutic dose | Noticeable appetite suppression, early weight loss |
7.5 mg | 4 weeks minimum | Intermediate escalation | Stronger effects, continued weight loss |
10 mg | 4 weeks minimum | Standard therapeutic dose | Significant appetite control, steady weight loss |
12.5 mg | 4 weeks minimum | Higher therapeutic dose | Strong effects for those needing more |
15 mg | Maintenance | Maximum dose | Maximum therapeutic effect |
At each dose, four weeks allows the drug to reach steady state at that level before judging efficacy. Some people achieve their goals at 5 mg. Others need 15 mg. The pharmacokinetics are the same. The therapeutic threshold differs.
For those using compounded formulations, the compound dosage chart and dosage in units chart translate milligram doses into practical syringe measurements. Accurate dosing depends on proper reconstitution and understanding your specific vial concentration.
A related question is whether dose timing affects duration. It does not change the half-life, but many researchers and clinicians suggest finding a consistent day and time for injections. Choosing the best time for your GLP-1 shot can optimize how the weekly effects pattern aligns with your lifestyle and eating schedule.
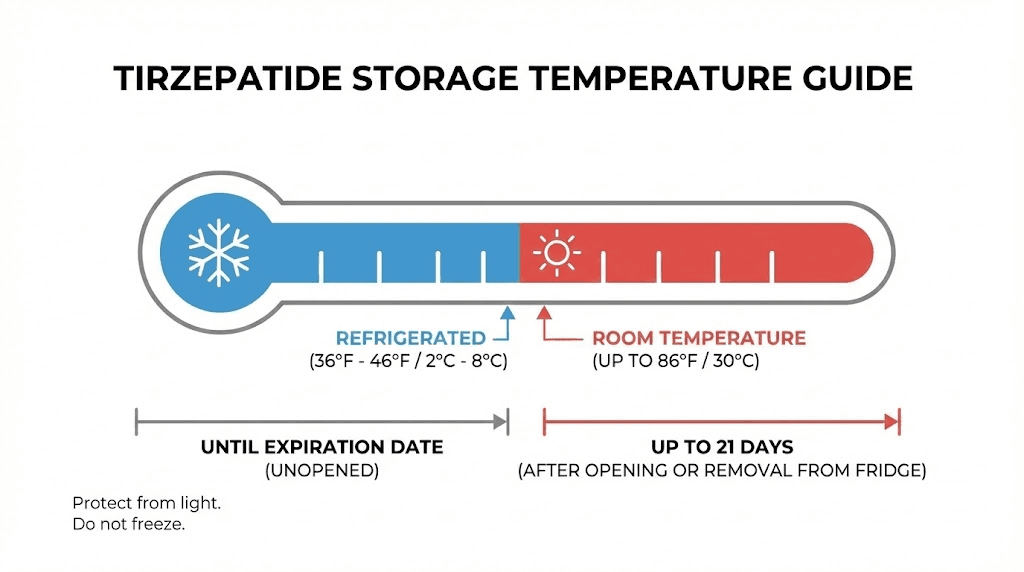
How long compounded tirzepatide lasts in storage
Many people searching "how long does tirzepatide last" are actually asking about shelf life and storage. While this guide focuses on how long the drug lasts in your body, the storage question deserves a clear answer too.
The complete details live in our dedicated guides on tirzepatide shelf life and how long tirzepatide lasts in the fridge, but here is the essential summary.
Brand-name pen devices (Mounjaro/Zepbound): Unopened pens can remain at room temperature up to 86 degrees Fahrenheit (30 degrees Celsius) for up to 21 days. Once used, follow the manufacturer guidance for that specific pen device. Most recommend using within 21 days.
Compounded lyophilized (powder) tirzepatide: Before reconstitution, properly stored lyophilized tirzepatide can last months in the refrigerator. The powder form is significantly more stable than liquid. Once reconstituted with bacteriostatic water, the clock starts. Most guidance suggests using reconstituted tirzepatide within 28 to 30 days when stored at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius).
Compounded liquid tirzepatide: Pre-mixed liquid formulations from compounding pharmacies typically require refrigeration and have shelf lives ranging from 28 to 90 days depending on the formulation and pharmacy. Always check your specific pharmacy instructions.
Key storage rules to protect your tirzepatide investment:
Never freeze tirzepatide. Freezing destroys the peptide molecular structure permanently.
Avoid refrigerator door storage where temperature fluctuates from opening and closing.
Inspect for clarity before each use. Discard if cloudy, discolored, or containing particles.
Once removed from refrigeration, track how long it has been out of the fridge.
Protect from light. UV exposure degrades peptides.
For related storage questions, does tirzepatide expire, does it need refrigeration, and what happens if it gets warm all provide deeper answers. And if you have used expired product, our guide on what happens if you use expired tirzepatide addresses that concern directly.
Traveling with GLP-1 medications requires additional planning. While our travel guide for semaglutide covers the logistics in detail, the same principles apply to tirzepatide. Keep it cool, keep it protected, and bring enough for your trip plus a buffer.
How tirzepatide duration compares to other GLP-1 medications
Tirzepatide is not the only GLP-1 receptor agonist available, and understanding how its duration compares to alternatives helps inform treatment decisions and potential transitions between medications.
Medication | Half-life | Dosing frequency | Time to steady state | Full clearance | Receptor targets |
|---|---|---|---|---|---|
Tirzepatide | ~5 days | Once weekly | ~4 weeks | 25-30 days | GIP + GLP-1 (dual) |
Semaglutide | ~7 days | Once weekly | 4-5 weeks | 35+ days | GLP-1 only |
Liraglutide | ~13 hours | Once daily | 3-5 days | 2-3 days | GLP-1 only |
Dulaglutide | ~5 days | Once weekly | 2-4 weeks | 25 days | GLP-1 only |
Retatrutide | ~6 days | Once weekly | ~4 weeks | 30 days | GIP + GLP-1 + Glucagon (triple) |
Several patterns emerge from this comparison.
Semaglutide actually has a longer half-life than tirzepatide, approximately 7 days versus 5 days. This means semaglutide takes longer to clear completely after discontinuation. For those comparing the two, our semaglutide vs tirzepatide comparison covers efficacy, side effects, and practical differences in detail. The side effect comparison is particularly useful when choosing between them.
Liraglutide sits at the opposite end of the spectrum. Its 13-hour half-life means daily injections are necessary and the drug clears within two to three days of stopping. This rapid clearance can be an advantage if you need to stop quickly for surgery or other medical reasons, but it demands more commitment to daily injection schedules.
Retatrutide represents the next generation, targeting three receptors instead of two. Its pharmacokinetic profile is similar to tirzepatide with a slightly longer half-life. For those considering a transition, understanding how long retatrutide takes to kick in after tirzepatide helps plan the switch. Comparisons like retatrutide vs semaglutide and survodutide vs tirzepatide provide additional decision-making context.
The dual agonist mechanism of tirzepatide, targeting both GIP and GLP-1 receptors simultaneously, distinguishes it from pure GLP-1 agonists like semaglutide and liraglutide. This dual action does not change the half-life, but it does change the clinical effects. The metabolic impact of dual receptor activation appears to produce greater weight loss in clinical trials compared to GLP-1-only medications at comparable doses.
When switching between medications, pharmacokinetic overlap matters. Going from semaglutide to tirzepatide or vice versa requires understanding that both drugs will be present during the transition period. The conversion chart helps map equivalent doses, but the pharmacokinetic overlap means you may temporarily have elevated combined drug levels during the first two to three weeks of a switch.
Other emerging GLP-1 options include orforglipron, an oral small molecule agonist, and CagriSema, which combines cagrilintide with semaglutide. Each has its own pharmacokinetic profile, and the landscape of available options continues to expand. SeekPeptides tracks these developments and provides updated comparisons as new data emerges.
Practical tips for managing tirzepatide duration and getting better results
Understanding pharmacokinetics is one thing. Applying it to your daily life is another. Here are evidence-based strategies for optimizing how tirzepatide works for you throughout its duration in your system.
Maintain consistent weekly timing. Pick a day. Pick a time. Stick with it. Consistency keeps your blood levels predictable and your body response stable. Most people choose a day when they can manage potential fatigue or body aches without it affecting work or social obligations. Injecting on Friday evening, for example, lets any side effects peak over the weekend.
Plan nutrition around your cycle. Since appetite suppression is strongest in days two through five, that is when structuring what you eat around protein and nutrient density matters most. Days six and seven, when effects taper slightly, benefit from having prepared meals and meal plans in place so that increased hunger does not lead to poor food choices.
Respect the dose escalation timeline. Four weeks at each dose. Minimum. This is not arbitrary. It is the time required to reach steady state. Judging a dose before steady state is like reviewing a movie after watching the first ten minutes. You are not seeing the full picture. If a dose feels insufficient at week two, wait. Week four may surprise you.
Track side effects relative to your injection day. Headaches, anxiety, insomnia, and muscle pain often follow patterns tied to the pharmacokinetic curve. Knowing when side effects peak and fade helps you manage them proactively rather than reactively. Many side effects are worst in the first one to two days after injection and diminish by day four or five.
Stay hydrated, especially early in the cycle. Tirzepatide slows gastric emptying, which can affect how you process fluids and nutrients. Constipation is one of the most common side effects, and it frequently correlates with dehydration. Proactive hydration during the peak drug effect window helps prevent this.
Consider alcohol timing. If you choose to drink, understanding alcohol interactions with tirzepatide helps you make informed decisions. Alcohol tolerance often decreases on GLP-1 medications, and the slower gastric emptying can change how quickly alcohol affects you.
Monitor beyond the scale. Tirzepatide duration is not just about weight. Track energy levels, sleep quality, mood, and how your menstrual cycle responds if applicable. The energy effects and metabolic changes often tell a richer story than weight alone.
For researchers managing their own protocols, SeekPeptides provides comprehensive protocol guides, dosage calculators, and community support that helps navigate these decisions with confidence. The pharmacokinetic knowledge in this guide gives you the foundation. Applying it consistently gives you the results.
Why understanding tirzepatide duration matters for long-term success
The difference between people who succeed long-term on tirzepatide and those who struggle often comes down to understanding what the drug is actually doing inside their body, and how long it keeps doing it.
Short-term thinking leads to common mistakes. Skipping a dose because you "feel fine" and assuming the drug is still working at full strength. Escalating too quickly because week two feels underwhelming. Stopping abruptly without a transition plan because you hit your goal weight. Each of these mistakes stems from misunderstanding tirzepatide duration.
Long-term thinking, grounded in pharmacokinetic reality, looks different.
It means understanding that the first four weeks at any dose are a building phase, not a judging phase. It means recognizing that the day-before-injection hunger dip is normal pharmacokinetics, not treatment failure. It means planning for discontinuation or dose reduction with the knowledge that appetite will return within one to two weeks and that maintaining lifestyle changes during that window is critical.
It also means comparing medications wisely. If you are weighing mazdutide vs tirzepatide, phentermine vs semaglutide, or combining phentermine with tirzepatide, pharmacokinetic duration should factor into your decision. How these medications overlap, interact, and persist in your system affects both safety and efficacy.
How long you stay on GLP-1 medications is itself a critical question. The clinical evidence increasingly suggests that obesity is a chronic condition requiring ongoing management, much like high blood pressure or diabetes. Whether that management involves continuous medication, intermittent treatment, or a transition to lower doses with robust lifestyle habits depends on individual factors that pharmacokinetic understanding helps clarify.
For those exploring the broader peptide landscape, peptides for weight loss beyond GLP-1 agonists offer complementary approaches. Understanding how peptides work at a foundational level makes every subsequent decision more informed. And resources like the peptide safety guide ensure that whatever protocol you pursue, you approach it with appropriate caution.
For researchers serious about optimizing their tirzepatide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Frequently asked questions
How long does a single tirzepatide injection last?
A single injection maintains detectable blood levels for approximately 25 to 30 days. However, the therapeutic effects, particularly appetite suppression, are strongest during the first 5 to 7 days. This is why weekly dosing is the standard protocol, ensuring consistent therapeutic coverage.
Does tirzepatide build up in your system over time?
Yes. With weekly dosing, tirzepatide accumulates to approximately 1.6 to 1.7 times the single-dose level over about four weeks. This accumulation reaches a plateau called steady state, where the amount entering equals the amount being cleared. This is why effects often strengthen during the first month of treatment, even without increasing the dose.
How long does tirzepatide appetite suppression last after stopping?
Most people report noticeable return of hunger within one to two weeks of their last injection. Appetite typically approaches pre-treatment levels within three to four weeks. However, the timeline varies. Some people retain partial appetite modification for up to six weeks due to residual drug levels and potential lasting receptor changes. Our appetite suppression timeline provides more detail.
Is tirzepatide half-life the same at all doses?
Yes. The elimination half-life of approximately 5 days remains consistent from the 2.5 mg starting dose through the 15 mg maximum dose. Higher doses produce higher peak levels and greater overall exposure, but the rate of clearance, expressed as half-life, does not change. The dose chart shows how escalation changes the amount of drug in your system, not how fast it clears.
Does body weight affect how long tirzepatide lasts?
Body weight affects the peak concentration and overall exposure, but not the half-life itself. A heavier person distributes the same dose across more tissue, resulting in lower peak levels. This is why the dosage calculator factors in body weight. The 5-day half-life applies regardless of weight.
How long should I wait after stopping tirzepatide before starting another medication?
Most clinicians suggest waiting at least one to two weeks after the last tirzepatide dose before starting a different GLP-1 agonist to minimize overlap and the risk of compounded side effects. For transitions to semaglutide or retatrutide, specific transition protocols exist that account for the pharmacokinetic overlap between medications.
Can I take tirzepatide every two weeks instead of weekly?
While some researchers experiment with extended dosing intervals, the pharmacokinetics suggest that every-two-week dosing would produce significant troughs where drug levels fall below therapeutic thresholds. By day 14, only about 25% of the original dose remains. Standard protocols maintain weekly dosing for consistent effects, though microdosing schedules offer alternative approaches for those seeking lower overall exposure.
How long does compounded tirzepatide last in the fridge?
Reconstituted compounded tirzepatide typically lasts 28 to 30 days when refrigerated at 36 to 46 degrees Fahrenheit. Lyophilized powder before reconstitution lasts significantly longer. Our complete fridge storage guide and shelf life guide cover every storage scenario in detail.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your steady state stay consistent, your appetite stay managed, and your protocols stay informed.