Feb 25, 2026

What if the number on your syringe is telling you the wrong story? You draw 75 units. You feel confident. But that number, those 75 little lines on the barrel, they do not tell you how many milligrams of tirzepatide you are actually injecting. Not even close. The answer depends entirely on one critical variable that changes everything, and getting it wrong means you are either underdosing (wasting time and money) or overdosing (risking unnecessary side effects). Thousands of people search for this exact conversion every month because the relationship between units and milligrams is genuinely confusing, especially with compounded tirzepatide where concentrations vary wildly from one pharmacy to the next.
The confusion is understandable. Insulin syringes measure volume, not drug content. A unit is simply 0.01 mL of liquid. That is all it is. So 75 units equals exactly 0.75 mL of whatever liquid is inside your vial. But 0.75 mL of a 10 mg/mL solution contains a very different amount of tirzepatide than 0.75 mL of a 20 mg/mL solution. The concentration printed on your vial label is the missing piece of the puzzle, and without it, the number 75 on your syringe is meaningless.
This guide breaks down every possible answer to the question. You will find complete conversion charts for every common concentration, the exact formula you can use for any scenario, practical tips for reading your vial label correctly, and the most common mistakes that lead to dosing errors. Whether you are using compounded tirzepatide from a pharmacy or working with reconstituted research peptides, this article covers it all. SeekPeptides has built conversion resources used by thousands of researchers, and this guide reflects that same commitment to accuracy and clarity.
The quick answer: 75 units of tirzepatide in milligrams
Here is the direct answer. 75 units of tirzepatide equals a different number of milligrams depending on your vial concentration. There is no single universal answer.
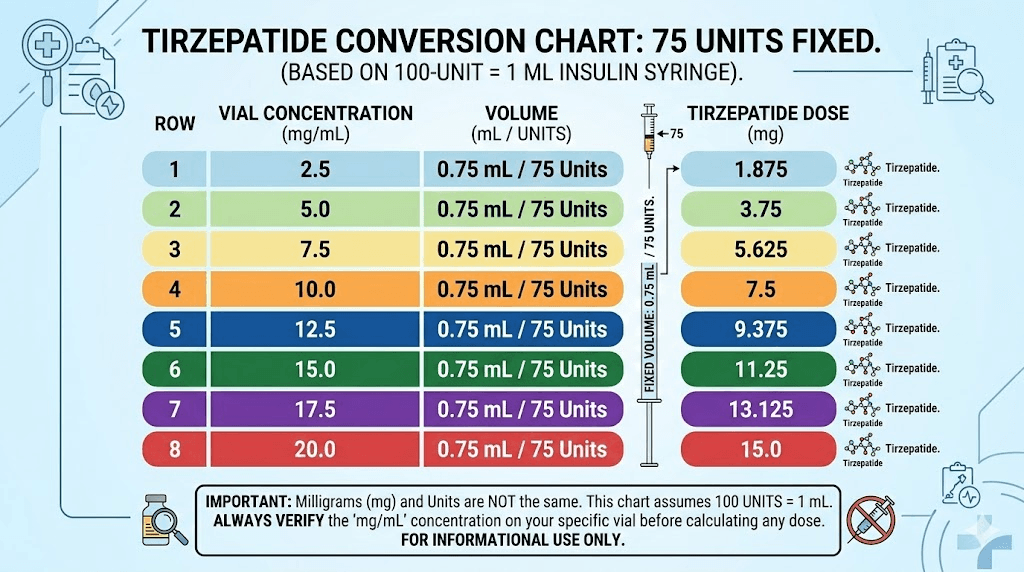
At 5 mg/mL, 75 units equals 3.75 mg. At 10 mg/mL, 75 units equals 7.5 mg. At 15 mg/mL, 75 units equals 11.25 mg. At 20 mg/mL, 75 units equals 15 mg. At 30 mg/mL, 75 units equals 22.5 mg. At 40 mg/mL, 75 units equals 30 mg. At 50 mg/mL, 75 units equals 37.5 mg. At 60 mg/mL, 75 units equals 45 mg.
The most common scenario is 10 mg/mL concentration, where 75 units delivers exactly 7.5 mg. This happens to be a standard tirzepatide dosing tier used in clinical protocols, which is why 75 units is such a commonly searched number.
But you cannot assume your vial is 10 mg/mL. You must check.
Understanding units, milligrams, and milliliters
Before diving into the conversion math, you need to understand what these three measurements actually represent. They measure completely different things, and confusing them is the root cause of nearly every dosing error with tirzepatide dosing in units.
What units measure
Units on an insulin syringe measure volume. Nothing more. A standard U-100 insulin syringe divides 1 mL of liquid into 100 equal markings. Each marking represents 1 unit, which equals 0.01 mL. So when you draw to the 75 unit line, you are pulling exactly 0.75 mL of liquid into the syringe. The syringe does not know or care what is dissolved in that liquid. It could be tirzepatide, semaglutide, saline, or anything else. The syringe simply measures how much liquid you have drawn.
This is where the confusion starts. People assume units have some inherent relationship to drug potency. They do not. Units are a volume measurement, period.
What milligrams measure
Milligrams measure the actual amount of active drug. When your provider prescribes 7.5 mg of tirzepatide, they are specifying how much of the actual medication your body should receive. This is the number that determines your therapeutic effect, your side effect risk, and whether your weight loss timeline stays on track.
Milligrams do not change based on concentration. 7.5 mg of tirzepatide is 7.5 mg of tirzepatide regardless of whether it is dissolved in 0.75 mL or 0.375 mL or 0.15 mL of liquid. The drug amount stays constant. Only the volume changes.
What milliliters measure
Milliliters measure liquid volume, just like units, but in a different scale. The relationship is simple and fixed. 1 mL equals 100 units on a U-100 insulin syringe. Always. So 0.75 mL equals 75 units. And 0.5 mL equals 50 units. This conversion never changes regardless of what medication you are working with.
How concentration ties them together
Concentration is the bridge between volume and drug amount. It tells you how many milligrams of tirzepatide are dissolved in each milliliter of liquid. A vial labeled 10 mg/mL contains 10 milligrams of tirzepatide in every 1 mL of solution. A vial labeled 20 mg/mL contains twice as much drug in the same volume. This is why the same 75 units can deliver vastly different doses depending on which vial you are drawing from.
Think of it like coffee. A teaspoon of regular coffee and a teaspoon of espresso are the same volume. But the espresso contains far more caffeine because it is more concentrated. The measuring spoon does not change. The concentration does. Your insulin syringe works the same way. It measures the liquid, not the drug inside it.
Understanding this distinction is fundamental to safe tirzepatide syringe dosage calculations. Every dosage calculator and conversion chart you will ever use relies on this same relationship between units, milligrams, and concentration.
The conversion formula explained step by step
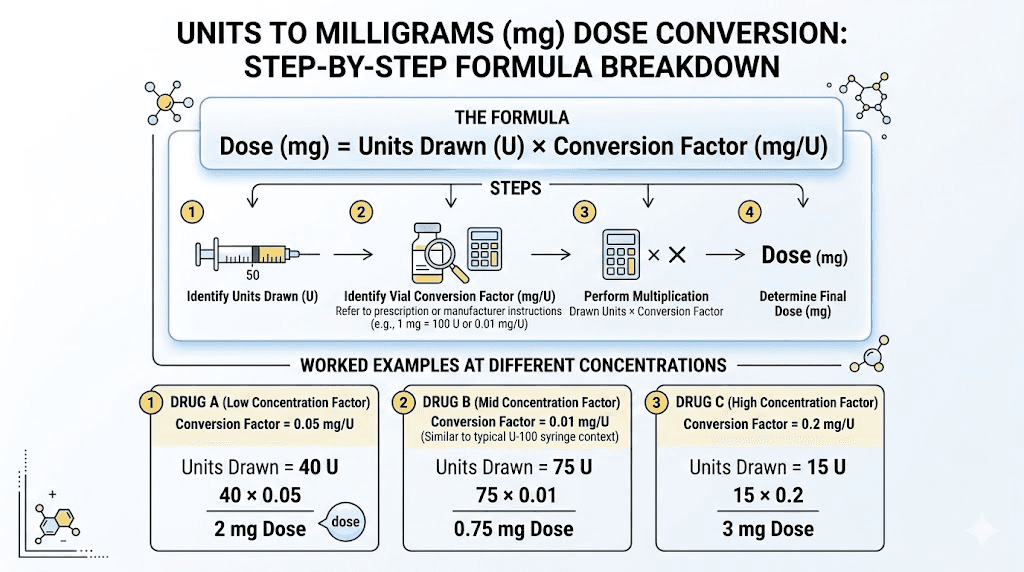
The formula is straightforward once you understand what each variable represents. You only need two numbers: the units you are drawing and the concentration on your vial label.
mg = (units / 100) x concentration
For 75 units, the math becomes: mg = (75 / 100) x concentration. That simplifies to mg = 0.75 x concentration.
That is the entire formula. Multiply 0.75 by whatever concentration is printed on your vial, and you have your answer in milligrams.
Worked example at 10 mg/mL
Your vial says 10 mg/mL. You draw 75 units.
mg = 0.75 x 10 = 7.5 mg
You are injecting 7.5 mg of tirzepatide. This aligns with a standard tirzepatide dose tier used in clinical research protocols.
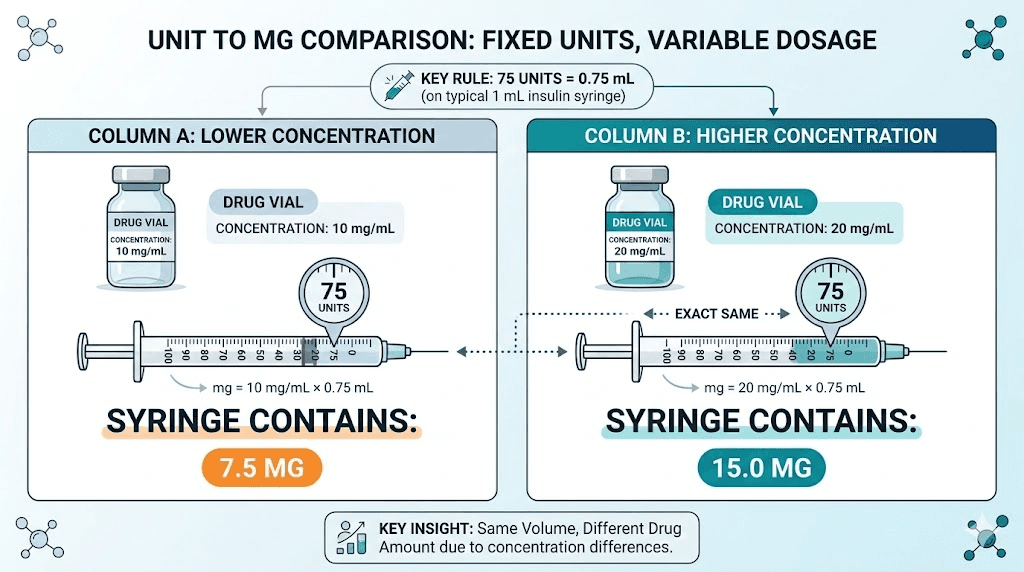
Worked example at 20 mg/mL
Your vial says 20 mg/mL. You draw the same 75 units.
mg = 0.75 x 20 = 15 mg
Now you are injecting 15 mg, which is the highest FDA-approved dose tier. Same syringe reading. Double the medication. This is exactly why checking your concentration matters so much, and why dosing charts organized by concentration are essential references.
Worked example at 5 mg/mL
Your vial says 5 mg/mL. Same 75 units.
mg = 0.75 x 5 = 3.75 mg
At this concentration, 75 units delivers only 3.75 mg. That falls between the 2.5 mg starting dose and the 5 mg second tier. Some providers use this as a custom intermediate step for people who are sensitive to side effects during early titration.
The reverse formula
Sometimes you need to go the other direction. You know the milligrams you want and need to figure out how many units to draw. The reverse formula is equally simple.
units = (desired mg / concentration) x 100
If you want 7.5 mg from a 10 mg/mL vial: units = (7.5 / 10) x 100 = 75 units. If you want 7.5 mg from a 20 mg/mL vial: units = (7.5 / 20) x 100 = 37.5 units. Same dose, different volume, because the concentration changed.
For quick calculations, the SeekPeptides peptide calculator handles both directions instantly. Enter your concentration and desired dose, and it returns the exact syringe units.
Complete 75-unit conversion chart for every concentration
This is the reference table you will want to bookmark. It covers every concentration commonly found in compounded and reconstituted tirzepatide vials, showing exactly how many milligrams 75 units delivers at each level.
Concentration (mg/mL) | 75 units equals | Standard dose tier? | Common source |
|---|---|---|---|
2 mg/mL | 1.5 mg | Below starting dose | Highly diluted reconstitution |
3 mg/mL | 2.25 mg | Near starting dose | Custom reconstitution |
5 mg/mL | 3.75 mg | Between tiers 1 and 2 | Some compounding pharmacies |
8 mg/mL | 6 mg | Between tiers 2 and 3 | Select compounding pharmacies |
10 mg/mL | 7.5 mg | Yes, tier 3 (7.5 mg) | Most common compounded concentration |
12 mg/mL | 9 mg | Between tiers 3 and 4 | Some compounding pharmacies |
15 mg/mL | 11.25 mg | Between tiers 4 and 5 | Higher concentration compounded |
17 mg/mL | 12.75 mg | Near tier 4 (12.5 mg) | Empower Pharmacy formulations |
20 mg/mL | 15 mg | Yes, tier 5 (15 mg) | High concentration compounded |
25 mg/mL | 18.75 mg | Above standard tiers | Research concentrations |
30 mg/mL | 22.5 mg | Above standard tiers | Research concentrations |
40 mg/mL | 30 mg | Above standard tiers | Research concentrations |
50 mg/mL | 37.5 mg | Above standard tiers | Research concentrations |
60 mg/mL | 45 mg | Above standard tiers | Research concentrations |
The highlighted rows at 10 mg/mL and 20 mg/mL are the most commonly encountered scenarios. At 10 mg/mL, 75 units delivers exactly 7.5 mg, which corresponds to the third dose tier in standard tirzepatide titration protocols. At 20 mg/mL, 75 units delivers 15 mg, the highest standard dose tier.
If your concentration does not appear in this table, use the formula from the previous section: multiply 0.75 by your specific concentration. The math works for any number.
Common tirzepatide concentrations and what 75 units means for each
Not all concentrations are equally common. Knowing which ones you are most likely to encounter helps you quickly identify your scenario and verify your calculations.
5 mg/mL concentration
At 5 mg/mL, drawing 75 units gives you 3.75 mg of tirzepatide. This concentration appears in some compounded starting dose formulations designed to make the initial low doses easier to measure accurately. With 5 mg/mL, even small unit changes translate to meaningful dose adjustments.
Drawing 75 units from this vial puts you between the 2.5 mg starting dose and the 5 mg second tier. Some providers intentionally prescribe 3.75 mg as a half-step for patients experiencing headaches or gastrointestinal side effects when jumping directly to 5 mg. The lower concentration makes this kind of fine-tuning practical.
10 mg/mL concentration
This is the most widely used concentration for compounded tirzepatide. At 10 mg/mL, 75 units delivers exactly 7.5 mg. Clean number. No rounding needed.
The 7.5 mg dose is the third tier in the standard tirzepatide titration schedule. Patients typically reach this level after spending at least four weeks at 5 mg (50 units at this concentration). At 7.5 mg, most people report noticeable appetite suppression and measurable weight loss results.
If you are on a 10 mg/mL vial and your provider tells you to take 7.5 mg, you draw to the 75 unit mark. Simple.
15 mg/mL concentration
At 15 mg/mL, 75 units gives you 11.25 mg. This falls between the 10 mg and 12.5 mg standard dose tiers. Higher concentration vials reduce injection volume, which some people prefer because smaller volumes tend to cause less injection site irritation.
If you need a standard dose from a 15 mg/mL vial, the math requires non-round unit numbers. For example, 7.5 mg would be 50 units, and 10 mg would be approximately 66.7 units. Having a dosage chart organized by concentration eliminates the mental math.
17 mg/mL concentration
Several pharmacies, including Empower Pharmacy, have used 17 mg/mL formulations. At this concentration, 75 units delivers 12.75 mg, which is very close to the 12.5 mg fourth dose tier. The 0.25 mg difference is clinically insignificant, but precision-minded researchers should note it. Empower Pharmacy tirzepatide formulations often include additional compounds like niacinamide, so always verify the exact formulation and concentration on your specific vial.
20 mg/mL concentration
At 20 mg/mL, 75 units equals 15 mg. This is the maximum dose tier in standard tirzepatide protocols. Higher concentration vials mean smaller injection volumes, which reduces discomfort and allows more doses per vial.
People on maintenance doses at 15 mg appreciate the convenience. Instead of injecting a full 1.5 mL (which would be needed at 10 mg/mL), they inject just 0.75 mL. Half the volume, same therapeutic dose. If you are at this level and wondering about plateau management or split dosing strategies, those are separate but related topics worth exploring.
30 mg/mL and higher concentrations
Concentrations above 20 mg/mL are less common in standard pharmacy compounding but appear in research settings and some specialty formulations. At 30 mg/mL, 75 units delivers 22.5 mg. At 40 mg/mL, it delivers 30 mg. These amounts exceed standard clinical dosing tiers and are typically only relevant for specific research protocols.
If you encounter a concentration this high, triple-check your calculations. The margin for error shrinks as concentration increases because small changes in unit readings translate to large changes in milligrams. Drawing just 10 units too many from a 40 mg/mL vial means an extra 4 mg of medication, which is a significant overshoot.
How to read your tirzepatide vial label
Your vial label contains every piece of information you need to convert units to milligrams. But labels can be confusing if you do not know where to look or what the numbers mean.
Finding the concentration
The concentration is usually printed as a ratio: mg/mL. Look for text like "10 mg/mL" or "10mg per mL" or sometimes "10 mg per 1 mL." This is the number that goes into your formula. Some labels display it prominently. Others bury it in small print alongside other details about the formulation.
Compounded tirzepatide vials from different pharmacies may format this information differently. Southend Pharmacy, ProRx, Orderly Meds, and Priority Meds each have their own label layouts. Regardless of format, the concentration expressed in mg/mL is always there somewhere.
Total content vs. concentration
Do not confuse total vial content with concentration. A label might say "30 mg" prominently and "10 mg/mL" in smaller text. The 30 mg is the total tirzepatide in the entire vial (3 mL at 10 mg/mL). The 10 mg/mL is the concentration, the number you need for your conversion. Using 30 instead of 10 in your formula would give you a wildly incorrect answer.
Here is a quick way to verify. If the label says 30 mg total in a 3 mL vial, then 30 divided by 3 equals 10 mg/mL. If it says 60 mg total in a 3 mL vial, then 60 divided by 3 equals 20 mg/mL. The math should always check out. If it does not, contact your pharmacy before drawing any medication.
Multi-component formulations
Some compounded tirzepatide with B12 or tirzepatide with glycine and B12 vials list multiple ingredients. The tirzepatide concentration is the one that matters for your unit-to-mg conversion. Additional ingredients like glycine, B6, or methylcobalamin are listed separately and do not affect the tirzepatide calculation.
Reconstituted vials
If you reconstituted the tirzepatide yourself, the concentration depends on how much bacteriostatic water you added. A 10 mg vial reconstituted with 1 mL of bac water gives you 10 mg/mL. The same vial reconstituted with 2 mL gives you 5 mg/mL. At 10 mg/mL, 75 units is 7.5 mg. At 5 mg/mL, 75 units is only 3.75 mg. The volume of water you add during reconstitution directly determines your concentration and therefore your dose per unit.
This is why keeping a record of exactly how much bacteriostatic water you mixed is absolutely essential. Guessing or forgetting leads to dosing errors that compound with every injection.
Reading your insulin syringe correctly
Accurate syringe reading is just as important as accurate math. Even if your formula is perfect, misreading the syringe by a few units throws everything off.
U-100 syringe markings
Standard U-100 insulin syringes come in three common sizes. The 1 mL syringe holds 100 units and typically has markings every 2 units. The 0.5 mL syringe holds 50 units and usually has markings every 1 unit. The 0.3 mL syringe holds 30 units and has markings every 0.5 or 1 unit.
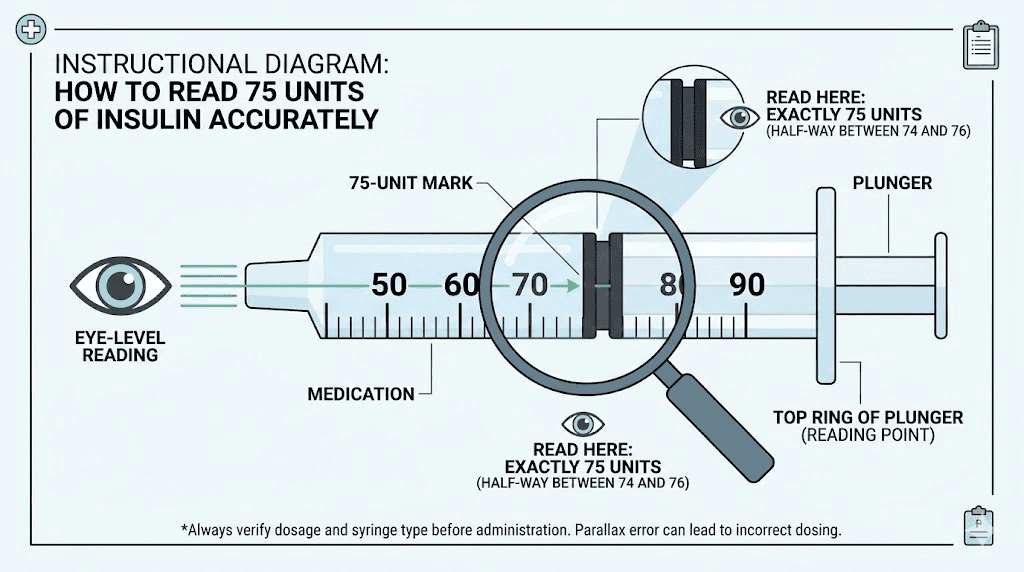
For 75 units, you need either a 1 mL (100 unit) syringe or you need to split the draw across two smaller syringes, which is not recommended due to potential volume loss. Use the 1 mL syringe. Count to 75 carefully. With markings every 2 units, the 75 unit line falls between the 74 and 76 markings, right on the midpoint line if your syringe has half-unit indicators.
Reading at eye level
Hold the syringe at eye level, not above or below. Looking up at the syringe makes the liquid line appear lower than it actually is. Looking down makes it appear higher. Both angles introduce parallax error that can shift your reading by 2 to 5 units. At a 10 mg/mL concentration, 5 units of error means 0.5 mg of medication, which is a meaningful difference during precise microdosing protocols.
The meniscus
Liquid in a syringe forms a slight curve at the top, called the meniscus. Read from the bottom of this curve, not the top. The bottom of the meniscus touching the 75 unit line is the correct reading. Reading from the top of the curve adds approximately 1 to 2 units of false volume.
Air bubbles matter
Air bubbles trapped in the syringe displace liquid and reduce your actual dose. A visible air bubble in a 75-unit draw might mean you only have 70 or 72 units of actual medication. Tap the syringe barrel with your finger to move bubbles to the top, then gently push the plunger to expel them before confirming your final volume at 75 units.
For a complete walkthrough on injection technique and syringe handling, those dedicated guides cover the physical process in detail.
Where 75 units falls in standard tirzepatide dosing tiers
Tirzepatide follows a structured titration schedule with specific dose tiers. Understanding where 75 units puts you on this schedule depends, again, on your concentration. But looking at the most common concentrations helps contextualize the dose.
The standard tirzepatide dose tiers
The FDA-approved titration schedule for tirzepatide moves through five dose levels. Tier 1 starts at 2.5 mg for the first four weeks. Tier 2 increases to 5 mg for weeks five through eight. Tier 3 moves to 7.5 mg. Tier 4 reaches 10 mg. And tier 5 goes to 12.5 mg or 15 mg for maintenance. Each tier lasts a minimum of four weeks before increasing.
At 10 mg/mL, 75 units (7.5 mg) lands you squarely on tier 3. This is a middle-ground dose where most people begin experiencing significant appetite suppression and weight loss. Studies show that tirzepatide begins working within the first few weeks, but the 7.5 mg dose is often where effects become pronounced and consistent.
75 units at different concentrations and their tier placement
At 5 mg/mL, 75 units delivers 3.75 mg, which sits between tier 1 and tier 2. This is a non-standard dose but useful for gradual titration.
At 10 mg/mL, 75 units delivers 7.5 mg. Tier 3. Standard dose.
At 15 mg/mL, 75 units delivers 11.25 mg. Between tier 4 and tier 5. Not a standard dose tier, but close to 10 mg.
At 20 mg/mL, 75 units delivers 15 mg. Tier 5 maximum dose. This is the ceiling for standard protocols, and some people stay at this dose for extended maintenance periods. If you are on 15 mg and wondering about how long results take or dealing with fatigue, those resources may help.
Custom and microdosing uses of 75 units
Not everyone follows the standard titration schedule. Microdosing protocols use lower concentrations to achieve sub-therapeutic doses for specific purposes like autoimmune modulation. At a 2 mg/mL concentration, 75 units delivers just 1.5 mg, well below the starting dose. At a 3 mg/mL concentration, 75 units gives 2.25 mg, close to but still below the standard 2.5 mg starting point.
Other people use 75 units as part of a split dosing approach, dividing their weekly dose into two injections. If a person is prescribed 15 mg weekly from a 10 mg/mL vial, they might inject 75 units (7.5 mg) twice per week instead of 150 units once. This approach can reduce side effects by maintaining more stable blood levels, though it should only be done under medical guidance.
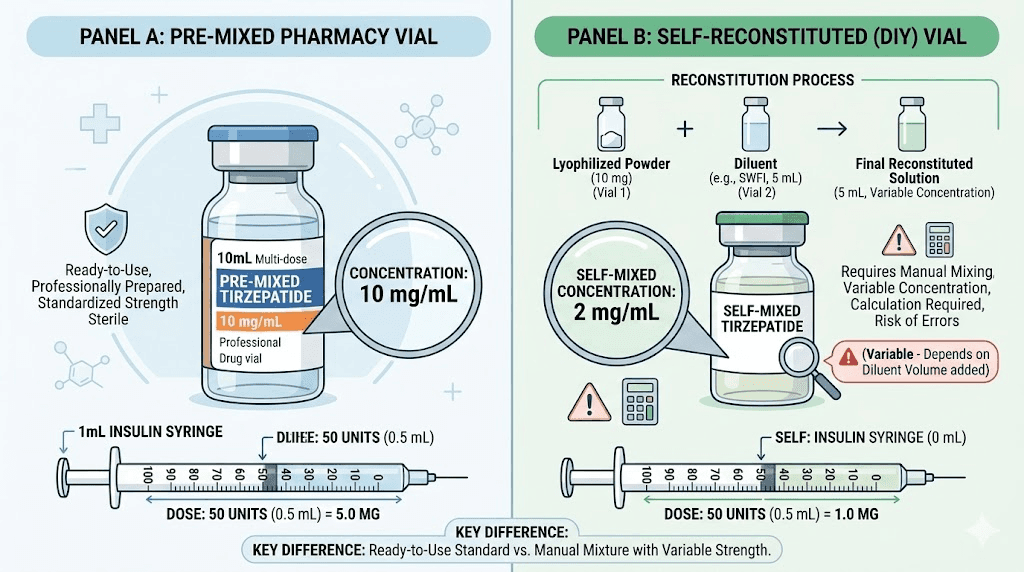
Reconstituted vs. pre-mixed: how it affects your 75-unit calculation
The source of your tirzepatide determines how the concentration was established, which affects how you should approach your calculations.
Pre-mixed compounded tirzepatide
When you receive a vial from a compounding pharmacy, the concentration is fixed. The pharmacist has already dissolved the tirzepatide at a specific ratio. Your label tells you the concentration, and it will not change throughout the life of the vial (assuming proper storage). The math is simple: read the label, apply the formula, draw your 75 units, done.
Pre-mixed vials from established pharmacies like Empower or Strive undergo quality testing to confirm the stated concentration. This adds a layer of confidence to your calculations that you might not get with self-reconstituted peptides.
Self-reconstituted tirzepatide
When you reconstitute lyophilized tirzepatide powder yourself, you control the concentration by deciding how much bacteriostatic water to add. This gives you flexibility but also introduces a point of potential error.
If you have a 10 mg vial and add 1 mL of bacteriostatic water, your concentration is 10 mg/mL. At this concentration, 75 units gives you 7.5 mg, using 75% of your vial in a single draw.
If you add 2 mL of bacteriostatic water to the same 10 mg vial, your concentration drops to 5 mg/mL. Now 75 units gives you only 3.75 mg, and you have enough liquid for more draws from the vial.
The common approach is to reconstitute with enough water so that your target dose corresponds to an easy-to-measure number of units. If your target dose is 7.5 mg and your vial contains 10 mg, adding 1 mL makes 7.5 mg equal 75 units. Adding 2 mL makes 7.5 mg equal 150 units, which exceeds a standard 1 mL insulin syringe. So 1 mL of water is the practical choice for a 10 mg vial targeting 7.5 mg doses.
Why this distinction matters for 75 units specifically
With pre-mixed vials, 75 units means one thing consistently throughout the vial. With reconstituted vials, the concentration can vary if you did not measure the water precisely, if some water evaporated, or if the powder did not fully dissolve. Small errors during reconstitution translate directly into dosing inaccuracies for every subsequent draw.
This is why reconstitution guides emphasize using precise syringes for measuring water, swirling (never shaking) to ensure full dissolution, and recording exactly how much water you added.
Common mistakes when converting 75 units to milligrams
Dosing errors with tirzepatide are more common than most people realize. Understanding the typical mistakes helps you avoid them.
Mistake 1: assuming a universal conversion
The most dangerous mistake is believing that 75 units always equals a specific number of milligrams regardless of concentration. This misconception likely comes from insulin, where U-100 insulin actually does have a fixed relationship: 75 units of U-100 insulin equals 75 international units of insulin activity. Tirzepatide does not work this way. There is no fixed unit-to-mg relationship because the concentration varies.
Someone who previously used insulin might draw 75 units of tirzepatide expecting a standard dose without ever checking the concentration. This person could receive anywhere from 3.75 mg to 45 mg depending on the vial. That range includes doses that are dangerously high. Always verify concentration first.
Mistake 2: confusing total vial content with concentration
As covered in the vial label section, a label showing "30 mg" for total content does not mean the concentration is 30 mg/mL. If that vial holds 3 mL of liquid, the concentration is actually 10 mg/mL. Using 30 in the formula instead of 10 would calculate 75 units as 22.5 mg instead of the correct 7.5 mg. That is a three-fold overdose.
Mistake 3: using the wrong syringe type
Not all syringes are U-100. Some specialty syringes use different unit scales. A U-40 syringe divides 1 mL into 40 units instead of 100. Drawing to the 75 mark on a U-40 syringe would actually be 1.875 mL, not 0.75 mL. At 10 mg/mL, this would deliver 18.75 mg instead of 7.5 mg. Always confirm you are using a standard U-100 insulin syringe when following any tirzepatide conversion guide or injection dosage chart.
Mistake 4: forgetting about air bubbles
A syringe that appears to read 75 units but contains a visible air bubble might actually hold only 70 to 73 units of liquid. At 10 mg/mL, that air bubble represents 0.2 to 0.5 mg of missing medication. Over weeks of injections, this cumulative shortfall adds up. Tap out bubbles before every injection.
Mistake 5: not accounting for concentration changes when switching vials
This happens when someone finishes one vial and starts a new one from a different pharmacy or batch with a different concentration. They draw their usual 75 units without realizing the new vial is 20 mg/mL instead of 10 mg/mL. Suddenly they are injecting 15 mg instead of 7.5 mg. Double the dose. The side effects hit hard, and the anxiety, body aches, and gastrointestinal distress can be severe.
Every new vial is a new calculation. Check the concentration label every single time, even if you are reordering from the same pharmacy. Formulations and concentrations can change between batches.
Mistake 6: rounding errors
Some concentration and dose combinations produce non-round unit numbers. At 15 mg/mL, getting exactly 7.5 mg requires 50 units, which is clean. But getting 10 mg requires 66.67 units. You cannot draw to 66.67 on a standard syringe. You either round to 66 or 67 units, which gives you 9.9 mg or 10.05 mg. These small differences are clinically insignificant, but they illustrate why choosing a concentration that produces round numbers for your target dose makes life easier.
The tirzepatide dosage calculator on SeekPeptides handles rounding automatically and flags when a dose-concentration combination requires imprecise syringe readings.
What to do when switching concentrations
Switching between vials with different concentrations is common. Pharmacies change formulations. Providers adjust prescriptions. Vials run out and replacements come from different sources. Here is how to handle the transition safely.
Step 1: identify both concentrations
Before anything else, write down your old concentration and your new concentration. Old vial: 10 mg/mL. New vial: 20 mg/mL. Having both numbers visible prevents the kind of mental shortcuts that lead to errors.
Step 2: recalculate your units
If your prescribed dose is 7.5 mg, calculate the new unit number for the new concentration. At 10 mg/mL, 7.5 mg equals 75 units. At 20 mg/mL, 7.5 mg equals 37.5 units. Write this down too. Some people use a marker to note the correct unit number directly on their new vial.
Step 3: double-check before drawing
On your first draw from the new vial, go through the full formula manually. Do not rely on memory or habit. Habits formed from months of drawing 75 units are strong, and it takes conscious effort to override them and draw 37.5 units instead. One mistake here could mean significant side effects from an accidental double dose.
Step 4: set up the new routine
After two or three draws from the new vial, the new unit number becomes familiar. Some people keep a small reference card with their supplies that lists their current concentration and corresponding units for each dose tier. This eliminates guesswork, especially for people who store their tirzepatide in the fridge alongside multiple vials.
If you are considering a broader change to your protocol, including switching to a completely different medication like semaglutide, the unit calculations will be entirely different because semaglutide concentrations do not match tirzepatide concentrations. Consult the semaglutide vs tirzepatide dosage chart for side-by-side comparisons, and always work with your provider when making medication changes.
75 units compared to other common tirzepatide unit draws
Putting 75 units in context with other commonly searched unit amounts helps illustrate the dose spectrum and shows where 75 units fits relative to starting, maintenance, and maximum doses.
How 75 units compares (at 10 mg/mL)
Units drawn | mg at 10 mg/mL | Dose tier | Typical use |
|---|---|---|---|
2.5 mg | Tier 1 | Starting dose, first 4 weeks | |
3 mg | Custom | Slow titration | |
4 mg | Custom | Conservative increase | |
5 mg | Tier 2 | Standard second dose | |
75 units | 7.5 mg | Tier 3 | Mid-range therapeutic dose |
10 mg | Tier 4 | Upper therapeutic dose | |
15 mg | Tier 5 | Maximum standard dose |
At 10 mg/mL, 75 units sits right in the middle of the dose spectrum. It is three times the starting dose and half of the maximum. For many people, the 7.5 mg tier is where they find their maintenance sweet spot, experiencing good results without the more intense side effects that sometimes accompany higher doses.
The same comparison at 20 mg/mL
At 20 mg/mL, the entire scale shifts. Now 75 units delivers 15 mg (the maximum standard dose), and much lower unit draws are needed for the earlier tiers.
Units drawn | mg at 20 mg/mL | Dose tier |
|---|---|---|
12.5 units | 2.5 mg | Tier 1 |
25 units | 5 mg | Tier 2 |
37.5 units | 7.5 mg | Tier 3 |
50 units | 10 mg | Tier 4 |
62.5 units | 12.5 mg | Between tier 4 and 5 |
75 units | 15 mg | Tier 5 (maximum) |
Notice how the same 75 units means tier 3 at one concentration and tier 5 at another. This table alone demonstrates why blind unit-based dosing without concentration awareness is dangerous.
Cross-referencing with semaglutide
For people who have previously used semaglutide measured in units, the conversion principles are identical but the concentrations and dose ranges differ. Semaglutide commonly comes in 5 mg/mL or 10 mg/mL concentrations. Drawing 75 units from a 5 mg/mL semaglutide vial gives a different dose than 75 units from a 10 mg/mL tirzepatide vial. The formula is the same. The medications and their appropriate dose ranges are not.
If you are comparing or choosing between semaglutide and tirzepatide, the dose conversions between the two medications do not follow a simple ratio. They are different drugs with different potencies, mechanisms, and dosing schedules.
Special considerations for 75 units
There are several practical factors specific to drawing and injecting 75 units that deserve attention.
Injection volume comfort
At 0.75 mL, a 75-unit injection is a moderate volume. Most people tolerate it well. However, it is more liquid than the smaller 25 or 50 unit injections many people start with, and some notice increased discomfort at the injection site. Choosing the right injection site helps. The abdomen typically handles larger volumes better than the thigh because of greater subcutaneous fat distribution in most people.
If 0.75 mL causes consistent injection site reactions, options include switching to a higher concentration vial (which reduces the volume for the same dose) or splitting the dose across two smaller injections.
Vial usage efficiency
How many 75-unit draws you get from a vial depends on the total vial volume. A standard 3 mL vial allows four full 75-unit draws (4 x 0.75 mL = 3 mL). A 2 mL vial allows two draws with 0.5 mL remaining. A 5 mL vial allows six draws with 0.5 mL left over.
That leftover liquid is still usable. At 10 mg/mL, 0.5 mL remaining in a vial equals 50 units (5 mg). Wasting it means wasting medication and money. Some people adjust their reconstitution volume specifically to avoid leftovers, making every draw come out even. This is especially relevant for people who are cost-conscious about affordable tirzepatide options.
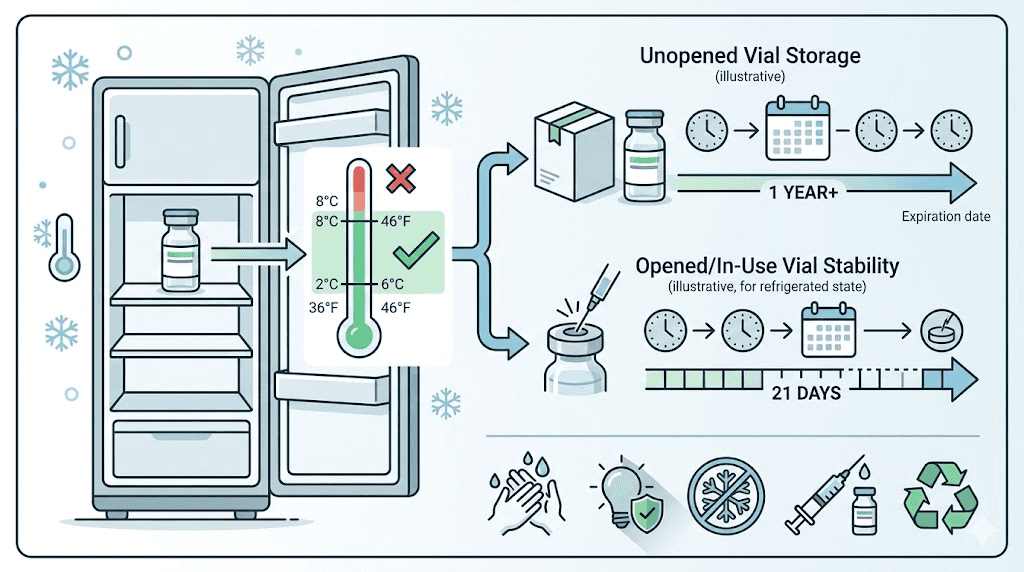
Storage after drawing
Once you puncture a vial with a needle, the clock starts on stability. Refrigerated tirzepatide generally remains stable for 28 to 56 days after first puncture, depending on the formulation. Room temperature stability is shorter. If you are drawing 75 units weekly from a multi-dose vial, make sure you will finish the vial within the stability window.
Planning your draws matters. A 3 mL vial at 75 units per week lasts four weeks. That fits comfortably within most stability windows. A larger 5 mL vial at the same draw rate lasts nearly seven weeks, which might push past the recommended storage duration. Check your pharmacy documentation for specific stability data, and review tirzepatide expiration guidelines if you have concerns.
Temperature and handling
Temperature fluctuations can degrade tirzepatide and potentially alter the effective concentration. If a vial was accidentally left warm or exposed to direct sunlight, the potency may have decreased. In that case, drawing 75 units might deliver less than the calculated milligrams because some of the active compound has degraded. When in doubt, use a fresh vial.
Using the formula for other unit amounts
Once you understand how 75 units converts, you can apply the same formula to any number of units. The math does not change. Here are quick references for the most commonly searched conversions, all using the same formula: mg = (units / 100) x concentration.
Lower unit amounts
For people in early titration phases or on microdosing schedules, smaller draws are common.
25 units at 10 mg/mL equals 2.5 mg. At 20 mg/mL, it equals 5 mg. At 5 mg/mL, it equals 1.25 mg.
10 units at 10 mg/mL equals 1 mg. This is a common microdose. At 20 mg/mL, 10 units equals 2 mg.
20 units at 10 mg/mL equals 2 mg. Slightly below the standard starting dose.
Higher unit amounts
For people at maintenance doses or on higher concentration vials.
40 units at 10 mg/mL equals 4 mg. At 20 mg/mL, it equals 8 mg.
50 units at 10 mg/mL equals 5 mg (tier 2). At 20 mg/mL, it equals 10 mg (tier 4).
100 units at 10 mg/mL equals 10 mg (tier 4). At 20 mg/mL, it equals 20 mg (above standard tiers).
Each of these conversions follows the exact same formula. The only variable that changes is the concentration. Bookmark the complete tirzepatide dosing chart in units for a comprehensive reference that covers all unit amounts at all common concentrations.
Safety considerations when measuring 75 units
Accurate measurement is a safety issue, not just a convenience issue. Here are the key safety practices for anyone drawing 75 units of tirzepatide.
Always verify with your provider
Online conversion charts and calculators, including this one, are educational tools. They are not a substitute for medical guidance. Before drawing 75 units (or any amount), confirm with your healthcare provider that the resulting milligram dose is appropriate for your current stage of treatment, your body weight, and your medical history.
Use clean technique
Wipe the vial stopper with an alcohol swab before every draw. Use a new, sterile syringe for each injection. Never reuse needles or syringes. Contamination is a real risk, especially with multi-dose vials that get punctured multiple times over weeks. For detailed injection technique and safety protocols, dedicated guides cover the full process.
Keep records
Record every injection: date, time, units drawn, concentration, calculated milligrams, and injection site. This log helps your provider adjust your protocol, helps you track your own progress timeline, and serves as a safety check if something seems off. If you suddenly experience unexpected side effects, reviewing your log might reveal a dosing discrepancy you missed in the moment.
Recognize overdose symptoms
If you accidentally inject more than intended (which can happen if you use the wrong concentration in your calculation), watch for severe nausea, vomiting, diarrhea, and abdominal pain. These symptoms at an extreme level differ from the mild gastrointestinal effects many people experience during normal titration. Contact your healthcare provider immediately if you suspect an overdose.
Watch for signs of underdosing
Underdosing is less immediately dangerous but still problematic. If your 75 units is delivering less medication than intended (due to air bubbles, wrong concentration, or degraded peptide), you may notice that tirzepatide seems to stop working or that your appetite suppression has decreased. Before assuming you need a higher dose, verify your conversion math and check your vial concentration.
Interactions and co-administered substances
The milligram dose of tirzepatide interacts with other factors in your protocol. If you are taking supplements alongside tirzepatide or combining it with other treatments, the actual dose matters for safety assessments. Your provider needs to know exactly how many milligrams you are taking, not how many units. Always communicate in milligrams when discussing your dose with medical professionals.
For researchers exploring SeekPeptides protocols, the platform provides dosing tools that automatically handle concentration-based calculations, reducing the risk of manual math errors.
Tirzepatide delivery methods and how they affect unit measurements
Not all tirzepatide comes in vials that require syringe measurement. Understanding the alternatives helps contextualize when unit-to-mg conversions are relevant and when they are not.
Pre-filled pens (brand-name Mounjaro and Zepbound)
Brand-name tirzepatide comes in pre-filled injection pens with fixed doses. Each pen delivers a specific milligram amount: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, or 15 mg. You do not measure units. You do not need to know the concentration. The pen handles everything. Unit-to-mg conversions are completely irrelevant for pre-filled pen users.
The only scenario where a pen user might care about units is if they are transitioning to compounded tirzepatide from a vial and need to replicate their pen dose using an insulin syringe.
Compounded vials with insulin syringes
This is the primary scenario where unit-to-mg conversions matter. Compounded tirzepatide from a pharmacy comes in a multi-dose vial with a rubber stopper. You draw your dose manually using an insulin syringe, which means you need to know your concentration and do the conversion math (or use a chart). This is where most people encounter the "how many mg is 75 units" question.
Oral tirzepatide formulations
Oral tirzepatide is an emerging option that bypasses injection entirely. Sublingual drops, tablets, and orally disintegrating formulations deliver tirzepatide in milligrams specified on the packaging. No syringe measurement needed. No unit conversions. The dose is what the label says.
If you are curious about whether oral tirzepatide compares to injectable in terms of effectiveness, that is a separate question from unit conversions, but worth exploring if syringe-based dosing is a barrier for you.
Reconstituted research peptides
Research peptides arrive as lyophilized (freeze-dried) powder that must be reconstituted with bacteriostatic water. The concentration depends entirely on how much water you add. This is where unit-to-mg conversions become most critical and most prone to error. Every detail from the reconstitution chart directly affects what 75 units means in milligrams.
Practical tips for accurate 75-unit measurements
Beyond understanding the math, there are practical techniques that improve measurement accuracy.
Use the right syringe size
A 1 mL (100 unit) syringe with 2-unit markings works for 75 units, but a 0.5 mL (50 unit) syringe is too small. If you have access to a 1 mL syringe with 1-unit markings (commonly available as allergy syringes), the finer gradations make hitting exactly 75 easier to confirm visually.
Draw slowly
Pulling the plunger too fast creates turbulence inside the syringe, introducing tiny bubbles and making the fluid level harder to read. Draw slowly and steadily. Pause at 75 units. Check the level. Adjust if needed by pushing slightly back and drawing again.
Prime the needle
Before your first draw from a new vial, some people "prime" the syringe by drawing a small amount of air, injecting it into the vial (to equalize pressure), then drawing their dose. This prevents the vacuum effect that can make accurate drawing difficult and reduces the risk of air bubbles in the medication.
Double-check with a second measurement
For critical doses, draw your 75 units, then look away and look back. Does it still read 75? Are there any bubbles you missed? Is the meniscus aligned correctly? This two-second double-check catches errors that hurried measurements miss.
Keep your supplies organized
If you have multiple vials with different concentrations (perhaps leftover from a previous prescription alongside a current one), label them clearly. Some people use colored tape or marker to distinguish between concentrations. Grabbing the wrong vial and drawing 75 units from a 20 mg/mL vial instead of a 10 mg/mL vial doubles your dose instantly.
Organizational habits matter more than math skills when it comes to safe syringe dosing. A well-organized supply setup prevents more errors than a perfect understanding of the formula.
When 75 units might need adjustment
Several situations might lead you or your provider to adjust your 75-unit draw up or down.
Side effects at current dose
If 75 units at your concentration is causing significant headaches, insomnia, joint pain, or persistent diarrhea, your provider might reduce your draw. At 10 mg/mL, dropping from 75 units (7.5 mg) to 60 units (6 mg) or even 50 units (5 mg) can meaningfully reduce side effects while maintaining some therapeutic benefit.
Insufficient results
If 75 units is not producing expected results and you have been at this dose for the recommended minimum of four weeks, your provider might increase to 100 units (10 mg at 10 mg/mL). Patience matters here. Tirzepatide takes time to reach full effect at each dose level, and premature increases lead to unnecessary side effects.
If you feel like your dose has plateaued, review why you might not be losing weight on tirzepatide before assuming the dose is the issue. Dietary factors, exercise patterns, sleep quality, and food choices all influence outcomes.
Weight changes
As you lose weight, your effective dose-per-kilogram increases even though the absolute milligrams stay the same. A 7.5 mg dose for a 100 kg person (0.075 mg/kg) becomes 0.094 mg/kg at 80 kg. This relative increase can intensify both effects and side effects. Some providers periodically reassess the dose as weight changes, potentially reducing from 75 units to a lower number.
Transitioning to maintenance
Once weight loss goals are reached, some people transition to a maintenance dose lower than their peak treatment dose. Dropping from 100 units (10 mg at 10 mg/mL) back to 75 units (7.5 mg) for long-term maintenance is a common pattern. The lower dose maintains appetite suppression and metabolic benefits with fewer side effects. Understanding the full weight loss timeline helps set expectations for each phase.
The relationship between 75 units and meal planning
Your tirzepatide dose directly affects your appetite and food tolerance, which makes the actual milligrams (not just units) relevant to your diet planning.
At 7.5 mg (75 units from a 10 mg/mL vial), most people experience moderate appetite suppression. They can eat but feel satisfied with smaller portions. Meal planning at this dose typically focuses on protein-forward meals with adequate fiber and hydration.
At 15 mg (75 units from a 20 mg/mL vial), appetite suppression is significantly stronger. Eating becomes more deliberate. Some people struggle to consume enough protein to prevent muscle loss. Foods to avoid at this dose include heavy, fatty meals that can exacerbate nausea and slow gastric emptying even further.
The point is that "75 units" tells you nothing about how the dose will affect your eating experience unless you know the milligrams. A person drawing 75 units from a 5 mg/mL vial (3.75 mg) will have a vastly different appetite than someone drawing 75 units from a 20 mg/mL vial (15 mg). Plan your meals based on the milligram dose, not the syringe reading.
Whether you should eat more or less on tirzepatide, what to prioritize nutritionally, and how to optimize food choices for GLP-1 medications in general are all important pieces of the puzzle. And alcohol considerations apply regardless of your unit count because alcohol interacts with the medication at the pharmacological level, not the volume level.
Working with your healthcare provider
Communication with your provider should always center on milligrams, not units. Here is why and how to structure those conversations.
Speak in milligrams
When your provider asks about your dose, say "7.5 milligrams" instead of "75 units." Units are meaningless without concentration context. Your provider needs to know the drug amount to make clinical decisions. If you say "75 units" and your provider assumes a different concentration than what you are using, miscommunication can lead to inappropriate dosing recommendations.
Report your concentration
Always tell your provider which concentration you are using. "I am taking 7.5 mg from a 10 mg/mL vial, which is 75 units" gives them the complete picture. This is especially important if you switch pharmacies, switch from brand-name pens to compounded vials, or change anything about your medication source.
Ask about titration plans
If you are currently at 75 units (7.5 mg at 10 mg/mL), ask your provider what the next step looks like. Will they increase to 100 units (10 mg)? Will they change your concentration? Will they keep you at this dose for longer? Understanding the plan helps you prepare mentally and logistically for dose changes, including having the right supplies ready.
For people researching protocols independently, SeekPeptides members access detailed titration schedules, dose-specific guidance, and community insights from others who have navigated the same questions about unit conversions and dose optimization.
Comparing 75 units across different GLP-1 medications
If you are comparing tirzepatide to other GLP-1 medications, understanding how 75 units translates across different drugs highlights important differences.
Tirzepatide vs. semaglutide at 75 units
Drawing 75 units from a semaglutide vial gives a completely different milligram dose than drawing 75 units from a tirzepatide vial, even at the same concentration. At 10 mg/mL, both would give you 7.5 mg of liquid medication. But 7.5 mg of semaglutide and 7.5 mg of tirzepatide are not equivalent doses. They are different molecules with different potencies.
Semaglutide is typically dosed much lower than tirzepatide: the maximum semaglutide dose for weight loss is 2.4 mg per week, while tirzepatide goes up to 15 mg per week. Drawing 75 units (7.5 mg) of semaglutide from a 10 mg/mL vial would be more than three times the maximum recommended semaglutide dose. This is why you can never transfer unit-based dosing knowledge between medications without recalculating from scratch.
For detailed dose comparisons, the semaglutide vs tirzepatide dosage chart maps equivalent therapeutic doses side by side.
Other GLP-1 comparisons
Newer GLP-1 medications are entering the market with different dosing structures. Survodutide, CagriSema, and orforglipron each have unique dosing ranges that make cross-medication unit comparisons misleading. Retatrutide, another triple-agonist peptide, has its own dosing protocols that share some conceptual similarities with tirzepatide but use entirely different dose ranges.
The universal lesson: units are a volume measurement, not a dose measurement. The same 75 units can mean wildly different things depending on the medication and concentration involved.
Building confidence with tirzepatide dosing
If you are new to measuring your own injections, the unit-to-milligram conversion can feel intimidating. That anxiety is normal. It fades with practice and understanding.
Start with the formula
Write the formula somewhere visible: mg = (units / 100) x concentration. Practice it with different numbers until it feels automatic. Test yourself. If your vial is 10 mg/mL and you draw 50 units, how many mg? Answer: 5 mg. If you draw 75 units? 7.5 mg. If you switch to a 20 mg/mL vial and draw 75 units? 15 mg. Repetition builds confidence.
Use tools
Online dosage calculators, the SeekPeptides peptide calculator, and GLP-1 plotter tools eliminate the possibility of arithmetic errors. Enter your concentration and units, get your milligrams. Use them every time until you trust your mental math.
Keep a reference chart
Print or save the conversion table from this article. Keep it with your injection supplies. When you draw 75 units, glance at the chart for your concentration to confirm the milligrams. This takes three seconds and prevents the most common errors.
Ask questions
If something does not make sense, ask. Ask your pharmacist. Ask your provider. Ask in SeekPeptides community forums where thousands of experienced researchers discuss dosing questions daily. No question about medication dosing is too basic. The only dangerous question is the one you do not ask.
Advanced considerations: dose timing and its interaction with unit accuracy
The timing of your injection can amplify or reduce the impact of small dosing variations inherent in syringe measurements.
Weekly consistency
Tirzepatide is a once-weekly medication. If you consistently draw slightly more or slightly less than 75 units due to measurement variability, the effect compounds over weeks. Drawing 77 units instead of 75 (only 2 units off) means an extra 0.2 mg per week at 10 mg/mL. Over four weeks, that is 0.8 mg of extra tirzepatide. Small numbers individually, but not insignificant over time.
Consistent technique minimizes this variation. Same lighting. Same hand position. Same eye level. Same syringe brand. Routine creates precision.
Best time to inject
While the best time to take a GLP-1 shot is primarily about side effect management and personal convenience, consistent timing also means consistent attention to measurement. If you always inject at the same time, in the same place, with the same routine, you are less likely to make errors than if you inject at random times when you might be distracted or rushed.
Can you take it a day early?
If your injection schedule shifts, some people wonder about taking tirzepatide a day early. The dosing flexibility is separate from the unit conversion math, but the milligram dose stays the same regardless of timing. 75 units at your concentration delivers the same milligrams whether you inject on day 6 or day 8 of your weekly cycle.
Frequently asked questions
Is 75 units of tirzepatide always 7.5 mg?
No. 75 units equals 7.5 mg only at a concentration of 10 mg/mL. At other concentrations, the milligram amount changes. At 5 mg/mL, 75 units is 3.75 mg. At 20 mg/mL, 75 units is 15 mg. Always check your vial concentration before calculating your dose.
How do I find the concentration on my tirzepatide vial?
Look for a number expressed as mg/mL on your vial label. It might say "10 mg/mL" or "10mg per mL" or list total content alongside volume (for example, "30 mg in 3 mL" which equals 10 mg/mL). If you cannot find it, contact your pharmacy. Never guess the concentration.
What syringe should I use for 75 units of tirzepatide?
Use a standard U-100 insulin syringe with a capacity of at least 1 mL (100 units). A 0.5 mL (50 unit) syringe is too small to hold 75 units. Choose a syringe with fine-gauge markings for more precise reading. For complete guidance on syringe selection and dosage technique, review our detailed guide.
Can I draw 75 units from any tirzepatide vial?
You can draw 75 units from any vial that contains at least 0.75 mL of liquid. However, the milligrams you receive will differ based on concentration. Always verify that the resulting milligram dose matches what your provider prescribed before drawing.
What if I accidentally drew more than 75 units?
If you have not injected yet, simply push the excess back into the vial or discard it by pushing the plunger until the syringe reads exactly 75. If you have already injected more than intended, calculate the extra milligrams using the formula and monitor for increased side effects. Contact your provider if you significantly exceeded your prescribed dose.
Is 7.5 mg of tirzepatide a good dose for weight loss?
The 7.5 mg dose (tier 3) is a therapeutic dose that produces meaningful weight loss in clinical studies. Most people reach this dose after 8 weeks of titration starting at 2.5 mg. Whether it is the right dose for you depends on your individual response, side effect tolerance, and treatment goals. Review tirzepatide dosing for weight loss for the full titration protocol.
How many doses can I get from a 3 mL vial at 75 units per draw?
A 3 mL vial contains 300 units total. At 75 units per draw, you get exactly 4 doses. There is no leftover. At 10 mg/mL, that is 4 weekly doses of 7.5 mg each, totaling 30 mg of tirzepatide per vial.
Does 75 units of tirzepatide hurt to inject?
A 75-unit (0.75 mL) injection is a moderate volume. Most people report minimal pain with proper technique. Using a 30 or 31 gauge needle, injecting slowly, and choosing a site with adequate subcutaneous fat like the abdomen all reduce discomfort. If you experience persistent injection site reactions, rotating sites and adjusting technique usually helps.
Can I use the same conversion formula for semaglutide?
Yes, the formula mg = (units / 100) x concentration works for any injectable medication measured with a U-100 insulin syringe. But remember that semaglutide and tirzepatide have very different therapeutic dose ranges. The semaglutide units to mg conversion follows the same math but applies to a different dose schedule.
Should I round up or down if my units do not come out to a whole number?
When your calculation produces a non-whole number (like 66.7 units), round to the nearest whole unit. For tirzepatide, the difference between rounding up or down by 1 unit at typical concentrations is less than 0.2 mg, which is clinically insignificant. If precision matters for your protocol, discuss with your provider or use a concentration that produces clean numbers for your target dose.
External resources
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven dosing calculators, and a community of thousands who have navigated these exact conversion questions.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your syringes stay precise, and your protocols stay consistent.