Feb 22, 2026

You are sitting at the highest dose of tirzepatide. The one that produced 22.5% body weight loss in clinical trials. The one that 57% of participants rode to a 20% or greater reduction in total weight. And right now, you are staring at a vial and a syringe, trying to figure out exactly how many units to draw for 15 mg.
Get it wrong, and you either waste expensive peptide or underdose yourself during the most critical phase of your protocol. The problem is that "15 mg" does not translate to a single number of units. It depends entirely on your compounded tirzepatide concentration, and concentrations vary wildly between pharmacies. A 10 mg/mL vial demands a completely different draw than a 20 mg/mL or 40 mg/mL vial. Confuse the two and you could inject double your intended dose, or half of it.
This guide gives you the exact unit counts for 15 mg of tirzepatide at every common concentration. You will find conversion tables, step-by-step calculation walkthroughs, syringe selection guidance (because 15 mg creates a unique problem at certain concentrations), and practical tips from the SeekPeptides research community. Whether you are using a standard insulin syringe or a tuberculin syringe, whether your vial reads 10 mg/mL or 60 mg/mL, the math is here. No guessing. No estimating. Just the numbers you need to dose accurately at 15 mg.
The quick answer: 15 mg of tirzepatide in units
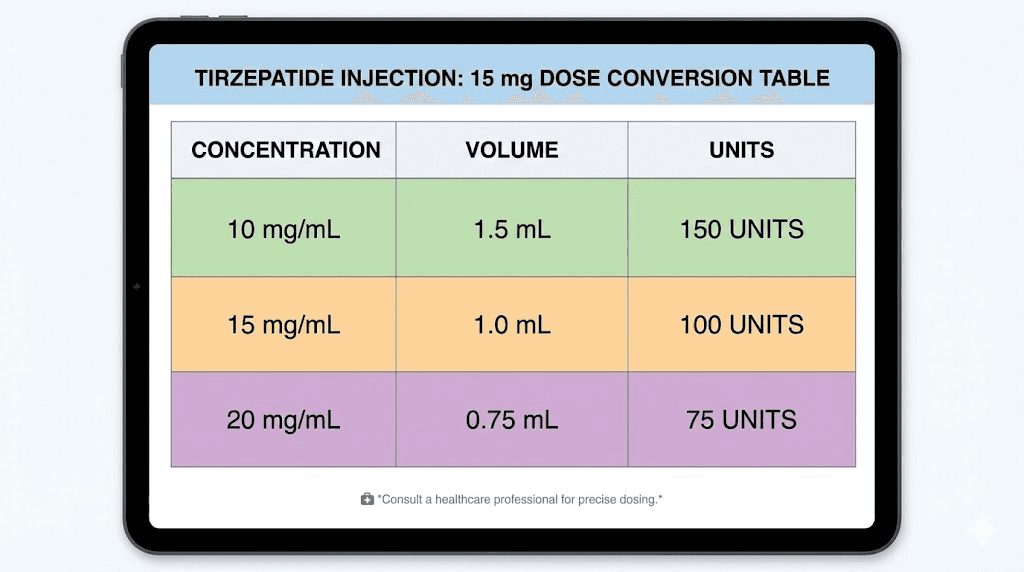
The number of units you draw for 15 mg of tirzepatide depends on one thing: the concentration printed on your vial. That concentration, measured in milligrams per milliliter (mg/mL), tells you how much tirzepatide is dissolved in each milliliter of solution. A higher concentration means more peptide packed into less liquid, which means fewer units on your syringe.
Here is the complete breakdown for every common concentration:
10 mg/mL concentration: 15 mg = 150 units (1.5 mL)
15 mg/mL concentration: 15 mg = 100 units (1.0 mL)
20 mg/mL concentration: 15 mg = 75 units (0.75 mL)
30 mg/mL concentration: 15 mg = 50 units (0.5 mL)
40 mg/mL concentration: 15 mg = 37.5 units (0.375 mL)
50 mg/mL concentration: 15 mg = 30 units (0.3 mL)
60 mg/mL concentration: 15 mg = 25 units (0.25 mL)
Notice something critical. At 10 mg/mL, you need 150 units. A standard insulin syringe only holds 100 units (1 mL). That means at the most common compounded concentration, a single insulin syringe cannot hold your full 15 mg dose. This is a real problem that catches people off guard, and we will solve it completely in the syringe section below.
At 20 mg/mL, the math works out to a clean 75 units, which fits comfortably in any standard syringe. At 30 mg/mL, you need just 50 units. And at the higher concentrations like 40 or 60 mg/mL, the injection volume shrinks to a tiny draw that requires precise measurement.
If you have used tirzepatide at lower doses, you already know the basics of this conversion from guides like our 2.5 mg unit conversion or 5 mg unit conversion. The formula is identical. But 15 mg introduces volume challenges that lower doses never encounter, which is why this guide exists.
The formula is simple: Units = (dose in mg / concentration in mg per mL) x 100. For 15 mg at 20 mg/mL, that is (15 / 20) x 100 = 75 units. For 15 mg at 10 mg/mL, that is (15 / 10) x 100 = 150 units. Same dose, completely different syringe draws. Always check your vial label before you pick up the syringe. For a deeper dive into unit conversions across all dose levels, see our complete tirzepatide dosage chart in units.
Why concentration changes everything about your 15 mg dose
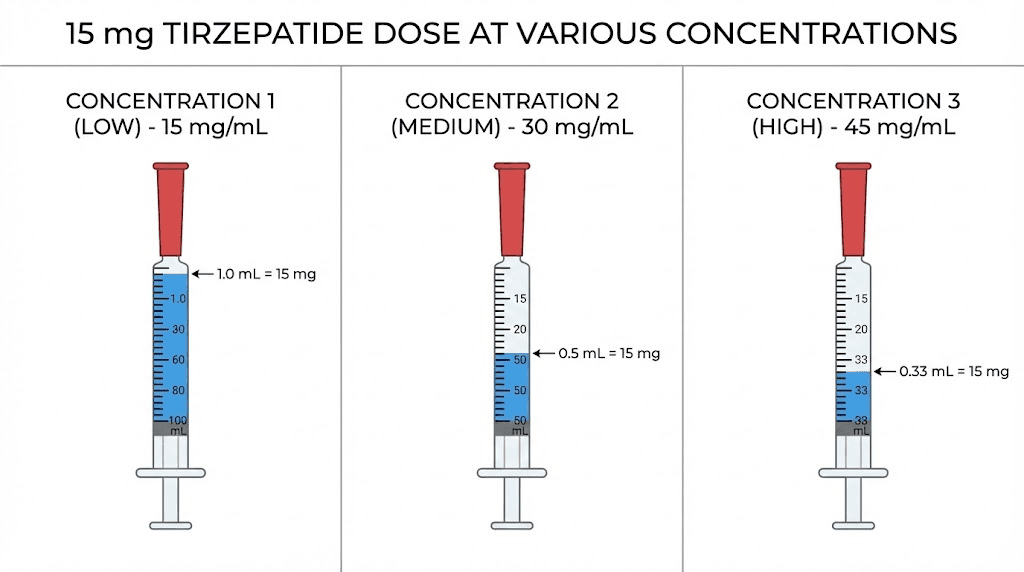
Concentration is the single most important number on your tirzepatide vial. It determines how many units you draw, which syringe you use, how much liquid enters your body, and whether your injection site can comfortably absorb the volume. At 15 mg, concentration matters more than at any other dose level because you are working with the largest milligram amount in the standard tirzepatide dosing protocol.
Think of it this way. Two vials sit on your counter. Both contain tirzepatide. One reads 10 mg/mL. The other reads 40 mg/mL. To get your 15 mg dose from the first vial, you draw 150 units of liquid. From the second, you draw just 37.5 units. Same medication, same dose, but one injection is four times the volume of the other.
That volume difference is not trivial.
Larger injection volumes mean more liquid pooling under the skin at the injection site. This can increase discomfort, cause more prominent lumps or welts, slow absorption, and sometimes trigger injection site reactions. At 1.5 mL (the volume for 15 mg at 10 mg/mL), you are injecting a substantial amount of fluid subcutaneously. Many practitioners prefer to split that into two separate injections of 75 units each, administered at different sites.
Higher concentrations solve this elegantly. At 20 mg/mL, your 15 mg dose is only 0.75 mL, a comfortable single injection. At 40 mg/mL, it shrinks to 0.375 mL, barely noticeable. This is why many compounding pharmacies transition patients to higher concentration vials once they reach the 10 mg dose level and above.
But higher concentration creates its own challenge. Reading 37.5 units on a syringe requires sharp eyes and steady hands. The markings on most insulin syringes show every 2 units, and hitting exactly 37.5 means landing precisely between the 36 and 38 unit lines. A half-unit error at 40 mg/mL concentration changes your actual dose by 0.2 mg, which is relatively small. The same half-unit error at 10 mg/mL changes your dose by only 0.05 mg. Lower concentrations are more forgiving of measurement imprecision.
Understanding your compounded tirzepatide dosage starts with reading that concentration label carefully. If you are unsure about your vial concentration, check with your compounding pharmacy before drawing any medication. Guessing is not an option at 15 mg.
Complete conversion table: 15 mg at every concentration
This table covers every concentration you are likely to encounter from compounding pharmacies. Some concentrations are more common than others, but having the full range ensures you can verify your calculation regardless of which pharmacy supplied your vial. For context on how these numbers compare to other dose levels, our tirzepatide dosage chart in units covers every dose from 2.5 mg through 15 mg.
Concentration (mg/mL) | Units to draw | Volume (mL) | Fits standard insulin syringe? | Notes |
|---|---|---|---|---|
5 mg/mL | 300 units | 3.0 mL | No (need 3 mL syringe) | Very uncommon at this dose |
10 mg/mL | 150 units | 1.5 mL | No (exceeds 100 unit max) | Split into two draws |
15 mg/mL | 100 units | 1.0 mL | Yes (exactly full) | Clean, full syringe draw |
20 mg/mL | 75 units | 0.75 mL | Yes | Most practical for 15 mg |
25 mg/mL | 60 units | 0.6 mL | Yes | Clean number, easy to read |
30 mg/mL | 50 units | 0.5 mL | Yes | Half syringe, very comfortable |
40 mg/mL | 37.5 units | 0.375 mL | Yes | Requires precise measurement |
50 mg/mL | 30 units | 0.3 mL | Yes | Small volume, clean number |
60 mg/mL | 25 units | 0.25 mL | Yes | Very small injection volume |
A few things jump out from this table. First, the two most commonly dispensed concentrations for compounded tirzepatide are 10 mg/mL and 20 mg/mL. If your pharmacy started you on a lower dose with a 10 mg/mL vial, they may switch you to 20 mg/mL or higher once you reach the 10 mg or 15 mg dose level. Always confirm which concentration you received when picking up a new vial.
Second, the "fits standard insulin syringe" column matters enormously. At 10 mg/mL, a standard 1 mL insulin syringe cannot hold your full 15 mg dose. You have two options: use a larger syringe (like a 3 mL luer lock syringe) or split your dose into two separate draws. We cover both approaches in detail below.
Third, notice that 37.5 units (at 40 mg/mL) falls between the standard syringe markings. If your syringe marks every 2 units, you need to estimate the midpoint between 36 and 38. For maximum accuracy at these concentrations, consider using a 0.5 mL insulin syringe with half-unit markings. These syringes show every single unit, making it much easier to hit 37 or 38 units precisely.
Compare these numbers to lower dose conversions you may have used before. At 7.5 mg, a 20 mg/mL vial requires just 37.5 units. At 10 mg, the same vial requires 50 units. Now at 15 mg, you need 75 units from that same concentration. The math scales linearly, but the practical implications at each dose level differ significantly.
For a broader reference covering every dose and concentration combination, the tirzepatide injection dosage chart provides a comprehensive matrix you can bookmark for ongoing reference.
The syringe problem at 15 mg (and how to solve it)
Here is the problem nobody warns you about until you are standing at the counter with a vial and a syringe that cannot hold your dose.
A standard insulin syringe holds 100 units. That is 1 mL of liquid. At 10 mg/mL concentration, which is the most common concentration dispensed by many compounding pharmacies, your 15 mg dose requires 150 units. One hundred and fifty. That is 50 units more than your syringe can physically hold.
This is not a rounding issue or a minor inconvenience. It is a fundamental mismatch between your dose and your equipment.
Three solutions exist, each with trade-offs.
Solution 1: Split the dose into two injections. Draw 75 units into one syringe and inject at one site (like the left side of your abdomen). Draw another 75 units into a second syringe and inject at a different site (like the right side of your abdomen). This keeps you within the capacity of standard insulin syringes and actually improves absorption because you are distributing the liquid across two sites instead of one. The downside is obvious: two needle sticks instead of one. For practical injection technique guidance, see our GLP-1 injection guide.
Solution 2: Use a larger syringe. A 3 mL luer lock syringe can hold 150 units and more. The problem is that these syringes have thicker needles and less precise gradation marks compared to insulin syringes. The lines are spaced further apart (typically marked in 0.1 mL increments rather than individual units), which can make precise measurement more difficult. If you go this route, attach a separate thin-gauge needle (27-31 gauge) for the actual injection to minimize discomfort.
Solution 3: Switch to a higher concentration vial. This is the cleanest solution. Ask your compounding pharmacy for a 20 mg/mL vial instead. At 20 mg/mL, your 15 mg dose is 75 units, which fits perfectly in a standard insulin syringe with room to spare. Many pharmacies automatically transition patients to higher concentrations when they reach the 10 mg or 15 mg dose. If yours has not, call and ask.
Which solution is best? For most people, solution 3 eliminates the problem entirely. If you cannot get a higher concentration vial, solution 1 (splitting the dose) is the safest and most practical approach. Most tirzepatide dosing protocols allow for split injections at the higher dose levels.
One thing to avoid: do not try to estimate or overfill your insulin syringe past the 100 unit mark. The barrel narrows near the plunger end, and forcing extra liquid in can cause inaccurate dosing, leakage, and even syringe failure during injection. Always stay within your syringe rated capacity.
Step-by-step: how to calculate units for 15 mg of tirzepatide
Memorizing conversion tables works. But understanding the formula means you can calculate the correct draw for any dose at any concentration, even if your pharmacy changes vials on you. The math takes about five seconds once you know it.
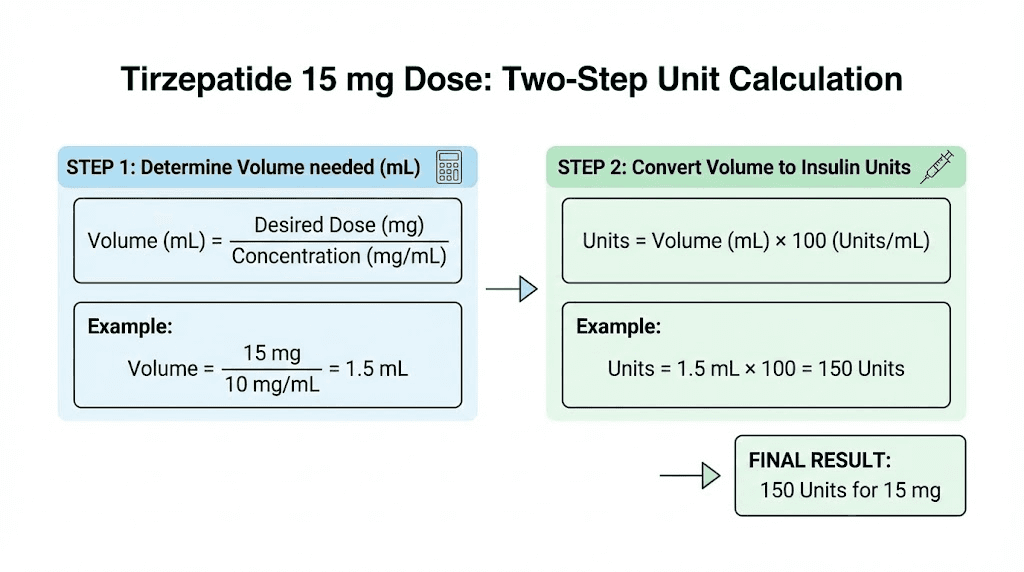
The formula:
Step 1: Divide your dose (in mg) by your vial concentration (in mg/mL).
Step 2: Multiply the result by 100 to convert mL to syringe units.
That is it. Two steps. Let us walk through several real examples for the 15 mg dose.
Example 1: 15 mg from a 10 mg/mL vial
Step 1: 15 mg / 10 mg per mL = 1.5 mL
Step 2: 1.5 mL x 100 = 150 units
Example 2: 15 mg from a 20 mg/mL vial
Step 1: 15 mg / 20 mg per mL = 0.75 mL
Step 2: 0.75 mL x 100 = 75 units
Example 3: 15 mg from a 30 mg/mL vial
Step 1: 15 mg / 30 mg per mL = 0.5 mL
Step 2: 0.5 mL x 100 = 50 units
Example 4: 15 mg from a 40 mg/mL vial
Step 1: 15 mg / 40 mg per mL = 0.375 mL
Step 2: 0.375 mL x 100 = 37.5 units
Example 5: 15 mg from a 60 mg/mL vial
Step 1: 15 mg / 60 mg per mL = 0.25 mL
Step 2: 0.25 mL x 100 = 25 units
See the pattern? Higher concentration means fewer units. The relationship is inversely proportional. Double the concentration, halve the units. This same formula works for every peptide dosage calculation you will ever need.
If you want to skip the math entirely, the SeekPeptides peptide calculator does this conversion instantly. Enter your dose, enter your concentration, and it gives you the exact units to draw. For tirzepatide specifically, the compounded tirzepatide dosage calculator is built specifically for these conversions.
A quick sanity check method: if your calculated units seem unreasonably high (over 200) or unreasonably low (under 10), re-read your vial label and recalculate. Errors usually come from misreading the concentration. A vial labeled "20 mg/2 mL" is 10 mg/mL, not 20 mg/mL. A vial labeled "30 mg/vial" in a 3 mL vial is also 10 mg/mL. Always convert to mg/mL before plugging into the formula.
This formula applies identically to semaglutide conversions too. If you are curious about the math for that medication, our semaglutide dosage in units guide uses the same approach. The principle never changes, only the numbers do.
Drawing 15 mg from a 10 mg/mL vial
The 10 mg/mL concentration is the most widely dispensed formulation from compounding pharmacies. If you started tirzepatide at a lower dose and gradually worked up through the standard dose escalation, your pharmacy may still be sending you 10 mg/mL vials. At the 2.5 mg starting dose, that concentration works perfectly because you only need 25 units. At 5 mg, it is 50 units. At 10 mg, it is 100 units, which fills your syringe exactly.
But at 15 mg, you need 150 units. And that creates the overflow problem.
Here is the step-by-step protocol for drawing 15 mg from a 10 mg/mL vial using the split-dose method:
What you need:
Two insulin syringes (1 mL / 100 unit capacity, 29-31 gauge needle)
Alcohol swabs
Your 10 mg/mL tirzepatide vial
The process:
Clean the vial stopper with an alcohol swab. Let it dry for 10 seconds. Take your first syringe and draw 75 units of air into the barrel. Insert the needle through the vial stopper and push the air in (this equalizes pressure and makes drawing easier). Invert the vial, pull the plunger back slowly to the 75 unit mark, tap out any air bubbles, and adjust to exactly 75 units. Remove the syringe and set it aside on a clean surface with the cap on.
Take your second syringe and repeat the process. Draw 75 units of air, insert into the vial, push air in, invert, draw to 75 units, remove air bubbles, verify the measurement. Now you have two syringes, each containing 75 units (7.5 mg of tirzepatide).
Inject the first syringe at one site, such as the left side of the abdomen, at least 2 inches from the navel. Inject the second syringe at a different site, such as the right side of the abdomen. Keep the injection sites at least 2 inches apart. For complete injection site guidance, refer to our guide on where to inject GLP-1.
Is splitting the dose less effective than a single injection? No. The total amount of tirzepatide entering your body is identical: 15 mg. The absorption rate may differ slightly between sites, but the overall pharmacokinetic profile remains consistent. Clinical protocols for higher-dose peptide administration routinely use split injections when volume exceeds comfortable single-site limits.
One practical tip: draw both syringes before injecting either one. This ensures you get exactly 150 units total from the vial without worrying about leftover volume calculations mid-injection. If your vial contains exactly 30 mg (a common size for 10 mg/mL formulations), you get exactly two 15 mg doses. If it contains 50 mg, you get three full 15 mg doses plus 5 mg remaining. Track your vial usage carefully at this dose level, as the higher volume means your vials deplete faster. For storage guidance between uses, see our tirzepatide refrigeration guide.
Drawing 15 mg from a 20 mg/mL vial
At 20 mg/mL, everything gets simpler. Your 15 mg dose requires exactly 75 units, which is 0.75 mL. That fits comfortably within a standard 100 unit insulin syringe, leaving 25 units of unused capacity in the barrel. No splitting. No special equipment. Just one clean draw and one injection.
This is why 20 mg/mL is often called the sweet spot for higher tirzepatide doses. The 20 mg/mL dosing chart shows clean, round numbers at most dose levels: 12.5 units for 2.5 mg, 25 units for 5 mg, 50 units for 10 mg, and 75 units for 15 mg. Easy to read on a syringe. Easy to draw accurately.
Here is the drawing protocol:
Clean the vial stopper with alcohol. Draw 75 units of air into your syringe. Insert the needle through the stopper and push the air in. Invert the vial. Pull the plunger back slowly past the 75 unit line (draw a little extra). Tap the barrel firmly to move any air bubbles to the top near the needle. Push the plunger forward gently until the top of the plunger rubber sits exactly at 75 units. Remove the syringe from the vial.
Verify your measurement. On most insulin syringes, 75 units sits three-quarters of the way up the barrel. The major markings should show 10, 20, 30, 40, 50, 60, 70, 80, 90, 100. Your plunger should sit exactly on the midpoint between 70 and 80. Some syringes mark every 5 units, which makes 75 even easier to identify.
Inject at your chosen site. Subcutaneous injection in the abdomen is the most common choice, but the thigh and upper arm also work. Rotate your injection sites weekly to prevent injection site reactions and lipodystrophy. The abdominal injection technique guide covers proper site selection and rotation patterns.
A 20 mg/mL vial labeled as containing 40 mg total (which is 2 mL of solution) gives you two full 15 mg doses with 10 mg remaining. A 60 mg vial (3 mL) gives you four 15 mg doses. Track your remaining volume by noting how much you draw each time or by weighing the vial on a precision scale before and after draws.
Many of the pharmacies featured in our Empower tirzepatide dosage chart and Southend pharmacy tirzepatide guide offer 20 mg/mL formulations specifically for patients at higher dose levels. If you are currently using 10 mg/mL and finding the split-dose approach inconvenient, requesting a concentration change is a straightforward conversation with your provider.
Drawing 15 mg from 30 mg/mL, 40 mg/mL, or higher concentration vials
Higher concentrations dramatically reduce your injection volume. At 30 mg/mL, you draw 50 units. At 40 mg/mL, just 37.5 units. At 50 mg/mL, only 30 units. And at 60 mg/mL, a mere 25 units delivers your full 15 mg dose.
Small volumes come with a trade-off: precision becomes critical.
At 60 mg/mL, each unit on your syringe represents 0.6 mg of tirzepatide. Drawing 26 units instead of 25 means injecting 15.6 mg instead of 15 mg. That is a 4% overdose from a single-unit error. At 10 mg/mL, drawing one extra unit only adds 0.1 mg, which is 0.67% deviation. The higher the concentration, the more each unit matters.
For concentrations above 30 mg/mL, consider using a smaller syringe. A 0.5 mL syringe (50 unit capacity) with half-unit markings gives you significantly better resolution for small draws. The markings are larger and more spaced out, making it easier to see exactly where 37.5 units falls. Some 0.3 mL syringes mark every single unit, which is ideal for the very small draws at 50 mg/mL and 60 mg/mL concentrations.
The drawing technique for high-concentration vials is identical to any other draw, but take extra care with air bubbles. A single large bubble at 25 units occupies a much larger percentage of your total draw than it would at 75 units. Remove all visible bubbles before finalizing your measurement. Tap the barrel firmly, push air out, and redraw to your target line.
These higher concentrations are particularly popular with pharmacies like those mentioned in our compound tirzepatide dosing chart. If you have been escalating through the standard tirzepatide dosage chart and reached 15 mg, discuss higher-concentration options with your provider. The convenience of smaller injection volumes at the maximum dose is significant for long-term adherence.
One more detail for accuracy: always draw with the vial inverted and the needle tip fully submerged in the liquid. At higher concentrations with smaller total vial volumes, you may need to tilt the vial to ensure the needle stays submerged as the liquid level drops. Drawing air instead of liquid is a common mistake with partially used high-concentration vials.
What 15 mg of tirzepatide actually does in the body
Understanding why 15 mg matters helps put the unit conversion in context. This is not an arbitrary dose. It is the maximum FDA-approved maintenance dose of tirzepatide, and the one that produced the most dramatic results in clinical trials.
Tirzepatide is a dual GIP/GLP-1 receptor agonist. It activates both glucose-dependent insulinotropic polypeptide (GIP) receptors and glucagon-like peptide-1 (GLP-1) receptors simultaneously. This dual mechanism distinguishes it from single-receptor agonists like semaglutide, which targets only GLP-1 receptors. The combined activation produces synergistic effects on appetite suppression, insulin sensitivity, fat metabolism, and gastric emptying.
At 15 mg, these effects reach their peak intensity.
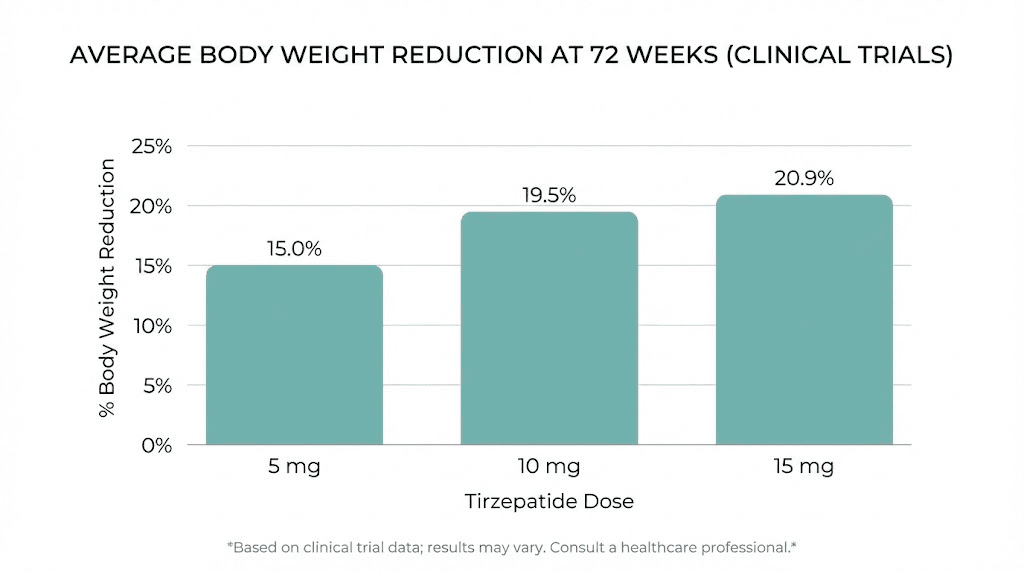
In the SURMOUNT-1 clinical trial, participants receiving 15 mg of tirzepatide weekly lost an average of 22.5% of their body weight over 72 weeks. For someone starting at 230 pounds, that translates to roughly 52 pounds of weight loss. By comparison, the 5 mg group lost 15%, and the 10 mg group lost 19.5%. The 15 mg dose delivered measurably superior results, confirming a clear dose-response relationship.
Even more striking, 57% of participants in the 15 mg group achieved a 20% or greater reduction in body weight. That level of weight loss was historically only achievable through bariatric surgery. Understanding these results helps explain why so many people work through the tirzepatide timeline to reach this maximum dose.
The appetite suppression at 15 mg is profound. Most users report dramatically reduced hunger and earlier satiety within the first few days after injection. This is GLP-1 receptor activation working on the hypothalamus and brainstem appetite centers. Many people at 15 mg report needing to set reminders to eat, as natural hunger signals become significantly diminished. For more on this phenomenon, our guide on tirzepatide appetite suppression timing covers the mechanism in detail.
Gastric emptying slows significantly at 15 mg. Food stays in the stomach longer, which contributes to the feeling of fullness but can also cause nausea, especially after large meals. This is why the tirzepatide foods to avoid list becomes particularly important at the maximum dose. High-fat, high-volume meals are the most likely to trigger nausea when gastric emptying is at its slowest.
Insulin sensitivity improvements at 15 mg are substantial. In the SURPASS trials (focused on type 2 diabetes), 15 mg of tirzepatide reduced HbA1c by up to 2.58 percentage points, bringing many participants to normal glycemic levels. Even for non-diabetic users, improved insulin sensitivity means better nutrient partitioning, reduced fat storage, and more stable energy throughout the day.
SeekPeptides members frequently discuss the difference between 10 mg and 15 mg in terms of practical experience. The consensus from the community is that the jump to 15 mg produces noticeable increases in appetite suppression and weight loss velocity, but also increases the likelihood and intensity of gastrointestinal side effects during the first 2-4 weeks at the new dose.
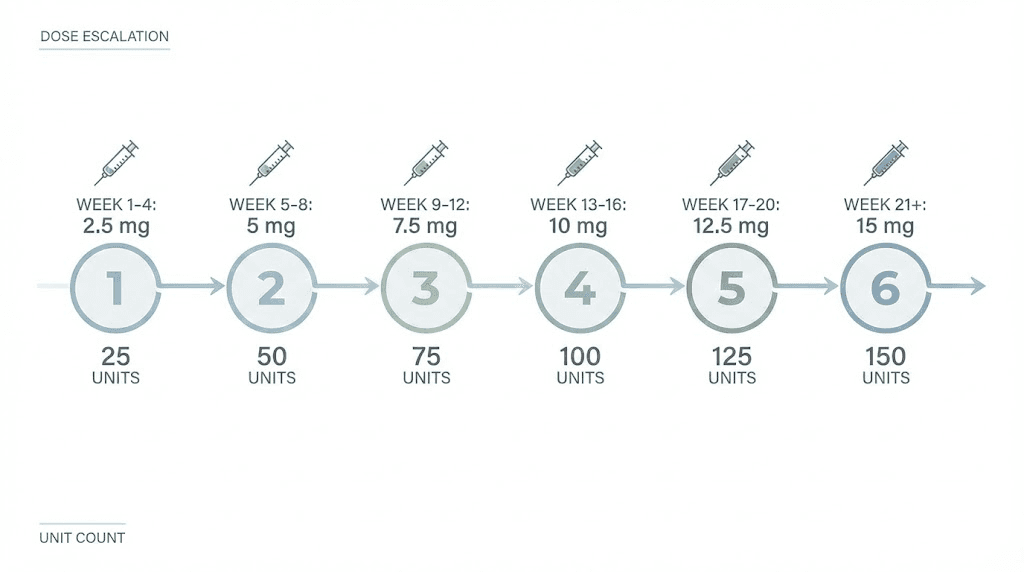
The dose escalation path to 15 mg
Nobody starts at 15 mg. The dose escalation protocol exists for good reason: it allows your body to adapt to the gastrointestinal effects of tirzepatide gradually, reducing the severity of nausea, diarrhea, and other common side effects that would be overwhelming at a full dose from day one.
The standard FDA-approved escalation follows this timeline:
Weeks 1-4: 2.5 mg weekly (unit conversion for 2.5 mg)
Weeks 5-8: 5 mg weekly (unit conversion for 5 mg)
Weeks 9-12: 7.5 mg weekly (unit conversion for 7.5 mg)
Weeks 13-16: 10 mg weekly (unit conversion for 10 mg)
Weeks 17-20: 12.5 mg weekly
Week 20+: 15 mg weekly (you are here)
That is a minimum of 20 weeks, nearly five months, before reaching the maximum dose. Some providers use a slower escalation schedule, spending 6-8 weeks at each dose level instead of 4. The slower approach reduces side effects further but extends the time to reach therapeutic maximum.
Not everyone needs to reach 15 mg. If you are seeing satisfactory weight loss results at 10 mg or 12.5 mg with tolerable side effects, there may be no clinical reason to escalate further. The general guidance is to increase the dose only when weight loss has plateaued at the current level and side effects are manageable. Our guide on tirzepatide not working anymore covers when a dose increase makes sense versus when other adjustments are more appropriate.
However, if you have worked through the full escalation and arrived at 15 mg, you are at the dose where clinical data shows the strongest outcomes. Commit to consistent weekly administration at this level for at least 8-12 weeks before evaluating whether the maximum dose is producing the results you need. Weight loss at 15 mg tends to accelerate compared to the initial lower-dose period, as the full pharmacological effect takes time to establish.
Some practitioners use microdosing approaches during the escalation to 15 mg, splitting the dose increase into smaller increments rather than jumping a full 2.5 mg at once. For example, moving from 12.5 mg to 13.75 mg for two weeks before reaching 15 mg. This can be helpful for individuals who experienced significant GI symptoms during earlier dose increases.
Side effects at the 15 mg dose level
Side effects at 15 mg are generally similar to those at lower doses, but they can be more pronounced, especially during the first 2-4 weeks after reaching the maximum dose. The SURMOUNT-1 trial reported a 6.2% treatment discontinuation rate in the 15 mg group due to adverse events, compared to 4.3% in the 5 mg group. That means the vast majority of participants, over 93%, tolerated the maximum dose well enough to continue treatment.
The most common side effects at 15 mg include:
Nausea. The most frequently reported side effect across all tirzepatide dose levels, and it tends to be most intense during dose escalation. At 15 mg, nausea typically peaks during the first 1-2 weeks at the new dose and gradually diminishes as your body adapts. Eating smaller, more frequent meals and avoiding high-fat foods helps significantly. Our guide on what to eat on tirzepatide provides specific meal strategies for managing GI symptoms.
Constipation. Slowed gastric motility at 15 mg can lead to constipation, particularly if fluid and fiber intake are inadequate. This side effect responds well to proactive management. Adequate hydration (at least 64 ounces of water daily), fiber supplementation, and regular physical activity are the first-line approaches. For persistent constipation, our tirzepatide constipation treatment guide covers pharmacological and lifestyle solutions.
Diarrhea. Somewhat paradoxically, diarrhea is also common at 15 mg, often alternating with constipation during the adjustment period. It typically resolves within 2-4 weeks. The tirzepatide diarrhea timeline article covers what to expect and when to seek medical attention.
Fatigue. Reduced caloric intake combined with metabolic changes can cause fatigue, especially at the maximum dose. This is partly a consequence of significant caloric restriction driven by reduced appetite, and partly a direct pharmacological effect. Many users find that adjusting their tirzepatide diet plan to include adequate protein and micronutrients helps maintain energy levels. The tirzepatide fatigue guide explores causes and solutions in depth.
Headaches. Some users report headaches at 15 mg, often related to dehydration or significant changes in eating patterns. Staying hydrated and maintaining consistent meal timing helps. See does tirzepatide cause headaches for detailed management strategies.
Injection site reactions. At higher volumes (particularly with 10 mg/mL concentration requiring 150 units), injection site redness, swelling, or itching may occur more frequently. Rotating injection sites and using proper technique minimizes these reactions. Consider supplements that support tirzepatide tolerance if side effects persist.
The important context is that most side effects are transient. They peak during dose escalation and diminish within a few weeks of stabilizing at 15 mg. The gastrointestinal system adapts. The body adjusts. And for the vast majority of users at 15 mg, the weight loss and metabolic benefits substantially outweigh the temporary discomfort of the adjustment period.
Common mistakes when measuring 15 mg
At the maximum dose, measurement errors carry the highest consequences. Here are the mistakes that catch people most often, and how to avoid every one of them.
Mistake 1: Using the wrong concentration in your calculation. This is the most dangerous error. If your pharmacy switches you from a 10 mg/mL vial to a 20 mg/mL vial and you do not notice, drawing the same number of units as before gives you double the intended dose. Always, always read the concentration on your current vial before drawing. Do not assume it matches your previous vial. If you receive a new shipment, verify the label before your next injection. This single habit prevents the most serious dosing errors.
Mistake 2: Confusing total vial content with concentration. A label that says "30 mg" might mean the vial contains 30 mg total at 10 mg/mL (3 mL of solution) or 30 mg per mL concentration. These are vastly different numbers. At 10 mg/mL, your 15 mg dose is 150 units. At 30 mg/mL, it is only 50 units. Triple-check whether the number on your label refers to total content or concentration. When in doubt, call your pharmacy.
Mistake 3: Drawing with the bevel facing down. When you insert the needle through the vial stopper and invert the vial, the needle bevel (the angled opening at the tip) should face upward, away from the bottom of the vial. Drawing with the bevel against the rubber stopper or vial glass can restrict flow and create air pockets that make accurate measurement difficult. This matters more at 15 mg because you are drawing a larger volume and any air contamination represents a dosing shortfall.
Mistake 4: Not removing air bubbles before measuring. Air bubbles take up space in the syringe barrel. A bubble occupying 5 units of space means you are injecting 5 fewer units of actual medication. At 75 units total (20 mg/mL), a 5-unit bubble means you are getting 70 units, which is only 14 mg instead of 15 mg. Tap the syringe barrel firmly to move bubbles to the top, push them out gently, then redraw to your target line.
Mistake 5: Reading the syringe at the wrong angle. Hold the syringe at eye level with the markings facing you. The plunger rubber has a slight dome shape. Read your measurement from the flat bottom edge of the rubber, not the top of the dome. Reading from the wrong edge can add or subtract 1-2 units from your intended draw, which matters at higher concentrations.
Mistake 6: Reusing the same syringe to draw twice for split doses. If you are splitting your 15 mg dose into two 75-unit draws from a 10 mg/mL vial, use two separate, fresh syringes. Reusing a syringe after injection introduces the possibility of contamination. The needle also dulls after the first use, making the second injection more painful and potentially less precise. Our peptide injections guide covers proper syringe handling in detail.
Mistake 7: Storing drawn syringes for later use. Some people draw their entire weekly dose in advance. While this is sometimes acceptable for short periods, tirzepatide stability in a drawn syringe is not the same as stability in the original vial. The peptide can adhere to the syringe walls, reducing the actual delivered dose. Draw and inject on the same day for maximum accuracy. For proper storage protocols, see our tirzepatide refrigeration requirements.
When 15 mg is too much (and what to do)
Not everyone thrives at the maximum dose. That is not a failure. It is information.
Signs that 15 mg may be too much include persistent nausea that does not improve after 4-6 weeks, unintended rapid weight loss exceeding 1-2% of body weight per week, severe fatigue that interferes with daily activities, or GI symptoms that significantly impact quality of life despite dietary modifications and supportive measures.
If you are experiencing intolerable side effects at 15 mg, the first step is not to stop tirzepatide entirely. Instead, discuss a dose reduction with your provider. Stepping back to 12.5 mg or even 10 mg often resolves the side effects while maintaining meaningful weight loss. The tirzepatide dosing for weight loss guide covers the full range of dose options and when each one makes sense.
Rapid weight loss at 15 mg also raises the question of muscle preservation. When caloric intake drops dramatically due to profound appetite suppression, the body can catabolize muscle tissue along with fat. This is why maintaining adequate protein intake (at least 1 gram per kilogram of goal body weight daily) is critical at the maximum dose. Our tirzepatide meal plan provides protein-prioritized meal structures specifically designed for the appetite challenges at higher doses.
Some people experience a phenomenon where 15 mg seems to stop working after several months. This is often called a plateau and typically is not true medication resistance. It usually reflects a new metabolic equilibrium where the body has adjusted to the lower caloric intake and weight loss rate has normalized. The guide on why you are not losing weight on tirzepatide addresses plateau-breaking strategies that do not require exceeding the maximum approved dose.
If you and your provider decide that tirzepatide is not the right fit at any dose, there are alternatives. Semaglutide works through a single GLP-1 receptor mechanism and some people tolerate it better. Newer agents like retatrutide add a third receptor (glucagon) and are being studied in clinical trials. And survodutide offers yet another dual-agonist profile with potentially different tolerability characteristics.
Storing your 15 mg tirzepatide properly
Proper storage preserves potency. At 15 mg per injection, each dose represents a significant investment, and degraded peptide from improper storage means reduced effectiveness that you will not notice until your results stall.
Keep your tirzepatide vial refrigerated between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius). This is the standard refrigerator temperature range. Place the vial upright in the main compartment, not in the door (which experiences temperature fluctuations) and not in the back near the cooling element (which can freeze the solution). Our tirzepatide storage guide covers optimal placement within your refrigerator.
Do not freeze tirzepatide. Freezing can cause the peptide to denature and form aggregates that reduce bioavailability and may cause injection site reactions. If your vial has been frozen accidentally, do not use it. Contact your pharmacy for a replacement.
Once punctured (after your first draw from the vial), most compounded tirzepatide formulations remain stable for 28-45 days when refrigerated properly. Check with your specific compounding pharmacy for their stability data, as formulations with different preservatives and excipients may have different shelf lives. At 15 mg per dose from a 10 mg/mL vial, a 30 mg vial gives you exactly two doses, meaning you will use the entire vial within two weeks, well within the stability window.
Traveling with tirzepatide at 15 mg requires an insulated carrying case with cold packs. The guide on tirzepatide out of the fridge details how long the peptide can remain unrefrigerated without significant potency loss. For travel periods exceeding 48 hours without refrigeration access, discuss alternative arrangements with your provider.
If you are also considering how tirzepatide interacts with other compounds, the community at SeekPeptides has extensive discussions on tirzepatide with B12, tirzepatide with glycine, and other common combinations at the 15 mg dose level.
Comparing 15 mg to other tirzepatide dose levels
Seeing how 15 mg stacks up against lower doses provides useful context for understanding where you sit in the dosing landscape and what changes you can expect compared to your previous dose level.
Dose | Units at 10 mg/mL | Units at 20 mg/mL | Units at 30 mg/mL | Avg weight loss (SURMOUNT-1) |
|---|---|---|---|---|
2.5 mg | 25 units | 12.5 units | 8.3 units | N/A (initiation dose) |
5 mg | 50 units | 25 units | 16.7 units | 15% body weight |
7.5 mg | 75 units | 37.5 units | 25 units | N/A (escalation dose) |
10 mg | 100 units | 50 units | 33.3 units | 19.5% body weight |
12.5 mg | 125 units | 62.5 units | 41.7 units | N/A (escalation dose) |
15 mg | 150 units | 75 units | 50 units | 22.5% body weight |
The jump from 10 mg to 15 mg represents a 50% dose increase. From the 10 mg level, where you needed 50 units at 20 mg/mL, you now need 75 units at the same concentration. That additional 25 units carries 5 extra milligrams of active peptide, and those 5 mg produce a measurable difference in both weight loss velocity and appetite suppression.
For researchers comparing tirzepatide to semaglutide at equivalent therapeutic levels, the semaglutide vs tirzepatide dosage chart provides a side-by-side comparison. The maximum semaglutide dose (2.4 mg for weight management) does not directly equate to 15 mg of tirzepatide in terms of milligrams, but the clinical outcomes can be compared. The conversion chart between the two medications helps those transitioning between them understand the dosing relationship.
If you have been tracking your results at each dose level, you may notice that the weight loss per milligram of dose increase is not linear. The jump from 2.5 mg to 5 mg (doubling the dose) produces less absolute weight loss than you might expect, while the jump from 10 mg to 15 mg (a 50% increase) can produce proportionally larger changes. This reflects the pharmacological curve of receptor saturation, where higher doses activate an increasing proportion of available receptors, producing progressively stronger effects until the receptors approach full saturation.
Those considering alternative dosing approaches at 15 mg, such as splitting the weekly dose into two half-doses given every 3-4 days, should consult the tirzepatide microdosing schedule for detailed protocols. Some practitioners believe that more frequent, smaller doses can smooth out side effects while maintaining efficacy, though clinical trial data supports the standard once-weekly protocol.
Practical tips for long-term success at 15 mg
Reaching 15 mg is a milestone. Staying there productively requires a few habits that become second nature after the first month.
Same day, same time, every week. Consistency in your injection schedule maintains steady blood levels of tirzepatide. Pick a day and a time, and stick to it. If you need to adjust by a day or two occasionally, that is fine, but avoid regularly shifting your injection day. For guidance on timing flexibility, see whether you can take tirzepatide a day early.
Eat enough protein. At 15 mg, your appetite suppression is at maximum. The temptation is to eat very little because you simply do not feel hungry. But inadequate protein intake at this dose level leads to muscle loss, fatigue, hair thinning, and reduced metabolic rate. Aim for at least 100-120 grams of protein daily, even when you do not feel like eating. The tirzepatide diet plan and food recommendations for GLP-1 medications provide structured approaches to hitting your macros despite reduced appetite.
Hydrate aggressively. Reduced food intake means reduced water intake from food. Combine that with potential GI effects (diarrhea or vomiting), and dehydration becomes a real risk at 15 mg. Aim for at least 80-100 ounces of water daily. Add electrolytes if you experience lightheadedness or muscle cramps.
Monitor for nutrient deficiencies. Long-term use of 15 mg tirzepatide with significantly reduced food intake can lead to deficiencies in B vitamins, iron, calcium, and vitamin D. Regular blood work every 3-6 months helps catch deficiencies early. Many users at this dose level take a daily multivitamin plus additional B12 supplementation. The supplements to take with tirzepatide guide covers the most important additions for users at the maximum dose.
Track your injections and vial usage. At 15 mg, you go through vials faster than at any other dose. A simple log noting the date, vial number, units drawn, and remaining volume prevents the frustrating situation of reaching injection day with an empty vial and no refill ready. Many users keep this log in a notes app or a simple spreadsheet.
Keep your provider in the loop. Regular check-ins with your prescribing provider are especially important at the maximum dose. Report any new or worsening symptoms, share your weight loss progress, and discuss whether 15 mg remains the appropriate dose for your situation. Some people eventually step back to 10 mg or 12.5 mg for maintenance after achieving their weight loss goals. Others stay at 15 mg indefinitely. The right answer depends on your individual response and your provider professional guidance.
For researchers navigating the broader landscape of GLP-1 peptides, SeekPeptides offers comprehensive protocols, dosing calculators, and community support that goes well beyond what any single blog post can cover. Members access personalized guidance for every dose level, from the initial 2.5 mg through the maximum 15 mg and beyond.
How 15 mg tirzepatide compares to other GLP-1 medications
At the maximum dose of tirzepatide, you are using what many researchers consider the most effective weight management peptide currently available. But how does it compare to the alternatives?
Tirzepatide 15 mg vs semaglutide 2.4 mg: The SURMOUNT-4 head-to-head trial showed that tirzepatide at its maximum dose produced greater average weight loss than semaglutide at its maximum dose. The dual GIP/GLP-1 mechanism of tirzepatide appears to provide additional metabolic benefits beyond what GLP-1 activation alone can deliver. The side effect profiles are broadly similar, though individual tolerance varies.
Tirzepatide 15 mg vs retatrutide: Retatrutide, a triple agonist (GIP/GLP-1/glucagon), is still in clinical trials and not yet FDA-approved. Early data from the trial program shows impressive weight loss results that rival or exceed tirzepatide at maximum doses. Our retatrutide comparison guides track the latest trial data as it becomes available. For those interested in the retatrutide dosing framework, the retatrutide dosage chart provides the current research protocols.
Tirzepatide 15 mg vs cagrilintide/semaglutide (CagriSema): The combination of cagrilintide and semaglutide adds amylin receptor agonism to GLP-1 activation. Phase 3 trial results show competitive weight loss numbers. The CagriSema vs tirzepatide comparison breaks down how these two maximum-dose regimens compare across efficacy, tolerability, and practical considerations.
Tirzepatide 15 mg vs oral alternatives: For those who prefer non-injectable options, oral tirzepatide is in development. The oral vs injection comparison explores the bioavailability differences and what oral dosing at equivalent efficacy levels might look like. Currently, tablet formulations require significantly higher milligram doses to achieve the same blood levels as injectable tirzepatide.
Regardless of which medication you use, the principles of accurate dosing, proper storage, consistent administration, and adequate nutrition remain the same. The peptide dosing guide covers these universal principles in depth.
Reconstitution considerations for 15 mg dosing
If you receive tirzepatide as a lyophilized powder (a freeze-dried cake in a vial), you need to reconstitute it before drawing your dose. The amount of bacteriostatic water you add determines the final concentration, which then determines how many units equal 15 mg.
This is where many people introduce errors. The powder itself has a fixed amount of tirzepatide (for example, 30 mg or 60 mg in the vial). The concentration you create depends entirely on how much water you add.
Here are common reconstitution scenarios for a 30 mg vial:
Add 1 mL of bac water = 30 mg/mL concentration. For 15 mg, draw 50 units.
Add 1.5 mL of bac water = 20 mg/mL concentration. For 15 mg, draw 75 units.
Add 2 mL of bac water = 15 mg/mL concentration. For 15 mg, draw 100 units.
Add 3 mL of bac water = 10 mg/mL concentration. For 15 mg, draw 150 units.
For a 60 mg vial:
Add 2 mL of bac water = 30 mg/mL concentration. For 15 mg, draw 50 units.
Add 3 mL of bac water = 20 mg/mL concentration. For 15 mg, draw 75 units.
Add 6 mL of bac water = 10 mg/mL concentration. For 15 mg, draw 150 units.
The tirzepatide reconstitution guide walks through the complete process step by step, including how to add water to the vial without damaging the peptide and how to mix without creating bubbles. The reconstitution chart provides a quick-reference table for multiple vial sizes and water volumes.
For users at 15 mg, a practical tip: if you are reconstituting your own vials, choose a water volume that produces a concentration where 15 mg translates to a convenient number of units. Adding 1.5 mL to a 30 mg vial gives you 20 mg/mL, meaning 15 mg = 75 units. That is an easy number to draw on a standard syringe, and the vial gives you exactly two 15 mg doses. Clean, simple, no waste.
If you are mixing with bacteriostatic water for the first time, our peptide mixing guide covers the general principles that apply to all reconstituted peptides, and the bacteriostatic water guide for tirzepatide addresses the specific considerations for this peptide.
The peptide reconstitution calculator on SeekPeptides automates this entire calculation. Enter your total peptide amount, enter how much water you added, and it tells you the resulting concentration and the exact units for any dose. Bookmark it. Use it every time you reconstitute.
Frequently asked questions
Is 15 mg the highest dose of tirzepatide available?
Yes, 15 mg is the maximum FDA-approved dose for both Mounjaro (diabetes) and Zepbound (weight management). This dose produced the strongest weight loss results in clinical trials, with participants losing an average of 22.5% of body weight over 72 weeks. While some compounding pharmacies may technically be able to prepare higher doses, the clinical safety data supports the 15 mg ceiling. See our tirzepatide dosing for weight loss guide for the complete approved dose range.
Can I use a regular insulin syringe for 15 mg at 10 mg/mL?
No. A standard insulin syringe holds 100 units (1 mL), and 15 mg at 10 mg/mL requires 150 units (1.5 mL). You either need to split the dose into two separate 75-unit injections using two syringes, use a larger syringe (like a 3 mL syringe), or switch to a higher concentration vial. The tirzepatide syringe dosage guide covers syringe selection in detail.
What happens if I accidentally draw too much?
If you notice the error before injecting, simply push the plunger forward to expel the excess and adjust to your correct dose. If you have already injected a dose higher than intended, monitor for increased side effects (particularly nausea and GI symptoms) and contact your healthcare provider. A single accidental overdose is unlikely to cause serious harm, but your provider should be aware. Review the peptide safety guide for general safety protocols.
How long does the 15 mg dose last in the body?
Tirzepatide has a half-life of approximately 5 days. After injecting 15 mg, the medication level in your blood peaks around 24-48 hours post-injection and then gradually declines over the following week. By day 7, when your next dose is due, approximately 50% of the previous dose has been cleared. This pharmacokinetic profile supports the once-weekly dosing schedule. The tirzepatide timeline guide covers how the effects play out over the week.
Should I switch to 15 mg if 10 mg stopped working?
A weight loss plateau at 10 mg does not automatically mean you need 15 mg. Plateaus can result from metabolic adaptation, dietary drift (gradually eating more without realizing it), reduced physical activity, or reaching a new set point. Before escalating, review your nutrition, exercise, and adherence. If you have genuinely optimized all other variables and your provider agrees, a dose increase to 12.5 mg and then 15 mg is a reasonable next step. Our tirzepatide plateau troubleshooting guide helps distinguish between true plateaus and correctable factors.
Can I split 15 mg into smaller doses throughout the week?
Some practitioners experiment with splitting the 15 mg weekly dose into two injections of 7.5 mg given 3-4 days apart. The theory is that smaller, more frequent doses reduce peak blood levels and minimize side effects while maintaining overall efficacy. This is an off-label approach without strong clinical trial support, but anecdotal reports from the research community suggest some people tolerate the split-dose protocol better. Discuss this option with your provider before changing your administration schedule. The microdosing schedule covers alternative dosing strategies.
How do I know my vial concentration if the label is unclear?
If your vial label lists total content (like "30 mg") without explicitly stating the concentration, you need to know the total volume of solution in the vial. Divide the total milligrams by the total milliliters: 30 mg in 3 mL = 10 mg/mL, while 30 mg in 1.5 mL = 20 mg/mL. If you cannot determine the concentration from the label, contact your compounding pharmacy directly before drawing any medication. Never guess your concentration at the 15 mg dose level, as the volume differences between concentrations are significant.
What if I am switching from semaglutide to 15 mg tirzepatide?
Switching from semaglutide to tirzepatide requires careful dose mapping because the two medications are not milligram-equivalent. A patient on maximum-dose semaglutide (2.4 mg weekly) does not typically start tirzepatide at 15 mg. Most providers begin the transition at 2.5 mg or 5 mg of tirzepatide and escalate from there. The semaglutide to tirzepatide switching guide provides detailed transition protocols, including timing considerations and dose mapping between the two medications.
External resources
For researchers serious about optimizing their tirzepatide protocols at every dose level, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, dosing calculators, and a community of thousands who have navigated these exact questions from first injection through maximum dose.
In case I do not see you, good afternoon, good evening, and good night. May your calculations stay accurate, your injections stay comfortable, and your results at 15 mg stay consistent.