Feb 8, 2026

You are drawing up exactly 20 units on your insulin syringe. The liquid fills to that familiar line. But here is the question that stops thousands of researchers every single week: how many milligrams of tirzepatide did you just pull into that syringe?
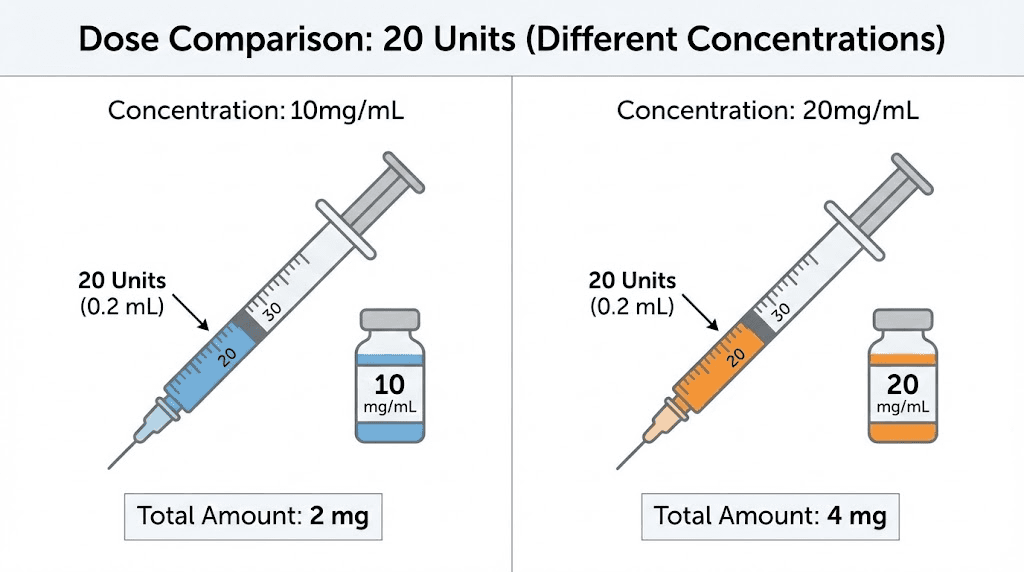
The answer is not as simple as you might hope. It depends entirely on one critical variable that changes everything, the concentration printed on your vial. Get this wrong, and you could be taking half the dose you intended. Or double it. A 10 mg/mL vial means 20 units equals 2 mg. A 20 mg/mL vial means those same 20 units deliver 4 mg. Same syringe line. Same 20 units. Completely different doses. This is the conversion problem that confuses people using compounded tirzepatide dosing in units, and getting it wrong has real consequences for results, side effects, and safety. SeekPeptides has helped thousands of researchers navigate these exact calculations, and this guide breaks down every concentration, every conversion, and every scenario you might encounter.
This guide covers the complete conversion math for 20 units across every common tirzepatide concentration. You will find step-by-step formulas, reference charts, real-world examples, and the most common mistakes that lead to dosing errors. Whether you are working with a 5 mg/mL, 10 mg/mL, 15 mg/mL, or 20 mg/mL vial, you will know exactly what 20 units means in milligrams before you finish reading.
Why 20 units does not equal a fixed number of milligrams
This is the single most important concept in tirzepatide dosing, and it trips up even experienced researchers. Units on a syringe measure volume. Milligrams measure the amount of active compound. These are two completely different things.
Think of it this way.
A standard U-100 insulin syringe treats 100 units as 1 mL of liquid. So 20 units equals exactly 0.2 mL. Every time. Regardless of what is dissolved in that liquid. The syringe does not know or care what compound you have loaded into it, it only measures how much liquid you have drawn up.
The milligram content hiding inside those 0.2 mL depends entirely on concentration. A vial labeled 10 mg/mL contains 10 milligrams of tirzepatide in every milliliter. A vial labeled 20 mg/mL packs twice as much compound into the same volume. So your 20 units, your 0.2 mL of liquid, could contain anywhere from 1 mg to 4 mg or more depending on what your compounding pharmacy put in the vial.
This is fundamentally different from brand-name Mounjaro or Zepbound, where the tirzepatide dose comes preloaded in a pen at a fixed concentration. With compounded tirzepatide, you are responsible for the conversion math. And the math must be right.
The universal conversion formula
Every tirzepatide unit-to-milligram conversion uses the same two-step formula. Learn this once, and you can calculate any dose at any concentration for the rest of your research.
Step 1: convert units to milliliters
On a standard U-100 syringe, 100 units equals 1 mL. So the conversion is straightforward.
mL = units / 100
For 20 units: 20 / 100 = 0.2 mL
This step never changes. Twenty units always equals 0.2 mL on a U-100 syringe.
Step 2: multiply by your vial concentration
Now take those 0.2 mL and multiply by the mg/mL number on your vial label.
mg = mL x concentration (mg/mL)
For a 10 mg/mL vial: 0.2 x 10 = 2 mg
For a 20 mg/mL vial: 0.2 x 20 = 4 mg
Two numbers. Two steps. That is all it takes. But let us walk through every common concentration so you have a complete reference. Understanding how to properly calculate your peptide dosages is essential for safe and effective research protocols. You can also use the SeekPeptides peptide calculator to verify these numbers instantly.
20 units at every common tirzepatide concentration
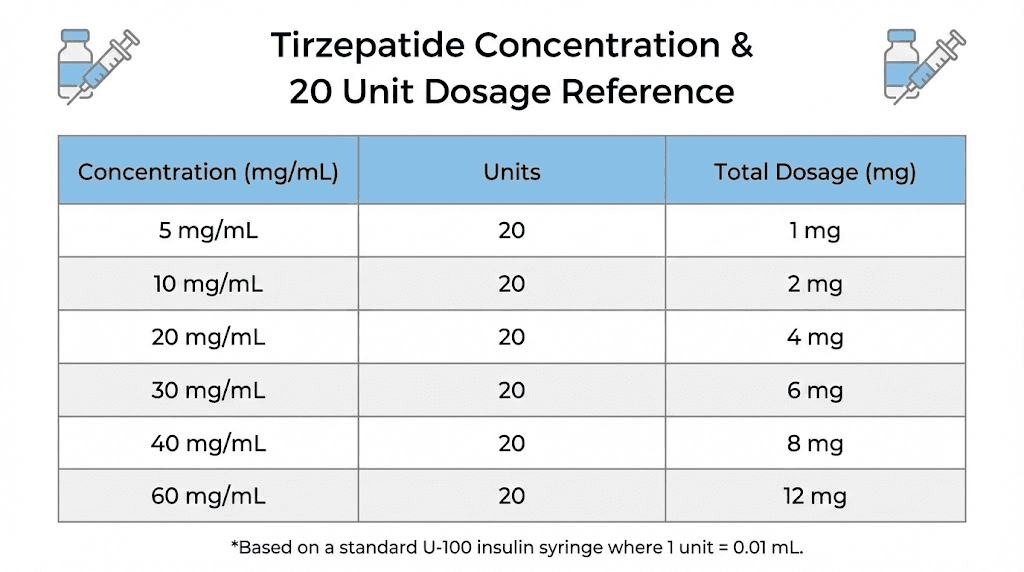
Compounded tirzepatide comes in several different concentrations depending on the pharmacy. Here is exactly what 20 units delivers at each one. Knowing the tirzepatide dosage in units for your specific concentration prevents costly errors.
5 mg/mL concentration
This is a lower concentration sometimes used for precise microdosing protocols.
20 units = 0.2 mL x 5 mg/mL = 1.0 mg
At this concentration, 20 units delivers just 1 milligram of tirzepatide. That is well below the standard starting dose of 2.5 mg, making this concentration useful for microdosing tirzepatide protocols where you need granular control over small amounts.
10 mg/mL concentration
This is one of the most commonly used concentrations from compounding pharmacies. Many researchers start here.
20 units = 0.2 mL x 10 mg/mL = 2.0 mg
Twenty units at 10 mg/mL gives you exactly 2.0 milligrams. This is slightly below the standard starting dose of 2.5 mg (which would require 25 units at this concentration). If your provider prescribed 2.5 mg, you need to draw up to 25 units, not 20. This distinction matters, as understanding how many units equals 2.5 mg of tirzepatide is one of the most common questions researchers ask.
15 mg/mL concentration
Higher concentration vials are common for researchers on escalated doses who want smaller injection volumes.
20 units = 0.2 mL x 15 mg/mL = 3.0 mg
At 15 mg/mL, 20 units delivers 3.0 milligrams. This falls between the 2.5 mg starting dose and the 5 mg escalation dose on the standard tirzepatide dose chart. Some researchers use this as an intermediate step-up dose during their first month.
20 mg/mL concentration
This is the highest commonly available concentration, designed for researchers on higher maintenance doses.
20 units = 0.2 mL x 20 mg/mL = 4.0 mg
At this concentration, 20 units packs 4.0 milligrams into just 0.2 mL of liquid. If you previously used a 10 mg/mL vial and switched to 20 mg/mL without adjusting your unit count, you just doubled your dose. This is one of the most dangerous mistakes in compounded tirzepatide use, and it happens more often than most people realize.
Quick reference table: 20 units across all concentrations
Vial concentration | 20 units (mL) | Milligrams delivered | Clinical context |
|---|---|---|---|
5 mg/mL | 0.2 mL | 1.0 mg | Sub-therapeutic microdose |
8 mg/mL | 0.2 mL | 1.6 mg | Low microdose |
10 mg/mL | 0.2 mL | 2.0 mg | Just below starting dose |
12 mg/mL | 0.2 mL | 2.4 mg | Near starting dose |
15 mg/mL | 0.2 mL | 3.0 mg | Between 2.5 and 5 mg dose |
20 mg/mL | 0.2 mL | 4.0 mg | Between 2.5 and 5 mg dose |
30 mg/mL | 0.2 mL | 6.0 mg | Above 5 mg dose tier |
40 mg/mL | 0.2 mL | 8.0 mg | Between 7.5 and 10 mg dose |
50 mg/mL | 0.2 mL | 10.0 mg | Equals 10 mg dose tier |
60 mg/mL | 0.2 mL | 12.0 mg | Between 10 and 12.5 mg dose |
The pattern is clear. Every 1 mg/mL increase in concentration adds 0.2 mg to your 20-unit dose. At the lower concentrations, 20 units barely registers. At the higher end, 20 units delivers a substantial dose. Your vial label is the only thing that determines which scenario you are in.
Understanding insulin syringe markings
Before we go further into conversion math, you need to understand the tool you are measuring with. Insulin syringes are not complicated, but they can be confusing if nobody has explained how the markings actually work.
The U-100 standard
Nearly every insulin syringe used for peptide injections is a U-100 syringe. The U-100 designation means the syringe is calibrated so that 100 units equals 1 mL of liquid. This standardization dates back to insulin dosing conventions, where 100 units of insulin were dissolved in 1 mL.
For tirzepatide dosing, this means the unit markings on your syringe are purely a volume measurement. Each unit equals 0.01 mL. Ten units equals 0.1 mL. Twenty units equals 0.2 mL. Simple division.
Common syringe sizes
Insulin syringes come in three standard sizes, and each one has different marking intervals. Using the right syringe for your dose volume matters for accuracy.
0.3 mL syringe (30 units max): Each small line represents 1 unit. This is the most precise option for doses under 30 units. For 20 units of tirzepatide, this syringe gives you the clearest markings and easiest reading. Numbered markings appear at 5, 10, 15, 20, 25, and 30.
0.5 mL syringe (50 units max): Each small line represents 1 unit on most models. Good for doses up to 50 units. Still offers clear precision for a 20-unit dose. Numbered markings typically appear at every 5 or 10 units.
1.0 mL syringe (100 units max): Each small line represents 2 units. This means you cannot easily dose odd numbers like 21 or 23 units. For a 20-unit dose, this works fine since 20 falls on an even marking. But for doses requiring single-unit precision, the smaller syringes are better. Knowing the right tools is just as important as understanding peptide dosing calculations.
Reading the meniscus
When you draw liquid into a syringe, the surface curves slightly at the edges. This curve is called the meniscus. Always read the dose at the bottom of the meniscus, not the top of the curve. Reading from the top can add 1-2 units of error, which at higher concentrations could mean a meaningful difference in milligrams.
Hold the syringe at eye level. Look straight across, not from above or below. The bottom of the curved surface should align exactly with your target marking. This technique applies to every peptide reconstitution and dosing measurement.
How 20 units compares to standard tirzepatide dose tiers
Tirzepatide follows a structured dose escalation schedule. Understanding where 20 units falls relative to these standard doses helps you contextualize your research protocol. The FDA-approved dosing for brand-name tirzepatide (Mounjaro and Zepbound) follows specific tiers designed around clinical trial data from the SURMOUNT and SURPASS programs.
Standard tirzepatide dose tiers
The clinical dose escalation ladder looks like this:
Dose tier | Weekly dose | Duration | Purpose |
|---|---|---|---|
Starting | 2.5 mg | 4 weeks | Tolerance assessment |
First escalation | 5.0 mg | 4+ weeks | Therapeutic entry |
Second escalation | 7.5 mg | 4+ weeks | Enhanced effect |
Third escalation | 10.0 mg | 4+ weeks | Full therapeutic dose |
Fourth escalation | 12.5 mg | 4+ weeks | Higher therapeutic dose |
Maximum | 15.0 mg | Ongoing | Maximum approved dose |
In the landmark SURMOUNT-1 trial, participants taking 15 mg weekly achieved an average weight loss of 22.5% of body weight over 72 weeks. The 10 mg group lost approximately 21.4%, and even the 5 mg group achieved 15% average weight loss. These results far exceeded what previous weight loss peptides had demonstrated in clinical settings.
Where 20 units lands at each concentration
Now let us map 20 units back to these dose tiers based on concentration.
At 10 mg/mL, your 20 units delivers 2.0 mg. That is below the starting dose. You would need 25 units to reach the 2.5 mg starting tier.
At 15 mg/mL, your 20 units delivers 3.0 mg. That sits between the 2.5 mg starter and the 5.0 mg first escalation. Some researchers use this as a gradual step-up rather than jumping from 2.5 to 5.0 mg.
At 20 mg/mL, your 20 units delivers 4.0 mg. Again between tiers, this gives a moderate dose that some find produces fewer gastrointestinal side effects than a full 5.0 mg jump. Understanding tirzepatide side effects like fatigue helps researchers adjust their dose escalation strategy.
At 30 mg/mL, your 20 units delivers 6.0 mg. This exceeds the 5.0 mg tier and approaches the 7.5 mg level, a meaningful therapeutic dose.
The takeaway is clear. Twenty units is not a dose. It is a volume. The dose depends on what you put in the syringe.
Complete conversion charts for every standard dose
While we are focused on 20 units, let us give you the full picture. Here are complete conversion charts for the two most common concentrations, so you can look up any dose instantly. These charts work the same way as the tirzepatide vs semaglutide dosage chart comparisons, giving you exact numbers rather than approximations.
10 mg/mL conversion chart
Desired dose (mg) | Volume (mL) | Syringe units | Dose tier |
|---|---|---|---|
1.0 mg | 0.10 mL | 10 units | Microdose |
1.25 mg | 0.125 mL | 12.5 units | Half starting dose |
1.5 mg | 0.15 mL | 15 units | Microdose |
2.0 mg | 0.20 mL | 20 units | Below starting dose |
2.5 mg | 0.25 mL | 25 units | Standard starting dose |
3.0 mg | 0.30 mL | 30 units | Between tiers |
3.75 mg | 0.375 mL | 37.5 units | Between tiers |
5.0 mg | 0.50 mL | 50 units | First escalation |
7.5 mg | 0.75 mL | 75 units | Second escalation |
10.0 mg | 1.00 mL | 100 units | Third escalation (full syringe) |
Notice that at 10 mg/mL, the 10.0 mg dose fills an entire 1 mL syringe. This is why many pharmacies offer higher concentrations for researchers who advance beyond 10 mg, as the injection volume becomes impractical.
20 mg/mL conversion chart
Desired dose (mg) | Volume (mL) | Syringe units | Dose tier |
|---|---|---|---|
1.0 mg | 0.05 mL | 5 units | Microdose |
2.0 mg | 0.10 mL | 10 units | Below starting dose |
2.5 mg | 0.125 mL | 12.5 units | Standard starting dose |
4.0 mg | 0.20 mL | 20 units | Between tiers |
5.0 mg | 0.25 mL | 25 units | First escalation |
7.5 mg | 0.375 mL | 37.5 units | Second escalation |
10.0 mg | 0.50 mL | 50 units | Third escalation |
12.5 mg | 0.625 mL | 62.5 units | Fourth escalation |
15.0 mg | 0.75 mL | 75 units | Maximum dose |
At 20 mg/mL, even the maximum 15 mg dose only requires 75 units, well within a single 1 mL syringe. This convenience is exactly why higher concentrations exist. They allow tirzepatide dosing for weight loss in units to stay manageable regardless of your dose tier.
Why concentration matters more than you think
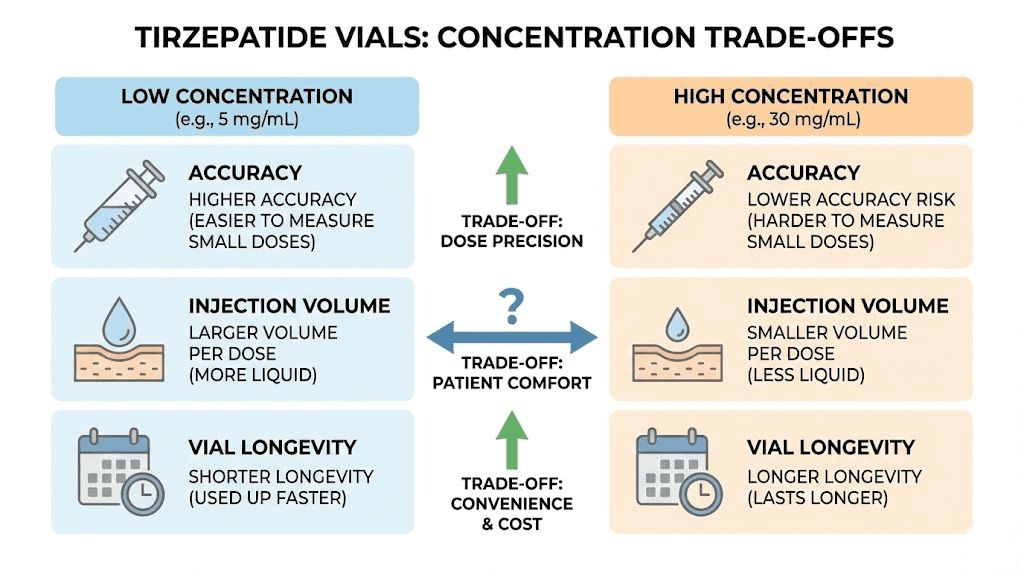
The concentration of your tirzepatide vial affects far more than just unit-to-mg math. It impacts accuracy, injection comfort, vial longevity, and even how well the peptide works. Understanding these factors helps you make better decisions about your peptide cycle planning.
Accuracy at different concentrations
Lower concentrations require larger volumes for the same dose. This is actually beneficial for accuracy. When your dose requires 50 units versus 12.5 units, you have far more room for error in the smaller measurement.
Consider the 2.5 mg starting dose. At 10 mg/mL, you draw 25 units. That is a clearly marked line on any syringe, easy to read, hard to mess up. At 20 mg/mL, the same dose requires 12.5 units. On a 1 mL syringe where each line represents 2 units, you are trying to stop precisely between the 12 and 14 unit marks. That is a recipe for imprecision.
For researchers who prioritize accuracy at lower doses, a lower concentration paired with a smaller syringe offers the best precision. The 0.3 mL syringe with 1-unit markings, combined with a 10 mg/mL concentration, lets you hit exact doses with confidence.
Injection volume and comfort
Every person who has injected peptides knows that volume matters for comfort. A 0.2 mL injection barely registers. A 1.0 mL injection can leave a noticeable lump under the skin that takes longer to absorb and may cause more injection site discomfort.
This is why concentration escalation often follows dose escalation. Researchers who start at 2.5 mg with a 10 mg/mL vial (25 units, comfortable) may switch to 20 mg/mL when they reach higher doses, keeping the injection volume manageable. At 10 mg on a 10 mg/mL vial, you would need 100 units, a full 1 mL syringe. At 20 mg/mL, the same dose requires only 50 units, half the volume and significantly more comfortable. Proper injection technique also plays a role in minimizing discomfort.
Vial longevity
Higher concentrations pack more total drug into the same vial volume, which means fewer vials needed over time. A 5 mL vial at 10 mg/mL contains 50 mg total. The same 5 mL vial at 20 mg/mL contains 100 mg total. If you are on a 10 mg weekly dose, the first vial lasts 5 weeks while the second lasts 10 weeks.
This directly impacts cost and convenience. Fewer vials means fewer pharmacy visits, fewer shipping charges, and less overall handling. But it also means each measurement error at higher concentrations costs you more milligrams of compound. Understanding how long tirzepatide lasts in the fridge becomes critical when your vial needs to remain potent for 10 or more weeks.
The most common conversion mistakes and how to avoid them
Dosing errors with compounded tirzepatide are alarmingly common. A case report published in Cureus documented a 39-year-old man who was hospitalized in the ICU after an unsupervised dose escalation led to severe hypoglycemia, organ dysfunction, and respiratory failure. While that case involved more than simple unit conversion errors, it illustrates how seriously wrong things can go when dosing mistakes compound.
Here are the five mistakes researchers make most often. Each one can be prevented with awareness and a simple verification process.
Mistake 1: assuming units equal milligrams
This is the most dangerous misconception. Someone reads that the starting dose is 2.5 mg and draws up 2.5 units, thinking units and milligrams are the same thing. At 10 mg/mL, 2.5 units is only 0.025 mL, which delivers a mere 0.25 mg of tirzepatide. That is one-tenth of the intended dose.
The reverse is equally dangerous. Someone told to take "25 units" assumes that means 25 mg. It does not. At 10 mg/mL, 25 units is 2.5 mg. The 25 mg dose would require 250 units (2.5 mL), far beyond what a standard syringe can hold and far beyond any safe dose.
Units are volume. Milligrams are mass. They are different measurements.
Mistake 2: not checking concentration when switching vials
You have been drawing 25 units from a 10 mg/mL vial for months. That gives you exactly 2.5 mg. Then your pharmacy sends a 20 mg/mL vial. You draw 25 units out of habit. You just injected 5 mg, double your intended dose, without realizing it.
This happens frequently when pharmacies change suppliers, when insurance changes, or when compounding pharmacies adjust their formulations. Always, always check the concentration label on every new vial before drawing your dose. The common peptide mistakes guide covers this and other critical errors to watch for.
Mistake 3: using the wrong syringe type
Not all syringes are U-100. Some specialty syringes use different scales. If you accidentally use a U-40 syringe (designed for U-40 insulin), the unit markings represent a different volume. Twenty units on a U-40 syringe equals 0.5 mL, not 0.2 mL. At 10 mg/mL, that delivers 5 mg instead of 2 mg.
Always verify that your syringe is labeled U-100 before performing any conversion calculations. The barrel should clearly state "U-100" or show 100 units at the 1 mL mark.
Mistake 4: confusing total vial content with concentration
A vial might say "30 mg/3 mL" on the label. Some researchers see "30 mg" and think the concentration is 30 mg/mL. It is not. Thirty milligrams divided by 3 milliliters equals 10 mg/mL. The total content (30 mg) and the concentration (10 mg/mL) are fundamentally different numbers.
Always look for the per-milliliter concentration, written as "mg/mL." If the label only shows total content and total volume, divide them yourself. Total mg divided by total mL equals your working concentration.
Mistake 5: rounding doses on imprecise syringes
On a 1 mL (100-unit) syringe, each small marking represents 2 units. If your calculated dose is 12.5 units, you cannot precisely measure this on a 100-unit syringe. You will either round down to 12 or up to 14, creating a 0.5-unit error.
At 20 mg/mL, that 0.5-unit difference equals 0.1 mg of tirzepatide. Across a 4-week dosing period, that is a cumulative 0.4 mg difference. Not catastrophic, but not ideal either.
The solution is simple. Use a 0.3 mL or 0.5 mL syringe with 1-unit markings when your dose falls between the 2-unit increments of a larger syringe. This eliminates rounding errors entirely. Proper peptide safety practices demand this level of precision.
Switching between concentrations safely
Concentration changes are inevitable for most researchers. Your pharmacy may change suppliers. You might switch pharmacies entirely. Or you might intentionally move to a higher concentration as your dose increases. Each transition requires recalculation. Here is how to handle it safely.
The golden rule for concentration switches
When switching concentrations, always recalculate from milligrams first. Do not try to convert from old units to new units directly. Start with the dose your provider prescribed in milligrams, then calculate fresh using the new concentration.
Example: You were taking 5 mg per week from a 10 mg/mL vial (50 units). You receive a 20 mg/mL vial.
Wrong approach: "I was taking 50 units, so I will take 50 units from the new vial." This gives you 10 mg, double your dose.
Right approach: "My dose is 5 mg. 5 mg divided by 20 mg/mL equals 0.25 mL, which is 25 units." Same dose, half the volume.
If you are switching between different GLP-1 compounds, the same principle applies, but the dose equivalencies are different. Always verify conversion ratios with your provider. You might also want to understand the differences between semaglutide and tirzepatide if considering a switch.
Concentration change verification checklist
Use this process every time you start a new vial, even if you think the concentration is the same:
1. Read the vial label. Find the mg/mL concentration.
2. Compare it to your previous vial concentration. Are they the same?
3. If different, recalculate your unit dose using the formula: units = (dose in mg / concentration in mg/mL) x 100.
4. Double-check by working backwards: new units / 100 x new concentration = your dose in mg. Does it match your prescribed dose?
5. Draw up the new amount and verify it looks reasonable before injecting.
This takes 60 seconds. It prevents potentially serious dosing errors. Make it a habit.
How 20 units of tirzepatide compares to semaglutide dosing
Many researchers have experience with semaglutide dosing in units and wonder how tirzepatide compares. The conversion principles are identical, but the clinical doses are completely different because these are different compounds with different potencies.
Same math, different numbers
The formula is universal. Units / 100 = mL. Then mL times concentration equals mg. This works for tirzepatide, semaglutide, retatrutide, or any compound in a vial.
But 20 units of tirzepatide at 10 mg/mL (2.0 mg) is not equivalent to 20 units of semaglutide at 10 mg/mL (also 2.0 mg). The clinical effect of 2.0 mg of tirzepatide is very different from 2.0 mg of semaglutide because the two peptides have different receptor binding profiles, different half-lives, and different dose-response curves.
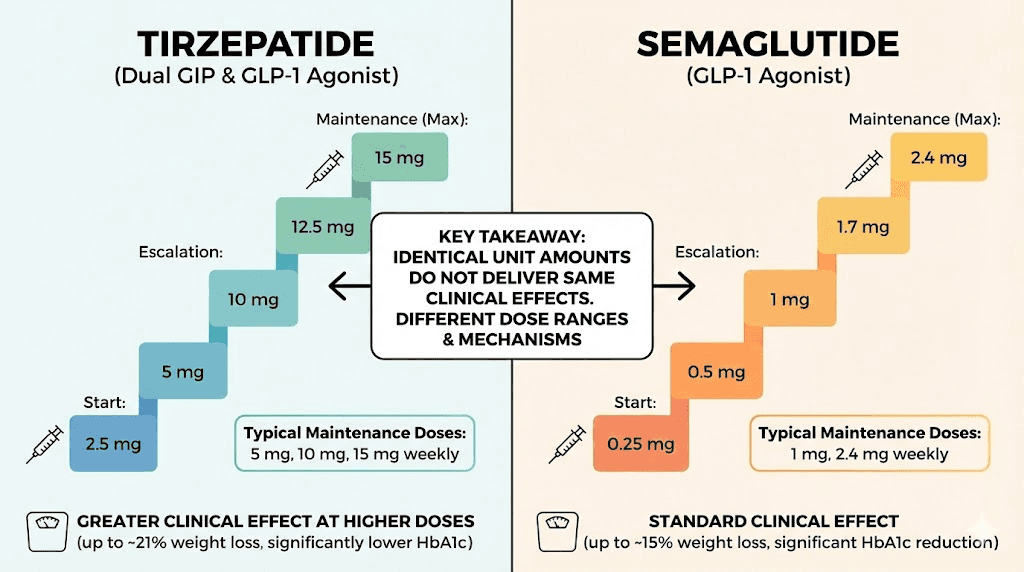
Tirzepatide is a dual GIP/GLP-1 receptor agonist. Semaglutide targets only GLP-1. This dual mechanism means tirzepatide generally produces greater weight loss at comparable milligram doses. In the SURPASS-2 trial, tirzepatide at 5 mg outperformed semaglutide 1 mg for weight loss by approximately 1.9 kg. At 15 mg, tirzepatide outperformed semaglutide by 5.5 kg. Understanding these GLP-1 receptor agonist differences matters for protocol design.
Dose comparison reference
Compound | Starting dose | Maximum dose | Dose escalation interval |
|---|---|---|---|
Tirzepatide | 2.5 mg weekly | 15.0 mg weekly | 4 weeks minimum |
Semaglutide | 0.25 mg weekly | 2.4 mg weekly | 4 weeks minimum |
Retatrutide | 1.0 mg weekly | 12.0 mg weekly | 4 weeks minimum |
Notice the massive difference in dose ranges. Semaglutide maxes out at 2.4 mg where tirzepatide maxes at 15 mg. These are not interchangeable numbers. Twenty units at 10 mg/mL gives you 2.0 mg of whichever compound you are using, but 2.0 mg of semaglutide is close to the maximum dose, while 2.0 mg of tirzepatide is below the starting dose. You can explore the 20 units of semaglutide conversion in our dedicated guide.
Using a dosage calculator for verification
While knowing the formula by heart is valuable, using a calculator provides an important safety check. Manual math errors happen, especially when you are tired, distracted, or working with an unfamiliar concentration. Calculators eliminate arithmetic mistakes, though they do not replace understanding the principles behind the numbers.
How tirzepatide calculators work
Every reputable tirzepatide dosage calculator asks for two inputs: your desired dose in milligrams and your vial concentration in mg/mL. It then outputs the number of syringe units to draw.
The math behind the calculator is the same formula you already know: units = (dose mg / concentration mg/mL) x 100. Nothing more, nothing less. The calculator just removes the possibility of an arithmetic slip.
The SeekPeptides peptide calculator handles these conversions instantly and works for multiple compounds. It also integrates with reconstitution calculations if you are working with lyophilized powder that needs to be mixed before use.
When to use a calculator vs manual math
Use a calculator when you are starting a new vial with a different concentration, when you are changing your dose, or when you simply want to double-check your mental math. Use manual calculation when you want to understand the logic, verify the calculator output, or when no calculator is available.
The best practice is both. Calculate manually first, then verify with a calculator. If the numbers match, proceed with confidence. If they do not match, find the error before injecting anything. This redundancy is a core principle of safe peptide research.
Tirzepatide reconstitution and its impact on concentration
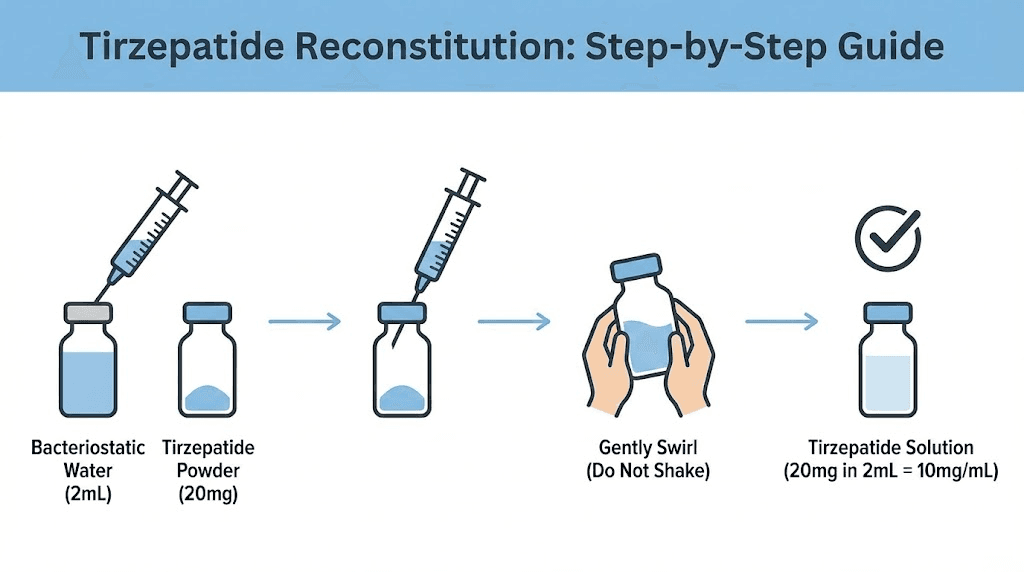
If you are working with lyophilized (freeze-dried) tirzepatide powder rather than a pre-mixed liquid, you control the concentration. The amount of bacteriostatic water you add determines the mg/mL, which in turn determines how many milligrams your 20 units contains.
How reconstitution creates concentration
The formula is straightforward. Concentration = total mg of peptide / total mL of bacteriostatic water added.
If you have a vial containing 10 mg of tirzepatide powder and add 1 mL of bacteriostatic water, your concentration is 10 mg/mL. Add 2 mL instead, and your concentration drops to 5 mg/mL. The same 20 units now delivers a different milligram dose depending on how much water you used.
Peptide amount | Bac water added | Resulting concentration | 20 units delivers |
|---|---|---|---|
10 mg | 0.5 mL | 20 mg/mL | 4.0 mg |
10 mg | 1.0 mL | 10 mg/mL | 2.0 mg |
10 mg | 2.0 mL | 5 mg/mL | 1.0 mg |
30 mg | 1.0 mL | 30 mg/mL | 6.0 mg |
30 mg | 1.5 mL | 20 mg/mL | 4.0 mg |
30 mg | 3.0 mL | 10 mg/mL | 2.0 mg |
60 mg | 2.0 mL | 30 mg/mL | 6.0 mg |
60 mg | 3.0 mL | 20 mg/mL | 4.0 mg |
60 mg | 6.0 mL | 10 mg/mL | 2.0 mg |
Our peptide reconstitution calculator takes the guesswork out of this step. Enter your peptide amount and desired concentration, and it tells you exactly how much bacteriostatic water to add. Getting this right is the foundation of accurate dosing. For detailed guidance on the mixing process itself, see the complete guide to mixing peptides with bacteriostatic water.
Choosing your reconstitution concentration wisely
The ideal concentration depends on your current dose and how precise you need to be.
For starting doses (2.5 mg), a 10 mg/mL concentration works well. It requires 25 units, a clean measurement on any syringe.
For moderate doses (5-7.5 mg), 10 mg/mL still works but requires 50-75 units. This is comfortable with a 1 mL syringe.
For higher doses (10-15 mg), 20 mg/mL or higher keeps injection volumes manageable. At 20 mg/mL, 15 mg requires only 75 units.
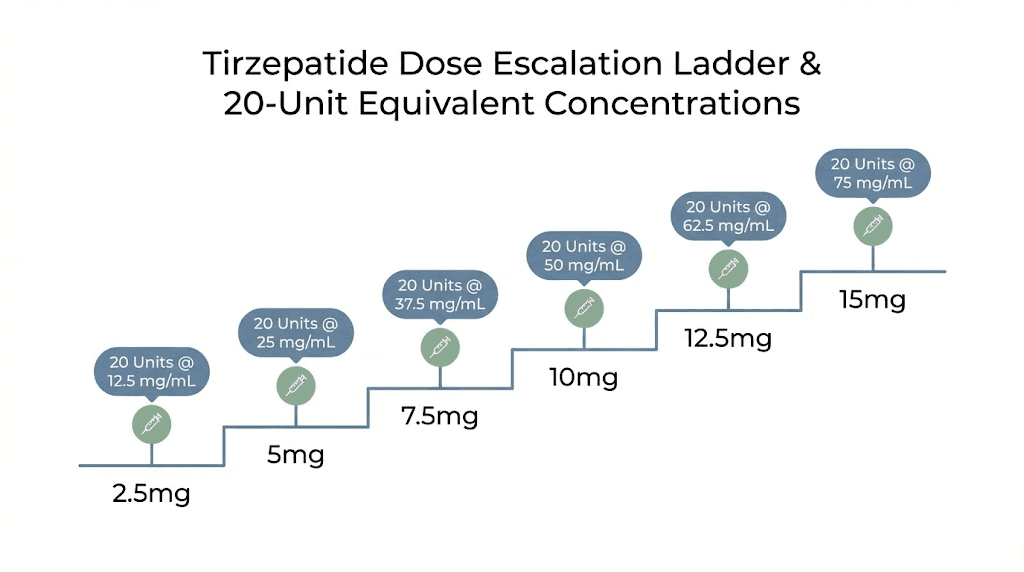
Some researchers choose a concentration that makes their specific dose land on a round number of units. If you take 5 mg weekly, a 10 mg/mL concentration gives you exactly 50 units, a clean number. Or 25 mg/mL gives you exactly 20 units. There is elegance in simplicity, and round numbers leave less room for error. For more on proper peptide storage after reconstitution, check our storage guide.
Bacteriostatic water considerations
The type and quality of water matters. Bacteriostatic water for peptides contains 0.9% benzyl alcohol as a preservative, which prevents bacterial growth in multi-use vials. Sterile water lacks this preservative and must be used within 24 hours of opening.
For compounded tirzepatide vials that will be used over multiple weeks, bacteriostatic water is essential. Understanding how much bacteriostatic water to add directly determines your concentration and therefore your unit-to-mg conversion.
Storage and stability considerations that affect dosing
Concentration is only meaningful if your tirzepatide maintains its potency. Degraded peptide means that your 20 units may nominally contain 2 mg (at 10 mg/mL), but the actual active compound could be significantly less. Storage directly impacts dosing accuracy over time.
Temperature requirements
Reconstituted tirzepatide should be stored at 36-46 degrees Fahrenheit (2-8 degrees Celsius), which is standard refrigerator temperature. Room temperature exposure accelerates degradation, reducing the actual milligram content of each dose even though the volume remains unchanged.
Understanding whether tirzepatide needs refrigeration is not optional. It does. Detailed peptide storage guidance covers optimal conditions for maintaining potency throughout your protocol.
Shelf life after reconstitution
Most compounding pharmacies assign a beyond-use date of 28-42 days for reconstituted tirzepatide stored under refrigeration. After this period, degradation may reduce potency below therapeutic levels. If you reconstituted your own powder, track the date carefully.
A vial that sits in the fridge for 6 weeks may still appear normal, clear liquid, no discoloration. But the active compound inside may have degraded by 10-20%, meaning your 20 units now delivers less than the calculated milligrams. For specific storage timelines, see our detailed guide on how long tirzepatide lasts in the fridge.
Signs of degradation
Never inject tirzepatide that shows visible changes: cloudiness, particles, color change, or unusual viscosity. These indicate breakdown products that may not only be less effective but potentially harmful. Clear liquid does not guarantee full potency, but visible changes guarantee compromised product.
Understanding compound stability is part of responsible peptide research. The peptide expiration guide covers degradation timelines for various storage conditions.
Dose escalation protocols and what 20 units means at each stage
Now let us put this all together with practical dose escalation scenarios. Most tirzepatide protocols follow the clinical trial model: start at 2.5 mg, hold for 4 weeks, then increase by 2.5 mg increments until reaching the target dose. Here is what 20 units represents at each stage of escalation, and why understanding this matters for how fast tirzepatide works.
Escalation scenario with 10 mg/mL
At 10 mg/mL, 20 units delivers 2.0 mg. Here is where that falls in a standard escalation:
Weeks 1-4 (2.5 mg target): You need 25 units. Twenty units is 0.5 mg below your target. Close, but not correct. Do not round down to 20 just because it is a rounder number.
Weeks 5-8 (5.0 mg target): You need 50 units. Twenty units is 3 mg below your target. Not even in the ballpark.
Weeks 9-12 (7.5 mg target): You need 75 units. Twenty units delivers less than a third of your intended dose.
The message is clear. At 10 mg/mL, 20 units (2.0 mg) is never the correct dose for any standard tirzepatide tier. It is useful only for sub-therapeutic microdosing or as a deliberate below-threshold starting point for sensitive individuals.
Escalation scenario with 20 mg/mL
At 20 mg/mL, the same 20 units delivers 4.0 mg. Different picture entirely.
Weeks 1-4 (2.5 mg target): You need 12.5 units. Twenty units would overshoot by 1.5 mg. Do not use 20 units during the starting phase at this concentration.
Weeks 5-8 (5.0 mg target): You need 25 units. Twenty units is 1 mg below target, but close enough that some researchers use it as a gradual step between 2.5 and 5.0 mg.
The escalation process requires patience. Many researchers experience fewer side effects, particularly the fatigue and gastrointestinal discomfort, when they follow the recommended 4-week minimum at each tier before increasing.
Microdosing with 20 units
Some researchers intentionally use sub-therapeutic doses to assess tolerance before committing to full protocols. This is where 20 units at lower concentrations becomes strategically useful.
At 5 mg/mL, 20 units delivers 1.0 mg. This is 60% below the standard starting dose and allows for gentle introduction to the compound. Some sensitive individuals, those with anxiety responses to new medications or histories of severe GI sensitivity, find this sub-threshold approach valuable.
The microdosing tirzepatide chart provides detailed protocols for this approach, including escalation schedules from microdoses up to therapeutic ranges.
Real-world calculation examples
Theory is one thing. Let us walk through five real-world scenarios that researchers commonly encounter. Each one involves 20 units somewhere in the calculation process. These examples reinforce the principles while giving you practical reference points.
Example 1: new researcher, first vial, 10 mg/mL
Maria receives her first tirzepatide vial. The label reads "Tirzepatide 10 mg/mL, 5 mL." Her provider prescribed a starting dose of 2.5 mg weekly.
Step 1: Find the concentration. It is on the label: 10 mg/mL.
Step 2: Calculate units needed. 2.5 mg / 10 mg/mL = 0.25 mL. Then 0.25 x 100 = 25 units.
Step 3: Maria draws 25 units, not 20. If she drew 20 units, she would only get 2.0 mg.
The difference between 20 and 25 units matters. It is the difference between 2.0 mg and 2.5 mg, a 20% underdose that could mean slower results and delayed appetite suppression.
Example 2: switching concentrations mid-protocol
James has been using a 10 mg/mL vial, drawing 50 units for his 5 mg weekly dose. His pharmacy now sends a 20 mg/mL vial.
Wrong: James draws 50 units from the new vial. He injects 10 mg, double his dose. He experiences severe nausea, vomiting, and fatigue for 3 days.
Right: James recalculates. 5 mg / 20 mg/mL = 0.25 mL = 25 units. He draws 25 units. Same dose, no issues.
James could also calculate 20 units from his new vial to find out what that delivers: 0.2 mL x 20 mg/mL = 4.0 mg. Not his prescribed dose. He sticks with 25 units.
Example 3: reconstituting from powder
Sofia has a 30 mg vial of lyophilized tirzepatide. She wants her 20 units to deliver exactly 2.5 mg (her starting dose). What concentration does she need?
Working backwards: 2.5 mg / 0.2 mL = 12.5 mg/mL. So she needs 12.5 mg/mL concentration.
To get 12.5 mg/mL from a 30 mg vial: 30 mg / 12.5 mg/mL = 2.4 mL of bacteriostatic water.
Sofia adds 2.4 mL of bacteriostatic water to her 30 mg vial. Her 20 units now delivers exactly 2.5 mg. This is an elegant approach, but it requires precise water measurement and careful reconstitution technique.
Example 4: checking a provider's instructions
David's provider says "inject 20 units weekly" without specifying milligrams. His vial is 15 mg/mL.
David calculates: 20 units = 0.2 mL. At 15 mg/mL: 0.2 x 15 = 3.0 mg.
Is 3.0 mg an appropriate dose? It does not match any standard tier (2.5, 5.0, 7.5, 10.0, 12.5, or 15.0 mg). David should contact his provider to confirm: "Did you mean 20 units at my concentration of 15 mg/mL, which equals 3.0 mg? Or did you mean a different number of units?"
This kind of verification prevents miscommunication errors. It is one of the most important things you can do for your own safety.
Example 5: comparing costs across concentrations
Two pharmacies offer tirzepatide. Pharmacy A sells 10 mg/mL vials (5 mL) for $200. Pharmacy B sells 20 mg/mL vials (5 mL) for $350.
Pharmacy A: 5 mL x 10 mg/mL = 50 mg total. Cost per mg: $200 / 50 mg = $4.00/mg.
Pharmacy B: 5 mL x 20 mg/mL = 100 mg total. Cost per mg: $350 / 100 mg = $3.50/mg.
At 20 units per week (2 mg from Pharmacy A, 4 mg from Pharmacy B), the weekly cost differs. Pharmacy A: 2 mg x $4.00 = $8.00/week. Pharmacy B: 4 mg x $3.50 = $14.00/week. But remember, these are different doses. Comparing cost per milligram is the only fair comparison. Understanding the financial side of peptide research is covered in our peptide cost calculator.
What to do if you accidentally inject the wrong amount
Mistakes happen. Even careful researchers occasionally draw the wrong number of units or forget to account for a concentration change. Here is what to know if you realize you injected too much or too little.
If you injected more than intended
Do not panic, but take the situation seriously. The most common symptoms of a tirzepatide overdose are gastrointestinal: severe nausea, vomiting, diarrhea, and abdominal pain. These can be intense but are typically self-limiting.
Stay hydrated. Electrolyte solutions are important since vomiting and diarrhea can cause dehydration rapidly. Monitor for signs of severe dehydration: dizziness, rapid heartbeat, dark urine, or inability to keep fluids down.
If you doubled your dose (took 5 mg instead of 2.5 mg, for example), skip the next weekly injection and resume your normal schedule the following week. Do not try to "compensate" by taking less next time, that introduces more variability.
Seek medical attention if symptoms are severe, if you experience signs of hypoglycemia (shakiness, confusion, cold sweats), or if the dose taken was dramatically above your prescribed amount. The peptide safety guide provides comprehensive emergency protocols.
If you injected less than intended
Under-dosing is less immediately dangerous but undermines your protocol. If you realize quickly that you drew too few units, you have options depending on how much time has passed.
If you realize within a few hours and still have the prepared syringe, you can administer the remaining units as a second injection. This is not ideal, as splitting a dose increases total injection volume and handling, but it is better than missing the balance entirely.
If you realize the next day, the simplest approach is to accept the lower dose for that week and return to your normal dose the following injection. Do not add extra units to your next dose to "make up" for the shortfall.
Tracking your doses helps prevent both scenarios. Many researchers use a simple log: date, vial concentration, units drawn, and milligrams calculated. This record catches errors before they become patterns and helps you identify whether tirzepatide is working as expected.
Beyond the math: optimizing your tirzepatide protocol
Getting 20 units right is the foundation. But a successful tirzepatide protocol involves much more than accurate measurement. Here are the factors that determine whether your research produces the results the clinical trials demonstrated.
Injection timing and consistency
Tirzepatide has a half-life of approximately 5 days. It is administered once weekly, ideally on the same day each week. Consistency in timing helps maintain stable blood levels and more predictable effects.
If you miss a dose, you can take it within 4 days of the scheduled time. If more than 4 days have passed, skip the missed dose and resume your normal schedule. Never double up. Consistent timing contributes significantly to how quickly tirzepatide produces results.
Injection site selection
Tirzepatide is administered subcutaneously, which means just under the skin, not into muscle. The recommended injection sites are the abdomen (at least 2 inches from the navel), the front of the thigh, and the upper arm.
Rotate injection sites with each dose. Using the same spot repeatedly can cause lipodystrophy, changes in the fat tissue that affect absorption and appearance. A simple rotation pattern (right abdomen, left abdomen, right thigh, left thigh) ensures adequate spacing between uses of each site.
Diet and lifestyle factors
Tirzepatide reduces appetite and slows gastric emptying. Many researchers find that their relationship with food changes dramatically. Meals feel satisfying faster. Cravings diminish. But these effects work best when supported by intentional nutritional choices.
Protein intake becomes especially important during tirzepatide use. Rapid weight loss without adequate protein leads to muscle loss alongside fat loss, an outcome that undermines metabolic health. Most protocols recommend 0.7-1.0 grams of protein per pound of body weight daily. For researchers struggling with reduced appetite, protein supplements can help meet targets without requiring large meal volumes. Understanding what foods to avoid while on tirzepatide can also help minimize gastrointestinal side effects.
The tirzepatide before and after results that impress most are from researchers who combine accurate dosing with structured nutrition and regular physical activity. The compound does its job. But so must the researcher.
Managing side effects
Gastrointestinal side effects are the most common complaint with tirzepatide. Nausea, constipation, and diarrhea affect a significant percentage of users, particularly during dose escalation phases. These effects typically diminish after 2-4 weeks at each dose tier.
Strategies that help include eating smaller, more frequent meals, avoiding high-fat foods (which slow gastric emptying further), staying well-hydrated, and escalating doses gradually rather than jumping tiers. Some researchers find that adding B12 to their tirzepatide protocol helps with energy levels during the adjustment period.
If side effects are severe or persistent, reducing the dose by stepping back one tier often resolves them. This is another reason why understanding unit-to-mg conversion matters. You need to know exactly how much to reduce, which means calculating the correct number of units for the lower dose at your specific concentration.
How SeekPeptides tools simplify these calculations
SeekPeptides built its calculator suite specifically for researchers who need accurate, fast conversions without the mental math burden. The platform addresses every step of the dosing process.
The peptide dosage calculator converts between milligrams, milliliters, and syringe units for any concentration. Enter your vial strength and desired dose, and get your unit count instantly.
The reconstitution calculator tells you exactly how much bacteriostatic water to add to achieve your target concentration, which feeds directly into your dosing calculation.
The cost calculator helps compare different vial sizes and concentrations on a cost-per-milligram basis, so you can find the most economical option.
Beyond calculators, SeekPeptides members access comprehensive protocol guides, stacking recommendations, and a community of experienced researchers who have navigated these exact questions. For researchers serious about getting their protocols right from day one, the platform eliminates guesswork and builds confidence in every measurement.
Frequently asked questions
Is 20 units of tirzepatide always the same as 2 mg?
No. Twenty units equals 2 mg only at a 10 mg/mL concentration. At 20 mg/mL, 20 units equals 4 mg. At 5 mg/mL, 20 units equals 1 mg. Always check your vial concentration before calculating. Use the peptide calculator to verify your conversion.
How do I know the concentration of my tirzepatide vial?
The concentration is printed on the vial label as mg/mL (for example, "10 mg/mL" or "20 mg/mL"). If the label shows only total content (like "50 mg/5 mL"), divide the milligrams by the milliliters: 50/5 = 10 mg/mL. If you reconstituted the peptide yourself, your concentration equals total peptide weight divided by total bacteriostatic water volume.
Can I use a regular syringe instead of an insulin syringe for tirzepatide?
Standard syringes are marked in milliliters rather than units, so the conversion step is different. For 20 units, draw to the 0.2 mL mark on a standard syringe. However, insulin syringes offer better precision for small volumes. A 0.3 mL insulin syringe with 1-unit markings gives the most accurate measurements for tirzepatide dosing.
What happens if I accidentally take 20 units instead of 25 units of tirzepatide?
At 10 mg/mL, this means you took 2.0 mg instead of 2.5 mg, a 20% underdose. The effect will be slightly reduced appetite suppression for that week. Do not try to compensate by adding extra units to your next dose. Simply take your normal 25 units at your next scheduled injection and continue as planned.
Why do some pharmacies use different concentrations?
Compounding pharmacies adjust concentrations based on clinical needs. Lower concentrations (5-10 mg/mL) allow more precise small-dose measurements. Higher concentrations (20-50 mg/mL) reduce injection volume for higher doses. Your provider may specify a preferred concentration based on your dose tier and syringe availability.
How many units of tirzepatide should I take per week?
The number of units depends entirely on your prescribed milligram dose and your vial concentration. A standard starting dose of 2.5 mg requires 25 units at 10 mg/mL, 12.5 units at 20 mg/mL, or 50 units at 5 mg/mL. Always follow your provider instructions for the specific milligram dose and calculate units based on your vial label.
Does the number of units change if I switch from Mounjaro to compounded tirzepatide?
Brand-name Mounjaro uses pre-filled pens with fixed doses, so you never measure units. When switching to compounded vials, your provider will prescribe the same milligram dose, and you calculate units based on the compounded vial concentration. The active compound is the same, but the measurement method changes completely. See our guide on compounded tirzepatide options for more details.
Is 20 units a good starting dose for tirzepatide?
That depends on your concentration. At 10 mg/mL, 20 units delivers 2.0 mg, which is below the standard 2.5 mg starting dose. Some providers use this as a gentle introduction for sensitive patients. At 20 mg/mL, 20 units delivers 4.0 mg, which exceeds the starting dose. Never choose a dose based on units alone. Always work from your prescribed milligram dose and calculate accordingly.
External resources
For researchers committed to optimizing every aspect of their tirzepatide protocol, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, precision calculators, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your concentrations stay verified, and your protocols stay consistent.