Feb 25, 2026
Some researchers drawing 10 units from their tirzepatide vial get 0.5 mg. Others get 4.0 mg. Same syringe marking. Same number on the barrel. Completely different doses delivered into the body. The difference is not a math error or a faulty syringe. It comes down to one variable that changes everything about your tirzepatide dosage in units, and most people overlook it entirely.
That variable is concentration.
Compounded tirzepatide vials come in different strengths, measured in milligrams per milliliter (mg/mL). A vial labeled 5 mg/mL contains a very different amount of active medication per unit than a vial labeled 20 mg/mL. When you draw 10 units on an insulin syringe, you are pulling 0.1 mL of liquid every single time, regardless of what is inside. But the milligrams of tirzepatide dissolved in that 0.1 mL? That depends entirely on what your pharmacy put in the vial. Understanding this relationship is not optional. It is the foundation of accurate dosing, and getting it wrong means either underdosing (wasting time and money) or overdosing (risking unnecessary side effects). This guide breaks down exactly how many milligrams 10 units delivers at every common concentration, gives you the formula to calculate it yourself, and walks you through the most dangerous mistakes people make when measuring tirzepatide doses in units.
The quick answer: what 10 units of tirzepatide equals in milligrams
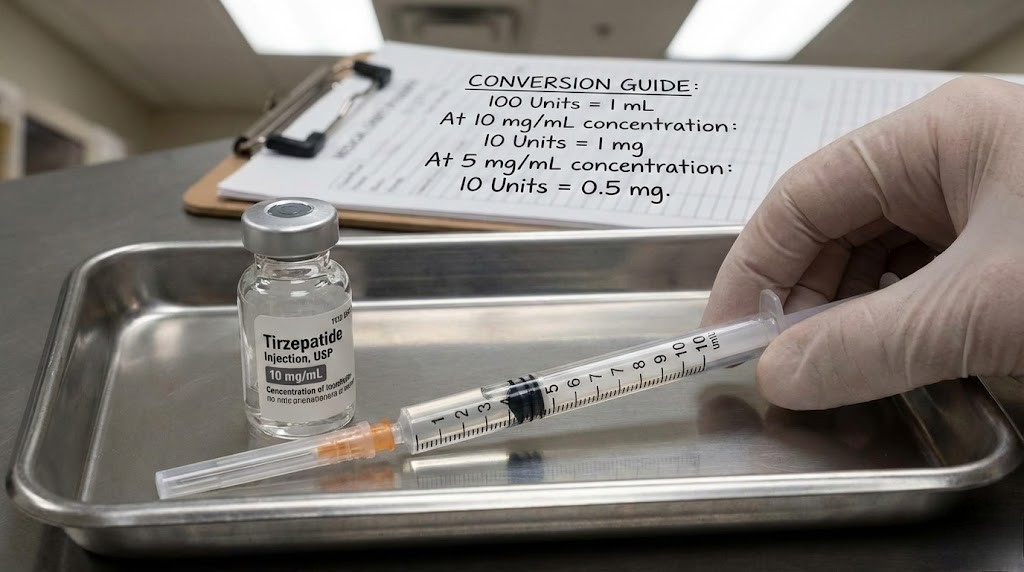
Here is the direct answer. Ten units on a U-100 insulin syringe equals 0.1 mL of liquid. The milligrams of tirzepatide in that 0.1 mL depends on your vial concentration:
At 5 mg/mL: 10 units = 0.5 mg of tirzepatide
At 10 mg/mL: 10 units = 1.0 mg of tirzepatide
At 15 mg/mL: 10 units = 1.5 mg of tirzepatide
At 20 mg/mL: 10 units = 2.0 mg of tirzepatide
At 30 mg/mL: 10 units = 3.0 mg of tirzepatide
At 40 mg/mL: 10 units = 4.0 mg of tirzepatide
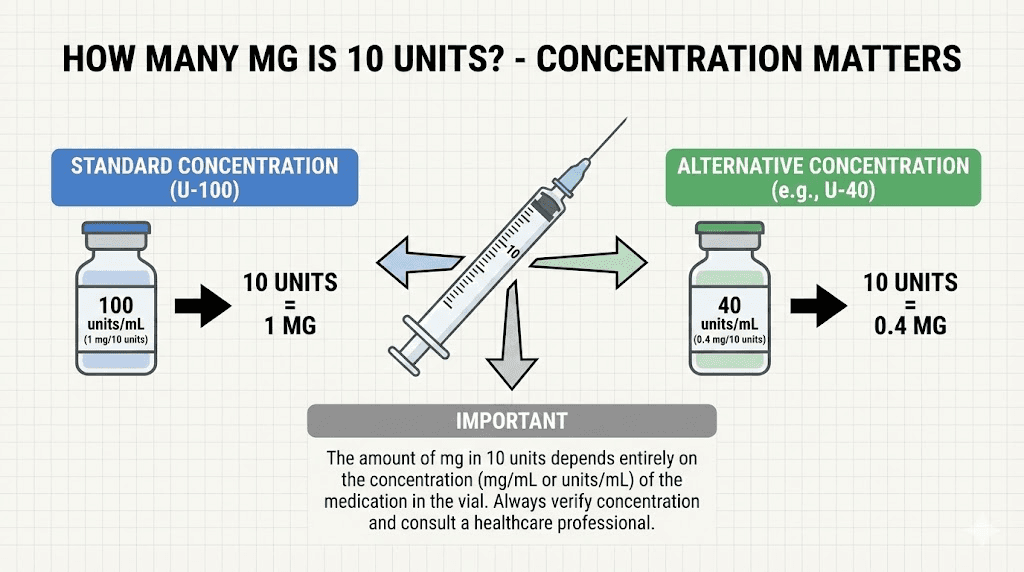
If you have a 10 mg/mL vial, which is the most common concentration from compounding pharmacies, then 10 units gives you exactly 1 mg of tirzepatide. Simple. But if your vial is 20 mg/mL, those same 10 units deliver 2 mg instead. Double the dose from the same syringe marking. That is why checking your tirzepatide conversion chart against your specific vial concentration matters every single time you prepare an injection.
Why concentration changes everything about your 10-unit dose
The word "units" on an insulin syringe does not measure medication strength. It measures volume. That distinction trips up more people than any other aspect of tirzepatide dosing.
Think of it this way. A standard U-100 insulin syringe holds 1 mL of liquid at full capacity, which is 100 units. Each unit marking represents 0.01 mL of volume. When you draw to the 10-unit line, you have pulled exactly 0.1 mL of liquid into the syringe. Not 10 milligrams. Not 10 anything related to the medication itself. Just 0.1 mL of whatever liquid is in that vial.
Now consider what happens with different concentrations.
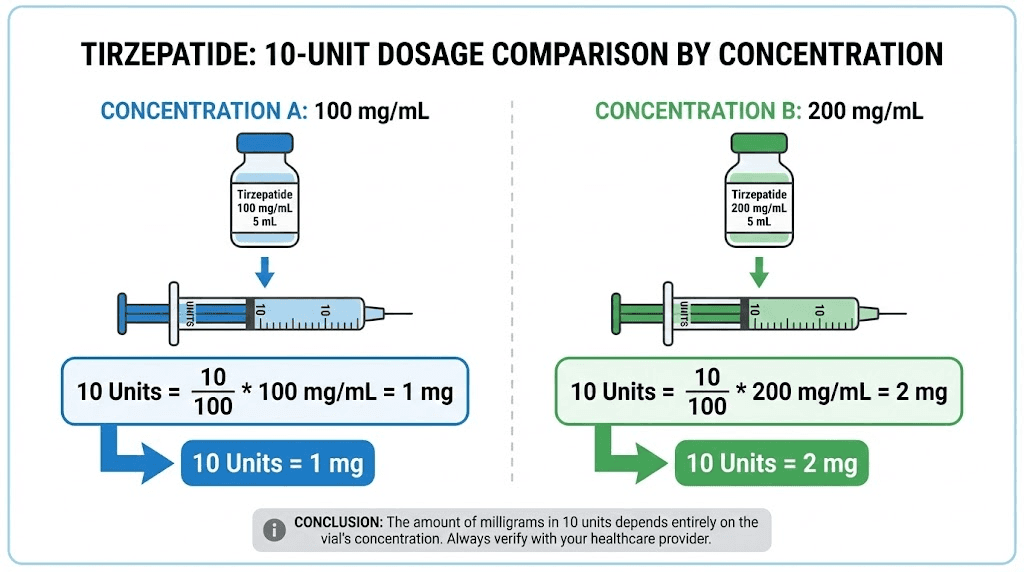
A compounding pharmacy that formulates tirzepatide at 5 mg/mL has dissolved 5 milligrams of active tirzepatide into every milliliter of solution. Pull 0.1 mL (10 units), and you get one-tenth of those 5 milligrams. That is 0.5 mg. A pharmacy using 20 mg/mL has packed four times as much tirzepatide into the same volume. Pull the same 0.1 mL, and you get 2.0 mg instead. The syringe looks identical. The number reads the same. But the actual dose is four times higher. This is why compounded tirzepatide dosage calculators always ask for your concentration first.
The concentration spectrum in compounded tirzepatide
Compounding pharmacies do not all use the same concentration. The most common options you will encounter include 5 mg/mL, 10 mg/mL, 17 mg/mL, 20 mg/mL, and 40 mg/mL. Some pharmacies add other compounds like niacinamide or B12, which does not change the tirzepatide concentration but does affect the overall formulation.
The 10 mg/mL concentration is the most widely used. Most clinics reference it in their dosing instructions. Most tirzepatide dosage charts in units default to this concentration. If your provider gave you a chart without specifying concentration, there is a good chance it assumes 10 mg/mL.
Higher concentrations like 20 mg/mL and 40 mg/mL exist for people on higher maintenance doses who want smaller injection volumes. At 15 mg weekly (the maximum FDA-approved dose), a 10 mg/mL vial requires 150 units, or 1.5 mL, per injection. That is a large volume. A 20 mg/mL vial cuts that to 75 units (0.75 mL), and a 40 mg/mL vial brings it down to just 37.5 units (0.375 mL). For the dosing chart in units at each concentration, the math shifts dramatically.
Why 10 mg/mL became the standard
The 10 mg/mL concentration hits a sweet spot. At the starting dose of 2.5 mg, you draw 25 units, which is a comfortable volume to measure accurately on most insulin syringes. At the maximum 15 mg dose, you need 150 units, which means either using a 1 mL syringe filled to 1.5 markings or splitting into two injections. It works for the full tirzepatide dosing range for weight loss without requiring extremely small or extremely large draws at either end of the scale.
Providers who prescribe higher maintenance doses often transition patients to 20 mg/mL vials once they reach 10 mg or higher. This keeps injection volumes manageable while maintaining dosing accuracy.
Complete conversion table: 10 units at every concentration
Here is the comprehensive reference table showing what 10 units delivers across all commercially available tirzepatide concentrations. Bookmark this. You will need it every time your pharmacy changes your vial or you switch providers.
Vial concentration | Volume drawn (10 units) | Tirzepatide delivered | Percentage of 2.5 mg starting dose |
|---|---|---|---|
5 mg/mL | 0.1 mL | 0.5 mg | 20% |
8 mg/mL | 0.1 mL | 0.8 mg | 32% |
10 mg/mL | 0.1 mL | 1.0 mg | 40% |
15 mg/mL | 0.1 mL | 1.5 mg | 60% |
17 mg/mL | 0.1 mL | 1.7 mg | 68% |
20 mg/mL | 0.1 mL | 2.0 mg | 80% |
30 mg/mL | 0.1 mL | 3.0 mg | 120% |
40 mg/mL | 0.1 mL | 4.0 mg | 160% |
Notice the "percentage of starting dose" column. At 10 mg/mL, drawing 10 units gives you 40% of the standard 2.5 mg starting dose. At 40 mg/mL, those same 10 units deliver 160% of the starting dose, which is well above the recommended initial amount. The stakes of knowing your concentration could not be higher.
For the reverse calculation, where you know the milligrams you want and need to figure out the units, check our guide on how many units is 2.5 mg of tirzepatide or our 5 mg to units conversion.
The formula: how to calculate tirzepatide units to milligrams yourself
You do not need to memorize conversion tables. One formula handles every scenario.
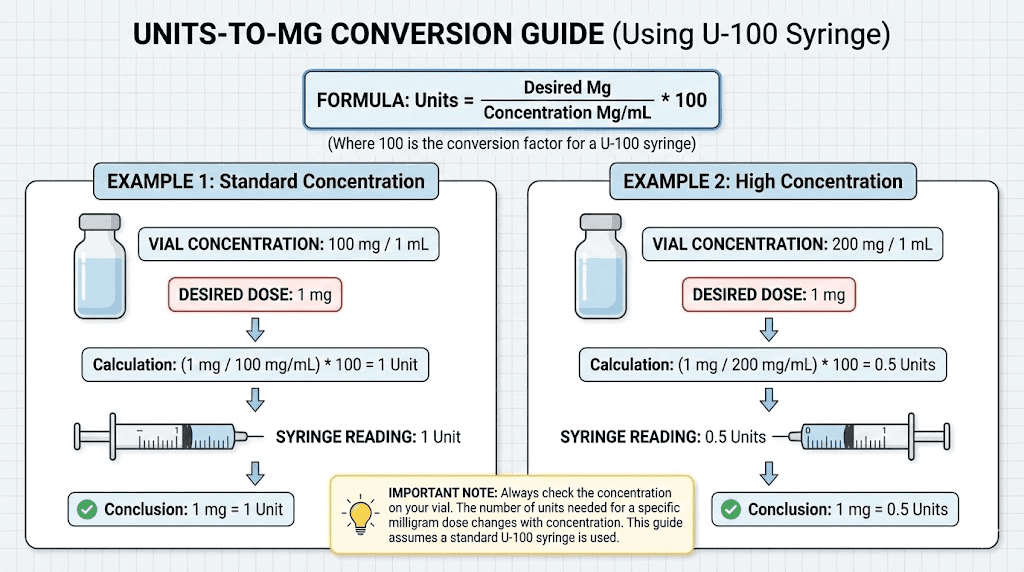
Milligrams = (Units / 100) x Concentration (mg/mL)
For 10 units at 10 mg/mL: (10 / 100) x 10 = 1.0 mg. For 10 units at 20 mg/mL: (10 / 100) x 20 = 2.0 mg. For 10 units at 5 mg/mL: (10 / 100) x 5 = 0.5 mg.
The formula works because dividing units by 100 converts them to milliliters (since 100 units = 1 mL on a U-100 syringe). Multiplying by concentration then tells you how many milligrams are dissolved in that volume. You can also use the SeekPeptides peptide calculator to run this calculation instantly without doing the math by hand.
Working the formula in reverse
Sometimes you know the dose in milligrams and need to figure out how many units to draw. The reverse formula is equally simple.
Units = (Desired mg / Concentration) x 100
Want 2.5 mg from a 10 mg/mL vial? (2.5 / 10) x 100 = 25 units. Want 5 mg from a 20 mg/mL vial? (5 / 20) x 100 = 25 units. Same number of units, but completely different milligram doses, because the concentrations differ. Our tirzepatide dosage chart in units provides pre-calculated tables for every standard dose at every concentration so you never have to rely on mental math during injection prep.
Why the formula matters more than memorized numbers
Memorizing that "25 units = 2.5 mg" is dangerous if you do not also remember which concentration that applies to. That equation is only true at 10 mg/mL. At 20 mg/mL, 25 units delivers 5 mg. At 5 mg/mL, 25 units delivers only 1.25 mg. The formula protects you from this trap because it forces you to input your specific concentration every time. If your provider gives you a compound dosing chart, verify it matches your vial before following it.
Understanding insulin syringes and tirzepatide measurement
Tirzepatide is not insulin. But most people use insulin syringes to inject it. This creates a layer of confusion that trips up beginners and experienced users alike.
A U-100 insulin syringe was designed so that 1 unit equals 1 unit of insulin. For insulin, that relationship between the syringe marking and the medication potency is straightforward because insulin is standardized at 100 units per mL. Tirzepatide does not follow this convention. The "units" on your syringe only tell you volume. Period. They say nothing about how much tirzepatide is in that volume.
Syringe sizes and their markings
Insulin syringes come in three common sizes. The 0.3 mL syringe holds 30 units maximum and has fine graduation markings, usually in 0.5-unit or 1-unit increments. The 0.5 mL syringe holds 50 units with 1-unit markings. The 1 mL syringe holds 100 units. For tirzepatide syringe dosage, the best choice depends on the volume you need to draw.
At 10 units, any of these syringes works. But the 0.3 mL syringe gives you the most precise reading because its markings are more spread out. When accuracy matters, and it always matters with tirzepatide injection dosing, choose the smallest syringe that fits your dose volume.
The TB syringe confusion
Here is where dangerous mistakes happen. Tuberculin (TB) syringes look similar to insulin syringes but use different markings. A TB syringe is marked in milliliters, not units. If someone draws to "0.25" on a TB syringe, they get 0.25 mL, which equals 25 units on an insulin syringe. But if they confuse the markings and draw to "25" thinking it means 25 units, they could actually be drawing 2.5 mL, which is 250 units. Ten times the intended dose.
Always use a U-100 insulin syringe for tirzepatide. Not a TB syringe. Not a different type. Only U-100. The injection guide for tirzepatide covers proper syringe selection in detail, and it is worth reviewing if you have any uncertainty about your equipment.
The most common concentrations and what 10 units delivers from each
5 mg/mL: the dilute formulation
At 5 mg/mL, your vial contains 5 milligrams of tirzepatide per milliliter of solution. Drawing 10 units pulls 0.1 mL, which contains 0.5 mg of tirzepatide. This is a sub-therapeutic dose for most applications, well below the standard starting dose of 2.5 mg.
The 5 mg/mL concentration requires larger injection volumes for standard doses. For the 2.5 mg starting dose, you need 50 units (0.5 mL). For 5 mg, you need 100 units (1.0 mL), which fills an entire 1 mL syringe. For anything above 5 mg, you need multiple injections per dose. This concentration is becoming less common as pharmacies move toward higher concentrations for patient convenience.
10 mg/mL: the most common concentration
Ten units from a 10 mg/mL vial delivers exactly 1.0 mg of tirzepatide. This is the most widely prescribed concentration and the one most dosage charts reference by default.
At this concentration, the standard titration schedule looks clean on an insulin syringe. The 2.5 mg starting dose is 25 units. The 5 mg dose is 50 units. The 7.5 mg dose is 75 units. The 10 mg dose is 100 units, which is the full capacity of a 1 mL syringe. For doses above 10 mg, you either need a larger syringe or split the dose across two injections. Our 10 mg/mL dosage chart lays out every dose increment at this concentration.
17 mg/mL: the niacinamide formulations
Several pharmacies compound tirzepatide at 17 mg/mL, often combined with 2 mg/mL of niacinamide. At this concentration, 10 units delivers 1.7 mg of tirzepatide. The tirzepatide niacinamide combination is popular because niacinamide may help reduce injection site reactions and support metabolic function. If your vial specifies this formulation, make sure your conversion calculations use 17 mg/mL, not 10 or 20.
20 mg/mL: the concentrated formulation
Drawing 10 units from a 20 mg/mL vial gives you 2.0 mg of tirzepatide. Nearly a full starting dose from just 10 units. This concentration cuts injection volumes in half compared to 10 mg/mL, which makes higher doses much more comfortable. The 20 mg/mL dosing chart shows that the 15 mg maximum dose requires only 75 units instead of 150.
The downside? Small measurement errors have bigger consequences. Drawing one extra unit at 20 mg/mL adds 0.2 mg to your dose. At 10 mg/mL, one extra unit only adds 0.1 mg. Precision becomes twice as important with the more concentrated formulation.
40 mg/mL: the ultra-concentrated formulation
At 40 mg/mL, 10 units delivers a full 4.0 mg of tirzepatide. This is a substantial dose from a tiny volume. The 40 mg/mL concentration is typically reserved for patients on higher maintenance doses, and it requires extremely careful measurement. One unit off means 0.4 mg of dosing error. Most tirzepatide dose charts recommend using 0.3 mL syringes with fine graduations when working with this concentration.
The science behind tirzepatide dosing: why milligrams matter at every level
Understanding why the exact milligram amount in your 10-unit draw matters requires knowing how tirzepatide works at the molecular level. Tirzepatide is a dual GIP/GLP-1 receptor agonist. That means it activates two different receptor types simultaneously, the glucose-dependent insulinotropic polypeptide (GIP) receptor and the glucagon-like peptide-1 (GLP-1) receptor. The degree of activation at each receptor depends directly on how many milligrams reach your bloodstream after injection.
At sub-therapeutic levels like 0.5 mg (10 units from a 5 mg/mL vial), receptor activation is minimal. The molecules bind to some receptors, but not enough to trigger the cascade of effects that produce appetite suppression, improved insulin sensitivity, and the metabolic changes that drive weight loss. Think of it like turning a dimmer switch. Half a milligram barely moves the dial. Two milligrams turns it noticeably. Five milligrams and above cranks it toward full effect.
The GIP receptor component is what makes tirzepatide unique compared to semaglutide and other pure GLP-1 agonists. GIP receptor activation enhances fat metabolism, improves lipid profiles, and may contribute to the superior weight loss results seen in clinical trials. But GIP receptor engagement requires sufficient drug concentration at the receptor sites, which ties directly back to your milligram dose. This is the reason why getting your 10-unit conversion right is not just an academic exercise. It determines whether you are actually activating the mechanisms that make tirzepatide work.
Dose-response relationship in clinical trials
The SURMOUNT clinical trial program tested tirzepatide at 5 mg, 10 mg, and 15 mg weekly doses. At 5 mg, participants lost an average of approximately 15% of body weight over 72 weeks. At 10 mg, that increased to around 19.5%. At 15 mg, weight loss reached approximately 20.9%. The pattern is clear: higher doses produce greater effects, though with diminishing returns at the top end.
Below 2.5 mg (the starting dose), no large-scale clinical data exists. This means that a 10-unit dose delivering 1.0 mg from a 10 mg/mL vial operates in uncharted territory from a research perspective. It does not mean the dose is useless or dangerous, but it does mean that expectations should be calibrated accordingly. The timeline for tirzepatide to work is established for standard doses, not sub-therapeutic ones.
Pharmacokinetics and injection volume
Tirzepatide has a half-life of approximately five days, which is why it works as a once-weekly injection. After subcutaneous injection, the medication absorbs from the injection site into the bloodstream over several hours. The rate of absorption can vary slightly based on injection volume, injection site, and individual factors like body composition.
Smaller injection volumes (like the 0.1 mL from a 10-unit draw) tend to absorb slightly faster than larger volumes. At higher concentrations, this means the same milligram dose delivered in a smaller volume may produce a slightly different absorption profile than a lower concentration requiring more volume. In practice, this difference is clinically insignificant for most people. But it helps explain why some users report slightly different experiences between concentration switches, even when the milligram dose remains the same.
The injection site also affects absorption. Abdominal injections typically absorb faster than thigh injections. The stomach injection guide covers optimal technique for the most consistent absorption patterns.
When drawing 10 units makes sense in a tirzepatide protocol
Not every dose involves round numbers on the syringe. Ten units is a specific amount that serves different purposes depending on your concentration and protocol stage.
Microdosing protocols
Some researchers use 10 units as part of a microdosing tirzepatide protocol. At 10 mg/mL, that delivers 1.0 mg, which is below the standard starting dose of 2.5 mg but above the ultra-low microdose range. The microdose schedule typically starts lower and builds gradually.
At 5 mg/mL, 10 units gives just 0.5 mg. Some practitioners use this as an introductory dose for patients who are particularly sensitive to GLP-1 side effects or who want to assess tolerance before committing to the standard titration. While clinical trial data on sub-2.5 mg doses is limited, the approach has gained traction in clinical practice.
Titration adjustments
During the standard tirzepatide weight loss timeline, doses increase every four weeks. But some providers adjust in smaller increments. Instead of jumping from 2.5 mg to 5 mg, they might go to 3.5 mg first. At 10 mg/mL, that 3.5 mg dose requires 35 units. A 10-unit draw (1.0 mg) could serve as a supplemental mid-week dose in some protocols, though split dosing strategies vary widely.
Testing a new vial
When receiving a vial from a new pharmacy or a different concentration than what you have used before, drawing a small test amount makes sense. Ten units is enough volume to verify the liquid draws smoothly, check for particulates, and assess the solution clarity. Before drawing your actual dose, this practice helps catch problems with vial integrity, contamination, or reconstitution errors.
Converting other common unit amounts to milligrams
Understanding the 10-unit conversion is great. But you will likely draw different amounts throughout your protocol. Here is how the math works for the most commonly drawn unit amounts at the two most popular concentrations.
At 10 mg/mL (most common)
Units drawn | Volume (mL) | Tirzepatide (mg) | Standard dose equivalent |
|---|---|---|---|
5 units | 0.05 mL | 0.5 mg | Sub-therapeutic (microdose) |
10 units | 0.10 mL | 1.0 mg | Sub-therapeutic (low microdose) |
25 units | 0.25 mL | 2.5 mg | Standard starting dose |
50 units | 0.50 mL | 5.0 mg | Second titration step |
75 units | 0.75 mL | 7.5 mg | Third titration step |
100 units | 1.00 mL | 10.0 mg | Fourth titration step |
For other specific unit conversions at this concentration, see our guides on 20 units to mg, 30 units to mg, 40 units to mg, and 50 units to mg.
At 20 mg/mL (concentrated)
Units drawn | Volume (mL) | Tirzepatide (mg) | Standard dose equivalent |
|---|---|---|---|
5 units | 0.05 mL | 1.0 mg | Sub-therapeutic |
10 units | 0.10 mL | 2.0 mg | Near starting dose |
12.5 units | 0.125 mL | 2.5 mg | Standard starting dose |
25 units | 0.25 mL | 5.0 mg | Second titration step |
37.5 units | 0.375 mL | 7.5 mg | Third titration step |
50 units | 0.50 mL | 10.0 mg | Fourth titration step |
75 units | 0.75 mL | 15.0 mg | Maximum dose |
Notice how 10 units at 20 mg/mL gives you 2.0 mg, almost an entire starting dose. At 10 mg/mL, you would need 25 units to get that same 2.5 mg. The concentration makes all the difference. Compare these numbers against the 25-unit conversion guide to see how the same syringe marking delivers wildly different doses across concentrations.
Common mistakes when measuring 10 units of tirzepatide
Getting the measurement right sounds simple. Ten units. Read the syringe. Done. In practice, several errors occur with alarming frequency, and any one of them can throw off your entire protocol.
Mistake 1: assuming all vials are the same concentration
This is the most dangerous error. You get comfortable drawing 25 units for your 2.5 mg dose from a 10 mg/mL vial. Your pharmacy sends a new vial. You draw 25 units out of habit. But the new vial is 20 mg/mL. You just injected 5 mg instead of 2.5 mg. Double the dose. This mistake explains a significant portion of the side effect reports where people suddenly experience intense headaches, severe constipation, or debilitating fatigue after what they thought was their normal dose.
Every time you receive a new vial, read the label. Confirm the concentration. Recalculate your units if anything has changed.
Mistake 2: reading the syringe from the wrong reference point
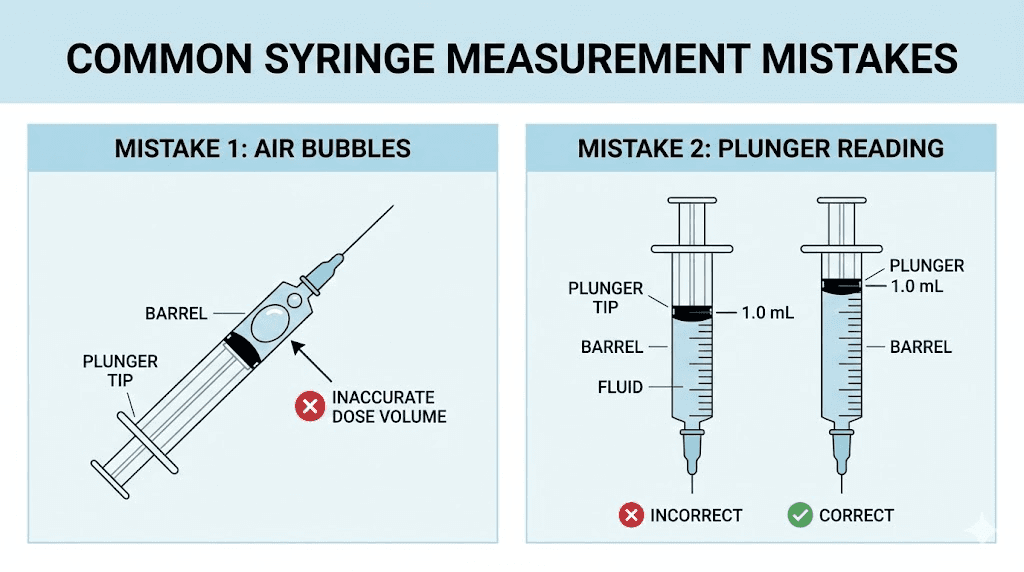
Insulin syringes have a rubber plunger tip that creates a slight optical illusion. The top edge of the plunger and the bottom edge can differ by about one unit. Always read from the top edge of the rubber plunger where it meets the barrel of the syringe. Reading from the wrong edge at 10 units could mean actually drawing 9 or 11 units. At 20 mg/mL, that one-unit difference changes your dose by 0.2 mg. Over weeks of consistent dosing, these small errors compound.
Mistake 3: air bubbles reducing the actual dose
Air bubbles take up space in the syringe without contributing any medication. If you draw to 10 units but there is a visible air bubble in the barrel, you have less than 0.1 mL of actual solution. The injection will still "feel" the same, but you received less tirzepatide than intended.
Fix this by tapping the syringe gently with the needle pointing up, pushing the air bubble to the top, and then pushing the plunger to expel it. Redraw to your 10-unit mark. The GLP-1 injection guide walks through proper technique step by step.
Mistake 4: using the wrong syringe type
We covered TB syringes earlier, but there is another issue. Some U-100 syringes have different total capacities. A 30-unit (0.3 mL) syringe has finer markings than a 100-unit (1 mL) syringe. Drawing 10 units on a 100-unit syringe is harder to see precisely than on a 30-unit syringe. For small doses like 10 units, always use the smallest syringe available for the most accurate measurement. Proper syringe selection is covered in detail in our tirzepatide syringe dosage guide.
Mistake 5: not accounting for dead space
Every syringe has "dead space," a tiny volume between the needle hub and the plunger that retains liquid after injection. In standard insulin syringes, this is typically 0.01 to 0.05 mL (1-5 units). When drawing small volumes like 10 units, this dead space can represent a significant percentage of your total dose. Low-dead-space syringes minimize this issue. If accuracy at small volumes matters to your protocol, investing in quality syringes is worth the cost.
How to verify your concentration before drawing 10 units
Never assume. Always verify. Here is the systematic approach to confirming your vial concentration before every injection session.
Step 1: read the vial label
The concentration is printed on the vial label in mg/mL format. Look for numbers like "10 mg/mL" or "20 mg/mL." Some labels list the total contents differently, showing "30 mg/3 mL" instead of "10 mg/mL." Both mean the same thing. Divide the total milligrams by the total milliliters to get your concentration.
Step 2: check the pharmacy documentation
Your compounding pharmacy should provide dosing instructions specific to the concentration they sent. These instructions should specify the units to draw for each milligram dose. Compare their chart against your own calculations using the formula above. If they do not match, call the pharmacy before injecting. Our guide on compounded tirzepatide dosage calculation can help you double-check their numbers.
Step 3: cross-reference with your provider
Your prescribing provider should know both the milligram dose they prescribed and the concentration of the vial you received. If your provider says "draw 25 units" but your vial is 20 mg/mL, that translates to 5 mg, not 2.5 mg. Ask them to confirm the milligram dose, then calculate the units yourself using the formula. Never follow unit-based instructions without knowing the concentration they were calculated for.
Step 4: mark your vial
Write the concentration on the vial with a permanent marker or attach a label. When you store multiple vials in the refrigerator, clear labeling prevents the dangerous mistake of grabbing the wrong concentration. Include the date opened and the expiration information as well.
Storage and handling factors that affect your 10-unit dose accuracy
Even with perfect measurement technique, storage and handling issues can change the actual amount of active tirzepatide in your 10-unit draw.
Temperature degradation
Tirzepatide is a peptide, and peptides degrade when exposed to heat. A vial that gets warm loses potency over time. Your syringe might show 10 units at 10 mg/mL, which should be 1.0 mg. But if the tirzepatide has partially degraded, the actual active ingredient could be less. Proper storage according to the refrigeration guidelines preserves the accuracy of your dose calculations.
Most compounded tirzepatide should be stored at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Leaving it at room temperature for extended periods reduces potency. The guidelines for tirzepatide outside the fridge specify maximum allowable time at room temperature, which varies by formulation.
Reconstitution accuracy
If your tirzepatide arrives as a lyophilized (freeze-dried) powder, the concentration depends entirely on how much bacteriostatic water you add. Add 1 mL of water to a 10 mg vial and you get 10 mg/mL. Add 2 mL and you get 5 mg/mL. The reconstitution chart shows exactly how different water volumes create different concentrations.
Getting the water measurement wrong during reconstitution means every subsequent dose will be off. If you aim for 10 mg/mL but actually create 8 mg/mL because you added slightly too much water, your 10-unit draw delivers 0.8 mg instead of 1.0 mg. Over a multi-week protocol, that 20% error accumulates. The peptide reconstitution calculator eliminates guesswork from this step.
Vial age and beyond-use dating
Compounded tirzepatide has a beyond-use date (BUD) set by the pharmacy. As the vial ages, peptide degradation occurs even under ideal storage conditions. A vial near its expiration may contain less active tirzepatide per milliliter than a fresh vial, effectively lowering the true concentration below what the label states. This is why following tirzepatide expiration guidelines matters for dosing accuracy, not just safety.
FDA-approved tirzepatide doses versus compounded unit conversions
Understanding where 10 units falls within the broader tirzepatide dosing landscape helps contextualize your protocol.
The FDA-approved dose range
Mounjaro and Zepbound, the brand-name tirzepatide products, come in pre-filled pens at six fixed doses: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, and 15 mg. Each pen delivers 0.5 mL of solution, regardless of the dose. The concentrations inside the pens vary to achieve different doses in the same volume. A 2.5 mg pen contains a 5 mg/mL solution. A 15 mg pen contains a 30 mg/mL solution.
With pre-filled pens, you never need to calculate units. The device handles everything. But pre-filled pens cost significantly more than compounded vials, which is why many people turn to affordable compounded tirzepatide options and manage their own unit-based dosing.
Where 10 units fits in standard titration
The standard titration starts at 2.5 mg for four weeks, then increases by 2.5 mg every four weeks up to the maintenance dose (maximum 15 mg). At 10 mg/mL, the 10-unit draw of 1.0 mg does not correspond to any standard titration step. It sits between zero and the starting dose. This means 10 units at 10 mg/mL is primarily relevant for microdosing, dose splitting, or situations where someone is on a 20 mg/mL vial and 10 units delivers their 2.0 mg target.
For the full titration schedule in units, our dosing chart covers every step from initiation through maximum dose at all concentrations.
How compounded concentrations map to FDA doses
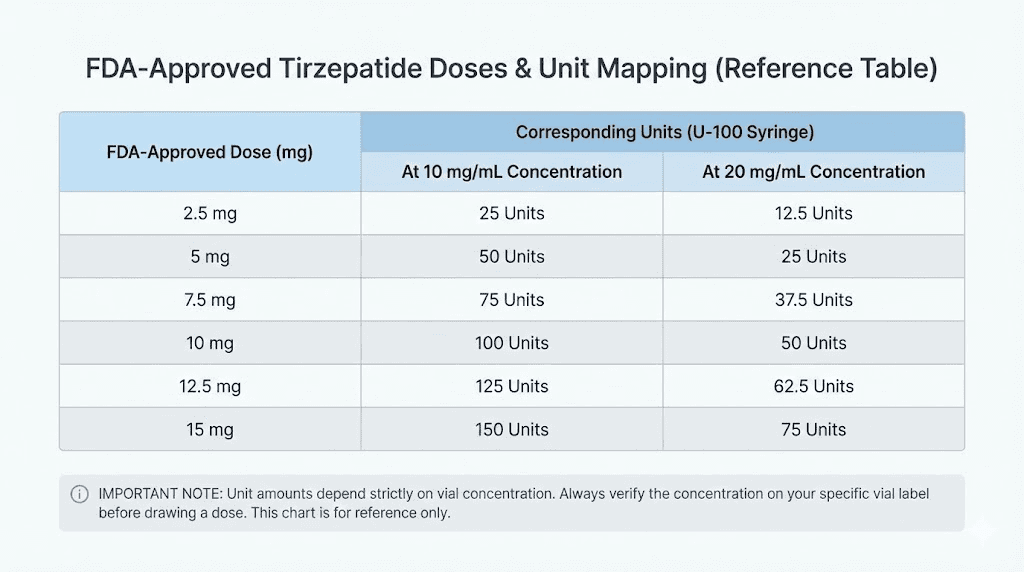
FDA dose | Units needed (5 mg/mL) | Units needed (10 mg/mL) | Units needed (20 mg/mL) | Units needed (40 mg/mL) |
|---|---|---|---|---|
2.5 mg | 50 units | 25 units | 12.5 units | 6.25 units |
5.0 mg | 100 units | 50 units | 25 units | 12.5 units |
7.5 mg | 150 units | 75 units | 37.5 units | 18.75 units |
10 mg | 200 units | 100 units | 50 units | 25 units |
12.5 mg | 250 units | 125 units | 62.5 units | 31.25 units |
15 mg | 300 units | 150 units | 75 units | 37.5 units |
This table reveals why higher concentrations become necessary at higher doses. At 5 mg/mL, the 10 mg dose requires 200 units, which is 2 mL. That is beyond the capacity of a standard insulin syringe and would require either two separate injections or a different syringe type entirely. The tirzepatide versus semaglutide dosage comparison shows similar scaling challenges across both medications.
What happens if you switch concentrations without recalculating
This scenario deserves its own section because it causes real problems for real people every week.
The accidental dose doubling
You have been on 10 mg/mL for months. Your dose is 5 mg, so you draw 50 units every week like clockwork. Your pharmacy runs out of 10 mg/mL and sends 20 mg/mL instead. They may or may not include updated dosing instructions. You draw 50 units out of muscle memory.
At 20 mg/mL, 50 units delivers 10 mg. You just doubled your dose. Within hours, you might experience severe nausea, vomiting, intense muscle pain, overwhelming anxiety, or extreme body aches. These side effects correspond to a dose jump that your body was not prepared for.
The accidental underdosing
The reverse happens too. You switch from 20 mg/mL to 10 mg/mL without recalculating. Your 12.5-unit draw for 2.5 mg at 20 mg/mL now gives you only 1.25 mg at 10 mg/mL. Half your intended dose. You might wonder why tirzepatide suddenly stopped working, your appetite returned, or you stopped losing weight. Before assuming the medication is the problem, check whether your concentration changed. Our guide on tirzepatide not working anymore covers this as one of the first troubleshooting steps.
How to safely transition between concentrations
When your pharmacy sends a different concentration, stop. Do not draw from the new vial until you have recalculated your units using the formula. Write the new unit amount on a piece of paper. Tape it to the vial. For the first injection from a new concentration, some providers recommend having someone else double-check your calculation.
If you are switching from tirzepatide to semaglutide or between different medications entirely, the conversions become even more complex. Each medication has its own concentration standards. The conversion charts between medications can help, but always verify with your provider.
How 10 units of tirzepatide compares to semaglutide conversions
Many people compare tirzepatide and semaglutide, and understanding how unit measurements translate between the two medications provides useful context.
Semaglutide is typically compounded at different concentrations than tirzepatide. Common semaglutide concentrations include 1 mg/mL, 2.5 mg/mL, and 5 mg/mL. At 5 mg/mL (the most common), 10 units of semaglutide equals 0.5 mg. At 2.5 mg/mL, 10 units delivers only 0.25 mg.
The key difference is that semaglutide doses are much smaller than tirzepatide doses. The standard semaglutide maintenance range is 0.25 to 2.4 mg per week, while tirzepatide ranges from 2.5 to 15 mg per week. So 10 units of semaglutide at 5 mg/mL (0.5 mg) represents a higher percentage of the typical semaglutide dose range than 10 units of tirzepatide at 10 mg/mL (1.0 mg) represents within the tirzepatide range.
For a detailed comparison of dosing between the two medications, see our semaglutide versus tirzepatide comparison. The semaglutide dosage in units guide covers the equivalent calculations for that medication, and semaglutide units to mg conversions follow the same formula with different typical concentrations.
Practical tips for accurate 10-unit tirzepatide dosing
Use proper lighting
Reading syringe markings in dim lighting leads to measurement errors. Always prepare injections under bright, direct light. Hold the syringe at eye level with the light source behind you. The liquid line should be clearly visible against the syringe markings. This matters more at small volumes like 10 units where one marking off means a larger percentage error.
Keep a dosing log
Record every injection: date, concentration, units drawn, calculated milligrams, and any notes about how you felt. This log helps you catch patterns, verify accuracy over time, and provides essential information for your provider at follow-up appointments. It also creates a record you can reference if your pharmacy switches your concentration, so you know exactly when the change happened relative to any symptom changes.
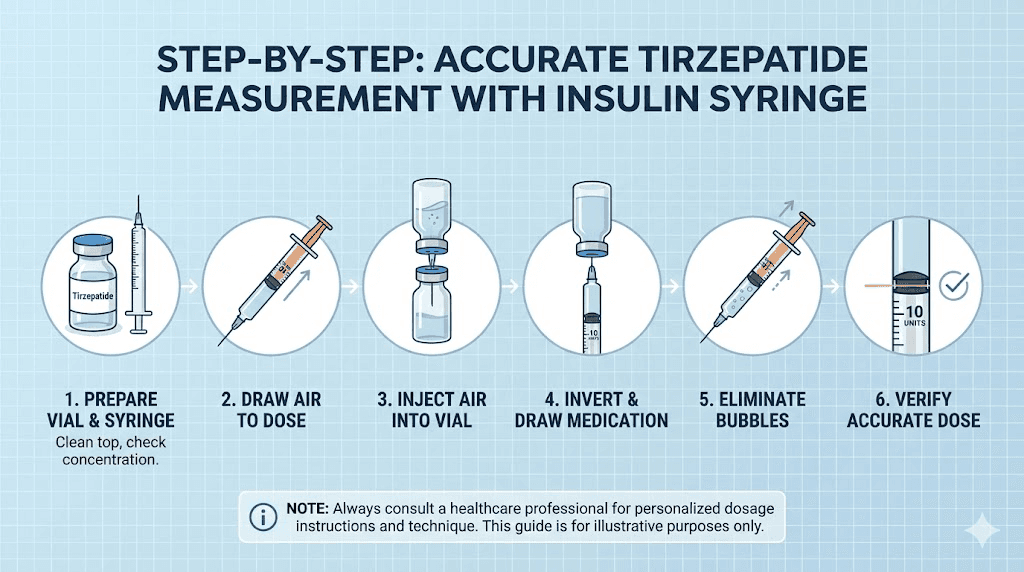
Set up a pre-injection checklist
Before drawing any dose, run through this sequence. Check the vial label for concentration. Calculate the units needed for your prescribed milligram dose. Verify the syringe type (U-100 insulin only). Draw the medication, checking for air bubbles. Confirm the final volume reads correctly. This takes 30 seconds and prevents errors that could affect weeks of progress.
Consider a dosing calculator
SeekPeptides offers a peptide calculator that handles the math for you. Input your concentration and desired dose, and it tells you exactly how many units to draw. This eliminates arithmetic errors and provides a safety check against your manual calculations. Some researchers keep the calculator bookmarked on their phone and run it every injection day as part of their routine.
Never eyeball sub-10-unit measurements
If your protocol requires drawing less than 10 units, use a syringe with 0.5-unit markings. Standard 1 mL syringes often have 2-unit increments, making anything between the markings a guess. A 0.3 mL syringe with 0.5-unit graduations gives you the precision needed for small volumes. This is especially important when working with higher concentration vials where even half a unit represents a meaningful amount of medication.
Advanced conversion scenarios
Splitting doses across the week
Some providers prescribe twice-weekly dosing to reduce side effects. If your weekly dose is 5 mg and you split it into two injections, each injection should be 2.5 mg. At 10 mg/mL, that is 25 units per injection. At 20 mg/mL, that is 12.5 units per injection. Splitting does not change the total weekly milligrams, but it does change the units per injection, and the smaller individual draws require more precise measurement.
Transitioning from pens to vials
If you previously used Mounjaro or Zepbound pre-filled pens and are switching to compounded vials, you need to translate your pen dose into units for your specific vial concentration. A 5 mg pen delivered exactly 5 mg with no math required. From a 10 mg/mL vial, that same 5 mg requires drawing 50 units. From a 20 mg/mL vial, 25 units. The complete dosage chart in units maps every pen dose to its equivalent vial measurement.
Adjusting for compounded formulations with additives
Many compounded tirzepatide formulations include additional compounds. Tirzepatide with glycine and B12 is one common combination. Tirzepatide with methylcobalamin is another. These additives do not change the tirzepatide concentration listed on the label. If your vial says 10 mg/mL tirzepatide with 1 mg/mL B12, the tirzepatide conversion math remains the same. Ten units still equals 1.0 mg of tirzepatide. You also get 0.1 mg of B12 in that same draw, but that does not affect the tirzepatide calculation.
Partial vial calculations
Compounded vials come in various sizes, commonly 2 mL, 3 mL, 4 mL, and 5 mL. A 2 mL vial at 10 mg/mL contains 20 mg total. If you draw 10 units (1.0 mg) per week, that vial lasts 20 weeks at that dose. But most people use higher doses. At 25 units (2.5 mg) per week, the same vial lasts 8 weeks. Tracking how many doses remain helps you order refills before running out and prevents the temptation to squeeze extra draws from an empty or near-empty vial. The peptide cost calculator can help you figure out cost per dose based on your vial size and concentration.
When to consult your provider about tirzepatide unit dosing
Self-calculating units is a necessary skill for anyone using compounded tirzepatide. But certain situations require professional guidance.
Contact your provider if your pharmacy changes your concentration without explanation. Contact them if the units your provider prescribed do not match the milligrams when you run the formula. Contact them if you accidentally injected the wrong dose. Contact them if your side effects suddenly change intensity without a dose change, which could indicate a concentration error.
Also consult your provider before making any dose adjustments on your own. The expected weight loss timeline varies by individual, and slower progress does not necessarily mean the dose needs increasing. Providers consider multiple factors beyond the scale when adjusting tirzepatide protocols.
SeekPeptides members get access to comprehensive dosing guides, protocol databases, and community support from experienced researchers who have navigated these exact dosing questions. For those managing their own compounded tirzepatide protocols, having a reliable resource to verify calculations and troubleshoot issues makes the difference between effective dosing and costly mistakes.
Tirzepatide dosing at 10 units for different goals
Weight loss protocols
For weight loss, 10 units at 10 mg/mL (1.0 mg) falls below the standard starting dose. However, some practitioners use this as a pre-titration assessment phase. The idea is to introduce the medication at a sub-therapeutic level to gauge individual tolerance before committing to the full weight loss dosing schedule. Results from these low-dose introductory periods vary widely. Most clinical weight loss data comes from the standard 2.5 mg starting dose and above.
At 20 mg/mL, however, 10 units delivers 2.0 mg. This is close enough to the 2.5 mg starting dose that some providers round up or down within this range based on patient sensitivity. The before and after results page shows outcomes from various dosing strategies.
Appetite suppression
The appetite suppression effects of tirzepatide are dose-dependent. At 1.0 mg (10 units from a 10 mg/mL vial), some people report mild appetite changes, while others notice nothing. The dual GIP/GLP-1 receptor activation that makes tirzepatide effective requires sufficient dosing to meaningfully engage both receptor pathways. Most people need at least the 2.5 mg starting dose to experience noticeable appetite changes.
Metabolic effects
Beyond weight loss, tirzepatide affects blood sugar regulation, insulin sensitivity, and metabolic rate. These effects also scale with dose. A 10-unit dose at lower concentrations provides minimal metabolic impact. At higher concentrations where 10 units delivers 2 mg or more, measurable metabolic changes become more likely. The relationship between dose and metabolic response is not perfectly linear, which is why tirzepatide onset timing varies between individuals.
Comparing 10-unit tirzepatide doses across pharmacy providers
Different compounding pharmacies ship different concentrations, which means the same "10-unit" measurement can have very different outcomes depending on where your vial comes from.
Empower Pharmacy commonly ships tirzepatide at multiple concentrations, and their dosage chart specifies which concentration applies to their instructions. Southend Pharmacy has its own concentration standards. Olympia Pharmacy uses yet another approach. The Mochi platform and Strive each work with their own compounding partners and concentration specifications.
The takeaway is straightforward. Do not follow a dosing chart from one pharmacy when using a vial from another. Every pharmacy-specific chart assumes a particular concentration. Using the wrong chart is functionally identical to using the wrong concentration, and it leads to the same dosing errors.
Tirzepatide forms beyond injectable vials
Tirzepatide is not limited to injectable formulations. Understanding how unit measurements relate to other delivery methods provides useful perspective.
Oral tirzepatide
Oral tirzepatide is dosed in milligrams directly, with no unit conversion needed. Oral tablets come in fixed strengths, and the dosing is much more straightforward than vials. However, oral bioavailability differs from injectable bioavailability, meaning the milligram dose for oral and injectable forms is not directly interchangeable. The oral versus injection comparison covers these differences in detail.
Sublingual tirzepatide
Sublingual formulations are dosed by volume using a dropper, not by syringe units. The tirzepatide drops guide explains this alternative delivery method, and the sublingual dosage chart provides concentration-specific instructions. If you are comparing delivery methods, the tablets versus injections analysis covers the trade-offs.
Combining tirzepatide with other compounds
Many tirzepatide users combine it with supplements or other peptides. Understanding your base tirzepatide dose in milligrams matters when adding other compounds to the protocol.
Common combinations include tirzepatide with glycine for metabolic support, tirzepatide with glycine protocols, and tirzepatide with B12 for energy support. The supplements to take with tirzepatide guide covers what works well alongside the medication, while the B6 combination guide addresses another popular pairing.
Some people combine tirzepatide with phentermine or AOD-9604. Others add cagrilintide to their protocol. In every case, knowing your exact tirzepatide milligram dose (not just the units drawn) is essential for tracking what you are actually taking and discussing your full protocol with your provider.
Diet and lifestyle factors that interact with your tirzepatide dose
Your 10-unit dose, regardless of the milligram equivalent, works within the context of your overall routine. What you eat on tirzepatide affects how the medication performs. The tirzepatide diet plan provides structured guidance, and knowing which foods to avoid reduces the risk of unpleasant gastrointestinal side effects.
Proper nutrition becomes especially important at lower doses where the appetite suppression effect is milder. At 1.0 mg (10 units from 10 mg/mL), you are unlikely to experience the dramatic appetite reduction that higher doses provide. Combining sensible dietary choices from the tirzepatide meal plan with your medication protocol maximizes results regardless of dose level.
Alcohol consumption while on tirzepatide is another consideration. The guide on drinking while on tirzepatide addresses how alcohol interacts with the medication and whether it affects dosing efficacy.
Side effects relative to dose size
The relationship between dose and side effects is important context for anyone considering a 10-unit draw. At lower milligram amounts, side effects tend to be milder. But this relationship is not always linear, and individual variation plays a significant role.
At 1.0 mg (10 units from 10 mg/mL), most people experience minimal or no side effects. This sub-therapeutic dose is below the level where the majority of adverse effects manifest in clinical trials. The body has very little receptor activation to respond to, so the gastrointestinal and systemic effects that higher doses produce simply do not occur at meaningful levels. Some people report mild nausea or a slight change in appetite, but these reports are rare at doses this low.
As doses increase through the standard titration, side effects become more common and potentially more intense. The 2.5 mg starting dose is where most people first notice gastrointestinal changes. Nausea is the most frequently reported effect, occurring in roughly 12 to 18% of people at the starting dose based on trial data. By 5 mg, that percentage increases. At 10 mg and above, nausea, reduced appetite, and gastrointestinal symptoms are common enough that providers consider them expected rather than surprising.
Gastrointestinal side effects by dose level
The most commonly reported side effects across the full dosing range include constipation, diarrhea, nausea, vomiting, and abdominal discomfort. These symptoms typically peak during the first one to two weeks after each dose increase and then gradually improve as the body adjusts. The severity correlates with the size of each dose increase, not just the absolute dose. Jumping from 2.5 mg to 5 mg (a 100% increase) tends to cause more side effects than moving from 10 mg to 12.5 mg (a 25% increase).
This is relevant to the 10-unit question because accidental overdosing due to concentration confusion produces sudden, unexpected dose jumps. If you are stable at 5 mg and accidentally inject 10 mg because you grabbed a 20 mg/mL vial instead of your usual 10 mg/mL, you have doubled your dose without the gradual titration your body expects. The resulting side effects can be severe and alarming.
Non-gastrointestinal side effects
Headaches are reported across all dose levels, though they tend to be more frequent during the titration phase. Fatigue and insomnia can occur, sometimes paradoxically at the same dose level. Some people experience body aches or muscle pain, particularly during the first few weeks of treatment. Others report anxiety or mood changes.
Injection site reactions occur independent of dose. Whether you inject 10 units or 100 units, the skin and subcutaneous tissue respond to the needle itself, the volume of fluid, and the solution composition. Reactions are more common with certain formulations, particularly those containing niacinamide. The injection site reaction treatment guide covers management strategies including rotation patterns, ice application, and technique adjustments.
Hair loss and other less common effects
Some users report hair thinning during tirzepatide use, an effect also seen with rapid weight loss from any cause. The GLP-1 hair loss guide explores this connection in detail. Hair loss appears more related to the rate of weight loss than to the medication itself, meaning that higher doses producing faster weight loss may indirectly increase hair thinning risk. At a 10-unit dose delivering 1.0 mg or less, weight loss is unlikely to be rapid enough to trigger this effect.
For women, additional considerations include effects on menstrual cycles and the important question of fertility changes while on the medication. Weight loss itself can alter hormonal balance and menstrual patterns. Women who are breastfeeding face additional considerations regarding medication use during lactation. These effects have been reported across all dose levels and are not specific to any particular unit count.
Troubleshooting common dosing scenarios
Scenario 1: your pharmacy sent a different concentration than usual
You open your monthly shipment and notice the vial looks different. The label says 20 mg/mL instead of your usual 10 mg/mL. Your previous dose was 50 units for 5 mg. What do you do?
Recalculate immediately. At 20 mg/mL, 5 mg requires only 25 units, not 50. If you had drawn 50 units from the new vial, you would have injected 10 mg, double your prescribed dose. Call your pharmacy to confirm the concentration change was intentional. Some pharmacies switch concentrations based on stock availability without always providing clear notice. Then recalculate every dose using the formula: Units = (Desired mg / Concentration) x 100.
Scenario 2: you cannot tell if you drew exactly 10 units
The syringe markings are small. You think you are at 10, but it could be 9 or 11. This happens frequently, especially with 1 mL syringes where the individual unit markings are closely spaced.
First, consider switching to a 0.3 mL syringe. The same 10-unit mark is much easier to read because the markings are more spread out. Second, hold the syringe at eye level with the barrel horizontal. Light should come from behind you so you can clearly see the meniscus of the liquid against the markings. Third, if you are consistently struggling with accuracy at low volumes, a peptide injection pen might offer more precise dosing than a manual syringe.
Scenario 3: you drew 10 units but realized you needed 25
You already pulled 10 units but your prescribed dose requires 25 units. Do you push the liquid back into the vial and redraw, or draw additional liquid?
You can carefully draw additional liquid without removing the needle from the vial. Push the air out of the syringe, reinsert into the vial (if you removed it), invert the vial, and draw to the 25-unit mark. If you already removed the needle and exposed it to air, the safest option is to use a new syringe to avoid contamination risk. Never push medication back into the vial from a used syringe, as this can introduce contaminants that accelerate degradation of the remaining solution.
Scenario 4: you are unsure which vial you drew from
You have two vials in your fridge, one at 10 mg/mL and one at 20 mg/mL (perhaps left over from a prescription change). You drew 10 units but cannot remember which vial you used.
This is exactly why labeling matters. If you truly cannot determine which vial you drew from, the safest course is to not inject and prepare a fresh dose from a clearly identified vial. Discard the prepared syringe. Then label both vials clearly with a permanent marker. Going forward, keep only one concentration in your refrigerator at a time to eliminate this risk entirely.
Scenario 5: your results suddenly changed without a dose change
You have been stable at 50 units weekly for months with good results. Suddenly, your weight loss stalls, your appetite returns, and the medication seems ineffective. You did not change your unit amount.
Check three things immediately. First, did your pharmacy change your concentration? A new vial at 5 mg/mL instead of 10 mg/mL means your 50 units now delivers 2.5 mg instead of 5 mg, cutting your effective dose in half. Second, check the expiration date on your vial. An expired or degraded vial delivers less active medication regardless of what the label says. Third, consider whether the vial was exposed to heat or temperature excursions that could have degraded the peptide. Our guide on tirzepatide not working anymore covers additional troubleshooting steps beyond concentration issues.
Long-term dosing management and record keeping
Managing tirzepatide dosing is not a one-time calculation. It is an ongoing process that spans months or years of treatment. The people who get the best results are the ones who treat every injection with the same attention to detail as their first one.
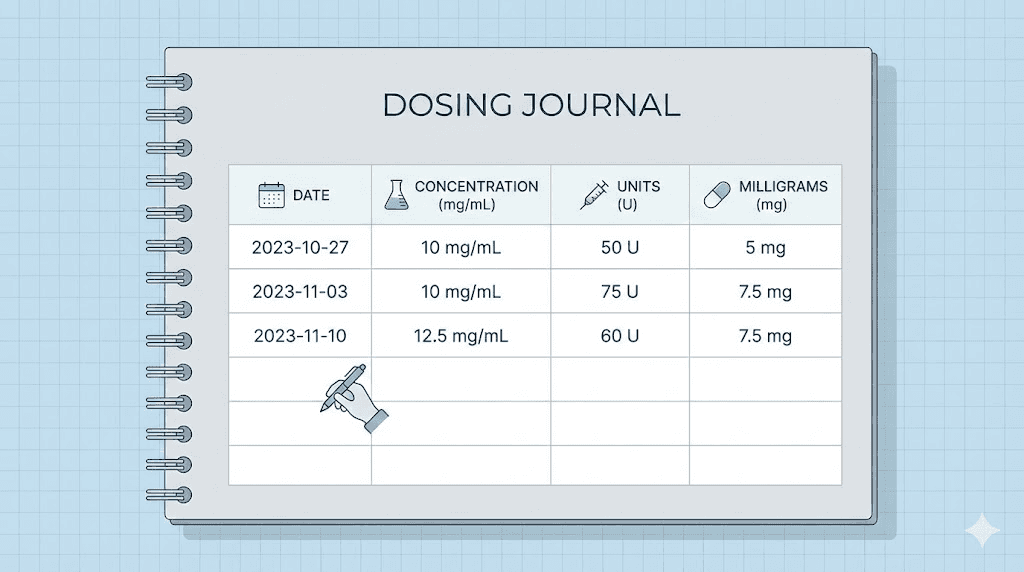
Creating a dosing journal
A simple notebook or spreadsheet with the following columns covers everything you need: date, vial concentration (mg/mL), units drawn, calculated milligrams, injection site used, and notes on how you felt in the following 48 hours. This journal becomes invaluable when you need to troubleshoot issues, discuss your protocol with your provider, or verify that a pharmacy change did not affect your results.
Over time, patterns emerge. You might notice that your appetite suppression is stronger when you inject in the abdomen versus the thigh. You might discover that certain foods trigger more side effects at certain doses. You might realize that your best results came during a specific dosing window. None of these insights are possible without consistent record keeping.
Planning for concentration changes
As your dose increases through the standard titration, you may eventually switch to a higher concentration vial. Planning for this transition prevents the accidental dosing errors discussed earlier. Before the switch, calculate your new unit amount at the new concentration. Write it down. Practice reading it on a dry syringe (without drawing medication) to confirm you can accurately identify the marking. Then make the switch with confidence.
Some providers manage this transition by overlapping vials, having you use the new concentration for a supervised injection at the clinic before sending you home with the new vials. If your provider does not offer this, you can create your own safety check by having someone verify your calculation and syringe reading for the first injection at a new concentration.
Traveling with tirzepatide
Maintaining dosing accuracy while traveling introduces additional challenges. Temperature control becomes critical, as tirzepatide outside the fridge degrades faster. You need to bring the right syringes, maintain your dosing journal, and potentially deal with different lighting conditions for syringe reading. Packing a small LED flashlight specifically for injection preparation is a practical tip that experienced travelers swear by. The peptide storage guide covers travel storage solutions in detail.
Building confidence with tirzepatide unit calculations
Understanding how many milligrams 10 units represents is just the beginning. The real goal is building confidence with the math so you never doubt whether you drew the right amount.
Practice the formula until it becomes automatic. (Units / 100) x Concentration = Milligrams. Run it for every injection, even when you think you remember the answer. Cross-check against a conversion chart or the calculator until the numbers feel intuitive.
Keep your resources bookmarked. The tirzepatide dosage in units guide, the dosage calculator, and the concentration-specific charts for 10 mg/mL and 20 mg/mL should be in your browser favorites. Pull them up every injection day until you no longer need them.
For researchers who want the most comprehensive dosing support available, SeekPeptides provides evidence-based protocol guides, verified conversion tools, and a community of thousands who have worked through these exact questions. Making accurate dosing decisions becomes much simpler when you have reliable resources at your fingertips.
Frequently asked questions
Is 10 units of tirzepatide the same as 10 mg?
No. Ten units is a volume measurement (0.1 mL), not a milligram measurement. The milligrams in 10 units depends on your vial concentration. At 10 mg/mL, 10 units equals 1.0 mg. At 20 mg/mL, 10 units equals 2.0 mg. Always check your concentration before calculating your dose. The 10 mg to units conversion shows how many units you actually need for a 10 mg dose.
What concentration do most compounding pharmacies use?
The most common compounding concentration is 10 mg/mL. However, 20 mg/mL and higher concentrations are increasingly popular for patients on higher maintenance doses. Always verify your specific vial rather than assuming a concentration. Our compound dosage chart covers calculations for all common concentrations.
Can I use 10 units as a starting dose?
At most concentrations, 10 units delivers less than the standard 2.5 mg starting dose. At 10 mg/mL, 10 units is only 1.0 mg. While some practitioners use sub-therapeutic introductory doses, the standard FDA-approved starting dose is 2.5 mg. The compounded tirzepatide starting dose guide discusses when lower starting doses might be appropriate.
How do I know if my pharmacy changed my concentration?
Check the vial label on every new shipment. Look for the mg/mL specification. Compare it to your previous vial. If it changed, recalculate your units before your next injection. Some pharmacies notify patients of concentration changes, but not all do. Keeping a dosing log helps you track changes over time.
Why do some charts show different numbers for 10 units?
Different charts assume different concentrations. A chart from Empower Pharmacy might assume 10 mg/mL while a chart from another provider assumes 20 mg/mL. The same unit amount converts to different milligrams at different concentrations. Always use a chart that matches YOUR vial concentration.
Is it safe to draw 10 units without knowing my concentration?
No. Drawing any amount without knowing your concentration is unsafe. At 40 mg/mL, 10 units delivers 4.0 mg, which is above the starting dose. At 5 mg/mL, it delivers only 0.5 mg. The eight-fold difference between these outcomes means guessing your concentration puts you at risk of significant overdosing or underdosing.
What is the smallest tirzepatide dose I can accurately measure?
With a 0.3 mL insulin syringe that has 0.5-unit graduations, you can reliably measure down to about 1-2 units. At 10 mg/mL, 2 units equals 0.2 mg. At lower concentrations, even smaller doses are possible. However, accuracy decreases with very small volumes, and clinical data on doses below 2.5 mg is limited. The microdosing chart provides guidance for sub-standard dose protocols.
Do I need a different syringe for 10 units than for 50 units?
You do not strictly need a different syringe, but you should use one. A 0.3 mL (30-unit) syringe gives much more precise readings at the 10-unit mark than a 1 mL (100-unit) syringe does. The finer graduations reduce measurement error. For 50 units, a 0.5 mL or 1 mL syringe works well. Matching syringe size to dose volume improves accuracy.
External resources
For researchers serious about getting their tirzepatide dosing right, SeekPeptides offers the most comprehensive conversion tools, protocol databases, and community support available, with evidence-based guides and verified calculators that remove the guesswork from every injection.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your concentrations stay verified, and your protocols stay consistent.