Feb 11, 2026

You have a vial of compounded tirzepatide sitting on your counter. Your protocol says 7.5 mg this week. You pick up the insulin syringe and stare at the unit markings. How far do you draw back? 75 units? 37.5 units? Something else entirely? The answer depends on one critical detail that most dosing guides gloss over, and getting it wrong means you either underdose or double your intended amount.
This is not a hypothetical problem. Researchers moving from the 5 mg dose to 7.5 mg hit this exact confusion every single day. The 7.5 mg step sits right in the middle of the tirzepatide dose escalation schedule, and it is the point where concentration differences between compounded formulations start creating real measurement challenges. A 10 mg/mL vial and a 20 mg/mL vial require completely different unit draws for the same 7.5 mg dose. Mix them up and you are either getting half your dose or twice your dose.
This guide breaks down every possible concentration scenario for 7.5 mg of tirzepatide. You will find the exact unit conversions, the math behind them, syringe selection tips, and practical strategies for making the 7.5 mg transition as smooth as possible. Whether you are working with a standard 10 mg/mL formulation, a concentrated 20 mg/mL version, or something else entirely, the conversion formula stays the same. Learn it once and you will never second-guess a draw again.
The universal formula for converting 7.5 mg to units
Every tirzepatide unit conversion starts with the same two-step formula. It does not matter what concentration you have. It does not matter what pharmacy compounded it. The math is identical every time.
Step one: Divide your dose in milligrams by your vial concentration in mg/mL. This gives you the volume in milliliters.
Step two: Multiply that volume by 100. This gives you the number of units on a standard insulin syringe.
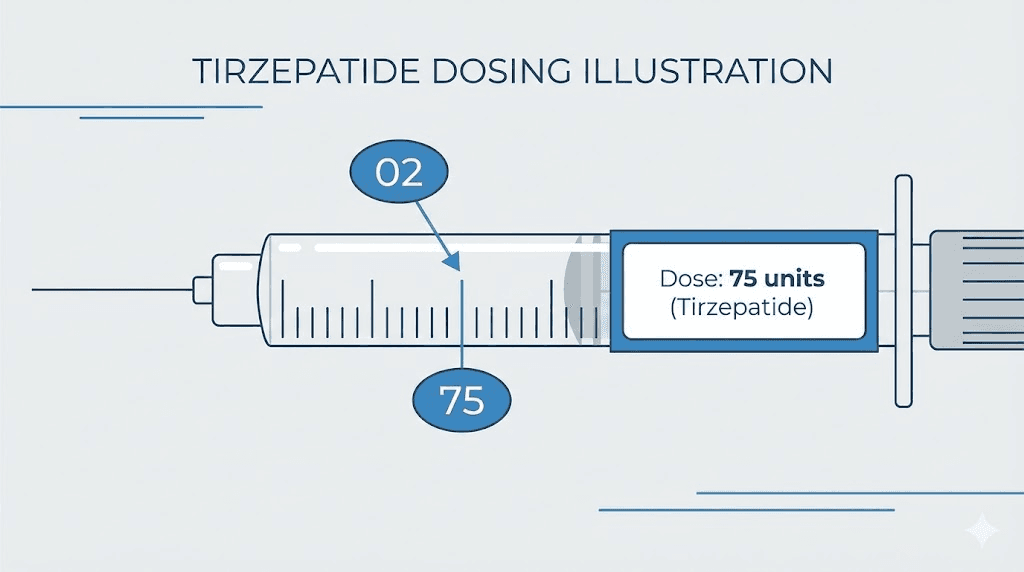
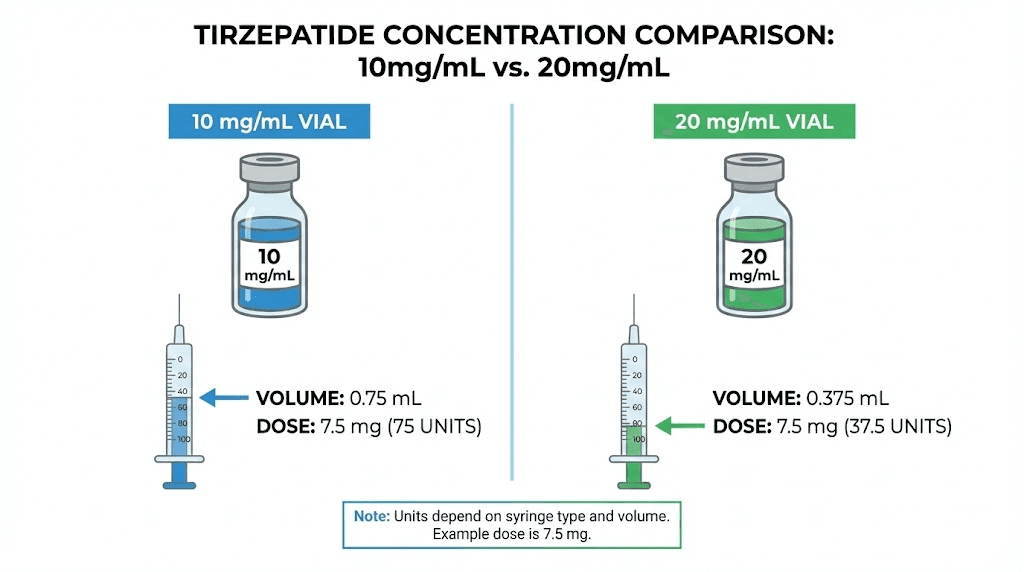
That is it. Two steps. For 7.5 mg of tirzepatide at a 10 mg/mL concentration, the calculation looks like this: 7.5 divided by 10 equals 0.75 mL. Then 0.75 times 100 equals 75 units. You draw to the 75 unit line on your syringe.
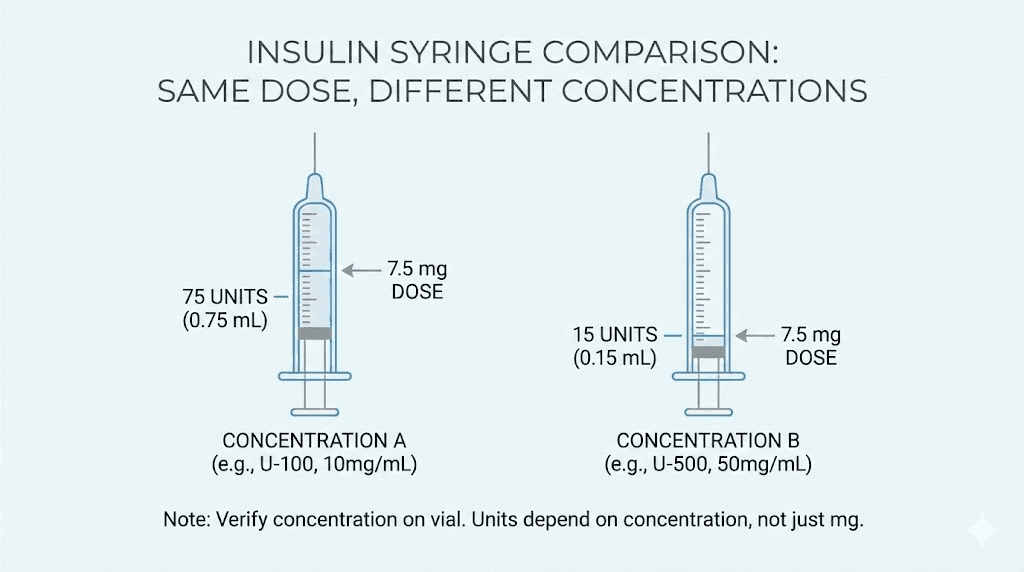
For a 20 mg/mL concentration, the same dose changes dramatically: 7.5 divided by 20 equals 0.375 mL. Then 0.375 times 100 equals 37.5 units. That is less than half the volume of the 10 mg/mL version. Same dose. Completely different syringe draw.
The formula works because insulin syringe units are just a way of measuring volume. One hundred units on an insulin syringe equals exactly one milliliter. So when you know the volume you need, converting to units is simple multiplication. The confusion comes not from the math itself but from the fact that compounded tirzepatide ships in multiple concentrations, and each one requires a different draw volume for the same milligram dose.
Write this formula down. Tape it to your vial. Save it in your phone. Every single time you prepare a dose, you should be running this calculation against the concentration printed on your specific vial label.
7.5 mg conversion chart for every common concentration
Different compounding pharmacies use different concentrations. Some ship 5 mg/mL. Others use 10 mg/mL. Many have moved to 20 mg/mL to reduce injection volume. A few specialty pharmacies even compound at 40 mg/mL. Each one changes the number of units you draw for your 7.5 mg dose.
Here is the complete breakdown:
Vial concentration | Volume for 7.5 mg | Units on insulin syringe | Best syringe size |
|---|---|---|---|
5 mg/mL | 1.50 mL | 150 units | 3 mL syringe (not insulin) |
10 mg/mL | 0.75 mL | 75 units | 1 mL (100 unit) insulin syringe |
15 mg/mL | 0.50 mL | 50 units | 0.5 mL (50 unit) or 1 mL syringe |
17 mg/mL | 0.44 mL | 44 units | 0.5 mL (50 unit) insulin syringe |
20 mg/mL | 0.375 mL | 37.5 units | 0.5 mL (50 unit) insulin syringe |
30 mg/mL | 0.25 mL | 25 units | 0.3 mL (30 unit) insulin syringe |
40 mg/mL | 0.1875 mL | 18.75 units | 0.3 mL (30 unit) insulin syringe |
Notice the massive range. At the lowest concentration, you need 150 units, which will not even fit in a standard insulin syringe. At the highest, you need fewer than 19 units. Same 7.5 mg dose, wildly different draws. This is why knowing your exact concentration is not optional. It is the single most important detail in your dosing protocol.
If you have worked with 2.5 mg doses or 5 mg doses before, the 7.5 mg step requires recalculating. Do not assume you can just add a proportional amount to your previous draw. Run the formula fresh every time you change doses.
Why concentration changes everything
Concentration is the amount of active tirzepatide dissolved in each milliliter of solution. A vial labeled 10 mg/mL contains 10 milligrams of tirzepatide in every single milliliter of liquid. A vial labeled 20 mg/mL contains twice as much medication in the same volume.
Think of it like coffee. A regular cup has one scoop per cup of water. A double-strength cup has two scoops per cup. If someone tells you to consume one scoop of coffee, you drink a full cup of regular or half a cup of double-strength. The amount of coffee is identical. The volume you drink is not.
Tirzepatide works the same way. Your prescribed dose is always in milligrams. The concentration determines how much liquid contains those milligrams.
This matters enormously for the 7.5 mg dose because it falls at a point in the tirzepatide dosing schedule where many people are switching between vial strengths. You might start with a 10 mg/mL vial for your 2.5 mg and 5 mg phases, then receive a 20 mg/mL vial when your pharmacy updates its formulation. If you draw the same number of units you used before without checking the new concentration, you will overdose.
The most common concentration scenario researchers encounter is the shift from 10 mg/mL to 20 mg/mL. At 10 mg/mL, your 7.5 mg dose requires 75 units. At 20 mg/mL, the same dose requires only 37.5 units. Drawing 75 units from a 20 mg/mL vial would give you 15 mg, exactly double what you intended. That kind of error can cause significant side effects and discomfort.
Always check the label. Every time. No exceptions.
How to find your concentration
Your vial label will display the concentration as a number followed by mg/mL. Common formats include:
10 mg/mL or 10mg/mL
20 mg/mL or 20mg/mL
10 mg per mL
Total content: 30 mg / 3 mL (which means 10 mg/mL)
Some labels list total content instead of concentration. If your vial says 60 mg in 3 mL, divide 60 by 3 to get 20 mg/mL. If it says 100 mg in 5 mL, that is also 20 mg/mL. If it says 50 mg in 5 mL, you have a 10 mg/mL solution.
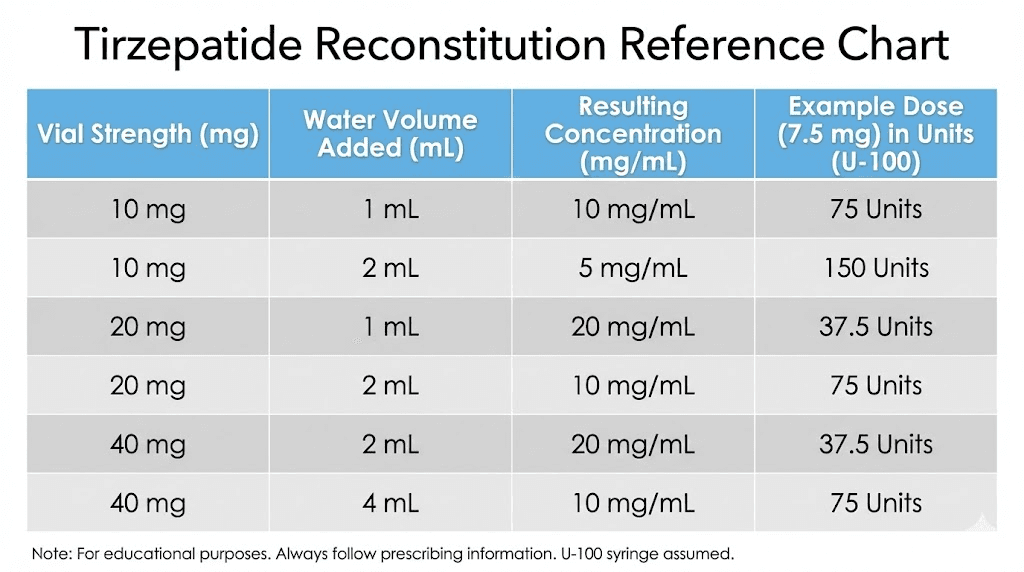
When in doubt, call your compounding pharmacy and ask them to confirm the concentration. They deal with this question constantly and will give you a clear answer. You can also cross-reference with the tirzepatide reconstitution chart for your specific product.
The 10 mg/mL conversion explained step by step
The 10 mg/mL concentration is the most widely used formulation for compounded tirzepatide. If your vial does not specify otherwise, there is a good chance it is 10 mg/mL. Here is the exact process for drawing your 7.5 mg dose from this concentration.
The math
7.5 mg divided by 10 mg/mL equals 0.75 mL. Then 0.75 mL times 100 equals 75 units.
You need to draw to the 75 unit line on a 100 unit insulin syringe. That is three-quarters of the syringe.
Practical drawing tips
The 75 unit mark sits right between the 70 and 80 unit lines on most standard insulin syringes. Each small line on a 100 unit syringe represents 2 units. So from the 70 line, count up 2.5 small lines to reach 75. This is one of the cleaner marks to hit because 75 falls on a visible graduation line on most quality syringes.
For accuracy at this volume, use a 1 mL (100 unit) insulin syringe rather than a 0.5 mL (50 unit) syringe. The 75 unit draw exceeds the capacity of a 50 unit syringe, so you need the larger size. The tirzepatide dosage chart in units provides additional visual reference for this concentration.
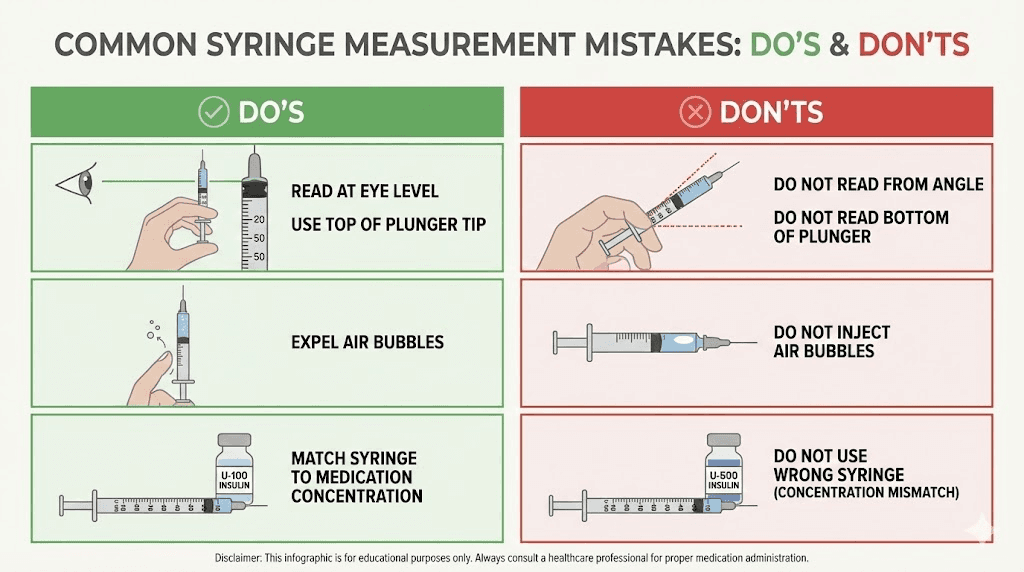
Draw slowly and deliberately. Hold the syringe at eye level when checking the volume. The bottom of the meniscus (the curved line at the top of the liquid) should sit exactly at the 75 unit mark. If you see any air bubbles in the syringe, tap them to the top and push them out before measuring. Air bubbles displace volume and will cause you to draw less medication than intended.
This volume produces a moderate injection, larger than the 50 units you drew at 5 mg but not uncomfortably so. Most researchers report no issues with the injection volume at this level when using a 29 or 31 gauge needle. The tirzepatide reconstitution guide covers proper preparation if you are working with lyophilized powder.
The 20 mg/mL conversion explained step by step
Many compounding pharmacies have shifted to 20 mg/mL formulations because the higher concentration means smaller injection volumes. This is especially convenient at higher doses, but it requires extra precision at the 7.5 mg level because of an unusual number.
The math
7.5 mg divided by 20 mg/mL equals 0.375 mL. Then 0.375 mL times 100 equals 37.5 units.
That is a tricky number. 37.5 units falls exactly between the 37 and 38 unit lines on a 50 unit syringe, or between the 36 and 38 lines on a 100 unit syringe where each graduation is 2 units. This is where careful measurement becomes critical.
Handling the half-unit challenge
Most standard insulin syringes do not have half-unit markings. This means drawing exactly 37.5 units requires you to estimate the midpoint between two lines. There are several strategies to handle this:
Option one: Use a half-unit insulin syringe. These syringes exist specifically for situations like this. They are typically 0.3 mL or 0.5 mL syringes with markings at every half unit, making it easy to draw to exactly 37.5. If you are using a 20 mg/mL concentration regularly, investing in half-unit syringes is worth the small additional cost.
Option two: Alternate between 37 and 38 units. Some researchers draw 37 units one week and 38 units the next. Over two weeks, this averages to 37.5 units per dose, which is effectively the same as hitting the mark perfectly each time. The difference between 37 and 38 units at 20 mg/mL is only 0.2 mg of tirzepatide, a negligible amount that will not affect results.
Option three: Round to 38 units. Drawing 38 units from a 20 mg/mL vial gives you 7.6 mg of tirzepatide. That is 0.1 mg over your target. In practical terms, this tiny overage is clinically insignificant and simplifies your measurement. Many protocols round to the nearest whole unit for this exact reason.
The tirzepatide 20mg/mL dosing chart provides a full breakdown of every dose at this concentration, including tips for handling half-unit measurements.
Syringe selection for 20 mg/mL
At 37.5 units, you have the option of using either a 50 unit syringe or a 100 unit syringe. The 50 unit syringe is the better choice because its graduations are spaced more widely apart, making it easier to see the 37.5 mark. Each small line on a 50 unit syringe represents 1 unit, compared to 2 units on a 100 unit syringe. That extra resolution makes half-unit accuracy much more achievable.
If you are moving up from the microdosing protocol at lower doses, you may already be comfortable with precise draws on smaller syringes. The same careful technique applies here.
When you reach the 7.5 mg dose in your protocol
The 7.5 mg dose is not a random number. It occupies a specific and important position in the standard tirzepatide dose escalation schedule. Understanding where it fits helps you prepare for the transition and know what to expect.
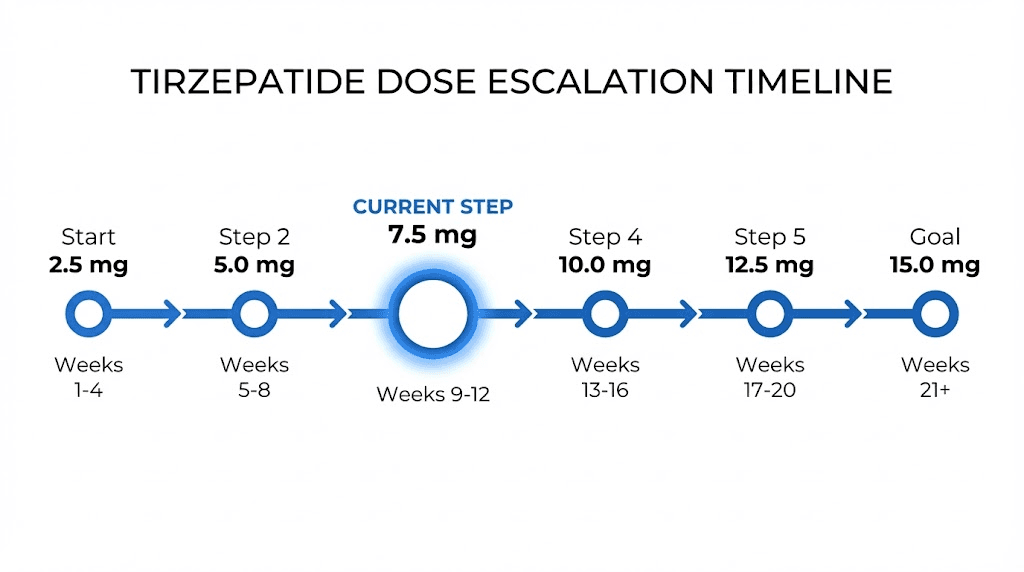
Standard dose escalation timeline
The FDA-approved tirzepatide dose schedule follows a structured escalation pattern:
Weeks 1 through 4: 2.5 mg once weekly (starting dose)
Weeks 5 through 8: 5 mg once weekly
Weeks 9 through 12: 7.5 mg once weekly
Weeks 13 through 16: 10 mg once weekly
Weeks 17 through 20: 12.5 mg once weekly (if needed)
Week 21 onward: 15 mg once weekly (maximum dose)
You reach 7.5 mg at approximately week 9. By this point, your body has already adapted to two months of tirzepatide exposure. The first month at 2.5 mg was primarily an acclimation phase, not expected to produce significant weight loss on its own. The second month at 5 mg is where most people begin seeing meaningful effects. The jump to 7.5 mg represents your third escalation step and the beginning of the mid-range therapeutic zone.
Some compounding pharmacies and clinics use slightly different escalation schedules. A few go directly from 5 mg to 10 mg, skipping 7.5 mg entirely. Others use 7.5 mg as a longer maintenance step, keeping patients at this dose for 6 to 8 weeks before deciding whether to increase further. The compound tirzepatide dosing chart shows several variations of this schedule.
Why 7.5 mg matters in the escalation
The 2.5 mg dose increments exist for a reason. Each step up gives the GLP-1 and GIP receptors time to adjust to increased stimulation. Jumping from 5 mg directly to 10 mg doubles the dose, which significantly increases the risk of gastrointestinal side effects. The 7.5 mg intermediary step represents only a 50% increase from 5 mg, which is much gentler on the system.
Clinical data from the SURMOUNT-1 trial showed that gastrointestinal adverse events were dose-dependent: 39% at 5 mg, 46% at 10 mg, and 49% at 15 mg. The 7.5 mg step helps smooth the transition between these ranges. Nausea, the most commonly reported side effect, typically peaks during dose escalation and then subsides within 1 to 2 weeks at the new dose level. Skipping the 7.5 mg step means hitting the 10 mg nausea window without the gradual adaptation.
Many researchers find that 7.5 mg is their sweet spot. Not everyone needs to reach 10 mg or higher. If appetite suppression is strong and weight loss is progressing steadily at 7.5 mg, there may be no need to increase further. Higher doses mean higher cost, more medication used per week, and potentially stronger side effects without proportionally better results.
Comparing 7.5 mg to other tirzepatide doses in units
Seeing how 7.5 mg relates to other common doses helps contextualize the conversion and makes it easier to verify you are drawing the right amount. Here is a comprehensive comparison at the two most common concentrations.
Dose (mg) | Units at 10 mg/mL | Units at 20 mg/mL | Dose escalation week |
|---|---|---|---|
2.5 mg | 25 units | 12.5 units | Weeks 1-4 |
5 mg | 50 units | 25 units | Weeks 5-8 |
7.5 mg | 75 units | 37.5 units | Weeks 9-12 |
10 mg | 100 units | 50 units | Weeks 13-16 |
12.5 mg | 125 units | 62.5 units | Weeks 17-20 |
15 mg | 150 units | 75 units | Week 21+ |
Notice the pattern. At 10 mg/mL, every 2.5 mg of tirzepatide adds 25 units to your draw. So going from 5 mg (50 units) to 7.5 mg (75 units) means drawing exactly 25 additional units. At 20 mg/mL, the same 2.5 mg increase adds 12.5 units.
This pattern is useful for sanity-checking your math. If you were drawing 50 units at 5 mg from a 10 mg/mL vial, your 7.5 mg dose should be 75 units, exactly 25 more. If your calculation gives you anything significantly different from this pattern, double-check the concentration on your vial.
You can use the peptide calculator on SeekPeptides to verify these numbers against your specific vial details. Entering the total vial content, the volume of liquid, and your target dose will give you the exact units to draw.
Common mistakes when drawing 7.5 mg
The 7.5 mg dose introduces specific measurement challenges that lower and higher doses do not share. Being aware of these common errors helps you avoid them.
Mistake 1: Using the wrong concentration assumption
The single most dangerous mistake is assuming your concentration without checking the label. If someone tells you that 7.5 mg equals 75 units, they are assuming a 10 mg/mL concentration. But if your vial is 20 mg/mL, drawing 75 units gives you 15 mg. That is double the intended dose.
This mistake happens most often when researchers switch pharmacies or when their pharmacy changes formulations. A new shipment might arrive at a different concentration than the previous one. The vials may look identical in size and color. The only difference is the number on the label.
Prevention: Read the concentration label on every new vial. Run the formula from scratch. Never assume a new vial matches the old one.
Mistake 2: Using a syringe that is too small
At 10 mg/mL, the 7.5 mg dose requires 75 units. A 50 unit (0.5 mL) insulin syringe cannot hold this volume. Some researchers try to do two draws, pulling 50 units and then 25 units in a second draw. This introduces air, wastes medication, and increases infection risk from repeated needle insertions into the vial.
Prevention: Use a 1 mL (100 unit) insulin syringe for concentrations of 10 mg/mL or lower at the 7.5 mg dose. Only use smaller syringes for concentrations of 15 mg/mL or higher.
Mistake 3: Ignoring air bubbles
Air bubbles displace liquid volume. If you draw to the 75 unit line but have a 5 unit air bubble trapped in the syringe, you actually have only 70 units of medication. That means you are getting approximately 7.0 mg instead of 7.5 mg. Over time, this systematic underdosing adds up.
Prevention: After drawing your dose, hold the syringe needle-up and tap firmly to float bubbles to the top. Push the plunger slightly to expel the air, then check your volume and adjust if needed. The tirzepatide preparation guide covers this technique in detail.
Mistake 4: Estimating the 37.5 unit mark poorly
On a 100 unit syringe, the 37.5 unit mark falls between the 36 and 38 unit graduation lines. Each line represents 2 units, so the half-unit point is not marked. Guessing where 37.5 falls leads to inconsistent doses.
Prevention: Switch to a 50 unit syringe where each line represents 1 unit, making the 37.5 mark easier to identify. Or use the alternating strategy described above (37 one week, 38 the next). Half-unit insulin syringes provide the most precise option.
Mistake 5: Not accounting for dead space
Every syringe has a small amount of dead space in the hub where the needle meets the barrel. This dead space holds liquid that never gets injected. On most insulin syringes, this is about 0.5 to 1 unit. Over an entire vial, this wasted medication adds up, potentially costing you a full dose by the time the vial is empty.
Prevention: Some researchers use low dead space syringes designed to minimize this waste. Others account for it by drawing slightly more than their target. The tirzepatide dosage chart in mL includes dead space considerations for precise measurement.
Syringe selection guide for 7.5 mg
The right syringe makes accurate measurement dramatically easier. The wrong one makes errors almost inevitable. Here is what you need for each concentration.
1 mL (100 unit) insulin syringe
Best for: 10 mg/mL concentration (75 units) and 5 mg/mL concentration (150 units, though a 3 mL syringe is better)
This is the standard workhorse syringe for the 7.5 mg dose at common concentrations. Each small graduation represents 2 units on most models. The 75 unit mark is clearly visible and falls directly on a graduation line, making it one of the easier draws. You can also see the syringe reading guide for tips on interpreting graduation lines.
Pros: Large enough for the full 75 unit draw. Widely available. Inexpensive.
Cons: 2 unit graduations make half-unit precision difficult. Not ideal for 20 mg/mL concentrations where you need 37.5 units.
0.5 mL (50 unit) insulin syringe
Best for: 20 mg/mL concentration (37.5 units) and 15 mg/mL concentration (50 units)
The smaller barrel means each graduation represents 1 unit instead of 2. This makes the 37.5 mark much easier to locate. The syringe also has a thinner barrel diameter, which magnifies small volume differences and improves measurement precision.
Pros: Better resolution for precise measurements. Easier to see half-unit marks. Less dead space waste.
Cons: Cannot hold the 75 units needed for 10 mg/mL formulations. More expensive than 100 unit syringes in some markets.
0.3 mL (30 unit) insulin syringe
Best for: 30 mg/mL concentration (25 units) and 40 mg/mL concentration (18.75 units)
The highest precision option, with 0.5 unit graduations on many models. This syringe is rarely needed for the 7.5 mg dose unless you are working with highly concentrated formulations.
Pros: Finest graduations available. Excellent for half-unit precision. Minimal dead space.
Cons: Very limited capacity. Not suitable for concentrations below 20 mg/mL at the 7.5 mg dose.
Half-unit insulin syringes
Best for: Any concentration where the unit calculation results in a half-unit number (like 37.5 or 12.5)
These specialty syringes have markings at every 0.5 units, eliminating the need to estimate between lines. They are available in both 0.3 mL and 0.5 mL sizes. If you are using a 20 mg/mL concentration and plan to stay at 7.5 mg for several weeks, a box of half-unit syringes is a worthwhile investment.
7.5 mg at less common concentrations
While 10 mg/mL and 20 mg/mL dominate the market, you might encounter other concentrations from specialty pharmacies. Here is how the 7.5 mg conversion works at each one.
5 mg/mL concentration
7.5 divided by 5 equals 1.5 mL, which equals 150 units. This exceeds the capacity of any standard insulin syringe. You will need a 3 mL syringe with a standard needle, not an insulin syringe. The markings on a 3 mL syringe show volume in mL directly, so draw to the 1.5 mL line.
This concentration is becoming less common because the large injection volume is uncomfortable. If your pharmacy offers it, ask whether they have a higher concentration option available. The reconstitution chart explains how different dilution volumes affect concentration.
15 mg/mL concentration
7.5 divided by 15 equals 0.5 mL, which equals 50 units. This is a clean, convenient number. You can use either a 50 unit or 100 unit insulin syringe. The 50 unit line is clearly marked on both sizes, making this one of the easiest draws for the 7.5 mg dose.
17 mg/mL concentration
Some compounding pharmacies use 17 mg/mL formulations. 7.5 divided by 17 equals approximately 0.441 mL, which equals about 44 units. This is a clean draw on both 50 unit and 100 unit syringes, falling between the 42 and 46 graduation lines on a 100 unit syringe or directly on the 44 line on a 50 unit syringe.
30 mg/mL concentration
7.5 divided by 30 equals 0.25 mL, which equals 25 units. Another clean number. Easy to draw on any insulin syringe. The 30 mg/mL concentration is relatively new to the compounded market and is primarily used for researchers on higher maintenance doses who want minimal injection volumes.
40 mg/mL concentration
7.5 divided by 40 equals 0.1875 mL, which equals 18.75 units. This is another half-unit situation requiring either a half-unit syringe or rounding. Most researchers round to 19 units (7.6 mg) for simplicity. The difference of 0.1 mg is clinically irrelevant.
If you are working with any of these less common concentrations and need help verifying your calculations, the peptide reconstitution calculator can confirm your math.
How to verify your conversion is correct
Running the formula is step one. Verifying the result is step two. Here are several cross-checks that catch errors before they become problems.
The proportion check
Your 7.5 mg dose should always be exactly 1.5 times your 5 mg dose in units. If you know your 5 mg draw was 50 units (at 10 mg/mL), then your 7.5 mg draw should be 75 units. Multiply any known dose-to-unit conversion by 1.5 and you should get your 7.5 mg unit value.
This works in reverse too. Your 7.5 mg draw should be exactly 75% of your 10 mg draw. If 10 mg at your concentration equals 100 units, then 7.5 mg equals 75 units. These quick ratio checks take seconds and catch calculation errors immediately.
The concentration check
Multiply your unit draw by your concentration and divide by 100. The result should equal your target dose. For example: 75 units times 10 mg/mL divided by 100 equals 7.5 mg. If the math checks out, your conversion is correct. If it does not, something went wrong.
The volume check
Your unit draw divided by 100 gives you the volume in mL. Multiply that volume by your concentration to confirm you are getting 7.5 mg. For 75 units: 75 divided by 100 equals 0.75 mL. Then 0.75 times 10 mg/mL equals 7.5 mg. Confirmed.
These verification steps take less than 30 seconds and could prevent a serious dosing error. The peptide dosage calculation guide walks through these verification methods in more detail for all peptide types.
What to expect at the 7.5 mg dose level
Moving from 5 mg to 7.5 mg represents a 50% dose increase. That is significant. Understanding what this change means for your body helps set realistic expectations and identify normal versus concerning responses.
Appetite suppression
The appetite suppression effect typically intensifies noticeably at 7.5 mg. Where 5 mg might reduce appetite moderately, 7.5 mg often produces more pronounced satiety. Meals feel complete sooner. Between-meal hunger decreases further. Some researchers report difficulty eating enough to meet basic nutritional needs during the first 1 to 2 weeks at this dose.
This heightened suppression usually moderates within 2 to 3 weeks as the body adapts. If it remains too intense after 3 weeks, discuss whether 7.5 mg is the right maintenance dose or if dropping back to 5 mg makes more sense. Not everyone needs to keep escalating.
Weight loss acceleration
Clinical trial data from SURMOUNT-1 showed dose-dependent weight loss with tirzepatide. While the trial tested maintenance doses of 5, 10, and 15 mg (not 7.5 mg specifically as a maintenance dose), the dose-response curve suggests that 7.5 mg produces weight loss results roughly between the 5 mg and 10 mg groups.
The 5 mg group achieved a mean weight loss of 15% at 72 weeks. The 10 mg group achieved 19.5%. Extrapolating, 7.5 mg likely produces results in the 16 to 18% range for most individuals who stay at this dose long-term. Individual results vary based on starting weight, diet, activity level, and metabolic factors.
Gastrointestinal effects
Nausea, the most common side effect, tends to reappear during dose escalation periods. If you experienced nausea when starting 5 mg, expect a milder version when moving to 7.5 mg. The body has already partially adapted to tirzepatide GLP-1 and GIP receptor activation at the lower dose, so the 7.5 mg transition is generally smoother than the initial start.
In clinical trials, gastrointestinal adverse events occurred in approximately 39% of patients at the 5 mg dose and 46% at 10 mg. The 7.5 mg dose falls between these rates, typically in the 40 to 44% range. Most events were mild to moderate in severity, transient, and peaked during the first 1 to 2 weeks after the dose increase.
Common GI effects at 7.5 mg include:
Mild nausea, especially in the first 48 hours after injection
Reduced bowel movement frequency
Occasional bloating after larger meals
Decreased tolerance for fatty or heavy foods
If you experienced significant anxiety or mood effects at lower doses, monitor these at 7.5 mg as well. Some researchers report temporary mood fluctuations during dose transitions that resolve as the body adapts.
Energy and fatigue patterns
Reduced caloric intake at 7.5 mg can sometimes cause temporary fatigue. This is not a direct pharmacological effect of tirzepatide but rather a consequence of eating significantly less than your body is accustomed to. Ensuring adequate protein intake (at least 0.7 grams per pound of body weight) and staying hydrated helps minimize this effect.
Managing the transition from 5 mg to 7.5 mg
The week you increase from 5 mg to 7.5 mg deserves some planning. A few practical strategies make the transition smoother and reduce the chance of uncomfortable side effects.
Timing your dose increase
If your 5 mg injections have been on a specific day of the week, keep the same day when you move to 7.5 mg. Consistency in injection timing helps maintain steady blood levels and reduces the intensity of any GI side effects that occur after each injection.
Some researchers prefer to increase on a day when they can rest the following day. If nausea tends to peak 12 to 24 hours after injection, scheduling your first 7.5 mg dose on a Friday allows Saturday for any initial adjustment effects. This is a personal preference, not a requirement, but it reduces stress about managing side effects during work or obligations.
Dietary adjustments
During the first week at 7.5 mg, eating smaller, more frequent meals is often more comfortable than three large meals. The enhanced gastric emptying delay from the higher dose means food sits in the stomach longer, and large meals can amplify nausea and bloating.
Focus on protein-rich foods, vegetables, and moderate portions of complex carbohydrates. Avoid high-fat meals in the first few days, as fat slows gastric emptying further and can compound the effect of tirzepatide on stomach motility. This is one of the key practical strategies that experienced researchers use during dose transitions.
Hydration protocol
Staying well-hydrated becomes more important at higher doses. The combination of reduced food intake (and therefore reduced water from food) and potential GI effects means dehydration can develop faster. Aim for at least 64 ounces of water daily, more if you are active or live in a warm climate. Electrolyte supplementation can help if you experience loose stools or reduced appetite to the point where food intake drops significantly.
When to hold at 7.5 mg versus continuing to escalate
Not everyone needs to reach 10 mg or higher. Consider staying at 7.5 mg if:
You are losing 1 to 2 pounds per week consistently
Appetite suppression is adequate to maintain a caloric deficit
Side effects are minimal and manageable
You are comfortable with the cost at this dose level
Consider continuing to 10 mg if:
Weight loss has plateaued for more than 3 weeks at 7.5 mg
Appetite suppression has diminished significantly
Your target weight is still far from current weight
Side effects at 7.5 mg are mild and tolerable
Many researchers use the troubleshooting guide to determine whether a dose increase is the right move or whether other factors like dietary compliance or sleep quality are affecting results.
The relationship between 7.5 mg units and vial management
Knowing how many units you draw per dose directly affects how many doses you can extract from each vial. This has significant cost implications, especially for researchers paying out of pocket for compounded tirzepatide.
Doses per vial at common vial sizes
Vial size | Concentration | Total units in vial | Units per 7.5 mg dose | Doses per vial |
|---|---|---|---|---|
2 mL | 10 mg/mL | 200 units | 75 units | 2.67 doses (2 full, partial third) |
3 mL | 10 mg/mL | 300 units | 75 units | 4 doses |
5 mL | 10 mg/mL | 500 units | 75 units | 6.67 doses (6 full, partial seventh) |
2 mL | 20 mg/mL | 200 units | 37.5 units | 5.33 doses (5 full, partial sixth) |
3 mL | 20 mg/mL | 300 units | 37.5 units | 8 doses |
The difference between concentrations is dramatic for vial management. A 2 mL vial at 10 mg/mL gives you fewer than 3 weekly doses at 7.5 mg. The same 2 mL vial at 20 mg/mL gives you more than 5 doses. That means fewer orders, less shipping cost, and less medication waste from expired partially-used vials.
Storage matters too. Once reconstituted, most compounded tirzepatide should be stored in the fridge and used within 28 to 56 days depending on the pharmacy. If your vial contains more doses than you can use before expiration, you are paying for wasted medication. Match your vial size to your dose schedule to minimize waste.
The peptide cost calculator can help you determine the most economical vial size for your specific dose and usage pattern.
Reconstituting tirzepatide for the 7.5 mg dose
If you are working with lyophilized (freeze-dried) tirzepatide powder rather than pre-mixed liquid, the amount of bacteriostatic water you add during reconstitution determines your concentration, which then determines how many units you draw for 7.5 mg.
How reconstitution volume affects your unit draw
A 30 mg vial of tirzepatide powder can be reconstituted to different concentrations depending on how much water you add:
Bac water added | Resulting concentration | Units for 7.5 mg |
|---|---|---|
1 mL | 30 mg/mL | 25 units |
1.5 mL | 20 mg/mL | 37.5 units |
2 mL | 15 mg/mL | 50 units |
3 mL | 10 mg/mL | 75 units |
6 mL | 5 mg/mL | 150 units |
The formula is straightforward: divide the total milligrams of powder by the milliliters of water added. A 30 mg vial reconstituted with 3 mL of bacteriostatic water produces a 10 mg/mL solution. The same vial reconstituted with 1.5 mL produces 20 mg/mL.
More water means lower concentration, which means more units per dose. Less water means higher concentration and fewer units per dose. The total amount of tirzepatide in the vial remains the same regardless of dilution.
The reconstituting tirzepatide chart provides complete dilution tables for every common vial size. You can also use the reconstitution calculator to determine exact volumes for your specific vial.
Choosing the right dilution for 7.5 mg
Most researchers reconstituting their own tirzepatide prefer concentrations between 10 and 20 mg/mL. Lower concentrations (like 5 mg/mL) require inconveniently large injection volumes. Higher concentrations (like 30 mg/mL) require very precise small-volume draws.
For the 7.5 mg dose specifically:
10 mg/mL is the easiest to measure accurately (75 units, clean mark on the syringe)
15 mg/mL gives the cleanest draw (50 units, dead center on a 100 unit syringe)
20 mg/mL offers the smallest injection volume but introduces the 37.5 unit half-unit challenge
If precision is your priority, reconstitute to 10 or 15 mg/mL. If minimizing injection volume matters more, go with 20 mg/mL and use a 50 unit syringe with half-unit markings.
Learn the full reconstitution process in the step-by-step tirzepatide reconstitution guide. Proper technique during reconstitution is just as important as accurate measurement during injection.
Comparing tirzepatide 7.5 mg to semaglutide equivalent doses
Researchers who have used semaglutide before switching to tirzepatide often want to know how the doses compare. While there is no exact one-to-one conversion because the medications work through different receptor pathways, approximate equivalencies exist based on clinical trial outcomes.
Approximate dose equivalency
Based on weight loss efficacy data from clinical trials:
Tirzepatide dose | Approximate semaglutide equivalent | Basis for comparison |
|---|---|---|
2.5 mg | 0.5 mg semaglutide | Starting dose comparison |
5 mg | 1.0 mg semaglutide | First therapeutic dose |
7.5 mg | 1.7 mg semaglutide | Mid-range therapeutic |
10 mg | 2.0 mg semaglutide | Standard maintenance |
15 mg | 2.4 mg semaglutide | Maximum dose |
The 7.5 mg tirzepatide dose roughly corresponds to 1.7 mg of semaglutide based on weight loss percentages observed in the SURMOUNT and STEP clinical trials. However, tirzepatide works on both GLP-1 and GIP receptors (it is a dual agonist), while semaglutide targets only GLP-1. This dual mechanism means the drugs are not truly interchangeable, and the dose comparison is approximate at best.
For researchers who are considering switching between the two, the conversion chart provides detailed guidance on transitioning safely.
Why the unit counts differ
Even at equivalent therapeutic doses, the unit draws for tirzepatide and semaglutide are completely different because the drugs have different concentrations, different molecular weights, and different formulation standards. Do not try to use semaglutide unit conversions for tirzepatide. They are separate calculations that happen to use the same type of syringe.
The SURMOUNT-5 trial directly compared tirzepatide against semaglutide for obesity treatment, with tirzepatide achieving 20.2% weight loss versus 13.7% for semaglutide at their respective maximum tolerated doses. This suggests tirzepatide has a meaningful efficacy advantage at equivalent escalation levels, making the 7.5 mg dose a particularly effective point in the titration schedule. The tirzepatide versus semaglutide dosage comparison explores this data in full detail.
Cost considerations at the 7.5 mg dose
Dose affects cost directly. Moving from 5 mg to 7.5 mg means using 50% more medication per week. Understanding the cost implications helps with planning and budgeting.
How dose increases affect monthly cost
At any given concentration, the cost per milligram of compounded tirzepatide stays roughly constant. So a 7.5 mg weekly dose costs approximately 50% more than a 5 mg weekly dose because you are using 50% more medication.
If your monthly cost at 5 mg was $100, expect approximately $150 at 7.5 mg. If it was $200, expect approximately $300. These are rough estimates since pricing varies widely between compounding pharmacies. The compounded tirzepatide cost guide compares pricing across popular providers.
Vial efficiency at 7.5 mg
Higher concentration formulations are generally more cost-effective because they pack more doses into each vial, reducing per-dose shipping costs and minimizing waste from partially used vials. A 20 mg/mL formulation at 7.5 mg per week allows 5+ doses from a 2 mL vial, compared to fewer than 3 doses from the same vial at 10 mg/mL.
Some pharmacies also offer larger vials at better per-milligram pricing. A 5 mL vial at 20 mg/mL contains 100 mg total, enough for 13+ weekly doses at 7.5 mg. That is over three months of supply in a single vial, which often comes at a significant per-dose discount.
Deciding whether the dose increase is worth the cost
If you are seeing strong results at 5 mg and the additional cost of 7.5 mg strains your budget, it is worth discussing with your provider whether staying at 5 mg longer is a viable option. Weight loss may be slower at the lower dose, but consistent results at a sustainable cost often beat faster results that you cannot afford to maintain. The cost analysis calculator can help you compare long-term costs at different dose levels.
Injection technique tips specific to the 7.5 mg volume
The volume you inject affects the injection experience. At 10 mg/mL, the 7.5 mg dose requires 0.75 mL, which is a moderately large subcutaneous injection. At 20 mg/mL, it requires only 0.375 mL, a much smaller and more comfortable volume. Here are technique tips for each scenario.
Injecting 75 units (0.75 mL)
A 0.75 mL injection is larger than what most people are accustomed to from the 5 mg dose (0.5 mL at 10 mg/mL). The extra volume may cause a slightly larger subcutaneous depot at the injection site, which can feel like a small, firm lump under the skin for a few hours. This is normal and resolves on its own.
To minimize discomfort at this volume:
Inject slowly over 10 to 15 seconds rather than pushing the plunger quickly
Use a 29 gauge or 31 gauge needle for less tissue disruption
Rotate injection sites between the abdomen, thigh, and upper arm to prevent tissue irritation at any single location
Allow the medication to reach room temperature before injecting (cold injections at this volume can sting)
The peptide injection guide covers proper subcutaneous injection technique in comprehensive detail, including needle angle, pinch technique, and site rotation patterns.
Injecting 37.5 units (0.375 mL)
This smaller volume is much more comfortable. There is less subcutaneous depot formation, less post-injection tenderness, and less visible injection site reaction. Most researchers report that injections at this volume are nearly painless with a fine-gauge needle.
The primary challenge with smaller volumes is ensuring you inject the full amount. Push the plunger all the way down and hold for 5 to 10 seconds before withdrawing the needle. This ensures all the medication leaves the syringe and enters the subcutaneous tissue rather than being pulled back into the needle track.
Injection site rotation
Regardless of volume, rotating injection sites prevents lipodystrophy (changes in subcutaneous fat tissue) that can occur with repeated injections in the same area. Use a rotation pattern such as:
Week 1: Left abdomen
Week 2: Right abdomen
Week 3: Left thigh
Week 4: Right thigh
Keep each injection at least 2 inches from the previous site in the same region. Avoid injecting within 2 inches of the navel or into areas with visible veins, scars, or skin abnormalities. The injection guide has visual diagrams of recommended rotation sites.
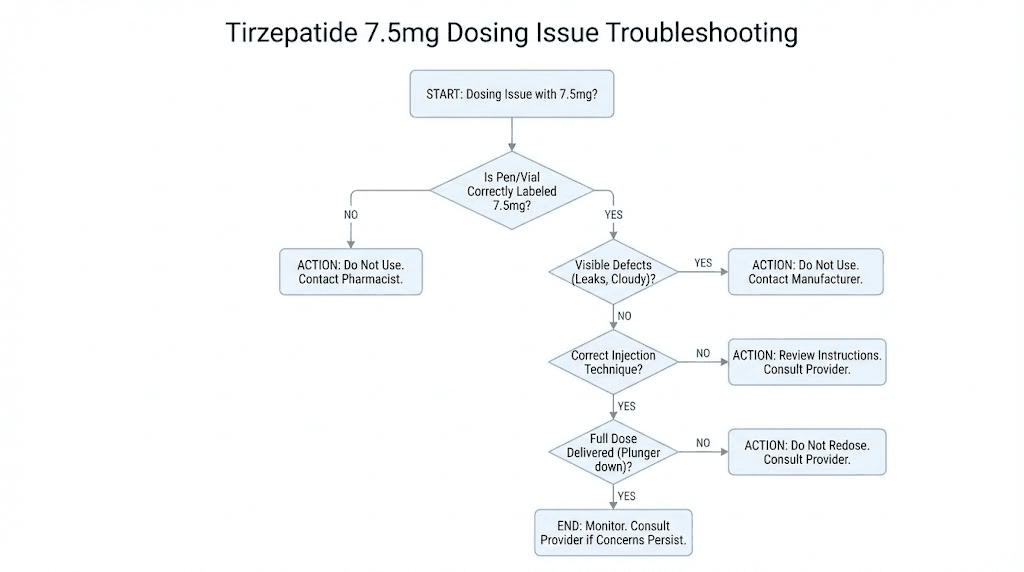
Troubleshooting common 7.5 mg dosing issues
Even with careful measurement, issues arise. Here are the most common problems researchers encounter at the 7.5 mg dose and how to address them.
Problem: Cannot draw to the exact unit mark
Air bubbles, vial pressure, and plunger friction can make it difficult to draw precisely to 75 or 37.5 units. If you consistently end up a unit or two off, the variance is clinically insignificant. The difference between 73 and 77 units at 10 mg/mL is only 0.4 mg of tirzepatide. That small variation will not affect outcomes.
If you are consistently off by more than 3 to 5 units, the issue is likely technique-related. Practice drawing with bacteriostatic water before using your actual medication. The bacteriostatic water guide explains proper handling techniques that translate directly to accurate drawing.
Problem: Side effects worse than expected at 7.5 mg
If nausea, fatigue, or GI effects are significantly worse than at 5 mg, consider whether you might have drawn more than intended. Verify your vial concentration and recalculate. If the dose is correct and side effects are genuinely more intense, they should diminish within 1 to 2 weeks as your body adapts.
If effects persist beyond 2 weeks or are severe enough to affect daily function, consider stepping back to 5 mg for an additional 2 to 4 weeks before attempting 7.5 mg again. Some protocols use an intermediate step of 6.25 mg (which is 62.5 units at 10 mg/mL) for a gentler transition. The comprehensive dosing guide discusses intermediate dose strategies.
Problem: Weight loss stalled after moving to 7.5 mg
A temporary stall when increasing doses is surprisingly common. The body sometimes holds water during metabolic adjustments, masking fat loss on the scale. Give the new dose at least 3 to 4 weeks before concluding it is not working.
If the stall continues beyond 4 weeks at 7.5 mg, evaluate whether dietary compliance has shifted. Enhanced appetite suppression sometimes causes researchers to eat too little protein, which can slow metabolism and reduce the thermic effect of food. Ensure you are meeting minimum protein targets even when appetite is low.
The detailed troubleshooting guide covers 15+ reasons for weight loss stalls and specific solutions for each.
Problem: Vial running out faster than expected
If your vial seems to contain fewer doses than you calculated, dead space and overfill variations are the likely culprits. Each draw wastes approximately 0.5 to 1 unit in the syringe hub. Over 4 doses at 75 units each, that adds up to 2 to 4 units of lost medication. Some vials also contain slightly less than the labeled volume due to manufacturing tolerances.
Budget for approximately 5% medication loss from these factors. If your vial should theoretically contain 4 doses at 75 units, plan for 3.8 effective doses instead. The proper storage guide also helps minimize potency loss that could reduce effective doses.
Working with your provider on the 7.5 mg dose
Even if you are managing your own compounded tirzepatide protocol, involving a healthcare provider adds a layer of safety. The 7.5 mg dose step is a good checkpoint to review progress, discuss side effects, and confirm that continued escalation is appropriate.
Questions to ask your provider
Is 7.5 mg the right next step based on my response to 5 mg?
Should I plan to hold at 7.5 mg or continue escalating to 10 mg?
Are there any blood markers I should check at this dose level?
How should I adjust if GI side effects are problematic?
What is the plan if weight loss stalls at 7.5 mg?
Monitoring recommendations
Many providers recommend baseline and periodic lab work during tirzepatide protocols. Key markers to track include:
Blood glucose and HbA1c (tirzepatide significantly affects glucose metabolism)
Lipid panel (cholesterol and triglycerides often improve with weight loss)
Thyroid function (GLP-1 receptor agonists carry warnings about thyroid C-cell tumors)
Kidney and liver function (routine monitoring)
Nutritional markers (B12, iron, vitamin D, especially with reduced food intake)
The 7.5 mg dose level is often where providers schedule the first follow-up labs, typically 8 to 12 weeks after starting tirzepatide. Results inform whether to continue escalation or optimize the current dose. The connection between tirzepatide and B12 supplementation is worth discussing with your provider, as reduced food intake can affect B12 absorption over time.
Advanced conversion scenarios
Some situations require more complex calculations than the standard formula. Here are the most common advanced scenarios researchers encounter at the 7.5 mg dose.
Splitting the dose into two injections
A small number of researchers split their weekly dose into two half-doses administered 3 to 4 days apart. For 7.5 mg, this means two injections of 3.75 mg each. The unit conversion for each half-dose:
At 10 mg/mL: 3.75 divided by 10 equals 0.375 mL, or 37.5 units per injection
At 20 mg/mL: 3.75 divided by 20 equals 0.1875 mL, or 18.75 units per injection
Split dosing may reduce GI side effects by spreading the medication absorption over two peaks instead of one. However, this protocol is off-label and should only be done with provider guidance. The complete dosage chart includes split-dose calculations for all common concentrations.
Stacking tirzepatide with other peptides
Researchers using tirzepatide alongside other peptides like BPC-157, TB-500, or cagrilintide need to track separate unit conversions for each compound. The same insulin syringe type can be used for different peptides, but never mix compounds in the same syringe unless specifically instructed by your provider.
The peptide stacking calculator helps coordinate multiple peptide protocols, and the stacking guide covers compatibility and timing considerations.
Converting between syringe types
If you need to switch from a 100 unit syringe to a 50 unit syringe (or vice versa), the unit number stays the same. 75 units is 75 units regardless of syringe size. The only difference is the physical spacing of the graduation marks. A 50 unit syringe cannot hold 75 units, so it is only usable for concentrations where the 7.5 mg dose calculates to 50 units or fewer.
If you are using a 3 mL syringe (which reads in mL rather than units), draw to the volume you calculated in step one of the formula. For 7.5 mg at 10 mg/mL, draw to 0.75 mL. For 7.5 mg at 20 mg/mL, draw to 0.375 mL. The mL markings on a 3 mL syringe are less precise than insulin syringe unit markings, so insulin syringes are preferred whenever the volume fits.
Quick reference card for 7.5 mg tirzepatide
Save this summary for easy reference before each injection:
Your vial says | Draw this many units | Use this syringe |
|---|---|---|
5 mg/mL | 150 units (use 3 mL syringe at 1.5 mL) | 3 mL standard syringe |
10 mg/mL | 75 units | 1 mL (100 unit) insulin syringe |
15 mg/mL | 50 units | 0.5 mL (50 unit) insulin syringe |
20 mg/mL | 37.5 units | 0.5 mL (50 unit) or half-unit syringe |
30 mg/mL | 25 units | 0.3 mL (30 unit) insulin syringe |
40 mg/mL | 18.75 units (round to 19) | 0.3 mL (30 unit) insulin syringe |
The formula: Units = (dose in mg / concentration in mg per mL) x 100
Always verify: Check your vial label. Run the formula. Cross-check with the ratio method. Then draw.
For automated calculations, the SeekPeptides peptide calculator handles all the math instantly. Enter your vial details and dose, and it returns the exact units to draw.
Frequently asked questions
Is 7.5 mg of tirzepatide 75 units on an insulin syringe?
Only if your vial concentration is 10 mg/mL. At that concentration, yes, 7.5 mg equals exactly 75 units. But at 20 mg/mL, the same dose is only 37.5 units. Always check your vial label before drawing. The number of units depends entirely on the concentration of your specific vial.
Can I use a 50 unit syringe for 7.5 mg of tirzepatide?
That depends on your concentration. If you have a 20 mg/mL vial (37.5 units needed), yes, a 50 unit syringe works perfectly and is actually the better choice for precision. If you have a 10 mg/mL vial (75 units needed), no, it will not fit. You need a 100 unit syringe for concentrations of 10 mg/mL or lower.
What if my syringe does not have a 37.5 unit marking?
Most standard insulin syringes do not have half-unit markings. You have three options: use a specialty half-unit insulin syringe that marks every 0.5 units, alternate between 37 and 38 units each week, or round to 38 units consistently. The difference is less than 0.2 mg, which is clinically insignificant. Learn more about syringe types in the injection equipment guide.
How do I know what concentration my tirzepatide is?
Check the label on your vial. It will show the concentration as a number followed by mg/mL (such as 10 mg/mL or 20 mg/mL). If the label shows total content instead (like 60 mg in 3 mL), divide the total mg by the total mL to get the concentration. If you are unsure, call your compounding pharmacy and ask them to confirm.
Is 7.5 mg a standard tirzepatide dose?
Yes. It is part of the standard dose escalation schedule, typically reached at weeks 9 through 12. The FDA-approved doses for Mounjaro and Zepbound escalate in 2.5 mg steps: 2.5, 5, 7.5, 10, 12.5, and 15 mg. Some people stay at 7.5 mg as their maintenance dose if they are seeing good results without needing to increase further. The complete dosing guide covers all standard dose levels.
What happens if I accidentally draw too many units?
If you draw too many units and inject the full amount, you will receive a larger dose than intended. At 10 mg/mL, every extra 10 units equals 1 mg of additional tirzepatide. This may increase side effects, particularly nausea and reduced appetite. Monitor your symptoms and contact your healthcare provider if you experience unusual effects. Do not try to compensate by reducing your next dose without medical guidance.
Can I draw from the same vial for multiple weeks at 7.5 mg?
Yes, most compounded tirzepatide vials are designed for multiple draws. A 3 mL vial at 10 mg/mL contains 30 mg total, which provides exactly 4 doses at 7.5 mg per dose. Ensure you store the vial properly between uses and use it within the expiration window specified by your pharmacy (typically 28 to 56 days after first puncture).
Should I take 7.5 mg all at once or split it into two injections?
The standard protocol is a single weekly injection of the full 7.5 mg dose. Some researchers experiment with splitting the dose into two half-doses (3.75 mg each) administered 3 to 4 days apart to reduce GI side effects. This is off-label and should only be done with provider guidance. The single weekly injection is effective for the vast majority of users.
External resources
For researchers serious about getting every dose exactly right, SeekPeptides provides the most comprehensive dosing resources available, with calculators, conversion charts, protocol guides, and a community of experienced researchers who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your syringes stay precise, and your protocols stay consistent.