Feb 23, 2026

Two people draw 50 units of semaglutide into an insulin syringe. Same marking on the barrel. Same volume of liquid. But one is injecting 2.5 mg of the active compound, while the other is injecting just 1.0 mg. One person is at the near-maximum approved dose for weight loss. The other is sitting comfortably in the middle of the escalation schedule. Same number on the syringe, completely different clinical realities.
This is the problem with asking whether 50 units is "a lot."
The answer depends entirely on a detail most people overlook: the concentration of semaglutide in their vial. Without that number, 50 units tells you almost nothing about your actual dose. It is like asking whether 50 miles is a long drive without knowing if you are on a highway or a dirt road. The distance is the same. The experience is not.
And this confusion is everywhere. Forums are filled with people comparing doses in units, not realizing they are using different concentrations. One person reports terrible nausea at 50 units while another feels nothing. Both think the other person is exaggerating. Neither realizes they are on completely different milligram doses. The semaglutide dosage in units system creates confusion precisely because units measure volume, not drug amount. This guide breaks down exactly what 50 units means at every common concentration, where it falls on the standard dosing schedule, whether it counts as high or moderate, and what signs suggest your dose needs adjusting. By the end, you will know exactly where you stand.
What does 50 units of semaglutide actually mean
Before answering whether 50 units is a lot, you need to understand what units actually measure. This is where most of the confusion starts, and it is worth getting right.
Units on an insulin syringe measure volume. Not milligrams. Not potency. Volume.
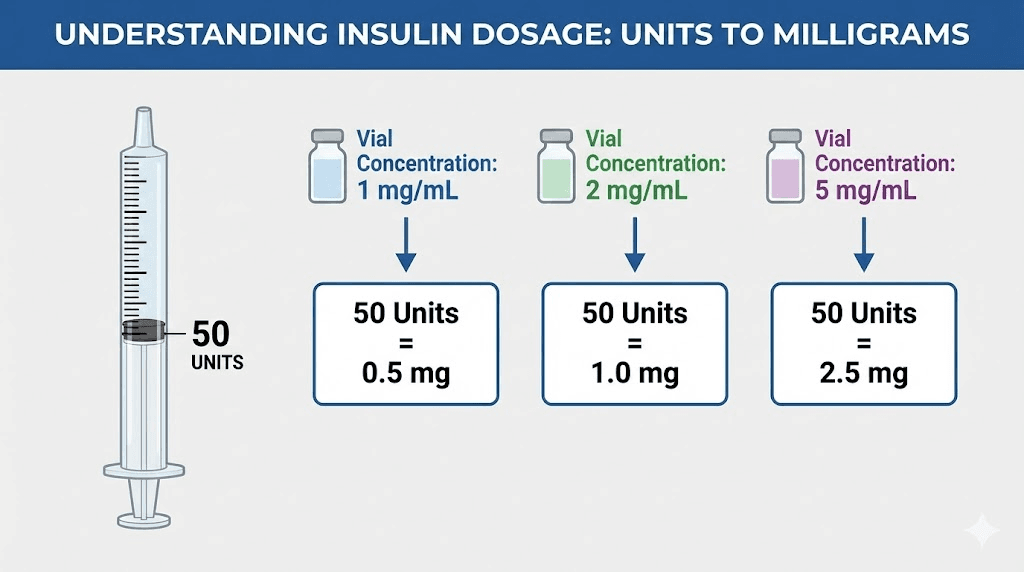
A standard insulin syringe holds 100 units, which equals exactly 1 mL of liquid. So 50 units equals 0.5 mL. That is half a milliliter of whatever liquid is in your vial. Whether that half milliliter contains a large or small amount of semaglutide depends on how concentrated the solution is. The semaglutide units to mg conversion changes based on this concentration, and ignoring it leads to dosing errors that can produce either underwhelming results or overwhelming side effects.
Think of it this way. A cup of espresso and a cup of decaf are both the same volume. But the caffeine content is drastically different. Semaglutide works the same way. Two syringes filled to the 50-unit line can deliver vastly different amounts of the actual drug, depending on how much semaglutide was dissolved into each milliliter of solution.
This is why questions like how many mg is 50 units of semaglutide do not have a single answer. The answer is always "it depends on your concentration." And that concentration is printed on your vial label, usually expressed as milligrams per milliliter (mg/mL).
Why concentration changes everything about 50 units
Semaglutide comes in multiple concentrations. Brand-name products like Ozempic use pre-filled pens with fixed doses, so the unit question rarely comes up. But compounded semaglutide ships in multi-dose vials that you draw from using an insulin syringe. This is where concentration becomes critical.
The most common compounded semaglutide concentrations are:
2 mg/mL
2.5 mg/mL
3 mg/mL
5 mg/mL
At each of these concentrations, 50 units delivers a different milligram dose. The math is straightforward, but missing it can mean the difference between a gentle starting dose and an aggressive maintenance dose. This is why checking your vial label is not optional. It is the single most important step in semaglutide dosing, and the semaglutide dosage calculator can help you verify exactly what you are injecting.
Some pharmacies also compound at less common concentrations like 1.25 mg/mL or 10 mg/mL. If your concentration is not listed among the common options above, the calculation method in a later section will show you how to figure out your specific dose. But for now, understand this: the concentration on your vial changes everything. Two people both injecting 50 units might be on completely different treatment protocols, experiencing completely different side effect profiles, and getting completely different results.
How 50 units translates at each semaglutide concentration
Here is the breakdown for every major concentration. This is the section to bookmark.
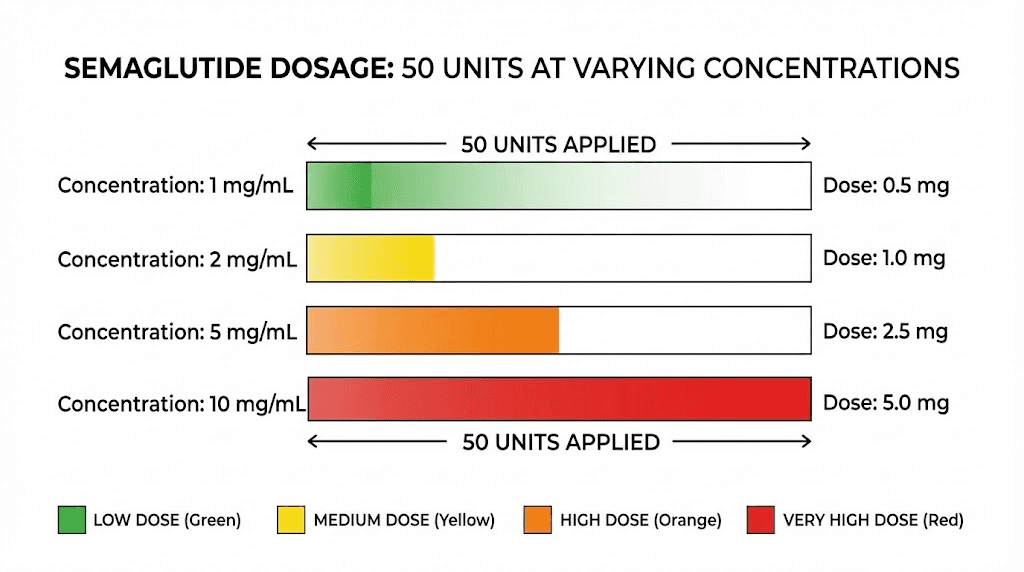
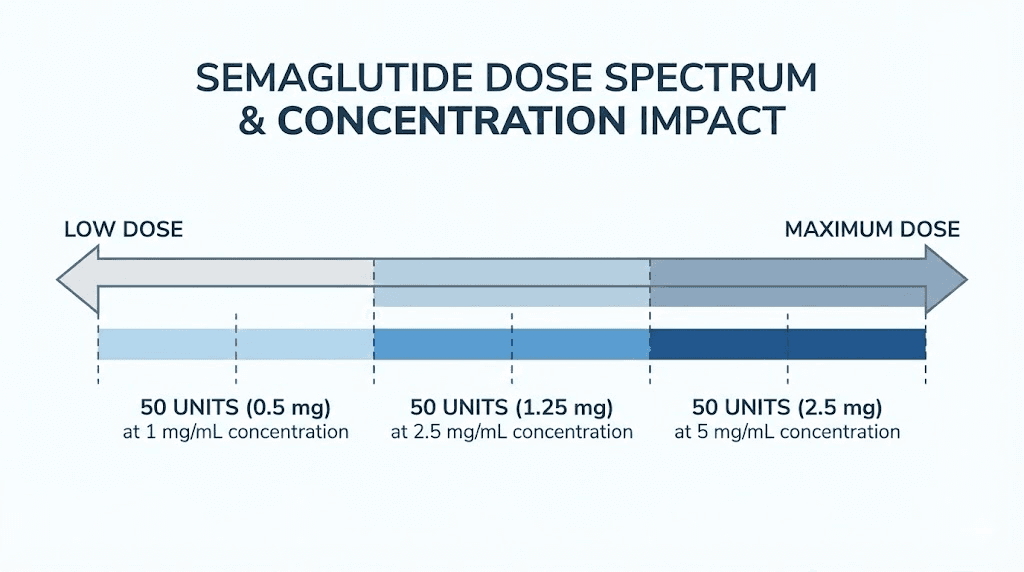
50 units at 5 mg/mL equals 2.5 mg
At the highest common compounded concentration, 50 units delivers 2.5 mg of semaglutide per injection. This is a significant dose. For context, the FDA-approved maximum weekly dose of semaglutide for weight loss (Wegovy) is 2.4 mg. So at this concentration, 50 units actually exceeds the standard maximum by 0.1 mg.
This means 50 units at 5 mg/mL is a lot. It is the highest standard maintenance dose range. Most people do not start anywhere near this amount. The semaglutide 5mg/mL dosage chart shows that typical starting doses at this concentration are just 5 units (0.25 mg), which means 50 units represents a tenfold increase from the beginning of the escalation schedule.
If you are taking 50 units from a 5 mg/mL vial and tolerating it well, you are on a full maintenance dose. If you are experiencing significant semaglutide fatigue, persistent nausea, or other concerning symptoms, this high concentration is likely the reason. And it is worth discussing with your prescriber whether a dose reduction makes sense.
50 units at 3 mg/mL equals 1.5 mg
At 3 mg/mL, drawing 50 units gives you 1.5 mg of semaglutide. This is a solid mid-range dose. It sits between the 1.0 mg step and the 1.7 mg step on the standard Wegovy escalation schedule, which makes it a moderate dose that many people use during the titration phase.
At this concentration, 50 units is not extreme. It is not conservative either. You are past the initial loading phases and into the territory where meaningful appetite suppression should be occurring. Most people at 1.5 mg weekly are seeing noticeable changes in hunger patterns and early weight loss results. If you have been on this dose for several weeks and are not losing weight on semaglutide, the dose may need to increase rather than decrease.
50 units at 2.5 mg/mL equals 1.25 mg
Drawing 50 units from a 2.5 mg/mL vial gives you 1.25 mg. This falls squarely in the mid-range of the dose escalation schedule, between the 1.0 mg and 1.7 mg steps. It is a reasonable dose for someone who has been escalating for 8 to 12 weeks and is building tolerance steadily.
At 1.25 mg, 50 units is a moderate amount. Not high. Not low. Right in the middle. This is the dose range where semaglutide starts working more noticeably for most people, with appetite reduction becoming more consistent and the medication reaching therapeutic levels in the bloodstream.
50 units at 2 mg/mL equals 1.0 mg
At the lowest common concentration, 50 units delivers just 1.0 mg of semaglutide. This is a moderate early-to-mid dose on the standard escalation schedule. For Wegovy, 1.0 mg is the third step (weeks 9 through 12) out of five escalation phases. For Ozempic (used off-label for weight loss), 1.0 mg is the standard maintenance dose.
So at 2 mg/mL, 50 units is not a lot. It is a standard therapeutic dose that most people tolerate well after the initial adjustment period. If you are experiencing minimal side effects at this level and not seeing the results you want, you likely have room to escalate. Your provider may suggest moving toward 2.4 mg, the full maintenance dose, over the coming weeks.
The table below summarizes all four concentrations at 50 units:
Vial concentration | 50 units equals | Dose category | Where it falls on Wegovy scale |
|---|---|---|---|
5 mg/mL | 2.5 mg | High (near maximum) | Exceeds standard max of 2.4 mg |
3 mg/mL | 1.5 mg | Moderate-high | Between step 3 and step 4 |
2.5 mg/mL | 1.25 mg | Moderate | Between step 3 and step 4 |
2 mg/mL | 1.0 mg | Moderate-low | Step 3 of 5 |
This is why the question "is 50 units a lot" has no universal answer. It ranges from conservative to near-maximum depending on a single variable printed on your vial. For a more detailed look at other unit conversions, see our guides on how many mg is 40 units of semaglutide and 20 units of semaglutide in mg.
Where 50 units falls on the standard dose escalation schedule
Every semaglutide protocol follows a gradual escalation. You do not start at the full dose. You build up to it over weeks, allowing your body to adapt to the medication and minimizing gastrointestinal side effects. Understanding where 50 units falls on this schedule helps you gauge whether your dose is early-stage, mid-stage, or late-stage.
The standard Wegovy escalation
The FDA-approved schedule for semaglutide (Wegovy) for chronic weight management follows five steps:
Weeks 1 to 4: 0.25 mg once weekly
Weeks 5 to 8: 0.5 mg once weekly
Weeks 9 to 12: 1.0 mg once weekly
Weeks 13 to 16: 1.7 mg once weekly
Week 17 onward: 2.4 mg once weekly (maintenance)
Each step lasts a minimum of four weeks. Some providers extend individual steps to six or eight weeks if a patient needs more time to adjust. The timeline for semaglutide to work depends partly on how quickly someone moves through these escalation phases, with most people reaching maintenance by week 17 at the earliest.
Now map 50 units onto this schedule by concentration:
5 mg/mL: 50 units = 2.5 mg, which places you at or slightly beyond the final maintenance step
3 mg/mL: 50 units = 1.5 mg, which places you between steps 3 and 4
2.5 mg/mL: 50 units = 1.25 mg, which places you between steps 3 and 4
2 mg/mL: 50 units = 1.0 mg, which places you at step 3
Compounded semaglutide escalation patterns
Compounded semaglutide follows similar escalation principles, though protocols can vary by pharmacy and prescriber. The most common approach mirrors the Wegovy schedule: start at 0.25 mg and increase by 0.25 to 0.5 mg increments every four weeks until reaching the target dose.
Some providers use more conservative escalation with compounded versions, increasing more slowly to reduce the risk of nausea and vomiting. Others use slightly faster timelines for patients who have previously been on GLP-1 medications. If you are wondering about how many units equal the starting 0.25 mg dose at your specific concentration, that calculation is essential before your first injection.
The key takeaway: at most concentrations, 50 units represents a dose that is well past the starting phase. You should have been on semaglutide for at least 8 to 12 weeks before reaching a dose that requires drawing 50 units, unless your vial concentration is very low. If someone prescribed 50 units as a starting dose from a 5 mg/mL vial, that would be 2.5 mg, which is dangerously high for a first injection. Always verify concentration against your prescribed milligram dose.
Is 50 units considered a high dose of semaglutide
The honest answer: it depends, but for most common concentrations, 50 units represents a moderate to high dose.
Here is a practical framework for thinking about it.
If you are using a 5 mg/mL vial and drawing 50 units, you are on a high dose. Full stop. At 2.5 mg, you are at the ceiling of standard treatment. Some providers will prescribe slightly above this for patients who are not responding adequately, but research on higher doses (up to 7.2 mg in clinical trials) is still emerging. For now, 2.5 mg puts you at the top of the established range. This is as high as most people will ever go on standard protocols.
If you are using a 3 mg/mL vial, 50 units is a moderate-high dose at 1.5 mg. You are past the initial loading phases and approaching the upper end of escalation. Most people at this dose are seeing significant appetite suppression and steady weight loss. It is not the maximum, but it is not gentle either.
If you are using a 2.5 mg/mL or 2 mg/mL vial, 50 units is moderate. At 1.0 to 1.25 mg, you are in the middle of the standard escalation. There is plenty of room to go higher if needed. This is a therapeutic dose, but not an aggressive one.
A useful comparison: the article on whether 20 units of semaglutide is too much walks through similar concentration-dependent analysis. At 5 mg/mL, 20 units equals 1.0 mg (moderate). At 2 mg/mL, 20 units equals just 0.4 mg (low). The principle is the same for 50 units, just further along the scale. And for those working with even larger volumes, understanding what 100 units equals in mg provides the upper boundary context.
Comparing to what clinical trials used
In the landmark STEP trials that led to Wegovy approval, participants escalated to 2.4 mg weekly. At that dose, average weight loss was approximately 15% of body weight over 68 weeks. More recent research has tested doses up to 7.2 mg and even 16 mg weekly, with greater weight loss but also increased gastrointestinal side effects.
So by current clinical standards, the maximum of what 50 units can deliver (2.5 mg at 5 mg/mL) is right at the established therapeutic ceiling. It is a lot in absolute terms, but it is not experimental or dangerous. It is the dose that was specifically tested and approved for chronic weight management.
Signs your semaglutide dose might be too high
Whether you are on 50 units or any other amount, recognizing when a dose is too aggressive matters. Semaglutide side effects are dose-dependent. The higher the milligram dose, the more likely you are to experience them, and the more intense they tend to be.
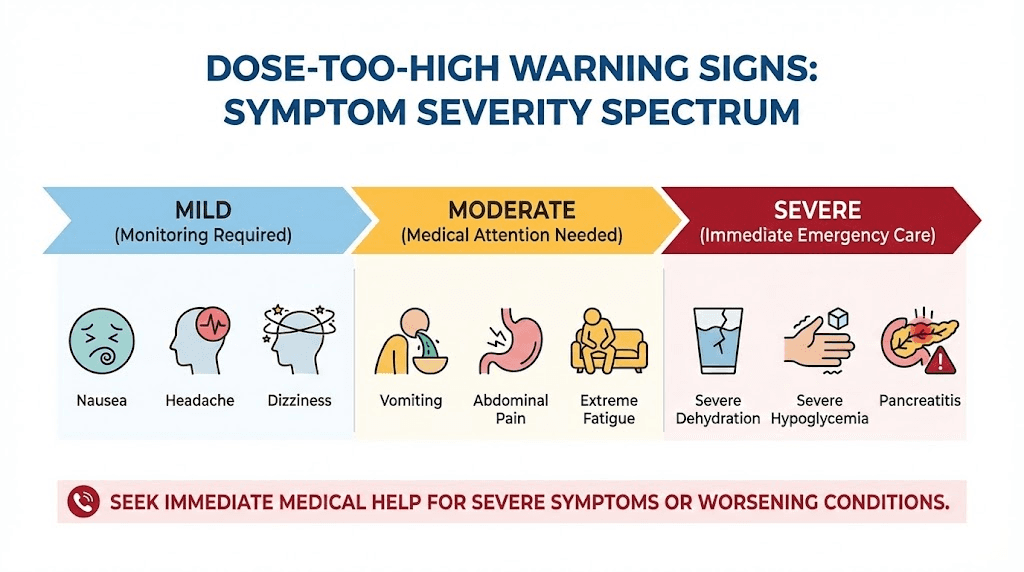
Gastrointestinal symptoms that signal trouble
The most common signs of an excessive dose involve your gut. Nausea is the hallmark side effect. At the 2.4 mg maintenance dose in clinical trials, approximately 44% of participants experienced nausea. About 25% experienced vomiting. These numbers are important because they represent the maximum approved dose, which is what 50 units approximates at 5 mg/mL concentration.
Normal, tolerable nausea looks like mild queasiness that comes and goes, usually in the first 24 to 48 hours after injection. It does not prevent eating. It does not cause dehydration. And it generally improves within a few weeks at each dose level. The semaglutide constipation treatment guide covers another common GI issue that tends to worsen with dose escalation.
Concerning nausea looks different. It lasts for days. It prevents you from keeping fluids down. It comes with persistent vomiting, severe abdominal pain, or complete loss of appetite to the point where you cannot eat anything at all. If this describes your experience, your dose may be too high.
Fatigue that does not improve
Some degree of fatigue with semaglutide is common, especially during dose escalation. Your body is adjusting to reduced caloric intake and metabolic changes. But fatigue that becomes debilitating, that prevents you from working or exercising, that does not improve after two to three weeks at a given dose, suggests the dose may be too aggressive for your current tolerance level. The broader category of GLP-1 fatigue affects a significant percentage of users and is worth understanding in detail.
Dizziness and lightheadedness
Semaglutide-related dizziness often indicates dehydration from insufficient fluid intake combined with reduced eating. At higher doses, the appetite suppression effect is stronger, which can lead people to eat and drink far less than their body needs. If you are experiencing regular dizziness, especially upon standing, your dose may be producing too dramatic a reduction in food and fluid intake.
Excessive burping and GI distress
Semaglutide slows gastric emptying, which is part of how it reduces appetite. But at higher doses, this slowing can become excessive, leading to persistent burping, bloating, acid reflux, and a feeling of fullness that never resolves. These symptoms suggest the dose is pushing gastric motility slower than your body can comfortably handle.
Sleep disturbances
Some people report insomnia on semaglutide, particularly at higher doses. This may be related to nausea disrupting sleep, hunger signals being suppressed in ways that interfere with circadian rhythm, or direct GLP-1 receptor effects in the brain. If sleep problems emerge after a dose increase, the new dose may be the culprit.
The key principle
Side effects should be manageable and temporary. Mild nausea for a few days after each injection is normal. Persistent, severe symptoms that interfere with daily life are not. The dose that works best is the lowest effective dose, meaning the smallest amount that produces the desired appetite suppression and weight loss without intolerable side effects. More is not always better.
When 50 units is exactly the right amount
Not everyone at 50 units is overdosing. For many people, this is the correct therapeutic dose that produces optimal results with manageable side effects. Here are the scenarios where 50 units is exactly where you should be.
You have been escalating gradually and tolerating well
If you started at a low dose, followed the standard semaglutide treatment timeline, increased by appropriate increments every four weeks, and your body has adapted at each step, then 50 units represents a natural progression. The escalation schedule exists precisely so that your GLP-1 receptors can upregulate gradually, your gastrointestinal system can adapt to delayed gastric emptying, and your brain can adjust to new hunger signals.
Your weight loss has plateaued at lower doses
Hitting a semaglutide plateau is common, especially at lower and moderate doses. If you were losing weight steadily at 30 or 40 units but progress has stalled for four or more weeks despite consistent diet and activity, increasing to 50 units is a reasonable clinical decision. The additional milligrams can provide the metabolic boost needed to resume progress. Some people experience no weight loss after four weeks at a given dose, which is often the trigger for escalation.
Your appetite suppression has weakened
Some people notice that the appetite-suppressing effects of semaglutide diminish at a given dose over time. This is not failure. It is a signal that your body has adapted and may benefit from an upward adjustment. If appetite suppression was strong initially but has faded at your current dose, moving to 50 units (if it represents a higher mg dose than your current one) could restore that effect.
Your provider has confirmed the dose is appropriate
This one matters most. If a qualified healthcare provider has reviewed your labs, weight loss progress, side effect profile, and overall health, and has specifically prescribed a dose that works out to 50 units on your syringe, then it is appropriate for you. Individual variation in semaglutide response is significant. Some people need higher doses than others to achieve the same effect. Some metabolize the drug faster. Some have more GLP-1 receptor resistance. Your provider accounts for these factors in ways that a general guide cannot.
How to calculate what 50 units means for your specific vial
If you want to verify your dose at home, the math is simple. You need two numbers: the volume you are drawing (in mL) and the concentration on your vial label (in mg/mL).
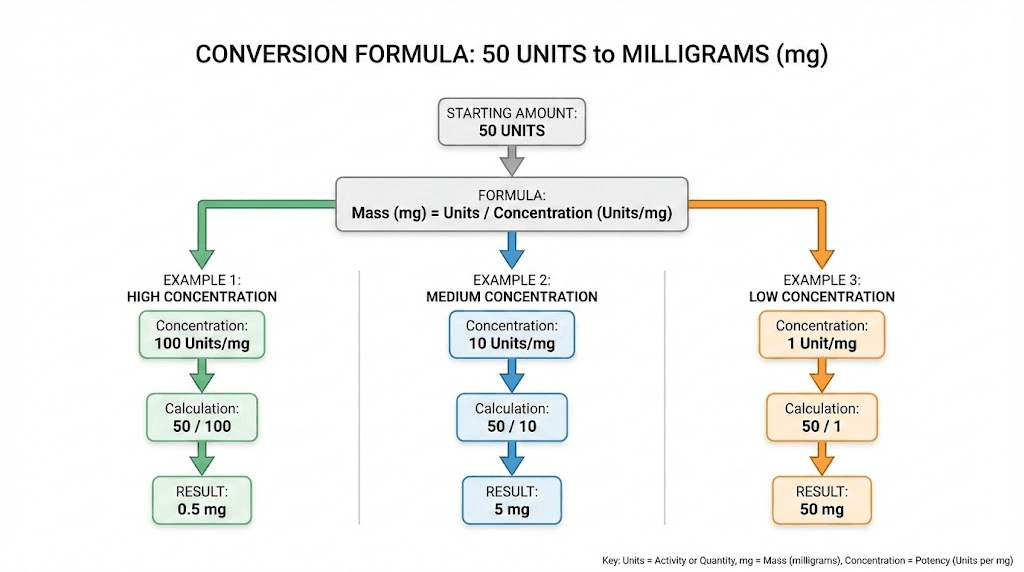
The formula
Dose in mg = (Units drawn / 100) x Concentration in mg/mL
Since 100 units = 1 mL on an insulin syringe:
50 units = 0.5 mL
Then multiply 0.5 mL by your concentration.
Worked examples
Example 1: 5 mg/mL vial
0.5 mL x 5 mg/mL = 2.5 mg
Example 2: 3 mg/mL vial
0.5 mL x 3 mg/mL = 1.5 mg
Example 3: 2.5 mg/mL vial
0.5 mL x 2.5 mg/mL = 1.25 mg
Example 4: 2 mg/mL vial
0.5 mL x 2 mg/mL = 1.0 mg
If your concentration does not match any of these common values, just plug your number into the formula. A 1.25 mg/mL vial at 50 units would give you 0.625 mg. A 10 mg/mL vial at 50 units would give you 5.0 mg, which is an extremely high dose and almost certainly not what was prescribed.
For those who prefer tools over manual math, the SeekPeptides semaglutide dosage calculator handles these conversions automatically. Enter your vial concentration and desired dose, and it tells you exactly how many units to draw. The peptide reconstitution calculator is also useful if you are working with lyophilized semaglutide that needs to be mixed with bacteriostatic water before use.
Double-check every time
Even experienced users should verify their calculation before every injection, especially when switching to a new vial or a new pharmacy. Compounded semaglutide concentrations can vary between pharmacies, and a switch from a 2.5 mg/mL vial to a 5 mg/mL vial means the same 50 units suddenly delivers twice the dose. The semaglutide injection guide covers the full process from calculation through injection technique.
What happens at doses above and below 50 units
Understanding where 50 units sits requires knowing what other common dose markings look like in practice. This context helps you see the full picture.
Common doses below 50 units
At 5 mg/mL concentration:
5 units (0.25 mg): Starting dose. Minimal side effects expected. The goal is not weight loss but rather getting your body accustomed to the medication.
10 units (0.5 mg): Second escalation step. Early appetite changes may begin. Most people start noticing reduced hunger around this dose. Learn more about what 10 units equals in mg across different concentrations.
20 units (1.0 mg): Mid-range dose where meaningful weight loss typically begins. Our guide on 20 units of semaglutide covers this dose in detail.
35 units (1.75 mg): Upper-mid dose. Strong appetite suppression. Side effects are well-managed by this point for most people who have escalated properly.
40 units (2.0 mg): High dose approaching maintenance. See 40 units of semaglutide in mg for detailed conversion information.
Common doses above 50 units
Drawing more than 50 units from a syringe is less common but does happen, particularly at lower concentrations where higher volumes are needed to reach therapeutic doses.
60 units at 2 mg/mL: 1.2 mg. Mid-range dose.
80 units at 2 mg/mL: 1.6 mg. Upper-mid dose.
100 units at 2 mg/mL: 2.0 mg. High dose. See our guide on 100 units of semaglutide in mg.
At higher concentrations, going above 50 units means very high milligram doses. Drawing 60 units from a 5 mg/mL vial would deliver 3.0 mg, which exceeds standard protocols. This is not recommended without specific medical guidance.
The sweet spot varies by person
There is no universal "right" number of units. The sweet spot depends on your concentration, body weight, metabolic response, and side effect tolerance. Some people achieve excellent results at 30 units. Others need 50 or more. The important thing is that the milligram dose behind those units aligns with established therapeutic ranges and that your escalation has been gradual.
Body weight, BMI, and how they influence your ideal dose
A question that comes up frequently: do heavier people need higher semaglutide doses? The answer is nuanced.
Semaglutide is not weight-based
Unlike some medications that are dosed by body weight (X mg per kg), semaglutide follows a fixed-dose escalation schedule. A person weighing 180 pounds follows the same 0.25 to 2.4 mg escalation as a person weighing 300 pounds. The BMI requirements for GLP-1 medications determine eligibility, but the dosing protocol itself is the same for everyone.
That said, clinical data shows some trends. People with higher starting body weight tend to lose a smaller percentage of their total weight compared to lighter individuals at the same dose, though they often lose more absolute pounds. This has led some researchers and clinicians to explore whether higher doses might be more appropriate for people with severe obesity.
Higher doses in research
Recent studies have tested semaglutide at doses up to 7.2 mg and even 16 mg weekly. At 7.2 mg (triple the standard maximum), participants lost an average of 13.2% of body weight compared to 10.4% at the standard 2.4 mg dose. Nearly a third of patients on the higher dose lost 25% or more of their starting weight.
These higher doses are not yet approved for clinical use. They are still in research phases. But they suggest that for some people, especially those with higher starting BMI, the current maximum of 2.4 mg may not be the optimal dose. This is relevant to the 50-unit question because at certain concentrations, 50 units represents a dose well below these experimental levels.
What this means for your 50-unit dose
If you are a larger individual and 50 units at your concentration equals 1.0 or 1.25 mg, you are likely on a moderate dose with room to increase. If you weigh less and 50 units equals 2.5 mg, you are on a relatively aggressive dose proportional to your body size. Body weight does not change the math of how many milligrams you are injecting, but it changes the context for interpreting whether that dose is appropriate for you specifically.
The speed at which semaglutide works also varies with body composition. Higher doses tend to produce faster initial results, but the trajectory of weight loss usually follows a similar curve regardless of starting dose, with the most dramatic losses occurring in the first three to six months.
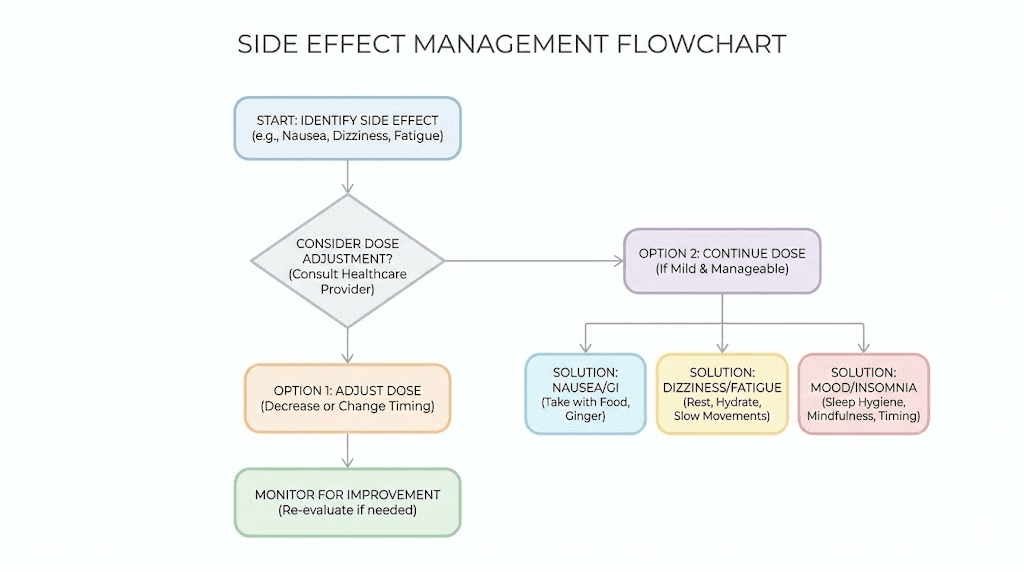
Managing side effects if 50 units feels like a lot
If you are experiencing uncomfortable side effects at 50 units, you have several options. The goal is not to suffer through side effects, but to find the dose that produces results while remaining tolerable.
Slow down the escalation
The standard schedule increases doses every four weeks. But this is a minimum, not a mandate. If 50 units is causing significant nausea, your provider may recommend staying at a lower dose for six to eight weeks instead of four before attempting to increase again. Many providers take a slower approach with compounded semaglutide, using smaller increments between dose steps.
Adjust injection timing
The best time of day to take semaglutide can affect how you experience side effects. Some people find that injecting in the evening allows them to sleep through the initial nausea peak. Others prefer morning injections so the queasiness passes during the active part of their day. Experiment with timing to see what works for your body.
Modify your diet around injection day
Eating smaller, lighter meals on the day of injection and the following day can reduce nausea significantly. Avoid fatty, greasy, or heavy foods during this window. The foods to eat while on semaglutide guide provides a detailed meal framework, and the semaglutide diet plan offers week-by-week nutrition guidance. There are also specific foods to avoid on semaglutide that tend to worsen GI symptoms at higher doses.
Stay hydrated
This sounds simple, and it is. But dehydration amplifies nearly every semaglutide side effect. Nausea feels worse when dehydrated. Dizziness worsens. Constipation compounds. Fatigue deepens. At higher doses where appetite is strongly suppressed, many people forget to drink enough water because the act of consuming anything feels unappealing. Make hydration intentional. Set reminders if needed.
Consider stepping back temporarily
If 50 units is genuinely intolerable, stepping back to your previous dose for two to four additional weeks is a valid strategy. This is not failure. It is smart dosing. The Wegovy prescribing information specifically states that patients who do not tolerate a dose during escalation should consider a four-week delay. Your body may need more time to adapt before attempting 50 units again.
Optimize injection technique
Proper injection technique affects absorption and side effect intensity. Injecting into a site with good subcutaneous fat, at the correct depth, at the right angle, all of these matter. Our guide on the best injection site for semaglutide covers optimal locations, and the broader where to inject GLP-1 guide explains rotation patterns that reduce injection site reactions and improve consistency.
Address specific symptoms
Different side effects have different solutions:
Constipation: The semaglutide constipation treatment guide covers fiber supplementation, osmotic laxatives, and dietary adjustments
Headaches: Often dehydration-related. The GLP-1 headache guide covers prevention and treatment
Fatigue: May improve with energy-supporting strategies and adequate protein intake
Hair thinning: A less common but documented side effect at higher doses, covered in our GLP-1 hair loss guide
Common questions providers hear about 50 units
Healthcare providers prescribing semaglutide hear certain questions repeatedly from patients drawing 50 units. Here are the most common ones, with the answers that experienced clinicians typically give.
Can I stay at 50 units long-term
Yes. If 50 units produces good results and tolerable side effects, there is no clinical reason to continue escalating. The goal is not to reach the maximum dose. The goal is to find the effective dose, the lowest amount that achieves your weight management objectives. Some people maintain excellent results at doses well below the maximum for years. Others need the full maintenance dose. Both are appropriate.
Understanding how long you stay on semaglutide depends on individual goals, but many people remain on the medication indefinitely for weight maintenance.
Should I increase past 50 units
Only if you meet three criteria: (1) you have been on the current dose for at least four weeks, (2) weight loss has stalled or appetite suppression has weakened, and (3) your provider agrees an increase is appropriate. Never increase your dose independently. The difference between effective dosing and overdosing can be narrow at higher concentrations.
Is it normal that 50 units causes more side effects than my previous dose
Completely normal. Side effects tend to re-emerge with each dose escalation and then settle within two to four weeks. This pattern is so consistent that it is built into the standard escalation protocol. The four-week minimum between increases exists specifically to allow your body time to adapt. If side effects from 50 units have not improved after four weeks, that is when to consider adjusting rather than waiting longer.
My friend takes 50 units too but from a different pharmacy. Are we on the same dose
Almost certainly not, unless you have verified that both vials have identical concentrations. Different pharmacies compound at different concentrations. One 50-unit dose could be 1.0 mg while another is 2.5 mg. This is why comparing doses in units with other people is misleading. Always compare in milligrams, and always verify concentration before assuming anything about dose equivalence.
Comparing 50 units across different GLP-1 medications
Semaglutide is not the only GLP-1 receptor agonist on the market. If you are considering switching medications, or if you are curious how your 50-unit semaglutide dose compares to other options, this section provides context.
Semaglutide vs tirzepatide at 50 units
Tirzepatide (the active ingredient in Mounjaro and Zepbound) is a dual GIP/GLP-1 agonist that also comes in compounded multi-dose vials. Like semaglutide, tirzepatide dosage in units depends entirely on vial concentration. At the same concentration, 50 units of tirzepatide delivers a different clinical effect than 50 units of semaglutide because the drugs have different potencies and mechanisms.
The tirzepatide vs semaglutide dosage chart provides a detailed head-to-head comparison of equivalent doses. In general, tirzepatide tends to produce greater weight loss at comparable escalation stages, though it uses a different dosing scale (starting at 2.5 mg and escalating to 15 mg). See also the semaglutide vs tirzepatide comparison for a broader overview of efficacy, side effects, and cost.
For those exploring the transition between these medications, the semaglutide to tirzepatide conversion chart maps equivalent doses. And the switching guide covers the process in the other direction, including how to translate your current unit dose between the two medications.
How side effects compare at equivalent doses
The semaglutide vs tirzepatide side effects profile is similar in character but can differ in intensity. Both cause nausea, vomiting, diarrhea, and constipation. Both have dose-dependent side effect rates. At comparable therapeutic doses, some studies suggest tirzepatide may cause slightly less nausea than semaglutide, though individual experiences vary widely.
Newer GLP-1 options
Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, is in late-stage clinical trials and showing even greater weight loss potential than current options. Our guides on retatrutide vs semaglutide and the retatrutide dose guide explore what this next-generation medication may offer. There are also emerging options like survodutide and mazdutide that target similar pathways with different pharmacological profiles.
Semaglutide formulations and how they affect the 50-unit question
The type of semaglutide product you are using also affects how to think about 50 units.
Brand-name pre-filled pens
If you are using Ozempic or Wegovy, the 50-unit question does not apply in the same way. These products use pre-filled multi-dose pens with dial-up dosing. You select your dose in milligrams using the pen mechanism, not by drawing units from a vial. The pen handles the concentration math for you. So "50 units" is not a concept that arises with these devices.
However, some patients switch from brand-name pens to compounded vials for cost reasons. When making this switch, the dose translation is critical. If you were on 1.0 mg of Ozempic and switch to a compounded 5 mg/mL vial, your 1.0 mg dose requires just 20 units, not 50. Drawing 50 units from the same vial would give you 2.5 mg, a 150% overdose. The compounded semaglutide guide covers this transition process in detail.
Compounded vials
This is where the 50-unit question is most relevant. Compounded semaglutide vials require you to draw the correct volume using an insulin syringe, and the concentration varies between products and pharmacies. Always verify your concentration before calculating your dose. If you are unsure about your vial, the guide on what color semaglutide should be can help you visually identify whether your vial appears normal.
Some compounded formulations include additives like vitamin B12, methylcobalamin, or glycine. These additives do not change the semaglutide concentration or the unit-to-mg conversion. The concentration listed on the label refers to the semaglutide content, not the total dissolved solids.
Oral and sublingual formulations
The 50-unit question does not apply to oral semaglutide drops or sublingual semaglutide formulations. These are dosed in milligrams directly, without the intermediate step of unit conversion. If you are using an oral formulation, your dose is straightforward. The comparison between injectable vs oral peptides covers the differences in bioavailability, dosing, and convenience.
Storage and handling at any dose
Regardless of whether 50 units is a high or moderate dose for your concentration, proper storage preserves the potency of every unit you inject. Poor storage means degraded medication, which means reduced efficacy, which means the dose you think you are getting is not the dose your body receives.
Compounded semaglutide must be refrigerated. The guide on how long compounded semaglutide lasts in the fridge covers shelf life in detail, and our guide on refrigeration requirements explains the temperature ranges that preserve potency. If you have accidentally left semaglutide out overnight, the impact on your dose effectiveness depends on how long and at what temperature the vial was exposed.
The overall shelf life of semaglutide and whether semaglutide expires after 28 days are common questions that affect dosing accuracy. Using expired or improperly stored medication is like injecting a lower dose than what the label claims, which means your 50 units may not actually be delivering the expected milligrams. Always check expiration dates and storage conditions, and see our guide on using expired semaglutide if you have concerns about your vial.
Practical tips for people on 50 units
Whether 50 units is your starting point, your current escalation step, or your maintenance dose, these practical considerations will help you get the most from your protocol.
Use the right syringe size
For 50 units, a 0.5 mL (50-unit) or 1.0 mL (100-unit) insulin syringe works. The smaller syringe offers more precise markings at the 50-unit level, making it easier to draw the exact amount. If you are drawing doses below 30 units, consider a 0.3 mL syringe for even better precision. The injection guide covers syringe selection in more detail.
Keep a dose log
Track your injection date, time, dose in units, dose in mg (calculated from your concentration), injection site, and any side effects. This log becomes invaluable when discussing dosing adjustments with your provider. It also helps you identify patterns, such as side effects being worse with certain injection sites or times of day. The GLP-1 plotter tool can help visualize your progress over time.
Plan around your injection day
At 50 units (especially at higher mg doses), the day of injection and the following day may bring stronger side effects. Schedule your injection for a day when you can afford to take it easy. Some people prefer Friday evenings so any nausea peaks on Saturday rather than during work. Find what works for your schedule, and check our best time to take GLP-1 shot guide for more timing strategies.
Do not skip doses
Missing a semaglutide injection can lead to a mini cycle of withdrawal-like symptoms, including appetite rebound and GI irregularity when you resume. Consistency matters more at higher doses where your body has adapted to steady GLP-1 receptor activation. If you need to travel, our guide on how to travel with semaglutide covers everything from TSA rules to temperature management on the go.
Support your nutrition
Higher doses suppress appetite more aggressively, which can lead to inadequate protein and micronutrient intake. This is not a minor issue. Insufficient protein accelerates muscle loss during weight loss, which undermines your metabolic rate and long-term outcomes. The semaglutide diet plan provides macro targets, while the protein shakes for GLP-1 guide covers supplementation strategies for people who struggle to eat enough on higher doses.
Monitor your results objectively
At 50 units, you should be seeing measurable changes if you have been on semaglutide for several weeks. Our semaglutide one-month results guide describes what typical progress looks like at each escalation stage. And the before and after semaglutide article provides real-world context for the range of outcomes people experience.
Drug interactions and lifestyle factors at higher doses
At 50 units (particularly at higher concentrations where the mg dose is significant), interactions with other substances and lifestyle factors become more relevant.
Alcohol
Combining semaglutide with alcohol is not contraindicated, but higher GLP-1 doses can alter how your body processes alcohol. Delayed gastric emptying means alcohol stays in the stomach longer, which can intensify its effects. Many people report lower alcohol tolerance on semaglutide. The semaglutide and alcohol guide covers safe consumption practices and warning signs to watch for.
Other medications
If you are taking phentermine alongside semaglutide, the combined appetite suppression at higher doses can be intense. Some providers prescribe this combination intentionally, but it requires careful monitoring. Our phentermine vs semaglutide comparison helps clarify when each medication is more appropriate and whether combining them makes sense for your situation. Understanding whether phentermine is a GLP-1 also helps clarify the difference between these drug classes.
Exercise
Higher semaglutide doses do not preclude exercise, but they may require adjustments. Intense workouts on days when nausea is peaking from a fresh injection are unpleasant and potentially unsafe if dehydration is present. Time your workouts for days when GI symptoms are lowest, typically three to five days after injection. And yes, you absolutely can lose weight on semaglutide without exercise, but combining the two produces better body composition outcomes.
Surgery considerations
If you are scheduled for surgery, your semaglutide dose becomes relevant. The delayed gastric emptying effect is dose-dependent, and anesthesiologists need to know you are taking it. Our guide on when to resume semaglutide after surgery covers pre-surgical holding periods and post-operative restart protocols.
Reconstitution and preparation for 50-unit doses
If you are working with lyophilized (freeze-dried) semaglutide that requires reconstitution, the concentration you create depends on how much bacteriostatic water you add. This means you directly control whether your 50 units will be a high dose or a moderate one.
The how to reconstitute semaglutide guide walks through the complete process. For a 5 mg vial specifically, the 5mg semaglutide reconstitution guide provides exact water volumes for different target concentrations. And the 10mg semaglutide mixing guide covers higher-quantity vials.
Here is the critical relationship between water volume and what 50 units delivers from a 5 mg vial:
Bacteriostatic water added | Resulting concentration | 50 units delivers |
|---|---|---|
1 mL | 5 mg/mL | 2.5 mg (high) |
2 mL | 2.5 mg/mL | 1.25 mg (moderate) |
2.5 mL | 2 mg/mL | 1.0 mg (moderate-low) |
5 mL | 1 mg/mL | 0.5 mg (low) |
Notice how adding more water makes the same 50 units deliver less active ingredient. This is why reconstitution accuracy matters enormously. The peptide reconstitution calculator can verify your concentration before you draw any doses, and the general peptide calculator provides additional verification.
What SeekPeptides members say about dose optimization
The dosing question, whether 50 units is a lot, is one of the most frequently discussed topics in the SeekPeptides community. Members consistently report that understanding concentration was the turning point in their semaglutide experience. Many were confused about their dose for weeks before realizing that comparing units without concentration is meaningless.
SeekPeptides provides personalized dosing calculators, comprehensive protocol guides, and community support specifically designed to eliminate this kind of confusion. Members access detailed escalation schedules tailored to their specific vial concentrations, troubleshooting resources for side effect management, and evidence-based guidance on when to escalate, hold, or reduce their dose.
Week-by-week expectations when escalating to 50 units
If your provider has prescribed a dose that works out to 50 units on your syringe, knowing what to expect during the escalation helps you stay on track and recognize whether your experience is normal.
The first four weeks at your new dose
The transition to a higher dose follows a predictable pattern, and knowing that pattern makes the adjustment significantly easier to navigate.
Week one after any dose increase is typically the roughest. Your body is encountering more GLP-1 receptor activation than it had at the previous dose, and the gastrointestinal system needs time to recalibrate. Expect increased nausea for two to four days following the first injection at the new dose. This usually peaks 24 to 48 hours after injection and then gradually fades.
By week two, most people notice the nausea becoming less intense. Appetite suppression, however, becomes more noticeable. You may find yourself forgetting to eat or feeling satisfied after very small portions. This is the medication working as designed. The challenge is ensuring you still consume adequate nutrition, particularly protein.
Weeks three and four represent the adaptation phase. Side effects should be settling into a manageable pattern. If they are not, if the nausea is still as intense as week one, your body is signaling that it needs more time. This is when to consult your provider about holding at the previous dose for an additional four weeks before re-attempting the increase.
Months two and three at 50 units
Once you have adapted to the dose, the next two months are where results accelerate. Weight loss typically follows a pattern: a modest initial drop (often partially water weight), followed by steady fat loss of 1 to 2 pounds per week at therapeutic doses. The exact rate depends on your caloric deficit, activity level, and metabolic factors.
During this period, you will likely notice changes beyond the scale. Clothes fitting differently. Energy levels stabilizing after the initial adjustment period. Appetite suppression becoming more consistent rather than fluctuating wildly between injection days. Some people describe a sense of "food noise" quieting, where the constant mental chatter about eating and snacking gradually fades into the background.
This is also when you should be tracking your progress systematically. Weigh yourself at the same time each week (not daily, as water weight fluctuations can be misleading). Take measurements. Note how your energy, sleep, and mood are trending. The semaglutide one-month results guide provides benchmarks for what typical progress looks like, so you can calibrate your expectations.
Long-term maintenance at 50 units
If 50 units becomes your maintenance dose, the long-term picture is generally positive. Clinical trials lasting 68 weeks showed that participants on semaglutide maintained significant weight loss throughout the treatment period, with continued improvements in metabolic markers including blood sugar, blood pressure, and cholesterol levels.
The key to long-term success at any dose is consistency. Taking your injection at the same time each week, maintaining supportive nutrition habits, staying active, and communicating with your provider about how the medication is working. Weight regain after stopping semaglutide is well-documented, which is why many people remain on the medication indefinitely as part of a chronic disease management approach. If you are considering whether to stay on or eventually discontinue, understanding potential semaglutide withdrawal symptoms helps you plan for either scenario.
Common mistakes people make at 50 units
After guiding thousands of semaglutide users through dosing questions, certain mistakes come up repeatedly. Avoiding these can save you from unnecessary side effects, wasted medication, and frustrating stalls in progress.
Comparing unit doses with other people
This is the number one mistake. You tell a friend you are on 50 units. They are on 50 units too. You assume you are on the same dose. You are not. Different concentrations mean different milligram doses. Always compare in milligrams, never in units. When someone asks about your semaglutide dose, give the answer in milligrams and mention your concentration. This prevents confusion and ensures any advice you receive from peers or online communities is relevant to your actual dose.
Skipping the escalation
Some people, eager for faster results, jump from 20 units straight to 50 units, skipping intermediate steps. This almost always backfires. The dose-dependent increase in side effects is not linear. Going from 1.0 mg to 2.5 mg in one step (at 5 mg/mL) is likely to produce severe nausea, vomiting, and potentially dehydration. The gradual escalation exists because each step allows your GLP-1 receptors, your gut motility, and your neurological appetite circuits to adapt incrementally.
Not adjusting when switching pharmacies
Switching compounding pharmacies without recalculating your dose is dangerous. If your old pharmacy used 2.5 mg/mL and your new one uses 5 mg/mL, your 50 units just went from 1.25 mg to 2.5 mg. That is a doubling of your dose with zero titration. Every time you start a vial from a different source, check the concentration and recalculate. Use the semaglutide dosage calculator to verify before your first injection from any new vial.
Ignoring injection site rotation
At 50 units, you are injecting a full 0.5 mL of liquid subcutaneously. That is a noticeable volume. Injecting into the same spot repeatedly can lead to lipodystrophy (changes in fat tissue), inconsistent absorption, and increased discomfort. Rotate between the abdomen, thigh, and upper arm. The best injection site guide maps out a rotation schedule that ensures each area has adequate recovery time between injections.
Not eating enough protein
At higher doses where appetite suppression is strong, many people default to eating whatever is easiest, which often means carbohydrates and processed foods in small amounts. This leads to muscle loss, metabolic slowdown, and a disappointing body composition even when the scale moves in the right direction. Aim for at least 0.7 grams of protein per pound of body weight daily. If eating that much solid food feels impossible on higher doses, the protein shake guide for GLP-1 users provides liquid alternatives that are easier to consume on suppressed appetite days.
Panicking about side effects during escalation
Some discomfort during dose escalation is expected. Mild nausea. Slightly reduced energy. Changes in bowel habits. These are signs that the medication is active and your body is adapting. The mistake is panicking and immediately reducing the dose before giving your body the standard two to four weeks to adapt. On the other hand, the bigger mistake is suffering through genuinely severe symptoms for weeks without contacting your provider. The line between "normal adjustment" and "dose is too high" is defined by severity and duration. Mild and temporary is normal. Severe and persistent is not.
Frequently asked questions
Is 50 units of semaglutide the same as 50 mg?
No. Units and milligrams measure completely different things. Units measure the volume of liquid in an insulin syringe (50 units = 0.5 mL). Milligrams measure the weight of the active drug in that liquid. At a 5 mg/mL concentration, 50 units contains 2.5 mg of semaglutide, not 50 mg. The difference between units and milligrams is one of the most common sources of dosing confusion.
Can 50 units of semaglutide be dangerous?
At most concentrations, 50 units falls within the established therapeutic range and is not dangerous when prescribed appropriately and escalated gradually. At 5 mg/mL concentration, 50 units delivers 2.5 mg, which slightly exceeds the standard 2.4 mg maximum. This is generally safe under medical supervision, but self-escalating to this dose without provider guidance is risky. Severe dizziness, persistent vomiting, or signs of dehydration warrant immediate medical attention regardless of dose.
How do I know if I should increase or decrease from 50 units?
Increase if weight loss has stalled for four or more weeks, appetite suppression has weakened, and side effects are minimal. Decrease if side effects are severe, persistent, or interfering with daily function. In either case, make the adjustment in consultation with your prescriber. Never change your dose independently. The 1.7 mg unit conversion guide can help if your provider recommends stepping up to the next standard dose.
Why does my pharmacy use a different concentration than my previous one?
Compounding pharmacies operate independently and use different formulation protocols. One pharmacy might compound at 5 mg/mL while another uses 2.5 mg/mL. Both are valid concentrations. But switching between them without adjusting your unit dose means your milligram dose changes dramatically. Always verify concentration when starting a vial from a new pharmacy and recalculate your units accordingly.
Is 50 units too much for a starting dose?
At virtually every concentration, yes. The standard starting dose is 0.25 mg weekly, which equals 5 units at 5 mg/mL or 12.5 units at 2 mg/mL. Starting at 50 units would deliver 1.0 to 2.5 mg depending on concentration, which is far above the recommended starting level and would likely cause severe nausea and vomiting. Always start at the lowest prescribed dose and escalate gradually.
How many mg is 50 units at a 1 mg/mL concentration?
At 1 mg/mL, 50 units (0.5 mL) delivers exactly 0.5 mg of semaglutide. This is the second step on the standard Wegovy escalation schedule and represents a very early, low dose. At this concentration, 50 units is not a lot at all. Check the units to mg conversion guide for additional concentration calculations.
Does body weight affect how 50 units feels?
Indirectly, yes. A larger person may process the same milligram dose differently than a smaller person, potentially experiencing less intense appetite suppression at the same dose. However, semaglutide is not dosed by body weight. The standard escalation schedule is the same regardless of starting weight. The BMI for GLP-1 guide covers eligibility, but body weight does not change the mg-per-unit conversion.
What if I accidentally drew more than 50 units?
If you drew slightly more (55 to 60 units), the additional dose is unlikely to cause serious harm but may increase side effects temporarily. Monitor for severe nausea and stay hydrated. If you accidentally drew significantly more (80 to 100 units), contact your healthcare provider immediately. Our guide on accidental dosing situations covers related scenarios and recommended responses.
For researchers serious about optimizing their semaglutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based dosing guides, personalized calculators, and a community of thousands who have navigated these exact dosing questions.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay clear, your calculations stay accurate, and your doses stay effective.