Feb 8, 2026

Two medications. Two completely different dosing schedules. And a mountain of confusion sitting between them.
If you have spent any time comparing tirzepatide and semaglutide, you already know the basics. Both are GLP-1 receptor agonists used for weight management. Both require weekly injections. Both follow a slow escalation protocol designed to minimize side effects. But the dosing charts? They look nothing alike. The milligram numbers do not translate one to one. The escalation timelines differ. The unit conversions from compounded vials add another layer of math most people were not expecting.
That gap between the two dosing charts is where mistakes happen. Researchers switch from one to the other without understanding conversion. They compare milligram numbers that were never meant to be compared directly. They plateau on semaglutide and wonder if the "equivalent" tirzepatide dose would work better, without realizing no true equivalence exists.
This guide puts both dosing charts side by side for the first time, with every escalation step, every unit conversion, and every piece of clinical data you need to understand the actual relationship between these two weight loss peptides. Whether you are starting fresh, comparing options, or considering a switch, the numbers here come directly from FDA prescribing information and clinical trial data. SeekPeptides has compiled everything into one reference, because the internet gives you bits and pieces of each chart but rarely puts them together in a way that actually helps.
No guessing. No rough estimates. Just the dosing data, organized the way it should have been from the start.
How semaglutide dosing works
Semaglutide was the first GLP-1 receptor agonist to gain widespread attention for weight management. It binds to GLP-1 receptors in the brain, gut, and pancreas, reducing appetite, slowing gastric emptying, and improving blood sugar regulation. The medication comes in both branded pen form (Wegovy for weight loss, Ozempic for diabetes) and compounded vial form.
The dosing follows a strict five-step escalation protocol. You do not start at the effective dose. You build up to it over 16 to 20 weeks.
Here is the complete schedule.
Semaglutide escalation chart (FDA approved for weight loss)
Phase | Weekly dose | Duration | Purpose |
|---|---|---|---|
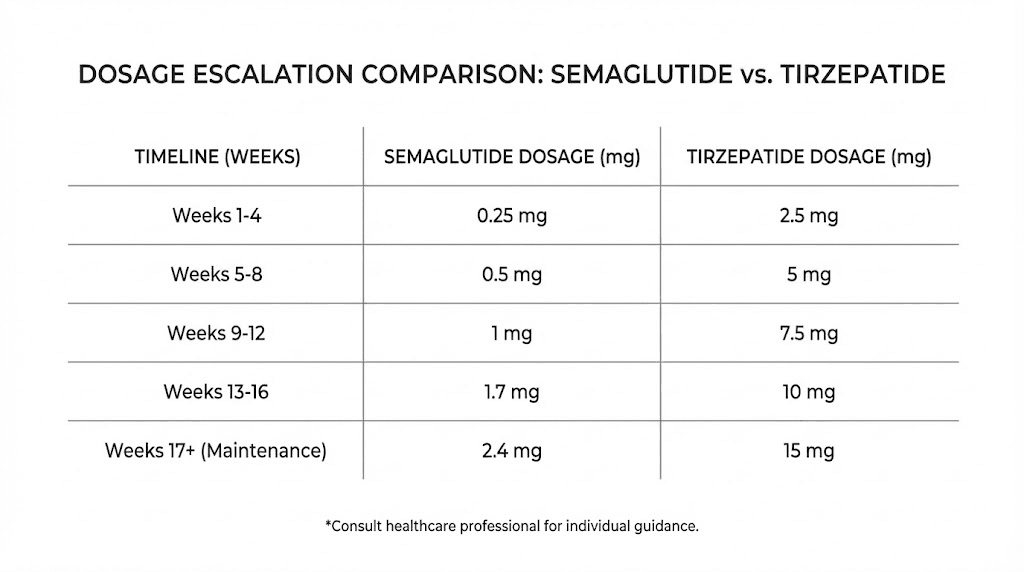
Step 1 | 0.25 mg | Weeks 1-4 | Initial tolerance assessment |
Step 2 | 0.5 mg | Weeks 5-8 | Low therapeutic range |
Step 3 | 1.0 mg | Weeks 9-12 | Moderate therapeutic dose |
Step 4 | 1.7 mg | Weeks 13-16 | High therapeutic dose |
Step 5 (max) | 2.4 mg | Week 17 onward | Maximum maintenance dose |
Each step lasts a minimum of four weeks. Some providers extend individual steps to six or eight weeks if side effects are significant. The goal is reaching 2.4 mg, but not everyone gets there. Some people find their optimal dose at 1.0 mg or 1.7 mg and stay there.
A few things most dosage charts do not mention. The 0.25 mg starting dose is not really therapeutic for weight loss. It exists purely for gastrointestinal adaptation. Most appetite suppression begins at 0.5 mg, with significant effects kicking in around 1.0 mg. The jump from 1.7 mg to 2.4 mg is where most people report the strongest appetite reduction, but also where side effects peak.
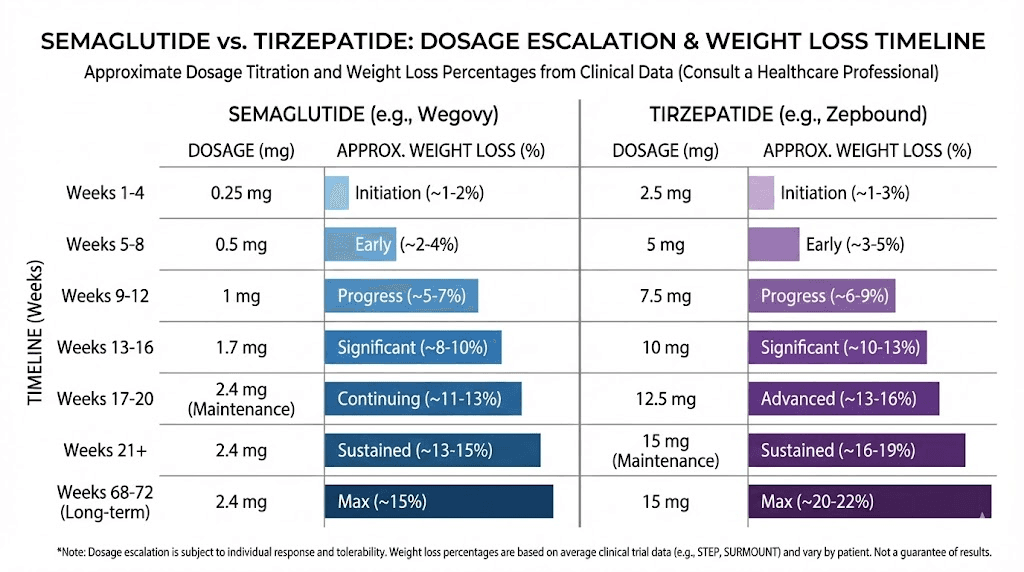
The STEP 1 clinical trial showed participants on 2.4 mg semaglutide lost an average of 14.9% of body weight over 68 weeks. That is roughly 33 pounds for someone starting at 220 pounds. But this number represents the average at maximum dose with full compliance. Real world results vary depending on how quickly someone escalates and whether they tolerate the full 2.4 mg.
Semaglutide units conversion for compounded vials
If you are using compounded semaglutide from a vial rather than a branded pen, you need to convert milligrams to units based on concentration. This is where things get tricky, because different pharmacies use different concentrations.
The most common compounded concentration is 2.5 mg/mL. Here is what that looks like on a standard insulin syringe (100 units = 1 mL).
Dose (mg) | Volume at 2.5 mg/mL | Units on syringe |
|---|---|---|
0.25 mg | 0.10 mL | 10 units |
0.5 mg | 0.20 mL | 20 units |
1.0 mg | 0.40 mL | 40 units |
1.7 mg | 0.68 mL | 68 units |
2.4 mg | 0.96 mL | 96 units |
At a concentration of 5 mg/mL (which some pharmacies provide), all the unit numbers get cut in half. A 2.4 mg dose becomes 48 units instead of 96. This is why you absolutely must verify your concentration before drawing a dose. Using our semaglutide dosage calculator eliminates the guesswork from this conversion. Just input your vial concentration and target dose, and it returns the exact units.
The formula is simple but unforgiving if you get it wrong: dose (mg) divided by concentration (mg/mL) multiplied by 100 equals units on syringe. A 1.0 mg dose at 2.5 mg/mL concentration equals 0.4 mL, which equals 40 units. Get the concentration wrong and you could easily double or halve your actual dose.
How tirzepatide dosing works
Tirzepatide is fundamentally different from semaglutide at the receptor level. Where semaglutide activates only GLP-1 receptors, tirzepatide activates both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors. This dual mechanism is why tirzepatide produces greater weight loss in clinical trials and why the dosing numbers look completely different.
The escalation protocol has six steps instead of five.
Tirzepatide escalation chart (FDA approved for weight loss)
Phase | Weekly dose | Duration | Purpose |
|---|---|---|---|
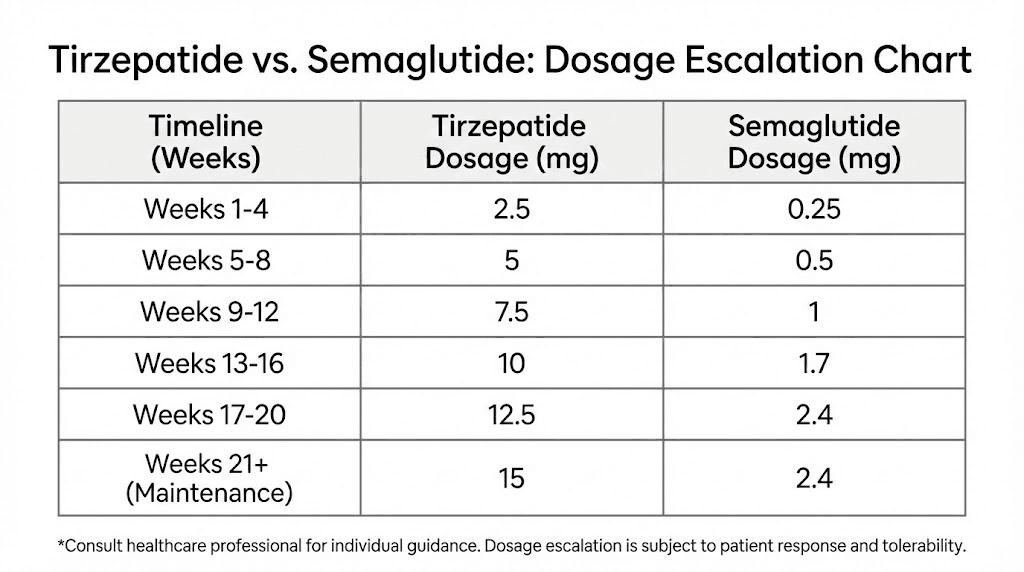
Step 1 | 2.5 mg | Weeks 1-4 | Initial tolerance assessment |
Step 2 | 5.0 mg | Weeks 5-8 | Low therapeutic range |
Step 3 | 7.5 mg | Weeks 9-12 | Moderate therapeutic dose |
Step 4 | 10.0 mg | Weeks 13-16 | High therapeutic dose |
Step 5 | 12.5 mg | Weeks 17-20 | Advanced dose |
Step 6 (max) | 15.0 mg | Week 21 onward | Maximum maintenance dose |
Notice the pattern. Every step increases by exactly 2.5 mg. This uniformity makes the tirzepatide escalation more predictable than semaglutide, where the jumps are uneven (0.25, then 0.5, then 0.7, then 0.7 again). Tirzepatide takes 20 weeks to reach maximum dose, compared to semaglutide's 16 weeks.
Like semaglutide, the starting dose of 2.5 mg is not the therapeutic dose. It exists to let your gut adjust. Meaningful appetite suppression typically begins at 5.0 mg, with significant weight loss acceleration happening at 10.0 mg and above.
The SURMOUNT-1 trial showed participants on 15 mg tirzepatide lost an average of 22.5% of body weight over 72 weeks. Even at 10 mg, weight loss averaged 19.5%. These numbers substantially exceed what semaglutide delivers at its maximum dose, which is exactly what you would expect from a medication hitting two receptor systems instead of one.
Do not make the mistake of comparing 2.4 mg semaglutide to 2.5 mg tirzepatide. Those numbers look similar but they describe completely different things. The milligrams refer to different molecular weights, different receptor affinities, and different potency profiles. A 2.5 mg dose of tirzepatide and a 0.25 mg dose of semaglutide are both "starting doses" that serve the same purpose, tolerance building, but the actual pharmacology behind each number is unique.
Tirzepatide units conversion for compounded vials
Compounded tirzepatide commonly comes in concentrations of 10 mg/mL or 20 mg/mL. Here is the conversion chart for each.
At 10 mg/mL concentration:
Dose (mg) | Volume at 10 mg/mL | Units on syringe |
|---|---|---|
2.5 mg | 0.25 mL | 25 units |
5.0 mg | 0.50 mL | 50 units |
7.5 mg | 0.75 mL | 75 units |
10.0 mg | 1.00 mL | 100 units |
12.5 mg | 1.25 mL | Requires two injections |
15.0 mg | 1.50 mL | Requires two injections |
At 10 mg/mL, anything above 10 mg requires more than 1 mL, which means you would need to split into two injections. This is why many pharmacies offer higher concentrations.
At 20 mg/mL concentration:
Dose (mg) | Volume at 20 mg/mL | Units on syringe |
|---|---|---|
2.5 mg | 0.125 mL | 12.5 units |
5.0 mg | 0.25 mL | 25 units |
7.5 mg | 0.375 mL | 37.5 units |
10.0 mg | 0.50 mL | 50 units |
12.5 mg | 0.625 mL | 62.5 units |
15.0 mg | 0.75 mL | 75 units |
The higher concentration keeps all doses in single-injection territory but requires more precise measuring. Drawing 12.5 units accurately on a standard insulin syringe is not easy. Many researchers prefer the 10 mg/mL concentration for lower doses and switch to 20 mg/mL once they pass 7.5 mg weekly.
The same formula applies: dose (mg) divided by concentration (mg/mL) multiplied by 100 equals units. Use our peptide calculator or the reconstitution calculator to double check your math. A miscalculation here means either wasted medication or an unexpectedly large dose.
Side-by-side dosage chart comparison
This is what most people are actually looking for. Both charts, next to each other, with all the context that makes the comparison meaningful.
Complete escalation comparison
Week | Semaglutide dose | Tirzepatide dose | Notes |
|---|---|---|---|
1-4 | 0.25 mg | 2.5 mg | Both starting doses for GI tolerance only |
5-8 | 0.5 mg | 5.0 mg | First therapeutic doses |
9-12 | 1.0 mg | 7.5 mg | Moderate appetite suppression begins |
13-16 | 1.7 mg | 10.0 mg | Strong therapeutic effect |
17-20 | 2.4 mg (max) | 12.5 mg | Semaglutide reaches max, tirzepatide continues |
21+ | 2.4 mg (maintenance) | 15.0 mg (max) | Tirzepatide reaches max 4 weeks later |
The timeline difference matters. Semaglutide reaches its ceiling at week 17. Tirzepatide does not hit maximum until week 21. That extra month of escalation gives the body more time to adapt and may contribute to tirzepatide's superior tolerability despite higher absolute doses.
But here is the detail that changes everything about this comparison. You cannot look at 2.4 mg semaglutide and 15 mg tirzepatide and think the numbers are proportional. These are different molecules with different molecular weights and different receptor binding profiles. The milligram dose reflects the mass of the peptide, not its biological activity. Comparing them by milligram is like comparing a mile to a kilometer. Both measure distance. Neither converts neatly into the other.
Clinical weight loss at each dose tier
The more useful comparison is what each dose actually achieves in terms of weight loss outcomes.
Dose tier | Semaglutide weight loss | Tirzepatide weight loss | Trial |
|---|---|---|---|
Low dose | ~6% at 0.5 mg | ~7% at 5 mg | STEP 2 / SURMOUNT-2 |
Mid dose | ~10% at 1.0 mg | ~15% at 10 mg | STEP 2 / SURMOUNT-1 |
Max dose | ~15% at 2.4 mg | ~22.5% at 15 mg | STEP 1 / SURMOUNT-1 |
Head to head (max) | 13.7% at max | 20.2% at max | SURMOUNT-5 |
The SURMOUNT-5 trial deserves special attention. This was the first head-to-head comparison, published in the New England Journal of Medicine. Participants received the maximum tolerated dose of either medication for 72 weeks. Tirzepatide delivered 20.2% body weight reduction versus 13.7% for semaglutide. That is a 6.5 percentage point difference, which on a 220 pound person translates to roughly 14 additional pounds lost.
Even more telling, gastrointestinal side effects causing treatment discontinuation were lower with tirzepatide (2.7%) than semaglutide (5.6%). The medication that produces more weight loss actually had fewer people quitting due to stomach problems. This challenges the assumption that more potent always means harder to tolerate.
Understanding dose equivalence (and why it does not exist)
This is the question everyone asks. What dose of tirzepatide equals what dose of semaglutide?
The honest answer is that no true equivalence exists. These medications work through different receptor mechanisms, have different pharmacokinetic profiles, and produce different physiological responses at every dose level. No medical organization has published an official conversion chart, and no clinical trial has established dose-for-dose equivalence.
That said, clinical experience has produced some rough approximations that providers use when switching patients. These are not official guidelines. They are practical observations.
Approximate dose correspondence (not equivalence)
Semaglutide dose | Approximate tirzepatide range | Clinical basis |
|---|---|---|
0.25 mg | 2.5 mg | Both are starting/tolerance doses |
0.5 mg | 2.5 - 5.0 mg | Similar GI and appetite effects |
1.0 mg | 5.0 - 7.5 mg | Comparable weight loss velocity |
1.7 mg | 7.5 - 10.0 mg | Matched by tolerability profile |
2.4 mg | 10.0 - 15.0 mg | Maximum dose range for both |
Notice how each semaglutide dose maps to a range of tirzepatide doses, not a single number. This ambiguity is intentional. The correspondence is loose at best. A person doing well on 1.7 mg semaglutide might transition to 7.5 mg tirzepatide and feel under-dosed, or they might find 10 mg too strong. Individual response varies enormously.
The GIP receptor component in tirzepatide adds a layer of unpredictability. Some people respond powerfully to GIP activation. Others barely notice it. This means two people on the same semaglutide dose could need very different tirzepatide doses to achieve similar effects.
What we do know from the switching protocols published by various clinical practices is that starting low and titrating up works better than trying to jump to an "equivalent" dose. The body needs time to adjust to the new receptor activation pattern regardless of prior GLP-1 experience.
Switching from semaglutide to tirzepatide: the dosing protocol
Switching is increasingly common. People plateau on semaglutide and want the greater weight loss potential of tirzepatide. Or they experience weight loss stalls on semaglutide and their provider recommends the dual-agonist approach.
The process is not as simple as stopping one and starting the other at what you think is equivalent.
Standard switching protocol
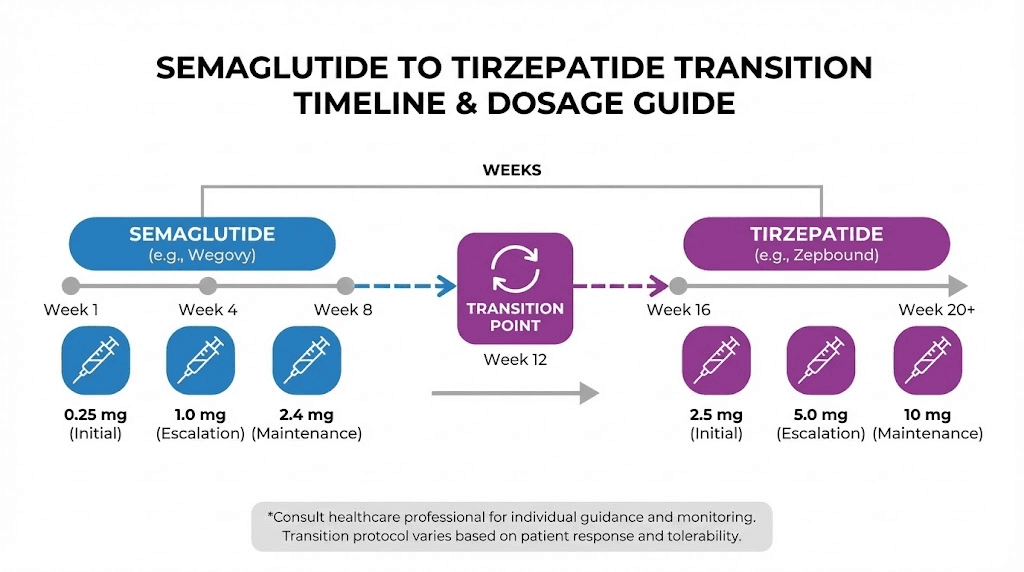
Step 1: Complete your last semaglutide dose. Take your final weekly injection as scheduled.
Step 2: Wait approximately one week. Start tirzepatide on your next scheduled injection day. The gap allows semaglutide levels to begin declining while maintaining some receptor coverage.
Step 3: Begin tirzepatide at 2.5 mg. Regardless of your previous semaglutide dose, every switching protocol starts here. Even if you were on maximum 2.4 mg semaglutide, you start at the lowest tirzepatide dose. This is not a step backward. It is a safety requirement because tirzepatide activates GIP receptors that semaglutide never touched.
Step 4: Escalate normally. Follow the standard 4-week escalation schedule. Some providers allow faster titration for patients who were on high dose semaglutide, moving to 5.0 mg after just 2 weeks instead of 4. But this is provider-specific and not standard practice.
What to expect during the transition
The first 2-4 weeks after switching often involve a temporary reduction in appetite suppression. You were on a therapeutic dose of semaglutide, and now you are on a sub-therapeutic starting dose of tirzepatide. This gap is normal.
Most people report appetite suppression returning by week 2-3 on tirzepatide, even at the 2.5 mg dose, because the GIP receptor activation adds effects that semaglutide alone could not provide. By the time you reach 5.0 mg tirzepatide (typically week 5), most people feel at least as much appetite control as they had on their previous semaglutide dose.
Nausea during the switch is possible but generally milder than when you first started semaglutide. Your GLP-1 receptors are already adapted. The new sensation comes from GIP receptor activation, which tends to produce less gastrointestinal distress than GLP-1 stimulation alone.
One practical consideration that catches people off guard: the storage requirements for tirzepatide may differ from what you are used to with semaglutide. Compounded tirzepatide typically needs refrigeration and has a different stability window than compounded semaglutide. Check your specific product before assuming the handling is identical.
Switching from tirzepatide to semaglutide: the reverse protocol
Less common, but it happens. Insurance changes, supply issues, cost concerns, or simply wanting to try the other option. The reverse switch has its own considerations.
Why someone would switch down
Cost is the biggest driver. Compounded tirzepatide often costs more than compounded semaglutide, and brand-name Zepbound can be significantly more expensive than Wegovy depending on insurance coverage. Some people switch after reaching their goal weight, reasoning that semaglutide may be sufficient for maintenance even if tirzepatide was needed for initial loss.
The protocol mirrors the forward switch but with an important difference: you may not need to start at the lowest semaglutide dose.
Reverse switching protocol
Step 1: Complete your final tirzepatide dose.
Step 2: Wait approximately one week.
Step 3: Start semaglutide at 0.5 mg or 1.0 mg. Because your GLP-1 receptors are already fully adapted from tirzepatide use, most providers skip the 0.25 mg initiation dose. Starting at 0.5 mg is common for patients who were on lower tirzepatide doses (5-7.5 mg), while 1.0 mg is typical for those coming from 10-15 mg tirzepatide.
Step 4: Escalate as tolerated to your target semaglutide dose.
Expect some reduction in appetite control during the switch. You are losing the GIP receptor activation that contributed to tirzepatide's effects. This can feel like a step backward even when the GLP-1 dosing is adequate. The body adjusts over 4-6 weeks, but the overall weight loss effect will likely be less than what tirzepatide provided.
For a complete guide on the reverse transition, see our detailed switching from tirzepatide to semaglutide article.
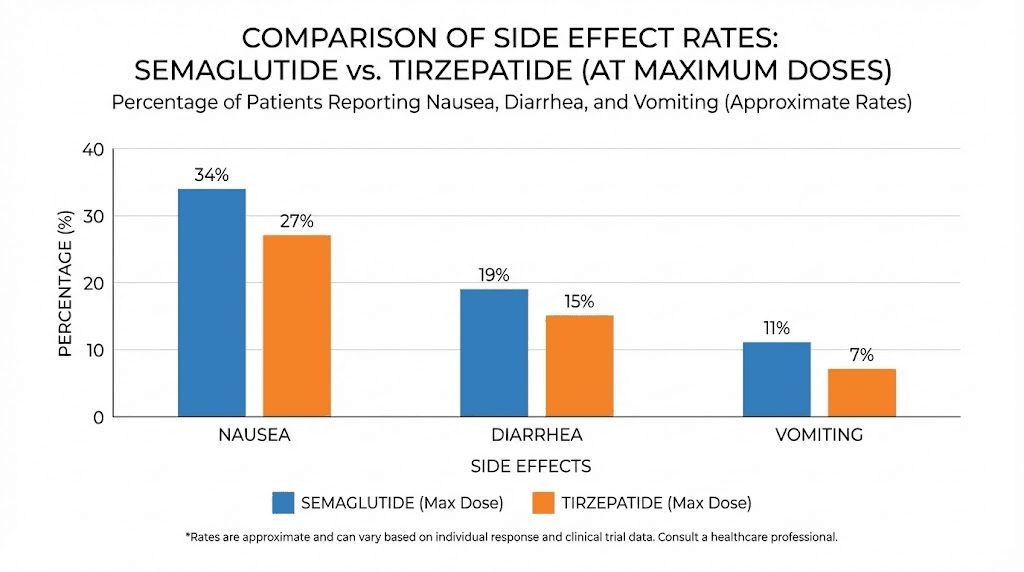
Side effects at each dose level: what the data actually shows
Side effects are dose dependent. Higher doses mean more gastrointestinal symptoms. But the pattern differs between the two medications in ways that matter for dosing decisions.
Semaglutide side effect rates by dose
Side effect | 0.5 mg | 1.0 mg | 2.4 mg |
|---|---|---|---|
Nausea | 16% | 20% | 44% |
Diarrhea | 10% | 15% | 30% |
Vomiting | 5% | 8% | 24% |
Constipation | 6% | 10% | 24% |
Abdominal pain | 6% | 8% | 20% |
The jump in side effects from 1.0 mg to 2.4 mg is dramatic. Nausea more than doubles. This is why the STEP trial protocol includes two intermediate doses (1.7 mg) before reaching 2.4 mg, and why many people find their sweet spot below maximum.
Tirzepatide side effect rates by dose
Side effect | 5 mg | 10 mg | 15 mg |
|---|---|---|---|
Nausea | 24% | 24% | 33% |
Diarrhea | 21% | 16% | 14% |
Vomiting | 6% | 10% | 9% |
Constipation | 12% | 8% | 11% |
Abdominal pain | 6% | 5% | 5% |
Something interesting shows up in the tirzepatide data. Look at the diarrhea row. It actually decreases at higher doses. This is unusual and may reflect the GIP component modulating gut motility at higher concentrations. Nausea increases with dose, as expected, but the slope is gentler than with semaglutide. And vomiting stays relatively flat across all three dose levels.
The SURMOUNT-5 head to head trial confirmed this pattern. Despite producing more weight loss, tirzepatide had lower rates of treatment discontinuation due to gastrointestinal adverse events (2.7% vs 5.6% for semaglutide). This means more people can stay on tirzepatide at effective doses compared to semaglutide, which is a meaningful advantage when the goal is long-term use.
For managing tiredness from tirzepatide or semaglutide side effects, the most effective strategy is the same for both: slow down your escalation. Staying at a dose for 6-8 weeks instead of the minimum 4 gives your body significantly more time to adapt before the next increase.
Mechanism differences that explain the dosing gap
Understanding why these two medications have such different dose ranges requires looking at what happens at the receptor level. This is not just academic. It directly explains why you cannot convert one dose to the other and why the weight loss numbers differ so significantly.
Semaglutide: single receptor, proven pathway
Semaglutide is a GLP-1 receptor agonist. Period. It mimics the natural GLP-1 hormone your body produces after eating. When it binds to GLP-1 receptors, three things happen.
First, the appetite centers in your brain get a strong "full" signal. This reduces hunger and food cravings, often dramatically.
Second, gastric emptying slows. Food stays in your stomach longer, which maintains the feeling of fullness between meals and can cause the nausea that most users experience during dose escalation.
Third, insulin secretion improves and glucagon release decreases, which stabilizes blood sugar. This is why semaglutide was originally developed for type 2 diabetes before its appetite suppression effects were recognized.
All of these effects are dose dependent. More semaglutide equals more GLP-1 receptor activation equals stronger effects (and more side effects). The dose ceiling of 2.4 mg represents the point where increasing the dose further produces diminishing returns with escalating gastrointestinal problems.
Tirzepatide: dual receptor, amplified effects
Tirzepatide activates both GLP-1 and GIP receptors simultaneously. The GIP component adds mechanisms that semaglutide simply cannot access.
GIP receptor activation improves insulin sensitivity through pathways independent of GLP-1. It affects fat metabolism directly, promoting fat oxidation and reducing fat storage. It also appears to modulate the gastrointestinal side effects of GLP-1 activation, which may explain why tirzepatide is better tolerated despite being more potent.
The dual mechanism means tirzepatide achieves greater biological effects per unit of receptor stimulation. Think of it this way. Semaglutide pushes one lever. Tirzepatide pushes two levers at once. The combined effect is greater than either lever alone, which is why 15 mg of tirzepatide produces weight loss that 2.4 mg of semaglutide cannot match. The milligrams are different because the mechanisms are different.
This also explains why there is no conversion formula. You cannot calculate how much "extra" effect the GIP component adds because it varies by individual. Some people are highly responsive to GIP activation. Others are not. The only way to find the right tirzepatide dose for someone coming from semaglutide is to start low and observe, which is exactly what every switching protocol recommends.
Research into next generation peptides is already exploring triple-agonist compounds like retatrutide, which activates GLP-1, GIP, and glucagon receptors simultaneously. The pattern of increasing receptor targets correlating with greater efficacy (and different dosing profiles) appears to be accelerating.
Compounded vs brand name: how dosing charts differ
The dosing charts we have discussed so far come from FDA clinical trials of branded medications (Wegovy/Ozempic for semaglutide, Zepbound/Mounjaro for tirzepatide). Compounded versions introduce variables that can change how you interpret these charts.
Concentration variability
Brand-name pens deliver a pre-measured dose. You click the pen, inject, done. No math required.
Compounded vials require you to calculate your own dose based on the vial concentration. And here is the problem: concentrations are not standardized across compounding pharmacies.
Common semaglutide concentrations: 1 mg/mL, 2.5 mg/mL, 5 mg/mL
Common tirzepatide concentrations: 5 mg/mL, 10 mg/mL, 15 mg/mL, 20 mg/mL
A 5 mg dose of tirzepatide from a 10 mg/mL vial requires 50 units. The same 5 mg dose from a 20 mg/mL vial requires 25 units. If you switch pharmacies and do not recalculate, you could inadvertently double or halve your dose.
Always verify your concentration. Every time you receive a new vial, even from the same pharmacy. Concentrations can change between batches. Use a reconstitution calculator to eliminate any doubt.
Additional ingredients in compounded formulations
Many compounded formulations include additional ingredients. Semaglutide with B12 is extremely common, as vitamin B12 supplementation helps address potential deficiencies caused by reduced food intake. Tirzepatide with niacinamide is another popular combination, where the niacinamide may support cellular energy metabolism during caloric restriction.
These additions do not change the dosing chart for the base medication. A 2.5 mg tirzepatide dose is still 2.5 mg tirzepatide whether it includes niacinamide or not. But the presence of additional ingredients can affect tolerability. Some people find that B12-enhanced semaglutide causes fewer energy crashes. Others report that niacinamide in tirzepatide reduces the flushing some people experience.
The tirzepatide glycine combination is another formulation gaining attention. Glycine may help with amino acid balance during the significant caloric restriction that comes with these medications. Again, the tirzepatide dosing remains the same, but the additional compound may influence how you feel during escalation.
Microdosing: an alternative dosing approach
Not everyone follows the standard escalation charts. Microdosing tirzepatide has become a popular alternative approach, particularly for people who are sensitive to gastrointestinal side effects or who want to extend their medication supply.
What microdosing looks like
Instead of following the standard 2.5 mg weekly starting dose for tirzepatide, some protocols begin at 1.0 or 1.5 mg weekly. Instead of escalating every 4 weeks, increases happen every 6-8 weeks in smaller increments (1.0-1.5 mg instead of 2.5 mg).
For semaglutide, microdosing might mean starting at 0.1 mg weekly instead of 0.25 mg, or staying at 0.25 mg for 8 weeks instead of 4 before escalating.
The tirzepatide dosing in units article covers the precise unit measurements for these smaller doses when using compounded vials. At a 10 mg/mL concentration, a 1.0 mg microdose of tirzepatide equals just 10 units on the syringe.
Is microdosing effective?
There is limited clinical data specifically on microdosing protocols. The published trials used standard escalation schedules. However, anecdotal reports from clinical practices suggest that many patients achieve meaningful weight loss at doses well below the maximum.
The trade-off is speed. Standard escalation reaches therapeutic doses faster. Microdosing takes longer to get there but may produce fewer side effects along the way. For someone who is not in a rush and prioritizes comfort, this approach has merit. For someone who needs rapid results (perhaps before a surgery or due to obesity-related health complications), standard escalation makes more sense.
SeekPeptides members can access detailed microdosing protocols, including week by week schedules and unit conversion charts for both medications at various concentrations.
Cost per dose comparison
Dosing charts matter for budgeting, not just biology. Higher doses cost more, and the two medications have very different price profiles.
Brand name cost comparison
Factor | Semaglutide (Wegovy) | Tirzepatide (Zepbound) |
|---|---|---|
Manufacturer | Novo Nordisk | Eli Lilly |
Monthly cost (brand, no insurance) | $1,300 - $1,700 | $1,000 - $1,200 |
Monthly cost (brand, with insurance) | $0 - $500 | $0 - $550 |
Dose affects cost? | All doses same price per pen | All doses same price per pen |
With branded pens, every dose level costs the same. A 0.25 mg Wegovy pen costs the same as a 2.4 mg pen per month. Same with Zepbound. This means there is no financial incentive to stay at a lower dose when using brand-name pens.
Compounded cost comparison
Compounded is different. Here, cost scales with dose because you are paying per milligram of active ingredient.
Dose level | Semaglutide cost/month (compounded) | Tirzepatide cost/month (compounded) |
|---|---|---|
Starting dose | $50 - $100 | $75 - $150 |
Mid dose | $100 - $200 | $150 - $300 |
Max dose | $150 - $350 | $250 - $500 |
These ranges vary enormously by pharmacy, location, and whether additional ingredients (B12, glycine, niacinamide) are included. But the pattern is consistent: tirzepatide costs more per month at every dose level because you need more milligrams of the active compound.
This cost difference is one reason some people start with semaglutide. If you respond well to GLP-1 stimulation alone, semaglutide gets you significant weight loss at a lower price point. If you plateau or need more aggressive results, you can switch to tirzepatide knowing the cost will increase.
Use the peptide cost calculator to estimate your specific monthly costs based on dose, concentration, and source. The difference between a 10 mg/mL and 20 mg/mL tirzepatide vial can be substantial, and the calculator accounts for concentration when estimating how long a vial will last at your current dose.
Who should choose which medication (and at what dose)
The dosing chart comparison only matters if you understand which medication fits your situation. Here is a framework based on the clinical evidence.
Semaglutide may be the better starting point if
You have moderate weight loss goals (10-15% of body weight). The semaglutide weight loss timeline is well established and predictable for this range. You are on a tighter budget and using compounded medication. The lower cost per month adds up significantly over 6-12 months of use. You have a history of GLP-1 related side effects and want the more extensively studied medication. Semaglutide has more years of real world data. You are primarily managing blood sugar with weight loss as a secondary goal. Both work for diabetes, but semaglutide (as Ozempic) has more specific diabetes dosing data.
Tirzepatide may be the better choice if
You have aggressive weight loss goals (15-25% of body weight). The tirzepatide clinical data consistently shows superior results in this range. You tried semaglutide and plateaued. The dual mechanism provides an additional pathway that may overcome GLP-1-only resistance. You are sensitive to nausea on semaglutide. Paradoxically, despite greater potency, tirzepatide's GIP component may reduce nausea compared to semaglutide at equivalent effect levels. You want to reach maintenance faster with a potentially lower maintenance dose relative to your peak. Some clinicians find that patients can maintain results on mid-range tirzepatide doses after losing weight at higher doses.
Neither medication is appropriate if
You have a personal or family history of medullary thyroid carcinoma. Both medications carry a black box warning for this. You have a history of pancreatitis. Both can potentially exacerbate this condition. You are currently pregnant or planning pregnancy. Weight loss medications for women require careful timing around reproductive plans.
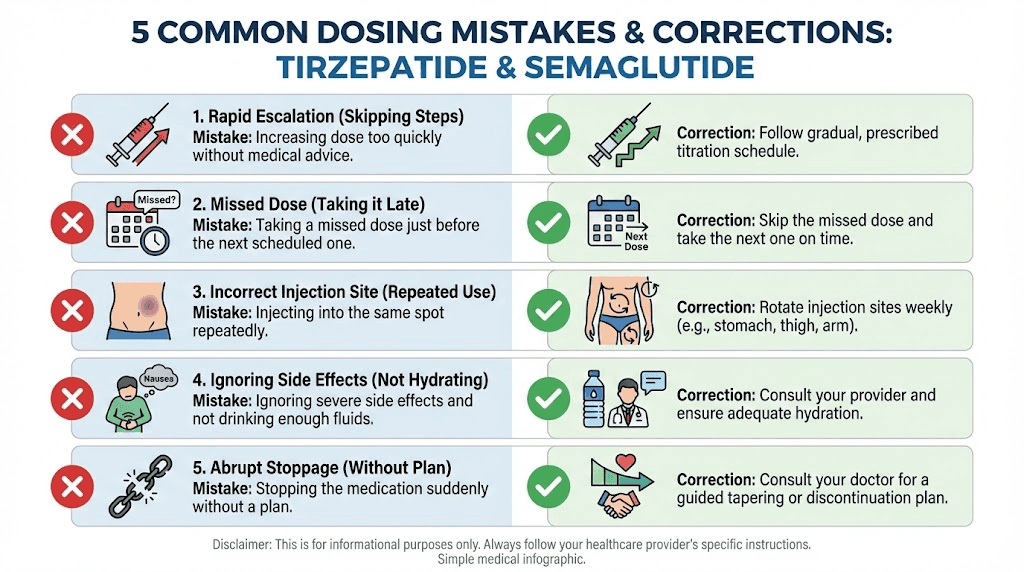
Common dosing mistakes (and how to avoid them)
The complexity of these dosing charts leads to predictable errors. Here are the most common ones, pulled from clinical practice reports and community discussions.
Mistake 1: comparing milligrams directly
Someone sees that their friend is on "only 5 mg tirzepatide" while they are on "2.4 mg semaglutide" and thinks they are on a higher dose. They are not. As we have established, these milligram numbers describe different molecules with different potencies. The only valid comparison is clinical outcome (weight loss, appetite suppression, blood sugar control), not milligram dose.
Mistake 2: escalating too fast
The four-week minimum between dose increases exists for a reason. Your gastrointestinal system needs time to adapt to each new level of receptor stimulation. Escalating every 2 weeks might seem like it will get you to the effective dose faster, but it dramatically increases the risk of severe nausea, vomiting, and diarrhea that could force you to stop entirely.
If you are using compounded medication and managing your own escalation, stick to the minimum four-week intervals. Better yet, wait 6-8 weeks if you are experiencing fatigue or significant GI symptoms at your current dose.
Mistake 3: not verifying compounded concentration
We have covered this but it bears repeating. Different pharmacies use different concentrations. Different batches from the same pharmacy can use different concentrations. Every time you receive a new vial, check the label and recalculate your units. A simple concentration mistake turns a therapeutic dose into a sub-therapeutic one (wasting money and time) or an overdose (risking serious side effects).
Mistake 4: stopping cold turkey at high doses
Both medications produce physiological changes that your body adapts to over months. Stopping a high dose abruptly can cause rebound hunger, rapid weight regain, and blood sugar instability. If you need to discontinue, taper down through the dose levels in reverse, spending 2-4 weeks at each step. The semaglutide withdrawal symptoms guide covers this process in detail.
Mistake 5: assuming the maximum dose is the goal
Not everyone needs 2.4 mg semaglutide or 15 mg tirzepatide. These are ceiling doses, not targets. If you are achieving satisfactory weight loss and appetite control at 1.0 mg semaglutide or 7.5 mg tirzepatide, staying there is perfectly valid. Lower doses mean fewer side effects, lower costs (for compounded), and more room to increase if results plateau later.
The clinical trials tested maximum doses because that is what trials do. Real world practice often finds the optimal individual dose somewhere in the middle range.
Long-term dosing considerations
Both medications are designed for long-term use. The dosing charts we have reviewed cover the escalation phase, but what happens after you reach your target dose matters just as much.
Maintenance dosing with semaglutide
Most clinical practice suggests staying on the maximum tolerated dose indefinitely. The STEP trials showed that weight regain begins within weeks of discontinuation, with participants regaining roughly two-thirds of lost weight within a year of stopping. This means semaglutide, for most people, is a long-term commitment at whatever dose maintains their results.
Some clinicians are experimenting with dose reduction after goal weight is achieved. The theory is that maintaining weight requires less pharmacological support than losing it. A patient who lost weight on 2.4 mg might maintain on 1.0 or 1.7 mg. The evidence for this approach is limited but growing.
Maintenance dosing with tirzepatide
Similar long-term patterns apply. The SURMOUNT-4 trial specifically studied what happens when tirzepatide is stopped after 36 weeks of treatment. Participants who continued tirzepatide kept losing weight. Those switched to placebo regained approximately half their lost weight within 52 weeks.
The dual mechanism may offer a slight advantage for maintenance. Because GIP receptor activation affects fat metabolism through pathways separate from appetite control, there is a theoretical basis for better weight maintenance at lower tirzepatide doses compared to equivalent semaglutide doses. But this theory needs more long-term data to confirm.
For either medication, understanding the full timeline is essential. Peak weight loss typically occurs at 60-72 weeks for both medications. The first few months show the fastest loss, followed by a gradual deceleration as you approach a new metabolic equilibrium.
Tolerance and dose adjustment over time
Some people report decreasing effectiveness at a given dose after 6-12 months. This is not true pharmacological tolerance in the classic sense, but rather the body finding a new equilibrium at the current level of receptor stimulation. When this happens, the options are:
Increase to the next dose tier (if not already at maximum).
Add lifestyle interventions (exercise, dietary changes) to complement the medication.
Switch to the other medication (semaglutide to tirzepatide or vice versa) for a different receptor activation pattern.
Consider combination approaches such as cagrilintide with semaglutide or other peptide stacking strategies.
SeekPeptides provides ongoing protocol adjustment guidance for members navigating these long-term decisions. The initial dosing chart gets you started, but the real complexity emerges when you are months into treatment and need to optimize rather than just escalate.
Special populations and dosing adjustments
The standard dosing charts apply to the general adult population. Several groups require modified approaches.
Type 2 diabetes patients
Both medications are approved for diabetes at different dose ranges than for weight loss. Semaglutide for diabetes (Ozempic) maxes out at 2.0 mg, not 2.4 mg. Tirzepatide for diabetes (Mounjaro) uses the same dose range as for weight loss (up to 15 mg). If you are using these primarily for blood sugar control, the dosing chart for your specific indication may differ from the weight loss charts presented here.
Older adults
No formal dose adjustment is required for age, but clinical practice often suggests slower escalation. Older adults may be more sensitive to gastrointestinal side effects and more vulnerable to the nutritional consequences of significantly reduced food intake. A 6-8 week escalation period between dose increases (instead of 4 weeks) is common in patients over 65.
Renal impairment
Semaglutide does not require dose adjustment for mild to moderate renal impairment. However, the gastrointestinal side effects (vomiting, diarrhea) can cause dehydration that worsens kidney function. Close monitoring is essential. Tirzepatide carries similar considerations.
Hepatic impairment
Neither medication requires dose adjustment for mild to moderate liver impairment. Both have limited data in severe hepatic impairment. Consult a healthcare provider for guidance in these situations.
Women of reproductive age
Both medications should be discontinued at least 2 months before planned pregnancy (semaglutide has a longer half-life and some guidelines suggest 2+ months of washout). The peptides for menopause weight loss and safe peptides for women guides provide additional context for female-specific dosing considerations.
The future of GLP-1 dosing
The dosing landscape is evolving rapidly. Several developments will likely change these charts within the next few years.
Oral formulations
Oral tirzepatide is in advanced clinical trials. The dosing for oral formulations will look completely different from injectable because oral bioavailability is much lower. Expect to see oral doses in the hundreds of milligrams to achieve what injectable doses accomplish in single-digit milligrams. Oral semaglutide (Rybelsus) already exists for diabetes, with daily doses of 3, 7, or 14 mg compared to the weekly injectable range of 0.25-2.4 mg.
The oral vs injectable comparison involves more than just dose conversion. Oral formulations must be taken on an empty stomach, absorbed differently, and may produce different side effect profiles despite delivering the same active compound.
Triple agonists
Retatrutide adds glucagon receptor activation to the GLP-1/GIP combination. Early trial data shows weight loss exceeding 24% at optimal doses, surpassing even tirzepatide. The retatrutide dose schedule follows yet another escalation pattern, and comparing it to tirzepatide or semaglutide requires the same caution about non-equivalent milligrams.
Other compounds in the pipeline include cagrilintide (an amylin analog often combined with semaglutide as CagriSema), mazdutide, and survodutide. Each will bring its own dosing chart with its own escalation schedule and its own non-transferable milligram numbers.
Patch delivery systems
GLP-1 patches like Onmorlo represent another delivery method that will change dosing entirely. Transdermal delivery bypasses the GI tract, which could alter both the effective dose range and the side effect profile. Patch dosing will be measured differently (typically in milligrams per day released through the skin) and will require entirely new comparison frameworks.
Practical dosing tools and calculators
Math errors with these medications can have real consequences. Always use a calculator to verify your doses, especially with compounded formulations.
Semaglutide dosage calculator - Input your vial concentration and target dose. Returns the exact units to draw on your syringe. Accounts for common concentrations including 1 mg/mL, 2.5 mg/mL, and 5 mg/mL.
General peptide calculator - Works for tirzepatide and any other peptide. Enter the vial size, amount of bacteriostatic water added, and desired dose in milligrams. Returns precise units.
Reconstitution calculator - Specifically designed for mixing peptides with bacteriostatic water. Tells you exactly how much water to add to achieve your desired concentration.
Cost calculator - Estimates monthly costs based on your dose, concentration, and vial size. Helps compare the economic reality of different dose levels and different medications.
Stack calculator - For those using multiple peptides simultaneously, this tool helps coordinate dosing schedules and check for timing conflicts.
These tools are free to use. SeekPeptides built them specifically because dosing miscalculations are one of the most common problems reported in the peptide research community. Bookmark them. Use them every time you draw a dose from a compounded vial.
Frequently asked questions
Is 2.5 mg tirzepatide the same as 0.25 mg semaglutide?
No. While both are starting doses designed for gastrointestinal tolerance building, they are not equivalent. Tirzepatide 2.5 mg activates both GLP-1 and GIP receptors, while semaglutide 0.25 mg activates only GLP-1 receptors. The milligram numbers reflect different molecular weights and different receptor binding profiles. The only similarity is that both are sub-therapeutic doses meant to prepare your body for higher amounts.
Can I use my semaglutide dosage chart for tirzepatide?
Absolutely not. The two medications have completely separate dosing schedules, different escalation increments, and different maximum doses. Semaglutide escalates in uneven steps (0.25, 0.5, 1.0, 1.7, 2.4 mg) while tirzepatide increases in uniform 2.5 mg increments (2.5, 5.0, 7.5, 10.0, 12.5, 15.0 mg). Always follow the specific chart for the medication you are actually using.
How many units is 5 mg of tirzepatide?
It depends entirely on your vial concentration. At 10 mg/mL, 5 mg equals 50 units. At 20 mg/mL, 5 mg equals 25 units. The formula is: dose (mg) divided by concentration (mg/mL) multiplied by 100. See our detailed tirzepatide units conversion guide and tirzepatide dosage in units article for complete conversion tables.
What dose of tirzepatide equals 2.4 mg semaglutide?
No universally accepted equivalence exists. Clinical experience suggests that the maximum dose range of semaglutide (2.4 mg) roughly corresponds to the 10-15 mg range of tirzepatide, but individual response varies significantly. The SURMOUNT-5 trial showed that maximum-dose tirzepatide produces about 47% more weight loss than maximum-dose semaglutide, so they are clearly not equivalent at their respective maximums.
Should I start at a higher tirzepatide dose if I was already on semaglutide?
The standard recommendation is to start tirzepatide at 2.5 mg regardless of your previous semaglutide dose. While your GLP-1 receptors are adapted, tirzepatide also activates GIP receptors that semaglutide never engaged. Your body needs time to adjust to this new receptor stimulation. Some providers make exceptions for patients who were on maximum semaglutide, but this is not standard practice.
Why does semaglutide max out at 2.4 mg while tirzepatide goes to 15 mg?
The different maximums reflect different molecular potencies and different receptor mechanisms. Semaglutide is a highly potent GLP-1 receptor agonist, and increasing beyond 2.4 mg produces diminishing returns with increasing side effects. Tirzepatide's dual mechanism allows for a higher dose ceiling because the GIP component modulates the gastrointestinal effects that would otherwise limit dosing. The milligram numbers are not comparable between the two molecules.
How long does it take to reach the maximum dose of each medication?
Semaglutide reaches its maximum of 2.4 mg at approximately week 17 (starting from 0.25 mg with four-week escalation intervals). Tirzepatide reaches its maximum of 15 mg at approximately week 21 (starting from 2.5 mg). Both can take longer if your provider recommends extended time at any dose level due to side effects.
Do I need a different syringe for tirzepatide vs semaglutide?
Standard insulin syringes work for both medications when using compounded vials. The key consideration is syringe size. For lower tirzepatide doses at high concentrations (like 2.5 mg at 20 mg/mL, which equals 12.5 units), a 0.3 mL syringe provides more precise measurement than a 1 mL syringe. For higher doses at lower concentrations (like 15 mg at 10 mg/mL, which equals 150 units), you may need to split into two injections since standard syringes hold a maximum of 100 units. See our peptide injection guide for syringe selection details.
External resources
SURMOUNT-5 Trial: Tirzepatide vs Semaglutide for Obesity (NEJM)
STEP 1 Trial: Semaglutide 2.4 mg for Weight Management (NEJM)
For researchers serious about optimizing their weight management protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based dosing guides, personalized protocol builders, and a community of thousands who have navigated these exact dosing decisions.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay accurate, your escalation stay smooth, and your results stay consistent.