Feb 22, 2026

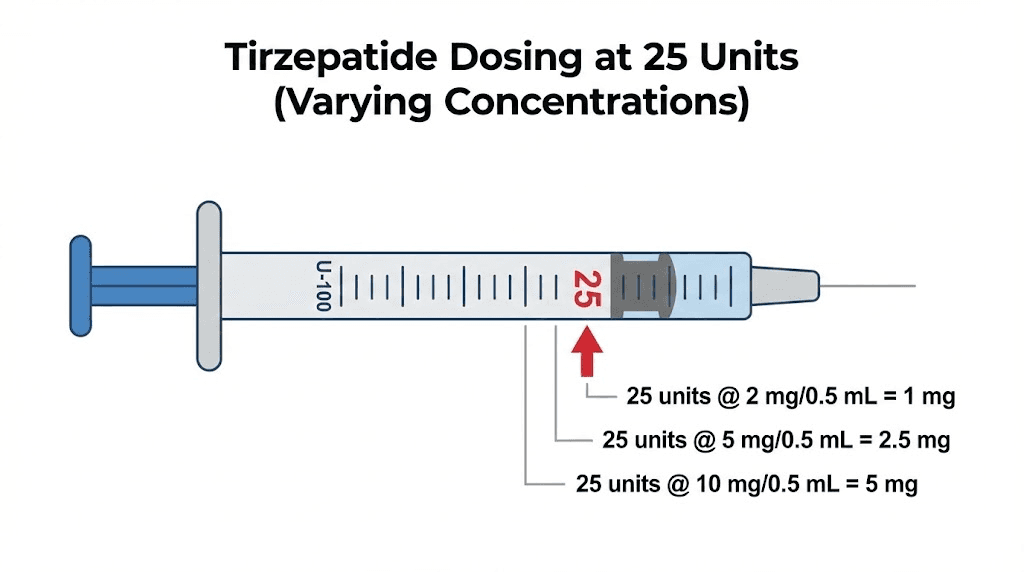
Before you draw up 25 units of tirzepatide, you need to know something critical. That number on your syringe does not tell you how many milligrams you are injecting. It tells you a volume. Nothing more. And depending on the concentration of the liquid inside your vial, 25 units could deliver anywhere from 1.25 mg to 15 mg of tirzepatide. That is the difference between a gentle starting dose and the absolute maximum dose approved for weight loss.
This matters more than most people realize. Drawing 25 units from a 10 mg/mL vial gives you 2.5 mg, which is the standard starting dose for tirzepatide weight loss protocols. Drawing the same 25 units from a 60 mg/mL vial delivers 15 mg, which is the maximum dose that even the most experienced users reach after months of careful escalation. Same syringe reading. Same number of units. Wildly different outcomes.
The confusion exists because compounded tirzepatide comes in dozens of different concentrations. Your vial might be 5 mg/mL, 10 mg/mL, 20 mg/mL, or something else entirely. The concentration determines everything about what those 25 units actually contain. And getting it wrong does not just mean a suboptimal dose. It means a potentially dangerous one.
This guide covers exactly what 25 units of tirzepatide equals at every common concentration, the formula for calculating any dose from any vial, and the mistakes that lead people to inject far more or far less than they intended. Whether you are starting your first compounded tirzepatide protocol or switching pharmacies and adjusting to a new vial concentration, this is the reference you need.
The quick answer: what 25 units of tirzepatide equals in milligrams
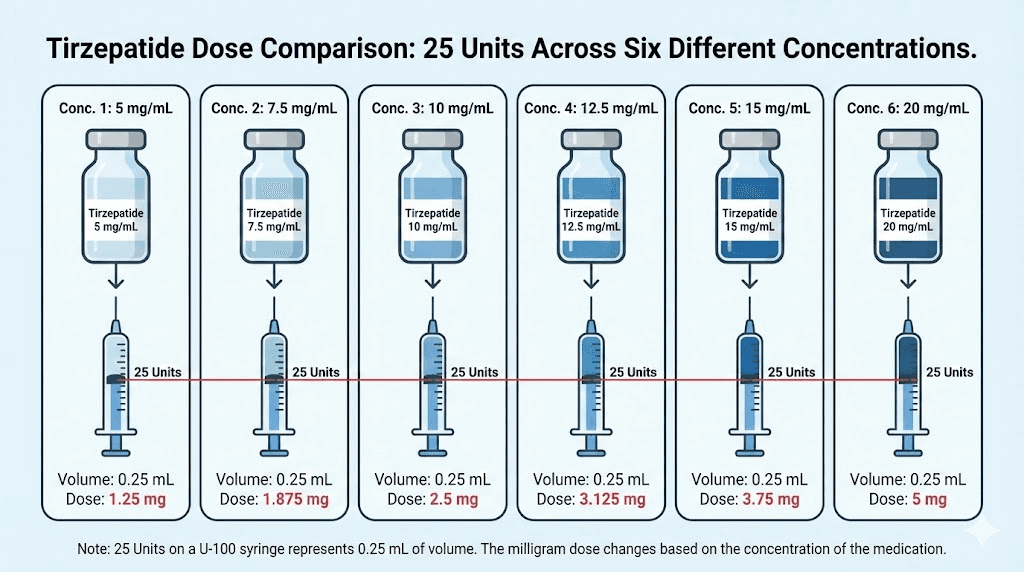
Here is the short version. Twenty-five units on an insulin syringe always means 0.25 mL of liquid. But the milligrams of tirzepatide inside that 0.25 mL depend entirely on the concentration printed on your vial.
Vial concentration | 25 units equals | Standard dose tier |
|---|---|---|
5 mg/mL | 1.25 mg | Below standard starting dose |
10 mg/mL | 2.5 mg | Starting dose |
15 mg/mL | 3.75 mg | Between starting and therapeutic |
20 mg/mL | 5 mg | First therapeutic dose |
30 mg/mL | 7.5 mg | Intermediate dose |
40 mg/mL | 10 mg | Maintenance dose |
50 mg/mL | 12.5 mg | Higher maintenance dose |
60 mg/mL | 15 mg | Maximum dose |
That table tells the entire story. The same 25 units spans every single dose tier that tirzepatide offers, from below the starting dose all the way to the maximum. If you have not checked your vial concentration before drawing 25 units, you are guessing. And guessing with a medication this powerful is not something anyone should do.
For a more detailed breakdown of every unit value across all concentrations, see our complete tirzepatide dosage in units guide and the full tirzepatide dosage chart in units.
Why the concentration on your vial changes everything
Concentration is the single most important number on your tirzepatide vial. It tells you how many milligrams of active medication are dissolved in each milliliter of liquid. And it is the only piece of information that converts the volume on your syringe into an actual dose.
Think of it this way. A 10 mg/mL vial contains 10 milligrams of tirzepatide in every milliliter. A 20 mg/mL vial packs twice as much medication into the same volume. So when you draw 25 units (0.25 mL) from the 10 mg/mL vial, you get 2.5 mg. Draw those same 25 units from the 20 mg/mL vial and you get 5 mg. Double the dose. Same syringe reading.
This is where most dosing errors originate.
Compounding pharmacies produce tirzepatide in a wide range of concentrations. Some use 5 mg/mL for patients who need very precise low-dose adjustments. Others compound at 20 mg/mL or higher to minimize injection volume for patients on higher doses. A few pharmacies even produce concentrations as high as 60 mg/mL, allowing maximum-dose patients to inject just 25 units per week instead of larger volumes.
The concentration typically appears on the vial label as a number followed by mg/mL. It might say "Tirzepatide 10 mg/mL" or "Tirzepatide 20mg/mL" or include additional compounds like tirzepatide with niacinamide at 17 mg/mL. Some labels list it as a total amount per vial, like "40 mg/2 mL" which you would need to divide to get 20 mg/mL. Always confirm the per-milliliter concentration before calculating any dose.
If you are working with a compounded vial and the label seems unclear, contact your pharmacy. Do not guess. The compounded tirzepatide dosage calculator can help verify your numbers, but your pharmacy should always confirm the concentration of your specific vial.
Understanding units versus milligrams versus milliliters
Three different measurements. Three entirely different things. Confusing them is the root cause of nearly every tirzepatide dosing error.
Units: what your syringe measures
Units are volume markings on an insulin syringe. They do not represent potency, strength, or milligrams of any medication. A standard U-100 insulin syringe divides 1 milliliter into 100 equal marks. Each mark is one unit. So 25 units equals exactly 0.25 milliliters, regardless of what liquid fills that syringe.
This is true whether you are drawing tirzepatide, semaglutide, insulin, saline, or water. The syringe does not know or care what is inside it. It only measures volume.
Milligrams: the actual dose
Milligrams measure the weight of the active medication, the tirzepatide itself. When your provider prescribes 2.5 mg or 5 mg or 10 mg of tirzepatide, they are specifying how many milligrams of the drug should enter your body. This is the number that determines your therapeutic effect, your side effect profile, and your position on the dose escalation schedule.
Milligrams are what matter medically. Units are just the tool you use to measure them.
Milliliters: the volume bridge
Milliliters connect units to milligrams. Since 100 units equals 1 milliliter, and concentration tells you milligrams per milliliter, the conversion chain works like this:
Units on syringe (divide by 100) = milliliters of liquid (multiply by concentration) = milligrams of tirzepatide
For 25 units: 25 divided by 100 = 0.25 mL. Then 0.25 mL multiplied by your concentration gives you the milligrams. At 10 mg/mL, that is 0.25 times 10, which equals 2.5 mg. At 20 mg/mL, that is 0.25 times 20, which equals 5 mg.
Understanding this chain prevents errors. If someone tells you to "inject 25 units" without specifying the concentration, they have given you incomplete instructions. The same way telling someone to "drive for 25 minutes" without specifying the speed does not tell them how far they will travel, telling someone to draw 25 units without knowing the concentration does not tell them how much tirzepatide they will receive.
For those working with semaglutide dosage in units, the exact same conversion principle applies. Units are always volume. The concentration always determines the dose.
The universal formula for converting tirzepatide units to milligrams
One formula works for every concentration, every dose, and every syringe size. Memorize it.
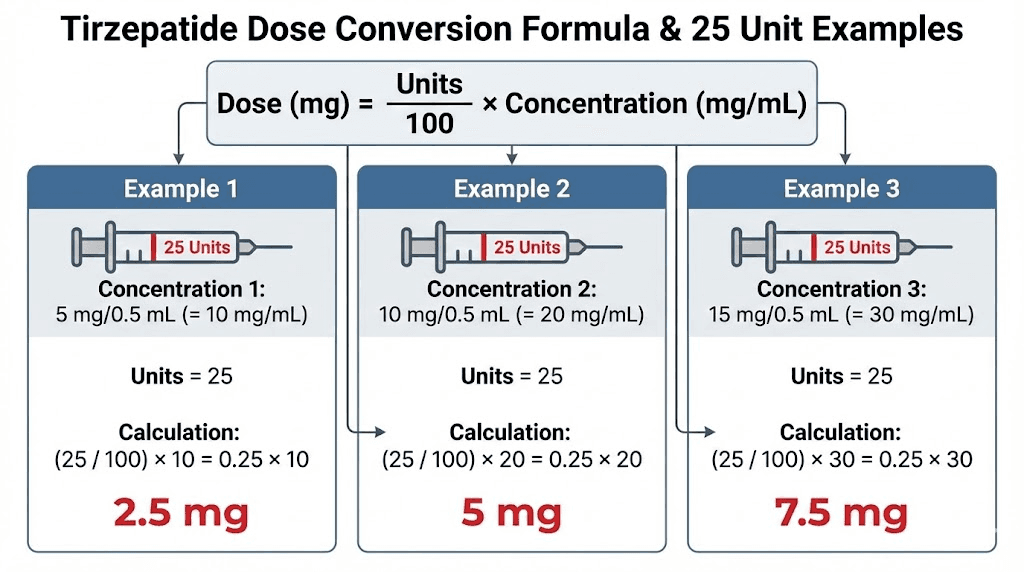
Milligrams = (units divided by 100) multiplied by concentration in mg/mL
That is it. Three numbers. One multiplication. No exceptions.
Worked examples with 25 units
Let us walk through every common concentration to eliminate any ambiguity.
Example 1: 5 mg/mL vial. Milligrams = (25 divided by 100) multiplied by 5. That gives 0.25 multiplied by 5, which equals 1.25 mg. This is below the standard starting dose of 2.5 mg. Some providers use this concentration for very gradual titration or microdosing tirzepatide protocols where precision at low doses matters.
Example 2: 10 mg/mL vial. Milligrams = (25 divided by 100) multiplied by 10. That gives 0.25 multiplied by 10, which equals 2.5 mg. This is the standard starting dose prescribed by most providers during the initial four-week introductory period.
Example 3: 20 mg/mL vial. Milligrams = (25 divided by 100) multiplied by 20. That gives 0.25 multiplied by 20, which equals 5 mg. This matches the first therapeutic dose, the level where most users begin experiencing meaningful appetite suppression and weight loss.
Example 4: 30 mg/mL vial. Milligrams = (25 divided by 100) multiplied by 30. That gives 0.25 multiplied by 30, which equals 7.5 mg. This is an intermediate dose between the 5 mg therapeutic level and the 10 mg maintenance level.
Example 5: 40 mg/mL vial. Milligrams = (25 divided by 100) multiplied by 40. That gives 0.25 multiplied by 40, which equals 10 mg. This represents the maintenance dose where many users find their optimal balance between weight loss results and manageable side effects.
Example 6: 60 mg/mL vial. Milligrams = (25 divided by 100) multiplied by 60. That gives 0.25 multiplied by 60, which equals 15 mg. This is the maximum approved dose. At this concentration, a patient on maximum dose only needs to draw 25 units per injection, minimizing volume and injection site discomfort.
The formula works in reverse too. If your provider prescribes a specific milligram dose and you need to figure out how many units to draw, flip it: Units = (milligrams divided by concentration) multiplied by 100. Our peptide calculator handles both directions instantly if you prefer not to do the math yourself.
Complete conversion tables for every common tirzepatide concentration
Bookmark this section. It covers every concentration you are likely to encounter, with full unit-to-milligram tables that extend well beyond just 25 units. These tables serve as a quick reference for any dose at any concentration.
5 mg/mL vials
This lower concentration appears less frequently but is useful for providers who want maximum precision at low doses. Every unit change shifts the dose by only 0.05 mg, giving very fine control.
Units | mL | Milligrams |
|---|---|---|
10 | 0.10 | 0.50 mg |
15 | 0.15 | 0.75 mg |
20 | 0.20 | 1.00 mg |
25 | 0.25 | 1.25 mg |
30 | 0.30 | 1.50 mg |
40 | 0.40 | 2.00 mg |
50 | 0.50 | 2.50 mg |
75 | 0.75 | 3.75 mg |
100 | 1.00 | 5.00 mg |
At 5 mg/mL, reaching even the starting dose of 2.5 mg requires drawing 50 units. This concentration works well for microdosing protocols where users start below the standard 2.5 mg to minimize gastrointestinal side effects during the adjustment period. If your provider has prescribed 25 units from a 5 mg/mL vial, your dose is 1.25 mg, which is a sub-therapeutic level used specifically for ultra-gradual titration.
10 mg/mL vials
One of the most common concentrations for compounded tirzepatide. This is the concentration where 25 units conveniently equals the standard starting dose.
Units | mL | Milligrams | Dose tier |
|---|---|---|---|
10 | 0.10 | 1.0 mg | Microdose |
15 | 0.15 | 1.5 mg | Microdose |
20 | 0.20 | 2.0 mg | Below starting |
25 | 0.25 | 2.5 mg | Starting dose |
50 | 0.50 | 5.0 mg | First therapeutic |
75 | 0.75 | 7.5 mg | Intermediate |
100 | 1.00 | 10.0 mg | Maintenance |
At 10 mg/mL, 25 units delivers exactly 2.5 mg. This is the most intuitive concentration for beginners because the standard dose tiers align neatly with round unit numbers. The starting dose of 2.5 mg is 25 units, the first therapeutic dose of 5 mg is 50 units, and the 7.5 mg intermediate dose is 75 units. Clean numbers. Hard to make mistakes.
The limitation is volume. A 10 mg maintenance dose requires drawing 100 units, which is the full capacity of a standard 1 mL insulin syringe. Higher doses become impractical because you would need more than one syringe per injection.
20 mg/mL vials
Another common concentration, especially from pharmacies that compound for patients on moderate to higher doses.
Units | mL | Milligrams | Dose tier |
|---|---|---|---|
6.25 | 0.0625 | 1.25 mg | Microdose |
12.5 | 0.125 | 2.5 mg | Starting dose |
25 | 0.25 | 5.0 mg | First therapeutic |
37.5 | 0.375 | 7.5 mg | Intermediate |
50 | 0.50 | 10.0 mg | Maintenance |
62.5 | 0.625 | 12.5 mg | Higher maintenance |
75 | 0.75 | 15.0 mg | Maximum dose |
At 20 mg/mL, 25 units delivers 5 mg. This is the first therapeutic dose where most users experience significant appetite suppression and begin losing weight. If you have been prescribed 25 units from a 20 mg/mL vial, you are past the introductory phase and into the dose range where real results typically begin.
Notice something important about this table. The starting dose of 2.5 mg requires only 12.5 units, which falls between two markings on most insulin syringes. This can make precise measurement more difficult. Many providers who use 20 mg/mL vials start their patients directly at 5 mg (25 units) or use a different concentration for the introductory phase.
30 mg/mL vials
Units | mL | Milligrams | Dose tier |
|---|---|---|---|
8.3 | 0.083 | 2.5 mg | Starting dose |
16.7 | 0.167 | 5.0 mg | First therapeutic |
25 | 0.25 | 7.5 mg | Intermediate |
33.3 | 0.333 | 10.0 mg | Maintenance |
41.7 | 0.417 | 12.5 mg | Higher maintenance |
50 | 0.50 | 15.0 mg | Maximum dose |
At 30 mg/mL, 25 units delivers 7.5 mg. This concentration creates awkward unit numbers for the standard dose tiers because 30 does not divide evenly into 2.5, 5, or 10. The fractional units can introduce measurement imprecision, which is one reason this concentration is less popular than 10 or 20 mg/mL options. However, some pharmacies offer it because it allows maximum-dose patients to use only 50 units per injection.
40 mg/mL vials
Units | mL | Milligrams | Dose tier |
|---|---|---|---|
6.25 | 0.0625 | 2.5 mg | Starting dose |
12.5 | 0.125 | 5.0 mg | First therapeutic |
18.75 | 0.1875 | 7.5 mg | Intermediate |
25 | 0.25 | 10.0 mg | Maintenance |
31.25 | 0.3125 | 12.5 mg | Higher maintenance |
37.5 | 0.375 | 15.0 mg | Maximum dose |
At 40 mg/mL, 25 units delivers 10 mg. This is a maintenance-level dose where many users achieve their best balance of weight loss results with tolerable side effects. The advantage of this concentration is compactness. Even the maximum dose of 15 mg requires only 37.5 units, keeping injection volumes small.
The disadvantage is that lower doses become very small unit values. The starting dose of 2.5 mg is just 6.25 units, which is nearly impossible to measure accurately on a standard syringe. For this reason, 40 mg/mL vials are typically reserved for patients who have already completed dose escalation and are maintaining at 10 mg or above.
60 mg/mL vials
Units | mL | Milligrams | Dose tier |
|---|---|---|---|
4.2 | 0.042 | 2.5 mg | Starting dose |
8.3 | 0.083 | 5.0 mg | First therapeutic |
12.5 | 0.125 | 7.5 mg | Intermediate |
16.7 | 0.167 | 10.0 mg | Maintenance |
20.8 | 0.208 | 12.5 mg | Higher maintenance |
25 | 0.25 | 15.0 mg | Maximum dose |
At 60 mg/mL, 25 units delivers the maximum approved dose of 15 mg. This ultra-concentrated formulation exists specifically for patients who have escalated through all lower dose tiers and want the smallest possible injection volume at their maintenance dose. The convenience is undeniable, but the margin for error is enormous. Drawing even 5 extra units by accident would mean injecting 18 mg, well above the maximum studied dose.
For a comprehensive view of all tirzepatide dose tiers and how they map to clinical outcomes, review the full dosing reference. And always verify your specific concentration with the pharmacy that dispensed your vial, because compounding formulations can vary between providers who offer affordable tirzepatide options.
How 25 units fits into the standard tirzepatide dose escalation schedule
The FDA-approved dose escalation for tirzepatide follows a structured pattern. You start low. You increase slowly. Each step gives the body time to adjust before moving higher.
The standard schedule looks like this:
Weeks 1 through 4: 2.5 mg once weekly (introductory, not considered therapeutic)
Weeks 5 through 8: 5 mg once weekly (first therapeutic dose)
Weeks 9 through 12: 7.5 mg once weekly (intermediate, if tolerated)
Weeks 13 through 16: 10 mg once weekly (maintenance dose)
Weeks 17 through 20: 12.5 mg once weekly (higher maintenance, if needed)
Week 21 onward: 15 mg once weekly (maximum dose)
Where does 25 units fit? It depends entirely on your concentration.
With a 10 mg/mL vial, 25 units is your week 1 through 4 starting dose of 2.5 mg. You are at the very beginning of your journey, letting the medication settle in before any real appetite suppression kicks in. Most users notice subtle changes at best during this phase, and that is perfectly normal. The body needs time to respond. Our guide on how long tirzepatide takes to work explains what to expect at each stage.
With a 20 mg/mL vial, 25 units puts you at 5 mg, the first therapeutic dose. This is where things start happening. Appetite drops noticeably. Cravings diminish. Some users begin losing weight within the first week at this level. If you are drawing 25 units from a 20 mg/mL vial, you are in the active treatment zone.
With a 40 mg/mL vial, 25 units means 10 mg, a full maintenance dose. Users at this level have typically been on tirzepatide for at least 12 to 16 weeks, have worked through the lower doses, and are experiencing significant weight loss. The results at this dose can be quite dramatic, with clinical trials showing average weight loss of 20% or more of body weight at the 10 mg level over 72 weeks.
With a 60 mg/mL vial, 25 units delivers the maximum 15 mg dose. Reaching this level means you have spent at least 20 weeks escalating through every lower tier. It is the ceiling. There is no higher approved dose. And at this concentration, each single unit on your syringe represents 0.6 mg of tirzepatide, making precise measurement absolutely critical.
Knowing where your 25 units falls on this schedule helps you understand what to expect in terms of appetite suppression, weight loss speed, and potential side effects. Lower dose tiers produce milder effects. Higher tiers intensify both benefits and side effects. If you are experiencing stronger effects than expected at 25 units, double-check your concentration. You may be taking more milligrams than you thought.
Common compounded tirzepatide formulations and their 25-unit values
Many compounding pharmacies do not sell plain tirzepatide. They combine it with other compounds intended to enhance effectiveness, reduce side effects, or improve stability. These combination formulations have their own concentrations that you must account for when converting units to milligrams.
Tirzepatide with niacinamide
One of the most common compounded formulations pairs tirzepatide with niacinamide (vitamin B3). Tirzepatide niacinamide compounds typically come in concentrations around 17 mg/mL of tirzepatide with additional niacinamide. At 17 mg/mL, drawing 25 units gives you 0.25 multiplied by 17, which equals 4.25 mg of tirzepatide, plus whatever dose of niacinamide is included.
Some versions of this formulation use 8 mg/mL concentration in larger vials. At that concentration, 25 units would deliver only 2 mg of tirzepatide. Always check both the tirzepatide concentration and the total vial volume when working with combination compounds.
Tirzepatide with glycine
Tirzepatide compounded with glycine is another popular formulation. Glycine is an amino acid that may help with sleep quality and has been shown to reduce certain gastrointestinal side effects. The tirzepatide concentration in these compounds varies by pharmacy, typically ranging from 10 to 20 mg/mL. At 10 mg/mL, 25 units is 2.5 mg of tirzepatide. At 20 mg/mL, it is 5 mg. The glycine dose is separate and typically fixed regardless of how many units you draw.
Tirzepatide with B12
Tirzepatide with B12 compounds add methylcobalamin or cyanocobalamin to support energy levels and prevent the B12 deficiency that can occur with reduced food intake. These formulations are available in various concentrations, with 8 mg/mL being common in combination products. At 8 mg/mL, 25 units delivers 2 mg of tirzepatide, slightly below the standard starting dose.
Tirzepatide with glycine and B12
The triple combination of tirzepatide, glycine, and B12 combines all three ingredients. These typically come in concentrations between 8 and 20 mg/mL for the tirzepatide component. Always read the label carefully to identify the tirzepatide concentration specifically, as the total concentration listed may include all ingredients combined.
With any compound formulation, the rule stays the same. Find the tirzepatide concentration in mg/mL. Multiply it by 0.25 (which represents your 25 units converted to milliliters). That gives you the milligrams of tirzepatide in your injection. The other compounds in the formulation do not change the tirzepatide calculation. They add additional active ingredients at their own fixed concentrations.
If you are considering which compound formulation might work best for your protocol, supplements to take with tirzepatide covers the evidence behind each common addition, including glycine, B12, niacinamide, and more.
Brand name tirzepatide versus compounded: why units matter differently
This entire article applies primarily to compounded tirzepatide from compounding pharmacies. Brand name tirzepatide, sold as Mounjaro for diabetes and Zepbound for weight loss, works very differently in terms of dose measurement.
Pre-filled pens eliminate the conversion problem
Mounjaro and Zepbound come in pre-filled, single-dose injection pens. Each pen contains one specific dose: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, or 15 mg. You do not draw liquid from a vial. You do not use an insulin syringe. You do not calculate units or concentrations. You simply click the pen and inject the full contents. The dose is predetermined at the factory.
This means the question "25 units is how many mg" does not apply to brand name tirzepatide at all. The concept of units is irrelevant when using a pre-filled pen because the volume and concentration are engineered to deliver exactly the labeled dose every time.
When compounded tirzepatide requires unit calculations
Compounded tirzepatide comes in multi-dose vials. You draw your prescribed amount using an insulin syringe, measuring in units. This is where concentration becomes critical and where errors can occur. The appeal of compounded tirzepatide is typically lower cost compared to brand name versions. The trade-off is that you must perform the unit-to-milligram conversion yourself or rely on your provider instructions.
Pharmacies like Empower Pharmacy, Lavender Sky, and others compound tirzepatide at various concentrations. Your provider should specify both the milligram dose and the number of units to draw based on your specific vial concentration. If they only tell you one of these numbers, ask for the other.
For those comparing semaglutide versus tirzepatide, the same principle applies. Brand name semaglutide pens (Ozempic, Wegovy) have pre-set doses, while compounded semaglutide requires unit calculations based on vial concentration.
Dangerous mistakes people make when measuring 25 units
Dosing errors with compounded tirzepatide happen more often than anyone wants to admit. Some are harmless, resulting in a slightly smaller or larger dose than intended. Others are serious.
Mistake 1: assuming all vials have the same concentration
This is the most common and most dangerous error. A user gets comfortable drawing 25 units from a 10 mg/mL vial, which delivers 2.5 mg. Their pharmacy switches them to a 20 mg/mL vial at refill time, sometimes without prominently highlighting the change. The user draws the same 25 units out of habit and receives 5 mg instead of 2.5 mg. Double their intended dose.
At the lower end of the dose scale, this kind of doubling is unpleasant but unlikely to be dangerous. The user might experience more nausea, increased fatigue, or digestive upset. But the same mistake at higher doses could mean injecting 20 or 30 mg when only 10 or 15 mg was intended, well beyond any studied dose and into genuinely risky territory.
Prevention is simple. Check the concentration label on every single vial before every single injection. Even if you have been using the same pharmacy for months. Even if the vial looks identical. Check the label.
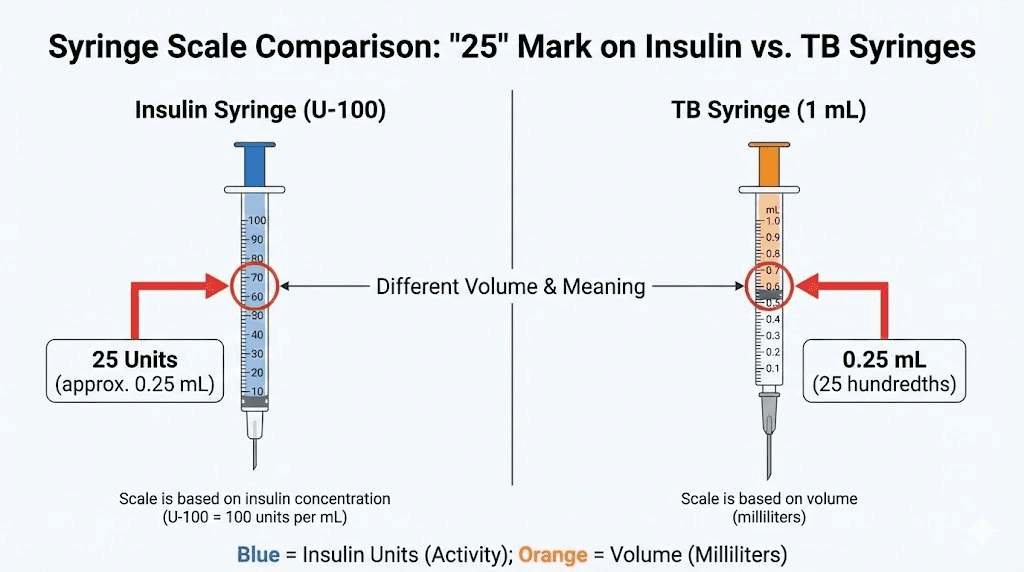
Mistake 2: confusing TB syringes with insulin syringes
Tuberculin (TB) syringes and insulin syringes look similar but measure differently. An insulin syringe marked in units divides 1 mL into 100 units. A TB syringe is marked in milliliters, often with 0.1 mL increments.
Drawing to the "25" mark on an insulin syringe gives you 0.25 mL (25 units). Drawing to a "25" mark on a TB syringe that is graduated differently could give you 0.25 mL or 2.5 mL, depending on the scale. At 2.5 mL from a 10 mg/mL vial, you would inject 25 mg of tirzepatide. That is nearly double the maximum approved dose from a single injection.
Always use a U-100 insulin syringe for compounded peptide injections. The markings are designed for the precision required. See our guide on how to inject GLP-1 medications for detailed syringe selection guidance.
Mistake 3: not accounting for dead space
Insulin syringes have a small amount of dead space in the hub, the area where the needle connects to the barrel. In standard syringes, this dead space can hold 0.05 to 0.1 mL of liquid that never gets injected. For small-volume injections like 25 units (0.25 mL), that dead space represents a significant percentage of the total dose.
Low dead space syringes minimize this issue and are recommended for precise dosing. They cost slightly more but ensure that the 25 units you draw is closer to the 25 units you actually inject.
Mistake 4: switching pharmacies without recalculating
Different compounding pharmacies use different concentrations. Switching from one pharmacy to another while keeping the same unit measurement is a recipe for a dosing error. If Pharmacy A compounded your tirzepatide at 10 mg/mL and you were drawing 50 units for your 5 mg dose, switching to Pharmacy B at 20 mg/mL means you need to draw only 25 units for that same 5 mg. Drawing 50 units from the new vial would give you 10 mg instead.
Whenever you receive a new vial, whether from the same pharmacy or a different one, verify the concentration on the label and recalculate your unit measurement. The compounded tirzepatide dosage calculator makes this verification take seconds rather than minutes of manual math.
How to correctly draw 25 units step by step
Getting the right dose requires the right technique. Here is the process, from vial to injection.
Step 1: verify your vial concentration
Read the label. Find the mg/mL concentration. Do this every time, even if you think you already know. Confirm that this is the same concentration your provider used to calculate your unit dose.
Step 2: choose the right syringe
Use a U-100 insulin syringe. For 25 units, a 0.3 mL (30 unit) or 0.5 mL (50 unit) syringe provides better precision than a full 1 mL (100 unit) syringe because the graduation marks are spaced farther apart on smaller syringes, making it easier to hit exactly 25 units. The needle gauge should be 29 to 31 gauge for subcutaneous injection, which matches the recommendations in our GLP-1 injection site guide.
Step 3: prepare the vial
If your vial has been in the refrigerator, let it warm to room temperature for 10 to 15 minutes. Cold liquid is thicker and harder to draw accurately. Wipe the rubber stopper with an alcohol swab and let it dry completely. For proper storage guidance, see our article on tirzepatide refrigeration requirements and how long tirzepatide lasts in the fridge.
Step 4: draw air into the syringe
Pull the plunger back to the 25-unit mark, filling the syringe with air. Insert the needle through the rubber stopper and push the air into the vial. This equalizes pressure inside the vial and makes drawing liquid easier. Without this step, the vacuum inside the vial can pull the plunger back unpredictably, making precise measurement more difficult.
Step 5: invert the vial and draw to 25 units
With the needle still in the vial, turn the vial upside down so the liquid covers the needle tip. Pull the plunger slowly until the top of the plunger (the flat edge of the rubber stopper inside the barrel) aligns with the 25-unit mark. Draw slowly. Rushing creates bubbles.
Step 6: check for air bubbles
Small air bubbles in the syringe reduce the actual volume of liquid you inject. A few tiny bubbles are not dangerous, but they do mean you are getting slightly less than 25 units of actual medication. Tap the side of the syringe firmly to move bubbles to the top, then push the plunger gently to expel them back into the vial. Re-draw to 25 units if necessary.
Step 7: verify before injecting
Before removing the needle from the vial, double-check that the plunger aligns precisely with 25 units. Once you withdraw the needle, making adjustments becomes messier and wastes medication.
If you are new to reconstituting and preparing tirzepatide, the preparation process before drawing is equally important. Incorrect reconstitution changes the concentration and invalidates every unit calculation.
Other tirzepatide unit conversions you should know
If you are working with 25 units today, there is a good chance your dose will change as you progress through the escalation schedule. Here is a quick reference for the most commonly searched unit values and what they equal at the two most popular concentrations.
Units | At 10 mg/mL | At 20 mg/mL |
|---|---|---|
10 units | 1.0 mg | 2.0 mg |
2.0 mg | 4.0 mg | |
25 units | 2.5 mg | 5.0 mg |
30 units | 3.0 mg | 6.0 mg |
4.0 mg | 8.0 mg | |
5.0 mg | 10.0 mg | |
75 units | 7.5 mg | 15.0 mg |
100 units | 10.0 mg | 20.0 mg |
Each of these conversions follows the same formula. And each carries the same warning: verify your concentration before trusting any of these numbers for your specific vial.
For semaglutide users who work with similar unit-based dosing, the conversion logic is identical but the concentrations and dose schedules differ. See our dedicated guides for semaglutide units to mg conversion, 10 units of semaglutide, 20 units of semaglutide, 40 units of semaglutide, 50 units of semaglutide, and 100 units of semaglutide.
When to adjust from 25 units based on your progress
Your dose does not stay at 25 units forever. Tirzepatide is designed to be escalated over time, with each increase expanding the appetite-suppressing and metabolic effects. Understanding when and why to adjust helps you work with your provider to optimize results.
Signs you may need to increase from 25 units
If you have been on 25 units for 4 or more weeks and appetite suppression has faded significantly, weight loss has stalled for 2 to 3 consecutive weeks, or you are tolerating the current dose with minimal side effects, these are signals that a dose increase may be appropriate. The standard protocol increases by one dose tier every 4 weeks as tolerated, following the schedule outlined by the FDA prescribing information.
However, dose escalation should always be guided by your healthcare provider. Increasing too quickly can trigger severe gastrointestinal side effects including persistent nausea, constipation, and anxiety. The goal is steady progress, not the fastest possible escalation.
Signs you should stay at 25 units
Active weight loss at your current dose is the clearest reason to stay put. If you are losing 1 to 2 pounds per week, the dose is working. There is no benefit to escalating faster when results are already occurring.
Persistent side effects at your current dose also suggest that your body has not fully adapted, and increasing would likely worsen them. Common side effects at early dose tiers include food aversions, sleep disruption, and fatigue. These typically resolve within 2 to 3 weeks at each dose level.
When 25 units stops working
Some users reach a plateau where tirzepatide seems to stop working. Before assuming you need a higher dose, evaluate your diet, exercise, sleep, and stress levels. Sometimes the medication is still doing its job, but other factors are counteracting the weight loss effect. Our guide on why you are not losing weight on tirzepatide covers every common cause and fix.
If a genuine plateau persists after addressing lifestyle factors, a dose increase is the standard next step. Work with your provider to determine whether to increase your unit count at the same concentration or switch to a higher concentration vial, which changes the milligrams per unit.
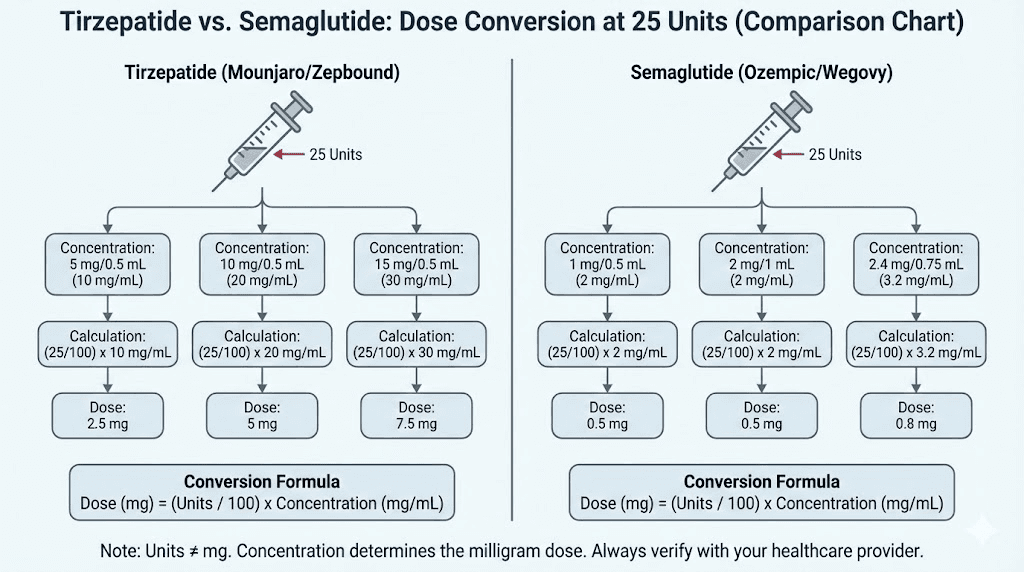
Comparing tirzepatide and semaglutide unit conversions
Many people switch between tirzepatide and semaglutide at some point during their weight loss journey, or consider one versus the other. The unit conversion process is identical for both medications, but the concentrations, dose schedules, and clinical effects differ substantially.
Key differences in conversion
Semaglutide is typically compounded at 5 mg/mL, though concentrations up to 10 mg/mL exist. Tirzepatide concentrations range much wider, from 5 to 60 mg/mL. This means that 25 units of semaglutide at 5 mg/mL delivers 1.25 mg, which is above the 0.25 mg starting dose and below the 2.4 mg maximum dose for semaglutide.
Meanwhile, 25 units of tirzepatide can represent any dose from 1.25 mg to 15 mg depending on concentration. The math is the same. The numbers are different.
Dose schedule differences
Semaglutide starts at 0.25 mg and escalates to a maximum of 2.4 mg (for weight loss). Tirzepatide starts at 2.5 mg and escalates to 15 mg. The milligram numbers are not directly comparable because the medications have different potencies and mechanisms. Tirzepatide activates both GLP-1 and GIP receptors, while semaglutide activates only GLP-1. More milligrams of tirzepatide does not mean more medication than fewer milligrams of semaglutide.
For users considering a switch, the semaglutide to tirzepatide conversion chart provides equivalent dose recommendations. And for a broader comparison of how the two medications stack up, see the tirzepatide versus semaglutide dosage chart and the side effect comparison.
The semaglutide dosage chart in units and semaglutide 5 mg/mL dosage chart provide the same type of conversion tables shown above but for semaglutide-specific concentrations.
Storing your tirzepatide vial properly to maintain accurate dosing
Concentration assumes that the tirzepatide in your vial has not degraded. Improper storage can reduce the potency of the medication, meaning that even if your math is perfect, the actual milligrams you inject may be lower than calculated.
Compounded tirzepatide should be stored in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Exposure to high temperatures, direct sunlight, or freezing can degrade the peptide and reduce its effectiveness. If your vial has been left out of the fridge for an extended period, the concentration on the label may no longer reflect the actual potency of the remaining liquid.
Check the expiration date on your tirzepatide as well. Compounded medications typically have shorter shelf lives than brand name versions, often 90 days from compounding. Using an expired or degraded vial means your 25 units might deliver the right volume but less than the expected milligrams of active tirzepatide.
For long-term storage considerations and how to know if your vial is still good, our tirzepatide refrigerator storage guide covers everything from first opening to the final draw.
Alternative forms of tirzepatide that bypass unit calculations entirely
Not everyone wants to deal with vials, syringes, and unit calculations. Several alternative forms of tirzepatide exist or are in development that eliminate the conversion problem altogether.
Oral tirzepatide is in late-stage clinical trials and would be taken as a pill with a predetermined dose, removing the need for injections and unit calculations entirely. Early results have been promising, and the oral versus injection comparison is generating significant interest among patients who prefer pills to needles.
Tirzepatide tablets represent another avenue, and sublingual tirzepatide drops are also available from some compounding pharmacies. These alternative delivery methods each have their own dosing considerations, but none require the unit-to-milligram conversion that makes injectable compounded tirzepatide confusing.
For now, the majority of compounded tirzepatide users rely on injectable formulations. And for those users, understanding the conversion between units and milligrams is not optional. It is essential.
Using SeekPeptides tools to verify your dose
The math behind tirzepatide dose conversion is straightforward once you understand it, but mistakes happen when you are tired, distracted, or rushing. That is why having a reliable verification tool matters. SeekPeptides provides free peptide calculators that handle the conversion instantly, and members access detailed dosing protocol guides with concentration-specific tables for every major compounding pharmacy formulation.
The advantage of using a calculator rather than doing mental math is error prevention. Entering your concentration and desired dose gives you the exact unit measurement in seconds. No rounding errors. No misplaced decimal points. No accidentally doubling your dose because you forgot your pharmacy changed concentrations.
For researchers serious about getting their protocols right, SeekPeptides members also access the semaglutide dosage calculator, peptide cost calculator, and reconstitution calculator alongside comprehensive dosing guides, side effect management protocols, and a community of experienced users who have navigated these exact questions. From understanding what to eat on tirzepatide to managing GLP-1 related fatigue, the platform covers every aspect of the peptide experience.
Frequently asked questions
Is 25 units of tirzepatide the same as 2.5 mg?
Only if your vial concentration is 10 mg/mL. At that specific concentration, 25 units (0.25 mL) multiplied by 10 mg/mL equals 2.5 mg. At any other concentration, 25 units delivers a different milligram amount. Always check the concentration on your compounded tirzepatide vial before assuming 25 units equals any specific milligram dose.
How do I know what concentration my tirzepatide vial is?
The concentration is printed on the vial label, typically expressed as a number followed by mg/mL (for example, 10 mg/mL or 20 mg/mL). If the label shows a total amount like 40 mg in 2 mL, divide the total milligrams by the total volume to get the concentration (40 divided by 2 equals 20 mg/mL). Contact your pharmacy if the labeling is unclear.
What happens if I accidentally inject 25 units from the wrong concentration vial?
The effect depends on how much the actual dose differs from your intended dose. Injecting more than intended typically intensifies gastrointestinal side effects like nausea and constipation. Injecting less means reduced appetite suppression and weight loss effect. If you realize you used the wrong concentration, contact your healthcare provider for guidance on whether to adjust your next scheduled dose.
Can I use any syringe to draw 25 units of tirzepatide?
Use only U-100 insulin syringes for compounded tirzepatide. TB syringes, standard medical syringes, and other types have different measurement scales that can lead to catastrophic dosing errors. A 0.3 mL or 0.5 mL U-100 insulin syringe provides the best precision for drawing 25 units. See our GLP-1 injection guide for detailed syringe recommendations.
Is 25 units a good starting dose for tirzepatide?
That depends on your concentration. At 10 mg/mL, 25 units delivers the recommended 2.5 mg starting dose, which is appropriate for most new users. At higher concentrations, 25 units delivers more than the starting dose and should not be used initially unless specifically directed by your provider. Your tirzepatide dosing protocol should always match the FDA-recommended escalation schedule.
How many units should I draw for other tirzepatide doses?
The number of units varies by concentration. For example, at 10 mg/mL: 2.5 mg requires 25 units, 5 mg requires 50 units, and 7.5 mg requires 75 units. At 20 mg/mL, those same doses require only 12.5, 25, and 37.5 units respectively. The full tirzepatide dosage chart covers every combination.
Why does my pharmacy use a different concentration than my previous one?
Compounding pharmacies choose concentrations based on their formulation processes, available equipment, and patient population. Some standardize on 10 mg/mL for simplicity. Others use 20 mg/mL to reduce injection volumes. There is no single standard concentration for compounded tirzepatide, which is why verifying the concentration on every new vial is so important.
Does the tirzepatide concentration affect how fast it works?
No. The concentration only determines how much medication is in a given volume. A 2.5 mg dose from a 10 mg/mL vial (25 units) works identically to a 2.5 mg dose from a 20 mg/mL vial (12.5 units). The milligrams of tirzepatide entering your body are the same. The timeline for tirzepatide to start working depends on the milligram dose, not the volume or concentration of the injection.
External resources
For researchers serious about optimizing their tirzepatide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based dosing guides, free calculators, and a community of thousands who have navigated these exact conversion questions.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your syringes stay precise, and your results stay consistent.