Feb 25, 2026
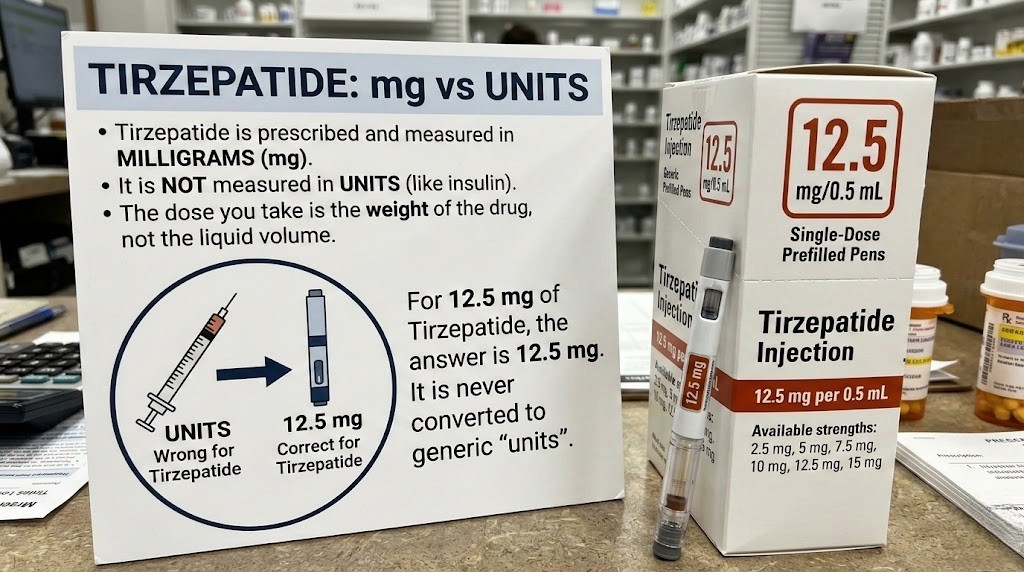
You are drawing the wrong number of units. Right now. And the worst part is, you do not even know it. Every week, people pull up their tirzepatide syringe, draw to a line they found on some chart, and inject a dose that could be half of what they need or dangerously more than they intended. The variable that changes everything sits right there on the vial label, and most people ignore it completely.
That variable is concentration. Measured in milligrams per milliliter, it determines how many units you need to draw on your insulin syringe to get exactly 12.5 mg of tirzepatide. Get the concentration wrong, and every unit marking on your syringe becomes meaningless. Get it right, and dosing becomes simple math that takes about ten seconds.
This guide exists because the question itself, how many units is 12.5 mg of tirzepatide, does not have one answer. It has seven. Maybe more. The number of units changes based on whether your vial is compounded at 5 mg/mL, 10 mg/mL, 15 mg/mL, 20 mg/mL, 30 mg/mL, 40 mg/mL, or 60 mg/mL. Each concentration requires a completely different number of units on your syringe. And each one is equally common depending on where you source your tirzepatide. SeekPeptides members regularly ask about these conversions, which is exactly why this guide covers every single scenario you might encounter. By the time you finish reading, you will know the exact number of units for your specific vial, the formula to calculate any future dose, and the step-by-step process for drawing it accurately every single time.
The quick answer for 12.5 mg of tirzepatide
Here is what you came for. The number of units you draw depends entirely on the concentration printed on your vial.
Vial concentration | Units to draw | Volume in mL | Syringe type needed |
|---|---|---|---|
5 mg/mL | 250 units | 2.50 mL | 3 mL syringe (too large for insulin syringe) |
8 mg/mL | 156 units | 1.56 mL | 3 mL syringe or split into two draws |
10 mg/mL | 125 units | 1.25 mL | 3 mL syringe or split into two draws |
15 mg/mL | 83 units | 0.83 mL | 1 mL insulin syringe |
20 mg/mL | 63 units | 0.63 mL | 1 mL insulin syringe |
30 mg/mL | 42 units | 0.42 mL | 1 mL or 0.5 mL insulin syringe |
40 mg/mL | 31 units | 0.31 mL | 0.5 mL insulin syringe |
60 mg/mL | 21 units | 0.21 mL | 0.3 mL or 0.5 mL insulin syringe |
That is the reference table. Bookmark it. Screenshot it. Print it and tape it to your fridge. But do not stop here, because understanding why these numbers differ, and how to verify them yourself, matters more than memorizing a chart. If your pharmacy changes your concentration or you switch providers, you need the formula, not just the table.
For a broader look at all tirzepatide dose levels converted to units, see the complete tirzepatide dosage in units guide. If you are working with a different dose entirely, the tirzepatide dosing for weight loss in units guide covers the full range from 2.5 mg through 15 mg.
Why concentration changes everything about your unit count
Here is the concept that trips people up. Units on an insulin syringe do not measure milligrams. They measure volume. Specifically, on a standard U-100 insulin syringe, 100 units equals exactly 1 milliliter of liquid. That is all. The syringe has no idea what is dissolved in that liquid. It does not know if you have tirzepatide, semaglutide, insulin, or saline in there. It simply measures how much liquid you are pulling into the barrel.
This is where concentration enters the equation. If your vial contains 10 mg of tirzepatide dissolved in every milliliter, then drawing 1 mL (100 units) gives you 10 mg. But if your vial contains 20 mg per milliliter, that same 100 units now delivers 20 mg. Twice the dose. From the exact same line on the syringe.
Think of it like coffee. A weak brew might have one scoop per cup. A strong brew might have three scoops per cup. Both cups hold the same volume of liquid, but the strength is completely different. Your tirzepatide works the same way. The volume you draw stays constant for a given unit marking, but the amount of active medication in that volume changes based on how concentrated the solution is.
Compounding pharmacies produce tirzepatide at various concentrations. Some use 10 mg/mL because it makes the math simple. Others use 20 mg/mL or even 60 mg/mL to reduce injection volumes at higher doses. Neither approach is better or worse, they just require different unit calculations. If you have been following a tirzepatide compound dosing chart, make sure the chart matches your specific vial concentration. A chart built for 10 mg/mL will give you dangerously wrong numbers if your vial is 20 mg/mL.
The tirzepatide conversion chart breaks this down across all dose levels. For now, understand this single principle: always check your vial label before drawing any dose. The concentration printed there determines everything.
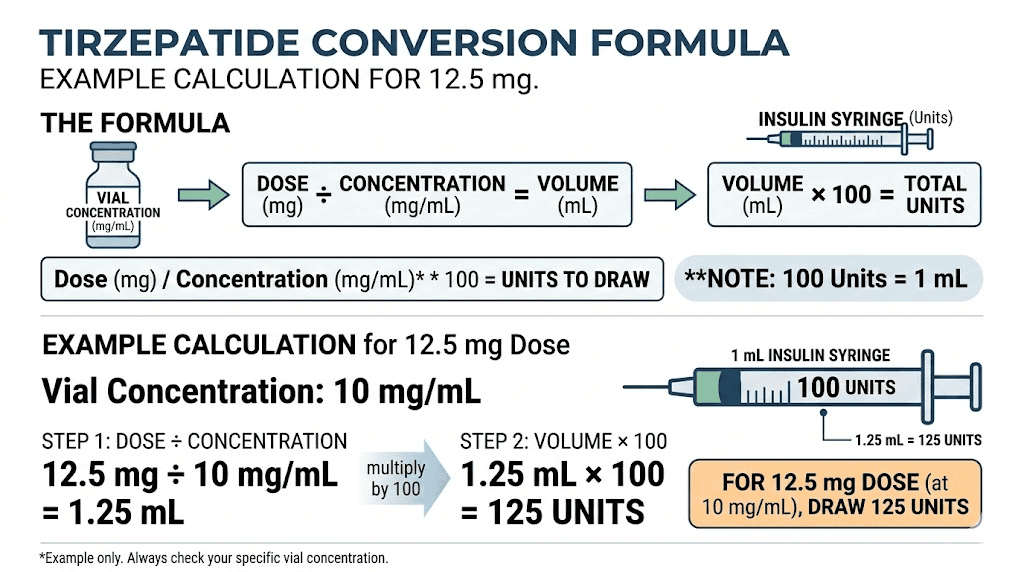
The universal conversion formula you need to memorize
Every tirzepatide unit conversion, at every dose level and every concentration, uses the same formula. Learn it once and you will never need a chart again.
Units = (Desired dose in mg / Concentration in mg per mL) x 100
That is it. Three numbers. One division. One multiplication. Done.
Let us walk through the math for 12.5 mg at the most common concentration of 10 mg/mL:
Step 1: Divide your desired dose by the concentration. 12.5 mg divided by 10 mg/mL equals 1.25 mL.
Step 2: Multiply by 100 to convert milliliters to units. 1.25 mL times 100 equals 125 units.
Now try it with 20 mg/mL:
Step 1: 12.5 mg divided by 20 mg/mL equals 0.625 mL.
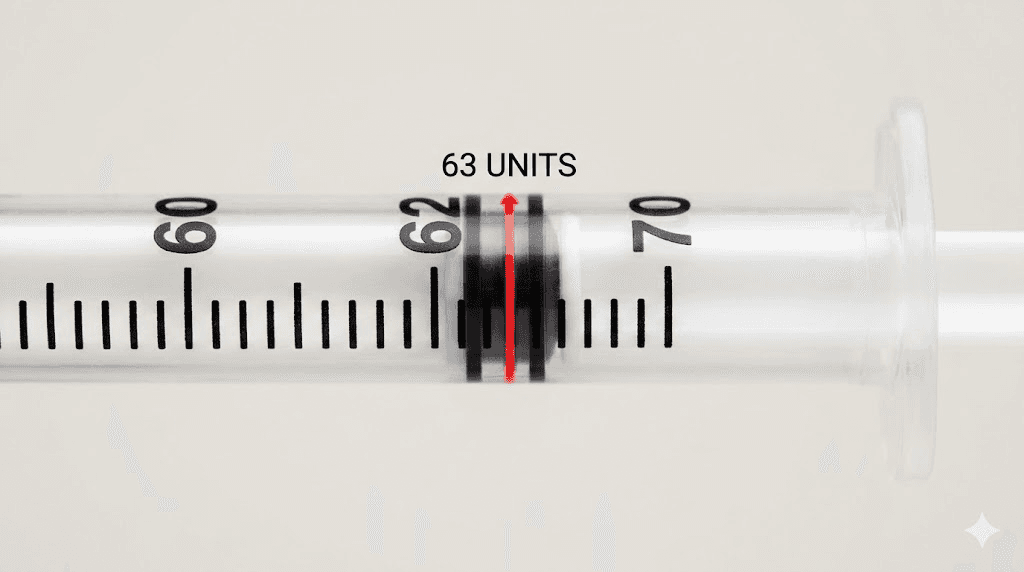
Step 2: 0.625 mL times 100 equals 62.5 units. Round to 63 units.
And with 60 mg/mL:
Step 1: 12.5 mg divided by 60 mg/mL equals 0.2083 mL.
Step 2: 0.2083 mL times 100 equals 20.83 units. Round to 21 units.
The formula works for any dose and any concentration. If your provider changes you to 7.5 mg or bumps you to 15 mg, the same formula applies. You can also use the compounded tirzepatide dosage calculator to verify your math, or the peptide calculator for a quick cross-check. But knowing the formula yourself means you never depend on a website being available when you are standing at your counter with a syringe in hand.
For general peptide dosage math that applies beyond tirzepatide, the how to calculate peptide dosages guide covers the universal approach that works for any injectable.
Complete breakdown by concentration: every scenario for 12.5 mg
Below is a detailed breakdown of what 12.5 mg looks like at each common compounding concentration. Each section includes the exact math, syringe recommendations, and practical notes you need.
12.5 mg at 5 mg/mL concentration
Units to draw: 250 units (2.5 mL)
This is the lowest concentration you will typically encounter, and it creates a problem. A standard 1 mL insulin syringe maxes out at 100 units. You need 250. That means you cannot use an insulin syringe at all for this concentration at the 12.5 mg dose level.
Your options here are limited. You can use a 3 mL standard syringe with a separate needle, which gives you enough volume but sacrifices the precision of an insulin syringe. Or you can split the dose into three separate insulin syringe draws, though this introduces more opportunities for error and requires multiple injection sites.
Most people at the 12.5 mg dose level should not be using 5 mg/mL vials. This concentration works well for starting doses of compounded tirzepatide at 2.5 mg (50 units) or 5 mg (100 units), but it becomes impractical for higher doses. If your pharmacy sends you a 5 mg/mL vial and your dose is 12.5 mg, ask about higher concentration options.
12.5 mg at 8 mg/mL concentration
Units to draw: 156 units (1.56 mL)
The 8 mg/mL concentration sometimes shows up with combination vials that include tirzepatide and niacinamide. At 156 units for a 12.5 mg dose, you still exceed the capacity of a standard insulin syringe. A 3 mL syringe or a split-dose approach would be necessary.
This concentration is not as common as 10 or 20 mg/mL, but if you encounter it, the math follows the same formula. Divide 12.5 by 8 to get 1.5625 mL, then multiply by 100 for 156.25 units. Round down to 156.
12.5 mg at 10 mg/mL concentration
Units to draw: 125 units (1.25 mL)
The 10 mg/mL concentration is one of the most common options from compounding pharmacies. The math is clean and straightforward. Unfortunately, 125 units still exceeds the 100-unit capacity of a standard insulin syringe.
Here is how most people handle it. They draw 100 units into one insulin syringe and 25 units into a second syringe, injecting both. Alternatively, a 3 mL syringe with a fine gauge needle works as a single draw. Some pharmacies offer 30 mg vials reconstituted with 3 mL of bacteriostatic water to achieve this 10 mg/mL concentration. See the how to reconstitute tirzepatide guide and the reconstituting tirzepatide chart if you are mixing your own vials.
For a complete dosing reference at this concentration, the tirzepatide 10 mg dosage chart covers all dose levels from 2.5 mg through 15 mg at the 10 mg/mL concentration.
12.5 mg at 15 mg/mL concentration
Units to draw: 83 units (0.83 mL)
Now we are in insulin syringe territory. At 83 units, a standard 1 mL (100-unit) insulin syringe handles this dose with room to spare. The math gives you 83.33 repeating, so you round to 83 units. That delivers approximately 12.45 mg, which is close enough to 12.5 mg that the clinical difference is negligible.
The 15 mg/mL concentration offers a sweet spot for the 12.5 mg dose. You get single-syringe convenience without requiring the extremely small volumes that make higher concentrations tricky to measure precisely. If you have the option to choose your concentration and your dose is at or near 12.5 mg, the 15 mg/mL option deserves serious consideration.
12.5 mg at 20 mg/mL concentration
Units to draw: 63 units (0.63 mL)
The 20 mg/mL concentration is extremely popular for people on higher tirzepatide doses. At 63 units for a 12.5 mg dose, you are well within the range of a standard insulin syringe. The exact calculation gives 62.5 units, which you round to 63. That delivers approximately 12.6 mg, a difference of less than 1% from your target dose.
This concentration works beautifully for the entire tirzepatide dosing chart in units range. At the starting dose of 2.5 mg, you would draw just 12.5 units (round to 13). At the maximum dose of 15 mg, you would draw 75 units. Everything fits within a single insulin syringe at every dose level. The tirzepatide 20 mg/mL dosing chart has the full breakdown.
12.5 mg at 30 mg/mL concentration
Units to draw: 42 units (0.42 mL)
Higher concentration vials start making precise measurement more important. At 42 units, each unit marking on your syringe represents about 0.3 mg of tirzepatide. Being off by even two units means being off by about 0.6 mg from your intended dose. That is a small amount in absolute terms, but precision matters when you are titrating for optimal results.
A 0.5 mL insulin syringe (50-unit capacity) with half-unit markings is ideal at this concentration and dose level. The finer markings allow you to draw exactly 42 units without guessing between lines. The tirzepatide 30 mg dosage chart covers all dose levels at this concentration.
12.5 mg at 40 mg/mL concentration
Units to draw: 31 units (0.31 mL)
At 40 mg/mL, the calculation gives you 31.25 units. Round to 31 units, delivering approximately 12.4 mg. This is a small volume, and each unit represents 0.4 mg of tirzepatide. A 0.5 mL insulin syringe with half-unit markings is strongly recommended here to maintain accuracy.
The advantage of high-concentration vials is that injections involve less liquid, which can reduce injection site discomfort. Some people report less injection site reaction with tirzepatide when using smaller volumes. The tradeoff is that measurement errors become more consequential.
12.5 mg at 60 mg/mL concentration
Units to draw: 21 units (0.21 mL)
The highest common concentration requires the smallest draw. At 21 units, each marking represents a full 0.6 mg of tirzepatide. Being off by a single unit means your dose shifts by 0.6 mg in either direction. A 0.3 mL insulin syringe (30-unit capacity) with half-unit markings provides the precision you need here.
The 60 mg/mL concentration works best for people on the maximum 15 mg dose (25 units), where the small injection volume is a clear benefit. At 12.5 mg, it is usable but requires careful measurement. If precision concerns you, a slightly lower concentration might be a better choice. The tirzepatide syringe dosage guide covers syringe selection for every concentration and dose combination.
How to read your vial label correctly
Your vial label contains the one number that makes all of this work. Here is where to find it and what it means.
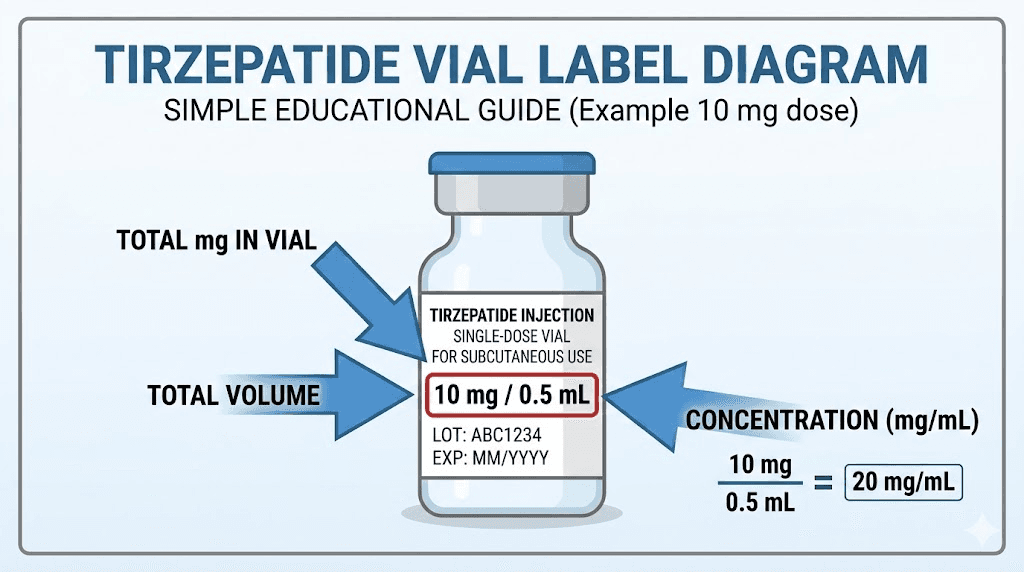
Look for the concentration, which is printed as a number followed by mg/mL. Common examples include 10 mg/mL, 20 mg/mL, or 60 mg/mL. Some labels write it differently. You might see "tirzepatide 200 mg / 10 mL" which means 200 mg total divided by 10 mL of liquid, equaling 20 mg/mL. Others might say "30 mg per 1.5 mL" which equals 20 mg/mL. The key is to get to a single number: how many milligrams are in each milliliter.
If your vial shows only a total amount (like 30 mg) and a total volume (like 3 mL), divide the milligrams by the milliliters. 30 mg divided by 3 mL equals 10 mg/mL. That is your concentration.
Some compounding pharmacies include a tirzepatide dosage chart in units directly on the label or on an accompanying instruction sheet. If yours does, cross-reference it with the formula above to make sure the numbers match. Errors in printed charts happen more often than you would expect.
For vials that contain additional ingredients like tirzepatide with B12 or tirzepatide with glycine, the concentration listed should refer specifically to the tirzepatide content. The added ingredients do not change how you calculate units for the tirzepatide dose. Always confirm this with your pharmacy if the label is ambiguous.
Step by step: drawing 12.5 mg with an insulin syringe
This is the practical section. Follow these steps exactly, every time. Skipping steps leads to dosing errors, contamination, or wasted medication.
Before you start
Gather your supplies. You need your tirzepatide vial, an alcohol swab, and the correct syringe for your concentration. Check the quick reference table above to determine which syringe size works for your vial. Make sure your tirzepatide has been stored properly in the refrigerator and is not expired. If you are unsure about expiration, the does tirzepatide expire guide covers shelf life details. The tirzepatide refrigerator storage article has specific temperature requirements.
Step 1: Calculate your units
Use the formula. Divide 12.5 by your concentration, then multiply by 100. Write the number down. Do not rely on memory when a syringe is in your hand.
Step 2: Clean the vial stopper
Swab the rubber stopper on top of your vial with the alcohol pad. Let it air dry for a few seconds. This prevents bacteria from entering the vial and contaminating the remaining medication.
Step 3: Draw air into the syringe
Pull back the plunger to the same unit marking as your dose. For a 20 mg/mL vial, you would pull air to the 63-unit line. This air goes into the vial to replace the liquid you are about to withdraw, which prevents a vacuum from forming.
Step 4: Inject air into the vial
Insert the needle through the rubber stopper. Push the plunger down to inject the air. Keep the needle in the vial.
Step 5: Invert the vial and draw your dose
Turn the vial upside down so the needle tip is submerged in liquid. Pull the plunger back slowly to your target unit line. Watch for air bubbles. If you see any, tap the syringe barrel gently with your finger to move the bubbles to the top, then push the plunger slightly to expel them. Draw again to your target line.
Step 6: Remove and inject
Pull the needle out of the vial. Choose your injection site following the guidance in our how to inject tirzepatide in the stomach guide. Clean the injection site with a fresh alcohol swab. Insert the needle at a 90-degree angle and push the plunger slowly and steadily. Wait a few seconds after the plunger is fully depressed before removing the needle. For detailed injection technique, the how to inject GLP-1 guide covers best practices.
If you need to split the dose across two syringes (for concentrations where the volume exceeds 1 mL), inject at two different sites. Rotate injection sites weekly to prevent lipodystrophy and reduce injection site reactions.
Choosing the right syringe for 12.5 mg
Not all syringes work for all concentrations. Using the wrong syringe leads to inaccurate doses or physical impossibility of drawing the correct volume. Here is what to use for each scenario at the 12.5 mg dose level.
When to use a 1 mL (100-unit) insulin syringe
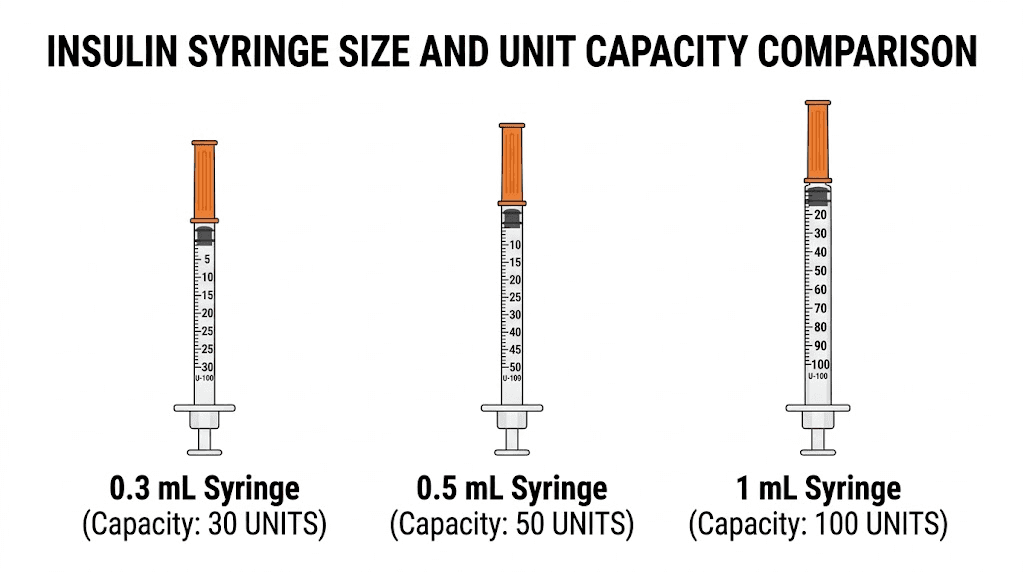
Use a standard 1 mL insulin syringe when your concentration produces a unit count of 100 or less. For 12.5 mg, that means concentrations of 15 mg/mL and above. This syringe type offers good precision for most doses and is widely available at pharmacies. The markings typically show every 2 units, which provides adequate accuracy for tirzepatide dosing.
When to use a 0.5 mL (50-unit) insulin syringe
For concentrations of 30 mg/mL and above, where your 12.5 mg dose requires 42 units or fewer, a 0.5 mL syringe with half-unit markings offers superior precision. Each line on this syringe represents a smaller increment, making it easier to draw exactly the right amount. The tirzepatide dosage chart in mL can help you cross-reference volumes with your syringe capacity.
When to use a 0.3 mL (30-unit) insulin syringe
At the 60 mg/mL concentration, your 12.5 mg dose is only 21 units. A 0.3 mL syringe with half-unit markings gives you the most precise measurement possible. These syringes are commonly used for very small volume injections and are available at most pharmacies, though you may need to ask specifically for them.
When you need a 3 mL syringe
Concentrations of 10 mg/mL and below require more than 1 mL of liquid for a 12.5 mg dose. In these cases, a standard insulin syringe simply cannot hold enough. A 3 mL syringe paired with a 27-gauge or 29-gauge needle provides the necessary volume. The injection technique remains the same, but you will need to purchase syringes and needles separately rather than using the integrated needle of an insulin syringe.
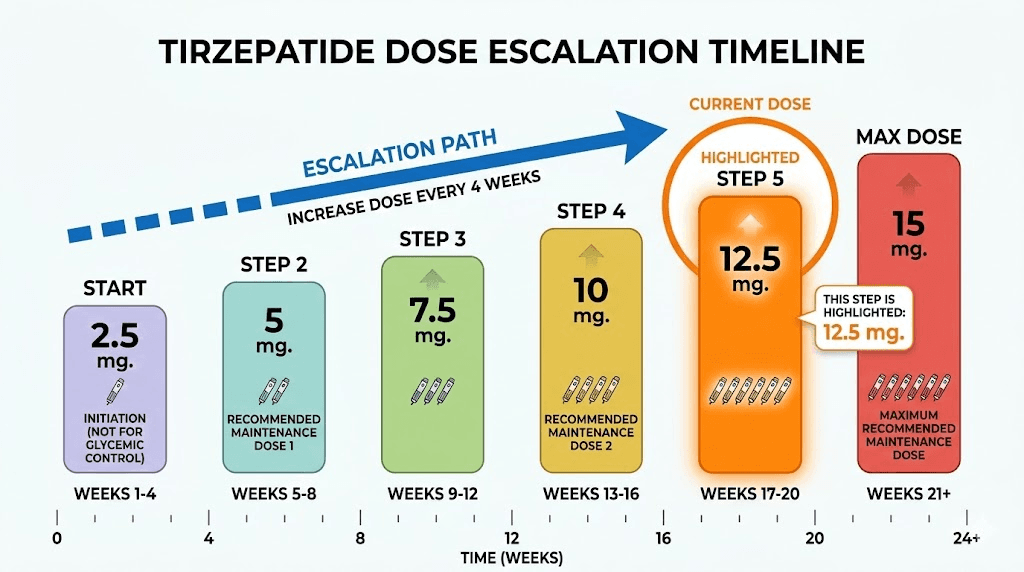
Where 12.5 mg fits in the tirzepatide titration schedule
The 12.5 mg dose is not where anyone starts. It sits near the top of the FDA-approved titration schedule, and reaching it takes time by design.
The standard titration follows this progression, with each step lasting a minimum of four weeks:
Step | Weekly dose | Minimum duration | Cumulative time |
|---|---|---|---|
1 | 2.5 mg | 4 weeks | Weeks 1 through 4 |
2 | 5 mg | 4 weeks | Weeks 5 through 8 |
3 | 7.5 mg | 4 weeks | Weeks 9 through 12 |
4 | 10 mg | 4 weeks | Weeks 13 through 16 |
5 | 12.5 mg | 4 weeks | Weeks 17 through 20 |
6 | 15 mg (maximum) | Ongoing | Week 21 onward |
At a minimum, you are looking at 16 weeks (four months) of titration before reaching 12.5 mg. Some providers extend certain steps to 6 or 8 weeks if side effects require more time to subside, which could push your arrival at 12.5 mg out to 6 months or longer.
This gradual approach exists for a good reason. Tirzepatide activates both GIP and GLP-1 receptors, and the gastrointestinal side effects that come with that dual activation are dose-dependent. Jumping too quickly to higher doses dramatically increases the risk of severe nausea, vomiting, and diarrhea. The compound tirzepatide dosing chart provides a detailed week-by-week schedule, and the conversion chart for tirzepatide dosing for weight loss maps out the complete journey from first injection to maintenance.
For context on how the 2.5 mg starting dose compares in units, or how the 5 mg dose, 7.5 mg dose, 10 mg dose, or 15 mg maximum dose translates to syringe units, each guide covers the conversions for that specific dose level.
What to expect at the 12.5 mg dose level
Reaching 12.5 mg means you have already been on tirzepatide for at least four months. Your body has adapted to the medication through progressive dose increases. But moving from 10 mg to 12.5 mg still represents a meaningful step up, and knowing what to expect helps you manage the transition.
Weight loss at 12.5 mg
The SURMOUNT-1 clinical trial tested tirzepatide at 5 mg, 10 mg, and 15 mg over 72 weeks. While 12.5 mg was not tested as a standalone maintenance dose, we can interpolate from the available data. The 10 mg group lost an average of 21.4% of body weight. The 15 mg group lost 22.5%. That puts 12.5 mg in the range of approximately 21 to 22% total body weight loss over 72 weeks for the average participant.
These numbers represent averages across large populations. Individual results vary significantly based on diet, activity level, starting weight, metabolic health, and adherence to the injection schedule. The tirzepatide weight loss timeline provides a more detailed week-by-week picture of what results look like in practice. For real-world examples, the tirzepatide before and after results and before and after tirzepatide weight loss results show what actual users have experienced. The men before and after tirzepatide article covers male-specific outcomes.
Appetite suppression at 12.5 mg
Most people notice a significant reduction in appetite by the time they reach 12.5 mg. The dual GIP and GLP-1 receptor activation slows gastric emptying, increases satiety signaling, and reduces hunger hormones. Many users report eating less than half of what they consumed before starting treatment.
If your appetite suppression has plateaued or weakened at 10 mg, the jump to 12.5 mg often restores it. This renewed suppression typically kicks in within 1 to 2 weeks of the dose increase. The how long tirzepatide takes to suppress appetite guide covers the timeline in detail. If you are experiencing reduced effectiveness at any dose, the tirzepatide not working anymore article addresses common causes and solutions.
Side effects at 12.5 mg
Side effects tend to increase with each dose escalation and then settle within 2 to 4 weeks as your body adjusts. At the 12.5 mg level, the most commonly reported side effects include:
Gastrointestinal effects: Nausea affects 20 to 33% of users across all dose levels. At 12.5 mg, you are at the higher end of that range during the first few weeks after stepping up. Diarrhea occurs in 18 to 23% of users, while vomiting affects 5 to 12%. These symptoms are usually transient. The tirzepatide constipation treatment and tirzepatide diarrhea duration guides cover management strategies for GI symptoms.
Fatigue: Some users feel more tired during dose transitions. This usually resolves within a week or two. The does tirzepatide make you tired article explores why this happens and what to do about it. Related: GLP-1 fatigue guide.
Headaches: Dose-related headaches affect a smaller percentage of users but can be persistent. The tirzepatide headaches guide and the GLP-1 headache guide cover prevention and treatment.
Injection site reactions: Redness, swelling, or itching at the injection site occurs in some users. Proper injection technique and injection site reaction management can minimize these effects.
Other effects: Some users report body aches, muscle pain, anxiety, or sleep disturbances at higher doses. The semaglutide vs tirzepatide side effects comparison can help if you are weighing your options between medications.
If side effects at 12.5 mg are intolerable, dropping back to 10 mg for an additional 4 to 8 weeks and then trying the increase again is a common and effective strategy. There is no clinical downside to spending extra time at a lower dose.
When to stay at 12.5 mg versus moving to 15 mg
Not everyone needs to reach the maximum 15 mg dose. In fact, many providers and researchers suggest that staying at 12.5 mg is the right choice for a significant number of users. Here is how to think about the decision.
Stay at 12.5 mg if:
You are still losing weight at a consistent rate. If the scale is moving downward and you feel good, there is no reason to increase. The clinical difference between 12.5 mg and 15 mg in terms of weight loss is smaller than the gap between 5 mg and 10 mg. SURMOUNT-1 data shows the 10 mg group lost 21.4% and the 15 mg group lost 22.5%, a difference of roughly 1 percentage point. The incremental benefit of an additional 2.5 mg diminishes at higher doses.
Side effects are manageable but present. If you are experiencing mild nausea or GI symptoms at 12.5 mg that you can live with, increasing to 15 mg will likely worsen those symptoms temporarily. Staying at a tolerable dose and maintaining consistency often produces better long-term outcomes than pushing for the maximum and dealing with severe side effects that reduce adherence.
You have reached a weight that you are satisfied with. If you are at or near your goal weight, 12.5 mg may serve as your maintenance dose indefinitely. The goal of tirzepatide is not to reach the highest possible dose but to find the dose that produces and maintains your desired results.
Move to 15 mg if:
Weight loss has stalled for 4 or more weeks at 12.5 mg despite consistent diet and exercise. A plateau at this dose level indicates that your body may have adapted, and the additional 2.5 mg could restart progress. The why not losing weight on tirzepatide guide covers other potential causes of plateaus that should be ruled out first.
Appetite suppression has weakened significantly. If hunger levels are returning to pre-treatment levels at 12.5 mg, your body is likely developing some tolerance to that dose level. The higher dose can restore appetite control.
Your provider recommends it based on your overall health metrics. Blood sugar management, metabolic markers, and body composition goals may all factor into the decision to increase.
For a complete comparison of the different dose levels, the tirzepatide dosing guide covers the clinical rationale for each tier. If you are curious about how the doses compare when measured on a syringe, the tirzepatide injection dosage chart provides a visual reference.
Common measurement mistakes at the 12.5 mg dose
Measurement errors are more common than most people realize, and at 12.5 mg, some specific pitfalls become more likely. Here are the mistakes that happen most often and how to avoid them.
Mistake 1: Using the wrong concentration in your calculation
This is the most dangerous error. If you switch pharmacies or receive a new vial with a different concentration, your old unit count becomes wrong. Always check the label on every new vial, even if it looks identical to the last one. Some pharmacies change concentrations without prominent notice.
Mistake 2: Confusing units with milliliters on the syringe
Some 3 mL syringes have markings in milliliters rather than units. If you are used to insulin syringe units and switch to a 3 mL syringe, remember that 1 mL equals 100 units. Drawing to the 0.63 mL line on a 3 mL syringe is the same as 63 units on an insulin syringe for a 20 mg/mL vial.
Mistake 3: Not accounting for dead space in the syringe
The hub of the needle and the very bottom of the syringe barrel contain a small amount of liquid that does not get injected. This "dead space" typically holds 0.02 to 0.07 mL, depending on the syringe type. For low-concentration vials where you are drawing larger volumes, this is negligible. But at 60 mg/mL where your entire dose is 21 units (0.21 mL), the dead space represents a meaningful percentage of your dose. Low dead space syringes exist specifically for this purpose.
Mistake 4: Drawing from a vial that has been improperly stored
Tirzepatide that has been left at room temperature too long may have reduced potency, meaning you could be injecting the right volume but getting less active medication than expected. The what happens if tirzepatide gets warm guide covers how temperature affects stability. Always check that your vial has been stored within the proper temperature range.
Mistake 5: Rounding in the wrong direction
When your calculation produces a fraction (like 62.5 units), some people round up and others round down. The general practice is to round to the nearest whole unit. At 62.5, you would round to 63. This delivers approximately 12.6 mg rather than 12.5, a difference that is clinically insignificant. However, consistently rounding up at every dose level and every injection adds small amounts that compound over time. If precision matters to you, alternate between rounding up and rounding down on consecutive injections.
For more on avoiding dosing errors with tirzepatide, the common peptide mistakes beginners make article covers a broader range of errors that apply to all injectables.
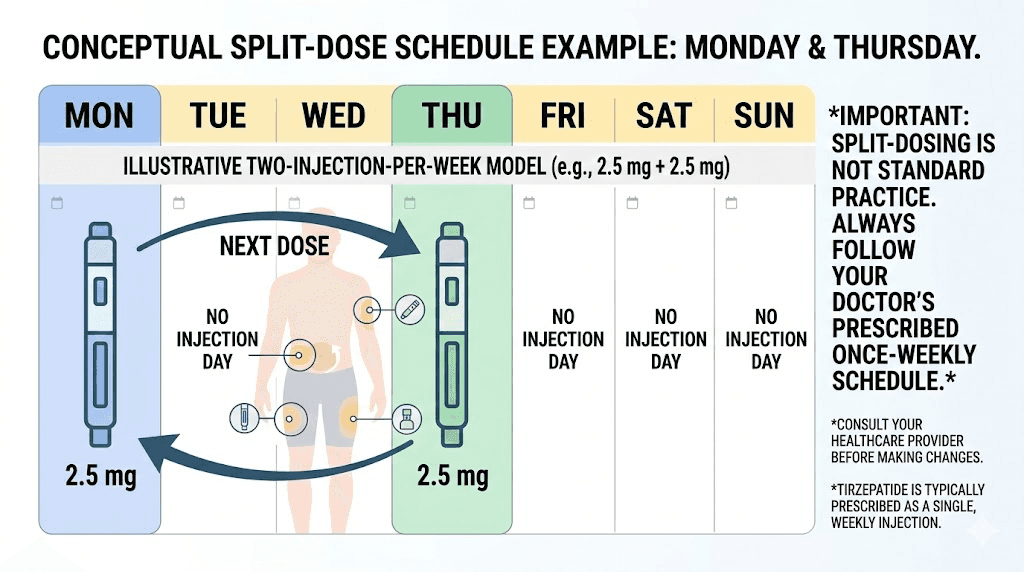
Splitting your 12.5 mg dose: when and how
Some users split their weekly tirzepatide dose into two smaller injections. Instead of a single 12.5 mg injection once per week, they inject 6.25 mg twice per week. This approach has gained popularity for several reasons.
Why people split the dose
The primary reason is side effect management. A single 12.5 mg injection delivers a large bolus of medication that peaks in the bloodstream within 8 to 72 hours. That peak can trigger nausea, vomiting, and other GI symptoms. Splitting the dose creates two smaller peaks, which some users find produces the same overall effect with milder side effects.
The second reason involves more consistent appetite suppression. Some users notice that their appetite returns toward the end of the week before their next injection. Splitting the dose provides more even blood levels throughout the week, maintaining suppression more consistently. The split tirzepatide dose twice a week guide explores this approach in detail.
How to calculate split-dose units
The math is simple. Take your full-dose unit count and divide by two. At 20 mg/mL, your 12.5 mg dose is 63 units. Split in half, each injection would be 31 or 32 units (alternating to average 31.5). At 15 mg/mL, your 83 units would split to 41 and 42 units.
Space the injections 3 to 4 days apart. If you inject on Monday, your second injection would go on Thursday or Friday. Maintaining consistent timing helps stabilize blood levels.
Important considerations
Dose splitting is not FDA-approved protocol. It represents an off-label approach that many providers support but some do not. Always discuss dose splitting with your healthcare provider before implementing it. The pharmacokinetics of tirzepatide, including its roughly 5-day half-life, suggest that splitting could theoretically maintain more consistent drug levels, but formal clinical trials have not confirmed this.
If you are considering microdosing tirzepatide on a schedule, the principles are similar but the doses are smaller. The microdosing tirzepatide chart covers specific protocols for that approach.
How reconstitution affects your unit count
If you receive lyophilized (freeze-dried) tirzepatide rather than a pre-mixed liquid, the concentration of your solution depends entirely on how much bacteriostatic water you add. This gives you direct control over the concentration and, by extension, the number of units you need to draw.
The relationship between water volume and concentration
Take a 30 mg vial of lyophilized tirzepatide as an example. The amount of water you add determines the concentration:
Bacteriostatic water added | Resulting concentration | Units for 12.5 mg |
|---|---|---|
1 mL | 30 mg/mL | 42 units |
1.5 mL | 20 mg/mL | 63 units |
2 mL | 15 mg/mL | 83 units |
3 mL | 10 mg/mL | 125 units |
Less water means higher concentration and fewer units per dose. More water means lower concentration and more units per dose. Neither is inherently better. Choose based on your syringe type and preference for injection volume.
For specific reconstitution instructions, the how to reconstitute tirzepatide guide walks through the entire process step by step. The tirzepatide reconstitution chart and PDF version provide quick reference tables. If you are mixing a 10 mg vial specifically, the how much bacteriostatic water to mix with 10 mg tirzepatide article covers the specifics.
The peptide reconstitution calculator automates this math and shows you exactly what concentration you will get based on the powder amount and water volume you choose.
Why reconstitution precision matters more at 12.5 mg
At lower doses like 2.5 mg, a small variation in water volume creates a minor difference in units. But at 12.5 mg, the same variation translates to a larger absolute difference in units and potentially milligrams. If you add 1.4 mL instead of 1.5 mL to a 30 mg vial, your concentration becomes 21.4 mg/mL instead of 20 mg/mL. For a 12.5 mg dose, that changes your draw from 63 units to 58 units. A 5-unit difference. Using a precise syringe for reconstitution and measuring water carefully reduces this error.
For general guidance on mixing any injectable peptide, the how to reconstitute peptides article covers universal techniques, and bacteriostatic water for peptides explains why this specific water type matters. If you want to understand how much bacteriostatic water to add to peptides generally, that guide covers the principles.
Comparing 12.5 mg unit counts across the tirzepatide dose range
It helps to see where 12.5 mg sits relative to other doses in terms of unit volume. This context is especially useful if you are transitioning from a different dose or planning your next titration step.
Dose | Units at 10 mg/mL | Units at 20 mg/mL | Units at 30 mg/mL | Units at 60 mg/mL |
|---|---|---|---|---|
25 | 13 | 8 | 4 | |
50 | 25 | 17 | 8 | |
75 | 38 | 25 | 13 | |
100 | 50 | 33 | 17 | |
12.5 mg | 125 | 63 | 42 | 21 |
150 | 75 | 50 | 25 |
Notice the pattern. At 10 mg/mL, the unit count exceeds 100 (a full insulin syringe) starting at the 12.5 mg dose. At 20 mg/mL, all doses fit within a single insulin syringe. At 60 mg/mL, even the maximum 15 mg dose requires only 25 units. This makes concentration selection a practical decision, not just a mathematical one.
If you are working with semaglutide instead of (or in addition to) tirzepatide, the conversion math is identical but the dose ranges are different. The semaglutide dosage in units guide and semaglutide units to mg converter cover those calculations. The semaglutide vs tirzepatide comparison explains the broader differences between the two medications.
Optimizing your 12.5 mg protocol beyond just the dose
Getting the unit count right is essential, but it is only one piece of the puzzle. Several factors influence how well your 12.5 mg dose works in practice.
Timing your injection
Consistency matters more than the specific day or time. Pick a day of the week and stick with it. Some users prefer injecting in the evening to sleep through the initial GI effects. Others prefer morning injections. The best time to take a GLP-1 shot guide explores the tradeoffs of different timing strategies.
Nutrition at the 12.5 mg dose
Appetite suppression at this dose level can be significant. Some users struggle to eat enough, which creates its own set of problems including nutrient deficiencies, muscle loss, and metabolic adaptation. Following a structured tirzepatide diet plan or using a tirzepatide meal plan can help ensure you meet minimum caloric and protein requirements. The what to eat on tirzepatide guide covers food choices that are easier to tolerate.
Certain foods may worsen GI side effects at higher doses. The tirzepatide foods to avoid guide lists specific triggers. High-fat and high-sugar meals tend to be the biggest culprits.
Supplements that support higher-dose tirzepatide use
At 12.5 mg, your body processes food more slowly and absorbs nutrients differently. The supplements to take with tirzepatide guide covers the most commonly recommended additions. B12 supplementation is particularly relevant since GLP-1 medications can affect B12 absorption. Many compounding pharmacies offer tirzepatide compounded with B12 specifically for this reason. Others add glycine and B12 to support liver function and nutrient levels simultaneously.
Alcohol and tirzepatide at 12.5 mg
Tirzepatide slows gastric emptying, which changes how your body processes alcohol. Most users find their alcohol tolerance decreases significantly, especially at higher doses. The can you drink on tirzepatide guide covers the specific interactions and practical guidelines.
Understanding the units for other common tirzepatide measurements
The 12.5 mg dose is the one you asked about, but you may encounter other unit-based questions as you manage your protocol. Here is a quick reference for related conversions that come up frequently.
If someone tells you they draw a certain number of units and you want to know the milligram equivalent, the reverse formula applies: milligrams equals units divided by 100 multiplied by the concentration. The 20 units of tirzepatide in mg, 30 units in mg, 40 units in mg, 50 units in mg, and 75 units in mg guides each walk through the specific math for those values. The 25 units of tirzepatide in mg article covers the starting dose equivalent.
These conversions matter because people in online communities often discuss their doses in units without specifying their concentration. Saying "I draw 63 units" means nothing without knowing the concentration. At 10 mg/mL, 63 units is 6.3 mg. At 20 mg/mL, 63 units is 12.6 mg. At 60 mg/mL, 63 units is 37.8 mg. Three completely different doses from the same unit number. Always ask about concentration when comparing notes with others.
Switching providers and what it means for your units
If you change compounding pharmacies or your provider switches you to a different product, your unit count will almost certainly change even though your dose stays at 12.5 mg. This is one of the most common sources of dosing errors.
Before drawing from any new vial, go through the following checklist:
1. Check the concentration. Compare it to your previous vial. If it changed, your unit count changes.
2. Recalculate using the formula. Do not assume anything. Run the math fresh.
3. Verify the syringe works. If you moved from 20 mg/mL to 10 mg/mL, your 63 units just became 125 units, and your insulin syringe can no longer hold the full dose.
4. Check storage instructions. Different pharmacies may have different stability data. The tirzepatide shelf life can vary between products.
If you are considering switching from tirzepatide to semaglutide or vice versa, the dose conversion is not a simple mathematical relationship. The semaglutide to tirzepatide conversion chart and the switching from tirzepatide to semaglutide guide cover the clinical considerations involved.
For cost-related considerations when choosing between providers, the affordable tirzepatide and cheap compounded tirzepatide shots articles compare options. SeekPeptides members get access to provider comparisons and dosing support that makes these transitions smoother.
The relationship between 12.5 mg and other GLP-1 medications
Tirzepatide at 12.5 mg is not directly equivalent to any specific dose of semaglutide or other GLP-1 receptor agonists. The medications have different mechanisms, different potencies, and different pharmacokinetic profiles.
However, for general reference, the tirzepatide vs semaglutide dosage chart provides an approximate comparison of dose levels. In the head-to-head SURMOUNT-5 trial, tirzepatide demonstrated 47% greater weight loss compared to semaglutide at their respective maximum doses. This suggests that tirzepatide 12.5 mg likely produces outcomes similar to or somewhat better than semaglutide at the 2.4 mg maximum dose.
If your provider is considering switching you between medications, the semaglutide to tirzepatide dose conversion chart offers guidance. The switching from semaglutide to tirzepatide dosage chart provides a step-by-step transition protocol.
For comparisons with newer GLP-1 medications, you might find the survodutide vs tirzepatide, orforglipron vs tirzepatide, and CagriSema vs tirzepatide comparisons useful. SeekPeptides keeps these comparison guides updated as new clinical data becomes available.
Practical tips for long-term success at 12.5 mg
Getting to 12.5 mg is an achievement. Staying there and getting the most out of it requires attention to a few details that become more important at higher doses.
Track your vial usage
Know how many doses each vial provides. A 30 mg vial at 12.5 mg per dose gives you 2.4 doses, so roughly two injections with a small amount remaining. A 60 mg vial gives you 4.8 doses. Understanding this helps you time your refills and avoid running out between shipments.
Maintain your injection technique
After months of weekly injections, technique can get sloppy. Rushed injections, skipping alcohol swabs, reusing needles, injecting into the same spot repeatedly. These shortcuts increase the risk of infections, lipodystrophy, and injection site reactions. The peptide injections guide is worth revisiting periodically as a refresher.
Monitor your body composition
At higher tirzepatide doses, the risk of muscle loss alongside fat loss increases if protein intake is inadequate. Aim for a minimum of 0.7 to 1 gram of protein per pound of body weight daily. Resistance training 2 to 3 times per week helps preserve lean mass. The protein shakes for GLP-1 users article covers supplementation strategies.
Know when to ask for help
If you experience persistent vomiting, severe abdominal pain, signs of pancreatitis, or any symptoms that concern you, contact your healthcare provider immediately. Higher doses carry higher risks of rare but serious side effects, and prompt medical attention matters.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of thousands who have navigated these exact questions.
Alternative delivery methods for 12.5 mg tirzepatide
While subcutaneous injection is the standard delivery method, awareness of alternative formats is growing. The tirzepatide tablets vs injections comparison and the oral vs injection analysis cover the developing landscape. Oral tirzepatide is in clinical development, and the oral tirzepatide complete guide tracks the latest progress.
Some pharmacies also offer tirzepatide drops and orally disintegrating tablet formulations. These alternatives have different bioavailability profiles, which means dosing does not directly convert from injectable units. If you are interested in non-injectable options, discuss them with your provider and understand that the unit conversion information in this guide applies specifically to injectable formulations.
Frequently asked questions
Is 12.5 mg of tirzepatide a high dose?
Yes, 12.5 mg is the second-highest FDA-approved dose. Only 15 mg is higher. Most people reach 12.5 mg after at least 16 weeks of titration starting from the 2.5 mg starting dose. The tirzepatide dose chart shows the full range from starting to maintenance doses.
Can I use the same syringe size at 12.5 mg that I used at lower doses?
It depends on your concentration. If your vial is 20 mg/mL or higher, a standard 100-unit insulin syringe works at all dose levels. If your concentration is 10 mg/mL, you will need a larger syringe or split draws at 12.5 mg and above since the volume exceeds 1 mL. Check the syringe recommendations in the conversion table above.
What if my calculation gives me a fraction like 62.5 units?
Round to the nearest whole number. 62.5 rounds to 63 units. The difference between 62 and 63 units at 20 mg/mL is 0.2 mg, which is clinically insignificant. Some syringes have half-unit markings that allow you to draw exactly 62.5 units. If yours does, use that precision. If not, rounding either way is acceptable.
How do I know if my pharmacy changed my concentration?
Check the vial label every single time you receive a new shipment. The concentration should be clearly printed on the label along with the total amount and total volume. If the label looks different from your previous vials, verify the concentration before drawing any dose. When in doubt, call the pharmacy.
Does 12.5 mg of tirzepatide interact with other medications?
Tirzepatide slows gastric emptying, which can affect the absorption of oral medications taken at the same time. This is true at all doses but becomes more pronounced at 12.5 mg and above. If you take oral medications, discuss timing strategies with your provider. The tirzepatide and phentermine interaction guide covers one common combination question.
Should I take 12.5 mg if I am still losing weight at 10 mg?
Not necessarily. If you are achieving satisfactory weight loss and tolerating 10 mg well, there is no requirement to increase. The titration schedule provides the option to increase, not an obligation. Many providers recommend staying at the lowest effective dose to minimize side effects. The how fast does tirzepatide work article discusses expected progress rates at different doses.
Can I go back to 10 mg if 12.5 mg causes too many side effects?
Absolutely. Stepping back to a previously tolerated dose is a standard and completely acceptable approach. Stay at 10 mg for another 4 to 8 weeks, then try increasing again if desired. Your provider can help determine whether the side effects warrant a permanent step-down or just a temporary pause. For more on managing the transition, the tirzepatide and metabolism article discusses how your body adapts to dose changes.
How many weeks of medication does one vial provide at 12.5 mg?
This depends on the total amount in the vial. A 30 mg vial provides 2.4 weekly doses at 12.5 mg (about 2 weeks plus a small remainder). A 60 mg vial provides 4.8 doses (about 5 weeks). A 120 mg vial provides 9.6 doses (about 10 weeks). Track your usage and order refills before running out.
External resources
SURMOUNT-1 clinical trial: tirzepatide for obesity treatment (New England Journal of Medicine)
Tirzepatide dosage guide and FDA-approved dose levels (Drugs.com)
Weight loss efficacy and safety of tirzepatide: systematic review (PubMed Central)
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your syringes stay precise, and your results stay consistent.