Feb 4, 2026

You are wasting medication. Right now, someone is staring at a vial of tirzepatide, drawing up what they think is the right amount, and injecting a dose that is either too high or too low. The syringe reads in units. The prescription reads in milligrams. The vial label shows a concentration in milligrams per milliliter. And somewhere between those three numbers, confusion takes hold. It happens more often than most people realize. A researcher draws 50 units thinking that equals 5 milligrams, but with a 20mg/mL concentration, 50 units actually delivers 10 milligrams, double the intended dose.
Another person calculates correctly but uses the wrong syringe size, and the markings throw everything off. These are not hypothetical scenarios, and they are among the most common mistakes peptide beginners make. They happen every single day in kitchens, bathrooms, and home offices around the world. The difference between an effective tirzepatide protocol and a miserable experience filled with nausea, vomiting, and wasted product often comes down to one thing: understanding how to convert milligrams to units on an insulin syringe. This guide exists to eliminate that confusion permanently. Every concentration, every dose level, every syringe size, mapped out in clear charts you can reference before each injection. Whether you are starting at the initial 2.5mg dose or working your way up through the full escalation schedule toward 15mg, the math behind peptide dosage calculations does not need to be complicated. It just needs to be correct. And by the time you finish reading this, you will never second-guess a tirzepatide unit conversion again.
How tirzepatide works for weight loss
Tirzepatide is not just another weight loss peptide. It belongs to a class of its own. Anyone who has explored the complete peptide list available for research knows that few compounds generate this level of clinical evidence.
Most GLP-1 receptor agonists target a single pathway. Semaglutide, for example, activates only the GLP-1 receptor. Tirzepatide does something fundamentally different. It activates two receptors simultaneously: GLP-1 and GIP. This dual mechanism earned it the nickname "twincretin," and the clinical data suggests this two-pronged approach delivers meaningfully greater weight loss than single-receptor drugs. If you have been researching the differences between semaglutide and tirzepatide, this dual agonism is the primary reason tirzepatide consistently outperforms in head-to-head comparisons.
GLP-1, or glucagon-like peptide-1, slows gastric emptying, reduces appetite, and enhances insulin secretion when blood sugar is elevated. These effects alone produce significant weight loss in many users. But the GIP receptor activation adds layers of metabolic benefit that researchers are still working to fully understand. GIP, or glucose-dependent insulinotropic polypeptide, appears to improve fat metabolism, enhance the body ability to use insulin efficiently, and may directly influence how fat tissue stores and releases energy. The combination creates a metabolic environment where the body burns more stored fat, craves less food, and processes nutrients more effectively.
Those exploring the GLP-3 peptide should note that it operates through an entirely different pathway than tirzepatide. The appetite suppression is what most people notice first. Food simply becomes less interesting. Portions shrink naturally. The constant background noise of hunger that drives overeating goes quiet. But tirzepatide does more than just reduce hunger. It fundamentally shifts how the body handles glucose and fat at the cellular level, which is why researchers studying peptides for weight loss have paid such close attention to the clinical trial results.
For anyone exploring the broader landscape of peptides for fat loss, tirzepatide represents the current gold standard in terms of sheer percentage of body weight lost. The SURMOUNT clinical trial program demonstrated weight reductions that were previously achievable only through bariatric surgery. At the highest approved dose of 15mg weekly, participants lost an average of 22.5% of their body weight over 72 weeks. That figure changed the entire conversation around pharmaceutical weight management.
For men specifically, the fat burning peptides for men guide places tirzepatide in context alongside other options. Understanding this mechanism matters for dosing because it explains why the escalation schedule exists. The body needs time to adjust to dual receptor activation. Jumping to a high dose immediately would overwhelm the GI system, which is why every tirzepatide protocol begins low and climbs gradually. The peptide dosing guide principles that apply to most research peptides apply here as well: start conservative, increase methodically, and let the body adapt at each level before moving forward.
Understanding units, milligrams, and milliliters
This is where most dosing errors begin. Three different measurement systems converge on a single syringe, and confusing any two of them leads to incorrect doses.
Let us start with clear definitions.
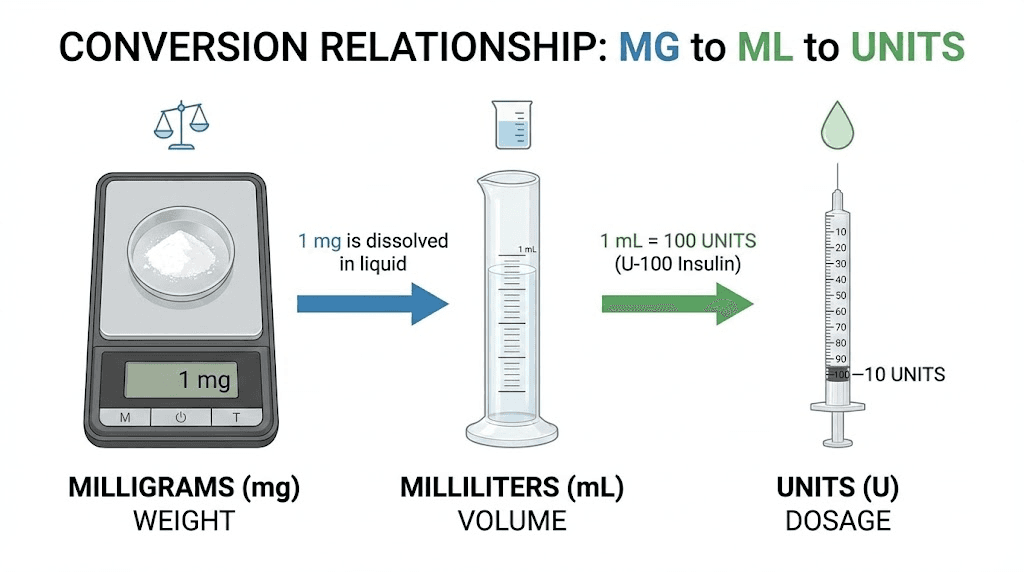
Milligrams (mg) measure the amount of active tirzepatide in your dose. When a protocol calls for 2.5mg or 10mg, it refers to how much actual tirzepatide you are injecting. This is the number that determines your therapeutic effect.
Milliliters (mL) measure the volume of liquid you draw into the syringe. One milliliter is a specific physical amount of fluid, regardless of what is dissolved in it. A vial of tirzepatide contains the peptide dissolved in a solution, and the concentration tells you how many milligrams of tirzepatide exist in each milliliter of that solution.
Units are the markings on an insulin syringe. A standard insulin syringe holds 100 units per 1 mL. This means 100 units equals 1 mL of liquid, 50 units equals 0.5 mL, and 25 units equals 0.25 mL. Units are simply a way of measuring volume using the syringe markings, and the peptide calculator can help verify these conversions instantly.
The critical relationship is this: Units = (Dose in mg / Concentration in mg per mL) x 100
That formula is all you need. Every conversion in this entire article flows from that single equation. If you know the dose your protocol calls for in milligrams and you know the concentration of your vial in milligrams per milliliter, you can calculate the exact number of units to draw every time.
Here is a quick example. You need 5mg of tirzepatide. Your vial concentration is 10mg/mL. The calculation: (5 / 10) x 100 = 50 units. You draw to the 50-unit mark on your insulin syringe. That gives you exactly 0.5 mL of liquid containing 5mg of tirzepatide.
Another example with a different concentration. Same 5mg dose, but your vial is 20mg/mL. The calculation: (5 / 20) x 100 = 25 units. Only 25 units this time, because each unit of liquid contains more tirzepatide when the concentration is higher. This is exactly why knowing your concentration matters so much, and why tools like the peptide reconstitution calculator exist to eliminate guesswork.
The most common mistake is assuming that the same number of units always delivers the same dose of tirzepatide. It does not. The concentration of your specific vial determines everything. Drawing 50 units from a 10mg/mL vial gives you 5mg. Drawing 50 units from a 20mg/mL vial gives you 10mg. Same syringe marking. Completely different dose. Anyone who has read a thorough peptide dosage chart knows that concentration is the variable that changes everything.
If you are reconstituting tirzepatide from lyophilized powder, you control the concentration based on how much bacteriostatic water you add. This is covered in detail in guides about how to reconstitute peptides and how to mix peptides with bacteriostatic water. The amount of water you add directly determines the concentration, which then determines how many units you draw for each dose. Get the reconstitution wrong, and every subsequent dose will be wrong too.
Tirzepatide dosing schedule for weight loss in units
The standard tirzepatide dose escalation for weight loss follows a structured timeline. Each dose level is maintained for a minimum of four weeks before increasing. This is not optional. The four-week minimum allows the body GI system to adapt to each new level of receptor activation, and skipping ahead is the single most common cause of severe nausea and vomiting.
Here is the complete schedule with unit conversions for the three most common concentrations.
At 10mg/mL concentration
This is one of the most widely available concentrations and the one most researchers encounter first. The tirzepatide dosing guide typically references this concentration as the standard.
Dose Level | Milligrams | Units to Draw | Volume (mL) | Minimum Duration |
|---|---|---|---|---|
Starting dose | 2.5mg | 25 units | 0.25 mL | 4 weeks |
Dose level 2 | 5mg | 50 units | 0.50 mL | 4 weeks |
Dose level 3 | 7.5mg | 75 units | 0.75 mL | 4 weeks |
Dose level 4 | 10mg | 100 units | 1.00 mL | 4 weeks |
Dose level 5 | 12.5mg | N/A - exceeds syringe | 1.25 mL | 4 weeks |
Dose level 6 | 15mg | N/A - exceeds syringe | 1.50 mL | Maintenance |
Notice something important at dose levels 5 and 6. At 10mg/mL concentration, 12.5mg requires 125 units, which exceeds the capacity of a standard 100-unit insulin syringe. At this concentration, you would need to either split the injection into two draws or switch to a higher concentration vial. Many researchers transition to a 20mg/mL concentration once they reach these higher doses, and the peptide cost calculator can help determine whether switching concentrations is more economical.
At 20mg/mL concentration
Higher concentration means smaller injection volumes. This is the preferred concentration for anyone dosing at 10mg or above.
Dose Level | Milligrams | Units to Draw | Volume (mL) | Minimum Duration |
|---|---|---|---|---|
Starting dose | 2.5mg | 12.5 units | 0.125 mL | 4 weeks |
Dose level 2 | 5mg | 25 units | 0.25 mL | 4 weeks |
Dose level 3 | 7.5mg | 37.5 units | 0.375 mL | 4 weeks |
Dose level 4 | 10mg | 50 units | 0.50 mL | 4 weeks |
Dose level 5 | 12.5mg | 62.5 units | 0.625 mL | 4 weeks |
Dose level 6 | 15mg | 75 units | 0.75 mL | Maintenance |
With 20mg/mL, every dose fits comfortably within a 100-unit syringe. The trade-off is that the smaller volumes at lower doses, particularly the 12.5 units for the starting 2.5mg dose, require very precise syringe reading. A 30-unit syringe with fine graduations works best for these small volumes, and anyone learning proper peptide injection technique should practice reading these fine markings before their first dose.
At 5mg/mL concentration
This lower concentration is less common but still available. It works well for the initial low doses but becomes impractical at higher dose levels.
Dose Level | Milligrams | Units to Draw | Volume (mL) | Minimum Duration |
|---|---|---|---|---|
Starting dose | 2.5mg | 50 units | 0.50 mL | 4 weeks |
Dose level 2 | 5mg | 100 units | 1.00 mL | 4 weeks |
Dose level 3 | 7.5mg | N/A - exceeds syringe | 1.50 mL | 4 weeks |
Dose level 4 | 10mg | N/A - exceeds syringe | 2.00 mL | 4 weeks |
Dose level 5 | 12.5mg | N/A - exceeds syringe | 2.50 mL | 4 weeks |
Dose level 6 | 15mg | N/A - exceeds syringe | 3.00 mL | Maintenance |
At 5mg/mL, you max out the syringe capacity at just 5mg. Everything above that requires multiple injections or a switch to a higher concentration. For this reason, most experienced researchers prefer 10mg/mL or 20mg/mL for the full escalation. The free peptide reconstitution calculator makes it easy to determine what concentration you will achieve based on the amount of diluent you add.
Understanding these numbers is foundational to safe tirzepatide use. Every person who has studied the broader topic of fat burning peptides knows that precision in dosing separates effective protocols from wasted time and money.
How to read an insulin syringe for tirzepatide
You have the numbers. Now you need to translate them onto the physical syringe in your hand.
Insulin syringes come in three standard sizes: 30 units (0.3 mL), 50 units (0.5 mL), and 100 units (1 mL). Each size has different graduation marks, and choosing the right syringe for your dose volume matters for accuracy.
The 100-unit syringe (1 mL)
This is the most common syringe and the one most people start with. It holds a full milliliter of liquid and is marked in 2-unit increments. Each small line represents 2 units. The numbered markings typically appear at every 10 units: 10, 20, 30, 40, 50, 60, 70, 80, 90, 100. For a dose of 50 units, you fill to the halfway mark. For 25 units, you fill to the line between the 20 and 30 markings. This syringe works well for doses that fall on even numbers but can be tricky for doses like 12.5 units or 37.5 units where you need to estimate between graduation lines.
The 50-unit syringe (0.5 mL)
This mid-size option marks each individual unit, making it much easier to measure odd or fractional doses. When your calculation calls for 37.5 units, you can count to exactly that line. The trade-off is limited capacity: any dose requiring more than 50 units will not fit. For the first few dose levels of tirzepatide at 20mg/mL concentration, this syringe offers excellent precision.
The 30-unit syringe (0.3 mL)
The smallest and most precise option. Each unit is clearly marked, and some models mark half-units as well. This is ideal for the very small volumes needed at 20mg/mL concentration during the early dose levels. When you need 12.5 units for a 2.5mg dose from a 20mg/mL vial, the 30-unit syringe lets you hit that mark with confidence. Anyone exploring what a peptide injection involves should know that syringe selection directly impacts dosing accuracy.
Practical tips for accurate drawing
Hold the syringe at eye level. Looking at it from above or below creates parallax error, and even a small misread translates to a meaningful dose difference. Draw slowly. Pull the plunger back past your target mark slightly, then push forward to the exact line. This removes any air that may have entered during the draw. Tap the syringe barrel if you see air bubbles. Air does not cause harm with subcutaneous injections, but it does displace liquid volume, meaning you get less medication than intended. These details matter. The resources at SeekPeptides cover injection technique extensively because small errors in preparation compound over weeks and months of use.
For anyone who works with multiple peptides, the fundamentals of syringe reading apply universally. Whether you are measuring tirzepatide, preparing a peptide stack, or working with any injectable peptide, the same principles of accurate volume measurement keep your dosing on track.
Complete tirzepatide dose escalation timeline
Here is what a full tirzepatide dose escalation looks like, week by week, from the very first injection to the maximum maintenance dose. This timeline assumes a standard four-week hold at each level, which is the minimum recommended period. Many researchers hold longer at certain levels, particularly when side effects need more time to subside.
Weeks 1 through 4: 2.5mg (starting dose)
This is not a therapeutic dose for weight loss. Think of it as an introduction. The body is meeting tirzepatide for the first time, and the GLP-1 and GIP receptors are beginning to respond to external activation. Most people notice mild appetite reduction within the first few days. Some notice nothing at all. Significant weight loss at this dose is uncommon, though some individuals do lose 2 to 5 pounds from reduced food intake alone.
Side effects at this level are generally mild. Slight nausea after eating. Maybe some stomach gurgling. Nothing that disrupts daily life for most people. This is the adjustment phase, and the getting started with peptides guide covers what to expect during these initial weeks regardless of which peptide you are using.
Weeks 5 through 8: 5mg (first therapeutic dose)
Now things start to happen. Five milligrams is the first dose level where meaningful weight loss typically begins. Appetite suppression becomes noticeably stronger. Portions shrink without effort. The constant mental negotiation around food, the "should I eat this" internal debate, starts to fade into the background.
This is also where GI side effects tend to peak for the first time. Nausea affects 18 to 29 percent of users, and most of those cases begin during the first week or two at 5mg. The body has doubled its exposure to dual receptor activation, and the digestive system needs time to catch up. Eating smaller meals, avoiding greasy foods, and staying hydrated help enormously. Many researchers find that this dose level is where they first feel the medication truly working.
For perspective on what this dose level produces in clinical settings, the SURMOUNT-1 trial showed that participants on 5mg lost an average of 16% of their body weight over 72 weeks. That is a remarkable result from what is actually the lowest therapeutic dose. If you are comparing this to other peptides considered best for fat loss, very few single compounds come close to that figure.
Weeks 9 through 12: 7.5mg
The transition to 7.5mg is usually smoother than the jump to 5mg. The body receptor systems are already activated and partially adapted. Still, expect a brief resurgence of nausea during the first week, typically milder than what you experienced at 5mg. Weight loss accelerates for most users at this level. Weekly losses of 1.5 to 2.5 pounds are common among those following reasonable dietary practices. The peptide transformation results that researchers document often show the most visible changes beginning around this dose level.
Weeks 13 through 16: 10mg
Ten milligrams represents a significant threshold. This is the level where many experienced researchers, including those following peptide strength protocols, report the most dramatic body composition changes. It is the dose at which the SURMOUNT-1 trial recorded an average weight loss of 21.4% of body weight over the full study period. Appetite suppression at this level is profound for most users. Some describe it as simply forgetting to eat, not through deprivation, but through a genuine absence of hunger signals.
The jump to 10mg may produce stronger GI effects than previous increases. The peptide safety and risks guide covers general approaches to managing dose-dependent side effects, and the principles apply directly here. If side effects are significant, holding at 10mg for six to eight weeks instead of four before considering further increases is a prudent approach.
Weeks 17 through 20: 12.5mg
Not everyone needs to reach this dose. If weight loss is progressing steadily at 10mg with manageable side effects, there is no requirement to continue escalating. The purpose of dose escalation is to overcome plateaus and achieve target weight loss, not to reach the maximum dose as quickly as possible.
Those who do progress to 12.5mg typically see continued improvement in body composition. The dual GIP/GLP-1 activation at this level appears to significantly improve how the body partitions energy between fat storage and utilization. Researchers tracking their progress with a structured peptide cycle planning guide often note that the 12.5mg level is where visible changes in body composition become dramatic.
Weeks 21 and beyond: 15mg (maximum dose)
The ceiling. At 15mg weekly, the SURMOUNT-1 trial recorded an average weight loss of 22.5% of body weight. Over 89% of participants at this dose level lost at least 5% of their body weight, and a substantial proportion lost 20% or more. These numbers are extraordinary in the context of pharmaceutical weight management.
Not everyone will reach or need 15mg. The ideal maintenance dose is the one that produces consistent weight loss with tolerable side effects. For some, that is 10mg. For others, the full 15mg is necessary to achieve their goals. A qualified healthcare provider can guide this decision based on individual response patterns. The semaglutide versus tirzepatide comparison page breaks down how these dose-response curves differ between the two most popular GLP-1 medications.
Conversion charts for every concentration
These are the reference tables you will return to before every injection. Print them. Save them. Bookmark this page. Accurate dosing starts here, and tools like the peptide calculator can double-check your math any time you want additional confirmation.
10mg/mL concentration: complete conversion chart
Dose (mg) | Units on Syringe | Volume (mL) | Best Syringe Size |
|---|---|---|---|
1.0mg | 10 units | 0.10 mL | 30-unit syringe |
1.5mg | 15 units | 0.15 mL | 30-unit syringe |
2.0mg | 20 units | 0.20 mL | 30-unit syringe |
2.5mg | 25 units | 0.25 mL | 30 or 50-unit syringe |
3.0mg | 30 units | 0.30 mL | 50-unit syringe |
3.5mg | 35 units | 0.35 mL | 50-unit syringe |
4.0mg | 40 units | 0.40 mL | 50-unit syringe |
5.0mg | 50 units | 0.50 mL | 50 or 100-unit syringe |
6.0mg | 60 units | 0.60 mL | 100-unit syringe |
7.5mg | 75 units | 0.75 mL | 100-unit syringe |
8.0mg | 80 units | 0.80 mL | 100-unit syringe |
10.0mg | 100 units | 1.00 mL | 100-unit syringe |
At 10mg/mL, the math is straightforward: multiply the desired dose in milligrams by 10 to get units. Five milligrams equals 50 units. Seven point five milligrams equals 75 units. The simplicity of this concentration is one reason it remains popular among researchers who prefer mental math over calculator apps, though the peptide calculator for milligram conversions is always available for verification.
20mg/mL concentration: complete conversion chart
Dose (mg) | Units on Syringe | Volume (mL) | Best Syringe Size |
|---|---|---|---|
1.0mg | 5 units | 0.05 mL | 30-unit syringe |
2.0mg | 10 units | 0.10 mL | 30-unit syringe |
2.5mg | 12.5 units | 0.125 mL | 30-unit syringe |
3.0mg | 15 units | 0.15 mL | 30-unit syringe |
4.0mg | 20 units | 0.20 mL | 30-unit syringe |
5.0mg | 25 units | 0.25 mL | 30 or 50-unit syringe |
6.0mg | 30 units | 0.30 mL | 50-unit syringe |
7.5mg | 37.5 units | 0.375 mL | 50-unit syringe |
8.0mg | 40 units | 0.40 mL | 50-unit syringe |
10.0mg | 50 units | 0.50 mL | 50 or 100-unit syringe |
12.5mg | 62.5 units | 0.625 mL | 100-unit syringe |
15.0mg | 75 units | 0.75 mL | 100-unit syringe |
The 20mg/mL concentration is the most versatile. Every dose in the standard escalation schedule fits within a 100-unit syringe. The volumes are smaller, which also means less discomfort at the injection site and less liquid to absorb subcutaneously. For those managing multiple peptides and looking to understand the economics, the peptide cost calculator helps compare costs across different vial sizes and concentrations.
The challenge with 20mg/mL is precision at the lower doses. Drawing 12.5 units accurately requires a high-quality syringe with fine graduations. If your syringe only marks every 2 units, you are estimating, and that estimate may be off by 10 to 20 percent at such a small volume. This is why syringe selection is not an afterthought. It is a critical part of the dosing equation, and something covered in detail in the peptide injections guide.
5mg/mL concentration: complete conversion chart
Dose (mg) | Units on Syringe | Volume (mL) | Best Syringe Size |
|---|---|---|---|
1.0mg | 20 units | 0.20 mL | 30-unit syringe |
1.5mg | 30 units | 0.30 mL | 50-unit syringe |
2.0mg | 40 units | 0.40 mL | 50-unit syringe |
2.5mg | 50 units | 0.50 mL | 50 or 100-unit syringe |
3.0mg | 60 units | 0.60 mL | 100-unit syringe |
4.0mg | 80 units | 0.80 mL | 100-unit syringe |
5.0mg | 100 units | 1.00 mL | 100-unit syringe |
At 5mg/mL, you hit the syringe ceiling at just 5mg. Anything above that requires more than 1 mL, which a standard insulin syringe cannot hold. This concentration is useful for the early stages of dose escalation when you want large, easy-to-read volumes on the syringe. Some researchers start with 5mg/mL for their first month at 2.5mg, drawing a nice easy 50 units, then switch to 10mg/mL or 20mg/mL as doses increase.
Choosing a concentration is not just about math. It also involves considering storage, how many doses you get per vial, and injection comfort. Resources on bacteriostatic water for peptides and the question of how much bacteriostatic water to add directly impact what concentration you end up with after reconstitution.
What the clinical trials actually show
Numbers matter. Claims are cheap. The clinical evidence behind tirzepatide for weight loss is among the most robust in pharmaceutical history, and understanding what the data actually says helps you set realistic expectations for each dose level.
SURMOUNT-1: the landmark trial
SURMOUNT-1 enrolled 2,539 adults with obesity or overweight, with at least one weight-related complication, but without type 2 diabetes. Participants received either tirzepatide at 5mg, 10mg, or 15mg weekly, or placebo, for 72 weeks. The results changed the field. The full scope of the evidence is tracked in the peptide research and studies library.
At 5mg weekly, participants lost an average of 16.0% of their body weight. At 10mg, the average was 21.4%. At 15mg, participants achieved an average weight loss of 22.5%. The placebo group lost 2.4%. These are not cherry-picked results. These are intention-to-treat analyses that include every enrolled participant, even those who dropped out or missed doses.
To put these numbers in perspective, a person weighing 250 pounds at enrollment would lose an average of 40 pounds on 5mg, 53.5 pounds on 10mg, or 56.25 pounds on 15mg over the 72-week study period. Those figures rival the outcomes of certain bariatric surgical procedures, and they represent averages, meaning roughly half of participants lost even more. For context on how these results compare to other options, the comprehensive review of peptides for weight loss places tirzepatide at the top of the efficacy hierarchy.
Response rates across dose levels
The percentage of participants who achieved clinically meaningful weight loss thresholds is equally impressive.
Threshold | 5mg | 10mg | 15mg | Placebo |
|---|---|---|---|---|
Lost 5% or more | 85% | 89% | 91% | 35% |
Lost 10% or more | 69% | 78% | 84% | 19% |
Lost 15% or more | 50% | 67% | 71% | 9% |
Lost 20% or more | 32% | 50% | 57% | 3% |
Look at the 10mg and 15mg columns. Nearly 9 out of 10 participants lost at least 5% of their body weight, a threshold that clinical guidelines consider meaningful for reducing cardiovascular risk, improving metabolic markers, and alleviating joint stress. Over half at the highest dose lost 20% or more. These response rates explain the explosive interest in tirzepatide as a weight loss intervention and why it consistently appears in discussions about the best peptide stacks for weight loss.
Metabolic improvements beyond weight loss
Tirzepatide did far more than reduce body weight in the clinical trials. Researchers observed significant improvements in nearly every metabolic marker measured.
Over 95% of participants who entered the trials with prediabetes converted to normal blood sugar levels. Insulin sensitivity improved dramatically across all dose groups. Inflammatory markers decreased. Triglycerides dropped. Blood pressure improved. Waist circumference, a key indicator of dangerous visceral fat, decreased substantially. These findings suggest that tirzepatide addresses the underlying metabolic dysfunction that drives weight gain, not just the surface-level number on the scale. For those specifically targeting abdominal fat, the guide on the best peptide for visceral fat loss explores this data in depth.
The metabolic benefits have important implications for dosing decisions. Even at the lower 5mg dose, metabolic improvements were clinically significant. A person who cannot tolerate higher doses due to GI side effects may still experience transformative health benefits at 5mg, even if the total weight lost is somewhat lower than what higher doses produce.
Managing side effects at each dose level
Side effects are not a sign that something is wrong. They are a sign that the medication is active. The GI system contains a dense network of GLP-1 receptors, and activating them produces predictable effects on digestion. Understanding what to expect at each dose level helps you prepare rather than panic.
Side effects at 2.5mg
Mild nausea in 5 to 10 percent of users. Occasional bloating. Slight decrease in appetite. Most people sail through this dose without any issues worth mentioning. Anyone new to what peptides are and what peptides are used for will find this introductory dose reassuringly gentle. If you experience significant nausea at 2.5mg, that is actually useful information, it suggests you may be particularly sensitive and should plan for slower escalation later.
Side effects at 5mg
This is where nausea becomes more common, affecting 18 to 29 percent of users in clinical trials. Diarrhea, constipation, and decreased appetite are also frequently reported. The first week at 5mg is typically the worst. By week three or four, the body adjusts and symptoms usually diminish significantly.
Management strategies that work:
Eat smaller meals throughout the day rather than two or three large ones
Avoid high-fat, greasy, or heavily spiced foods during the first two weeks at a new dose
Stay well hydrated, sipping water throughout the day rather than drinking large amounts at once
Ginger tea or ginger supplements can reduce nausea naturally
Eat slowly and stop at the first sign of fullness, pushing past satiety is the fastest path to nausea
Take the injection at bedtime so the initial peak effects occur while sleeping
These same strategies apply to managing side effects from other peptides. The common peptide mistakes beginners make article covers how ignoring early side effect signals leads to worse outcomes down the line.
Side effects at 7.5mg and 10mg
Most users who tolerated 5mg well will find 7.5mg manageable. The increase is smaller in relative terms (50% more than 5mg, compared to 100% more when going from 2.5mg to 5mg), and the receptor systems are already partially adapted. Ten milligrams may trigger another wave of GI symptoms, particularly in the first week. Some researchers use peptides alongside GLP-1 medications for gut healing to manage these GI effects. Constipation becomes more common at this level, and some users report what researchers call "sulfur burps," a distinctive side effect related to slowed gastric emptying.
Importantly, if side effects at 10mg are severe, you do not need to push through them. Dropping back to 7.5mg for an additional four to eight weeks, then reattempting 10mg, is a legitimate and often more successful strategy than trying to endure severe nausea. Understanding your body response patterns is crucial, and tracking them helps. SeekPeptides members often use protocol tracking tools to monitor how they respond at each dose level, making escalation decisions more data-driven and less guesswork-based.
Side effects at 12.5mg and 15mg
At the highest dose levels, the GI side effects that do occur tend to be more about constipation and early satiety than acute nausea. The body has had months to adapt to GLP-1 and GIP receptor activation by this point. That said, some users do experience renewed nausea at each increase, and the management strategies remain the same: smaller meals, hydration, ginger, and patience.
Rare but more serious side effects that warrant medical attention include severe abdominal pain (which could indicate pancreatitis), persistent vomiting lasting more than 48 hours, and signs of allergic reaction such as swelling or difficulty breathing. These are uncommon but real, and anyone using tirzepatide should be aware of them. The peptide safety and risks resource provides a broader framework for understanding when side effects cross from expected into concerning territory.
A point that bears repeating: side effect management is not about toughing it out. It is about optimizing the relationship between efficacy and tolerability. The dose that produces steady weight loss with manageable side effects is the right dose, whether that ends up being 5mg or 15mg. Aggressive escalation that causes severe nausea often leads to poor adherence, missed injections, and worse outcomes than a slower, more tolerable approach.
When to increase your tirzepatide dose (and when to wait)
Knowing when to move up is just as important as knowing how many units to draw.
The default guidance is simple: hold each dose for a minimum of four weeks, then increase if weight loss has stalled or slowed significantly and side effects at the current dose are manageable. But real-world dosing is rarely that clean. Bodies do not follow textbook timelines. Some people respond beautifully at 5mg and stay there for months. Others need 15mg to see meaningful results. The key is understanding the signals, something the peptides for gut health guide also emphasizes when discussing GI adaptation.
Signs that suggest it may be time to increase
Weight loss has stopped for two or more consecutive weeks despite consistent diet and exercise habits. Appetite suppression has noticeably weakened, and old eating patterns are starting to return. You have been at your current dose for at least four weeks with no significant GI side effects. These are the classic indicators that the body has adapted to the current dose and a higher level of receptor activation may be needed to continue progress.
Weight loss plateaus are normal and expected. They do not mean the medication has stopped working. The body metabolic rate adjusts as weight decreases, and a dose that produced robust weight loss at 280 pounds may produce slower loss at 240 pounds. This is basic physiology, not a failure of the medication. The guide on how long peptides take to work explains why patience and realistic timelines matter more than dose maximization.
Signs that suggest you should wait
You are still experiencing notable nausea, vomiting, or diarrhea at your current dose. Weight loss is still occurring, even if slowly. You have been at the current dose for less than four weeks. You recently changed your diet, exercise routine, or other medications. Any of these conditions mean the current dose still has room to work, and increasing would likely produce side effects that offset any additional benefit.
Some researchers hold at a dose for eight or even twelve weeks before increasing. There is no penalty for going slowly. The total weight lost over six months tends to be similar whether someone escalates aggressively or conservatively, because the aggressive escalator often has to pause or reduce doses due to side effects while the conservative escalator progresses steadily without interruption.
The staircase method versus the fast track
Two philosophical approaches exist. The staircase method follows the standard four-week minimum at each level, increasing only when weight loss plateaus. This tends to produce fewer side effects and better long-term adherence. The fast track pushes to the maximum tolerable dose as quickly as possible, on the theory that higher doses produce faster results. Clinical data from SURMOUNT-1 supports the staircase approach, as it is the protocol that produced the headline weight loss numbers.
For those who use the peptide stack calculator to plan multi-compound protocols, conservative dose escalation becomes even more important. Adding complexity to an already aggressive escalation schedule compounds both the potential benefits and the potential risks.
Common dosing mistakes and how to avoid them
Mistakes happen. They happen less when you know what to watch for.
Mistake 1: ignoring the concentration on the vial
This is the most dangerous error. A person receives a 20mg/mL vial but doses as if it were 10mg/mL, drawing twice as many units as needed. Or the reverse: treating a 10mg/mL vial as 20mg/mL, getting half the intended dose. Always, always, always check the concentration on your specific vial before calculating units. Write it on a sticky note and attach it to the vial if needed. Use the peptide reconstitution calculator every single time until the math becomes second nature.
Mistake 2: using the wrong syringe
Not all syringes are created equal. A tuberculin syringe, for example, also measures in milliliters but does not use the same unit scale as an insulin syringe. Drawing from a tuberculin syringe while reading a chart designed for insulin syringes produces incorrect doses. Always use a standard U-100 insulin syringe for tirzepatide dosing. The "U-100" designation means the syringe is calibrated for 100 units per milliliter, which is the standard that all the conversion charts in this article are based on.
Mistake 3: escalating too quickly
Impatience is the enemy of effective dosing. Someone who jumps from 2.5mg to 7.5mg or 10mg to avoid the "slow" intermediate steps almost always regrets it. The GI side effects that result from skipping dose levels can be severe enough to cause dehydration, missed work, and complete abandonment of the protocol. Four weeks at each level is not arbitrary. It is the minimum time needed for GI adaptation, and even that is not always enough. The peptide dosing guide emphasizes gradual escalation for exactly this reason, and it applies to virtually every compound in the peptide research space.
Mistake 4: not accounting for air bubbles
An air bubble in the syringe displaces liquid volume. If you draw to the 50-unit mark but 5 units of that is air, you are injecting 45 units of medication. Over weeks, this adds up. After drawing your dose, hold the syringe needle-up, tap the barrel to move bubbles to the top, then push the plunger gently until the air is expelled and a tiny drop of liquid appears at the needle tip. Only then is your measured dose accurate.
Mistake 5: inconsistent injection timing
Tirzepatide is a once-weekly injection. Taking it every 5 days one week and every 9 days the next creates uneven blood levels that reduce efficacy and increase side effects. Choose a day and stick to it. If you miss a dose, the general guidance is to take it as soon as you remember if you are within a few days of your scheduled day, then resume your regular schedule the following week. Anyone who has read about how peptides work understands that consistent timing is essential for maintaining stable receptor activation. The peptide forum guide is filled with reports from users who learned this lesson the hard way.
Mistake 6: switching concentrations without recalculating
A researcher who has been drawing 50 units from a 10mg/mL vial (5mg dose) receives a new vial at 20mg/mL. Out of habit, they draw 50 units again, but now that delivers 10mg, double the intended dose. Every time you open a new vial, verify the concentration and recalculate your unit dose from scratch. This is non-negotiable. The guide on how to calculate peptide dosages walks through this recalculation process step by step.
Mistake 7: poor storage affecting potency
Tirzepatide that has been stored improperly may lose potency without any visible change. You draw what should be an effective dose, but the degraded peptide delivers less biological activity. The result looks like a dosing problem but is actually a storage problem. Proper storage protocols, covered extensively in the peptide storage guide and the guide on how to store peptides after reconstitution, protect your investment and ensure each dose delivers full potency. Understanding how long peptides last in the fridge and at room temperature prevents this silent form of waste.
Tirzepatide dosing for different weight loss goals
Not every person needs the same endpoint. A 300-pound individual seeking to lose 80 pounds has different dosing considerations than a 200-pound person aiming to lose 30 pounds. The clinical data helps frame expectations for different scenarios.
Moderate weight loss (10-15% body weight)
If your goal is to lose 10 to 15 percent of your body weight, the lower end of the dose escalation, between 5mg and 7.5mg weekly, may be sufficient. The SURMOUNT-1 trial showed that even the 5mg dose produced an average 16% weight loss, which falls right in this range. Many individuals achieve their target at these moderate doses without ever needing to escalate to 10mg or above.
Staying at a lower dose means fewer side effects, lower weekly cost, and a simpler protocol. For women exploring peptide options, the peptides for weight loss in women guide discusses how female hormonal factors can influence dose response, making moderate doses particularly effective for some women.
Significant weight loss (15-20% body weight)
Losing 15 to 20 percent of body weight typically requires doses of 7.5mg to 10mg weekly, sustained over six months or longer. This is the sweet spot where the dual GIP/GLP-1 mechanism delivers its most dramatic effects on body composition while side effects remain manageable for most users. The transition from visible weight loss to genuine body transformation often happens in this range.
At this level, combining tirzepatide with resistance training and adequate protein intake becomes especially important for preserving lean muscle mass. Weight loss of this magnitude without exercise can result in significant muscle loss along with fat loss, which reduces metabolic rate and makes weight regain more likely. The principles discussed in peptides for muscle growth and the guide on peptides for both weight loss and muscle gain become relevant for anyone losing significant body weight.
Maximum weight loss (20%+ body weight)
Achieving 20 percent or greater weight loss consistently requires the higher dose levels of 10mg to 15mg weekly, maintained over nine months to a year or longer. In SURMOUNT-1, over half the participants at 15mg lost 20% or more of their body weight. These results are transformative, often involving the loss of 50 to 100+ pounds depending on starting weight.
Protocols at this level demand careful monitoring. Regular blood work to track metabolic markers, consistent protein intake of at least 0.7 to 1 gram per pound of lean body mass, and structured exercise are all important. The journey is a marathon, not a sprint. Resources covering peptide cycle planning can help structure a long-term approach that accounts for dose escalation, potential plateaus, and maintenance planning.
Maintenance after reaching goal weight
An often-overlooked aspect of tirzepatide dosing is what happens after you reach your target weight. Stopping the medication abruptly typically results in significant weight regain, as the appetite-suppressing effects wear off and old eating patterns return. Many healthcare providers recommend transitioning to a lower maintenance dose, often 5mg to 7.5mg weekly, rather than discontinuing entirely.
The maintenance phase is where good habits established during weight loss become critical. If tirzepatide taught you to eat smaller portions, choose nutrient-dense foods, and listen to satiety signals, continuing those practices on a lower dose can sustain your results. The peptides before and after results page showcases what sustained commitment to a protocol looks like over months and even years of consistent use.
Comparing tirzepatide dosing to other weight loss peptides
Tirzepatide does not exist in isolation. Understanding how its dosing compares to other weight loss compounds helps frame expectations and supports informed decision-making.
Semaglutide, the active ingredient in Ozempic and Wegovy, follows a different escalation schedule: 0.25mg for four weeks, 0.5mg for four weeks, 1mg for four weeks, 1.7mg for four weeks, and finally 2.4mg for maintenance. The maximum semaglutide dose of 2.4mg produces roughly 15 to 17 percent weight loss in trials, compared to tirzepatide 15mg at 22.5 percent. The semaglutide dosage calculator handles the unit conversions for that compound specifically, and the semaglutide versus tirzepatide comparison breaks down the differences in depth. For those considering alternatives to branded semaglutide products, the Ozempic alternatives overview covers the available options.
Retatrutide, an emerging triple agonist targeting GLP-1, GIP, and glucagon receptors, has shown even greater weight loss potential in early trials. Its dosing schedule differs significantly from tirzepatide, and the retatrutide dosage chart and the retatrutide 20mg dosing guide cover its unique escalation protocol. For anyone researching retatrutide availability, the retatrutide buy guide and retatrutide cost guide provide practical information.
Cagrilintide is another compound that has generated interest in the weight loss peptide space. It works through the amylin pathway rather than GLP-1, and some researchers are combining it with tirzepatide for potentially synergistic effects. The cagrilintide for weight loss article covers its mechanism, while the cagrilintide dosage with tirzepatide guide addresses combination protocols. Related resources include the cagrilintide dosing overview and the cagrilintide for men guide.
Older peptides like AOD-9604 and 5-amino-1MQ offer different mechanisms for fat loss with considerably different dosing structures. The AOD-9604 complete guide and AOD-9604 dosage guide cover that compound in detail, while the 5-amino-1MQ guide explores a non-injectable option. Some researchers also explore tesofensine as an alternative approach to appetite control, and lipotropic peptides offer yet another pathway to enhanced fat metabolism.
What sets tirzepatide apart is the magnitude of its effect. No other single-compound protocol currently matches its clinical weight loss data. This does not mean it is the right choice for everyone. Side effect tolerance, cost, availability, and individual metabolic response all play roles in the decision. But on raw efficacy, tirzepatide stands alone. The broader conversation about bioactive precision peptides for weight loss continues to evolve as new compounds enter clinical trials, and SeekPeptides tracks these developments closely.
Practical tips for your tirzepatide protocol
Knowledge without execution is useless. Here are actionable practices that make tirzepatide dosing safer and more effective from week one.
Label everything
Write the concentration on the vial with a permanent marker. Note the date of reconstitution if applicable. Record which dose level you are currently on and the date you started it. Memory is unreliable when you are managing weekly injections over months, especially if you are also following a broader peptide cycle plan or working with peptide vials from different batches. A simple log prevents mistakes that memory alone cannot.
Pick a consistent injection day and time
Most researchers choose a day when they can be home and relatively inactive for the hours following injection. Some people experience mild fatigue or nausea in the first few hours after their weekly dose. Injecting on a Friday evening, for instance, allows any initial effects to pass over the weekend. Whatever day you choose, consistency matters. The same day each week, roughly the same time, creates the steadiest blood levels. The peptides for men guide and the peptides for belly fat guide both emphasize this consistency principle for maximizing fat loss outcomes.
Rotate injection sites
Tirzepatide is a subcutaneous injection, meaning it goes into the fat layer beneath the skin. The recommended sites are the abdomen (at least two inches from the navel), the front of the thighs, and the back of the upper arms. Rotating between these sites prevents localized reactions like lipodystrophy, where the fat tissue at a repeatedly used site changes texture. The peptide injections guide covers site rotation in comprehensive detail.
Track your response
Keep a weekly log of: body weight, dose level, injection site, notable side effects, appetite level on a scale of 1 to 10, and general energy. This data becomes invaluable when deciding whether to escalate, hold, or reduce a dose. Patterns that are invisible week-to-week become obvious when you review a month of logged data. SeekPeptides provides protocol tracking frameworks that make this simple and systematic.
Understand the role of protein
When losing significant weight on tirzepatide, protein intake is not optional. Adequate protein preserves lean muscle mass, supports metabolic rate, and improves satiety. Aim for at least 0.6 to 1.0 grams of protein per pound of target body weight daily. This becomes harder as appetite decreases, which is precisely why protein should be the priority at every meal. Planning high-protein meals and snacks ensures that reduced caloric intake does not mean reduced nutrition quality.
Work with reliable sources
The tirzepatide market, like the broader peptide market, includes products of varying quality. Working with reputable sources is critical for dose accuracy because if the stated concentration on the vial is inaccurate, every unit conversion based on that concentration will be wrong. Guides like the best peptide vendors review and the discussion of grey market peptides provide context for evaluating source quality. Understanding peptide regulation developments and the legal landscape of peptides also helps inform sourcing decisions.
Consider oral versus injectable forms
Oral tirzepatide formulations are in development and may change the dosing landscape significantly. Currently, the injectable form is standard, and all the unit-based dosing in this guide assumes subcutaneous injection. The oral tirzepatide guide covers what is known about these emerging formulations. For a broader understanding of the differences between delivery methods, the injectable versus oral peptides comparison provides important context.
Building a complete tirzepatide protocol
Dosing in units is one piece of a larger puzzle. A truly effective tirzepatide protocol integrates dosing with diet, exercise, monitoring, and long-term planning.
Start with your healthcare provider. Establish baseline blood work including fasting glucose, HbA1c, lipid panel, thyroid function, liver enzymes, and kidney function. These baselines let you objectively measure the metabolic improvements that tirzepatide produces, and they also screen for contraindications that may affect whether or how you use the medication. Understanding the basics of whether peptides show up on drug tests may also be relevant for some researchers, as is the broader peptides versus steroids comparison for those evaluating different approaches to body composition.
Build your nutritional framework around protein first, vegetables second, and then fill remaining calories with healthy fats and complex carbohydrates. Tirzepatide will reduce your total caloric intake naturally through appetite suppression, so making every calorie count becomes more important, not less. A 1,200-calorie day composed of processed foods provides far less nutritional support than a 1,200-calorie day of lean proteins, vegetables, and whole grains. Those dealing with menopause-related weight challenges will find tailored guidance in the peptides for menopause weight loss resource.
Add resistance training at least three times per week. This is not about becoming a bodybuilder. It is about sending the signal to your body that muscle tissue is needed and should not be broken down for energy. Walking, while excellent for general health, does not provide this signal. Lifting weights, using resistance bands, or performing bodyweight exercises does. The resources on peptides for muscle growth and the safest peptides for muscle growth discuss how to support lean mass during aggressive weight loss.
Plan for monthly check-ins with your protocol. Review your weight trend, side effects, dosing history, and overall well-being at least once per month. Decide at each check-in whether to hold the current dose or escalate. These scheduled reviews prevent both impulsive dose changes and the opposite problem of staying at a suboptimal dose out of inertia.
The peptide therapy cost guide and the guide to peptide costs help with budgeting for the long term, because tirzepatide protocols often run six months to a year or longer. Knowing the financial commitment upfront prevents interrupted protocols due to unexpected costs. For those looking at clinical settings, the peptide therapy near me guide and online peptide therapy guide cover the available options for supervised use.
Some researchers explore stacking tirzepatide with other compounds. The peptide stacks guide covers the general principles, and the peptide stack calculator helps plan multi-compound protocols. If you are considering adding other peptides, understanding how many peptides you can take at once and whether you can cycle different peptides becomes essential. The cagrisema dosing and cagrilintide and semaglutide resources provide context for combination approaches that specifically target weight loss through multiple pathways.
Frequently asked questions
How many units of tirzepatide is 2.5mg?
It depends entirely on the concentration of your vial. At 10mg/mL, 2.5mg equals 25 units. At 20mg/mL, 2.5mg equals 12.5 units. At 5mg/mL, 2.5mg equals 50 units. Always apply the formula: (Dose in mg / Concentration in mg per mL) x 100 = Units. The peptide calculator can verify this conversion for any concentration.
How many units of tirzepatide is 5mg?
At 10mg/mL concentration, 5mg equals 50 units. At 20mg/mL, it equals 25 units. At 5mg/mL, it equals 100 units, the full capacity of a standard insulin syringe. The concentration is the variable that determines everything, which is why checking your vial label before every injection is a non-negotiable habit.
How many units of tirzepatide is 10mg?
At 10mg/mL, 10mg equals 100 units, a full 1 mL syringe. At 20mg/mL, 10mg equals just 50 units, half the syringe. This is why many researchers switch to 20mg/mL concentration as they escalate to higher doses. The smaller injection volume is also more comfortable.
What is the maximum dose of tirzepatide for weight loss?
The maximum approved dose is 15mg weekly. In clinical trials, this produced an average weight loss of 22.5% of body weight over 72 weeks. Not everyone needs the maximum dose. Many individuals achieve their weight loss goals at 5mg, 7.5mg, or 10mg. The optimal dose is the lowest one that produces consistent results with manageable side effects. The tirzepatide dosing guide provides detailed information about finding your optimal dose level.
Can I split a tirzepatide dose into two injections per week?
Some researchers split their weekly dose into two smaller injections, typically three or four days apart. This approach is not part of the standard clinical protocol, but anecdotal reports suggest it may reduce GI side effects because each injection delivers a smaller spike of medication. If you choose to split doses, the total weekly amount should remain the same. For example, instead of one 10mg injection, you would do two 5mg injections. The unit calculation is the same for each injection; you simply use a smaller amount each time.
How do I convert tirzepatide units if I reconstitute from powder?
The amount of bacteriostatic water you add determines the concentration. For example, if you have a 10mg vial and add 1 mL of bacteriostatic water, the concentration is 10mg/mL. If you add 2 mL, the concentration is 5mg/mL. If you add 0.5 mL, the concentration is 20mg/mL. From there, the standard unit formula applies. The peptide reconstitution calculator handles this math automatically, and the guides on how to reconstitute peptides and what water to mix with peptides cover the complete process.
What happens if I miss a tirzepatide dose?
If you miss your scheduled injection by one or two days, take it as soon as you remember and then resume your regular schedule the following week. If more than four days have passed since your missed dose, skip that week entirely and take your normal dose on the next scheduled day. Do not double up doses to compensate for a miss. Consistency matters more than perfection, and one missed dose will not undo weeks of progress.
Do I need to refrigerate tirzepatide?
Unreconstituted tirzepatide (in powder form) should be stored in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Once reconstituted, it should also be refrigerated and used within the timeframe recommended for the specific formulation, which varies. The peptide storage guide and the guide on how long reconstituted peptides last in the fridge cover storage in detail. Understanding whether peptides expire is also important for maintaining dose accuracy over time.
Is tirzepatide safe to use long-term?
Clinical trials running up to 72 weeks have shown a manageable safety profile with primarily GI-related side effects. Long-term data beyond the trial periods is still being collected. The most common concerns involve gallbladder events, pancreatitis risk, and potential thyroid effects, all of which occur at low rates but warrant monitoring through regular medical check-ups. The peptide research and studies section tracks ongoing safety data as it becomes available.
Can I use tirzepatide with other peptides?
Some researchers combine tirzepatide with other compounds, but this should be approached with caution and ideally under medical supervision. Combining multiple GLP-1 agonists (like tirzepatide and semaglutide simultaneously) is generally not recommended as it amplifies GI side effects without proportional benefit. However, combining tirzepatide with peptides targeting different pathways, such as BPC-157 for gut health or growth hormone secretagogues for body composition, is more common. The BPC-157 guide, TB-500 guide, and ipamorelin benefits page provide information on these individual compounds. Also worth exploring are the CJC-1295 guide and sermorelin benefits for understanding growth hormone secretagogue options that some researchers use alongside GLP-1 compounds.
External resources
SURMOUNT-1 Trial Publication, New England Journal of Medicine - The landmark clinical trial data for tirzepatide in obesity treatment
FDA Prescribing Information for Mounjaro (tirzepatide) - Official FDA label with complete dosing, safety, and pharmacological information
Mayo Clinic: Tirzepatide Side Effects and Dosage - Patient-focused overview of side effects, precautions, and proper use
Eli Lilly Medical: How Should Tirzepatide Doses Be Increased - Manufacturer guidance on dose escalation from the company behind Mounjaro
PubMed Central: SURMOUNT-MAINTAIN Trial Design - Research on maintaining weight loss after initial tirzepatide treatment
Understanding tirzepatide dosing in units is not complicated once you know the formula and have the right charts. The relationship between milligrams, milliliters, and syringe units follows a consistent, predictable pattern. Whether you are using tirzepatide, exploring lipo-C peptide, or working with any injectable peptide on the market, the same conversion principles apply. Concentration determines everything. The formula, (Dose in mg / Concentration in mg per mL) x 100, works for every concentration, every dose level, and every syringe size. Print the conversion chart for your specific concentration. Check the vial label before every draw. Use the right syringe for your volume. And never let habit override recalculation when you open a new vial with a different concentration.
Your weight loss journey with tirzepatide is deeply personal. The clinical data provides a roadmap, but your body will write its own version of that story. Some people achieve extraordinary results at 5mg. Others need 15mg. Some breeze through dose escalation. Others need extra weeks at every level to manage side effects. All of these paths are valid, and all of them can lead to transformative outcomes when the dosing is precise, the escalation is patient, and the protocol is consistent.
SeekPeptides exists to cut through the confusion surrounding peptide protocols, including the exact kind of unit-to-milligram conversion questions that bring people to articles like this one. Members access personalized protocol guidance, detailed dosing calculators, and a research library that covers every compound discussed in this guide and dozens more. Whether you are starting your first tirzepatide injection or optimizing an existing protocol, the tools and knowledge at SeekPeptides make the process clearer, safer, and more effective.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your doses stay precise, and your progress stay consistent.