Feb 9, 2026

You are wasting semaglutide. Right now. With every injection.
That is not an exaggeration. The FDA has received over 520 adverse event reports tied to compounded semaglutide, and a staggering number of those cases trace back to one root cause: dosing errors. Patients have injected five to twenty times their intended dose because they confused units, milligrams, and milliliters. Some ended up in the hospital. Others burned through an entire vial in a single week when it should have lasted a month. The difference between a correct dose and a dangerous overdose, when working with a 5mg/ml concentration, can be as small as a few tiny lines on a syringe. Understanding your semaglutide dosage calculator conversions is not optional. It is essential.
This guide exists because the margin for error is razor thin. A 5mg/ml vial of semaglutide concentrates twice the medication into the same volume as a 2.5mg/ml vial. That means the units you draw look completely different even though the milligram dose stays the same. Draw the same number of units from both concentrations and you have just doubled your dose. The math matters. The chart matters. Reading your syringe correctly matters more than almost anything else in your protocol.
What follows is the most comprehensive semaglutide 5mg/ml dosage chart available anywhere. Every conversion. Every escalation step. Every syringe marking explained. You will learn the universal formula that works for any concentration, see exactly how 5mg/ml compares to other strengths, understand the standard dose escalation schedule from 0.25mg all the way to 2.4mg, and discover the specific mistakes that send people to the emergency room. SeekPeptides built this resource because accurate dosing should never be a guessing game, and because the consequences of getting it wrong are too serious to ignore.
Understanding semaglutide 5mg/ml concentration
Before you touch a syringe, you need to understand what 5mg/ml actually means. It is not a dose. It is a concentration. Five milligrams of semaglutide are dissolved in every single milliliter of liquid in your vial. This number tells you how much medication exists per unit of volume, and it is the foundation of every calculation you will ever make with this peptide.
Think of it like coffee. A double espresso and a regular coffee might both be served in the same size cup, but the double has twice the caffeine per sip. Semaglutide works the same way. A 5mg/ml vial holds twice the medication per milliliter compared to a 2.5mg/ml formulation. The liquid looks identical. The volume you draw looks identical. But the actual dose is double. This is precisely where dangerous mistakes happen, and it is why the dosage calculation process demands your full attention.
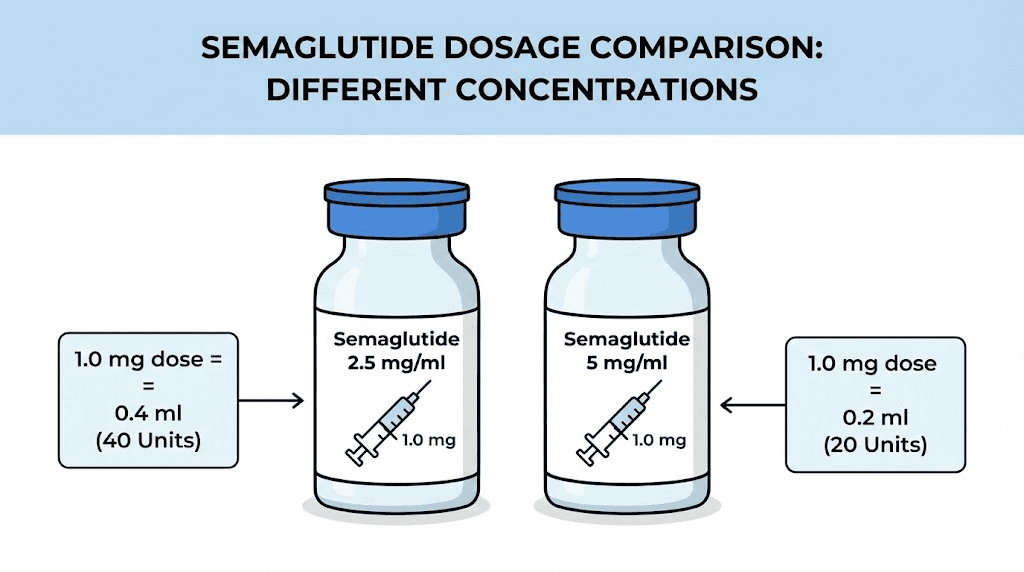
Compounded semaglutide vials come in several concentrations. The most common include 1mg/ml, 2mg/ml, 2.5mg/ml, 3mg/ml, and 5mg/ml. Each concentration requires completely different unit calculations for the same milligram dose. A 0.5mg dose from a 2.5mg/ml vial requires 20 units on your syringe. That same 0.5mg dose from a 5mg/ml vial requires only 10 units. Draw 20 units from the 5mg/ml vial thinking you are getting 0.5mg and you have just given yourself 1mg, double what you intended.
This matters enormously.
Your concentration determines everything about how you read your syringe, how many units you draw, how long your vial lasts, and whether your dose escalation follows the safe, gradual path it needs to follow. Every single conversion in this guide is specific to the 5mg/ml concentration. If your vial says anything other than 5mg/ml on the label, these numbers will not apply to you, and using them could put you at serious risk. Always verify your concentration before calculating anything. The peptide calculator can help you confirm your numbers regardless of which concentration you are working with.
How 5mg/ml vials are typically supplied
Most compounding pharmacies supply semaglutide at 5mg/ml in either 2ml or 3ml multi-dose vials. A 2ml vial at 5mg/ml contains 10mg total of semaglutide. A 3ml vial contains 15mg total. The total milligrams in the vial determine how many weeks of doses you can draw before needing a new vial, and this calculation changes depending on where you are in your dose escalation schedule.
At the starting dose of 0.25mg per week, a 10mg vial contains 40 weekly doses. That is nearly ten months of medication from a single vial. At the maintenance dose of 2.4mg per week, that same 10mg vial lasts just over four weeks. The difference is dramatic, and understanding it helps you plan your costs and ordering schedule accurately.
Some providers also supply semaglutide with vitamin B12 added to the formulation. These combination vials follow the same concentration math for the semaglutide component, but you should always confirm the stated concentration with your provider before drawing any dose. The label is your truth. Nothing else.
The complete semaglutide 5mg/ml dosage chart
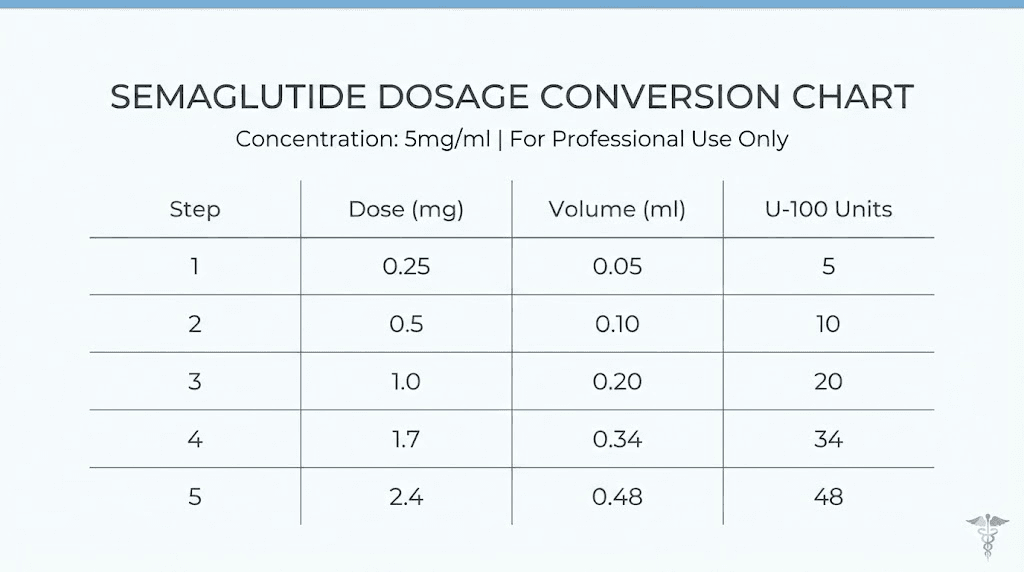
This is the chart you came here for. Print it. Save it. Tape it to your refrigerator. Reference it every single time you prepare an injection until the numbers become second nature. For a 5mg/ml concentration, here is every standard dose converted to both milliliters and insulin syringe units.
Dose (mg) | Volume (mL) | Insulin syringe units | Escalation phase |
|---|---|---|---|
0.25mg | 0.05mL | 5 units | Weeks 1-4 (starting) |
0.5mg | 0.10mL | 10 units | Weeks 5-8 |
0.75mg | 0.15mL | 15 units | Optional intermediate |
1.0mg | 0.20mL | 20 units | Weeks 9-12 |
1.25mg | 0.25mL | 25 units | Optional intermediate |
1.5mg | 0.30mL | 30 units | Optional intermediate |
1.7mg | 0.34mL | 34 units | Weeks 13-16 |
2.0mg | 0.40mL | 40 units | Optional intermediate |
2.4mg | 0.48mL | 48 units | Week 17+ (maintenance) |
2.5mg | 0.50mL | 50 units | Extended (if prescribed) |
Every number in this chart follows a single, consistent formula. There are no exceptions. There are no special cases. The math is clean and predictable because the 5mg/ml concentration divides evenly into standard insulin syringe markings. That mathematical simplicity is one reason many providers prefer this concentration for patients who self-administer.
Notice that every 0.25mg increase equals exactly 5 additional units on your syringe. This pattern makes it easy to verify your calculation mentally. If you know your current dose in units, adding or subtracting 5 units changes your dose by exactly 0.25mg. This consistent relationship between milligrams and units is something you should commit to memory, because it serves as a built-in error check every time you draw a dose. You can also verify this using the units to milligrams conversion guide or the 20 units conversion reference.
Reading the chart correctly
Column one shows your prescribed dose in milligrams. This is what your provider tells you to take. Column two shows how many milliliters of liquid that dose equals at the 5mg/ml concentration. Column three translates that volume into insulin syringe units, which is what you actually read on the syringe when drawing your dose. Column four shows where each dose falls in the standard escalation timeline.
Here is a critical point that trips people up. The "units" on an insulin syringe are not milligrams. They are not universal medication units. They are simply volume markers. One hundred units on a standard insulin syringe equals exactly one milliliter. That is the entire relationship. Units are volume, not dose. Your dose in milligrams depends entirely on how concentrated the liquid is. This is why the same number of units from different concentration vials gives you completely different doses, and why the peptide dosage chart you reference must match your specific concentration.
If your provider prescribes 1mg of semaglutide and your vial is 5mg/ml, you need 20 units. Period. Not 100 units. Not 10 units. Twenty.
The universal conversion formula
Charts are useful. Understanding the math behind the chart is better. Once you know the formula, you can calculate any dose from any concentration without needing to look anything up. The formula is simple, and it works every time.
Dose in units = (Dose in mg / Concentration in mg/mL) x 100
That is it. Three numbers. One division. One multiplication. Let me walk through several examples so the math becomes automatic. The complete guide to peptide dosage calculations covers this formula in depth for all peptides, but here it applies specifically to semaglutide.
Example 1: starting dose of 0.25mg from 5mg/ml
Plug in the numbers. Dose is 0.25mg. Concentration is 5mg/ml.
0.25 / 5 = 0.05
0.05 x 100 = 5 units
Draw to the 5-unit mark on your insulin syringe. Done.
Example 2: escalation dose of 1.0mg from 5mg/ml
1.0 / 5 = 0.20
0.20 x 100 = 20 units
Draw to the 20-unit mark. Straightforward.
Example 3: maintenance dose of 2.4mg from 5mg/ml
2.4 / 5 = 0.48
0.48 x 100 = 48 units
Draw to the 48-unit mark. This is almost half a milliliter, which means you are drawing nearly half the syringe on a standard 1ml insulin syringe. If that number surprises you, it should reinforce why starting at just 5 units matters so much for building tolerance gradually.
Example 4: the same dose from a different concentration
This is where the formula proves its power. Say you switch from a 5mg/ml vial to a 2.5mg/ml vial but your prescribed dose stays at 1.0mg.
1.0 / 2.5 = 0.40
0.40 x 100 = 40 units
Same dose. Double the units. If you drew 20 units from the 2.5mg/ml vial thinking the math was the same as your old 5mg/ml vial, you would only get 0.5mg instead of 1.0mg. You would wonder why the medication stopped working. And if you went the other direction, drawing 40 units from a 5mg/ml vial, you would inject 2.0mg, double your intended dose. Both scenarios are common, and both are preventable with this formula. The peptide reconstitution calculator handles these conversions automatically if you prefer a digital verification step.
Why 100 appears in the formula
The number 100 is in the formula because standard insulin syringes are calibrated at 100 units per milliliter. When you divide your dose by the concentration, you get the volume in milliliters. Multiplying by 100 converts that volume to syringe units. If you ever use a different type of syringe with different calibration, this multiplier would change. But for the standard U-100 insulin syringes that virtually everyone uses for semaglutide, 100 is always the number.
Comparing 5mg/ml vs 2.5mg/ml vs other concentrations
Switching between concentrations is one of the most dangerous moments in a semaglutide protocol. Your provider might change your concentration when you refill. Your pharmacy might reformulate. You might switch providers entirely. Whatever the reason, understanding how the same dose looks different across concentrations can prevent a serious error.
Dose (mg) | Units at 1mg/ml | Units at 2.5mg/ml | Units at 3mg/ml | Units at 5mg/ml |
|---|---|---|---|---|
0.25mg | 25 units | 10 units | 8.3 units | 5 units |
0.5mg | 50 units | 20 units | 16.7 units | 10 units |
1.0mg | 100 units | 40 units | 33.3 units | 20 units |
1.7mg | N/A (exceeds syringe) | 68 units | 56.7 units | 34 units |
2.4mg | N/A (exceeds syringe) | 96 units | 80 units | 48 units |
Study this table carefully. The pattern is clear. Higher concentrations mean fewer units for the same dose. Lower concentrations mean more units. A 1mg/ml concentration requires a full syringe just for a 1.0mg dose, and higher doses literally do not fit in a standard 1ml syringe. This is one reason the 5mg/ml concentration exists, because it keeps even the highest maintenance doses well within the capacity of a standard syringe.
The 5mg/ml concentration also produces cleaner numbers. Look at the 3mg/ml column. Those decimals, 8.3, 16.7, 33.3, are harder to measure precisely on a syringe. The 5mg/ml concentration gives you whole numbers or simple halves at every standard dose level. That precision advantage reduces the chance of measurement errors and is one of the practical reasons many dosing guides recommend it.
What happens when you switch concentrations
Here is a real scenario that plays out constantly. Someone has been taking 1.0mg of semaglutide weekly from a 2.5mg/ml vial. They draw 40 units every week. Their vial runs out and their new vial arrives labeled 5mg/ml. Out of habit, they draw 40 units again.
They just injected 2.0mg. Double their dose.
The nausea hits within hours. Vomiting follows. Some people experience severe abdominal pain. In the worst cases, acute pancreatitis can develop. All because the number on the syringe looked the same, but the concentration behind that number had changed. This exact scenario accounts for a large portion of the adverse events the FDA has documented.
The fix is simple but it requires discipline. Every single time you open a new vial, read the concentration on the label. Recalculate your units using the formula. Cross-reference with the chart. Never assume your new vial matches your old one. A few seconds of verification is all that separates a safe injection from a trip to the emergency room.
Standard dose escalation schedule for weight loss
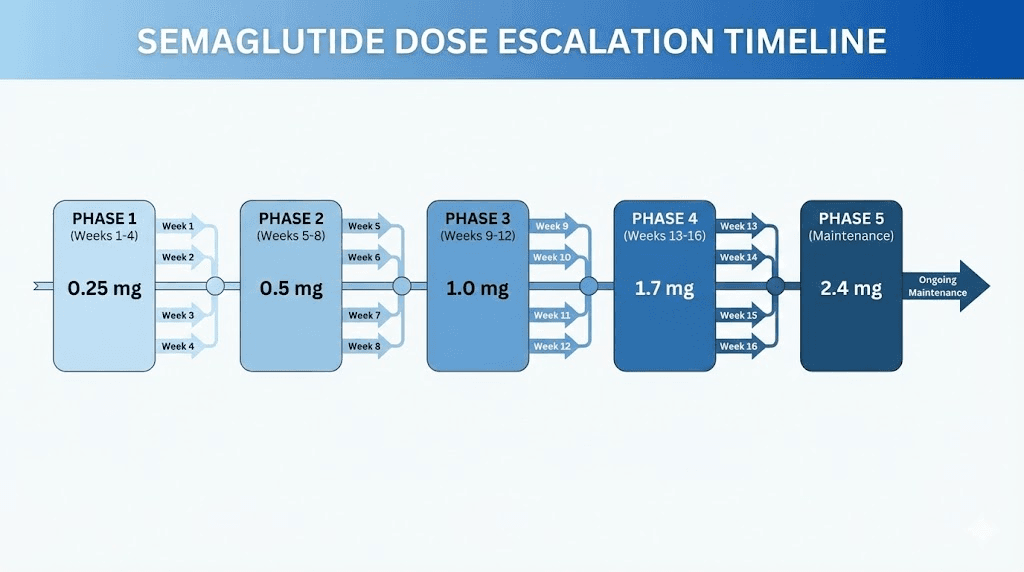
Semaglutide does not start at its full dose. It cannot. The gastrointestinal side effects at higher doses are too significant for most people to tolerate without a gradual buildup period. The standard escalation protocol increases your dose in stages over 16 to 20 weeks, giving your body time to adapt to each level before moving to the next. Understanding where you are in this schedule, and what your corresponding units should be at 5mg/ml, is critical for both safety and effectiveness.
Phase | Weeks | Dose (mg) | Units at 5mg/ml | Purpose |
|---|---|---|---|---|
Phase 1 | 1-4 | 0.25mg | 5 units | GI adaptation, tolerance building |
Phase 2 | 5-8 | 0.5mg | 10 units | Initial appetite reduction begins |
Phase 3 | 9-12 | 1.0mg | 20 units | Noticeable appetite suppression |
Phase 4 | 13-16 | 1.7mg | 34 units | Significant weight loss acceleration |
Phase 5 | 17+ | 2.4mg | 48 units | Maximum therapeutic dose |
Each phase lasts a minimum of four weeks. That is not arbitrary. It takes approximately four to five weeks of consistent weekly dosing for semaglutide to reach what researchers call steady-state concentration in your bloodstream. You need to experience the full effect of each dose before deciding whether escalation is appropriate. Jumping ahead means you have not given the current dose enough time to show what it can do, and you are inviting side effects you could have avoided. The timeline for semaglutide effects explains this pharmacokinetic reality in detail.
Phase 1: the 0.25mg starting dose (5 units)
Do not expect weight loss during this phase. That is not what these four weeks are for. Phase 1 exists to let your gastrointestinal system adjust to a GLP-1 receptor agonist. Some people feel a slight reduction in appetite. Others notice nothing at all. Both responses are normal. The important thing is that you are giving your GI tract time to accommodate the medication before you increase it.
At 5 units on the syringe, this is a tiny volume. You will barely see the liquid in the barrel. That is correct. It is supposed to be small. Resist the temptation to draw more just because it looks like nothing. Five units at 5mg/ml is exactly 0.25mg, and that is exactly where you need to start.
Phase 2: stepping up to 0.5mg (10 units)
After four weeks at 0.25mg, the standard protocol doubles the dose to 0.5mg. On your syringe, this means drawing to the 10-unit mark. Many people begin noticing appetite suppression during this phase. The medication is starting to interact with your GLP-1 receptors at a therapeutically meaningful level, and the food noise that many people describe, that constant background hum of thinking about eating, often begins to quiet.
Gastrointestinal side effects are most likely to appear at this stage. Mild nausea after eating is common. It typically fades within one to two weeks as your body adjusts. If nausea is manageable, stay the course. If it is severe enough to interfere with daily functioning, some providers recommend extending Phase 2 by an additional two to four weeks rather than escalating on schedule.
Phase 3: the 1.0mg therapeutic threshold (20 units)
One milligram is where most people begin to see meaningful changes on the scale. Clinical trials consistently show that significant weight loss begins at this dose level and above. At 20 units on your 5mg/ml syringe, you are now drawing a volume that is clearly visible in the barrel, which makes measurement somewhat easier than the tiny volumes of the earlier phases.
This is also the dose used for type 2 diabetes management under the Ozempic brand, and it represents the point where semaglutide is working at full therapeutic strength for blood sugar control. For weight loss specifically, additional escalation beyond 1.0mg provides additional benefit, but 1.0mg is the floor of effective dosing for most people. Some individuals achieve satisfactory results here and do not need to escalate further. If you are not seeing results at this dose, the linked guide explores common reasons and solutions.
Phase 4: the 1.7mg acceleration dose (34 units)
The jump from 1.0mg to 1.7mg is the largest single escalation in the standard protocol, a 0.7mg increase compared to the 0.25mg and 0.5mg jumps earlier. This is where many providers pay closest attention to side effect tolerance. The 34-unit draw at 5mg/ml puts you at a dose that produces substantial appetite suppression and notable metabolic effects. Many people report that this dose feels qualitatively different from the lower tiers.
Weight loss acceleration at 1.7mg is typically measurable. In clinical trials, participants at this dose level showed significantly greater weight reduction compared to those who remained at 1.0mg. The trade-off is a higher incidence of gastrointestinal side effects. Nausea affects roughly 30 to 35 percent of people at this level, compared to about 15 percent at 0.5mg. The difference in side effect burden is real, and it is the primary reason the escalation process exists rather than starting everyone at the target dose.
Phase 5: the 2.4mg maintenance dose (48 units)
This is the maximum FDA-approved dose of semaglutide for weight management, the dose used in the pivotal STEP clinical trials that demonstrated an average of 15 to 17 percent body weight reduction. At 48 units on your 5mg/ml syringe, you are drawing nearly half a milliliter. The clinical data at this dose is robust. The side effects at this dose are also the most pronounced, with nausea affecting approximately 44 percent of participants in trials.
Not everyone needs to reach 2.4mg. Some people achieve their weight loss goals at 1.0mg or 1.7mg and see no reason to increase further. Others reach 2.4mg and find the side effects too burdensome, stepping back down to 1.7mg for a better balance between efficacy and tolerability. The escalation schedule is a guide, not a mandate. Your provider should help you find the dose that works for your body, your goals, and your tolerance. For a broader perspective on how long to stay on semaglutide and when to adjust, that resource provides detailed guidance.
Optional intermediate doses
The chart above includes several "optional intermediate" doses at 0.75mg, 1.25mg, 1.5mg, and 2.0mg. These exist because not everyone tolerates the standard escalation jumps well. If the increase from 0.5mg to 1.0mg triggers significant nausea, stepping to 0.75mg first can ease the transition. Similarly, the large jump from 1.0mg to 1.7mg can be split into 1.25mg followed by 1.5mg followed by 1.7mg for people with sensitive gastrointestinal systems.
The beauty of the 5mg/ml concentration is that these intermediate doses all land on clean syringe markings. 0.75mg is exactly 15 units. 1.25mg is exactly 25 units.
No fractional units, no trying to estimate between lines. Every 5-unit increment gives you a precise 0.25mg step, which provides maximum flexibility for customizing your escalation speed.
How to read an insulin syringe for semaglutide
The syringe is your measuring instrument. If you cannot read it accurately, nothing else in this guide matters. Most people using compounded semaglutide from vials use standard U-100 insulin syringes, and understanding the markings on these syringes is a skill that takes five minutes to learn but can prevent months of dosing errors.
Syringe sizes and their markings
U-100 insulin syringes come in three standard volumes. Each one has different line spacing, which affects how precisely you can measure small doses.
The 0.3ml syringe (30-unit capacity) has the finest markings. Each small line represents half a unit. This syringe is ideal for the early escalation phases when you are drawing 5 to 15 units. The lines are spread far apart relative to the volume, making it easy to see exactly where you are. The downside is that it cannot hold more than 30 units, so once you escalate past 1.5mg (30 units at 5mg/ml), you need a larger syringe.
The 0.5ml syringe (50-unit capacity) is the most versatile option for a 5mg/ml protocol. It covers every dose from the starting 0.25mg (5 units) all the way to 2.5mg (50 units). Each small line typically represents one unit. This is the syringe most providers recommend for the full escalation journey because it handles every dose level without needing to switch sizes.
The 1.0ml syringe (100-unit capacity) provides the most room, but the markings are closer together, making precise measurement harder at low volumes. For doses under 20 units, the lines can feel cramped and difficult to distinguish. This syringe works fine for maintenance doses of 34 to 48 units, but it introduces unnecessary measurement difficulty at starting doses. For general injection guidance including syringe selection, that resource covers the full landscape.
Reading the markings step by step
Hold the syringe at eye level with the needle pointing up. The plunger sits at the bottom. The numbers printed on the barrel increase from bottom to top. The top of the rubber plunger (the edge closest to the needle) is your measurement line. That edge is where you read your dose.
On a 0.5ml syringe, you will see numbers printed at 5, 10, 15, 20, 25, 30, 35, 40, 45, and 50. Between each numbered line are smaller lines representing individual units. To draw 5 units, pull the plunger down until the top edge of the rubber aligns exactly with the 5 marking. For 10 units, align with the 10 marking. And so on.
For the 34-unit dose at Phase 4, you need to count four small lines past the 30 marking. For the 48-unit dose at Phase 5, count three small lines below the 50 marking (since you are counting down from the top). These odd-numbered draws require more attention than the round-number doses, but with a 0.5ml syringe, each line represents exactly one unit, so counting is straightforward.
Air bubbles distort your reading. Always tap the syringe with the needle pointing up and push any bubbles out before measuring. Even a small bubble occupies space in the barrel that displaces medication, which means your actual dose is less than what the plunger position suggests. This is a common source of under-dosing that people rarely consider. The common peptide mistakes guide covers this and several other easily avoidable errors.
Step-by-step injection guide for semaglutide 5mg/ml
Knowing your dose is half the equation. Administering it correctly is the other half. Semaglutide is a subcutaneous injection, meaning it goes into the fat layer just beneath the skin. Not into muscle. Not into a vein. Into fat. The technique is simple, but each step matters for consistent absorption and minimal discomfort.
Before you begin
Wash your hands with soap and warm water for at least twenty seconds. Dry them with a clean towel. Remove the vial from the refrigerator and check the label. Confirm the concentration reads 5mg/ml. Check the expiration date. Inspect the liquid for particles or discoloration. Clear, colorless liquid is what you want. Anything cloudy, colored, or containing visible particles means the medication should not be used. Understanding expiration guidelines helps you avoid using degraded medication.
Wipe the rubber stopper on the vial with an alcohol swab. Let it air dry. Do not blow on it.
Drawing the dose
Remove the cap from your insulin syringe. Pull the plunger back to your target unit number, drawing air into the syringe equal to the volume you intend to withdraw. For a 10-unit dose, pull back to 10. Insert the needle through the rubber stopper of the vial. Push the air in. This equalizes pressure inside the vial and makes drawing the liquid easier.
Turn the vial upside down with the syringe still inserted. Make sure the needle tip is submerged in the liquid. Pull the plunger back slowly and steadily to your target marking. Watch for air bubbles forming in the barrel. If you see any, tap the barrel firmly with your fingernail until the bubbles rise to the top, then push the plunger gently to expel them. Re-draw to your target marking if needed.
Double-check the plunger position against your dose chart. At 5mg/ml, your numbers should match exactly. Five units for 0.25mg. Ten for 0.5mg. Twenty for 1.0mg. Remove the syringe from the vial.
Selecting and preparing the injection site
Three areas of the body are appropriate for subcutaneous semaglutide injections. The abdomen is the most common site, at least two inches away from the navel in any direction. The front of the thigh is the second option. The back of the upper arm is the third, though this site is harder to reach without assistance.
Rotate your injection site every week. If you injected into the left side of your abdomen last week, use the right side this week. Or switch to your thigh. Consistent rotation prevents the development of lipodystrophy, a condition where the fat layer at the injection site becomes lumpy or hardened from repeated use, which can affect how the medication absorbs. Understanding peptide injections in general, including site rotation strategies, prevents this common problem.
Clean the chosen injection site with a fresh alcohol swab. Use a circular motion, starting at the center and moving outward. Let the alcohol dry completely before proceeding. Injecting into wet alcohol stings.
Performing the injection
Pinch a fold of skin at the injection site between your thumb and forefinger. This lifts the fat layer away from the muscle beneath it. Hold the syringe like a pencil or a dart in your dominant hand. Position the needle at a 90-degree angle to the skin surface. If you are very lean with minimal subcutaneous fat, a 45-degree angle may be more appropriate to ensure the medication reaches the fat layer rather than the muscle.
Insert the needle quickly and smoothly in one motion. Hesitation makes it hurt more. Once the needle is fully inserted, release the skin fold. Slowly depress the plunger over two to three seconds. Do not rush. Rapid injection can cause localized pain and may affect absorption consistency. When the plunger reaches the bottom, pause for five to ten seconds before withdrawing the needle. This allows the full dose to disperse into the tissue.
Withdraw the needle at the same angle you inserted it. Apply gentle pressure to the site with a clean gauze pad or cotton ball for a few seconds. Do not rub the area. Rubbing can cause bruising and may spread the medication outside the intended injection zone.
Dispose of the used syringe immediately in a sharps container. Never recap the needle. Never reuse syringes. Never throw sharps in the regular trash. For a comprehensive walkthrough of injection technique with visual references, the peptide injection guide provides additional detail. You may also want to explore whether a peptide injection pen suits your needs better than traditional syringe-and-vial preparation.
Timing and schedule
Semaglutide is administered once weekly. Choose the same day each week. The time of day does not matter. You can inject in the morning, afternoon, or evening. You can inject with food in your stomach or on an empty stomach. The medication is not affected by meal timing. What matters is consistency, same day, every week, without skipping. If you miss your scheduled day, inject as soon as you remember as long as it is within five days of the missed dose. If more than five days have passed, skip that dose and return to your regular schedule.
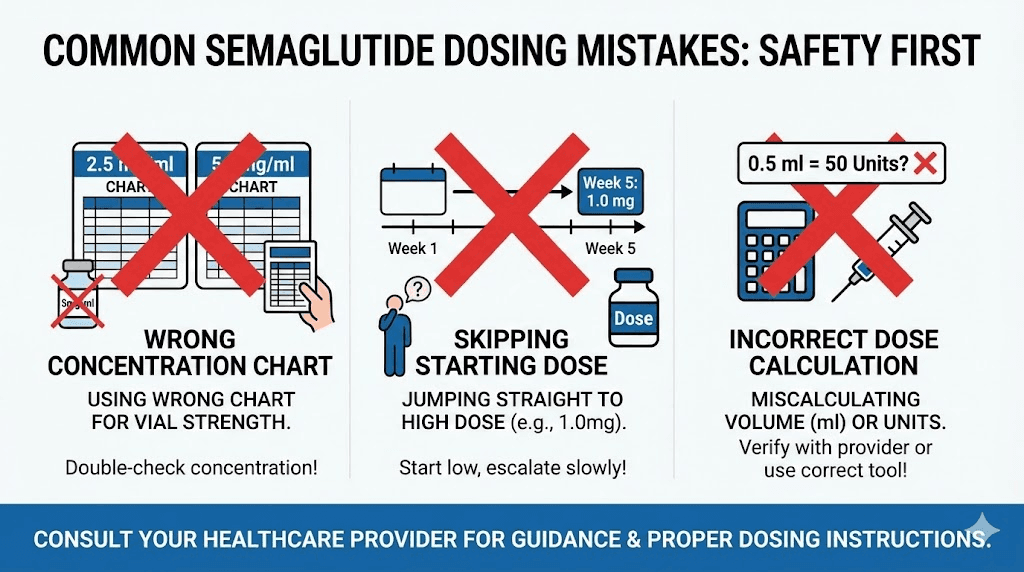
Common dosing mistakes and how to avoid them
The FDA does not issue safety alerts casually. When they documented over 520 adverse events tied to compounded semaglutide, they identified specific patterns of errors that keep repeating. Each one is preventable. Every single one. But you have to know what they are before you can avoid them.
Mistake 1: using the wrong concentration chart
This is the single most dangerous and most common error. A patient gets a 5mg/ml vial but uses a chart written for 2.5mg/ml. Or they switch pharmacies, receive a different concentration than before, and keep drawing the same number of units out of habit. The result ranges from getting half the intended dose (ineffective, frustrating) to getting double the intended dose (nauseating, potentially dangerous).
The prevention is absolute: match your chart to your label. Read the concentration printed on your vial before every single injection. Not once. Every time. The semaglutide dosage calculator eliminates this risk by requiring you to input your specific concentration before generating unit values.
Mistake 2: confusing units, milligrams, and milliliters
These three measurements are related but not interchangeable. Milligrams measure the weight of the active medication. Milliliters measure the volume of liquid. Units are syringe markings that correspond to volume. At 5mg/ml, 1 unit equals 0.01ml equals 0.05mg. But at 2.5mg/ml, 1 unit equals 0.01ml equals 0.025mg. The volume per unit stays the same. The milligrams per unit change with concentration. This distinction is not intuitive, and it confuses even experienced practitioners.
If your provider says "take 0.5mg," you need to calculate the units yourself based on your concentration. If they say "draw 10 units," you should verify that 10 units at your specific concentration equals the milligram dose they intend. Never assume. Always verify. The guide on converting 40 units to mg walks through this specific calculation in detail.
Mistake 3: skipping the starting dose
Some people look at the 0.25mg starting dose, correctly identify that it is not a therapeutically significant dose for weight loss, and decide to start at 1.0mg or higher. This is a recipe for severe gastrointestinal distress. The starting phases exist to train your GI system. Skipping them does not save time. It often costs time, because the resulting nausea and vomiting can be severe enough to put the entire protocol on hold for weeks.
Start at 5 units. Always. Even if you have used semaglutide before and are restarting after a break of more than a few weeks. Your GI tolerance resets. The beginner guide to peptides reinforces why gradual introduction matters for all peptides, not just semaglutide.
Mistake 4: escalating too quickly
The four-week minimum at each dose level is not a suggestion. It reflects the pharmacokinetic reality of semaglutide, which has a half-life of approximately one week. It takes four to five weekly doses to reach steady-state blood levels at any given dose. If you escalate after two weeks, you have not experienced the full effect of the lower dose. You might tolerate the escalation fine. Or you might hit steady state at the higher dose two weeks later and suddenly experience debilitating nausea that would not have occurred with proper timing.
Patience during escalation is not conservative. It is strategic. And it is the approach that clinical trials used to produce the weight loss numbers that everyone references. For perspective on how long semaglutide takes to work, that guide manages expectations around the timeline.
Mistake 5: not removing air bubbles
A bubble in the syringe is not dangerous. Tiny amounts of air injected subcutaneously are harmless. But the bubble does affect your dose accuracy. Every unit of space occupied by air is a unit not occupied by medication. A 3-unit air bubble in a 10-unit draw means you are actually injecting only 7 units of medication, or 0.35mg instead of 0.5mg. Over weeks of consistent under-dosing due to bubbles, you might conclude that semaglutide is not working for you when the real problem is that you have never been taking the full dose.
Mistake 6: reusing or sharing syringes
This should be obvious, but it happens more than it should. Insulin syringes are single-use devices. The needle dulls after one use, the lubricant coating degrades, and the sterility is compromised. Reusing a syringe increases injection pain, infection risk, and the chance of contaminating your vial with bacteria from your skin. The peptide safety and risks guide covers contamination prevention in comprehensive detail. New syringe, every time. No exceptions.
Side effects at each dose level
Side effects are not random. They follow a predictable pattern that correlates directly with dose level. Understanding what to expect at each stage of escalation helps you distinguish between normal adaptation and signals that something is wrong. It also helps you make informed decisions about whether to continue escalating, hold at your current dose, or step back down.
Side effects at 0.25mg (5 units)
Most people experience nothing at this dose. A slight decrease in appetite is possible but not universal. Mild constipation or loose stools may occur as the GLP-1 receptors in your gut begin responding to the medication. These effects are typically minor enough that many people wonder whether the medication is working at all. It is. The low dose is doing its job, priming your system for what comes next.
Side effects at 0.5mg (10 units)
This is where gastrointestinal side effects typically make their first noticeable appearance. Approximately 16 percent of people experience nausea at this dose level. The nausea tends to be mild, often described as a queasy feeling that comes and goes rather than constant sickness. It is usually worst in the first few days after injection and fades as the week progresses. Eating smaller meals, avoiding high-fat foods, and staying hydrated help manage it.
Some people also notice increased burping, mild heartburn, or a feeling of fullness that arrives earlier than usual during meals. These are GLP-1 effects on gastric motility, the medication slows how quickly your stomach empties, which is part of how it reduces appetite.
Side effects at 1.0mg (20 units)
Nausea incidence rises to about 20 percent at this dose. The character of the nausea may change from occasional queasiness to a more persistent feeling, especially in the 24 to 48 hours following injection. Constipation becomes more common. Some people experience headaches during the first week or two at this dose level, which typically resolve as the body adjusts.
This is also the dose where some people first notice changes in their relationship with food beyond simple appetite reduction. Specific food aversions can develop, often toward fatty, greasy, or very sweet foods. These aversions are not concerning. They are a reflection of the medication changing how your gut and brain communicate about food preferences. The peptides for weight loss overview discusses these GLP-1 mediated changes across the broader class of weight management peptides.
Side effects at 1.7mg (34 units)
The jump from 1.0mg to 1.7mg is the escalation phase where the most new side effects tend to appear. Nausea affects 30 to 35 percent of people at this level. Vomiting, which is uncommon at lower doses, begins to affect approximately 10 percent of users. Diarrhea or constipation may intensify. Some people experience injection site reactions, small red bumps or mild itching at the injection location, that were not present at lower doses.
Fatigue is sometimes reported during the first two weeks at this dose, though it is difficult to determine whether this is a direct effect of the medication or a consequence of significantly reduced caloric intake. When you are eating substantially less food than your body is accustomed to, energy levels can dip regardless of medication effects.
Side effects at 2.4mg (48 units)
The full maintenance dose produces the highest incidence of side effects. Clinical trial data shows nausea in approximately 44 percent of participants, vomiting in about 24 percent, diarrhea in 30 percent, and constipation in 24 percent. These numbers are higher than at any previous dose level. However, they also represent peak incidence, and most people find that their GI system adapts over the first four to eight weeks at the maintenance dose.
More serious but less common side effects to watch for at this dose include acute pancreatitis (symptoms: severe abdominal pain radiating to the back, nausea, vomiting), gallbladder problems (symptoms: sudden pain in the upper right abdomen, fever, jaundice), and significant hypoglycemia if combined with certain diabetes medications. These are medical emergencies. If you experience any of these, stop the medication and contact your healthcare provider immediately. Understanding the broader landscape of peptide safety considerations provides context for recognizing warning signs across all peptide types. Some individuals also report concerns about hair thinning during GLP-1 treatment, which that guide explores in depth.
Managing side effects without abandoning the protocol
Nausea is the side effect that causes the most people to quit semaglutide, and in many cases, it is manageable with straightforward adjustments. Eat smaller meals. Five small meals per day often works better than three large ones. Avoid foods high in fat, as fat slows gastric emptying and semaglutide already slows gastric emptying, meaning the combination can create prolonged discomfort.
Ginger helps. Studies support its anti-nausea properties, and many semaglutide users find that ginger tea, ginger chews, or ginger capsules taken 30 minutes before meals reduce queasiness noticeably. Stay well hydrated, but avoid drinking large volumes of liquid with meals, which exacerbates the fullness sensation. Peppermint tea is another option that some find soothing.
Do not lie down immediately after eating. An upright position allows gravity to assist with gastric emptying, which reduces the bloated, overly full feeling that triggers nausea. Walking gently after meals can also help.
If side effects at a new dose are severe, discuss a temporary dose reduction with your provider. Dropping back to the previous dose for two to four weeks and then attempting the escalation again often works. The body sometimes needs a second attempt to tolerate a given dose level, and there is no penalty for taking the escalation more slowly than the standard schedule suggests. The goal is to reach an effective dose that you can sustain long-term, not to rush to 2.4mg at the cost of misery.
Storage and handling for 5mg/ml vials
Proper storage directly affects potency. Semaglutide is a peptide. Peptides degrade when exposed to heat, light, or contamination. A vial that has lost potency due to poor storage will look identical to a fresh one, but the medication inside may be partially or completely inactive. You would never know from looking at it. You would only know because your results stopped or your side effects disappeared, both signs that the active compound has broken down.
Refrigeration requirements
Store semaglutide vials at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). This is standard refrigerator temperature. Place the vial toward the back of the refrigerator where temperature is most stable, not in the door where it swings through temperature changes every time the door opens. The compounded semaglutide fridge life guide covers ideal storage conditions in more detail.
Never freeze semaglutide. Freezing and thawing can cause the peptide to aggregate and lose its structure, potentially rendering it inactive or altering its absorption characteristics. If your vial accidentally freezes, discard it. The potential loss of one vial is less costly than weeks of injecting inactive medication without knowing it.
How long does a 5mg/ml vial last once opened?
Once you puncture the rubber stopper with a needle for the first time, the clock starts. Most compounding pharmacies assign a beyond-use date of 28 to 42 days for opened semaglutide vials stored in the refrigerator. This varies by compounder and by the specific preservative system used. Check your vial label or paperwork for the specific beyond-use date assigned to your product.
Write the date you first used the vial on the label with a marker. This simple habit prevents you from losing track and using a vial past its assigned dating. The peptide fridge storage timeline and the comprehensive peptide storage guide provide additional context on shelf life expectations for various peptide types.
Protecting from light
Semaglutide is light-sensitive. Ultraviolet radiation and even bright ambient light can accelerate degradation. Keep the vial in its original box if one was provided, or store it in an opaque bag or container within the refrigerator. Do not leave the vial sitting on a countertop in a sunny kitchen while you prepare your injection. Take it out, draw your dose, and put it back. The entire process should take less than five minutes.
Travel considerations
Semaglutide must stay cold during travel. Use an insulated cooler bag with ice packs, but add a barrier (a small towel or paper towels) between the ice packs and the vial to prevent accidental freezing. Many pharmacies sell small medical travel cases designed for this exact purpose. Do not leave the medication in a hot car, in checked luggage in an unheated cargo hold during winter, or in direct sunlight during transport. The room temperature stability guide explains how quickly peptides degrade outside of refrigeration, which informs how urgently you need to get your medication back to a cold environment during travel.
For understanding how semaglutide compares to other storage-sensitive peptides, the reconstituted peptide shelf life resource provides a useful reference point. Additionally, the peptide expiration guide covers what happens chemically as peptides degrade over time.
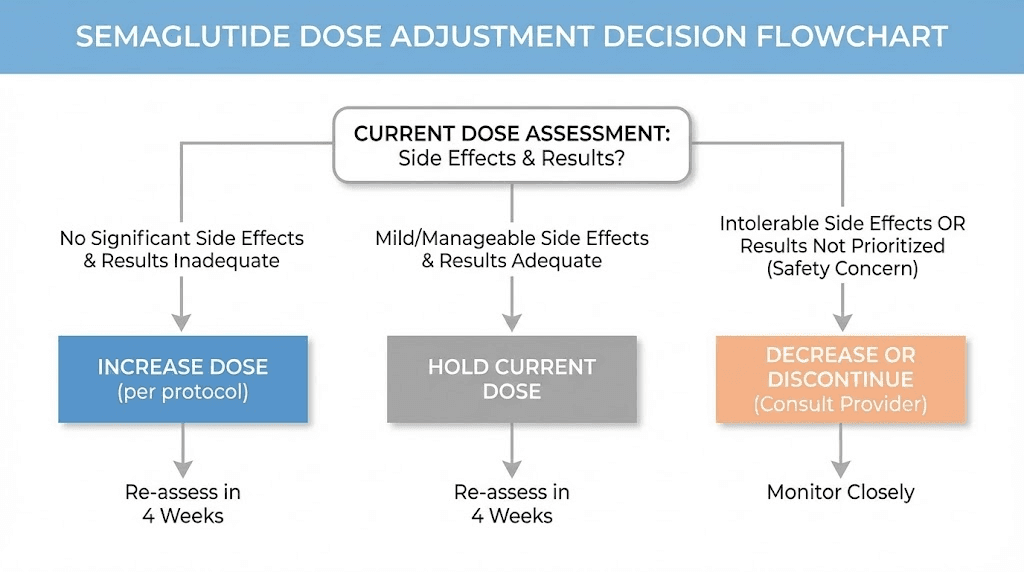
When to adjust your dose
The dose escalation schedule provides a framework. Real-world use rarely follows a framework perfectly. Bodies respond differently. Goals shift. Side effects vary. Knowing when and how to adjust your dose, whether that means holding, increasing, decreasing, or stopping, is an essential skill for anyone on a semaglutide protocol.
Holding at a lower dose
You do not have to reach 2.4mg. If you are losing weight steadily at 1.0mg or 1.7mg with manageable side effects, there is no clinical mandate to escalate further. The target dose is the lowest dose that produces satisfactory results, not necessarily the highest dose available. Some providers advocate staying at the lowest effective dose to preserve room for future escalation if weight loss plateaus later. This conservative approach has merit because it keeps a higher dose in reserve as a strategic tool.
If you have achieved your weight loss goal entirely, the conversation shifts from dose escalation to dose maintenance, which is a different discussion that involves your provider and depends on individual factors like metabolic rate, dietary habits, and whether the weight remains stable at a reduced dose. The peptide cycle planning guide discusses maintenance strategies across various peptide protocols.
Dose reduction for side effects
If a dose increase triggers side effects that do not improve after two to three weeks, stepping back down to the previous dose is the standard approach. Stay there for four to eight weeks. Then try the escalation again. Many people tolerate a dose on the second attempt that their body rejected the first time. This is because each additional week on semaglutide gives your GLP-1 receptors more time to adapt, and adaptation is cumulative even at lower doses.
Plateaus and when to escalate
A plateau is typically defined as less than one percent of body weight lost over a four to six week period while adhering to the protocol. If you plateau at a sub-maximal dose, escalation is the logical next step. But first, verify that the plateau is real and not caused by other factors: water retention, increased muscle mass from exercise, dietary drift, or inconsistent injection timing.
The troubleshooting guide for semaglutide weight loss stalls covers the full diagnostic process for identifying what is actually causing a plateau before assuming the dose needs to increase.
Switching from another GLP-1 to semaglutide
If you are transitioning from tirzepatide to semaglutide, or from another GLP-1 agonist, the dose equivalencies are not straightforward one-to-one conversions. Semaglutide and tirzepatide have different receptor binding profiles, different potencies, and different side effect patterns. Your provider needs to determine an appropriate starting dose for semaglutide based on your previous medication, how long you have been on it, and your individual tolerance. Do not attempt to self-calculate a cross-medication dose conversion without professional guidance. The semaglutide versus tirzepatide dosage comparison explores the clinical differences between these two compounds in depth.
What to do if you accidentally overdose
If you realize immediately after injection that you drew more than intended, there is nothing you can do to remove the medication. It has been injected. What you should do is monitor yourself closely for severe symptoms, specifically severe nausea, persistent vomiting, abdominal pain, signs of dehydration, or confusion. Mild to moderate nausea following an accidental overdose, while unpleasant, is usually self-limiting. Stay hydrated. Eat bland foods in very small amounts if you can tolerate them. Rest.
If you experience severe or persistent vomiting that prevents you from keeping fluids down, severe abdominal pain, or any symptoms that feel like more than standard GI distress, contact your healthcare provider or go to the emergency room. Semaglutide overdoses can, in rare cases, trigger acute pancreatitis, which is a medical emergency. The FDA adverse event data confirms that hospitalizations have occurred from dosing errors, predominantly in the five-to-twenty-times-intended-dose range.
Skip your next scheduled dose to allow the excess medication to clear your system, then resume at your intended dose. Do not reduce your next dose to "compensate." Just skip it entirely and restart on your normal schedule.
How your semaglutide 5mg/ml protocol fits into the bigger picture
Semaglutide is one compound within a broader landscape of peptides and GLP-1 receptor agonists. Understanding where it sits relative to other options helps you evaluate whether your current protocol is optimized and whether alternative or complementary approaches might enhance your results.
The GLP-1 agonist category now includes multiple compounds beyond semaglutide. Tirzepatide, which acts on both GLP-1 and GIP receptors, has shown even greater average weight loss in head-to-head trials. The tirzepatide dose chart follows a different escalation structure that is worth understanding if you are evaluating alternatives. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, represents the next generation, and the retatrutide calculator supports dosing for those exploring that compound. CagriSema, the combination of cagrilintide and semaglutide, is another development showing promise, as detailed in the CagriSema dosing guide.
For weight management specifically, some people combine their GLP-1 protocol with other peptides that support different aspects of the process. The best peptide stacks for weight loss resource explores which combinations have research support and which do not. If you are interested in the broader category of weight loss peptides, that guide covers the full spectrum, including compounds like AOD-9604, tesofensine, 5-amino-1MQ, and lipo-C.
The important context is that semaglutide at 5mg/ml is a concentration, not a treatment plan. Your concentration determines how you measure your dose. Your treatment plan encompasses everything else: which dose you take, when you escalate, how you manage side effects, what supporting habits you build around the medication, and whether complementary compounds add value. SeekPeptides members access comprehensive protocol resources, detailed comparison tools, and expert-reviewed stacking guides that address all of these dimensions.
Reconstitution and mixing for research vials
Some semaglutide arrives as a lyophilized (freeze-dried) powder that must be reconstituted before use. This is different from the pre-mixed liquid vials discussed throughout most of this guide, and the reconstitution process adds a layer of responsibility that directly affects your final concentration. If you receive a 5mg vial of lyophilized semaglutide and add 1ml of bacteriostatic water, you get a 5mg/ml concentration. Add 2ml of water instead, and you get 2.5mg/ml. The volume of water you add determines the concentration, which determines everything about your dosing.
The peptide reconstitution guide covers the full process in detail, including sterile technique, proper water selection, and mixing procedures. For semaglutide specifically, the bacteriostatic water mixing guide explains the precise process. The reconstitution calculator takes the math out of the equation entirely, calculating your final concentration based on the powder amount and water volume you input.
When reconstituting a lyophilized vial, direct the stream of water down the side of the vial, not directly onto the powder. Let it dissolve gently. Do not shake. Swirl the vial slowly if needed. Aggressive shaking can damage the peptide structure and reduce potency. Once dissolved, the solution should be clear and colorless. Any cloudiness or particles indicate a problem, and the vial should not be used. The guide on selecting the right water for peptide mixing explains why bacteriostatic water is preferred over sterile water for multi-dose vials and how the preservative in bacteriostatic water protects against contamination during repeated needle punctures.
Once reconstituted, store the vial in the refrigerator immediately and follow the same 28-to-42-day beyond-use dating that applies to pre-mixed vials. Lyophilized peptides in their dry, unmixed form have a much longer shelf life. The powder-form peptide longevity guide covers how long they remain stable before reconstitution.
Microdosing and non-standard protocols
Not everyone follows the standard escalation to 2.4mg. Microdosing semaglutide, using doses below the standard therapeutic range, has gained attention as an approach for people who want modest appetite suppression with minimal side effects. Doses of 0.125mg (2.5 units at 5mg/ml) or even 0.0625mg (1.25 units) fall well below the standard starting dose but have anecdotal support in some communities.
Clinical data on semaglutide microdosing is limited. The pivotal trials tested 0.25mg as the lowest dose, and even that was considered a non-therapeutic escalation dose. Anything below 0.25mg has not been studied in rigorous trials for weight management outcomes. That does not mean it does not work for some people. It means the evidence base is thin, and expectations should be calibrated accordingly.
For comparison, microdosing tirzepatide has its own chart and dedicated following. The principle is similar: lower doses, fewer side effects, potentially slower but more comfortable weight loss. Whether microdosing any GLP-1 agonist produces clinically meaningful results remains an open question in the research literature.
Some practitioners also use semaglutide in combination protocols, pairing it with B12 injections, peptide stacks, or other compounds. The guide on combining multiple peptides discusses safety considerations, timing, and practical logistics for multi-compound protocols. Whether you cycle different peptides sequentially or run them concurrently affects both the protocol design and the results you can expect.
Alternative delivery methods
While the 5mg/ml vial-and-syringe method is the focus of this guide, semaglutide is also available in other formats that have their own dosing considerations. Ozempic and Wegovy are pre-filled injection pens that eliminate the concentration math entirely, as the pen dial selects the dose in milligrams directly. These branded products remove the unit-conversion step but are significantly more expensive than compounded vials and less flexible for non-standard dosing.
Oral semaglutide (Rybelsus) uses completely different doses, up to 14mg daily, because oral bioavailability is dramatically lower than injectable. The oral and injectable doses are not interchangeable, and the milligram numbers between them are not comparable. The injectable versus oral peptides comparison explains the bioavailability differences that drive these dose discrepancies.
Newer delivery methods under development include GLP-1 transdermal patches, which would bypass injection entirely, and oral tirzepatide formulations. Sublingual peptide delivery and nasal spray formulations represent additional alternative routes being explored across the peptide category, and peptide capsules offer yet another non-injection approach. For now, injectable vials remain the most widely used and most cost-effective form of compounded semaglutide, which is why mastering the 5mg/ml dosage chart is so important for anyone using this specific format.
Understanding the legal and sourcing landscape
Compounded semaglutide exists in a regulatory space that every user should understand. The peptide legality guide covers the current regulatory framework in detail. Compounded medications are legal when prescribed by a licensed provider and dispensed by a licensed compounding pharmacy. They are not FDA-approved products, meaning they have not undergone the same approval process as brand-name Ozempic or Wegovy, but they are legal when handled through proper medical channels.
The grey market peptide landscape is different. Research-labeled peptides sold without prescriptions occupy a legal grey area that varies by jurisdiction, and quality control for these products is not standardized. If you are sourcing semaglutide, the vendor evaluation guide helps you assess quality indicators. Understanding the difference between research-grade and pharmaceutical-grade peptides informs purchasing decisions that directly affect both safety and efficacy.
Cost is a practical consideration. The peptide therapy cost breakdown covers what to expect across different sourcing routes. Compounded semaglutide typically costs a fraction of the branded alternatives, which is a significant driver of its popularity. The general peptide cost guide provides broader context on pricing across the peptide category. For those exploring medically supervised options, the online peptide therapy guide reviews telehealth platforms that provide prescriptions and clinical oversight.
Regulatory developments in this space are ongoing. The peptide regulation news resource tracks changes that may affect availability and legality. Staying informed is not optional when using compounded medications, because the rules can change with relatively little notice.
Tracking your progress and results
A dosage chart tells you what to inject. A tracking system tells you whether it is working. Without systematic tracking, you are guessing about your protocol effectiveness, and guessing leads to premature dose changes, unnecessary escalation, and abandoned protocols that might have worked with more patience.
Track these metrics weekly at minimum: body weight (same time, same conditions, preferably morning before eating), waist circumference, how you feel subjectively (energy, hunger, mood), any side effects and their severity, and your injection details (date, time, dose, site). The before and after results resource shows what realistic timelines look like and helps calibrate expectations. The peptide transformation guide provides frameworks for evaluating progress beyond just the scale number.
Weight fluctuates daily. Do not make dose decisions based on a single weigh-in. Look at trends over weeks. A consistent downward trend of 0.5 to 1.5 percent of body weight per week while on a therapeutic dose is a typical range. Faster than that is aggressive but possible at higher doses. Slower than that may indicate a need for dose adjustment, dietary evaluation, or investigation of other factors.
SeekPeptides provides tracking tools, progress frameworks, and evidence-based protocol guides that help members interpret their data and make informed decisions about their semaglutide journey. For a broader understanding of how results develop with peptides generally, the how peptides work resource explains the biological mechanisms behind the changes you observe.
Gender-specific considerations
While semaglutide works through the same mechanism in all bodies, there are practical differences in how men and women tend to respond and what considerations apply to each group. The standard dose escalation schedule applies to both, and the 5mg/ml concentration chart does not change based on gender. However, the context around dosing can differ.
Women tend to experience more gastrointestinal side effects at each dose level in clinical trial data, though the difference is not large enough to warrant a different escalation schedule. Hormonal fluctuations throughout the menstrual cycle can affect how side effects manifest, with some women reporting that nausea is more pronounced during certain phases of their cycle. The peptides for weight loss in women guide addresses these nuances specifically. The best peptides for women resource takes a broader view across the peptide category.
Men generally have higher body weight at baseline, which means the same milligram dose represents a lower dose per kilogram of body weight. Some providers account for this by escalating more aggressively or targeting higher maintenance doses in heavier individuals, regardless of gender. The fat burning peptides for men guide and the comprehensive peptides for men resource cover male-specific protocol considerations.
The weight-loss-specific peptide calculator can help adjust calculations based on individual factors, and the visceral fat loss guide discusses how different peptides target the specific fat deposits that matter most for metabolic health in both men and women. The broader peptides for fat loss resource page aggregates the most relevant information across all approaches.
Working with your healthcare provider
A dosage chart is a reference tool. It is not a substitute for medical supervision. Semaglutide is a prescription medication that interacts with your endocrine system, your gastrointestinal function, and potentially with other medications you take. The chart tells you how many units correspond to how many milligrams at 5mg/ml. Your provider tells you which milligrams are right for you, when to escalate, when to hold, and when to stop.
Bring your dosage chart to appointments. Show your provider exactly what you are drawing and how you are calculating it. Ask them to verify your numbers. This takes thirty seconds and provides a safety check that catches errors before they become adverse events. If your provider prescribed your dose in milligrams, confirm the unit conversion together. If they prescribed in units, confirm which concentration those units assume.
Report side effects honestly. Do not minimize them to avoid having your dose reduced. Do not exaggerate them to get attention. Accurate reporting helps your provider make decisions that optimize your outcome. The peptide vial research guide provides context on what to look for when assessing your medication source, and the complete peptide list gives both you and your provider a reference for the broader category of compounds available.
For those navigating the peptide space for the first time, SeekPeptides offers a structured starting point with its getting started guide and personalized protocol building tools. Whether you are researching semaglutide dosing for the first time or refining an existing protocol, having both a reliable dosage chart and informed clinical guidance makes the difference between a protocol that works and one that wastes time, money, and medication.
Frequently asked questions
How many units is 0.25mg of semaglutide at 5mg/ml?
At a 5mg/ml concentration, 0.25mg equals 5 units on a standard U-100 insulin syringe. This is the standard starting dose during the first four weeks of escalation. The calculation is straightforward: 0.25 divided by 5 equals 0.05ml, multiplied by 100 equals 5 units. Use the semaglutide dosage calculator to verify this conversion for your specific vial.
How many units is 1mg of semaglutide at 5mg/ml?
One milligram of semaglutide from a 5mg/ml vial equals 20 units. This is the Phase 3 dose typically reached during weeks 9 through 12 of the standard escalation protocol. At this dose level, most people begin experiencing meaningful appetite suppression and weight loss.
What is the difference between 5mg/ml and 2.5mg/ml semaglutide?
The only difference is concentration. A 5mg/ml vial contains twice the medication per milliliter compared to a 2.5mg/ml vial. This means you draw half the volume (half the units) for the same milligram dose. A 0.5mg dose is 10 units at 5mg/ml but 20 units at 2.5mg/ml. The medication itself is the same. The charts are different. Never use a chart from one concentration to dose from a different concentration. The dosage calculation guide explains this principle in depth.
How long does a 5mg vial of semaglutide last?
A 5mg total vial (1ml at 5mg/ml) lasts different amounts of time depending on your dose. At 0.25mg per week, it lasts 20 weeks. At 0.5mg per week, 10 weeks. At 1.0mg per week, 5 weeks. At 2.4mg per week, just over 2 weeks. A 10mg total vial (2ml at 5mg/ml) doubles these numbers. Planning your vial purchases around your current and anticipated dose levels prevents running out. The cost calculator helps estimate expenses across different dose schedules.
Can I use the same syringe for multiple injections?
No. Insulin syringes are designed for single use. The needle dulls after one puncture, increasing pain and tissue damage on subsequent uses. The sterility is compromised after the first use, raising infection risk. The lubricant coating on the needle degrades. Always use a new, sterile syringe for every injection. The peptide safety guide explains why single-use sterile technique is non-negotiable.
What happens if I accidentally inject too much semaglutide?
An accidental overdose of semaglutide typically manifests as severe gastrointestinal symptoms: intense nausea, vomiting, and abdominal pain. For moderate overdoses (two to three times the intended dose), symptoms are usually self-limiting. Stay hydrated, rest, and skip your next scheduled dose. For severe overdoses (five or more times the intended dose), seek medical attention, as there is a risk of acute pancreatitis. The FDA has documented cases of patients injecting five to twenty times their intended dose due to concentration confusion.
Should I inject semaglutide in the morning or evening?
There is no clinical evidence that injection timing affects efficacy. Choose a time that fits your schedule and stick with it for consistency. Some people prefer morning injections because nausea, if it occurs, tends to manifest within a few hours, and they prefer to deal with it during waking hours. Others prefer evening injections so they can sleep through any initial discomfort. Personal preference guides this decision.
Can I take semaglutide with other peptides?
Combining semaglutide with other peptides is a question for your healthcare provider. Some combinations have research support, while others are untested. The guide to taking multiple peptides and the peptide stack calculator help evaluate potential combinations. Never combine medications without clinical guidance.
Why do I feel nothing at the 0.25mg starting dose?
The 0.25mg dose is sub-therapeutic for weight loss. Its purpose is gastrointestinal adaptation, not clinical effect. Feeling nothing at this dose is completely normal and expected. The medication begins producing noticeable effects for most people at 0.5mg to 1.0mg. Do not increase your dose ahead of schedule just because the starting dose feels inactive. The semaglutide onset timeline explains the expected progression.
How do I switch from a 2.5mg/ml vial to a 5mg/ml vial?
When switching concentrations, your milligram dose stays the same. Only your unit draw changes. If you were taking 1.0mg from a 2.5mg/ml vial (40 units), switching to a 5mg/ml vial means drawing 20 units for the same 1.0mg dose. Recalculate every dose level using the formula or the semaglutide calculator. Write down your new numbers before your first injection from the new vial. Triple-check them. This transition point is when most dosing errors occur.
External resources
For researchers serious about optimizing their semaglutide protocols, SeekPeptides provides the most comprehensive resource available, with evidence-based dosing guides, personalized protocol builders, a dedicated semaglutide calculator, and a community of thousands who have navigated these exact dosing questions and escalation decisions.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay verified, your escalations stay gradual, and your calculations stay accurate.