Feb 9, 2026

Drawing 40 units from your tirzepatide vial could mean 2 mg. It could also mean 4 mg. Or 6 mg. Or even 12 mg. The answer changes completely based on one number you absolutely must know before every single injection: your vial concentration.
This is not a minor detail. Getting this wrong means you are either underdosing and wasting weeks waiting for results that will never come, or overdosing and spending the next 48 hours dealing with severe nausea, vomiting, and a trip to the emergency room that could have been avoided entirely. The difference between the right dose and a dangerous mistake comes down to a simple math formula that takes ten seconds once you understand it.
The confusion exists because tirzepatide dosing in units works differently than most medications people encounter. Insulin syringes measure volume in units. But the actual milligrams of tirzepatide in that volume depend entirely on how concentrated your specific vial is. A vial labeled 5 mg/mL contains half the tirzepatide per milliliter compared to a 10 mg/mL vial. So 40 units drawn from each would deliver completely different doses. This guide will walk you through every concentration, every conversion, and the exact formula you need to never second-guess your dose again. Whether you are using branded Mounjaro pens, compounded tirzepatide from a pharmacy, or figuring out your first injection, the math works the same way every time. SeekPeptides created this resource because dosing errors are the most common and most preventable problem in peptide research.
The quick answer: 40 units of tirzepatide in milligrams by concentration
Here is what 40 units equals for every common tirzepatide concentration. Find your vial concentration on the label, then match it below.
Vial concentration | 40 units (0.4 mL) equals | Common use case |
|---|---|---|
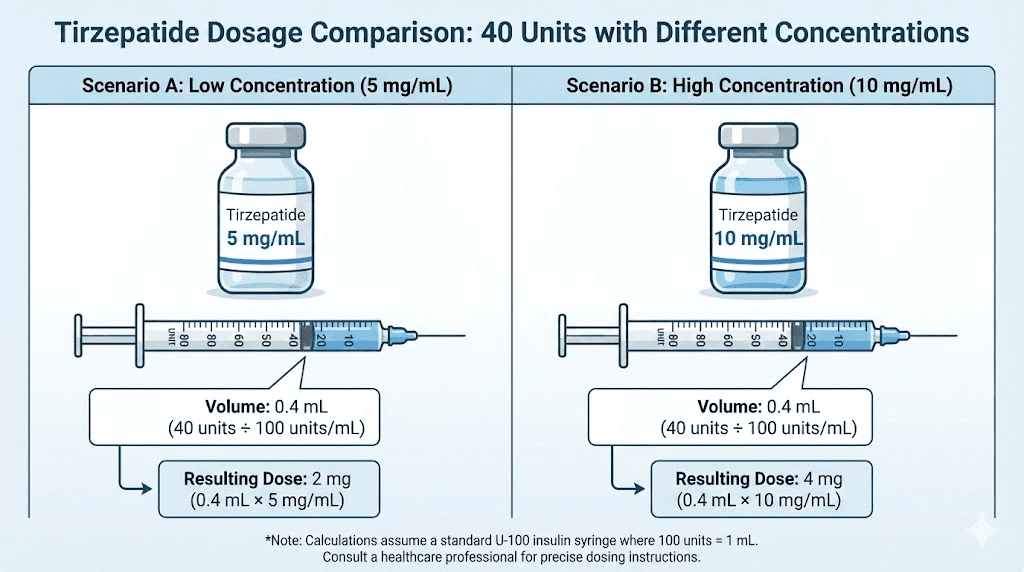
5 mg/mL | 2 mg | Low-concentration compounded vials |
10 mg/mL | 4 mg | Standard compounded tirzepatide |
15 mg/mL | 6 mg | Mid-range compounded vials |
20 mg/mL | 8 mg | High-concentration compounded vials |
30 mg/mL | 12 mg | Ultra-concentrated compounded vials |
That is the short answer. But if you do not understand why these numbers are what they are, you risk making a calculation error the next time your pharmacy sends a different concentration. Keep reading.
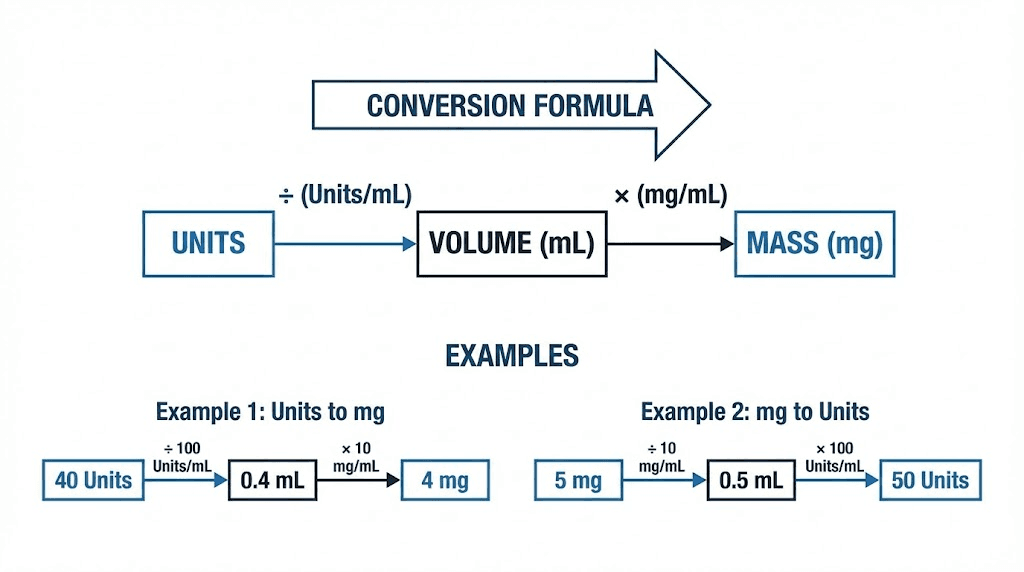
Understanding the conversion formula
Every tirzepatide conversion uses the same three-step formula. Learn it once, use it forever.
Step 1: convert units to milliliters
An insulin syringe measures volume in units. There are 100 units in 1 milliliter. Always. This never changes regardless of what medication is in the syringe. So the conversion is straightforward.
Units divided by 100 = milliliters
For 40 units: 40 / 100 = 0.4 mL
This means when you draw to the 40-unit mark on your insulin syringe, you are pulling exactly 0.4 milliliters of liquid into the syringe. That part is simple.
Step 2: multiply by your vial concentration
Now multiply the volume (in mL) by whatever concentration is printed on your vial label. The concentration tells you how many milligrams of tirzepatide are dissolved in each milliliter of liquid.
Milliliters x concentration (mg/mL) = milligrams of tirzepatide
For 40 units from a 10 mg/mL vial: 0.4 mL x 10 mg/mL = 4 mg
For 40 units from a 20 mg/mL vial: 0.4 mL x 20 mg/mL = 8 mg
Same syringe reading. Double the dose. This is exactly why concentration matters so much.
Step 3: verify against your prescribed dose
Before injecting, compare your calculated milligrams against what your provider prescribed. If your prescription says 5 mg weekly and your calculation shows 4 mg or 8 mg, something is wrong. Go back and check your concentration, recheck the math, and confirm with your provider if needed. The SeekPeptides peptide calculator can help you double-check these conversions instantly.
The complete formula in one line
(Units / 100) x concentration (mg/mL) = dose in milligrams
Or working backwards from a prescribed dose:
(Prescribed mg / concentration) x 100 = units to draw
Both formulas are two sides of the same equation. Memorize either one and you can always figure out the other. This applies to every tirzepatide dosage in units conversion you will ever need.
Complete conversion tables for every concentration
The tables below cover every common unit amount across every standard compounded tirzepatide concentration. Bookmark this section. You will come back to it.
5 mg/mL concentration conversion table
This is the lowest concentration you will typically encounter. It requires drawing more liquid to reach your target dose, which makes it easier to measure small doses precisely. Many providers start patients on 5 mg/mL vials for exactly this reason. The larger injection volumes make fine-tuning easier during the tirzepatide dose escalation phase.
Units on syringe | mL drawn | Dose (mg) at 5 mg/mL |
|---|---|---|
10 units | 0.10 mL | 0.5 mg |
20 units | 0.20 mL | 1.0 mg |
25 units | 0.25 mL | 1.25 mg |
30 units | 0.30 mL | 1.5 mg |
40 units | 0.40 mL | 2.0 mg |
50 units | 0.50 mL | 2.5 mg |
60 units | 0.60 mL | 3.0 mg |
70 units | 0.70 mL | 3.5 mg |
80 units | 0.80 mL | 4.0 mg |
100 units | 1.00 mL | 5.0 mg |
Notice that at 5 mg/mL, reaching even the standard starting dose of 2.5 mg requires drawing 50 units, which is half a milliliter. Higher doses become impractical because you would need more than a full syringe. This is why most people eventually switch to higher concentrations as their dose increases.
10 mg/mL concentration conversion table
The 10 mg/mL concentration is the most commonly prescribed compounded tirzepatide strength. It offers a good balance between manageable injection volumes and the ability to cover the full tirzepatide dosing range without needing extremely small or extremely large draws.
Units on syringe | mL drawn | Dose (mg) at 10 mg/mL |
|---|---|---|
10 units | 0.10 mL | 1.0 mg |
15 units | 0.15 mL | 1.5 mg |
20 units | 0.20 mL | 2.0 mg |
25 units | 0.25 mL | 2.5 mg |
30 units | 0.30 mL | 3.0 mg |
40 units | 0.40 mL | 4.0 mg |
50 units | 0.50 mL | 5.0 mg |
60 units | 0.60 mL | 6.0 mg |
75 units | 0.75 mL | 7.5 mg |
100 units | 1.00 mL | 10.0 mg |
At this concentration, 40 units delivers exactly 4 mg. That is a common intermediate dose during the tirzepatide escalation protocol. The standard starting dose of 2.5 mg requires just 25 units, making it easy to measure accurately with any standard insulin syringe.
15 mg/mL concentration conversion table
Some compounding pharmacies produce 15 mg/mL formulations as a middle ground between standard and high-concentration options. This concentration works well for people on moderate to higher doses who want smaller injection volumes without jumping to 20 mg/mL.
Units on syringe | mL drawn | Dose (mg) at 15 mg/mL |
|---|---|---|
10 units | 0.10 mL | 1.5 mg |
17 units | 0.17 mL | 2.5 mg |
20 units | 0.20 mL | 3.0 mg |
33 units | 0.33 mL | 5.0 mg |
40 units | 0.40 mL | 6.0 mg |
50 units | 0.50 mL | 7.5 mg |
67 units | 0.67 mL | 10.0 mg |
83 units | 0.83 mL | 12.5 mg |
100 units | 1.00 mL | 15.0 mg |
The challenge with 15 mg/mL is that some standard doses fall on odd unit numbers. Drawing exactly 17 units for 2.5 mg is trickier than drawing 25 units from a 10 mg/mL vial. This is not impossible, but it does require more careful measurement and a steady hand. Consider whether precision at lower doses matters more than convenience at higher doses when choosing between concentrations.
20 mg/mL concentration conversion table
High-concentration vials are increasingly common for people on established doses of 7.5 mg and above. The benefit is obvious: smaller injection volumes mean less liquid under the skin, which can reduce injection site reactions and discomfort. The tradeoff is that small measurement errors translate to larger dosing errors. Drawing 5 units too many from a 20 mg/mL vial adds a full extra milligram to your dose. That same 5-unit error with a 10 mg/mL vial only adds 0.5 mg. Keep this in mind as you review the tirzepatide dosage in units chart below.
Units on syringe | mL drawn | Dose (mg) at 20 mg/mL |
|---|---|---|
5 units | 0.05 mL | 1.0 mg |
10 units | 0.10 mL | 2.0 mg |
13 units | 0.13 mL | 2.5 mg |
20 units | 0.20 mL | 4.0 mg |
25 units | 0.25 mL | 5.0 mg |
38 units | 0.38 mL | 7.5 mg |
40 units | 0.40 mL | 8.0 mg |
50 units | 0.50 mL | 10.0 mg |
63 units | 0.63 mL | 12.5 mg |
75 units | 0.75 mL | 15.0 mg |
At 20 mg/mL, 40 units delivers a hefty 8 mg dose. That is more than triple the starting dose. If someone who was previously using a 10 mg/mL vial switches to 20 mg/mL and draws the same 40 units out of habit, they would inject double their intended dose. This exact scenario is one of the most commonly reported dosing errors with compounded tirzepatide.
30 mg/mL concentration conversion table
Ultra-concentrated formulations exist for people on the highest therapeutic doses who want minimal injection volumes. These are less common but worth understanding, especially as dose escalation reaches 10 mg and above. Every unit matters significantly at this concentration.
Units on syringe | mL drawn | Dose (mg) at 30 mg/mL |
|---|---|---|
8 units | 0.08 mL | 2.5 mg |
10 units | 0.10 mL | 3.0 mg |
17 units | 0.17 mL | 5.0 mg |
25 units | 0.25 mL | 7.5 mg |
33 units | 0.33 mL | 10.0 mg |
40 units | 0.40 mL | 12.0 mg |
42 units | 0.42 mL | 12.5 mg |
50 units | 0.50 mL | 15.0 mg |
At 30 mg/mL, 40 units equals 12 mg of tirzepatide. That is near the maximum therapeutic dose. Only people who have been carefully titrated up over many months under medical supervision should be anywhere near this level. The margin for error at this concentration is razor-thin. A 3-unit mistake adds nearly a full milligram to your dose.
Why concentration changes everything
The single most important number on your tirzepatide vial is not the total amount of peptide in the vial. It is the concentration, measured in milligrams per milliliter (mg/mL). This number determines everything about your dosing math.
How concentration works
Think of concentration like mixing a drink. You have a glass of water and a packet of flavoring. If you dissolve one packet in a large glass, each sip is mild. Dissolve the same packet in a shot glass, and each sip is intensely concentrated. The total amount of flavoring is identical. The concentration per sip is completely different.
Tirzepatide works the same way. A vial might contain 50 mg total. But how those 50 mg are distributed across the liquid volume changes the concentration entirely.
50 mg in 5 mL of liquid = 10 mg/mL
50 mg in 2.5 mL of liquid = 20 mg/mL
50 mg in 10 mL of liquid = 5 mg/mL
Same total tirzepatide. Completely different doses per unit drawn. This is why you cannot simply look at the total milligrams in a vial and assume you know how much to draw. The unit-to-milligram relationship depends entirely on concentration.
Branded pens vs. compounded vials
If you use branded Mounjaro or Zepbound pens, you do not need to worry about concentration calculations at all. Each pen delivers a fixed, pre-measured dose. The 2.5 mg pen always delivers 2.5 mg. The 5 mg pen always delivers 5 mg. No math required. No room for error. This is one of the main advantages of branded pens, and it is why the FDA requires them to come in fixed-dose configurations.
Compounded tirzepatide is different. It comes in multi-dose vials where you draw your own dose using an insulin syringe. The concentration varies between compounding pharmacies, between different products from the same pharmacy, and sometimes even between batches. You must check the label on every new vial you receive.
This is not optional. This is not something you can assume.
Every. Single. Vial.
What happens when concentration changes mid-treatment
This scenario catches people constantly. You have been using a 10 mg/mL vial for weeks. Your pharmacy sends your refill. Same medication, same label design, same packaging. But the concentration is now 20 mg/mL. Maybe the pharmacy switched suppliers. Maybe they reformulated. Maybe they simply ran out of the lower concentration.
If you draw the same 50 units you always drew, you just doubled your dose from 5 mg to 10 mg. The side effects at that unexpected dose will be severe. Nausea that lasts days. Vomiting. Dehydration. Fatigue that makes it impossible to function. All because you assumed the concentration was the same as last time.
Always, always recalculate when you open a new vial. Especially if the liquid volume looks different from what you are used to. A half-full vial where you usually see a full one is a clear sign the concentration has changed. You can verify your calculations anytime using the peptide dosage calculator at SeekPeptides.
The tirzepatide dosing schedule and where 40 units fits
Understanding where 40 units falls in the standard tirzepatide protocol helps you verify whether your calculated dose makes sense for your current treatment stage.
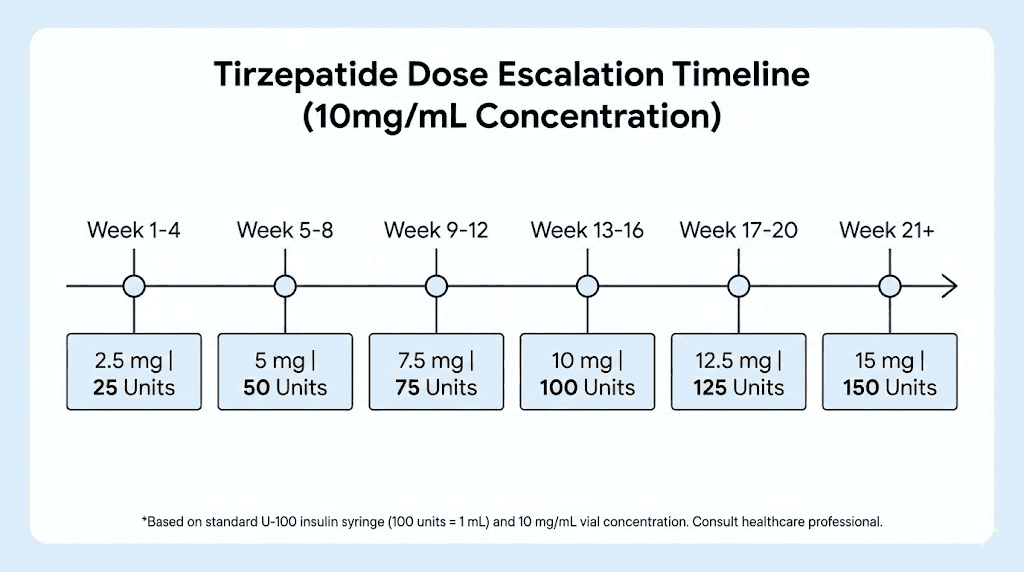
Standard FDA-approved dosing escalation
The FDA-approved tirzepatide dosing schedule, used in the SURMOUNT and SURPASS clinical trials, follows this pattern:
Weeks 1 to 4: 2.5 mg once weekly (starting dose)
Weeks 5 to 8: 5 mg once weekly
Weeks 9 to 12: 7.5 mg once weekly (optional increase)
Weeks 13 to 16: 10 mg once weekly (optional increase)
Weeks 17 to 20: 12.5 mg once weekly (optional increase)
Week 21 and beyond: 15 mg once weekly (maximum dose)
Each dose increase happens after a minimum of four weeks at the current dose. The gradual escalation gives your body time to adjust and reduces gastrointestinal side effects that are most common during dose changes. Jumping doses or increasing too quickly is the primary cause of severe nausea and vomiting that leads people to discontinue treatment entirely.
Where 40 units falls in each concentration
Depending on your vial concentration, 40 units could place you anywhere from an early-stage dose to a near-maximum dose:
Concentration | 40 units = mg | Dosing stage | Typical week range |
|---|---|---|---|
5 mg/mL | 2 mg | Below starting dose (microdosing) | Pre-week 1 or tapering |
10 mg/mL | 4 mg | Between starting and second dose | Transitional dosing |
15 mg/mL | 6 mg | Between second and third dose | Weeks 5 to 12 range |
20 mg/mL | 8 mg | Mid-range therapeutic dose | Weeks 9 to 16 range |
30 mg/mL | 12 mg | High therapeutic dose | Weeks 17+ range |
If your math shows 40 units delivering 12 mg but you are only in your second month of treatment, something is likely wrong. Either the concentration is not what you think it is, or you are about to massively overdose. The microdosing tirzepatide chart can help you understand appropriate dosing for early-stage treatment where lower, more precise doses matter most.
Clinical trial results by dose
The SURMOUNT-1 clinical trial demonstrated clear dose-dependent weight loss results with tirzepatide. Understanding these numbers helps contextualize why accurate dosing matters so much. Higher doses produced better results, but only when reached through proper escalation.
5 mg weekly: Average 16% total body weight reduction over 72 weeks
10 mg weekly: Average 21.4% total body weight reduction
15 mg weekly: Average 22.5% total body weight reduction
Placebo: Average 2.4% reduction
These are remarkable numbers. At the 15 mg dose, over 50% of participants lost at least 20% of their body weight. But these results came from consistent, properly dosed weekly injections over many months. Inconsistent dosing due to calculation errors undermines the entire protocol. Every incorrect dose, whether too high or too low, disrupts the steady-state blood levels that drive these outcomes.
Understanding the relationship between tirzepatide dosing for weight loss in units and actual milligrams delivered is what separates people who get clinical-trial-level results from those who wonder why the medication is not working.
How to read your tirzepatide vial label
The vial label contains every piece of information you need to calculate your dose correctly. But labels vary between manufacturers, and not all information is presented the same way. Here is exactly what to look for.
Finding the concentration
The concentration is typically printed in one of these formats:
mg/mL (most common): "10 mg/mL" means 10 milligrams per milliliter
mg/X mL (sometimes used): "50 mg/5 mL" means the total vial contains 50 mg in 5 mL, which equals 10 mg/mL
Total amount only (rare): "50 mg" with a separate notation of total volume
If the label only shows total milligrams and total volume, divide the total mg by the total mL to get concentration. For example: a vial containing 100 mg in 5 mL has a concentration of 100/5 = 20 mg/mL.
Other critical label information
Beyond concentration, check these details every time you receive a new vial. They affect storage, potency, and how long you can use the vial once opened.
Expiration date: Never use expired medication. Potency degrades over time, meaning your calculated dose may deliver less active tirzepatide than expected. Check the tirzepatide storage and shelf life guide for details on how temperature and time affect potency.
Storage requirements: Most compounded tirzepatide requires refrigeration between 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit). Improper storage degrades the peptide.
Total volume: Knowing the total volume helps you estimate how many doses remain in the vial
Beyond-use date (BUD): Different from the expiration date, this tells you how long the medication remains stable after the pharmacy prepared it
When the label is confusing or unclear
If you cannot determine the concentration from the vial label, do not guess. Call the pharmacy that prepared the vial. Ask them directly: what is the concentration in milligrams per milliliter? Write it on the vial with a marker so you do not have to call again. Store this information somewhere accessible, like a note on your phone, alongside your injection schedule.
Some compounding pharmacies include dosing instructions with the vial. These typically specify the exact number of units to draw for common doses at that specific concentration. If you receive these instructions, follow them. But always verify the math yourself using the formula above. Mistakes happen at pharmacies too, and a quick calculation takes seconds.
Insulin syringes and tirzepatide: what you must know
The syringe itself introduces another layer of potential confusion. Not all insulin syringes are the same, and using the wrong one can throw off your entire dose.
U-100 insulin syringes (standard)
The vast majority of insulin syringes sold in pharmacies are U-100 syringes. This means they are calibrated so that 100 units equals 1 milliliter. When we say "40 units = 0.4 mL," we are assuming a U-100 syringe. This is the correct syringe type for compounded tirzepatide.
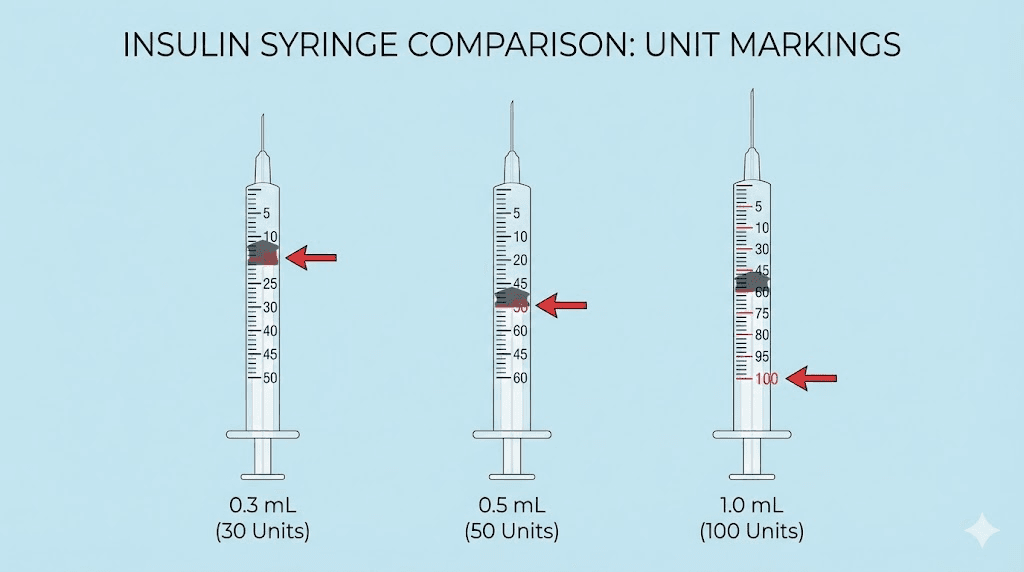
U-100 syringes come in several sizes:
0.3 mL (30 units max): Best for low doses, highest precision for small volumes. Markings are typically in 0.5 or 1-unit increments.
0.5 mL (50 units max): Good middle ground. Works for doses up to 5 mg at 10 mg/mL concentration.
1.0 mL (100 units max): Covers the full dosing range but with less precision for very small doses. Markings are typically in 2-unit increments.
For a 40-unit draw, either the 0.5 mL or 1.0 mL syringe works. The 0.5 mL syringe gives you slightly better precision since the markings are closer together, making it easier to read exactly 40 units. If you are using the smaller unit doses like 20 units, a 0.3 mL syringe provides the most accurate measurement.
U-40 syringes (danger zone)
U-40 syringes exist but are rare in the United States. They are calibrated so that 40 units equals 1 milliliter instead of 0.4 milliliters. If you accidentally used a U-40 syringe for tirzepatide, drawing to the "40 unit" mark would pull 1.0 mL instead of 0.4 mL, giving you 2.5 times the intended dose.
This would be a serious overdose. At 10 mg/mL, you would inject 10 mg instead of 4 mg. At 20 mg/mL, you would inject 20 mg, which is above the maximum therapeutic dose and potentially dangerous.
How to verify: look at the syringe packaging. It should clearly say "U-100" or show 100 units per mL. The barrel itself will have markings going up to 30, 50, or 100 at the 0.3 mL, 0.5 mL, or 1.0 mL marks respectively. If the markings do not match these patterns, you may have the wrong syringe type. When in doubt, ask your pharmacist for a standard U-100 insulin syringe specifically. This applies to all peptide injection protocols, not just tirzepatide.
Needle gauge and length
For subcutaneous tirzepatide injections, the needle gauge and length matter for comfort and proper delivery but do not affect dosing calculations. Common choices include:
29 gauge, 0.5 inch: Standard for most people, good balance of comfort and reliability
30 gauge, 0.5 inch: Thinner needle, slightly less discomfort, slightly harder to draw from vial
31 gauge, 5/16 inch: Thinnest common option, minimal pain, best for lean individuals with less subcutaneous fat
The needle does not change how much liquid you draw. A 40-unit draw is 40 units regardless of needle size. What changes is comfort and how quickly the liquid flows through the needle during injection. Thinner needles are more comfortable but draw medication more slowly. This is purely a comfort preference, not a dosing consideration.
Step-by-step injection guide for 40 units
Once you have confirmed your concentration and calculated your milligram dose, the actual injection process follows the same steps every time. Here is the complete procedure for drawing and administering 40 units of tirzepatide.
Preparation
Gather everything before you start. You need your tirzepatide vial, an appropriately sized insulin syringe (0.5 mL or 1.0 mL for a 40-unit draw), an alcohol swab, and a sharps container for disposal.
Wash your hands thoroughly with soap and water. Dry them completely. Inspect the vial, checking the liquid for unusual cloudiness, particles, or discoloration. Clear and colorless is normal for most compounded tirzepatide. If something looks off, do not use the vial. Contact your pharmacy.
Drawing the medication
Clean the vial rubber stopper with an alcohol swab and let it dry for 10 seconds
Remove the syringe cap without touching the needle
Pull the plunger back to the 40-unit mark, filling the syringe with air
Insert the needle through the rubber stopper into the vial
Push the plunger to inject air into the vial (this equalizes pressure and makes drawing easier)
Turn the vial upside down with the needle still inserted
Pull the plunger back slowly to the 40-unit mark
Check for air bubbles. If you see any, tap the syringe barrel gently to move them to the top, then push the plunger slightly to expel the air. Pull back to 40 units again.
Remove the needle from the vial
Accuracy matters here. Make sure the top of the rubber plunger tip (not the bottom) aligns with the 40-unit marking. Reading from the wrong edge of the plunger is a common source of 1 to 2 unit measurement errors. At high concentrations, even this small discrepancy matters.
Choosing the injection site
Tirzepatide is injected subcutaneously, meaning just under the skin into the fat layer. The three FDA-approved injection sites are:
Abdomen: At least 2 inches from the belly button. Avoid the area directly around the navel.
Front of the thigh: Middle third of the thigh, avoiding the inner thigh
Back of the upper arm: The fatty area on the back, typically requires someone else to administer
Rotate between these sites each week. Do not inject in the same spot consecutively. Repeated injections in one location can cause lipodystrophy, where the fat tissue under the skin becomes lumpy, hard, or discolored. This is not just cosmetic. Damaged tissue absorbs medication differently, leading to inconsistent dosing even when your syringe measurements are perfect. The same principles apply whether you are administering tirzepatide or any other injectable peptide.
Performing the injection
Clean the injection site with an alcohol swab. Let it dry completely. Injecting into wet alcohol stings.
Pinch a fold of skin at the injection site with your non-dominant hand
Hold the syringe at a 90-degree angle to the skin surface
Insert the needle fully into the pinched skin fold in one smooth motion
Release the skin pinch
Push the plunger slowly and steadily until all medication is delivered
Wait 5 to 10 seconds before removing the needle (this prevents medication from leaking back out)
Remove the needle and apply gentle pressure with a clean cotton ball or gauze if needed
Dispose of the syringe in a sharps container immediately
Do not rub the injection site. Do not apply ice beforehand (it can affect absorption). Do not massage the area after. Simply let the medication absorb naturally. Some minor redness, slight burning, or a small bump at the injection site is completely normal and typically resolves within a few hours.
Common dosing mistakes and how to avoid them
These errors happen constantly. Knowing about them before they happen to you is the best defense.
Mistake 1: assuming concentration stays the same between refills
This is the most dangerous error. Your pharmacy sends a new vial. You draw the same units as before without checking the label. But the concentration changed. If it doubled, so did your dose.
Prevention: Check the concentration printed on every single new vial. Write the concentration on a sticky note and attach it to your vial. Compare it to your previous vial before drawing your first dose from the new one.
Mistake 2: confusing total mg with concentration
A vial that says "50 mg" tells you the total tirzepatide in the vial, not the concentration. If that 50 mg is dissolved in 5 mL, the concentration is 10 mg/mL. If it is dissolved in 2.5 mL, it is 20 mg/mL. Same total. Completely different dose per unit.
Prevention: Always look for the mg/mL number specifically. If the label only shows total mg and total volume, divide to calculate concentration yourself before drawing any medication.
Mistake 3: using the wrong syringe
U-40 syringes, tuberculin syringes, and U-100 syringes all have different calibrations. Using anything other than a standard U-100 insulin syringe will result in the wrong volume drawn for your intended unit count.
Prevention: Only use U-100 insulin syringes. Verify by checking the package labeling. The syringe barrel markings should show 100 units at the 1.0 mL mark (or proportional for smaller syringes).
Mistake 4: not accounting for air bubbles
Air bubbles in the syringe displace medication. If you draw to 40 units but there is a 5-unit air bubble trapped in the barrel, you actually have only 35 units of medication. That is 0.5 mg less at a 10 mg/mL concentration.
Prevention: After drawing, hold the syringe needle-up. Tap the barrel to float bubbles to the top. Push the plunger gently until the bubbles exit. Then pull back to your exact target of 40 units and verify no bubbles remain.
Mistake 5: reading the syringe wrong
The plunger has a rubber tip with a slightly conical shape. The top edge and bottom edge of this rubber tip show different readings on the syringe markings. Reading from the wrong edge gives you a 1 to 2 unit error, which matters more with higher concentrations.
Prevention: Always read from the top edge of the rubber plunger tip, where it is closest to the needle. Hold the syringe at eye level. Do not read it from an angle, as this introduces parallax error. These fundamentals apply to every peptide dosage calculation.
Mistake 6: drawing from a cold vial
Tirzepatide is stored in the refrigerator. Cold liquid is more viscous and harder to draw accurately. It also tends to create more air bubbles as it warms in the syringe. This can lead to inaccurate draws and painful injections since cold medication stings more upon injection.
Prevention: Remove the vial from the refrigerator 15 to 20 minutes before your injection. Let it reach room temperature naturally. Do not heat it, microwave it, or place it in hot water, as heat degrades the peptide. Room temperature medication draws more smoothly and injects more comfortably.
What to do if you drew the wrong dose
Mistakes happen. Here is what to do depending on when you catch the error.
Before injecting
If you realize the dose is wrong before the needle goes in, simply push the medication back into the vial and redraw the correct amount. Nothing is wasted, and nothing is harmed. This is the best-case scenario, which is why double-checking before every injection is so important.
After injecting too much
You cannot "un-inject" medication. Once it is in your tissue, it will absorb. Here is what to do:
Small overage (1 to 2 mg over): Monitor for increased nausea, which is the most common dose-related side effect. Stay hydrated. Eat bland, small meals. The effects typically resolve within 24 to 48 hours. Your next dose should be at the correct amount.
Moderate overage (3 to 5 mg over): Contact your healthcare provider. You may experience significant nausea, vomiting, and possibly diarrhea. Have anti-nausea medication on hand if prescribed. Stay hydrated with electrolyte solutions. Your provider may advise skipping the next weekly dose.
Large overage (more than 5 mg over): This is a medical situation. Contact your healthcare provider immediately or go to urgent care. Severe vomiting and dehydration are possible. Do not wait to see how you feel. The side effects from tirzepatide overdose can be debilitating and may require IV fluids.
After injecting too little
If you underdosed, the situation is less urgent but still important to address.
Small underage (1 to 2 mg under): Do not inject additional medication to make up the difference. Simply take your full correct dose at the next scheduled injection. One slightly lower dose will not significantly impact your overall progress.
Large underage (missed most of the dose): Contact your provider. They may advise an additional partial dose within the same day or adjusting the following week dose. Never double-dose without explicit medical guidance.
The safest approach is always to prevent errors in the first place. Use the formula. Check the concentration. Verify the math. And use tools like the peptide calculator to confirm before every injection.
Switching between concentrations: a complete guide
At some point during treatment, most people switch concentrations. Maybe your pharmacy changed suppliers. Maybe you moved to a higher dose that requires less volume. Maybe availability issues forced a switch. Whatever the reason, transitioning between concentrations is where the majority of dosing errors occur.
How to recalculate when concentration changes
Use this process every single time you switch to a new concentration.
Write down your current prescribed dose in milligrams (not units, milligrams)
Note the new vial concentration from the label
Calculate new unit amount: (prescribed mg / new concentration) x 100 = new units to draw
Verify the math: (new units / 100) x new concentration should equal your prescribed dose
Compare to old draw volume: the number of units will be different, but the dose in mg must be the same
Example: You were drawing 50 units from a 10 mg/mL vial (5 mg dose). Your new vial is 20 mg/mL.
New units: (5 mg / 20 mg/mL) x 100 = 25 units
Verification: (25 / 100) x 20 = 5 mg. Correct.
You went from drawing 50 units to drawing 25 units. Same 5 mg dose. If you had drawn 50 units from the new vial out of habit, you would have injected 10 mg instead of 5 mg. Double your dose. This exact mistake is reported frequently in forums, and it is completely avoidable with a 30-second calculation. Understanding this relationship is fundamental to all peptide dosage conversions.
Concentration switch reference table
This table shows how the number of units changes for common prescribed doses across different concentrations. Use this when switching between vials to quickly verify your new draw volume.
Prescribed dose (mg) | Units at 5 mg/mL | Units at 10 mg/mL | Units at 15 mg/mL | Units at 20 mg/mL | Units at 30 mg/mL |
|---|---|---|---|---|---|
2.5 mg | 50 units | 25 units | 17 units | 13 units | 8 units |
5 mg | 100 units | 50 units | 33 units | 25 units | 17 units |
7.5 mg | N/A (150 units) | 75 units | 50 units | 38 units | 25 units |
10 mg | N/A (200 units) | 100 units | 67 units | 50 units | 33 units |
12.5 mg | N/A | N/A (125 units) | 83 units | 63 units | 42 units |
15 mg | N/A | N/A (150 units) | 100 units | 75 units | 50 units |
"N/A" means the required volume exceeds 1.0 mL, which is the maximum capacity of a standard insulin syringe. In these cases, you need a higher concentration vial to administer your prescribed dose in a single injection. Never attempt to split a dose across two injections unless specifically instructed by your provider, as absorption rates and peak blood levels will differ from a single injection.
Tirzepatide and semaglutide: dosing differences
Many people compare tirzepatide to semaglutide, either because they are considering switching or because they want to understand both options. The dosing math works the same way for both medications, but there are important differences worth understanding.
How the unit conversion differs
Both tirzepatide and semaglutide use the same formula: (units / 100) x concentration = milligrams. But the standard dose ranges are completely different. Semaglutide doses range from 0.25 mg to 2.4 mg for weight management. Tirzepatide doses range from 2.5 mg to 15 mg. These are different medications with different potencies and different mechanisms.
If someone tells you "40 units" without specifying which medication, the dose could be anything from less than 1 mg of semaglutide to 12 mg of tirzepatide depending on the drug and concentration. Context matters enormously. This is why understanding semaglutide unit conversions separately from tirzepatide conversions is essential.
The dual mechanism advantage
Tirzepatide works differently from semaglutide at a fundamental level. While semaglutide activates only the GLP-1 receptor, tirzepatide is a dual GIP and GLP-1 receptor agonist. This 39-amino-acid synthetic peptide activates both glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide 1 (GLP-1) receptors simultaneously. The dual action produces enhanced insulin secretion, improved insulin sensitivity, greater appetite suppression, and more potent weight loss compared to GLP-1 activation alone.
In head-to-head clinical trials, tirzepatide at 15 mg outperformed semaglutide at 1 mg for both glycemic control and weight reduction. This superior efficacy is partly why tirzepatide doses are higher in absolute milligrams. The medication simply works through additional pathways that single-receptor agonists cannot access.
Conversion between the two
There is no direct milligram-to-milligram conversion between tirzepatide and semaglutide because they are fundamentally different molecules. Switching from one to the other requires medical supervision and a new titration schedule. If you are considering switching, your provider will determine the appropriate starting dose of the new medication based on your current treatment response, not a mathematical conversion from your current dose. The complete guide to switching from tirzepatide to semaglutide covers this process in detail.
Using the SeekPeptides peptide calculator for tirzepatide
Manual calculations work. But calculators eliminate the possibility of arithmetic errors, which is especially valuable when you are dealing with medications where mistakes have real consequences.
How the calculator works
The SeekPeptides peptide calculator requires three inputs:
The total amount of peptide in your vial (in mg)
The volume of liquid in your vial (in mL)
Your desired dose (in mg)
From these three numbers, it calculates your concentration automatically and tells you exactly how many units to draw on your insulin syringe. No mental math. No opportunity for errors. The peptide reconstitution calculator handles the related calculation of how much bacteriostatic water to add when preparing lyophilized peptides.
When to use a calculator vs. manual math
Use the calculator:
Every time you open a new vial with a different concentration
When you receive a new prescription with a dose change
Anytime the numbers do not feel right or you are second-guessing yourself
When teaching someone else to prepare their injection
Use manual math:
As a verification check on the calculator output
When you do not have internet access
When you have been on the same concentration and dose for so long that the number is memorized
The ideal approach is both. Calculate manually, then verify with the calculator. Or calculate with the tool, then verify the math makes sense. Two methods reaching the same answer means you got it right.
SeekPeptides members access additional dosing tools, including personalized protocol builders that account for individual factors like body weight, treatment stage, and dose history. These go beyond simple unit-to-milligram conversions and help you optimize your entire approach to peptide research.
Special dosing situations
Standard conversions cover most scenarios. But these edge cases come up frequently enough to address specifically.
Microdosing tirzepatide below 2.5 mg
Some providers prescribe below the standard 2.5 mg starting dose for patients who are particularly sensitive to GLP-1 medications or who experienced significant side effects with the standard starting dose. Microdosing at 1 mg, 1.25 mg, or even 0.5 mg is becoming more common as providers recognize that some people need an even more gradual introduction. The microdosing tirzepatide chart covers this approach in detail.
At these low doses, precision matters enormously. Drawing 5 units instead of 10 units from a 10 mg/mL vial means getting 0.5 mg instead of 1 mg. That is a 50% dose error. Use the smallest syringe available (0.3 mL) for the most precise markings at low unit counts.
Splitting a dose across the week
Some providers prescribe split dosing, where the weekly dose is divided into two injections given 3 to 4 days apart. For example, instead of 5 mg once weekly, you might inject 2.5 mg on Monday and 2.5 mg on Thursday. This can help reduce gastrointestinal side effects by avoiding a large single dose peak.
When calculating units for split doses, remember to divide your weekly milligram dose by the number of injections, then calculate units based on that per-injection dose. Do not calculate units for the full weekly dose and then try to divide the liquid volume in the syringe. Calculate milligrams first, then convert to units.
Tirzepatide with additional compounds
Some compounded formulations combine tirzepatide with additional ingredients like vitamin B12, niacinamide, or glycine. The addition of these compounds does not change the tirzepatide concentration or the dosing calculation. The concentration listed on the label refers specifically to the tirzepatide content. Additional ingredients are present in the same liquid volume but do not affect how you calculate your tirzepatide dose.
However, always confirm this with your pharmacy. In rare cases, a pharmacy might list the combined concentration of all active ingredients rather than tirzepatide alone. If the label says something like "tirzepatide 10 mg/B12 1 mg per mL," the 10 mg/mL refers to tirzepatide specifically. But if it says "12 mg/mL total active ingredients," you need to know how much of that 12 mg is tirzepatide.
What about oral tirzepatide?
For people interested in non-injectable forms, oral tirzepatide is in development and follows completely different dosing rules. Oral formulations account for lower bioavailability through the digestive system by using higher total milligram amounts. The unit conversion math in this guide does not apply to oral forms. Oral dosing is measured in milligrams taken by mouth, not units drawn into a syringe.
Tracking your doses over time
Consistent tracking prevents errors and gives your provider the information they need to adjust your protocol effectively.
What to record for every injection
Keep a simple log with these details:
Date and time of injection
Vial concentration (mg/mL)
Units drawn
Calculated milligrams
Injection site (rotate between abdomen, thigh, upper arm)
Side effects (nausea, fatigue, injection site reactions, anything notable)
Weight (if tracking, weigh yourself at the same time each day for consistency)
This log serves multiple purposes. It helps you verify you are drawing the correct amount each week. It gives your provider concrete data to guide dose adjustments. It helps you identify patterns, like whether certain injection sites produce more side effects, or whether increasing from 5 mg to 7.5 mg caused more nausea than the previous increase. All of this information helps optimize your tirzepatide results over time.
When to reassess your dose
Standard protocol reassesses every four weeks before any potential increase. But beyond the escalation phase, here are signs that your dose might need adjustment:
Plateau in weight loss for 3+ weeks: May indicate it is time to increase. But rule out dietary and activity factors first. Check the troubleshooting guide for tirzepatide weight loss stalls before assuming the dose needs to change.
Persistent side effects that are not improving: May indicate the current dose is too high. Dropping back one level and trying a more gradual increase sometimes works better than pushing through discomfort.
Appetite suppression wearing off before next dose: This can indicate the dose is being metabolized faster than average for you, or that a small increase would provide more consistent coverage throughout the week.
Consistently losing more than 1% body weight per week: Rapid weight loss can cause muscle loss, gallstone issues, and nutritional deficiencies. Your provider may slow the escalation or hold at the current dose.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Frequently asked questions
Does 40 units of tirzepatide always equal the same mg?
No. The milligrams in 40 units depend entirely on your vial concentration. At 5 mg/mL, 40 units equals 2 mg. At 10 mg/mL, it equals 4 mg. At 20 mg/mL, it equals 8 mg. Always check your vial label for the concentration before calculating your dose. Use the SeekPeptides peptide calculator to verify.
Can I use any insulin syringe for tirzepatide?
Use only U-100 insulin syringes. These are standard in the United States and calibrated so 100 units equals 1 milliliter. U-40 syringes, which are rare but do exist, have different calibration and would cause a 2.5x overdose if used accidentally. Check the syringe package for the "U-100" designation. The peptide injection guide covers syringe selection in detail.
What happens if I accidentally inject too many units?
A small overage of 1 to 2 mg over your prescribed dose will likely cause increased nausea and fatigue that resolves within 24 to 48 hours. For larger overages of 3 mg or more above your prescribed dose, contact your healthcare provider. Severe overdoses can cause persistent vomiting and dehydration requiring medical attention. Never try to compensate by taking less at your next scheduled dose without medical guidance.
Why did my pharmacy change the concentration of my tirzepatide?
Compounding pharmacies may change concentrations due to supply chain issues with raw ingredients, changes in compounding regulations, switching to a new supplier, or standardizing their product line. Always verify the concentration on each new vial you receive. Treat every refill as potentially different until you confirm the label matches your previous vial.
Is 40 units the same as 0.4 mL?
Yes, when using a standard U-100 insulin syringe, 40 units equals exactly 0.4 milliliters. This relationship is constant regardless of what medication is in the syringe. The medication concentration determines how many milligrams are dissolved in that 0.4 mL, but the volume itself is always 0.4 mL at 40 units.
How do Mounjaro pen doses compare to compounded tirzepatide units?
Mounjaro pens deliver fixed doses (2.5, 5, 7.5, 10, 12.5, or 15 mg) in 0.5 mL each. The pen handles all measurement automatically, so no conversion is needed. With compounded tirzepatide vials, you must calculate units based on your vial concentration to match these same milligram doses. The tirzepatide dose chart shows equivalencies across both formats.
Can I mix different concentration vials together?
No. Never combine medication from different vials, even if they contain the same medication. Mixing vials with different concentrations creates an unknown combined concentration that makes accurate dosing impossible. Use one vial at a time until it is empty, then switch to the next. If switching concentrations, recalculate your unit draw amount completely.
What is the most common tirzepatide concentration?
10 mg/mL is the most widely used concentration for compounded tirzepatide. It offers good precision at starting doses (25 units for 2.5 mg) while still allowing doses up to 10 mg within a single 1 mL syringe capacity. Higher concentrations like 20 mg/mL are growing in popularity for patients on established higher doses.
External resources
SURMOUNT-1 clinical trial results (New England Journal of Medicine)
Tirzepatide dual GIP/GLP-1 receptor agonist mechanism of action (PubMed)
In case I do not see you, good afternoon, good evening, and good night. May your calculations stay accurate, your concentrations stay verified, and your results stay consistent.