Dec 29, 2025

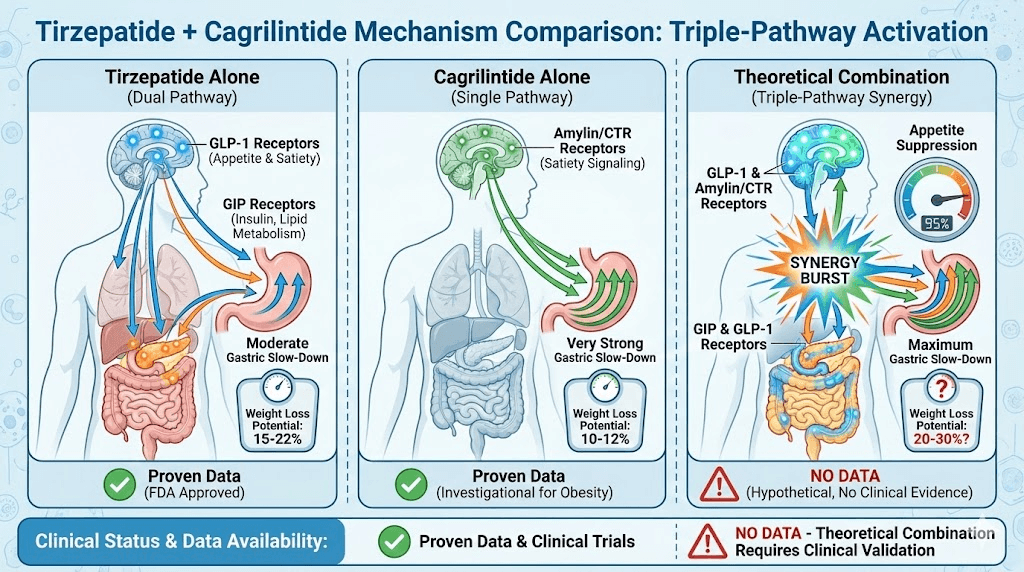
The weight loss peptide landscape just got more complex. Tirzepatide (Mounjaro/Zepbound) already delivers 15-22% body weight loss through dual GIP/GLP-1 receptor activation - making it one of the most powerful single-agent options available.
Meanwhile, cagrilintide produces 10-12% weight loss via a completely different amylin pathway.
The obvious question: what happens when you combine them?
Unlike the well-studied CagriSema combination (cagrilintide + semaglutide) with proven 15-25% weight loss results from Phase 3 trials, adding cagrilintide to tirzepatide remains completely unstudied. No clinical trials. No published protocols. No safety data. Just theoretical potential based on complementary mechanisms and a growing number of biohackers experimenting on themselves.
Combining cagrilintide with tirzepatide could theoretically produce 20-30% body weight loss by targeting three distinct pathways (GIP, GLP-1, and amylin), but the lack of clinical data means dosing protocols are speculative, side effect profiles unknown, and safety unclear.
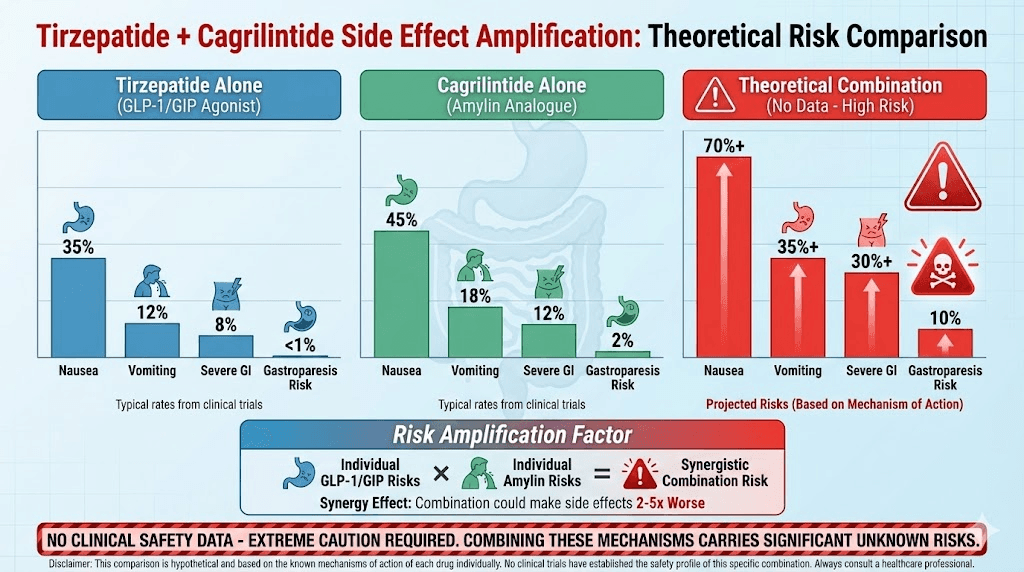
Tirzepatide's powerful gastric emptying effects combined with cagrilintide's even stronger gastric slowing could create severe GI complications.
Cost also becomes prohibitive at $1,200-2,400 monthly for both research peptides.
This guide examines theoretical cagrilintide dosage protocols when combined with tirzepatide, potential synergies and risks, conservative vs aggressive dosing strategies, comparing this combination to proven alternatives (CagriSema, tirzepatide monotherapy), who might consider this experimental approach, and safer evidence-based options that deliver comparable results.
Let's start by understanding why this combination is tempting but problematic.
Why combine cagrilintide with tirzepatide: theoretical rationale
The mechanistic case for synergy exists on paper.
Tirzepatide's dual receptor mechanism
How tirzepatide works:
Dual GIP/GLP-1 receptor agonist
Single molecule, two pathways
GIP (glucose-dependent insulinotropic polypeptide) + GLP-1
Weekly subcutaneous injection
FDA approved for diabetes and obesity
GIP pathway effects:
Enhances insulin secretion
Improves insulin sensitivity
Promotes fat metabolism
Reduces inflammation
Works synergistically with GLP-1
GLP-1 pathway effects:
Suppresses appetite (central brain effects)
Slows gastric emptying (moderate)
Increases satiety
Reduces glucagon
Improves glucose control
Combined tirzepatide results:
15-22% average body weight loss (monotherapy)
Superior to semaglutide (GLP-1 alone)
Well-tolerated in trials
Approved and available
See our tirzepatide dosing guide, semaglutide vs tirzepatide, and peptides for weight loss at SeekPeptides.
Cagrilintide's amylin mechanism (different pathway)
How cagrilintide works:
Amylin receptor agonist
Long-acting weekly injection
Investigational (not FDA approved)
Different receptors than GIP/GLP-1
Amylin pathway effects:
Very strong gastric emptying delay (stronger than GLP-1)
Central appetite suppression (area postrema)
Reduces meal frequency
Suppresses glucagon
Enhances satiety
Cagrilintide monotherapy results:
10-12% average body weight loss
Significant GI side effects (stronger gastric slowing)
Currently in Phase 3 trials
Not yet available pharmaceutically
See our cagrilintide weight loss, cagrilintide dosing, and cagrilintide and semaglutide guides.
Theoretical synergy: three pathways working together
Triple-pathway hypothesis:
Pathway | Peptide | Primary Mechanism | Gastric Emptying Effect | Appetite Suppression | Expected Contribution |
|---|---|---|---|---|---|
GIP | Tirzepatide | Insulin sensitivity, fat metabolism | Minimal | Indirect | 5-7% weight loss |
GLP-1 | Tirzepatide | Central appetite, glucose control | Moderate | Strong | 8-10% weight loss |
Amylin | Cagrilintide | Satiety, gastric slowing | Very Strong | Strong | 10-12% weight loss |
Combined | Both | All pathways activated | Maximum | Maximum | 20-30% theoretical |
Why it might work:
Non-overlapping receptor pathways
Complementary not redundant
Multiple appetite suppression mechanisms
Enhanced metabolic effects
Potential for greater weight loss than either alone
Comparison to proven combinations:
CagriSema (semaglutide + cagrilintide): 15-25% proven
Tirzepatide alone: 15-22% proven
Theoretical tirzepatide + cagrilintide: 20-30% unproven
The critical problem: no clinical data
What we DON'T know:
Is the combination safe?
Do side effects multiply or synergize dangerously?
What's the optimal dosing?
Does adding cagrilintide to tirzepatide provide additional benefit?
Could tirzepatide's dual action already maximize what's achievable?
Why this matters:
Tirzepatide alone already very powerful (15-22%)
May already be optimizing GIP/GLP-1 pathways maximally
Adding amylin might only add 2-5% more weight loss
But could significantly increase side effects
Risk-benefit ratio unknown
Contrast with CagriSema:
CagriSema: Extensively studied, Phase 3 trials, known safety
Tirzepatide + cagrilintide: Zero studies, no safety data, speculative
Learn about evidence-based approaches at SeekPeptides - explore best peptides for weight loss and best peptide stack for weight loss.
Theoretical cagrilintide dosage protocols with tirzepatide
Speculative approaches based on known monotherapy dosing.
Conservative combination protocol (if attempting)
Rationale for conservative approach:
No safety data available
Both peptides slow gastric emptying significantly
Risk of severe GI complications
Start low, go slow principle
Tirzepatide component:
Follow standard FDA-approved titration
Weeks 1-4: 2.5mg weekly
Weeks 5-8: 5mg weekly
Weeks 9-12: 7.5mg weekly
Weeks 13-16: 10mg weekly
Week 17+: 12.5mg weekly (or stay at 10mg)
Some reach 15mg weekly (maximum)
Cagrilintide component (reduced from standard):
Start AFTER tirzepatide stabilized at therapeutic dose (week 13+)
Week 13-16: 0.6mg weekly (lower than standard)
Week 17-20: 1.2mg weekly
Week 21-24: 1.8mg weekly (may be maximum tolerable)
Consider 2.4mg only if tolerating perfectly
Conservative dosing comparison:
Week | Tirzepatide Dose | Cagrilintide Dose | Combined Weekly Cost | Expected Side Effects | Cumulative Weight Loss |
|---|---|---|---|---|---|
1-12 | 2.5-10mg titrating | None (tirzepatide only) | $300-500 | Moderate (GLP-1/GIP) | 8-15 lbs |
13-16 | 10mg | 0.6mg | $500-900 | Moderate-High | 18-25 lbs |
17-20 | 12.5mg | 1.2mg | $600-1,100 | High | 28-38 lbs |
21+ | 12.5mg | 1.8mg | $700-1,300 | Very High | 40-55+ lbs (projected) |
Why sequential is safer:
Tirzepatide establishes baseline first
Can attribute new side effects to cagrilintide
Easier to manage one variable at a time
Option to stop cagrilintide if intolerable
Less overwhelming than both simultaneously
Expected benefits:
18-25% total weight loss (conservative estimate)
Potentially superior to tirzepatide alone (15-22%)
But incremental benefit may be modest (3-5% additional)
Use SeekPeptides to plan sequential peptide additions safely. Our peptide cycle planning guide helps coordinate complex protocols.
Aggressive simultaneous protocol (higher risk)
Simultaneous start (both from week 1):
Tirzepatide standard titration:
Same as conservative: 2.5mg → 12.5mg over 16 weeks
Cagrilintide standard titration (parallel):
Weeks 1-4: 0.6mg weekly
Weeks 5-8: 1.2mg weekly
Weeks 9-12: 1.8mg weekly
Week 13+: 2.4mg weekly
Aggressive dosing table:
Week Range | Tirzepatide | Cagrilintide | Total Peptides Active | Gastric Emptying Impact | Nausea Risk | Monthly Cost |
|---|---|---|---|---|---|---|
1-4 | 2.5mg | 0.6mg | Both low | Moderate | 40-50% | $600-1,000 |
5-8 | 5mg | 1.2mg | Both escalating | High | 60-70% | $800-1,400 |
9-12 | 7.5mg | 1.8mg | Approaching max | Very High | 70-80% | $1,000-1,800 |
13-16 | 10mg | 2.4mg | Both at target | Extreme | 80%+ | $1,200-2,000 |
17+ | 12.5mg | 2.4mg | Maximum | Extreme | 80%+ | $1,200-2,400 |
Why this is risky:
Compounding side effects from start
Very difficult to tolerate
High dropout risk
Unclear if any additional benefit
Both hitting stomach simultaneously
Potential maximum weight loss:
20-30% body weight (theoretical)
Example: 240 lbs → 168-192 lbs (48-72 lbs lost)
But tolerability extremely questionable
Who might attempt:
Exceptional GI tolerance
Prior success with GLP-1s without nausea
Closely monitored by physician
Willing to accept high side effect risk
Can afford $1,200-2,400/month
Understands experimental nature
Lower cagrilintide doses with tirzepatide
Moderate approach:
Tirzepatide: Standard titration to 10-15mg
Cagrilintide: Maximum 1.2-1.8mg (lower than standard 2.4mg)
Rationale:
Tirzepatide doing heavy lifting already
Cagrilintide just adds amylin pathway
Don't need maximum cagrilintide dose
Better tolerability
Significantly lower cost
Moderate dosing comparison:
Tirzepatide Dose | Cagrilintide Dose | Expected Weight Loss | Side Effect Severity | Monthly Cost (Research) | Tolerability | Recommended? |
|---|---|---|---|---|---|---|
10-12.5mg | None | 15-20% | Moderate | $300-500 | Good | Yes - proven effective |
10mg | 0.6mg | 16-21% | Moderate-High | $500-1,000 | Fair | Maybe - minimal benefit |
10mg | 1.2mg | 17-23% | High | $700-1,400 | Poor | Questionable - high sides |
12.5mg | 1.8mg | 18-25% | Very High | $900-1,800 | Very Poor | No - CagriSema safer |
15mg | 2.4mg | 20-30% | Extreme | $1,200-2,400 | Extremely Poor | No - unsafe, no data |
Verdict: Lower cagrilintide doses (0.6-1.2mg) might be tolerable but benefit questionable.
See our peptide dosing guide, peptide dosage chart, and how to calculate peptide dosages.
Side effects and safety concerns
The combination amplifies risks significantly.
Compounded gastrointestinal effects
Individual GI effects:
Peptide | Gastric Emptying Delay | Nausea Incidence | Vomiting Risk | Constipation | Severity Rating |
|---|---|---|---|---|---|
Tirzepatide 10-15mg | Moderate-Strong | 30-40% | 10-15% | 20-30% | Moderate |
Cagrilintide 2.4mg | Very Strong | 40-50% | 15-20% | 30-40% | Moderate-High |
Both Combined (theoretical) | Extreme | 60-80%+ | 30-40%+ | 50-60%+ | Very High-Extreme |
Expected combined GI profile:
Severe nausea (weeks 4-12 especially)
High vomiting risk
Significant constipation
Potential gastroparesis (delayed stomach emptying severe enough to be pathologic)
Difficulty eating adequate nutrition
Gastroparesis risk:
Both peptides slow stomach dramatically
Combined effect could be dangerous
Severe cases may need IV hydration
Could require hospitalization
Potential for long-term stomach dysfunction
Managing severe GI effects:
Liquid nutrition (protein shakes, bone broth)
Very small frequent meals (6-8 per day)
Ginger supplementation
Prescription anti-nausea (Zofran essential)
Stool softeners/laxatives daily
Consider reducing or stopping one peptide
Medical supervision critical
Nutritional deficiency risks
Extreme appetite suppression dangers:
May be unable to eat >1,000 calories daily
Protein intake severely compromised (<50g)
Vitamin/mineral deficiencies
Muscle wasting accelerated
Fatigue, weakness, hair loss
Immune suppression
Mitigation strategies:
Protein shakes (30-40g per shake, 2-3 daily)
Liquid meal replacements
Comprehensive multivitamin
B12 injections
Iron supplementation if needed
Regular bloodwork (monthly)
May need to reduce doses despite wanting weight loss
Unknown drug interaction effects
What we don't know:
Do tirzepatide and cagrilintide interact at receptor level?
Metabolic pathway interference?
Cumulative organ stress (pancreas, liver)?
Long-term safety of combination?
Increased pancreatitis risk?
Theoretical concerns:
Both affect glucagon (additive effect?)
Both slow gastric emptying (dangerous synergy?)
Pancreatic stress from dual stimulation?
Thyroid tumor risk (seen with GLP-1s in animals)?
Prudent approach:
Physician supervision mandatory
Regular monitoring (monthly visits)
Bloodwork every 4-8 weeks
Immediate medical attention if severe symptoms
Consider safer alternatives first
See our peptide safety and risks and common peptide mistakes beginners make at SeekPeptides.
Comparing to proven alternatives
Better-studied options that deliver similar results.
CagriSema (cagrilintide + semaglutide) - proven alternative
Why CagriSema is superior choice:
Factor | CagriSema (Cagri + Sema) | Tirzepatide + Cagrilintide | Verdict |
|---|---|---|---|
Clinical Data | Extensive Phase 3 trials | Zero studies | CagriSema wins - proven safe |
Weight Loss | 15-25% proven | 20-30% theoretical | Similar potential - CagriSema proven |
Side Effects | Well-characterized | Unknown synergy | CagriSema wins - predictable |
FDA Status | Likely approval 2025-26 | Both investigational | CagriSema wins - closer to approval |
Dosing Protocols | Established, tested | Speculative | CagriSema wins - clear guidance |
Cost | $950-1,900/month | $1,200-2,400/month | CagriSema wins - slightly cheaper |
Medical Acceptance | Growing physician support | Experimental only | CagriSema wins - more accepted |
CagriSema advantages:
Proven 15-25% weight loss in trials
Safety profile established
Optimal dosing known (both at 2.4mg)
Physicians familiar with semaglutide
Clear titration schedule
Responder rates documented
On path to FDA approval
When to choose CagriSema over tirzepatide + cagrilintide:
Want evidence-based approach
Value safety data
Physician-supervised
Insurance might cover eventually
Don't want to be guinea pig
See our comprehensive cagrilintide and semaglutide guide and semaglutide dosage calculator.
Tirzepatide monotherapy - simpler and proven
Why tirzepatide alone might be enough:
Tirzepatide alone achievements:
15-22% average weight loss
Approaching CagriSema results
FDA approved, widely available
Well-tolerated in most patients
Single injection weekly
Proven cardiovascular benefits
Insurance coverage available
Adding cagrilintide to tirzepatide:
Theoretical 3-8% additional weight loss
Significantly worse side effects
2-3x higher cost
No safety data
Requires two injections
Experimental approach
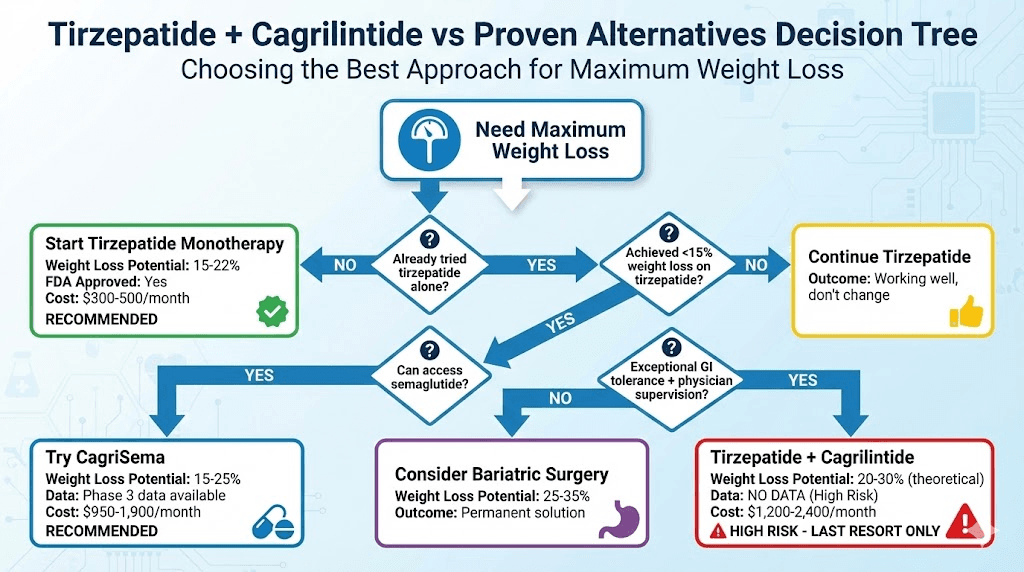
Cost-benefit analysis:
Approach | Weight Loss | Tolerability | Cost/Month | FDA Status | Recommendation |
|---|---|---|---|---|---|
Tirzepatide 10-15mg alone | 15-22% | Good | $300-500 | Approved | Recommended |
Tirzepatide + Cagrilintide | 20-30%? | Poor | $1,200-2,400 | Investigational | Not recommended |
CagriSema | 15-25% | Moderate | $950-1,900 | In trials | Better alternative |
Semaglutide alone | 10-15% | Good | $150-300 | Approved | Good baseline |
Verdict: For most people, tirzepatide alone delivers excellent results without the risks and costs of adding cagrilintide.
Semaglutide + metabolic peptides - different synergy
Alternative combination strategy:
Semaglutide + CJC-1295/Ipamorelin:
Semaglutide: 2.4mg weekly (weight loss)
CJC-1295: 200-300mcg 5x weekly (muscle preservation)
Ipamorelin: 200-300mcg 5x weekly (body composition)
Benefits:
Better muscle retention during weight loss
Improved body composition
Different mechanisms (GLP-1 + GH)
Well-tolerated combination
Complementary not competing
Semaglutide + BPC-157:
Semaglutide: 2.4mg weekly (weight loss)
BPC-157: 250-500mcg twice daily (gut health)
BPC-157 may reduce GI side effects
Supports gut during weight loss
Safe combination
See our peptide stacks guide, peptide stack calculator, CJC-1295 dosage calculator, Ipamorelin benefits, BPC-157 guide, BPC-157 dosage calculator, and peptides for muscle growth.
Who might consider this experimental combination
Very limited scenarios justify the risk.
Ideal candidate profile (if any)
Would need ALL of these:
Exceptional GI tolerance (no nausea on GLP-1s)
Failed tirzepatide alone (reached plateau <15% loss)
Failed CagriSema or can't access semaglutide
Physician supervision with frequent monitoring
Can afford $1,200-2,400/month indefinitely
Willing to accept experimental risk
No history of gastroparesis
No gallbladder disease
No pancreatitis history
Excellent overall health
BMI 40+ with severe obesity
Exhausted other options
Realistically:
Almost no one fits this profile
Better alternatives exist for everyone
Risk-benefit ratio unfavorable
When to absolutely avoid
Do NOT attempt if:
First-time peptide user (start with monotherapy)
History of severe nausea/vomiting
Gastroparesis or severe GERD
Gallstones or gallbladder disease
Pancreatitis history
Eating disorders
Unable to afford long-term
No physician oversight
Tirzepatide alone working well
BMI <35 (not severe enough to justify risk)
Safer alternatives:
Tirzepatide monotherapy (15-22% loss)
CagriSema when available (15-25% loss, proven)
Semaglutide monotherapy (10-15% loss, proven)
Bariatric surgery if BMI >40 (25-35% loss, permanent)
Making the decision: risk vs reward
Potential reward:
3-8% additional weight loss beyond tirzepatide
Example: 240 lbs person
Tirzepatide alone: 36-53 lbs lost → 187-204 lbs
Cagrilintide: 48-72 lbs lost → 168-192 lbs
Additional: 12-19 lbs potentially
Risks:
Severe GI complications (gastroparesis)
Nutritional deficiencies
Muscle wasting
Unknown drug interactions
Potential organ damage
$14,400-28,800 yearly cost
No medical support (experimental)
Recommendation: Risk outweighs potential reward for 99% of people. Pursue proven alternatives.
Plan evidence-based weight loss strategies at SeekPeptides - we help you choose safe, effective protocols with clinical backing rather than experimental combinations.
Practical implementation (if proceeding despite warnings)
For the few who still choose this path.
Pre-combination requirements
Medical screening mandatory:
Comprehensive metabolic panel
Lipid panel
Thyroid function (TSH, Free T4)
A1c (even if not diabetic)
Liver enzymes
Kidney function
Gallbladder ultrasound
Upper GI evaluation if any symptoms
Baseline EKG
Physician supervision:
Find doctor willing to monitor (may be difficult)
Monthly visits minimum
Bloodwork every 4-8 weeks
Clear escalation plan for emergencies
Access to IV hydration if needed
Baseline measurements:
Weight
Body composition (DEXA scan ideal)
Waist circumference
Photos
Quality of life assessment
GI symptom diary
Monitoring protocol during combination
Weekly tracking:
Weight (same day, time, conditions)
Side effects severity (1-10 scale)
Caloric intake estimate
Protein intake (grams)
Bowel movements (frequency, consistency)
Energy levels
Any concerning symptoms
Monthly medical checks:
Weight and vital signs
Review symptom diary
Dose adjustments if needed
Bloodwork review
Physical exam
Gallbladder palpation
Assessment of nutritional status
Red flags requiring immediate medical attention:
Severe persistent vomiting (can't keep liquids down)
Severe abdominal pain (especially upper right)
Signs of dehydration (dizziness, dark urine, rapid heart rate)
Pancreatitis symptoms (severe upper abdominal pain radiating to back)
Jaundice (yellowing of skin/eyes)
Unexplained fever
Extreme weakness or fatigue
When to stop the combination
Absolute discontinuation criteria:
Pancreatitis
Gastroparesis diagnosis
Gallstones with symptoms
Severe malnutrition
Unable to maintain >800 calories daily
Unable to achieve >40g protein daily
Severe persistent vomiting
Weight loss >3 lbs/week sustained (too fast)
Any serious adverse event
Consider stopping if:
Side effects severely impacting quality of life
Not losing more weight than tirzepatide alone
Cost becoming unsustainable
Physician recommends discontinuation
Better alternatives become available
How you can use SeekPeptides for safer weight loss
SeekPeptides helps you achieve maximum weight loss through evidence-based approaches rather than experimental combinations. Our platform guides you toward proven protocols - tirzepatide monotherapy, CagriSema when available, or semaglutide-based stacks - that deliver comparable results without the risks.
Get personalized recommendations based on your weight loss history, GI tolerance, budget, and goals. Our AI advisor helps you determine if you're a candidate for aggressive protocols or if safer alternatives are better suited. Access clinical trial data, real-world results, and safety profiles for all major weight loss peptides.
Use our calculators - peptide calculator, semaglutide dosage calculator, peptide cost calculator, peptide stack calculator, peptide reconstitution calculator - for precise protocols.
Learn proper administration through our guides - peptide injections guide, how to reconstitute peptides, peptide storage guide, getting started with peptides.
Access our best peptide vendors for quality sourcing and peptide safety and risks for comprehensive safety information.
Final thoughts
Combining cagrilintide with tirzepatide represents an experimental approach with theoretical weight loss potential of 20-30% but zero clinical data supporting safety or efficacy.
The lack of studies means dosing protocols are speculative, side effect profiles unknown, and risks potentially severe - particularly gastroparesis from combined extreme gastric slowing.
Proven alternatives deliver comparable results with established safety: tirzepatide monotherapy produces 15-22% weight loss with FDA approval and extensive clinical data, while CagriSema (cagrilintide + semaglutide) delivers 15-25% weight loss with Phase 3 trial validation and clearer path to medical acceptance.
The theoretical 3-8% additional weight loss from adding cagrilintide to tirzepatide doesn't justify the significantly amplified side effects, 2-3x higher cost ($1,200-2,400 monthly), lack of physician support for experimental protocols, and unknown long-term safety profile. For 99% of people seeking maximum medical weight loss, better options exist.
If you've plateaued on tirzepatide alone achieving <15% weight loss, the next step should be transitioning to proven CagriSema (if you can access semaglutide) or considering bariatric surgery for BMI >40, not adding cagrilintide to create an unstudied three-pathway combination with extreme GI risks.
The rare individual who might consider this combination needs exceptional GI tolerance proven on prior GLP-1s, physician supervision with frequent monitoring, ability to afford $15,000-30,000 annually, understanding they're experimenting on themselves, and willingness to stop immediately if severe side effects emerge.
Helpful resources for weight loss peptides
Peptide calculator - Calculate all doses
Semaglutide dosage calculator - Semaglutide dosing
Peptide cost calculator - Budget protocols
Peptide stack calculator - Plan combinations
Peptide reconstitution calculator - Mix correctly
Free peptide reconstitution calculator - Alternative calculator
Cheers. Take care of yourself.