Feb 22, 2026

Before you take another dose after your procedure, read this. The decision to restart semaglutide after surgery is not as simple as picking up where you left off. Get the timing wrong, and you risk nausea so severe it delays your recovery. Get it right, and you protect both your surgical outcome and every pound you have lost so far.
This matters more than most people realize.
Semaglutide slows gastric emptying. That is the mechanism behind its appetite suppression, but it is also the reason anesthesiologists lose sleep before operating on GLP-1 patients. Food lingers in the stomach far longer than normal. Under anesthesia, that undigested food can travel into the lungs. The medical term is pulmonary aspiration, and it can turn a routine procedure into a life-threatening emergency. Case reports have documented patients who fasted for more than ten hours yet still had solid food sitting in their stomachs at the time of intubation. The American Society of Anesthesiologists initially responded by recommending that all weekly GLP-1 medications be stopped one full week before any elective surgery. That guidance has since evolved. A multisociety update involving five major medical organizations now takes a more nuanced approach, allowing many patients to continue their medication with proper risk assessment.
But the question everyone asks after the procedure is just as critical as the one before it. When exactly is it safe to start again? This guide walks through the complete timeline for resuming semaglutide after every type of surgery, from minor outpatient procedures to major abdominal operations. It covers dose re-titration protocols, wound healing considerations, nutrition strategies during the gap, and the specific mistakes that derail recovery. Whether you are managing weight loss or using semaglutide for metabolic health, the information here will help you make the safest decision for your body.
Why semaglutide matters for surgical patients
Semaglutide is not just another weight loss medication. It is a GLP-1 receptor agonist that fundamentally changes how your digestive system operates. Understanding those changes is essential for anyone facing surgery, because the same mechanisms that help you lose weight create unique risks on the operating table and unique considerations during recovery.
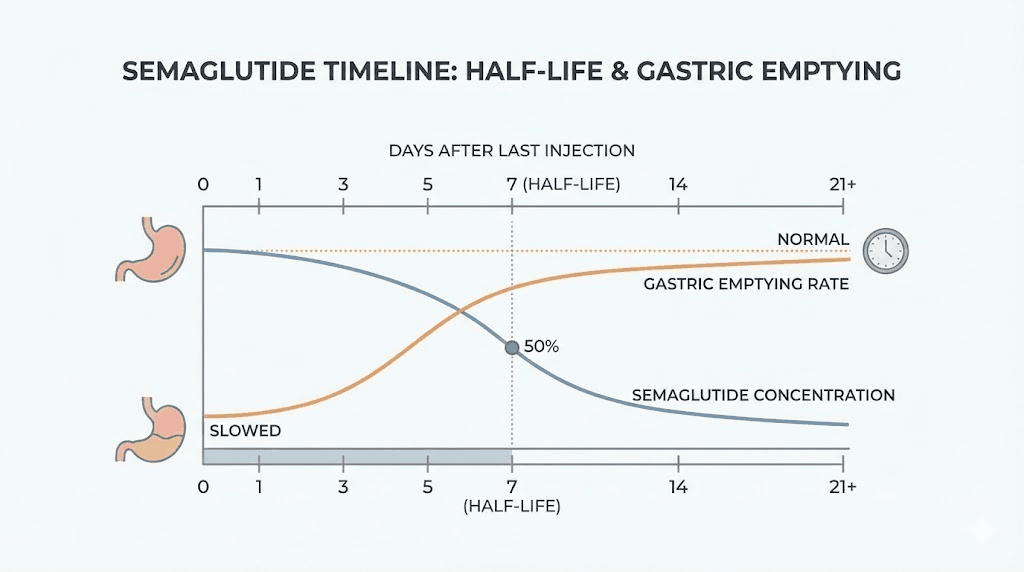
The drug works by mimicking a natural hormone called glucagon-like peptide-1. This hormone tells your brain you are full. It slows digestion. It regulates blood sugar. And it does all of this with a half-life of approximately seven days, meaning the effects linger long after your last injection. For a detailed breakdown of how this medication functions, review the relationship between GLP-1 and branded medications.
Here is why that matters for surgery.
General anesthesia requires an empty stomach. Protective reflexes like coughing and swallowing disappear under sedation, so any food remaining in the stomach can reflux into the airway. Semaglutide delays gastric emptying significantly, sometimes by hours beyond what fasting guidelines anticipate. A study published by the American Academy of Orthopaedic Surgeons found that patients who stopped their GLP-1 medication only three to five days before surgery had an independently elevated risk of aspiration pneumonitis. Patients who discontinued the drug fourteen or more days prior showed no increased risk compared to non-users. That fourteen-day threshold has become a key reference point in surgical planning, and knowing it helps you understand why restarting requires similar care.
The number of surgical patients using semaglutide has grown dramatically. Millions of prescriptions have been filled. Surgeons, anesthesiologists, and primary care physicians are all navigating this new reality simultaneously, and the guidelines continue to evolve as more data emerges. If you are currently on a structured dosing schedule, your surgical team needs to know about it well before your procedure date. Full transparency with every member of your medical team is not optional. It is the foundation of a safe surgical experience.
The growing intersection of GLP-1 therapy and surgery
Consider the math. Semaglutide users often lose significant body weight. That weight loss frequently motivates additional procedures. Skin removal surgery after major weight loss. Joint replacements that become feasible at a lower body weight. Cosmetic procedures that patients have delayed for years. The very success of semaglutide creates a pipeline of patients who eventually need surgical care, making this question one of the most common in pre-operative consultations today.
Patients using semaglutide for weight management often reach a point where they have lost enough weight to qualify for elective procedures they previously avoided. This is a positive outcome, but it requires careful coordination between your prescribing physician and your surgical team. If you are tracking your progress and considering surgery at some point in your journey, tools like the semaglutide dosage calculator can help you stay organized with your protocol details, which your surgeon will want to review.
How semaglutide affects your body before surgery
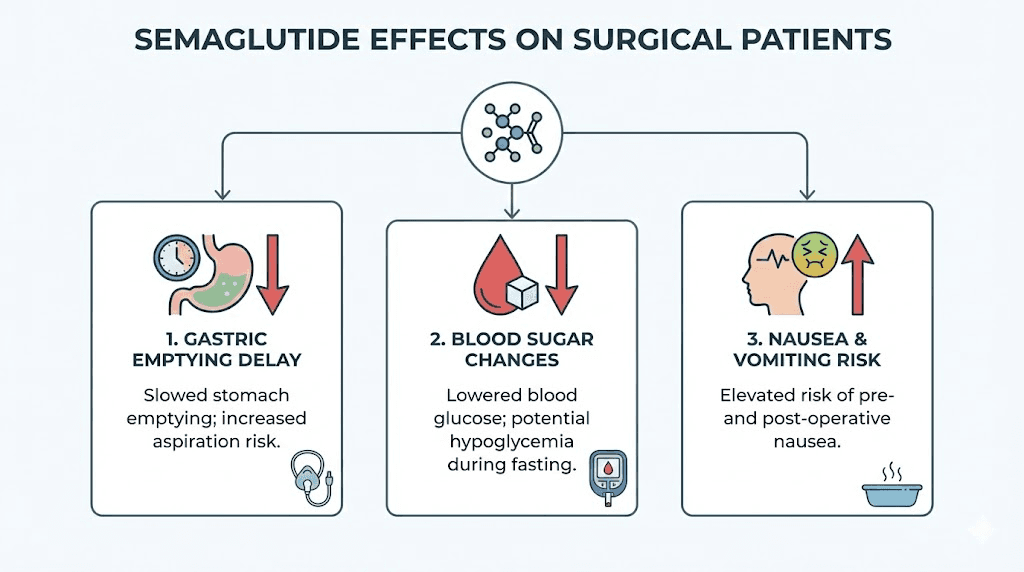
The mechanism is straightforward but the consequences are significant. Semaglutide binds to GLP-1 receptors throughout your body, triggering a cascade of effects that extend far beyond appetite suppression. For surgical patients, three of these effects demand attention.
Delayed gastric emptying and aspiration risk
This is the primary concern. Semaglutide slows the rate at which food moves from your stomach into your small intestine. Under normal circumstances, a person who fasts for eight hours before surgery has an empty stomach. Semaglutide can extend that emptying time dramatically, sometimes to twelve hours or more for solid foods. The result is that standard fasting protocols may not be sufficient.
Aspiration pneumonitis occurs when stomach contents enter the lungs. It is rare in the general surgical population, but the risk increases when the stomach is not empty at the time of intubation. Case reports in anesthesia literature have described patients on GLP-1 agonists who followed standard fasting instructions, presented for routine procedures, and were found to have significant gastric contents upon induction. Some of these cases resulted in aspiration events requiring intensive care admission.
The data is sobering. That AAOS study found that stopping GLP-1 medications only three to five days before surgery was an independent risk factor for aspiration pneumonitis. The takeaway is clear. These drugs need adequate washout time before anesthesia, and the same caution applies when restarting afterward while your body is still recovering from the procedure. If you have experienced gastrointestinal symptoms like burping or constipation on semaglutide, those symptoms may be amplified in the post-surgical period when your GI tract is already sluggish from anesthesia and pain medications.
Blood sugar regulation
Semaglutide lowers blood sugar. For diabetic patients, this is a primary benefit. For surgical patients, it creates a balancing act. Surgery itself triggers a stress response that raises blood glucose. Stopping semaglutide removes one layer of glycemic control precisely when the body is under maximum stress. Diabetic patients who discontinue semaglutide before surgery may need temporary adjustments to their insulin regimen or other glucose-lowering medications to maintain safe blood sugar levels throughout the perioperative period.
This is especially relevant for patients using semaglutide alongside other therapies. If you are exploring combination approaches, understanding how to manage your semaglutide and B12 protocol or other supplementation during surgical breaks is important.
Nausea and post-operative GI function
Surgery already causes nausea in many patients. Anesthesia slows gut motility. Opioid pain medications make it worse. Adding semaglutide back too soon layers another source of GI slowdown on top of an already compromised digestive system. The result can be severe nausea, vomiting, and an inability to tolerate food or fluids, which directly undermines surgical recovery. Your body needs nutrition to heal. Anything that prevents you from eating adequately after surgery delays wound healing, increases infection risk, and prolongs your overall recovery timeline.
Understanding the fatigue patterns associated with semaglutide is also helpful here, because post-surgical fatigue combined with medication-related fatigue can create a compounding effect that makes early recovery more difficult than expected. Patients who have experienced dizziness while on semaglutide should be especially cautious about restarting before they are fully mobile and hydrated after surgery.
When to stop semaglutide before surgery
The guidance on this question has shifted significantly, and understanding the current recommendations helps frame when and how you should resume afterward. The timeline for stopping directly influences the timeline for restarting.
Original ASA recommendation
The American Society of Anesthesiologists initially issued a straightforward recommendation. Stop all weekly GLP-1 receptor agonists one week before any elective surgery requiring anesthesia. This was a conservative, blanket approach designed to minimize aspiration risk across all patients. It did not differentiate between dose levels, duration of therapy, or the presence of GI symptoms.
Updated multisociety guidance
The updated guidance, developed collaboratively by the ASA and four additional medical societies, takes a more individualized approach. It recognizes that not all semaglutide patients carry the same level of risk and that the blanket one-week discontinuation may be unnecessarily restrictive for some patients while potentially insufficient for others.
The key points of the updated guidance are significant.
Most patients on stable maintenance doses can continue their GLP-1 medication with appropriate risk assessment. Patients in the dose escalation phase, typically the first four to eight weeks of treatment, should defer elective procedures until they reach a stable dose. If you are still titrating your dose upward, that is the highest-risk period for unpredictable GI effects, and surgery should wait.
Patients experiencing active GI symptoms such as nausea, vomiting, bloating, or significant appetite changes should postpone elective surgery until those symptoms resolve. The presence of these symptoms suggests particularly delayed gastric emptying, which directly increases aspiration risk.
For patients on higher doses, following a liquid diet for twenty-four hours before the procedure is recommended even if the medication is continued. This reduces the volume of gastric contents at the time of surgery.
Point-of-care gastric ultrasound can be used at the time of surgery to assess stomach contents in real time. This technology allows the anesthesiologist to make an informed decision about whether to proceed, even if there is uncertainty about gastric emptying status. Knowing these details helps you have productive conversations with your surgical team and understand the logic behind their pre-operative instructions, whether they ask you to stop the medication entirely or simply adjust your diet beforehand. For patients weighing their options, tools like the semaglutide versus tirzepatide comparison page may be useful for understanding how different GLP-1 drugs handle surgical situations differently.
Risk categories for surgical patients on semaglutide
Not every patient on semaglutide faces the same level of surgical risk. The updated guidelines effectively create three risk tiers.
Lower risk: Patients on a stable maintenance dose for more than eight weeks, with no active GI symptoms, and undergoing a procedure with moderate aspiration risk. These patients may be able to continue their medication with dietary modifications before surgery.
Moderate risk: Patients on higher doses, those with intermittent GI symptoms, or those undergoing procedures with higher aspiration risk. These patients typically benefit from holding one to two doses before surgery and following a strict liquid diet.
Higher risk: Patients still in the dose escalation phase, those with persistent GI symptoms such as ongoing constipation or frequent nausea, and those undergoing emergency surgery where gastric emptying status is unknown. These patients should discontinue semaglutide with maximum lead time before elective procedures, or have point-of-care ultrasound assessment if surgery cannot be delayed.
Timeline for resuming semaglutide after surgery
This is the question that brought you here. The answer depends on what kind of surgery you had, how your recovery is progressing, and whether you can tolerate oral intake normally. There is no single universal timeline, but there are clear guidelines for different situations.
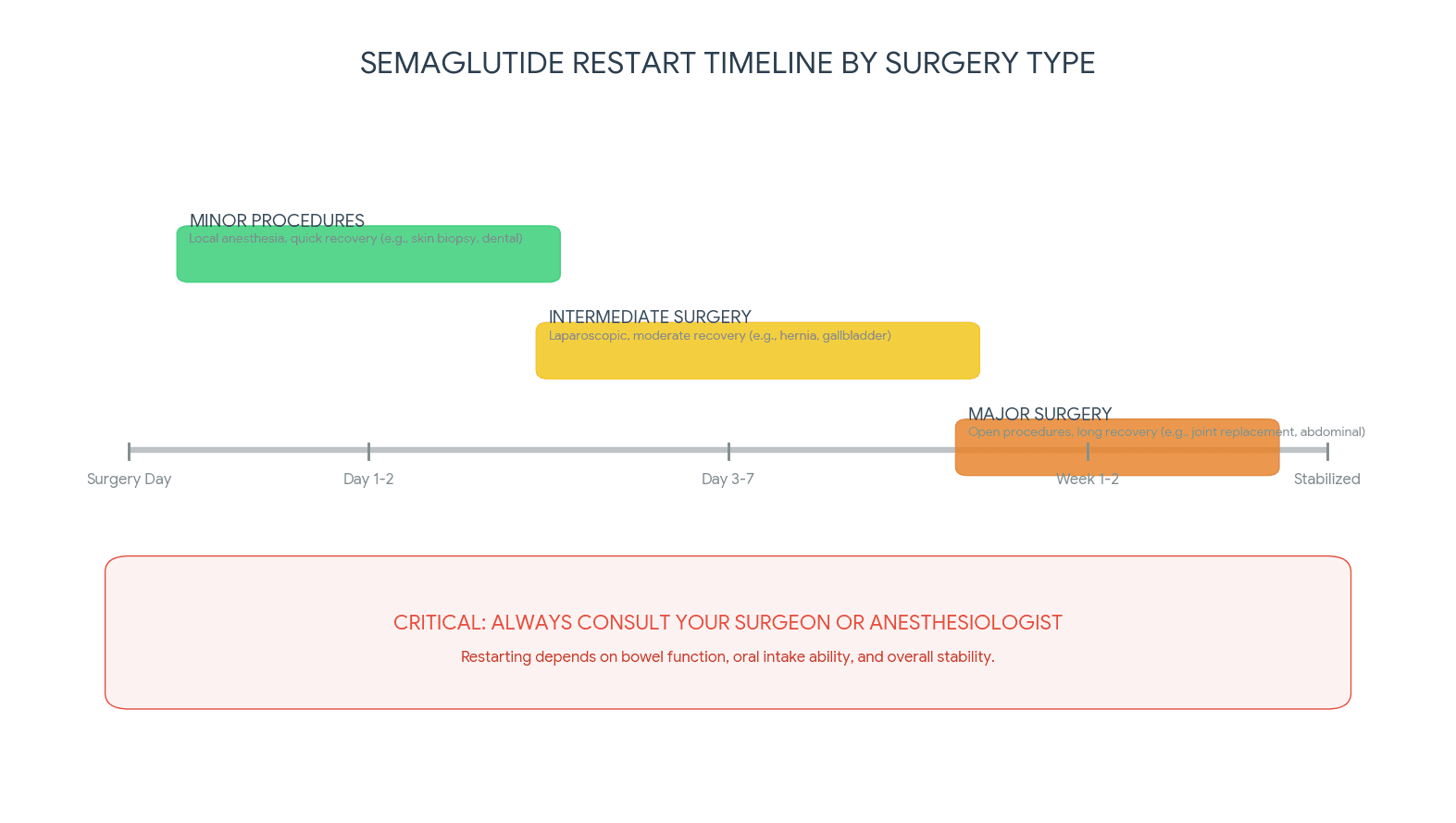
Minor outpatient procedures
For minor surgeries, think dental procedures under sedation, endoscopy, minor dermatological surgery, or simple orthopedic procedures, the restart timeline is relatively short. Most patients can resume semaglutide forty-eight to seventy-two hours after the procedure, provided they meet three conditions.
First, you must be tolerating food and fluids normally. If you are still nauseated or unable to eat solid food, adding semaglutide will only make it worse. Second, you should be off IV fluids and managing your own hydration. Third, you should have had at least one normal bowel movement, indicating your GI tract has recovered from anesthesia effects. If you are checking your dosage in units before restarting, make sure the numbers match what you were taking before the procedure.
Major surgery with general anesthesia
Major procedures require more patience. This category includes abdominal surgery, cardiac procedures, major orthopedic operations like joint replacements, and any surgery requiring extended general anesthesia or significant post-operative pain management with opioids.
The recommended waiting period is one to two weeks after surgery. Why so long? Several factors converge after major surgery. Opioid pain medications slow GI motility dramatically. Your body is diverting resources to wound healing, not digestion. Post-operative ileus, a temporary paralysis of the intestines, is common after abdominal procedures and can last days. Adding a drug that further slows gastric emptying into this environment is counterproductive and potentially dangerous.
Wait until you are eating a full regular diet, have stopped or significantly reduced opioid use, and have confirmed with your surgical team that your recovery is on track. Most surgeons want to see you at a follow-up appointment before clearing you to restart any medications that affect GI function.
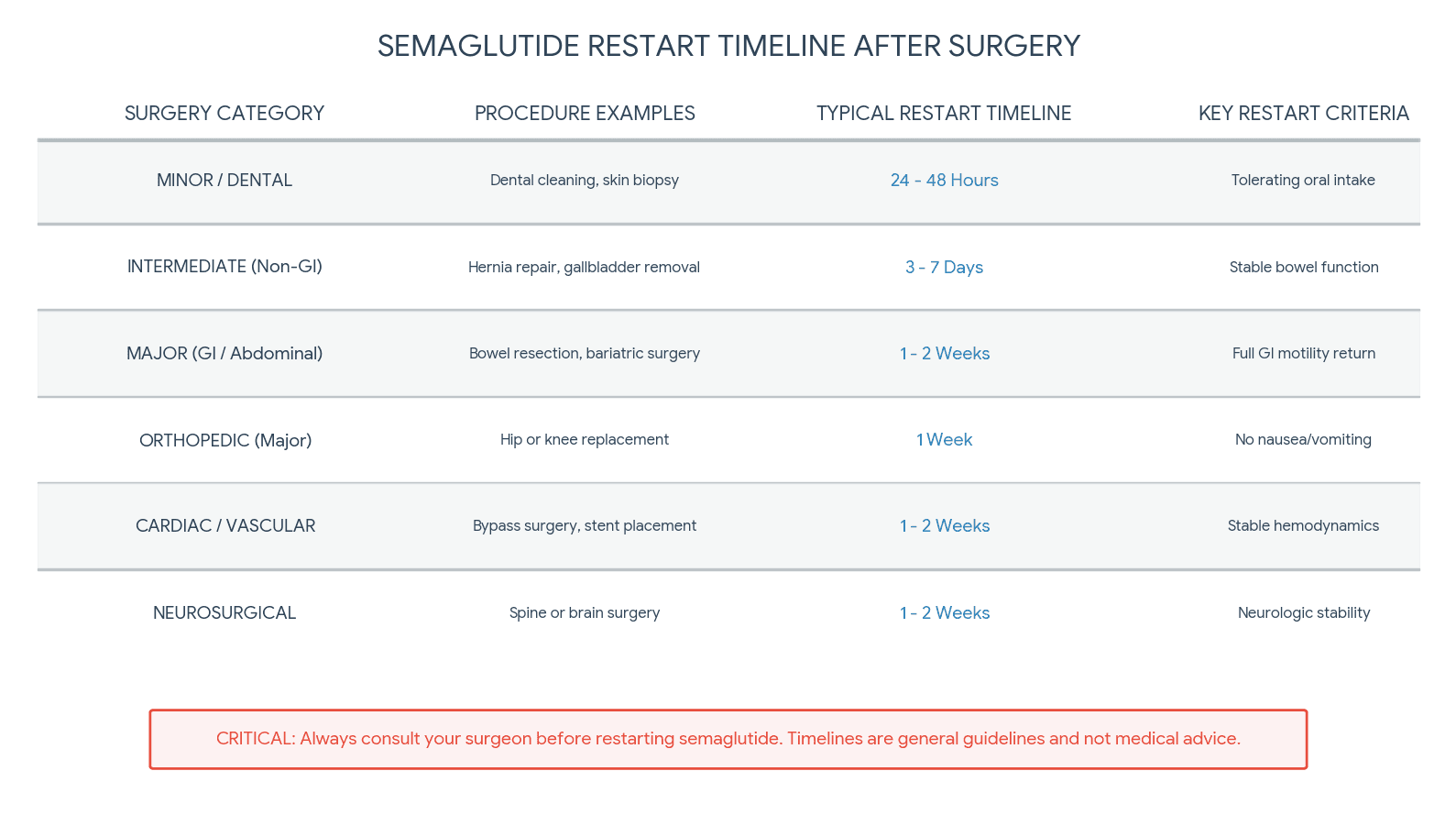
Surgery type restart timeline
Here is a practical reference for common procedures. These are general guidelines, and your surgeon may recommend different timing based on your specific situation.
Dental surgery under sedation: Resume in forty-eight to seventy-two hours once eating normally.
Endoscopy or colonoscopy: Resume in twenty-four to forty-eight hours if no complications.
Laparoscopic cholecystectomy: Resume in five to seven days once tolerating regular diet.
Hernia repair: Resume in five to seven days for laparoscopic, seven to fourteen days for open repair.
Joint replacement: Resume in seven to fourteen days once off strong opioids and eating normally.
Bariatric surgery: Wait a minimum of two to four weeks, and only under direct guidance from your bariatric surgeon.
Abdominoplasty or panniculectomy: Resume in ten to fourteen days with close wound monitoring.
Cardiac surgery: Resume in two to four weeks after surgical team clearance.
These timeframes assume an uncomplicated recovery. Any post-operative complications, particularly infection, wound healing problems, or persistent GI dysfunction, should extend the waiting period. When you do restart, having your dosage conversion chart handy makes the transition smoother.
Signs you are ready to resume
Beyond the calendar, your body will tell you when it is ready. Look for these indicators before taking your first post-surgical dose.
You are eating three meals per day without nausea or vomiting. Your bowel function has returned to normal. You are no longer taking opioid pain medications, or have reduced to occasional use only. Your surgical incisions are healing well with no signs of infection. You have adequate energy for daily activities. Your surgeon has cleared you for medication resumption at your follow-up visit.
If any of these criteria are not met, wait longer. There is no benefit to rushing. The weight you might regain during a two-week pause is trivial compared to the complications that can arise from restarting too early. For context on how quickly semaglutide begins working once you resume, review the guide on how long semaglutide takes to work and the timeline for appetite suppression effects.
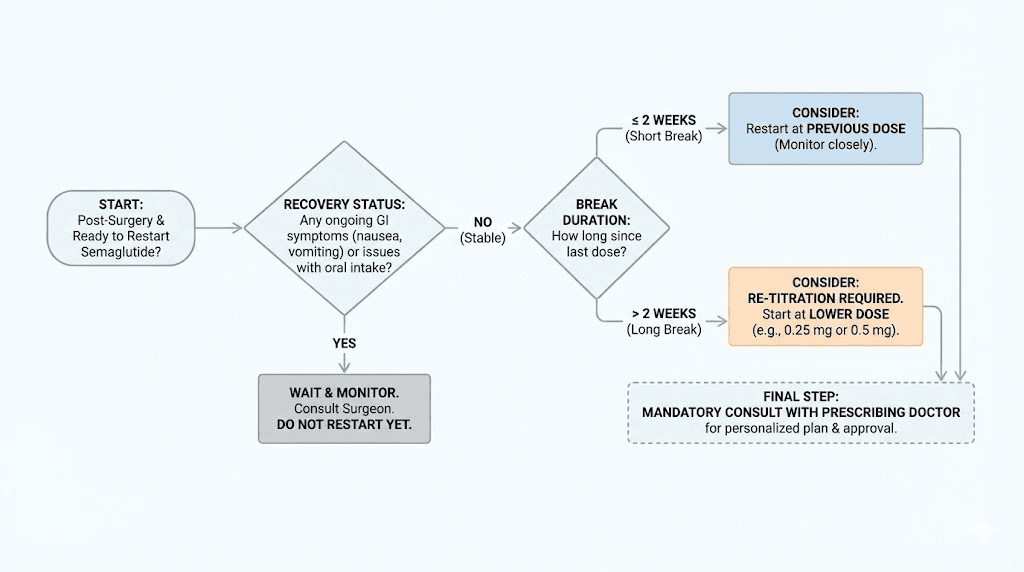
How to restart your semaglutide dose safely
The length of your break determines your restart strategy. This is not a detail you should guess about, because getting the dose wrong can cause severe side effects that set back your recovery.
If you stopped for less than two weeks
Good news. If your surgical break was shorter than two weeks, you can typically resume at your previous dose. Your body has not lost its tolerance to the medication in this timeframe. The GLP-1 receptors remain sensitized, and the side effect profile should be similar to what you experienced before surgery.
That said, listen to your body on that first dose back. If you experience more nausea than usual, it may be because your GI system is still recovering from the surgical stress, anesthesia, and any pain medications you took. This does not necessarily mean you need to drop your dose, but it does mean you should pay attention and report any significant symptoms to your prescribing physician. Having a clear dosing chart in units available ensures you do not accidentally overshoot your restart dose.
If you stopped for more than two weeks
This changes things significantly.
After a gap of more than two weeks, your body begins losing its acclimation to semaglutide. Receptor sensitivity shifts. GI tolerance decreases. Restarting at your previous maintenance dose will almost certainly cause intense nausea, vomiting, and digestive distress. Do not do this.
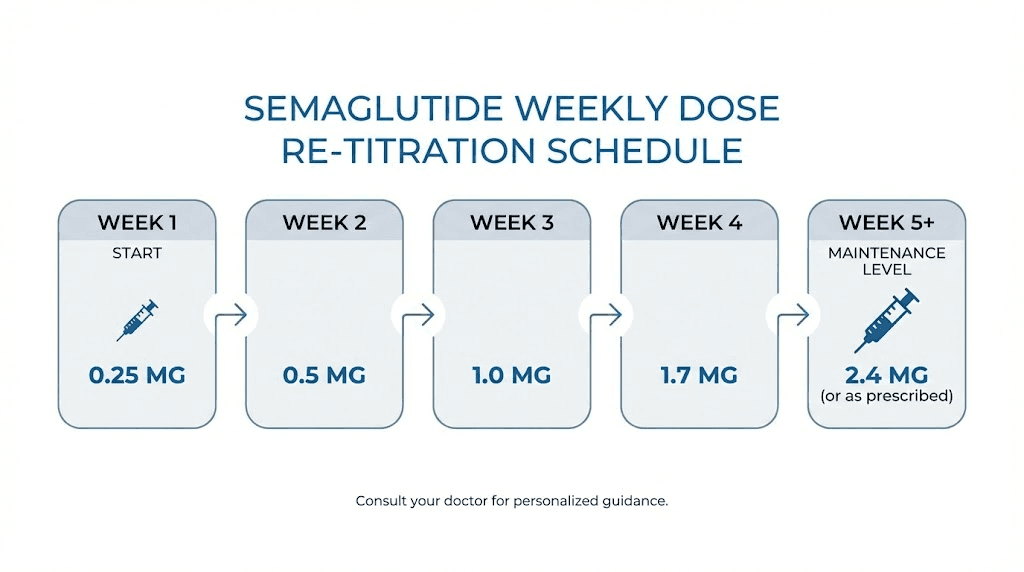
Instead, restart at a lower dose and re-titrate upward. The standard restart protocol is 0.25 mg per week for four weeks, then 0.5 mg per week for four weeks, then gradual increases back to your previous maintenance dose. Yes, this means it may take eight to twelve weeks to get back to where you were. That timeline feels frustrating, but the alternative, restarting at a full dose and spending days unable to eat or drink, is far worse for your surgical recovery.
Use the semaglutide dosage calculator to plan your re-titration schedule. If you were on a compounded formulation, check the compounded semaglutide dose chart for the specific concentrations you need. And if your vial sat in the refrigerator during your recovery, verify it is still within its shelf life window before using it.
Re-titration protocol for extended breaks
Here is the exact approach most clinicians recommend for patients restarting after breaks of two weeks or longer.
Weeks one through four: 0.25 mg weekly. This is the introductory dose. It reacquaints your GI system with the drug. Expect mild appetite changes but minimal side effects if you follow the titration properly.
Weeks five through eight: 0.5 mg weekly. Most patients begin noticing meaningful appetite suppression at this dose. GI side effects may increase slightly. If you tolerate this well, proceed to the next step.
Weeks nine through twelve: 1.0 mg weekly. This is where significant clinical effects resume for most patients. Monitor your response carefully.
Week thirteen and beyond: If your previous maintenance dose was higher than 1.0 mg, continue titrating upward in increments as directed by your prescribing physician. Refer to the 5mg dosage chart or the 10mg dosage chart depending on your vial concentration.
Do not rush this process. The weeks you spend re-titrating are protecting your surgical recovery and preventing side effects that could interfere with wound healing, nutrition, and hydration. If you need guidance on reconstituting your medication after the break, the semaglutide reconstitution guide walks through every step, and the reconstitution calculator handles the math for you.
What about missed injection timing?
If you were on a strict weekly injection schedule before surgery, restarting means picking a new injection day and sticking with it. Choose a day when you are at least forty-eight hours past your last surgical follow-up, so any issues from the injection can be evaluated separately from post-surgical concerns. Some patients find it helpful to review the best time of day to take semaglutide and the optimal GLP-1 timing guide to establish a new routine that fits their recovery schedule.
Injection site selection also matters during recovery. Avoid injecting near or around your surgical incision. The best injection site guide covers all viable locations. If your surgery was abdominal, use the thigh. If your surgery was on a limb, use the abdomen at least three inches from any incision. The injection technique guide provides step-by-step instructions for proper administration at any site.
Surgery types and semaglutide considerations
Different surgeries carry different considerations for semaglutide users. The type of procedure, the anesthesia required, the expected recovery trajectory, and the specific risks associated with that surgery all influence when and how you should restart.
Cosmetic and plastic surgery
This is a complicated category. Research data on semaglutide and cosmetic surgery outcomes is mixed, and it deserves careful attention.
On one hand, semaglutide helps patients lose the weight that motivates cosmetic procedures in the first place. On the other hand, data from non-diabetic plastic surgery patients suggests that GLP-1 use may increase wound complication rates. One study found wound complications of 4.7 percent in panniculectomy patients using GLP-1 agonists compared to 2.7 percent in non-users. For abdominoplasty, the difference was even more pronounced: 9.8 percent versus 3.6 percent.
These numbers require context. Patients on semaglutide have often lost substantial weight rapidly, which can affect tissue quality, blood supply to the skin, and nutritional status. It may not be the drug itself causing complications but rather the metabolic changes associated with rapid weight loss. Regardless, most plastic surgeons now recommend stopping semaglutide at least two weeks before body contouring procedures and waiting until wound healing is well established before resuming, typically ten to fourteen days after surgery with no signs of wound complications.
If you are considering cosmetic procedures after weight loss, understanding your overall semaglutide transformation journey can help set realistic expectations for surgical timing. The key is patience. Reach a stable weight, let your body adjust, and then pursue surgery with clear guidance from both your prescribing physician and your surgeon.
Bariatric surgery
Semaglutide and bariatric surgery have a unique relationship. Some patients use semaglutide before bariatric surgery to reduce operative risk by losing weight preoperatively. Others start semaglutide after bariatric surgery to address weight regain, which affects a significant percentage of bariatric patients over time.
For post-bariatric semaglutide use, the research is encouraging. Studies have shown that patients who started semaglutide after bariatric surgery for weight regain achieved approximately 6 percent total weight loss at three months and 10.3 percent at six months. These are meaningful numbers for a population that has already undergone the most aggressive weight loss intervention available.
However, there are nutritional concerns. Bariatric surgery already limits the amount of food patients can eat and the nutrients they can absorb. Adding semaglutide further suppresses appetite and slows GI motility. Research has documented decreases in serum albumin, vitamin B12, and zinc in bariatric patients using semaglutide. These deficiencies can impair wound healing, immune function, and energy levels.
If you have had bariatric surgery and are considering semaglutide for weight regain, discuss this extensively with your bariatric team. Nutritional monitoring becomes essential. Consider supplementation strategies, particularly semaglutide combined with B12 or semaglutide with methylcobalamin, to offset potential deficiencies. SeekPeptides provides detailed protocol guidance for managing these complex medication combinations safely.
Orthopedic surgery
Joint replacements and other major orthopedic procedures present a interesting data point for semaglutide users. For diabetic patients undergoing orthopedic surgery, GLP-1 agonist use was associated with notably better outcomes: 12 percent lower readmission rates, 29 percent lower wound reopening rates, and 56 percent lower hematoma risk. These benefits likely reflect the anti-inflammatory properties of GLP-1 agonists and their positive effects on blood sugar control during the recovery period.
For orthopedic patients, the restart timeline typically falls in the seven to fourteen day range. The key determining factor is opioid use. Orthopedic surgery often requires significant pain management, and opioids combined with semaglutide create a compounding effect on GI motility that can be debilitating. Wait until you have transitioned to non-opioid pain management or are using opioids only occasionally before restarting your regular semaglutide schedule.
Abdominal surgery
Any surgery involving the abdominal cavity requires the longest restart timeline. The GI tract itself has been manipulated, and post-operative ileus is common. Adding a drug that slows gastric emptying before the gut has fully recovered its normal motility is a recipe for severe nausea, vomiting, and potentially dangerous complications like bowel obstruction.
For open abdominal surgery, wait a minimum of two weeks. For laparoscopic abdominal procedures, one to two weeks is generally appropriate. In both cases, full return of bowel function is the most important milestone, not the calendar. You should be having regular bowel movements, tolerating a normal diet without nausea, and feeling that your digestion has returned to baseline before considering your first dose back.
Dental surgery and minor procedures under sedation
Dental procedures requiring IV sedation or general anesthesia carry the same aspiration risk as any other surgery during the procedure itself. However, the recovery is typically much faster, and the restart timeline is shorter.
Most patients can resume semaglutide forty-eight hours after dental surgery, provided they are eating and drinking normally. If your procedure involved only local anesthesia with no sedation, you do not need to stop semaglutide at all, though you may want to ensure you can eat comfortably afterward before your next dose.
Cardiac surgery
Cardiac procedures demand the most conservative approach. These surgeries involve significant physiological stress, extended anesthesia, and complex recovery protocols. Many cardiac patients are also diabetic, adding another layer of complexity to GLP-1 management.
Wait a minimum of two to four weeks after cardiac surgery before restarting semaglutide. Your cardiologist and surgical team should be involved in this decision. Blood sugar management during the intervening period should be handled with other medications as needed. The metabolic benefits of semaglutide are significant, but they are secondary to cardiac recovery in the immediate post-operative period. Patients who are exploring alternatives during this break may want to review the side effect profiles of semaglutide versus tirzepatide or review the broader landscape of GLP-1 alternatives.
Semaglutide and wound healing after surgery
This is where the research gets genuinely complicated. The data points in different directions depending on the patient population and the type of surgery, and understanding both sides will help you make informed decisions about your restart timing.
Evidence suggesting GLP-1 promotes healing
At the cellular level, GLP-1 receptor agonists appear to have several wound-healing benefits. Research has demonstrated that semaglutide promotes angiogenesis, the formation of new blood vessels that deliver oxygen and nutrients to healing tissue. It also appears to enhance keratinocyte migration, which is the process by which skin cells move to close a wound. These mechanisms suggest that semaglutide could theoretically improve wound healing.
The diabetic surgery data supports this theory. Remember those numbers from orthopedic studies: 29 percent lower wound reopening and 56 percent lower hematoma risk in GLP-1 users. For diabetic patients, the combination of better blood sugar control and direct cellular effects seems to create a net positive for wound healing.
Understanding how peptides interact with healing processes is a broader topic that extends beyond semaglutide. If you are interested in the science of tissue repair, the comprehensive guide to peptide mechanisms covers the fundamental pathways, and specific peptides like BPC-157 have their own body of research related to tissue healing. The peptides for gut health resource is particularly relevant for patients recovering from GI-related surgeries.
Evidence suggesting GLP-1 may impair healing
The plastic surgery data tells a different story. Those higher wound complication rates in abdominoplasty and panniculectomy patients using GLP-1 agonists cannot be ignored. Several mechanisms could explain this.
Reduced caloric intake impairs healing. Period. Your body needs protein, calories, vitamins, and minerals to repair tissue. Semaglutide suppresses appetite, and patients recovering from surgery often already have reduced appetites from pain, nausea, and medication side effects. The compounding effect can push nutritional intake below the threshold needed for optimal wound healing.
GLP-1 agonists reduce GI motility, which can decrease the efficiency of nutrient absorption even when patients do eat. If food moves through the GI tract more slowly, the timing and bioavailability of nutrients may be altered. This is a subtle effect but potentially significant in the context of surgical recovery, when nutritional demands are elevated. The research on foods to avoid on semaglutide and the recommended food list become especially important for surgical patients trying to maximize nutritional intake from limited amounts of food.
Rapid weight loss itself affects tissue quality. Patients who have lost significant weight on semaglutide may have skin with compromised blood supply, reduced collagen density, and impaired elastic recoil. These tissue changes can independently increase surgical wound complications regardless of whether the patient is actively taking the medication at the time of surgery.
The practical takeaway on wound healing
Do not restart semaglutide until your wounds are healing well. This is the simplest and safest approach. Check your incisions daily. Look for signs of healthy healing: edges that are coming together, no redness spreading beyond the immediate wound area, no drainage, no warmth or swelling that is worsening rather than improving. If anything looks concerning, delay restarting and contact your surgical team. The potential benefit of a few extra days of appetite suppression is negligible compared to the risk of a wound complication that could require additional surgery or prolonged recovery.
Nutrition and recovery while off semaglutide
The gap between stopping semaglutide before surgery and restarting afterward is a vulnerable period. Your appetite returns. The drug-assisted portion control disappears. And you are simultaneously recovering from a procedure that demands optimal nutrition. Managing this period well protects both your surgical outcome and your weight loss progress.
Expect your appetite to return
This is the part nobody warns you about. Within days of your last semaglutide dose, your appetite begins to come back. For many patients, the return is dramatic. Food suddenly tastes incredible again. Portion sizes that felt adequate on the medication now feel like a snack. Cravings resurface with startling intensity. Understanding semaglutide withdrawal symptoms can help you prepare mentally for this shift and develop strategies to manage it.
This is normal. It is not a failure. It is the predictable result of removing a drug that was actively suppressing your hunger hormones. Knowing this in advance allows you to prepare rather than panic.
Prioritize protein above everything
Surgical recovery demands protein. Your body uses amino acids to build new tissue, fight infection, and synthesize collagen for wound closure. The general recommendation for post-surgical recovery is 1.2 to 1.5 grams of protein per kilogram of body weight per day, significantly higher than standard dietary guidelines.
Without semaglutide suppressing your appetite, meeting this protein target becomes easier. Use this period to focus on high-quality protein sources: eggs, lean meats, fish, dairy, and protein supplements if needed. If you have been reading about protein shakes optimized for GLP-1 users, the off-medication period is actually the easiest time to implement those strategies because your stomach can handle larger volumes.
A structured semaglutide diet plan adapted for the surgical recovery period focuses on nutrient density rather than calorie restriction. Every bite should deliver protein, vitamins, or minerals that support healing.
Stay hydrated aggressively
Hydration is easy to overlook during surgical recovery, and dehydration is one of the most common preventable complications. Surgery, anesthesia, pain medications, and reduced oral intake all contribute to fluid deficits. Aim for a minimum of sixty-four ounces of water daily, more if you are experiencing vomiting, diarrhea, or fever.
If you experienced dizziness on semaglutide before surgery, that was likely partially related to hydration status. The post-surgical period compounds these risks, so aggressive hydration becomes non-negotiable.
Managing weight during the gap
Some weight regain during a surgical break from semaglutide is common and expected. Most of the initial regain is water weight and increased GI contents from your appetite returning to normal, not true fat gain. The average patient regains two to five pounds during a two-week break, and much of this comes off quickly once the medication is restarted.
Do not try to diet aggressively during surgical recovery. Your body needs calories to heal. Restricting intake to prevent weight gain while recovering from surgery is counterproductive and potentially dangerous. Focus on nutrient quality rather than calorie counting. The weight will be manageable when you restart, especially if you follow the expected results timeline for the re-titration period.
If you are concerned about maintaining momentum, consider that patients who prioritize proper healing and nutrition during their surgical break typically get back to their weight loss trajectory faster than patients who compromise their recovery by restarting too early or eating too little. A smooth recovery means a smoother restart, which means getting back to your long-term semaglutide protocol without setbacks.
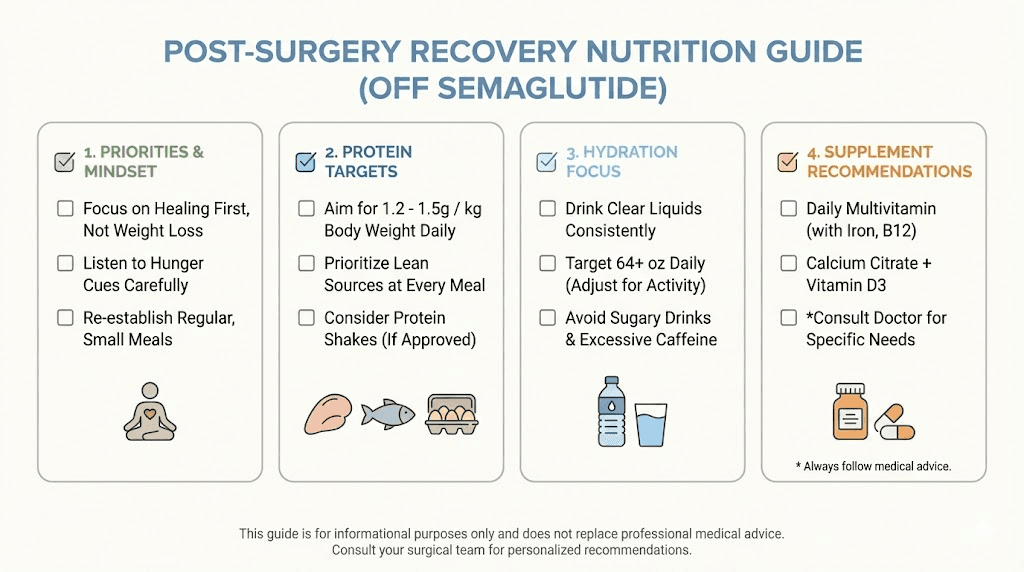
Supplements to consider during the gap
Surgical recovery depletes specific nutrients at an accelerated rate. Vitamin C supports collagen synthesis and immune function. Zinc promotes wound healing and cell division. Iron may be needed if there was significant blood loss during surgery. Vitamin D supports immune function and bone healing if your procedure involved the skeletal system.
If you were taking B12 with your semaglutide or using a glycine combination, continue those supplements through the surgical period. B12 supports energy production and neurological function during recovery, and glycine is a key amino acid for collagen synthesis. The supplement guide for GLP-1 users provides a comprehensive overview of nutritional support strategies that apply equally well during a surgical break.
Common mistakes when restarting semaglutide after surgery
People make these errors constantly. Every one of them is avoidable if you know what to watch for.
Mistake one: restarting at your previous full dose after a long break
This is the single most common and most consequential mistake. Patients who were on 1.0 mg or higher, took three or four weeks off for surgery, and then injected their previous dose on restart almost universally experience severe nausea, vomiting, and GI distress. Some end up back in the emergency room with dehydration. This is particularly dangerous during surgical recovery when your body is already under stress.
The fix is simple. If your break was longer than two weeks, go back to 0.25 mg and re-titrate. Yes, it takes time. Yes, it feels like going backward. It is still the right approach. Reference the unit-based dosage chart to ensure your restart dose is accurate.
Mistake two: not telling your surgeon about semaglutide use
Patients sometimes fail to disclose GLP-1 use during pre-operative assessments. This is dangerous. Your anesthesiologist needs this information to plan your airway management. Your surgeon needs it to evaluate wound healing risk. Your prescribing physician needs to coordinate the stop and restart timeline. Full disclosure to every member of your care team is essential. The peptide safety guide emphasizes this point broadly: transparency with healthcare providers is foundational to safe peptide use.
Mistake three: restarting before you can eat normally
If you are still on a liquid diet, still experiencing post-operative nausea, or still unable to eat solid food, you are not ready for semaglutide. The drug will make these problems worse. Wait until you are eating regular meals, tolerating them fully, and maintaining your hydration independently. If you are unsure whether semaglutide starts suppressing appetite immediately upon restart or if there is a delay, the answer varies by individual, but assume effects begin within twenty-four to forty-eight hours of injection.
Mistake four: ignoring new GI symptoms after restarting
Some GI discomfort when restarting is expected. Severe or persistent symptoms are not. If you experience vomiting that prevents you from keeping fluids down, abdominal pain that is different from your surgical pain, signs of bowel obstruction like no bowel movements combined with nausea and abdominal distension, or any other symptoms that feel wrong, stop the medication and contact your healthcare provider immediately. The GLP-1 side effect comparison guide can help you distinguish between expected and concerning symptoms.
Mistake five: using expired or improperly stored medication
Semaglutide vials that sat in the refrigerator during your surgical recovery may have expired. Compounded semaglutide has specific shelf life limitations, and using expired medication means unpredictable potency and potential contamination risk. Check the 28-day expiration rules, confirm your storage has been correct using the refrigeration requirements guide, and review how long compounded semaglutide lasts in the fridge to verify your supply is still viable.
If there is any doubt about the integrity of your medication, do not use it. The cost of replacing a vial is negligible compared to the cost of injecting degraded medication that either does nothing or causes unpredictable side effects. Check whether your vial was exposed to temperature excursions during your hospital stay or recovery period. The guide on what happens if semaglutide gets warm explains exactly what temperature exposure does to the medication, and the broader expired semaglutide safety guide covers whether partially expired medication has any remaining efficacy.
Mistake six: not adjusting for changed body weight
If your surgery involved significant tissue removal, such as panniculectomy or bariatric surgery, or if you lost weight during the recovery period from reduced intake, your body weight may have changed meaningfully. Some semaglutide protocols are weight-based, and your optimal dose may be different now than it was before surgery. Discuss this with your prescribing physician and recalculate using the peptide calculator if needed.
Mistake seven: restarting without follow-up
Restarting semaglutide should ideally happen after a post-surgical follow-up visit where your surgeon confirms adequate healing. Restarting blindly, without a physician verifying that your wounds are closing properly and your recovery is on track, is a gamble. Schedule the follow-up. Get the clearance. Then restart with confidence.
Special considerations for specific patient populations
Diabetic patients
If you use semaglutide for type 2 diabetes, the restart timeline carries additional urgency. Blood sugar management suffers without GLP-1 therapy, and post-surgical stress further elevates glucose levels. Work with your endocrinologist to create a bridging plan that manages blood sugar during the gap using insulin or other medications, then transitions back to semaglutide when your surgical recovery allows. The metabolic benefits of restarting are significant for diabetic patients, but the GI risks remain the same. Do not let urgency override safety.
Patients switching medications after surgery
Some patients use the surgical break as an opportunity to switch GLP-1 medications. If you are considering a transition from semaglutide to tirzepatide or vice versa, the post-surgical period requires careful planning. Use the switching dosage chart for guidance, and be aware that switching compounds the restart challenges because you are introducing a new drug to a body that is simultaneously recovering from surgery. The conversion chart helps with dose equivalencies, but starting at the lowest dose of the new medication is the safest approach regardless of your previous semaglutide dose.
For patients exploring the switch, the detailed switching guide and the tirzepatide to semaglutide dosage chart provide bidirectional conversion protocols. The combined dosage comparison chart gives a side-by-side view of both drugs at every dose level. SeekPeptides maintains up-to-date conversion resources that reflect the latest clinical recommendations for medication transitions.
Patients using compounded semaglutide
Compounded semaglutide introduces additional variables. Vial concentrations differ from branded products, mixing ratios vary by pharmacy, and shelf life may be shorter. Before restarting a compounded formulation after surgery, verify your medication is still within its use window. The compounded semaglutide guide covers everything you need to know about working with compounded formulations.
If you need to reconstitute a new vial, consult the 5mg reconstitution guide or the appropriate reconstitution chart for your specific vial size. The bacteriostatic water mixing guide for 5mg and the 10mg mixing guide walk through the exact volumes needed. Double-check your work against the mixing chart to ensure accuracy, and use the 5mg mixing chart or 10mg mixing chart depending on your vial.
If you are using a compounded formulation that includes B12, check the B12 combination dosage chart and the semaglutide B12 dosage chart for restart dosing. The reconstitution charts specific to your concentration are also important: 5mg reconstitution chart or 10mg reconstitution chart.
Patients who travel for surgery
Medical tourism and traveling for specialized surgical care are common. If you traveled for your procedure, you will need to manage your semaglutide supply during the trip and recovery period. The semaglutide travel guide covers cold chain management, TSA regulations, and international travel considerations. Proper peptide storage during travel is essential for maintaining medication integrity, and understanding post-reconstitution storage requirements prevents you from unknowingly using degraded medication.
Understanding dose conversions for your restart
When restarting semaglutide after surgery, accurate dosing is critical. Whether you are going back to your previous dose or re-titrating from a lower level, knowing your exact numbers prevents errors.
Unit-to-milligram conversions
If your semaglutide is measured in units on your syringe but your physician prescribed in milligrams, conversion accuracy is essential. The relationship between units and milligrams depends entirely on the concentration of your specific formulation. A common source of confusion is that different vial concentrations produce different unit-to-milligram ratios.
Review the units to mg conversion guide for a comprehensive explanation. For specific conversions, these dedicated resources cover the most common questions: 40 units in milligrams, 50 units in milligrams, 100 units in milligrams, 10 units in milligrams, and 20 units in milligrams.
For volume-based measurements, the 20 units to ml conversion is one of the most commonly referenced. You can cross-reference all of these with the syringe dosage conversion chart and the visual syringe dosage chart for hands-on accuracy.
If you are unsure whether your current dose is appropriate after surgery, the question of whether 20 units is too much is a common one, especially during re-titration when you are trying to find the right level again.
Vial-specific dosage charts
Depending on your vial size and concentration, use the appropriate chart for accurate dosing during re-titration.
For 5mg vials: The 5mg dosage chart, the 5mg/ml concentration chart, and the 5mg vial-specific chart provide the numbers you need. If you reconstituted with a specific water volume, the 5mg in 2ml chart may be most applicable.
For 10mg vials: Use the 10mg dosage chart and the 10mg vial chart for accurate re-titration dosing.
The peptide cost calculator can help you estimate the cost of the re-titration period, which will use medication at a lower rate than your maintenance dose, potentially extending the life of your current vial.
Alternative delivery methods during recovery
Some patients explore alternative semaglutide delivery methods during surgical recovery, particularly if injection sites are compromised by surgical incisions or if they want to avoid needles during a period of heightened discomfort.
Sublingual semaglutide has emerged as an option for patients who cannot or prefer not to inject. The oral semaglutide drops guide covers another non-injection option. Understanding the differences between delivery methods helps you make an informed decision about the best approach during recovery. The broader question of injectable versus oral peptide delivery is relevant here, as each route has different bioavailability profiles and onset times.
However, switching delivery methods during re-titration adds complexity. If you were using injectable semaglutide before surgery, restarting with the same delivery method is generally the most straightforward approach. Save delivery method changes for after you have re-established your baseline dose and confirmed stable tolerance.
Lifestyle factors that affect your restart success
Alcohol and semaglutide after surgery
Alcohol is generally off-limits during surgical recovery regardless of semaglutide use. But when you do resume drinking, be aware that the interaction between alcohol and semaglutide affects tolerance, blood sugar, and GI function. The alcohol and semaglutide guide covers this interaction in detail. During the restart period, avoiding alcohol entirely is the safest approach until you have re-established tolerance to the medication.
Exercise during the restart period
Physical activity during surgical recovery follows its own timeline, which may not align with your semaglutide restart. Many patients worry about weight gain when they cannot exercise and are off their medication simultaneously. The evidence suggests that semaglutide can support weight management even without exercise, so restarting the medication before you are cleared for physical activity is still beneficial.
That said, restarting semaglutide while sedentary carries a higher risk of fatigue because the drug reduces caloric intake at a time when your body is already fatigued from recovery. Monitor your energy levels carefully. If you find yourself unable to complete basic recovery tasks, such as short walks or physical therapy exercises, because of medication-related fatigue, discuss dose adjustment with your physician.
Hormonal considerations
For female patients, semaglutide can affect menstrual patterns. If your surgery coincides with hormonal fluctuations, restarting the medication during this period may amplify certain side effects. The resource on semaglutide and menstrual effects provides detailed information about what to expect.
Energy and the restart
One question patients frequently ask is whether semaglutide will give them an energy boost during recovery. The answer is nuanced. The guide on semaglutide and energy levels explains the mechanisms at play. While some patients report improved energy from better blood sugar regulation, others experience fatigue from reduced caloric intake. During surgical recovery, the fatigue side of this equation is more likely to dominate.
What to do if weight loss stalls after restarting
Re-titration means slower progress. Accept this upfront. You will not see the same rapid results you experienced when you first started semaglutide because the lower doses used during re-titration produce less appetite suppression. This is temporary.
If you have been back on your maintenance dose for several weeks and still are not seeing results, review the common causes of no weight loss after four weeks and the comprehensive troubleshooting guide for weight loss stalls. Surgical recovery can change your metabolic baseline in ways that require dose adjustment or dietary modification. The semaglutide plateau guide addresses strategies for breaking through periods of stalled progress.
SeekPeptides members have access to detailed troubleshooting protocols and personalized guidance for navigating post-surgical medication restarts, including dose optimization strategies that account for surgical recovery and changed metabolic baselines.
Working with your medical team
Restarting semaglutide after surgery is not a solo decision. It requires coordination between at minimum two physicians: your surgeon and your prescribing doctor. In some cases, an anesthesiologist, an endocrinologist, or a nutritionist may also need to be involved.
Before your surgery, create a clear plan. Who decides when to restart? What criteria must be met? What dose will you restart at? Who do you call if you have problems? Having these answers documented before you go under anesthesia prevents confusion during the foggy post-operative recovery period.
Ask your surgeon specifically about semaglutide at your pre-operative visit. Many surgeons are familiar with GLP-1 management because of how common these medications have become. But do not assume they know you are on it. Bring it up proactively. Show them your current dose, your dosing schedule, and how long you have been on the medication. This information directly impacts their surgical planning and post-operative care instructions.
For patients who are navigating the broader landscape of GLP-1 therapy, the getting started with peptides guide provides foundational context, and the peptide dosing guide covers principles that apply across all peptide medications. Understanding where semaglutide fits within the broader peptide landscape helps you have more productive conversations with your medical team.
Pharmacy and supply considerations
A surgical break means your refill schedule gets disrupted. If you are using a branded product, your next refill may need to be delayed or adjusted. If you are using a compounded formulation, you need to verify that your existing supply will still be viable when you are ready to restart.
Contact your pharmacy before surgery to discuss your planned break and coordinate refill timing. This is especially important for compounded formulations from specific pharmacies like Empower Pharmacy, Olympia Pharmacy, or Direct Meds, where production timelines and shipping schedules need to be planned in advance. The semaglutide sourcing guide and the compounded semaglutide overview cover your options for obtaining medication when you are ready to restart.
Comparing semaglutide restart with other GLP-1 medications
If you are considering whether semaglutide is still the right GLP-1 medication for you after surgery, or if your surgeon has suggested exploring alternatives, understanding the comparative landscape is important.
Tirzepatide, a dual GIP/GLP-1 agonist, has different pharmacokinetics and may have different surgical considerations. The tirzepatide onset of action differs from semaglutide, and the tirzepatide dosing protocol follows its own titration schedule. Both the dietary considerations for tirzepatide and the comparative dosage charts between the two medications provide useful context for patients evaluating their options.
The question of whether to continue with the same medication or switch during a surgical break deserves a thorough discussion with your prescribing physician. The semaglutide versus tirzepatide comparison page provides a comprehensive head-to-head analysis of both medications across multiple dimensions.
Some patients also explore combination approaches during their restart period. Adding phentermine alongside semaglutide is one approach, though the comparison between phentermine and semaglutide should be reviewed carefully, especially in the post-surgical context where stimulant medications may carry additional risks.
Long-term planning after surgical restart
Once you have successfully restarted semaglutide and returned to your maintenance dose, take stock of your situation. Surgery often represents a turning point in a weight management journey, and your approach going forward may need adjustment.
If surgery removed significant tissue, your caloric needs may have changed. If the procedure improved your mobility, you may be able to increase physical activity in ways that were not possible before. If the surgery addressed a condition that was complicating your weight management, you may find semaglutide is even more effective now.
Review your overall protocol with your prescribing physician once you are fully recovered. The long-term semaglutide use guide can help frame this conversation. Consider whether your target dose is still appropriate, whether your dietary strategy needs updating, and whether additional interventions might complement your GLP-1 therapy going forward.
SeekPeptides offers comprehensive protocol guidance for patients at every stage of their GLP-1 journey, from initial dosing through surgical breaks and beyond. Members access detailed restart protocols, dose optimization tools, and a community of experienced users who have navigated these exact challenges. The GLP-1 plotter tool helps you visualize your medication levels over time, including how they drop during a surgical break and rebuild during re-titration.
Preventing hair loss during the restart period
Rapid weight loss combined with surgical stress can trigger telogen effluvium, a temporary form of hair shedding. Adding semaglutide back into the equation can extend this shedding period if nutritional intake is not adequate. The GLP-1 and hair loss guide covers prevention strategies and what to expect. If you notice increased shedding during your restart period, increase protein intake and consider supplementation before assuming the problem requires medical intervention. Adequate nutrition is the best defense.
Managing headaches and other restart side effects
Headaches are among the most common side effects when restarting GLP-1 medications. The GLP-1 headache guide covers causes and management strategies. Dehydration, caffeine changes, blood sugar fluctuations, and the medication itself can all contribute. During the restart period, when your body is still recovering from surgery, headaches can be more frequent and more intense. Maintaining hydration, eating regularly, and following the re-titration schedule rather than jumping to higher doses too quickly are the best prevention strategies.
For patients interested in the broader category of peptides for fat loss beyond GLP-1 medications, understanding the full landscape of options can help inform long-term planning discussions with your healthcare team. The comprehensive peptides for weight loss guide covers multiple approaches, though semaglutide remains one of the most well-studied options available.
Breastfeeding and semaglutide after surgical procedures
For women who underwent cesarean section or other surgery while breastfeeding, the question of when to restart GLP-1 medications is especially complex. The GLP-1 and breastfeeding guide addresses current safety data and recommendations. In general, semaglutide is not recommended during breastfeeding, and surgical recovery adds another reason to delay restarting until the breastfeeding period has concluded.
Injection technique reminders for the restart
If it has been several weeks since your last injection, a quick refresher on technique is worthwhile. The GLP-1 injection guide covers the fundamentals, and the injection site selection guide helps you choose the best location, which is particularly important when surgical incisions limit your options. Proper technique prevents medication waste, reduces injection site reactions, and ensures consistent absorption.
The syringe injection technique guide is essential reading for patients using compounded formulations that require manual syringe preparation. And the syringe conversion chart ensures your drawn-up dose matches your intended dose, which is especially important during re-titration when precision matters most.
Frequently asked questions
Can I restart semaglutide the day after minor surgery?
For very minor procedures performed under local anesthesia with no sedation, same-day or next-day restart is generally safe if you are eating and drinking normally. However, if your procedure involved any form of sedation or general anesthesia, wait at least forty-eight hours. The deciding factor is whether your GI function has returned to baseline, not simply the time elapsed. Always confirm with your surgeon before restarting.
What happens if I restart semaglutide too early after surgery?
Restarting too early typically results in severe nausea, vomiting, and inability to eat or drink adequately. In the context of surgical recovery, this is more than uncomfortable. It can lead to dehydration, delayed wound healing, increased infection risk, and potentially hospital readmission. The safest approach is to wait until all restart criteria are met, even if that means an extra few days beyond what feels necessary.
Will I gain back all my weight during a surgical break from semaglutide?
No. A two to four week break typically results in modest weight gain, much of which is water weight and increased GI contents rather than true fat accumulation. Most patients regain two to five pounds during a short break. This weight comes off relatively quickly once the medication is restarted. The one-month results timeline can help calibrate expectations for the restart period.
Do I need to re-titrate if I only missed one dose?
No. Missing a single weekly dose does not require re-titration. You can take your next scheduled dose at the regular time. If you miss two consecutive doses, totaling approximately two weeks, you can still resume at your previous dose. Re-titration becomes necessary only when the gap exceeds two weeks.
Should I choose a different injection site after abdominal surgery?
Absolutely. Inject at least three inches away from any surgical incision to avoid disrupting healing tissue. If your surgery was on the abdomen, use the outer thigh or upper arm instead. The injection site guide covers all viable locations with visual references.
Can my surgeon prescribe semaglutide, or do I need to go back to my original prescriber?
Surgeons can prescribe semaglutide if they are comfortable managing GLP-1 therapy. However, most prefer to defer to the original prescribing physician for ongoing medication management. The ideal approach is coordinated care where your surgeon clears you for restart and your prescribing physician determines the dose and monitoring plan.
Is it safe to use semaglutide that was stored during my hospital stay?
Only if storage conditions were maintained. Semaglutide must be refrigerated between 36 and 46 degrees Fahrenheit. If the medication was left at room temperature for extended periods, or if it traveled with you to the hospital and was not properly stored, its potency may be compromised. Review temperature sensitivity guidelines and storage duration limits before using any medication that may have experienced storage interruptions.
What if I have an emergency surgery while on semaglutide?
Emergency surgery does not allow time for planned medication cessation. Your anesthesiologist will be informed that you are on a GLP-1 agonist and will use point-of-care gastric ultrasound to assess stomach contents before proceeding. They may choose rapid sequence intubation or other airway protection techniques. Post-operatively, the same restart guidelines apply, but you will need to account for whatever dose you had on board at the time of surgery when calculating your break duration.
External resources
American Society of Anesthesiologists - GLP-1 Preoperative Guidance
Society of American Gastrointestinal and Endoscopic Surgeons
For researchers and patients serious about optimizing their GLP-1 protocols through surgical breaks and beyond, SeekPeptides provides the most comprehensive resource available, with evidence-based restart guides, personalized dosing tools, and a community of thousands who have navigated these exact challenges. The peptide dosage chart library and the full suite of calculators make accurate dosing straightforward at every stage of your journey.
In case I do not see you, good afternoon, good evening, and good night. May your recovery stay smooth, your doses stay accurate, and your progress stay on track.