Mar 10, 2026

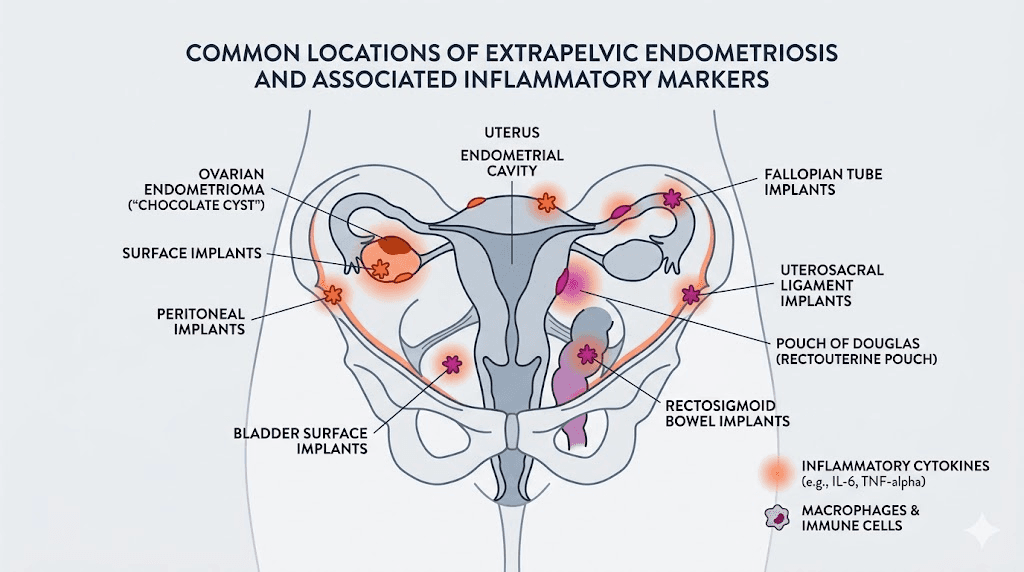
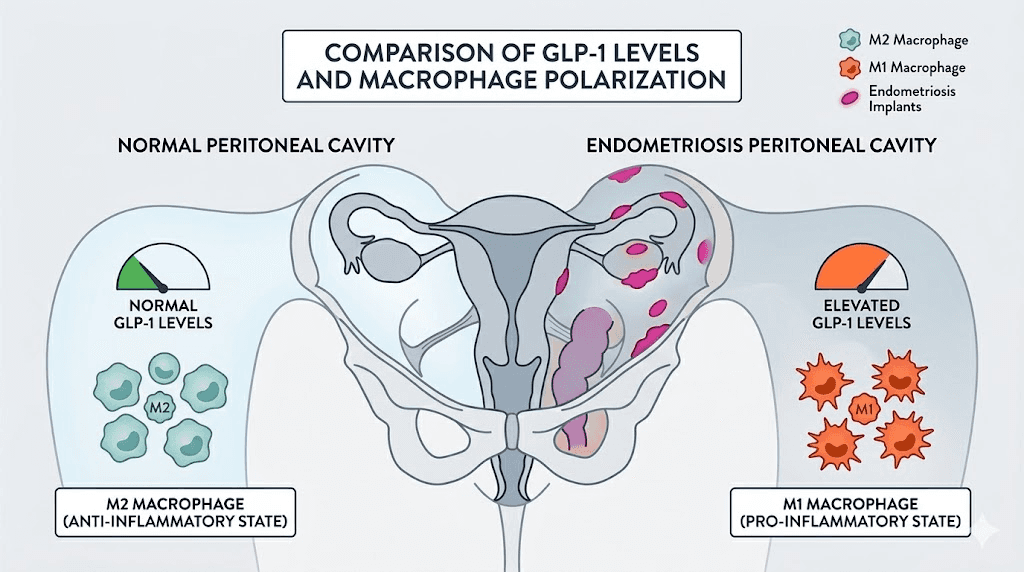
Inside the peritoneal cavity of someone with endometriosis, a quiet chemical war is raging. Inflammatory cytokines flood the space. Macrophages shift toward pro-inflammatory phenotypes. And here is something most people have never heard: GLP-1 levels in that same peritoneal fluid are significantly reduced. Not slightly. Significantly, with a p-value of 0.009 in published research. That finding alone has sparked a wave of scientific interest in whether GLP-1 receptor agonists, the same medications reshaping weight management, might offer something meaningful for the roughly 190 million women worldwide living with endometriosis.
This is not a settled question. No one has run a Phase 3 clinical trial on semaglutide for endometriosis. No regulatory body has approved any GLP-1 medication for this condition. But the biological evidence is stacking up in ways that serious researchers cannot ignore, and early survey data from endometriosis patients already using these medications tells a story worth examining carefully.
What follows is everything the current research reveals about the intersection of GLP-1 and endometriosis. The mechanisms. The data. The limitations. And what it might mean for the millions of people searching for better options than what conventional treatment currently offers.
Understanding endometriosis and why current treatments fall short
Endometriosis is a chronic inflammatory condition where tissue similar to the uterine lining grows outside the uterus. It attaches to the ovaries, fallopian tubes, pelvic lining, and sometimes organs far beyond the reproductive system. The result is pain. Sometimes debilitating pain. Sometimes pain that reshapes entire lives.
The numbers are staggering. Roughly 10% of reproductive-age women are affected, which translates to approximately 190 million people globally. In the United States alone, more than 6.5 million women carry this diagnosis. But diagnosis itself is a problem, with average delays of 7 to 10 years between symptom onset and confirmation.
Symptoms extend far beyond painful periods. Chronic pelvic pain occurs in 50 to 80% of affected individuals. Dysmenorrhea, painful intercourse, painful bowel movements, bloating (often called "endo belly"), fatigue, and depression and anxiety are all part of the picture. Infertility affects roughly 30 to 50% of those diagnosed.
Why conventional treatments are not enough
Current treatment options fall into two broad categories: hormonal therapy and surgery. Neither is a cure.
Hormonal treatments include combined oral contraceptives, progestins like dienogest, and GnRH agonists. They work by suppressing estrogen, which fuels endometrial growth. But suppressing estrogen comes with consequences. Hot flashes. Bone density loss. Mood changes, including depression. Vaginal dryness. Weight gain. And for many patients, the side effects become as burdensome as the disease itself.
GnRH agonists, considered second-line therapy, can significantly reduce lesions but create a menopausal state. Add-back therapy with low-dose hormones helps offset symptoms, but it adds complexity and cost. Danazol, an older option, carries androgenic effects like acne, hirsutism, and liver dysfunction.
Surgery, typically laparoscopic excision, removes visible lesions. It provides relief for many. But recurrence rates remain high, and repeated surgeries carry their own risks, including adhesion formation. None of these approaches address the underlying inflammatory cascade driving the disease at its core.
That gap, the one between symptom suppression and actual disease-mechanism targeting, is precisely where GLP-1 receptor agonists have entered the conversation.
What are GLP-1 receptor agonists and how do they work
GLP-1 stands for glucagon-like peptide-1. It is a hormone your body naturally produces in the gut after eating. It signals the pancreas to release insulin, slows gastric emptying, and tells the brain you are full. Simple enough.
But GLP-1 does far more than regulate blood sugar and appetite. Receptors for this hormone exist throughout the body, on immune cells, in the brain, in the cardiovascular system, in the kidneys, and in adipose tissue. When researchers began studying semaglutide and tirzepatide for weight loss and diabetes, they discovered something unexpected. These medications had powerful anti-inflammatory effects that extended well beyond metabolic improvement.
Those effects were partially independent of weight loss. Even in patients who did not lose significant weight, inflammatory markers dropped. That observation opened the door to investigating GLP-1 agonists for conditions driven primarily by inflammation rather than obesity.
The specific GLP-1 medications in current use
Three GLP-1 receptor agonists dominate the current landscape. Semaglutide is the most widely used, available as both injection and oral formulation. Tirzepatide is a dual GIP/GLP-1 agonist that targets two incretin receptors simultaneously, producing more pronounced metabolic effects. Liraglutide was the first widely adopted GLP-1 agonist, though it requires daily rather than weekly dosing.
Each works by mimicking natural GLP-1 but with modifications that dramatically extend the half-life. Natural GLP-1 survives only minutes in the bloodstream. These synthetic versions last days to weeks, maintaining sustained receptor activation throughout the dosing period. Understanding how long GLP-1 takes to start working matters for anyone considering these medications for any purpose.
The endometriosis connection: GLP-1 deficiency in the pelvis
Here is where the story gets genuinely interesting.
In a published study, researchers measured GLP-1 levels in the peritoneal fluid of women with and without endometriosis. The finding was striking. Women with endometriosis had significantly lower GLP-1 concentrations in their peritoneal fluid compared to controls, with statistical significance at p = 0.009.
This was not a minor observation. It suggested that the pelvic environment in endometriosis is actively depleted of a hormone with known anti-inflammatory properties. Proteases in the peritoneal fluid appear to degrade GLP-1 faster than normal, creating a pro-inflammatory environment where the natural braking mechanisms on inflammation are weakened.
The decreased GLP-1 levels correlated with changes in macrophage behavior. Specifically, reduced GLP-1 was associated with altered expression of the pro-inflammatory macrophage marker CD86. Macrophages are the immune cells that should be clearing endometrial debris from the pelvic cavity. When their polarization shifts, that clearance fails, and endometrial implants survive and grow where they should not.
Think about it this way. The very environment where endometriosis develops is deficient in GLP-1. And GLP-1 receptor agonists flood the system with synthetic versions of that exact molecule. The therapeutic hypothesis almost writes itself.
Five anti-inflammatory mechanisms that matter for endometriosis
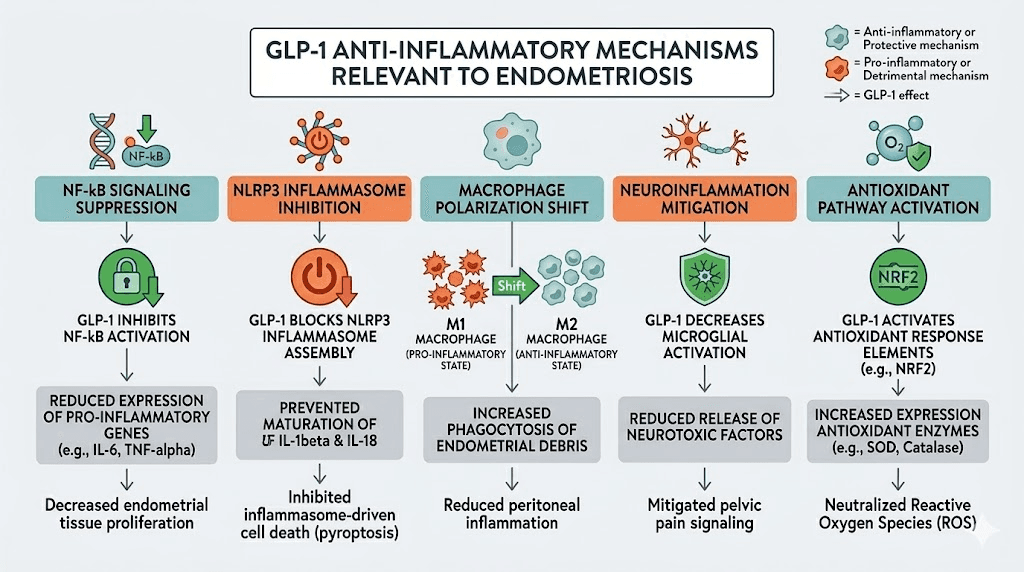
The anti-inflammatory effects of GLP-1 agonists are not vague or theoretical. They operate through specific, well-documented pathways. For endometriosis, at least five of these mechanisms are directly relevant.
NF-kB pathway inhibition
Nuclear Factor-kappa B is one of the master regulators of inflammation in the human body. When NF-kB translocates to the cell nucleus, it switches on the transcription of pro-inflammatory cytokines including TNF-alpha, IL-6, and IL-1-beta. These are precisely the cytokines elevated in the peritoneal fluid of endometriosis patients.
GLP-1 receptors are expressed on macrophages, monocytes, and endothelial cells. When GLP-1 receptor agonists activate these receptors, they prevent the nuclear translocation of NF-kB. The transcription switch stays off. The cytokine production slows. This mechanism has been demonstrated in cardiovascular research, kidney disease studies, and liver inflammation models, and the same pathway is active in the pelvic environment.
NLRP3 inflammasome suppression
The NLRP3 inflammasome is molecular machinery responsible for assembling and activating the inflammatory response. Think of it as an amplifier. When it assembles, it triggers a cytokine storm, a cascade of inflammatory signals that recruit more immune cells and perpetuate the cycle.
GLP-1 agonism blocks NLRP3 inflammasome assembly. This is not subtle modulation. It is a direct blockade of one of the primary engines driving chronic inflammatory states. For a disease like endometriosis, where chronic inflammation is not a side effect but the central mechanism, this matters enormously.
Macrophage polarization from M1 to M2
Macrophages exist on a spectrum. M1 macrophages are pro-inflammatory. They produce cytokines, recruit other immune cells, and amplify the inflammatory response. M2 macrophages are anti-inflammatory. They promote tissue repair, resolve inflammation, and clear cellular debris.
In endometriosis, macrophages in the peritoneal fluid tend toward the M1 phenotype, perpetuating inflammation and allowing endometrial implants to establish and grow. GLP-1 receptor agonists have been shown to shift macrophage polarization toward the M2 phenotype, the anti-inflammatory direction. This shift could improve the immune system ability to clear misplaced endometrial tissue rather than feeding it with inflammatory signals.
This mechanism connects directly to the immune system optimization that researchers study across multiple peptide categories.
Central sensitization and neuroinflammation reduction
Chronic pain in endometriosis is not solely about peripheral tissue damage. Over time, the central nervous system itself becomes sensitized. Pain signals amplify. The brain begins interpreting normal stimuli as painful. This process, called central sensitization, involves neuroinflammation, specifically activation of microglial cells in the brain and spinal cord.
GLP-1 receptors exist in the dorsal vagal complex of the brainstem. When GLP-1 agonists reach these receptors, they reduce microglial activation and dampen neuroinflammatory signals. For endometriosis patients who experience pain far out of proportion to visible disease, or who continue experiencing pain even after surgical excision of lesions, this central mechanism could explain why some report meaningful improvement on GLP-1 medications.
The connection between brain health and chronic pain is one of the most important frontiers in endometriosis research.
Antioxidant pathway enhancement
Oxidative stress is elevated in the peritoneal environment of endometriosis patients. Reactive oxygen species damage tissue, fuel inflammation, and promote the survival of ectopic endometrial cells. GLP-1 agonists upregulate antioxidant enzymes including HO-1 (heme oxygenase-1) and NQO1 (NAD(P)H quinone dehydrogenase 1), providing a counterbalance to the oxidative damage occurring in the pelvis.
This antioxidant enhancement works alongside the anti-inflammatory effects, addressing two of the three primary pathological drivers of endometriosis simultaneously. The third driver, estrogen dependence, is also potentially influenced by GLP-1 medications, through a different mechanism entirely.
The estrogen connection: how weight loss changes the equation
Endometriosis is an estrogen-dependent disease. Endometrial implants have their own aromatase activity, meaning they can produce estrogen locally. But systemic estrogen levels also matter, and adipose tissue is a significant source of estrogen production through peripheral aromatase conversion.
GLP-1 receptor agonists produce substantial weight loss. The international survey of endometriosis patients on GLP-1 medications found a mean weight reduction of 12.07 kilograms. That is not trivial. Reduced adipose tissue means reduced peripheral aromatase activity, which means lower systemic estrogen levels. Less estrogen feeding the endometrial implants.
This creates an indirect but potentially meaningful therapeutic effect. Unlike GnRH agonists that create an artificial menopause to suppress estrogen, the weight-mediated estrogen reduction through GLP-1 agonists is more physiological. It does not cause the same bone density loss, hot flashes, or mood disruption that characterizes estrogen-suppressive therapies.
For patients interested in understanding peptides for weight loss in women, this connection between adipose tissue reduction and hormonal balance adds another dimension to consider. The semaglutide dosage calculator can help determine appropriate starting points for those exploring these medications.
Insulin sensitization and aromatase activity
There is another layer. Insulin resistance increases aromatase activity. When cells respond poorly to insulin, the body compensates by producing more, and elevated insulin drives aromatase expression in both adipose tissue and endometrial tissue. GLP-1 agonists improve insulin sensitivity directly, independent of weight loss, which further reduces aromatase-driven estrogen production.
This dual mechanism, weight-mediated and insulin-mediated aromatase reduction, may explain why some endometriosis patients see improvements that seem disproportionate to their weight loss alone. The metabolic correction runs deeper than the scale suggests.
Progesterone resistance: a key piece of the puzzle
One of the most frustrating aspects of endometriosis treatment is progesterone resistance. In a healthy uterine lining, progesterone counterbalances estrogen and promotes tissue stability. But endometrial implants in endometriosis often have reduced progesterone receptor expression. They do not respond to progesterone the way they should.
This is why progestin therapy, while helpful for some, fails completely for others. The tissue it is supposed to calm simply does not have enough receptors to hear the signal.
Laboratory research has revealed something remarkable. In endometrial cell models, GLP-1 agonists increased progesterone receptor expression. The cells became more responsive to progesterone signaling. When GLP-1 agonists were combined with progestin therapy, the response was stronger than with progestin alone.
If this translates from laboratory models to human tissue, it could mean GLP-1 medications make existing hormonal therapies more effective. A patient who failed progestin therapy might respond when GLP-1 agonism restores the receptor expression those progestins need to work.
This is still speculative for clinical endometriosis. But the laboratory data is clear, and it aligns with the clinical observations of patients who report improvement when adding GLP-1 medications to their existing treatment regimens. Understanding peptide interactions with hormone balance is critical for anyone navigating these complex treatment decisions.
What the survey data actually shows
While we wait for randomized controlled trials, the best clinical evidence we have comes from an international cross-sectional survey of endometriosis patients who used GLP-1 receptor agonists. The study recruited participants through endometriosis advocacy platforms, social media, and clinical networks, targeting women aged 18 to 55 with confirmed or suspected endometriosis and current or prior GLP-1 medication use.
The results deserve careful examination.
Medication breakdown
Among participants, 75.2% used semaglutide and 19.9% used tirzepatide. The remaining small percentage used liraglutide or other GLP-1 agents. This distribution mirrors the general GLP-1 market, where semaglutide dominates prescribing patterns.
Symptom improvement rates
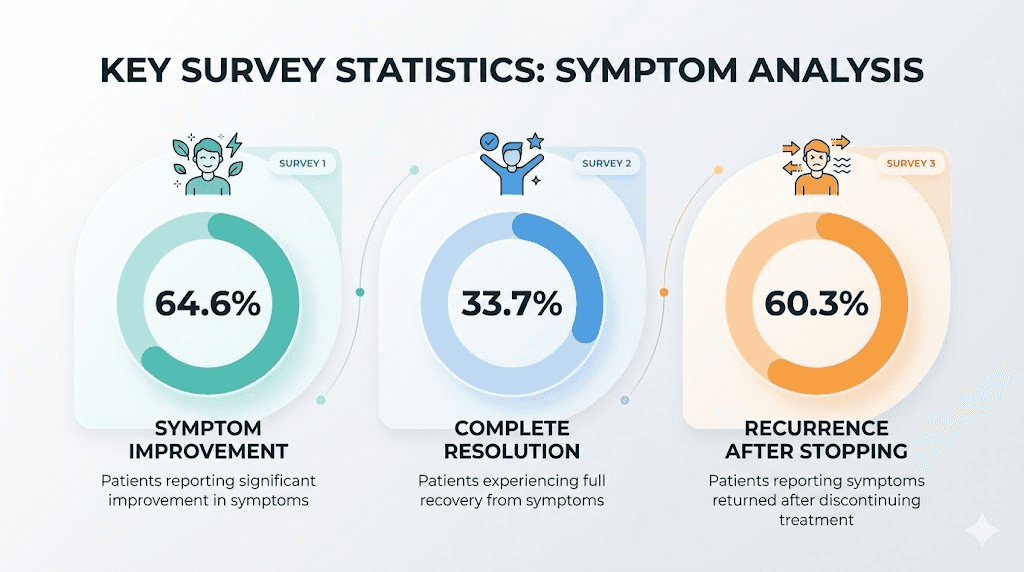
Overall, 64.6% of respondents reported improvement in at least one endometriosis-related symptom. That is nearly two-thirds of participants experiencing some degree of benefit. Even more striking, 33.7% reported complete resolution of at least one symptom. Not improvement. Resolution.
The specific symptoms showing significant improvement included pelvic pain, bloating, and lower back pain. These are three of the most debilitating and treatment-resistant symptoms in endometriosis. The fact that meaningful numbers of patients reported improvement in all three is noteworthy.
Weight loss correlation
Mean weight reduction across participants was 12.07 kilograms. Greater weight loss correlated with greater improvement in overall quality of life scores. This correlation does not tell us whether the symptom improvement was driven by weight loss, direct anti-inflammatory effects, or both, but it confirms that the metabolic improvements tracked alongside the symptom improvements.
For context on what to expect from these medications, resources on semaglutide results week by week and tirzepatide weight loss timeline provide detailed breakdowns.
Quality of life improvements
Multiple quality-of-life domains showed significant improvement. This extends beyond just pain scores. Participants reported improvements in daily functioning, emotional wellbeing, and overall life satisfaction. The medication and alternative therapy use among participants also decreased significantly, suggesting that GLP-1 medications may reduce the need for additional symptom management strategies.
The recurrence problem
Among those who discontinued GLP-1 therapy, 60.3% reported symptom recurrence. This is important for several reasons. First, it suggests that the benefits require ongoing treatment rather than producing permanent changes. Second, it argues against a pure placebo effect, because placebo responses tend to diminish more gradually. Third, it raises questions about the optimal duration of therapy and whether intermittent dosing might maintain benefits.
Understanding semaglutide withdrawal symptoms and what happens when stopping these medications provides additional context for this finding.
Semaglutide and endometriosis: the most studied connection
As the most widely prescribed GLP-1 agonist, semaglutide has the most patient-reported data for endometriosis-related outcomes. Beyond the survey data discussed above, individual case reports and patient communities describe a range of experiences.
Some patients describe surprisingly meaningful symptom relief. Less bloating. Fewer flares. Improved pain levels. Reduced reliance on pain medications. Better energy, which matters deeply for people managing semaglutide-related fatigue or the bone-deep exhaustion that endometriosis itself produces.
Others notice no change in endometriosis symptoms despite significant weight loss, which suggests the anti-inflammatory benefits do not affect all patients equally. And some experience worsening gastrointestinal symptoms, particularly bloating, constipation, and nausea, that overlap uncomfortably with endometriosis symptoms and make it difficult to determine what is causing what.
Fibrosis research
One particularly interesting finding comes from research on semaglutide and fibrosis. In intrauterine adhesion models, semaglutide demonstrated anti-fibrotic properties, inhibiting epithelial-mesenchymal transition (the process by which epithelial cells transform into fibrotic, scar-like tissue). Endometriosis involves significant fibrosis, and anti-fibrotic effects could theoretically reduce adhesion formation and tissue scarring that contributes to pain and organ dysfunction.
This research is preclinical, conducted in laboratory models rather than human endometriosis tissue. But it adds another mechanistic thread to the case for investigating semaglutide in endometriosis patients. Those interested in the broader effects of semaglutide should explore the benefits beyond weight loss that research continues to uncover.
Menstrual cycle considerations
For people with endometriosis, anything that affects the menstrual cycle warrants attention. Research has shown that GLP-1 medications can influence menstrual patterns. Understanding how semaglutide affects your period and how tirzepatide affects your period is essential for endometriosis patients considering these medications. Changes in cycle length, flow, and timing have been reported, though the relationship between these changes and endometriosis symptom improvement is not yet understood.
Tirzepatide and endometriosis: the dual-agonist advantage
Tirzepatide offers something semaglutide does not: dual agonism of both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors. This dual mechanism produces more pronounced weight loss in clinical trials compared to semaglutide alone, which could mean greater estrogen reduction through adipose tissue loss.
Whether the additional GIP receptor activation provides extra anti-inflammatory benefit for endometriosis specifically remains unknown. GIP receptors are present on immune cells, and GIP itself has demonstrated immunomodulatory properties in laboratory studies. But no research has examined the difference between single-agonist (semaglutide) and dual-agonist (tirzepatide) approaches specifically for endometriosis outcomes.
In the international survey, 19.9% of participants used tirzepatide. The study did not break down results by specific medication, so we cannot determine whether tirzepatide users experienced more or less improvement than semaglutide users. A detailed semaglutide vs tirzepatide comparison covers the broader differences between these medications, and the side effect comparison is particularly relevant for endometriosis patients weighing options.
Microdosing considerations
Some endometriosis patients are exploring microdosing tirzepatide for inflammation rather than using standard weight-loss doses. The theory is that lower doses might provide anti-inflammatory benefit with fewer gastrointestinal side effects. This approach is entirely off-label and unvalidated, but it reflects the creative problem-solving that patients pursue when conventional options fail.
Understanding the tirzepatide dosage in units and semaglutide dosage in units helps patients and clinicians discuss dosing strategies more precisely. The microdosing tirzepatide chart provides a visual reference for these lower-dose protocols.
The Warburg effect: endometriosis as a metabolic disease
Emerging research is reframing endometriosis as a metabolic disease, not just a reproductive one. Endometriotic lesions exhibit what researchers call Warburg-like metabolic effects, relying heavily on glycolysis even in the presence of oxygen. This metabolic pattern, first identified in cancer cells, allows endometrial implants to survive and proliferate in ectopic locations.
GLP-1 receptor agonists influence cellular metabolism at a fundamental level. They improve mitochondrial function, reduce reliance on glycolysis, and restore normal metabolic patterns in multiple tissue types. If endometriotic lesions rely on aberrant metabolism for survival, medications that correct metabolic dysfunction could theoretically undermine the metabolic support those lesions depend on.
This metabolic perspective also connects endometriosis to the broader category of autoimmune and inflammatory conditions where GLP-1 agonists show promise. The same metabolic dysfunction that characterizes endometriosis appears in varying degrees across Hashimoto thyroiditis and other conditions where chronic inflammation drives tissue damage.
It is a paradigm shift. If endometriosis is partly a metabolic disease, then metabolic medications are not treating a side effect. They are addressing a root cause.
Practical considerations for endometriosis patients
SeekPeptides members frequently ask about practical aspects of GLP-1 medication use, and these questions become even more important when endometriosis is part of the picture. Here is what current evidence and clinical experience suggest.
Starting a GLP-1 medication with endometriosis
The standard approach applies: start low, titrate slowly. For semaglutide, that typically means beginning at 0.25mg weekly and increasing gradually. For tirzepatide, 2.5mg weekly is the standard starting dose. The first week on semaglutide guide covers what to expect during the initial period.
Slow titration matters more for endometriosis patients because gastrointestinal side effects from GLP-1 medications overlap with endometriosis symptoms. Nausea, bloating, and constipation can worsen temporarily, making it crucial to distinguish medication side effects from disease flares. Keeping a symptom diary during the first 4 to 8 weeks helps separate these overlapping symptom sources.
For injection guidance, understanding where to inject GLP-1, the best injection sites, and how to inject properly ensures consistent medication delivery.
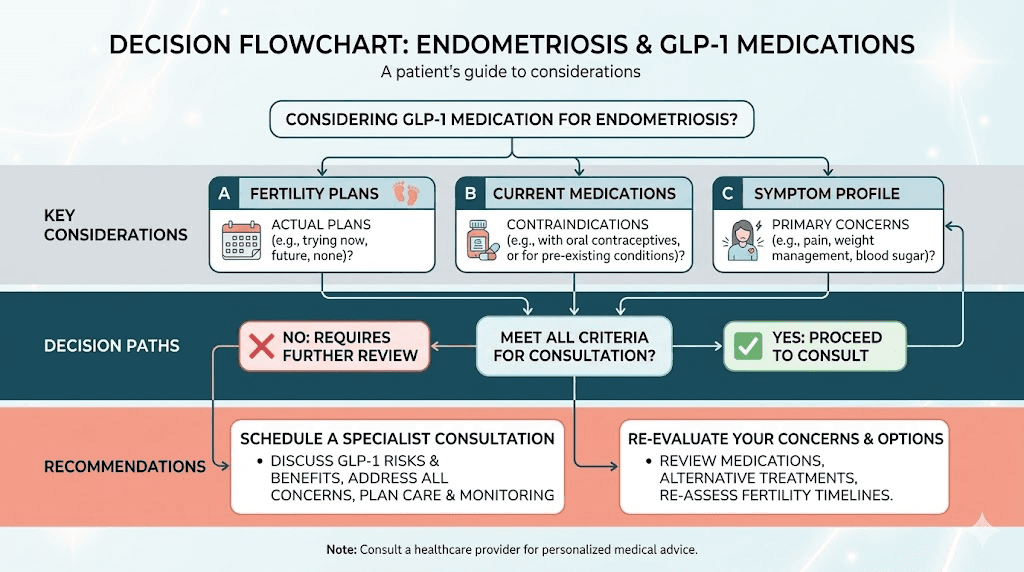
Drug interactions with endometriosis treatments
This is critical. GLP-1 medications slow gastric emptying, which can reduce the absorption of oral medications. If you take oral contraceptives or oral progestins for endometriosis management, the delayed gastric emptying from GLP-1 agonists may reduce their effectiveness.
This does not mean you cannot use both. But it means discussing timing and potentially switching to non-oral formulations (patches, injections, IUDs) for hormonal endometriosis treatment if you are also taking a GLP-1 medication. Your prescribing clinician needs to know about all medications you are taking.
For those interested in the interaction between GLP-1 medications and other compounds, understanding supplements to take with tirzepatide and formulations like semaglutide with B12 or tirzepatide with B12 provides useful context.
Fertility considerations
Endometriosis and fertility are deeply intertwined, with 30 to 50% of affected individuals experiencing difficulty conceiving. GLP-1 medications must be discontinued before conception. Current guidelines recommend stopping semaglutide at least two months before attempting pregnancy.
Recent research has raised questions about the impact of GLP-1 receptor agonists on endometrial receptivity and implantation. A study published in Acta Obstetricia et Gynecologica Scandinavica explored the "hidden impact" of these medications on the endometrial environment needed for embryo implantation. While the full implications are still being studied, this is a conversation every endometriosis patient of reproductive age should have with their fertility specialist before starting a GLP-1 medication.
Resources on GLP-1 and breastfeeding, tirzepatide while breastfeeding, and pregnancy on tirzepatide address related reproductive concerns.
Side effects that overlap with endometriosis symptoms
One of the practical challenges of using GLP-1 medications for endometriosis is the significant overlap in side effect profiles. Understanding what comes from the medication versus what comes from the disease requires careful attention.
Gastrointestinal effects
GLP-1 medications commonly cause nausea, bloating, constipation, and diarrhea. Endometriosis commonly causes bloating (endo belly), constipation, diarrhea, and nausea. The overlap is almost complete.
During the first weeks of GLP-1 therapy, many patients experience a temporary worsening of GI symptoms before they improve. For someone already managing endo belly, this worsening period can feel like a disease flare. Detailed guides on managing tirzepatide bloating, tirzepatide constipation, tirzepatide diarrhea duration, and semaglutide constipation treatment can help distinguish between medication effects and disease symptoms.
Fatigue and energy
Both endometriosis and GLP-1 medications can cause fatigue. GLP-1-related fatigue is well-documented, as is the crushing exhaustion many endometriosis patients experience. Monitoring energy levels through the treatment transition period helps determine whether the medication improves, worsens, or has no effect on endometriosis-related fatigue. Some patients actually report improved energy once the initial adjustment period passes, as described in our guide on semaglutide and energy.
Headaches
Headaches occur with both GLP-1 medications and endometriosis. The GLP-1 headache guide, tirzepatide headache information, and tirzepatide headache treatment resources help differentiate and manage this overlapping symptom.
Mood and mental health
Endometriosis significantly impacts mental health. Depression and anxiety are common comorbidities. GLP-1 medications can cause mood changes in some patients. Tirzepatide and anxiety research provides context on this potential interaction. Monitoring mental health during the transition to GLP-1 therapy is essential, and any significant mood changes should prompt immediate discussion with a healthcare provider.
Musculoskeletal symptoms
Endometriosis frequently involves lower back pain and body aches. Some GLP-1 medication users report muscle pain and body aches as side effects. Again, the overlap complicates assessment. The survey data found lower back pain among the symptoms showing significant improvement, which suggests that for many patients, the net effect is positive despite potential side effects.
Bone density concerns
Rapid weight loss from any cause can affect bone density. For endometriosis patients who have already experienced bone density reduction from GnRH agonist therapy, adding another potential contributor to bone loss requires careful monitoring. DEXA scans before starting and periodically during GLP-1 therapy provide objective tracking.
Nutrition and lifestyle on GLP-1 medications with endometriosis
Managing nutrition becomes doubly important when combining GLP-1 medication use with endometriosis. Reduced appetite means every calorie consumed needs to count more.
Anti-inflammatory nutrition principles align with both endometriosis management and GLP-1 medication support. Omega-3 fatty acids, leafy greens, colorful vegetables, lean proteins, and foods rich in antioxidants address the inflammatory component of endometriosis while supporting nutritional needs during weight loss.
Detailed nutritional guidance is available through several resources: best foods to eat on semaglutide, foods to avoid on tirzepatide, tirzepatide diet plan, semaglutide diet plan, and complete food lists for semaglutide users.
Alcohol interactions also deserve mention. Both endometriosis and GLP-1 medications affect how the body processes alcohol. Guides on drinking on semaglutide and drinking on tirzepatide cover this topic in detail.
GLP-1 breakfast ideas and dinner ideas provide practical meal suggestions that support both anti-inflammatory goals and adequate nutrition on reduced appetite.
GLP-1 and endometriosis-related cancer risk
A recent study examined the effects of GLP-1 receptor agonists on incident gynecologic cancer outcomes in endometriosis patients compared to metformin. Endometriosis increases the risk of certain gynecologic cancers, particularly ovarian cancer, and any medication that modulates the endometrial environment needs cancer risk assessment.
The anti-inflammatory and metabolic effects of GLP-1 agonists could theoretically reduce cancer risk by lowering inflammation and improving metabolic parameters. However, the research is in very early stages, and no definitive conclusions about cancer protection or risk can be drawn from current data.
This is an area where future research will be critically important. For now, the standard cancer screening recommendations for endometriosis patients should continue regardless of GLP-1 medication use.
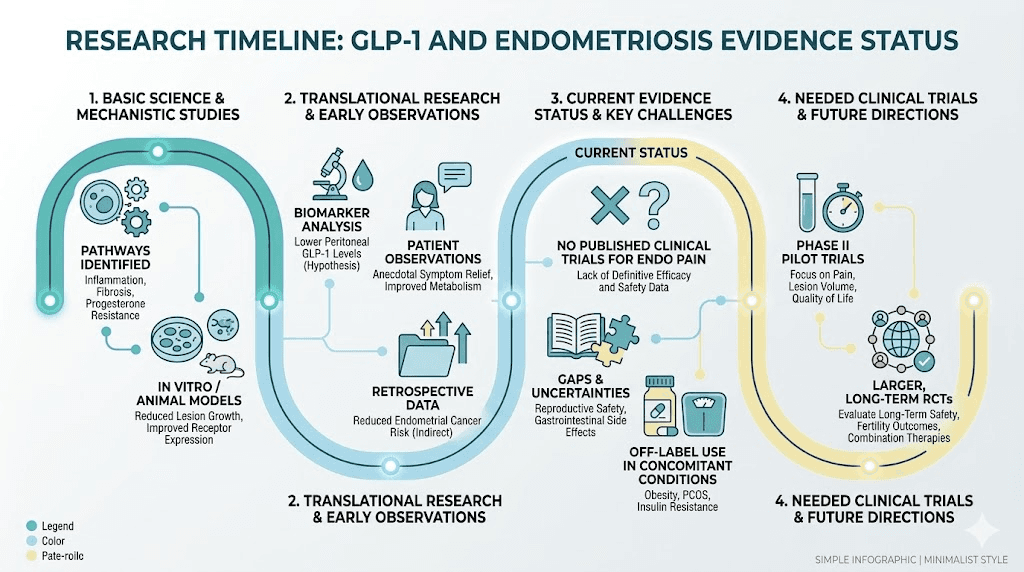
What we still do not know
Intellectual honesty requires acknowledging the enormous gaps in current evidence. Here is what we do not know.
We do not know whether GLP-1 agonists actually reduce endometriotic lesion size. The symptom improvement reported in surveys could result from anti-inflammatory effects that reduce pain without changing disease extent. Only imaging studies and surgical follow-up could answer this question.
We do not know the optimal dose for endometriosis benefit. Standard weight-loss doses may be too high, causing unnecessary side effects. Lower doses might provide anti-inflammatory benefit with better tolerability. Without dose-finding studies, this remains guesswork.
We do not know which endometriosis patients are most likely to respond. The survey showed 64.6% improved, but 35.4% did not. What distinguishes responders from non-responders? We have no idea. Possible factors include disease stage, lesion location, inflammatory profile, and metabolic status, but none of this has been studied.
We do not know whether the effects are sustained long-term. The 60.3% recurrence rate after stopping suggests ongoing treatment is needed, but long-term safety data for this specific population does not exist.
We do not know whether semaglutide, tirzepatide, or liraglutide is most effective for endometriosis. The survey did not compare medications head-to-head, and no controlled study has been conducted.
We do not know whether GLP-1 medications interact with endometriosis pathology in ways we have not considered. The positive effects may come with trade-offs we have not measured.
These knowledge gaps are not reasons to dismiss the research. They are reasons to interpret it carefully and to advocate for proper clinical trials. Large Phase 3 randomized controlled trials specific to endometriosis and GLP-1 medications are described as being in "nascent stages." Until they are completed, we are working with biological plausibility, mechanistic evidence, and self-reported survey data, valuable but incomplete.
Comparing GLP-1 to conventional endometriosis treatments
How do GLP-1 medications stack up against the treatments currently available for endometriosis? This comparison requires major caveats, since GLP-1 medications are not approved for endometriosis and the evidence base is incomparable. But for patients and clinicians weighing options, a framework helps.
Factor | Hormonal therapy (progestins, COCs) | GnRH agonists | Surgery | GLP-1 agonists (investigational) |
|---|---|---|---|---|
Mechanism | Estrogen suppression | Complete estrogen suppression | Physical removal | Anti-inflammatory, metabolic |
Pain relief | Moderate for many | Significant | Significant (variable durability) | 64.6% report improvement (survey) |
Bloating improvement | Variable | Some improvement | Variable | Significant improvement (survey) |
Fertility preservation | Suppresses ovulation | Creates menopause | Can improve fertility | Discontinue before conception |
Bone density | Generally preserved | Loss without add-back | No direct effect | Potential loss with rapid weight loss |
Weight effect | Possible gain | Variable | No direct effect | Significant loss (mean 12 kg) |
Approval status | Approved | Approved | Standard of care | Not approved for endometriosis |
The key distinction is that conventional treatments primarily target hormonal pathways (suppressing estrogen), while GLP-1 agonists target inflammatory and metabolic pathways. These approaches are not mutually exclusive. A patient could potentially benefit from combining hormonal therapy with GLP-1 treatment, addressing different aspects of the disease simultaneously.
The phentermine vs GLP-1 comparison addresses another question some patients have about weight management alternatives, while the broader peptides for weight loss guide covers the full landscape of options.
The role of other peptides in endometriosis management
GLP-1 agonists are not the only peptides with potential relevance to endometriosis. The broader peptide landscape includes several compounds with anti-inflammatory, immune-modulating, or tissue-repair properties that researchers are investigating for inflammatory conditions.
KPV peptide is an alpha-MSH derivative with potent anti-inflammatory properties that works through NF-kB inhibition, the same pathway affected by GLP-1 agonists. BPC-157 demonstrates tissue-healing and anti-inflammatory properties in research models. Thymalin and immune-modulating peptides address the immune dysregulation component of endometriosis from different angles.
Understanding what peptides are and how they work provides foundational knowledge for evaluating these options. The peptide safety guide covers essential risk considerations, and best peptides for women addresses gender-specific considerations that are particularly relevant for endometriosis patients.
SeekPeptides provides comprehensive resources on these peptide categories, including detailed mechanism guides, dosing protocols, and stacking strategies for those exploring multi-compound approaches.
Emerging GLP-1 medications and future research directions
The GLP-1 medication landscape is expanding rapidly. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously, is advancing through clinical trials and may offer even more pronounced anti-inflammatory and metabolic effects than current options. Mazdutide, cagrilintide, and orforglipron (an oral GLP-1 agonist) represent additional next-generation options that could offer different benefit-risk profiles for endometriosis patients.
New delivery methods are also emerging. GLP-1 patches, oral drops, and tablet formulations may improve accessibility and tolerability for patients who struggle with injectable medications.
The research directions that matter most for endometriosis include randomized controlled trials comparing GLP-1 medications to placebo in confirmed endometriosis patients, imaging studies assessing whether lesion size changes with GLP-1 treatment, biomarker studies identifying which patients are most likely to respond, and combination studies examining whether GLP-1 medications enhance the effectiveness of conventional hormonal treatments.
The GLP-1 legal landscape is also evolving, with implications for access and availability that endometriosis patients should monitor.
What to discuss with your doctor
If you have endometriosis and are considering a GLP-1 medication, whether for weight management, metabolic health, or potential anti-inflammatory benefit, here are the essential conversations to have with your healthcare provider.
First, discuss your complete medication list. The interaction between GLP-1 medications and oral hormonal treatments can affect absorption and efficacy. Your provider may need to adjust formulations or timing.
Second, discuss fertility plans. If conception is in your near future, the timing of GLP-1 medication use needs careful planning. The impact on endometrial receptivity is still being studied, and a washout period before attempting pregnancy is essential.
Third, discuss monitoring. Baseline inflammatory markers (CRP, ESR, IL-6 if available), imaging of known endometriotic lesions, a bone density scan if you have had prior GnRH agonist use, and metabolic parameters provide objective data to track whether the medication is producing measurable changes.
Fourth, discuss realistic expectations. GLP-1 medications are not approved for endometriosis. The evidence is promising but preliminary. Improvement is possible but not guaranteed. The 64.6% improvement rate from the survey means 35.4% of patients did not report benefit.
Fifth, discuss access and cost. GLP-1 medications prescribed off-label for endometriosis may not be covered by insurance. Understanding the BMI requirements for GLP-1 prescriptions and insurance coverage options helps navigate the financial aspects. Compounded semaglutide and compounded tirzepatide represent potential lower-cost alternatives, though quality and consistency considerations apply.
The bigger picture: endometriosis and metabolic health
The GLP-1 and endometriosis connection is part of a larger scientific shift toward understanding endometriosis as a systemic metabolic and inflammatory disease rather than a purely reproductive condition. This shift has profound implications for treatment approaches.
If endometriosis involves systemic inflammation, then systemic anti-inflammatory approaches make biological sense. If it involves metabolic dysfunction, then metabolic correction is therapeutically rational. If it involves immune dysregulation, then immunomodulation deserves investigation.
GLP-1 receptor agonists happen to address all three of these dimensions simultaneously. That convergence is rare in pharmacology, and it explains why the research interest is so intense despite the absence of formal clinical trials.
For the millions of people living with endometriosis who have exhausted conventional options or cannot tolerate their side effects, the emerging evidence around GLP-1 medications represents genuine, if cautious, hope. Not a cure. Not a miracle. But a new mechanistic approach to a disease that desperately needs fresh thinking.
SeekPeptides members access detailed protocols, evidence-based guides, and a community of experienced researchers navigating these exact questions. For anyone serious about understanding peptide options for women and perimenopause management, the depth of resources available goes far beyond what any single article can cover.
Frequently asked questions
Can GLP-1 medications cure endometriosis?
No. No medication currently cures endometriosis. GLP-1 receptor agonists may reduce symptoms through anti-inflammatory and metabolic mechanisms, but they do not eliminate endometrial implants or cure the underlying condition. The 60.3% symptom recurrence rate after discontinuation confirms that ongoing treatment appears necessary for sustained benefit.
Which GLP-1 medication is best for endometriosis?
No head-to-head comparison exists for endometriosis specifically. In the international survey, 75.2% of participants used semaglutide and 19.9% used tirzepatide. Both showed benefit, but results were not broken down by medication. The semaglutide vs tirzepatide comparison covers broader differences that may help guide decisions.
Will my insurance cover GLP-1 medications for endometriosis?
Likely not for endometriosis specifically, since these medications are not approved for this indication. However, if you also meet criteria for obesity (BMI 30+) or overweight with comorbidities (BMI 27+), you may qualify for coverage under weight management indications. The insurance coverage guide provides detailed information.
Can I take a GLP-1 medication while on birth control for endometriosis?
Yes, but with important caveats. GLP-1 medications slow gastric emptying, which can reduce absorption of oral contraceptives. Consider non-oral contraceptive methods (IUD, patch, implant) or discuss timing strategies with your prescriber. Never stop hormonal endometriosis treatment without medical guidance.
How long before I might notice endometriosis symptom improvement on a GLP-1 medication?
The survey data did not specify timeline to improvement. Based on general GLP-1 timelines, anti-inflammatory effects likely begin within weeks, but meaningful symptom changes may take 2 to 3 months as both direct effects and weight-mediated estrogen reduction accumulate. Expect initial GI side effects to potentially worsen endometriosis symptoms before improvement occurs.
Are there endometriosis-specific dosing protocols for GLP-1 medications?
No. No validated endometriosis-specific dosing exists. Standard titration protocols are used. Some patients and clinicians are exploring microdosing for inflammation rather than full weight-loss doses, but this approach is entirely unvalidated. Use the semaglutide dosage calculator or tirzepatide dosage calculator to understand standard dosing frameworks.
Should I stop my current endometriosis medications before starting a GLP-1?
Generally no. GLP-1 medications appear to complement rather than replace conventional endometriosis treatments. The laboratory evidence that GLP-1 agonists increase progesterone receptor expression suggests they may actually enhance the effectiveness of progestin therapy. Any medication changes should be discussed with your prescribing physician.
Does weight loss from GLP-1 medications help endometriosis even without direct anti-inflammatory effects?
Likely yes. Adipose tissue produces estrogen through aromatase conversion. Reducing adipose tissue lowers systemic estrogen, which can reduce stimulation of endometrial implants. The mean weight loss of 12.07 kg in the survey represents a meaningful reduction in estrogen-producing tissue. However, the anti-inflammatory effects of GLP-1 agonists appear to provide benefit beyond what weight loss alone would explain.
External resources
Acta Obstetricia et Gynecologica Scandinavica - GLP-1 and Endometrial Receptivity
PubMed - GLP-1 Levels in Peritoneal Fluid of Women with Endometriosis
In case I do not see you, good afternoon, good evening, and good night. May your inflammation stay quiet, your research stay thorough, and your protocols stay effective.