Mar 21, 2026

Before you combine these two medications, stop and read this entire guide. That is not a suggestion. It is a warning born from the dozens of questions flooding online forums every week, questions from real people who take bupropion for depression and want to add tirzepatide for weight loss but have no idea whether the combination is safe. The short answer is that no direct drug interaction has been identified between wellbutrin and tirzepatide. The longer answer, the one that actually matters, involves gastric emptying changes, seizure threshold concerns, overlapping side effects, and a mental health landscape that shifts dramatically when you start losing weight rapidly. If you are currently taking bupropion and considering tirzepatide for weight loss, you need more than a simple yes or no. You need to understand how these medications interact with your body individually before you can grasp what happens when they work simultaneously. You need to know what to monitor, when to worry, and what conversations to have with your prescriber. This guide covers every angle of the wellbutrin and tirzepatide combination, from pharmacology to practical protocols, from side effect management to mental health considerations. Read it carefully. Your safety depends on understanding the details, not just skimming the headlines.
What bupropion actually does in the body
Bupropion, sold under the brand name Wellbutrin, is not your typical antidepressant. Most antidepressants target serotonin. Bupropion ignores serotonin almost entirely and instead focuses on two other neurotransmitters that play critical roles in mood, motivation, and energy: dopamine and norepinephrine.
This distinction matters enormously when we talk about combining it with tirzepatide. Selective serotonin reuptake inhibitors, the SSRIs like fluoxetine and sertraline, tend to cause weight gain. Bupropion does not. In fact, bupropion is one of the only antidepressants associated with modest weight loss rather than weight gain, which is precisely why so many people taking it become interested in tirzepatide weight loss protocols in the first place.
The mechanism works like this. Bupropion blocks the reuptake of dopamine and norepinephrine at the synaptic cleft, meaning more of these neurotransmitters remain available for your neurons to use. Dopamine drives reward, motivation, and pleasure. Norepinephrine drives alertness, energy, and the fight-or-flight response. Together, they create a neurochemical environment that reduces depressive symptoms while simultaneously providing a mild stimulant-like effect.
Bupropion comes in three formulations. The immediate-release version is taken two to three times daily. The sustained-release version, Wellbutrin SR, is typically taken twice daily. The extended-release version, Wellbutrin XL, is taken once daily. Doses range from 150mg to a maximum of 450mg per day, though most prescribers keep patients at 300mg daily as the standard therapeutic dose. Understanding these dosing details becomes important when we discuss timing protocols later in this guide.
There are several critical things to know about bupropion before adding any medication to it. First, it lowers the seizure threshold. This is the single most important safety consideration with this drug. The risk is dose-dependent, meaning higher doses carry higher risk, and it increases significantly above 450mg daily. Second, bupropion can raise blood pressure in some individuals, a concern that becomes relevant when combined with medications that cause fluid shifts. Third, it causes nausea in a meaningful percentage of users, particularly during the first few weeks of treatment. Keep that nausea detail in mind. It will become very relevant when we discuss what happens when tirzepatide enters the picture.
Beyond depression, bupropion is prescribed for seasonal affective disorder, smoking cessation under the brand name Zyban, and as part of the combination drug Contrave, which pairs bupropion with naltrexone specifically for weight management. That last point is particularly interesting. The FDA already approved bupropion as part of a weight loss medication, which tells us something about its compatibility with weight management strategies and how researchers have studied appetite suppression mechanisms across different drug classes.
One additional detail about bupropion that becomes relevant when combined with GLP-1 therapy concerns its effect on energy. Many patients describe a noticeable increase in energy and motivation when starting bupropion, a welcome change from the lethargy that depression causes and from the fatigue some people experience on tirzepatide. The norepinephrine boost creates a sense of alertness that can help maintain activity levels during the calorie deficit that tirzepatide creates. People who combine physical activity with their GLP-1 weight loss protocol often find that bupropion energizing effect makes exercise more accessible than it was before treatment. Following a structured diet plan designed for GLP-1 therapy alongside the combination can maximize the weight loss benefits while ensuring adequate nutrition to support both medications.
It is also worth noting how bupropion interacts with other common medications that tirzepatide users take. Many people on tirzepatide also take metformin alongside tirzepatide for blood sugar management. Bupropion has minimal interaction with metformin, making a three-drug combination of bupropion, metformin, and tirzepatide generally manageable under medical supervision. Others take supplements alongside their tirzepatide, and knowing which supplements interact with bupropion versus which interact with tirzepatide helps you build a safe and effective medication stack.
How tirzepatide works differently
Tirzepatide operates in a completely different universe from bupropion. While bupropion works in the brain on dopamine and norepinephrine, tirzepatide works primarily in the gut, the pancreas, and appetite centers in the hypothalamus. It is a dual GIP and GLP-1 receptor agonist, meaning it activates two incretin hormone pathways simultaneously. This dual mechanism is what makes it the most effective weight loss medication ever studied in clinical trials.
Let me break down what that actually means.
GLP-1 stands for glucagon-like peptide-1. When you eat food, your gut releases natural GLP-1, which tells your pancreas to produce insulin, tells your liver to slow glucose production, and tells your brain that you are getting full. Natural GLP-1 lasts only a few minutes before enzymes break it down. Tirzepatide mimics this hormone but lasts an entire week, creating sustained appetite suppression and blood sugar control that natural GLP-1 could never achieve. This is why people experience such dramatic results on their tirzepatide weight loss first month.
GIP stands for glucose-dependent insulinotropic polypeptide. This is where tirzepatide separates itself from semaglutide and other GLP-1-only medications. GIP enhances fat metabolism, improves insulin sensitivity in adipose tissue, and may protect against some of the nausea that pure GLP-1 agonists cause. The combination of GIP and GLP-1 activation creates a synergistic effect that neither pathway achieves alone, which explains why tirzepatide outperforms semaglutide in head-to-head comparisons.
The SURMOUNT clinical trial program demonstrated average weight loss of 20.9% of body weight at the highest dose of tirzepatide over 72 weeks. That translates to roughly 50 pounds for someone who weighs 240 pounds. These numbers shattered every previous record for a pharmaceutical weight loss intervention, including semaglutide results from the STEP trials. The before and after results across GLP-1 medications tell a powerful visual story of what these drugs can accomplish.
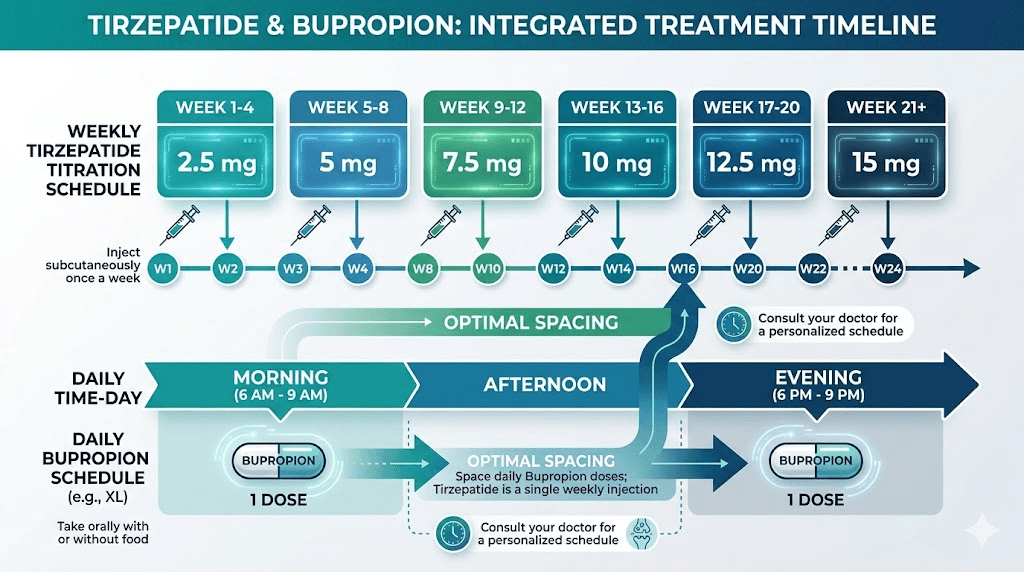
Tirzepatide is administered as a weekly subcutaneous injection. The dosing schedule follows a careful titration pattern: 2.5mg for the first four weeks, then 5mg, then increases of 2.5mg every four weeks as tolerated up to a maximum of 15mg weekly. This slow escalation exists specifically to manage the gastrointestinal side effects that hit hardest during the first weeks at each new dose level. Learning proper injection technique is essential for anyone starting this medication.
Here is where the connection to bupropion starts becoming clear. Tirzepatide significantly delays gastric emptying. Food sits in your stomach longer, which is one mechanism behind the appetite suppression. But delayed gastric emptying also affects how quickly oral medications are absorbed. If you swallow a bupropion pill and it sits in your stomach two to three times longer than usual, the absorption kinetics change. This does not necessarily create a dangerous interaction, but it is a variable that both you and your prescriber need to understand.
The side effect profile of tirzepatide is dominated by gastrointestinal complaints. Nausea affects approximately 39% of users. Diarrhea, constipation, vomiting, and bloating are all common. These side effects are usually worst during the first two to four weeks at each dose level and tend to improve with time. For people already managing side effects from bupropion, adding tirzepatide gastrointestinal effects on top requires careful planning and monitoring. Some users also experience sulfur burps, a particularly unpleasant but generally harmless effect of delayed gastric emptying.
Beyond the gastrointestinal effects, tirzepatide can cause body aches, joint pain, and muscle pain that may be confused with bupropion side effects if you are not aware of which medication is more likely responsible. Keeping track of when symptoms appear relative to your injection day and your oral medication timing helps you and your provider identify the source. People switching between different GLP-1 medications, such as those switching from semaglutide to tirzepatide, should know that side effect profiles differ between these drugs even though they target similar pathways.
Can you take wellbutrin and tirzepatide together
Yes. Based on currently available evidence, you can take wellbutrin and tirzepatide together. No direct pharmacological interaction has been identified between these two medications.
That single paragraph could be the entire section. But it should not be. Because "no direct interaction" does not mean "no concerns," and it definitely does not mean "take them however you want without thinking about it." The reality is more nuanced, more interesting, and more important than a simple compatibility check.
Drugs.com, which maintains one of the most comprehensive drug interaction databases available to the public, lists no interaction between tirzepatide and bupropion. The FDA prescribing information for tirzepatide does not list bupropion as a contraindicated medication. The FDA prescribing information for bupropion does not list GLP-1 receptor agonists as problematic co-administered drugs. From a pure pharmacological standpoint, these medications work on entirely different systems through entirely different mechanisms.
Bupropion is metabolized primarily by the CYP2B6 enzyme in the liver. Tirzepatide is a peptide that is broken down through general proteolysis, not through cytochrome P450 enzymes. This means they do not compete for the same metabolic pathways, which eliminates one of the most common sources of drug-drug interactions. They will not increase or decrease each other serum concentrations through enzymatic competition. This is fundamentally different from combining two oral medications that share hepatic enzymes, like the complex considerations involved when people ask about phentermine versus GLP-1 medications or whether phentermine qualifies as a GLP-1.
However, several indirect interactions deserve attention. These are not drug-drug interactions in the traditional pharmacological sense. They are clinical considerations that arise when two medications with overlapping effect profiles are used simultaneously. Professionals monitoring patients on both medications track these considerations carefully, and platforms like SeekPeptides provide resources to help people understand these nuances.
The first concern is overlapping nausea. Both medications cause nausea independently. Bupropion causes nausea in roughly 10-15% of users, primarily during initiation. Tirzepatide causes nausea in roughly 39% of users, predominantly during dose escalation. When you combine them, you may experience compounded nausea that is worse than either medication would cause alone. This is not a pharmacological interaction. It is an additive side effect profile. Knowing how to manage this, including understanding which foods to avoid, makes the combination far more tolerable.
The second concern involves the seizure threshold, and this one requires serious attention. Bupropion lowers the seizure threshold in a dose-dependent manner. Seizure risk increases with dehydration, electrolyte imbalances, rapid dose changes, and conditions that cause metabolic stress. Tirzepatide causes gastrointestinal side effects, including diarrhea and vomiting, that can lead to dehydration and electrolyte imbalances. The connection is indirect but clinically meaningful. If tirzepatide causes you to become dehydrated, and you are already on bupropion which has lowered your seizure threshold, the combined situation could increase seizure risk beyond what either medication would cause independently.
The third concern relates to gastric emptying and absorption timing, which we will explore in dedicated detail in a later section. The fourth concern involves blood pressure effects, as bupropion can elevate blood pressure while tirzepatide metabolic changes and weight loss generally lower it. Understanding these dynamics helps you work with your provider to find the right monitoring schedule.
Many physicians across the country are prescribing both medications concurrently with good results. The combination is not considered high-risk. It simply requires informed monitoring and attention to the indirect interactions described above. If your prescriber is comfortable managing both medications and you understand what to watch for, there is no pharmacological reason to avoid the combination.
For context, the drug interaction profile of wellbutrin and tirzepatide is considerably simpler than many other combinations people ask about. The question of whether you can take phentermine and tirzepatide together involves much more complicated stimulant overlap. Even phentermine and semaglutide combinations raise more flags. The question of combining semaglutide and tirzepatide together involves redundant receptor agonism, and even alternating between the two requires careful transition planning. Compared to those scenarios, the wellbutrin and tirzepatide combination is relatively clean. Different targets. Different mechanisms. Different metabolic pathways. The indirect concerns described above are real but manageable with the right approach and the right provider.
How the combination affects weight loss
This is where the conversation gets genuinely exciting. Because when you combine the weight loss mechanisms of bupropion with the weight loss mechanisms of tirzepatide, you are attacking excess weight from two completely different angles simultaneously.
Bupropion promotes weight loss through central nervous system mechanisms. It increases dopamine and norepinephrine activity, which reduces food cravings, particularly cravings for high-calorie comfort foods driven by emotional eating patterns. It also provides a mild thermogenic effect, slightly increasing metabolic rate. The weight loss from bupropion alone is modest, typically 2-5% of body weight over several months, and it is often categorized as "weight-neutral" compared to other antidepressants rather than as a weight loss medication per se. This stands in stark contrast to the dramatic before and after results seen with tirzepatide.
Tirzepatide promotes weight loss through peripheral and central mechanisms that are entirely distinct from bupropion. It suppresses appetite through GLP-1 receptor activation in the hypothalamus. It delays gastric emptying so you feel full longer after meals. It improves insulin sensitivity, which shifts your body metabolic machinery toward fat utilization rather than fat storage. The GIP component enhances lipid metabolism directly in adipose tissue. Together, these mechanisms produce the 15-20% average body weight loss seen in the clinical trials, results that changed what the medical community considered possible with pharmacological intervention.
When these two mechanism profiles combine, the theoretical framework is compelling. Bupropion handles the dopaminergic, reward-driven eating patterns that tirzepatide may not fully address. Tirzepatide handles the hormonal appetite signaling and metabolic dysfunction that bupropion barely touches. One works from the top down through the brain. The other works from the bottom up through the gut. There is minimal overlap in their weight loss mechanisms, which suggests potential synergy rather than redundancy.
Some retrospective data supports this theory. Studies examining patients on antidepressants who started GLP-1 receptor agonists found that those on bupropion specifically tended to fare better in terms of weight loss compared to those on SSRIs like sertraline or fluoxetine. The SSRIs actively work against weight loss through serotonergic mechanisms that increase appetite and promote fat storage. Bupropion, being dopaminergic rather than serotonergic, does not create this antagonistic effect. If you are wondering about your own response, tracking your weight loss timeline carefully can reveal how both medications are contributing.
There is, however, an important caveat buried in the research data. A study examining weight outcomes in patients using GLP-1 agonists found that those concurrently taking any antidepressant, including bupropion, lost slightly less weight on average compared to those not taking antidepressants. Specifically, the antidepressant group lost an average of 0.73 kg over the study period compared to 1.74 kg in the non-antidepressant group. Before you interpret this as evidence that bupropion hinders tirzepatide effectiveness, consider the confounders. People taking antidepressants have depression. Depression itself affects metabolism, motivation for lifestyle changes, adherence to dietary modifications, and cortisol levels, all of which influence weight loss. The reduced weight loss may reflect the underlying condition rather than a pharmacological interference.
Real-world clinical experience shows many patients achieving excellent weight loss results on the combination. Some physicians actually prefer that their patients remain on bupropion during tirzepatide treatment because the dopaminergic support helps maintain motivation and prevents the emotional eating rebound that can sabotage weight loss efforts. The dietary planning component of weight loss becomes easier when dopamine-driven cravings are managed by bupropion while hormonal hunger is managed by tirzepatide.
For anyone tracking their progress, remember that weight loss is not linear on either medication. Plateaus happen. Stalls happen. The combination does not guarantee faster results. But it does address a wider range of the physiological and psychological mechanisms that drive overeating and weight retention, which means more of the problem is being treated at any given time.
One practical consideration for maximizing weight loss on the combination involves diet optimization. Because tirzepatide dramatically reduces appetite, the food you do eat matters enormously. Every calorie needs to count nutritionally. Following a structured tirzepatide meal plan that prioritizes protein, fiber, and micronutrient density ensures you lose fat rather than muscle. Starting your day with a protein-rich breakfast is especially important when taking morning bupropion, as it helps buffer the medication on the stomach while providing essential nutrition. For dinner, focusing on GLP-1 friendly dinner recipes that are easy to digest can reduce overnight GI discomfort.
Some patients also wonder whether the effectiveness of tirzepatide might fade over time when combined with bupropion. This is a common concern regardless of what other medications are in the picture. Tirzepatide effectiveness can plateau as the body adapts, which is why the titration schedule exists, to increase the dose as tolerance develops. Bupropion does not accelerate or contribute to tirzepatide tolerance. If your weight loss stalls, the issue is far more likely to be tirzepatide dose-related, dietary, or metabolic than anything caused by bupropion.
Side effects to watch when combining these medications
Combining wellbutrin and tirzepatide means managing two side effect profiles simultaneously. Neither medication has a clean safety record in isolation. Together, the list of potential effects grows longer, and some effects amplify each other in ways that require deliberate monitoring.
Nausea sits at the top of the list. It deserves that position.
Tirzepatide causes nausea in approximately 39% of users across clinical trials. The nausea is typically worst during the first two to four weeks at each dose level, then gradually fades as the body adapts. Bupropion causes nausea in roughly 10-15% of users, also most prominently during initiation. If you start both medications at the same time, which you should never do, the nausea could be debilitating. Even if you are already stabilized on bupropion and then begin tirzepatide at the starting dose of 2.5mg, the added tirzepatide nausea may feel more intense than it would for someone not on bupropion. Managing nausea through careful food choices and meal timing becomes essential.
Gastrointestinal distress beyond nausea is the second major concern. Tirzepatide commonly causes constipation, diarrhea, bloating, and sometimes vomiting. Bupropion can cause constipation and abdominal pain. The overlapping constipation risk deserves particular attention because severe constipation is one of the most common reasons people discontinue GLP-1 receptor agonists. Adding bupropion constipation on top of tirzepatide constipation creates a compounded problem that may require proactive management with fiber supplements and hydration. SeekPeptides members frequently discuss strategies for managing these overlapping gastrointestinal effects.
Seizure risk elevation is the most serious safety consideration. Bupropion carries an FDA black box warning regarding seizure risk. The incidence is approximately 0.4% at doses up to 450mg daily, which sounds small until you realize that certain conditions dramatically increase this baseline risk. Those conditions include rapid dose escalation of bupropion, concurrent use of medications that lower the seizure threshold, eating disorders with purging behavior, alcohol withdrawal, and critically for our discussion, dehydration and electrolyte imbalances. Tirzepatide side effects can cause exactly these electrolyte disruptions. Vomiting depletes potassium and chloride. Diarrhea depletes sodium and potassium. Reduced food intake can cause hyponatremia. If you are on bupropion 300mg daily and develop significant GI side effects from tirzepatide that lead to dehydration, your seizure risk climbs. This is manageable with proper hydration and monitoring, but it must be on your radar.
Blood pressure changes create another layer of complexity. Bupropion can raise blood pressure, an effect seen in roughly 6% of users. Tirzepatide and weight loss in general tend to lower blood pressure. These opposing effects might seem like they would cancel each other out. Sometimes they do. But the trajectory matters. Early in tirzepatide treatment, before significant weight loss has occurred but while GI side effects are causing fluid shifts, blood pressure can fluctuate unpredictably. Monitoring is essential, especially in the first three months of combination therapy. Checking your blood pressure is one of the monitoring tools for home use that anyone on this combination should employ.
Insomnia and sleep disruption deserve mention. Bupropion has stimulant-like properties that commonly cause insomnia, particularly when taken too late in the day. Tirzepatide can also disrupt sleep through GI discomfort, nausea, and the general metabolic shifts that accompany rapid weight loss. Poor sleep increases cortisol, which impedes weight loss and worsens mood, potentially undermining both medications intended effects.
Headaches occur with both medications. Bupropion causes headaches in roughly 26% of users. Tirzepatide causes headaches in approximately 12-16% of users, particularly during dose transitions. The headache management strategies that work for GLP-1 agonists alone may need modification when bupropion is part of the picture.
Dry mouth is common with bupropion and can be exacerbated by the dehydration risks from tirzepatide GI effects. This seems minor until you consider that chronic dry mouth increases dental decay risk, reduces quality of life, and signals inadequate hydration that has implications for seizure threshold. Staying well-hydrated is not optional on this combination. It is medically necessary.
Fatigue rounds out the major shared side effects. Both medications can cause tiredness, though through different mechanisms. Bupropion fatigue tends to be paradoxical, occurring despite the stimulant-like mechanism, often as a sign that the dose needs adjustment. Tirzepatide fatigue tends to stem from reduced caloric intake, the metabolic demands of rapid weight loss, and the general adaptation process the body undergoes during GLP-1 agonist therapy.
Temperature regulation changes are another side effect that surprises people. Many tirzepatide users report feeling cold as they lose weight, which makes physiological sense since fat tissue provides insulation and generates metabolic heat. Bupropion does not typically cause temperature sensitivity, but the stimulant-like properties can cause sweating in some users, creating a confusing situation where someone feels cold from tirzepatide weight loss but sweats from bupropion norepinephrine activity.
For women, menstrual changes deserve attention. Tirzepatide can affect menstrual cycles through weight loss related hormonal shifts, changes in estrogen levels from reduced fat tissue, and the general metabolic disruption of rapid weight change. Bupropion typically does not affect menstrual cycles directly, but the stress of managing overlapping side effects and the physiological demands of concurrent weight loss and psychiatric medication can contribute to cycle irregularity. Similarly, some users taking other GLP-1 agonists report period changes, suggesting this is a class-wide effect rather than specific to tirzepatide.
Injection site reactions are purely a tirzepatide concern and have nothing to do with bupropion, but they are worth mentioning because injection site reaction treatment sometimes involves anti-inflammatory medications that could interact with other drugs in your regimen. Knowing where to inject tirzepatide and rotating sites properly minimizes this concern and keeps the focus on managing the more significant overlapping effects.
Hair loss is one side effect that causes significant distress, and the complete guide to GLP-1 related hair loss explains why rapid weight loss can trigger telogen effluvium. This is not a bupropion effect. It is a weight loss effect. But for someone already managing depression, hair loss on top of everything else can feel devastating. Being prepared for this possibility and understanding that it is temporary and treatable helps maintain the psychological resilience needed to continue both medications.
Gastric emptying and medication absorption
This section matters more than most people realize. Tirzepatide fundamentally changes how your stomach processes everything that enters it, and that includes oral medications like bupropion.
Under normal conditions, the stomach empties a standard meal in approximately four to five hours. Gastric emptying of liquids is faster, typically 20 to 30 minutes. Oral medications dissolve in the stomach, pass into the small intestine, and get absorbed into the bloodstream through the intestinal wall. The entire process follows a predictable timeline that pharmaceutical companies use to design dosing schedules. Every controlled-release formulation of bupropion was engineered based on normal gastric emptying rates.
Tirzepatide slows this process significantly. Studies show that GLP-1 receptor agonists can delay gastric emptying by 30 to 50 percent, meaning food and medications sit in the acidic stomach environment substantially longer than designed. For tirzepatide specifically, the delay is most pronounced at higher doses and during the first few weeks at each new dose level. This is the same mechanism that makes people feel full after small meals, and it is partly why some people report still feeling hungry on tirzepatide at lower doses where gastric emptying is less affected.
What does this mean for bupropion absorption? The answer depends on which formulation you take.
For comparison, oral semaglutide timing faces even stricter requirements regarding food and water intake windows. Bupropion immediate-release tablets are designed to release their entire dose quickly in the stomach. Delayed gastric emptying means the drug sits in stomach acid longer before reaching the intestines where it gets absorbed. This could theoretically lead to more degradation of the drug in the stomach and slightly reduced bioavailability. However, bupropion is reasonably stable in acidic environments, so the clinical significance may be minimal.
Bupropion sustained-release and extended-release formulations present a different consideration. These tablets use specially designed coatings and matrices to control the rate of drug release over 12 to 24 hours. When gastric emptying is delayed, these formulations spend more time in conditions they were not designed for. The release kinetics could change, potentially leading to more drug being released in the stomach and less in the intestines, or to a more compressed absorption window that alters peak blood levels. These are theoretical concerns, and real-world clinical experience has not shown clinically dangerous absorption changes in most patients. But they are worth understanding and discussing with your prescriber.
The practical implication is straightforward. Take bupropion at a consistent time relative to your tirzepatide injection. Most clinicians suggest taking oral medications at least one hour before eating when on GLP-1 agonists, and separating important oral medications from the tirzepatide injection day is not necessary since tirzepatide effects on gastric emptying are continuous throughout the week rather than acute on injection day.
The FDA addressed delayed gastric emptying in the tirzepatide prescribing information. Their guidance states that patients taking oral medications should be aware that absorption rates may change and that monitoring for medication effectiveness and side effects should be increased during dose transitions. They specifically mention oral contraceptives, where delayed absorption could reduce efficacy, but the principle applies to any oral medication with a narrow therapeutic window. Bupropion does not have an extremely narrow therapeutic window, but consistent absorption is still important for maintaining stable antidepressant effects and avoiding seizure threshold fluctuations.
One practical strategy many prescribers recommend is taking bupropion first thing in the morning on an empty stomach, 30 to 60 minutes before eating. This allows the medication to begin dissolving and moving through the stomach before food intake triggers the maximal gastric emptying delay. This timing also aligns with best practices for tirzepatide timing and helps establish a consistent routine.
Other medications besides bupropion are also affected by this gastric emptying delay. If you take supplements with your GLP-1 therapy, the absorption of those supplements may also change. This is particularly relevant for time-sensitive supplements like iron, thyroid medications, and certain vitamins that have specific absorption requirements. For patients also taking metformin or other oral diabetes medications, the same delayed absorption principles apply. Discuss your complete medication and supplement list with your pharmacist, not just your doctor, because pharmacists are specifically trained in drug absorption interactions and timing optimization.
Travel adds another layer of complexity to this timing equation. Traveling with tirzepatide requires planning for proper refrigeration and storage, and time zone changes can disrupt your carefully timed bupropion schedule. If you are crossing multiple time zones, the general recommendation is to gradually shift your bupropion timing by one to two hours per day rather than abruptly changing. Your tirzepatide injection day can simply shift to the local equivalent of your usual day, since a day or two variation in the weekly injection schedule does not significantly affect outcomes, as discussed in the guide on taking tirzepatide early. Making sure your tirzepatide stays properly stored during travel, including understanding how long tirzepatide lasts in the fridge, prevents potency loss that could affect your side effect and weight loss experience.
Mental health on tirzepatide while taking wellbutrin
This is the section nobody writes about. And it might be the most important one in this entire guide.
People take wellbutrin because they have depression, anxiety, seasonal affective disorder, or some combination of mental health conditions that require pharmacological support. These conditions do not disappear when you start tirzepatide. In fact, the rapid physiological changes that come with significant weight loss can challenge mental health in ways that even seasoned psychiatrists sometimes underestimate.
Let us start with the good news. Weight loss itself has well-documented antidepressant effects. Reduced inflammation, improved sleep quality, better physical mobility, enhanced self-image, and the social reinforcement that comes with visible physical changes all contribute to improved mood. Many patients on the combination of bupropion and tirzepatide report feeling better than they have in years. The bupropion handles the neurochemical component of depression while tirzepatide addresses the physical health component, and together they create a positive feedback loop where improving physical health improves mental health, which in turn improves adherence to healthy behaviors. Some people who were previously struggling to lose weight on GLP-1 therapy alone find that addressing their depression with bupropion unlocks the lifestyle changes needed for the medication to work as intended.
Now for the complicated part.
Rapid weight loss changes your relationship with food in ways that can be psychologically destabilizing. If food has been a coping mechanism for emotional distress, and it is for many people with depression, tirzepatide appetite suppression can remove that coping tool overnight. The result is often a period of increased anxiety or emotional volatility as the brain scrambles to find alternative ways to manage stress. Being on bupropion provides some neurochemical buffer against this destabilization, but it does not eliminate it entirely. People experiencing anxiety on tirzepatide should take this psychological mechanism seriously.
Body image changes during rapid weight loss are another psychological challenge that catches people off guard. Losing 40 to 60 pounds over several months changes how you look in ways that your brain may struggle to process. Some people develop a disconnect between how they look and how they perceive themselves, a phenomenon sometimes called "phantom fat" that resembles mild body dysmorphia. Others experience anxiety about loose skin, about how others perceive their changing body, or about whether they deserve to look different. These are real psychological challenges that bupropion does not directly address.
There is also the question of identity. For people who have been overweight for years or decades, weight is woven into their sense of self. Losing a significant portion of body weight can trigger an identity crisis that manifests as depression, anxiety, or emotional confusion. Again, bupropion provides baseline neurochemical support, but the psychological work of adjusting to a new body and a new identity requires more than medication. It often requires therapy, support groups, or at minimum, honest conversations with people who understand the process. SeekPeptides members share these experiences within a community that understands the intersection of peptide therapy and mental health.
The neurochemical changes of weight loss add another layer. Fat tissue is metabolically active. It produces hormones, cytokines, and other signaling molecules that affect brain function. Rapid fat loss changes the neurochemical environment in ways that can temporarily worsen or alter mood. Leptin levels drop as fat stores decrease. Ghrelin patterns shift. Inflammatory markers change. All of these affect neurotransmitter function, potentially requiring adjustments to bupropion dosing that would not have been anticipated before starting tirzepatide.
Some patients report that their bupropion seems less effective after losing significant weight on tirzepatide. This could be due to pharmacokinetic changes, since drug distribution changes when body composition changes significantly. Or it could reflect the psychological challenges described above manifesting as apparent medication failure. Either way, if you notice a return of depressive symptoms while losing weight on tirzepatide, do not assume it means the medications are interacting poorly. It may mean your mental health treatment plan needs updating to account for your changing body and circumstances.
Monitor your mood carefully. Keep a simple daily log. Note energy levels, anxiety levels, sleep quality, and overall emotional state. This data becomes invaluable for your prescriber in making dosage adjustments and determining whether the combination is working as intended. Understanding how these medications make you feel is a critical part of managing the combination safely.
The timeline for psychological adjustment varies enormously between individuals. Some people adapt to the mental health changes within the first month. Others find that the psychological impact deepens as weight loss accumulates over months. There is no standard timeline, and anyone who tells you otherwise is oversimplifying. What matters is having a support system, having a prescriber who understands the intersection of psychiatric medication and weight loss therapy, and being honest with yourself about how you are really feeling versus how you think you should be feeling. The timeline for side effects varies on GLP-1 agonists generally, and emotional side effects are no exception. If you are concerned about discontinuation effects, understanding withdrawal symptoms from GLP-1 agonists helps you plan for the possibility that you might need to stop tirzepatide at some point while continuing bupropion.
Dosage adjustments and timing protocols
Getting the timing right when taking wellbutrin and tirzepatide together is not just about convenience. It is about optimizing effectiveness while minimizing overlapping side effects. Here is a detailed breakdown of what evidence-based protocols look like.
First, the foundational rule. Never start both medications simultaneously. If you are not yet on either medication, start bupropion first. Allow four to six weeks for stabilization before introducing tirzepatide. This approach lets you establish a baseline for bupropion side effects, confirm the antidepressant dose is correct, and ensure you tolerate the medication before adding the complexity of tirzepatide. If you are already stable on bupropion, as most people asking about this combination are, you can proceed directly to tirzepatide initiation at the standard starting dose.
Tirzepatide titration follows a specific protocol. Start at 2.5mg weekly for at least four weeks. This initial dose is not expected to produce significant weight loss. It exists solely to let your body adapt to the GLP-1 and GIP receptor activation and the associated gastrointestinal effects. After four weeks, increase to 5mg weekly. Continue increasing by 2.5mg every four weeks as tolerated, up to a maximum of 15mg weekly. Understanding the unit conversion for starting doses helps ensure accuracy. Some people find their optimal dose well below the maximum, and the dosage calculator can help estimate appropriate levels based on body weight. For those considering a more conservative introduction, the microdose tirzepatide schedule offers an even gentler ramp-up that minimizes the GI effects most likely to interact with bupropion side effects. Some clinicians also explore microdosing tirzepatide for inflammation benefits rather than purely for weight loss, which involves even lower doses with less GI impact.
When in the day should you take each medication?
Bupropion XL should be taken once daily in the morning. Take it on an empty stomach if possible, 30 to 60 minutes before breakfast, with a full glass of water. This timing accomplishes several things. It separates the medication from food, which means gastric emptying delays from tirzepatide have less impact on absorption. It positions the stimulant-like effects of bupropion during waking hours, reducing insomnia risk. And it creates a consistent routine that supports medication adherence.
Bupropion SR should be taken twice daily, with the first dose in the morning and the second dose in the early afternoon, at least six to eight hours before bedtime. The same principles apply regarding taking it before meals when possible. The early afternoon timing of the second dose is critical for avoiding the sleep disruption that can plague people on this medication.
Tirzepatide should be injected once weekly on the same day each week. The best day to take tirzepatide depends on your schedule and when you can best manage potential side effects. Many people inject on Thursday or Friday evening so that the peak side effect period, typically 24 to 48 hours post-injection, falls on the weekend when they can rest if needed. Others prefer Monday morning to get the injection done at the start of the week. What matters most is consistency. Choose a day and a time and stick with it.
Should you take bupropion and tirzepatide on the same day? Yes, this is perfectly fine. The tirzepatide injection is subcutaneous, not oral, so gastric emptying has no effect on tirzepatide absorption. And the effects of tirzepatide on gastric emptying are continuous throughout the week, not spiked on injection day. There is no pharmacological reason to separate the two medications by day.
Some clinicians recommend a microdosing approach to tirzepatide for patients who are particularly sensitive to side effects. This involves using doses lower than the standard starting dose for an extended introductory period. For patients on bupropion, this conservative approach has merit because it reduces the likelihood of severe GI side effects that could lead to the dehydration and electrolyte imbalances that increase seizure risk. A microdosing tirzepatide chart can guide this more gradual introduction.
What about dose adjustments to bupropion while on tirzepatide? Generally, no changes to bupropion dosing are required when starting tirzepatide. However, as you lose weight, your body composition and metabolic rate change, which can alter drug pharmacokinetics. Some prescribers reassess bupropion dosing after every 20 to 30 pounds of weight loss. Others wait until the patient reports either reduced efficacy or increased side effects. The key is staying in communication with your prescriber rather than trying to self-adjust either medication.
If you are considering splitting your tirzepatide dose into twice-weekly injections to reduce side effects, know that this is a strategy some physicians employ specifically for patients who are managing overlapping side effects from other medications. Splitting the dose can reduce peak-level side effects while maintaining overall weekly exposure.
Proper injection technique matters as well. Whether you inject in the abdomen, thigh, or upper arm, following the correct stomach injection technique or using the optimal injection site for weight loss ensures consistent medication absorption. Poor injection technique can lead to variable absorption rates that create inconsistent side effect profiles, making it harder to distinguish tirzepatide effects from bupropion effects during the combination period.
If at any point you and your provider decide to discontinue either medication, the tapering protocol matters. Weaning off tirzepatide should be done gradually to avoid rebound hunger and rapid weight regain. Stopping tirzepatide cold turkey is possible but can cause uncomfortable appetite surges and GI adjustment symptoms. Bupropion also should not be stopped abruptly, as discontinuation can cause irritability, insomnia, and mood destabilization. If you are stopping one medication while continuing the other, manage the transition in coordination with both prescribers to ensure continuity of care.
Understanding how to reconstitute tirzepatide properly is essential for anyone using compounded formulations, as improper reconstitution can lead to inaccurate dosing that makes side effect management unpredictable. This is especially important for patients on bupropion, where consistency in tirzepatide dosing translates directly to consistency in the side effect profile and predictability in the seizure risk calculation. The peptide calculator on SeekPeptides can help ensure accurate dosing calculations.
Who should not combine wellbutrin and tirzepatide
While most people can safely take these medications together, several specific populations face elevated risks that may make the combination inadvisable. These contraindications are not suggestions. They are clinical red lines that require serious discussion with your healthcare provider before proceeding.
People with a history of seizures or epilepsy face the highest risk. Bupropion is already contraindicated in patients with seizure disorders in most clinical guidelines. Even the cardiovascular concerns with GLP-1 agonists are simpler to manage than seizure risk in this population. Adding tirzepatide, with its potential to cause dehydration and electrolyte disturbances that further lower seizure threshold, compounds an already unacceptable risk. If you have any history of seizures, this combination requires extreme caution and possibly avoidance entirely.
People with current or recent eating disorders, particularly bulimia nervosa and anorexia nervosa, represent another high-risk group. Bupropion is specifically contraindicated in patients with bulimia due to the dramatically increased seizure risk associated with the electrolyte imbalances that come with purging behavior. Tirzepatide extreme appetite suppression can exacerbate disordered eating patterns and may be psychologically harmful for individuals with active eating disorders. The combination in this population is potentially dangerous on multiple levels and should be approached only under close psychiatric and medical supervision, if at all.
People with uncontrolled hypertension need careful evaluation. Bupropion can raise blood pressure. While tirzepatide and weight loss generally improve blood pressure over time, the early weeks of combination therapy can involve unpredictable blood pressure fluctuations. If your blood pressure is not well-controlled before starting the combination, the added variables make management significantly more difficult.
People taking MAO inhibitors cannot take bupropion at all, which means the combination with tirzepatide is irrelevant for this group. But it bears mentioning because patients switching from an MAO inhibitor need a minimum 14-day washout period before starting bupropion, and tirzepatide should not be initiated during this transition period when neurochemistry is already in flux.
People with severe kidney disease face increased risks because both dehydration-related complications from tirzepatide and bupropion metabolite accumulation from impaired renal clearance create a compounded problem. Kidney function monitoring becomes essential, and some prescribers choose lower doses of both medications in this population. Understanding kidney-related concerns with GLP-1 agonists provides additional context for this consideration.
People with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should not take tirzepatide. This is a tirzepatide-specific contraindication based on findings in rodent studies and is unrelated to bupropion. But it eliminates the combination for these individuals. Those with concerns about thyroid nodules and tirzepatide should discuss screening with their endocrinologist before starting treatment.
People with significant hepatic impairment require dose adjustments for bupropion, as it is metabolized through the liver. Combining a hepatically-challenged metabolism of bupropion with the general metabolic demands of tirzepatide therapy requires careful monitoring of liver enzymes and possibly reduced dosing of bupropion.
Pregnant or breastfeeding individuals should not take tirzepatide. The medication is category X in pregnancy, meaning known fetal harm outweighs any potential benefit. Anyone who becomes pregnant while on tirzepatide should discontinue it immediately and consult their OB-GYN. The stories shared by women who got pregnant on tirzepatide underscore how quickly this situation can arise and how important immediate medical guidance is. The question of tirzepatide while breastfeeding is equally clear: do not do it. If pregnancy is a possibility, contraception must be reliable, and note that tirzepatide may reduce the effectiveness of oral contraceptives through delayed gastric emptying.
Finally, people with a history of alcohol use disorder deserve special mention. Bupropion seizure risk increases with alcohol withdrawal. Tirzepatide has anecdotally been associated with reduced alcohol cravings in some users, but if a person with alcohol use disorder stops drinking suddenly while on bupropion, the withdrawal period combined with the lowered seizure threshold creates a genuinely dangerous situation. The interaction between alcohol and tirzepatide is an important topic for anyone on this combination. Similarly, understanding alcohol interactions with other GLP-1 agonists provides broader context for this concern.
People with autoimmune conditions like Hashimoto thyroiditis or endometriosis should discuss the combination with their specialist. GLP-1 agonists have complex interactions with the immune system and inflammatory pathways. While these are not contraindications to the wellbutrin and tirzepatide combination specifically, autoimmune conditions add variables that require individualized risk assessment and more frequent monitoring. Those dealing with conditions like lipedema may find that the combination offers unique benefits, as bupropion addresses the depression that frequently accompanies chronic pain conditions while tirzepatide addresses the weight management component.
Men considering this combination should be aware that both medications can affect hormonal balance. Bupropion may increase dopamine-mediated testosterone activity, while rapid weight loss from tirzepatide affects testosterone levels through changes in fat tissue aromatase activity and sex hormone binding globulin levels. Some men also ask about erectile dysfunction and tirzepatide, a concern that bupropion may actually help mitigate since it is one of the few antidepressants associated with improved rather than impaired sexual function.
Blood work and monitoring when using both medications
If you are going to take wellbutrin and tirzepatide together, commit to monitoring. This is not one of those situations where you can take both medications and check in with your doctor once a year. Active monitoring is what turns a manageable combination into a safe one.
Here is what to track and when.
Baseline blood work before starting the combination should include a comprehensive metabolic panel covering sodium, potassium, chloride, bicarbonate, BUN, creatinine, and glucose. It should also include a complete blood count, thyroid function tests including TSH and free T4, liver function tests including ALT, AST, and bilirubin, lipid panel, hemoglobin A1c if you have any degree of insulin resistance, and blood pressure measured at rest. This baseline establishes your pre-combination values against which all future labs will be compared. Understanding what shows up in blood work on tirzepatide helps you interpret your results accurately.
During the first three months of combination therapy, blood work should be repeated every four to six weeks. This frequency may seem excessive, but the first three months represent the highest-risk period. You are titrating tirzepatide doses while your body adapts to the medication. GI side effects are most intense. Dehydration risk is highest. And the metabolic shifts of early weight loss are most dramatic. Key values to watch during this period include electrolytes, especially sodium and potassium, kidney function markers, and fasting glucose if applicable.
Blood pressure monitoring should be more frequent than blood work. Ideally, check blood pressure at home two to three times per week during the first three months, then weekly once the combination is stabilized. Record the readings and share them with your prescriber at every visit. A consistent upward trend, even within the "normal" range, warrants attention because bupropion can cause gradual blood pressure elevation that does not trigger alarm on any single reading but becomes concerning over weeks.
After the first three months, assuming you are tolerating the combination well and have reached a stable tirzepatide dose, monitoring can transition to every three months. The quarterly labs should continue to include a comprehensive metabolic panel, thyroid function, and liver function. Lipid panels can shift to every six months once stable. HbA1c every three to six months is appropriate if you have metabolic concerns.
Weight tracking is obvious but worth discussing because the method matters. Weigh yourself at the same time each day, preferably in the morning after using the bathroom but before eating or drinking. Use the same scale. Record every measurement. Do not obsess over daily fluctuations, which can range by 2 to 4 pounds due to water retention, bowel contents, and hormonal cycles. Instead, look at the weekly trend line. If you notice an unexpected weight gain trend or a complete stop in weight loss, discuss it with your provider rather than self-adjusting medications.
Hydration monitoring is critical and often overlooked. You should be consuming at least 64 ounces of water daily, and more if you are experiencing GI side effects like diarrhea or vomiting. Signs of dehydration include dark urine, reduced urine output, dizziness upon standing, headache, and dry mouth. On bupropion, dehydration is not just uncomfortable, it is a seizure risk factor. Treat hydration as a medical requirement, not a lifestyle suggestion.
Mood monitoring, as discussed in the mental health section, should be ongoing. A simple daily rating of mood on a 1-10 scale, noting energy level and any anxiety or unusual emotional states, provides data that your prescriber can use to adjust bupropion dosing if needed. This is especially important during periods of rapid weight loss when neurochemical changes are most significant.
SeekPeptides provides members with access to monitoring protocols and community support from others managing similar medication combinations. Tracking your blood work trends over time helps you and your provider make data-driven decisions about continuing, adjusting, or stopping either medication.
Heart rate monitoring is another metric worth tracking. Both medications can affect heart rate, bupropion through norepinephrine stimulation and tirzepatide through the cardiovascular effects of GLP-1 agonism. A resting heart rate consistently above 100 beats per minute warrants medical evaluation. Most fitness trackers and smartwatches can provide continuous heart rate data that supplements your clinical monitoring.
Gallbladder health is a monitoring area that often gets overlooked but deserves attention. Rapid weight loss is a known risk factor for gallstone formation, and tirzepatide gallbladder concerns are well documented in the clinical literature. Bupropion does not independently affect gallbladder function, but the combination creates rapid weight loss conditions that could precipitate gallstone formation. If you experience right upper quadrant abdominal pain, particularly after eating fatty foods, report it to your provider promptly.
For patients who want to understand the fuller picture of how their blood work might change, it is helpful to know what tirzepatide itself does to lab values. Hemoglobin A1c typically drops, even in non-diabetic patients. Triglycerides often improve dramatically. LDL cholesterol may decrease. These are positive changes, but they need to be tracked systematically so that your providers can see the trend and adjust other medications accordingly. The semaglutide dosage calculator and other tools on the platform help patients understand their medication levels alongside their lab values, creating a more complete picture of treatment progress.
Finally, if your provider suggests trying berberine alongside tirzepatide or adding NAD+ supplementation, make sure they know about your bupropion. While neither berberine nor NAD+ has significant interactions with bupropion, the cumulative effect of multiple metabolically active compounds requires holistic monitoring. Each addition to your protocol introduces new variables that can affect everything from GI comfort to energy levels to sleep quality.
Frequently asked questions
Does wellbutrin cancel out tirzepatide weight loss?
No. Bupropion does not cancel out tirzepatide weight loss. Unlike serotonergic antidepressants such as sertraline and paroxetine, which can promote weight gain and potentially counteract GLP-1 agonist effects, bupropion is weight-neutral to slightly weight-loss promoting. The dopaminergic mechanism of bupropion may actually complement tirzepatide by reducing reward-driven eating behaviors that tirzepatide hormonal appetite suppression does not fully address. Some retrospective data shows patients on antidepressants lose slightly less weight overall on GLP-1 agonists, but this likely reflects the underlying depression rather than a pharmacological conflict. Most clinical experience supports good weight loss outcomes when both are used together.
How far apart should I take wellbutrin and tirzepatide?
There is no required separation between the two medications. Tirzepatide is injected subcutaneously, so gastric emptying has no effect on its absorption. Bupropion is taken orally, and while tirzepatide does delay gastric emptying, this effect is continuous throughout the week rather than spiked on injection day. Take bupropion at your normal scheduled time regardless of when you inject tirzepatide. For optimal bupropion absorption, take it in the morning on an empty stomach, 30 to 60 minutes before your first meal. Your tirzepatide injection timing can remain independent of your bupropion schedule.
Will tirzepatide affect my wellbutrin blood levels?
Tirzepatide is unlikely to significantly affect wellbutrin blood levels. The two medications use completely different metabolic pathways. Bupropion is metabolized by CYP2B6 in the liver while tirzepatide is broken down through proteolysis. They do not compete for enzymes. However, tirzepatide delayed gastric emptying could theoretically alter the absorption kinetics of oral bupropion, potentially shifting when peak blood levels occur without necessarily changing the total amount absorbed. If you notice changes in how your wellbutrin feels, specifically its effectiveness or side effects, after starting or increasing your tirzepatide dose, discuss this with your prescriber. Blood level testing for bupropion is available but rarely needed.
Can I start both medications at the same time?
This is strongly discouraged. Starting both medications simultaneously makes it impossible to identify which medication is causing which side effects, makes dose titration dangerous because you cannot isolate responses, and maximizes the risk of overlapping side effects like nausea. If you are not on either medication, start bupropion first and allow four to six weeks for stabilization before beginning tirzepatide at 2.5mg weekly. If you are already stable on bupropion, you can proceed to start tirzepatide while continuing bupropion at your current dose. Understanding what to expect after the first dose helps you differentiate tirzepatide effects from bupropion effects.
Should I tell my psychiatrist about starting tirzepatide?
Absolutely yes. Every prescriber managing your medications needs to know your complete medication list. Your psychiatrist needs to know about tirzepatide for several reasons. They need to monitor for mood changes during rapid weight loss. They need to assess whether bupropion dose adjustments are needed as your body composition changes. They need to be aware of the increased dehydration risk and its implications for seizure threshold. And they need to understand the psychological impact that significant body changes can have on patients with depression or anxiety. Do not assume your weight loss provider will communicate with your psychiatrist. Take responsibility for ensuring both providers have complete information.
What if I experience severe nausea on both medications?
Severe nausea when combining wellbutrin and tirzepatide should be addressed promptly. First, ensure you are staying hydrated, as vomiting from nausea can cause dehydration that increases seizure risk on bupropion. Second, consider whether the nausea timing suggests one medication is primarily responsible, such as nausea that worsens after taking your morning bupropion versus nausea that peaks 24 to 48 hours after your tirzepatide injection. Third, discuss anti-nausea strategies with your provider, including dietary modifications outlined in tirzepatide food guides. If nausea is severe enough to prevent adequate fluid intake, contact your prescriber immediately rather than waiting for your next appointment.
Is contrave (bupropion/naltrexone) safe to take with tirzepatide?
Contrave combines bupropion with naltrexone and is an FDA-approved weight loss medication in its own right. Combining Contrave with tirzepatide means you are taking three pharmacologically active compounds, bupropion, naltrexone, and tirzepatide, which creates additional complexity. While no direct pharmacological interaction exists between naltrexone and tirzepatide, the combination has not been studied in clinical trials. Some prescribers do use all three together, but this requires particularly careful monitoring. Many prefer to discontinue Contrave when starting tirzepatide rather than layering a second weight loss medication on top of a more effective one. This decision should be made by your prescriber based on your individual clinical picture. Comparing different weight loss medication approaches can help you understand why tirzepatide often makes older weight loss drugs redundant.
How long does it take to see weight loss results on the combination?
Weight loss timelines on the combination are primarily driven by tirzepatide rather than bupropion. Most people begin noticing reduced appetite within the first one to two weeks of starting tirzepatide. Measurable weight loss typically begins within two to four weeks. However, the rate of weight loss on tirzepatide increases as the dose is titrated upward over months. The most significant weight loss usually occurs between the 5mg and 15mg dose levels, typically months two through six of treatment. Bupropion contribution to weight loss is modest and gradual, often not noticeable independently against the more dramatic tirzepatide effect. If you are not seeing expected results, review the comprehensive guide on why weight loss might stall before adjusting your approach.
External resources
Drugs.com interaction checker: tirzepatide and bupropion, the most widely used public drug interaction database for checking medication compatibility
FDA prescribing information for tirzepatide (Mounjaro), the complete official label including warnings, contraindications, and drug interaction data
FDA prescribing information for bupropion (Wellbutrin), the complete official label including seizure risk data and dosing guidelines
SURMOUNT-1 trial results in the New England Journal of Medicine, the landmark clinical trial demonstrating tirzepatide weight loss efficacy in adults with obesity
NIH review of GLP-1 agonist effects on gastric emptying and drug absorption, published research on how GLP-1 receptor agonists alter oral medication pharmacokinetics
Taking wellbutrin and tirzepatide together is not the simple question people want it to be. It is not dangerous. It is not prohibited. But it is a combination that requires understanding, monitoring, and communication with your healthcare providers. The absence of a direct pharmacological interaction does not mean you can autopilot through it.
You need to stay hydrated. You need to monitor your blood pressure. You need to watch for signs of electrolyte imbalance. You need to track your mood with the same attention you give to your weight. You need to take your bupropion consistently and at the right time. You need to titrate tirzepatide slowly and report side effects rather than powering through them. You need to keep every provider in the loop.
The reward for all this diligence is real. Addressing depression and obesity simultaneously, with two medications that work through complementary mechanisms and do not interfere with each other pharmacologically, represents one of the more elegant treatment combinations available today. When managed properly, the combination supports both mental health and physical health in ways that neither medication could achieve alone.
SeekPeptides members access detailed protocols for managing medication combinations, monitoring guides, and a community of people navigating the same decisions. If you are serious about optimizing your treatment approach, the resources and community support available through membership can make the difference between guessing and knowing what to do at each step.
Understanding the full picture of how your medications work together, from the dopamine pathways in your brain to the GIP receptors in your gut, puts you in the strongest possible position to make informed decisions about your health. You do not need to be a pharmacologist. You just need to care enough to read guides like this one and bring the right questions to your next appointment.
Whether you are just starting to explore how to qualify for GLP-1 therapy, comparing side effect profiles between medications, or planning how to maintain your weight loss long-term, the journey requires both the right medications and the right information. One without the other leaves you vulnerable to mistakes that are entirely preventable.
If you are still in the research phase, comparing phentermine versus semaglutide or weighing alternatives to tirzepatide, understanding how each option interacts with your existing psychiatric medications is the most important variable in your decision. The fact that bupropion plays well with tirzepatide is a genuine advantage. Not every antidepressant can say the same. And if you are curious about newer options on the horizon, the comparison between semaglutide, tirzepatide, and retatrutide gives you a sense of where the field is heading and what future combinations might look like.
Learning what to say when requesting GLP-1 options from your provider can help you navigate the conversation about adding tirzepatide to your existing bupropion regimen. Come prepared with specific questions about monitoring schedules, side effect management plans, and criteria for dose adjustments. The more informed you are, the more productive the conversation will be, and the safer the combination will be in practice.
Stay informed. Stay monitored. Stay safe.
In case I do not see you, good afternoon, good evening, and good night. May your protocols stay safe, your medications stay compatible, and your progress stay consistent.