Feb 28, 2026

Before you pile on three sweaters and blame your thermostat, there is something you should know about tirzepatide and body temperature. It is not broken equipment. It is not your imagination. And it is probably not a sign that something has gone seriously wrong with your health.
The cold you feel is real. Bone-deep, hard to shake, sometimes settling into your fingers and toes like you walked barefoot through snow. Thousands of people taking tirzepatide, whether as Mounjaro or Zepbound, report the same experience. They sit at their desk and shiver. They wrap up in blankets during summer. They wonder if something is wrong because no one warned them about this particular side effect.
Here is the complicated part. Feeling cold on tirzepatide is not technically listed as a common side effect in clinical trial data. The FDA prescribing information does not mention it prominently. Yet forums, patient communities, and healthcare providers see it constantly. The disconnect between official documentation and lived experience is striking, and it leaves people confused about what is happening inside their body, whether they should worry, and what they can actually do about it.
This guide covers everything. The physiological mechanisms behind tirzepatide cold sensitivity. The timeline for when it starts and when it stops. The red flags that separate normal cold intolerance from something that requires medical attention. And a complete protocol for managing the chill so it does not derail your progress. Because quitting a medication that is working, simply because you cannot get warm, would be a mistake. Understanding what is happening is the first step toward fixing it. SeekPeptides has compiled the most thorough breakdown available, combining published research, clinical data, and real-world patient reports into one comprehensive resource.
Why tirzepatide makes you feel cold
The answer is not simple. There is no single switch that flips when you inject tirzepatide and suddenly makes you cold. Instead, several interconnected physiological changes happen simultaneously, and they compound each other. Understanding each mechanism separately helps explain why the cold sensation can feel so intense and so persistent.
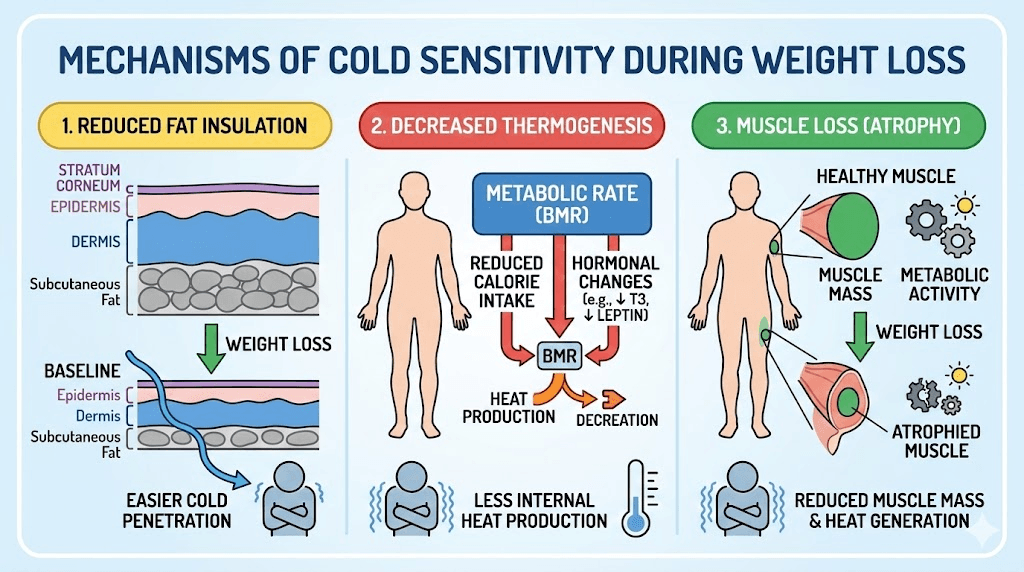
Fat loss reduces your natural insulation
This is the most straightforward explanation, and it accounts for a significant portion of the cold sensitivity people experience. Subcutaneous fat, the layer directly beneath your skin, functions as thermal insulation. It reduces heat loss from your core to the environment in much the same way a wetsuit works for a swimmer. When tirzepatide produces significant weight loss, that insulating layer shrinks. Clinical trials show participants losing 15 to 21 percent of their body weight over 72 weeks. That is a substantial reduction in the thermal barrier between your internal organs and the outside air.
Think about it practically. Someone who starts at 220 pounds and loses 35 pounds has removed a meaningful amount of insulating tissue. The areas where fat loss is most noticeable, the abdomen, arms, thighs, and face, are also areas where cold sensitivity becomes most apparent. People report feeling the chill in their extremities first, hands and feet especially, because those areas already have less insulation and are furthest from the warm core.
The rate of fat loss matters too. Tirzepatide often produces faster results than many other weight loss approaches, and rapid fat reduction gives your body less time to adapt. A gradual 10-pound loss over six months feels different than a 10-pound loss in six weeks. The speed at which your insulation disappears directly influences how dramatically you notice the temperature change.
Your body is producing less heat from food
Every time you eat, your body generates heat through a process called diet-induced thermogenesis. Digesting, absorbing, and metabolizing food requires energy, and a byproduct of that energy expenditure is warmth. You have probably noticed this yourself. After a large meal, you feel warmer. After skipping meals, you feel cooler.
Tirzepatide works partly by suppressing appetite and slowing gastric emptying. Both mechanisms reduce the total amount of food moving through your digestive system at any given time. Less food processing means less diet-induced thermogenesis. Less thermogenesis means less internal heat production. The math is straightforward, but the physical sensation can be jarring. Your body is simply generating fewer calories as heat because fewer calories are coming in.
This is particularly noticeable in the hours after your weekly injection when appetite suppression tends to peak. Many patients report that cold sensitivity is worst one to two days post-injection, exactly when the appetite-suppressing effects are strongest. The correlation is not coincidental.
Muscle loss slows metabolic heat production
Muscle tissue is metabolically active. Even at rest, muscle burns calories and generates heat. It is one of the primary contributors to your basal metabolic rate, the energy your body uses just to keep functioning. When you lose weight rapidly, you do not lose fat exclusively. Some muscle mass goes with it, especially if protein intake is inadequate or resistance training is absent.
The muscle-related effects of tirzepatide can compound the cold sensitivity problem. Less muscle means a lower basal metabolic rate. A lower basal metabolic rate means less resting heat production. Combined with reduced food intake and diminished fat insulation, the drop in muscle mass creates a triple threat against your ability to stay warm.
Research suggests that roughly 25 to 40 percent of weight lost during GLP-1 agonist treatment can come from lean mass rather than fat. That percentage varies based on protein intake, exercise habits, starting body composition, and individual genetics. But the takeaway is clear. Preserving muscle through adequate protein consumption and resistance training is not just about aesthetics or strength. It directly impacts your ability to regulate body temperature.
Adaptive thermogenesis kicks in
This one is sneaky. Adaptive thermogenesis is your body intentionally reducing energy expenditure below what the math would predict based on your new weight alone. It is a survival mechanism. When your body detects rapid energy loss, it conserves resources by turning down the metabolic furnace. Not slightly. Significantly.
Studies on adaptive thermogenesis show that energy expenditure can decrease by 15 to 20 percent beyond what reduced body mass would account for. Your body is actively suppressing heat production to conserve calories. It does this through several pathways, including reduced sympathetic nervous system activity and decreased levels of thyroid hormones that drive metabolism. Both of these changes directly lower the amount of heat your body produces at rest.
For people on tirzepatide who are experiencing substantial weight loss, adaptive thermogenesis amplifies every other cold-producing mechanism. You have less insulation, less food-generated heat, potentially less muscle mass, AND your body is deliberately dialing down energy output. The cumulative effect explains why the cold sensation can feel so much more intense than what you would expect from weight loss alone.
The hypothalamus connection
Tirzepatide is a dual GIP and GLP-1 receptor agonist, and both of these receptor types exist in the brain. The hypothalamus, which serves as your body temperature control center, contains GLP-1 receptors. Research is still ongoing, but evidence suggests that GLP-1 receptor activation in the hypothalamus may directly influence thermoregulatory setpoints.
In animal studies, GLP-1 receptor activation has been shown to affect brown fat signaling pathways through the hypothalamus. While human data is limited, the theoretical framework suggests that tirzepatide may alter how your brain perceives and responds to temperature, independent of the indirect effects from weight loss and reduced caloric intake. This could explain why some people experience cold sensitivity early in treatment, before significant weight loss has occurred.
The dual mechanism of tirzepatide, acting on both GIP and GLP-1 receptors, potentially amplifies this effect compared to semaglutide which only targets GLP-1. Whether GIP receptor activation adds to or modifies the thermoregulatory effects remains an active area of investigation.
Peripheral vasoconstriction redirects blood flow
When your body senses that it needs to conserve heat, it redirects blood flow away from extremities toward the core. This peripheral vasoconstriction is why your hands, feet, nose, and ears get cold first. The cardiovascular system prioritizes keeping vital organs warm at the expense of peripheral comfort.
Weight loss and reduced caloric intake both trigger this response. Your body interprets the energy deficit as a situation requiring conservation. Blood vessels in your fingers and toes constrict, reducing warm blood flow to those areas. The result is exactly what so many tirzepatide users describe: icy hands and feet that no amount of hand-rubbing seems to fix.
This response is particularly pronounced in the evening hours when body temperature naturally dips, and during periods of extended fasting between meals. People who are already on a structured eating plan with tirzepatide may notice their extremities getting especially cold during longer gaps between meals.
How common is cold sensitivity on tirzepatide?
The gap between clinical trial reporting and real-world experience is wider for this side effect than almost any other. Understanding why requires looking at both data sets.
What clinical trials say
In the SURMOUNT and SURPASS clinical trial programs, cold sensitivity was not listed among the common adverse effects. The most frequently reported side effects were gastrointestinal: nausea at 12 to 24 percent, diarrhea at 7 to 23 percent, and decreased appetite at 10 to 19 percent. The Mayo Clinic lists "chills" under the "incidence not known" category, meaning the effect has been observed but its frequency was not established during controlled trials.
Why the gap? Clinical trials typically use structured questionnaires to assess adverse events. If "feeling cold" or "cold sensitivity" was not specifically asked about, it would only be captured if patients volunteered the information. Given that GI effects tend to dominate the conversation during clinical visits, a side effect like feeling cold may have been underreported. It does not cause acute distress in the way that nausea does. It is uncomfortable, not alarming. So patients may not have mentioned it.
What patients actually report
The picture looks very different when you examine patient forums, Reddit communities, and telehealth provider observations. Anecdotal reports suggest that cold sensitivity affects a substantial proportion of tirzepatide users, with some providers estimating that 30 to 50 percent of their patients mention it at some point during treatment. Many describe it as one of the most persistent and noticeable non-GI side effects, alongside fatigue and hair thinning.
Descriptions range from mild to dramatic. Some people notice they need an extra layer when they previously did not. Others describe a bone-deep freeze that no amount of bundling seems to resolve. The intensity tends to correlate with the amount of weight lost and the speed of that loss, though individual variation is significant.
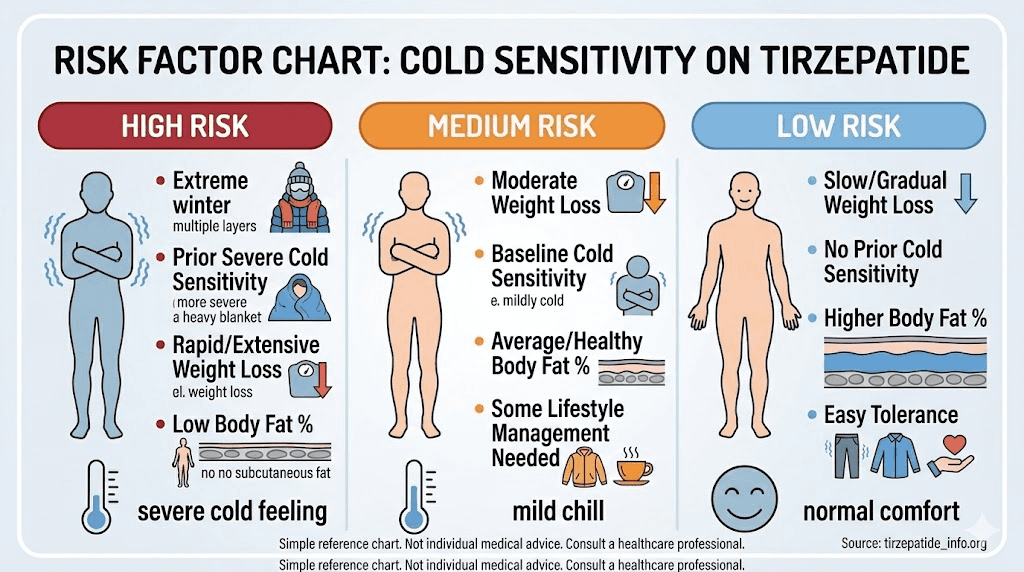
Who is most likely to experience it
Several factors increase the likelihood and severity of cold sensitivity on tirzepatide:
Higher starting BMI with rapid loss: More fat loss means more insulation removed. People who lose 15 percent or more of their body weight are more likely to notice dramatic temperature sensitivity changes.
Lower baseline muscle mass: Less muscle to start with means less metabolic heat generation. Women and older adults may be more affected for this reason.
Cold climate or season: Environmental factors amplify the sensation. Starting tirzepatide in autumn or winter makes cold sensitivity more noticeable than a summer start.
Inadequate caloric intake: People who eat very little due to appetite suppression, significantly below their maintenance needs, produce less diet-induced thermogenesis.
Pre-existing thyroid conditions: Hypothyroidism already causes cold intolerance. Tirzepatide-related changes can compound this.
Higher doses: Higher tirzepatide doses produce more aggressive appetite suppression and weight loss, increasing the physiological triggers for cold sensitivity.
When does cold sensitivity start and how long does it last?
Timing matters. Knowing when to expect cold sensitivity and how long it typically persists helps set realistic expectations and prevents unnecessary worry.
The typical timeline
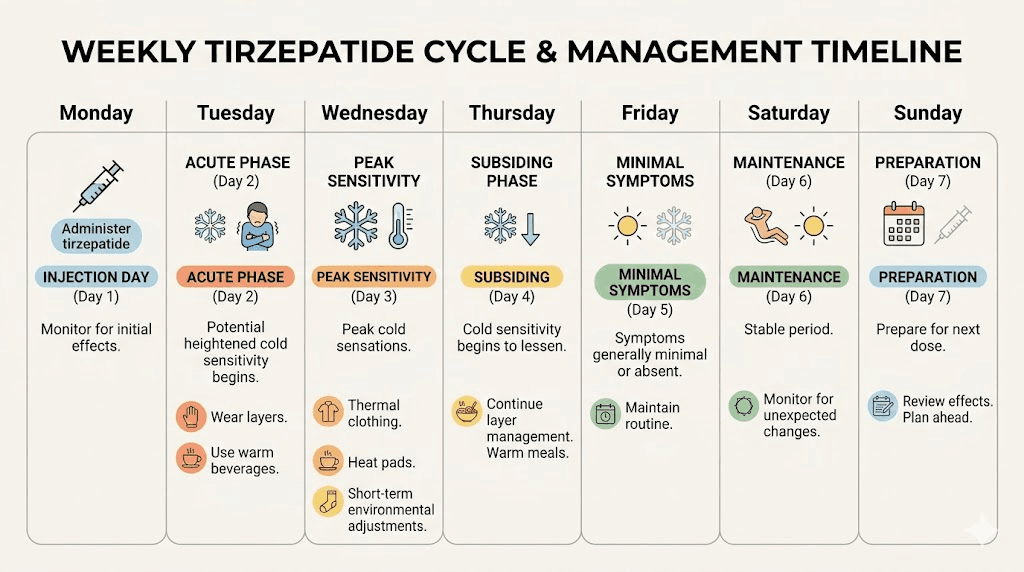
Most patients report cold sensitivity emerging within the first 6 to 8 weeks of treatment, though the onset varies considerably. Some notice it within the first week or two, especially on the days immediately following their injection. Others do not experience it until they have lost enough weight for the insulation reduction to become noticeable, which might take several months.
The pattern for many users follows a predictable cycle tied to their injection schedule. Cold sensitivity peaks one to two days after the weekly injection, when appetite suppression and metabolic effects are strongest. It then gradually eases before the next injection. Over time, this cyclical pattern may become less pronounced as the body adjusts to consistent medication levels.
For people who are just starting tirzepatide, the cold sensation during the first few weeks is often a combination of direct metabolic effects and the sudden reduction in food intake. The body has not had time to adapt, and the shift from normal caloric intake to significantly reduced consumption creates an immediate drop in diet-induced thermogenesis.
Dose escalation and temperature changes
Tirzepatide treatment follows a dose escalation schedule, typically starting at 2.5 mg weekly and increasing every four weeks through 5 mg, 7.5 mg, 10 mg, 12.5 mg, and potentially up to 15 mg. Each dose increase tends to temporarily intensify cold sensitivity.
The mechanism is straightforward. Higher doses produce stronger appetite suppression, faster weight loss, and more pronounced metabolic effects. Each step up resets the adaptation process to some degree. People who have adjusted to the cold sensation at 5 mg may find it returns with new intensity when they move to 7.5 mg. Understanding the full dosing schedule helps anticipate when these intensification periods will occur.
Some individuals find that the cold sensitivity at higher doses is simply too uncomfortable. In these cases, conversations with healthcare providers about microdosing approaches or staying at a lower maintenance dose may be appropriate. The goal is finding the balance between therapeutic benefit and manageable side effects.
Does it ever go away?
Yes. For most people.
Cold sensitivity typically improves through two pathways. First, the body gradually adapts to its new weight, composition, and energy intake. Metabolic processes stabilize, adaptive thermogenesis moderates, and the thermoregulatory system recalibrates. This adaptation takes weeks to months, not days.
Second, cold sensitivity decreases as weight loss plateaus. When your body reaches a relatively stable weight on tirzepatide, the rapid changes that drive the most intense cold sensation slow down. You are no longer losing insulation at a rapid pace. Your caloric intake stabilizes at a new baseline. Your body stops perceiving an emergency energy deficit. People who have been on tirzepatide for 6 to 12 months and reached a weight plateau often report that cold sensitivity is much more manageable than it was during the active weight loss phase.
However, some degree of increased cold sensitivity may persist indefinitely if you maintain a significantly lower body weight than your starting point. Less fat insulation means less warmth, period. This is not a medication side effect at that point. It is a consequence of having a leaner body composition. Many naturally lean people have always been cold-sensitive for this exact reason.
Cold sensitivity on tirzepatide vs. semaglutide
If you are considering switching medications or wondering whether a different GLP-1 agonist would spare you the chill, this comparison helps set expectations.
Do all GLP-1 medications cause cold sensitivity?
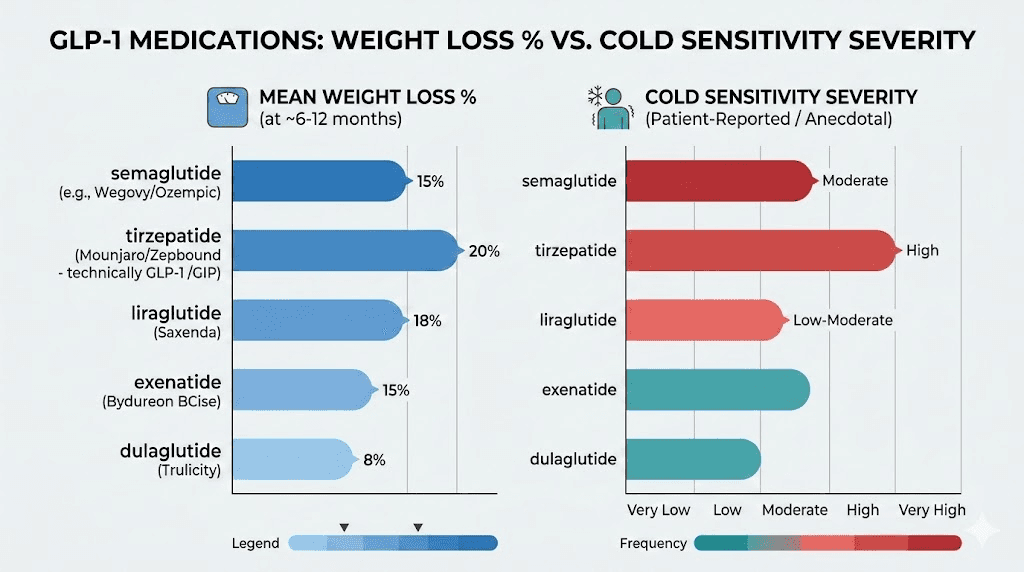
Yes. Cold sensitivity has been reported with every GLP-1 receptor agonist on the market, including semaglutide (Ozempic, Wegovy), liraglutide (Saxenda), and tirzepatide (Mounjaro, Zepbound). The mechanism is fundamentally the same across all of them: appetite suppression leads to reduced caloric intake, which leads to weight loss, which leads to reduced insulation and metabolic adaptation.
However, the degree of cold sensitivity is not identical across medications. The intensity correlates primarily with how much weight a person loses and how quickly they lose it. Since different medications produce different magnitudes of weight loss, the cold sensitivity profiles differ accordingly.
Side-by-side comparison
Factor | Tirzepatide (Mounjaro/Zepbound) | Semaglutide (Wegovy/Ozempic) |
|---|---|---|
Average weight loss | 15-21% over 72 weeks | 12-15% over 68 weeks |
Cold sensitivity severity | Often more pronounced | Moderate |
Rate of weight loss | Faster, especially at higher doses | Moderate pace |
Receptor targets | Dual GIP + GLP-1 | GLP-1 only |
Appetite suppression | More aggressive | Strong but less intense |
Time to onset | Often within 4-8 weeks | Often within 6-12 weeks |
Improvement timeline | As weight stabilizes (months) | As weight stabilizes (months) |
The comparison shows a clear pattern. Tirzepatide tends to produce more pronounced cold sensitivity because it produces more weight loss, faster. But this is not a flaw. It is the flip side of greater efficacy. Understanding the complete side effect profiles of both medications helps in making informed decisions about treatment.
Why dual agonism matters
Tirzepatide targets both GIP and GLP-1 receptors, while semaglutide targets only GLP-1. The GIP receptor component adds complexity to the metabolic picture. GIP receptors are found in adipose tissue, and their activation influences fat metabolism and storage patterns. This dual action may affect how and where fat is lost, potentially influencing the insulation reduction pattern.
Additionally, the dual mechanism produces more aggressive appetite suppression in many patients. Greater appetite suppression means less food, which means less diet-induced thermogenesis. The cascade effect is more pronounced with tirzepatide than with semaglutide for most people, though individual responses vary significantly. Some people tolerate tirzepatide with minimal cold sensitivity while struggling with it on semaglutide, and vice versa. Comparing the full range of GLP-1 options can help identify the best fit for individual tolerance profiles.
For those exploring alternatives, newer agents like survodutide, CagriSema, and orforglipron will likely produce similar cold sensitivity profiles to the degree that they produce similar weight loss. The cold comes from the loss, not the molecule.
When cold sensitivity signals something more serious
Most cold sensitivity on tirzepatide is benign. Uncomfortable, yes. Annoying, absolutely. But not dangerous. However, there are situations where feeling cold indicates an underlying problem that requires medical evaluation. Knowing the difference prevents both unnecessary panic and dangerous complacency.
Normal cold sensitivity vs. red flags
Normal tirzepatide cold sensitivity looks like this: you feel colder than you used to, especially in your hands and feet. You need an extra layer. You prefer warmer beverages. You notice it more on injection days and during periods between meals. Your core body temperature, if you measure it, remains within the normal range of 97 to 99 degrees Fahrenheit.
Red flags look different. Watch for these warning signs that suggest something beyond normal medication effects:
Core body temperature below 95 degrees Fahrenheit (35 degrees Celsius): This constitutes hypothermia and requires immediate medical attention.
Severe fatigue and weakness beyond normal tiredness: While some fatigue is common on GLP-1 medications, extreme exhaustion paired with cold intolerance suggests thyroid or other metabolic issues.
Unexplained weight changes in the wrong direction: If you are gaining weight on tirzepatide while also feeling increasingly cold, thyroid function should be evaluated.
Hair loss beyond mild shedding: Significant hair loss combined with cold intolerance, fatigue, and dry skin strongly suggests thyroid involvement.
Brittle nails and dry skin: These, alongside cold sensitivity, point toward nutritional deficiencies or thyroid dysfunction.
Cognitive changes: Brain fog, slowed thinking, and memory issues paired with cold intolerance may indicate hypothyroidism or severe B12 deficiency.
Slow heart rate or low blood pressure: Cardiovascular changes alongside cold sensitivity warrant cardiac and thyroid evaluation.
Numbness or tingling in extremities: This is different from simple cold sensation. Numbness suggests potential peripheral neuropathy, which may be related to B12 deficiency or other neurological concerns.
Thyroid function and GLP-1 medications
Thyroid disorders and tirzepatide cold sensitivity can mimic each other almost perfectly. Hypothyroidism causes cold intolerance, fatigue, weight gain, dry skin, and cognitive slowing. These overlap significantly with the side effects some people experience on GLP-1 medications.
The concern is real because GLP-1 receptor agonists carry a boxed warning about thyroid C-cell tumors based on animal studies. While the risk of thyroid cancer in humans remains under investigation, the warning means providers should be monitoring thyroid health in patients on these medications. If cold sensitivity is disproportionate to the amount of weight lost, or if it develops suddenly rather than gradually, thyroid function testing is appropriate.
A basic thyroid panel including TSH, free T3, and free T4 can quickly rule out or confirm thyroid involvement. If you already had borderline thyroid function before starting tirzepatide, the metabolic changes from weight loss could tip the balance into clinical hypothyroidism.
Vitamin B12 deficiency connection
This is an underrecognized issue. GLP-1 receptor agonists, by slowing gastric emptying and altering gut motility, can reduce B12 absorption over time. B12 deficiency causes a range of symptoms including fatigue, cognitive changes, numbness and tingling in extremities, and yes, cold sensitivity.
The connection to cold specifically occurs because B12 is essential for red blood cell production and nerve function. Deficiency can lead to anemia, which reduces oxygen delivery to tissues and impairs thermoregulation. It can also cause peripheral neuropathy, which may present as cold sensations in the hands and feet that are actually nerve-related rather than temperature-related.
Many tirzepatide formulations now include vitamin B12 or methylcobalamin specifically to address this risk. If your formulation does not include B12, periodic monitoring of B12 levels is prudent, especially if cold sensitivity is accompanied by tingling, numbness, or unusual fatigue. The supplement guide for tirzepatide users covers B12 and other recommended additions in detail.
Peripheral neuropathy vs. simple cold intolerance
There is an important distinction between feeling cold and feeling numb. Simple cold intolerance means your hands and feet feel uncomfortably cold but retain normal sensation. You can feel texture, pressure, and temperature differences. The cold is unpleasant but your nerves are functioning normally.
Peripheral neuropathy presents differently. Your extremities may feel cold, but they may also tingle, burn, feel "pins and needles," or lose sensation entirely. You might not feel the temperature difference between hot and cold water on your fingertips. You might drop things because your grip sensation is impaired.
If your cold sensitivity includes any sensory changes beyond simple temperature discomfort, report it to your healthcare provider promptly. Peripheral neuropathy has multiple potential causes in tirzepatide users, including B12 deficiency, rapid weight loss affecting nerve compression points, and blood sugar fluctuations. Early identification allows for early intervention.
When to contact your healthcare provider
Make an appointment if you experience any of the following:
Cold sensitivity that is severe enough to interfere with daily activities
Cold sensitivity that develops suddenly rather than gradually
Cold sensitivity accompanied by numbness, tingling, or loss of sensation
Cold sensitivity paired with significant hair loss, extreme fatigue, or cognitive changes
Core body temperature consistently below 97 degrees Fahrenheit
Cold sensitivity that worsens despite stable weight
Any suspicion that your symptoms go beyond normal medication effects
Your provider can order appropriate bloodwork including thyroid panel, complete blood count, B12 levels, iron studies, and metabolic panel to rule out underlying causes. In most cases, the results will be reassuring. But catching a treatable condition early makes all the difference.
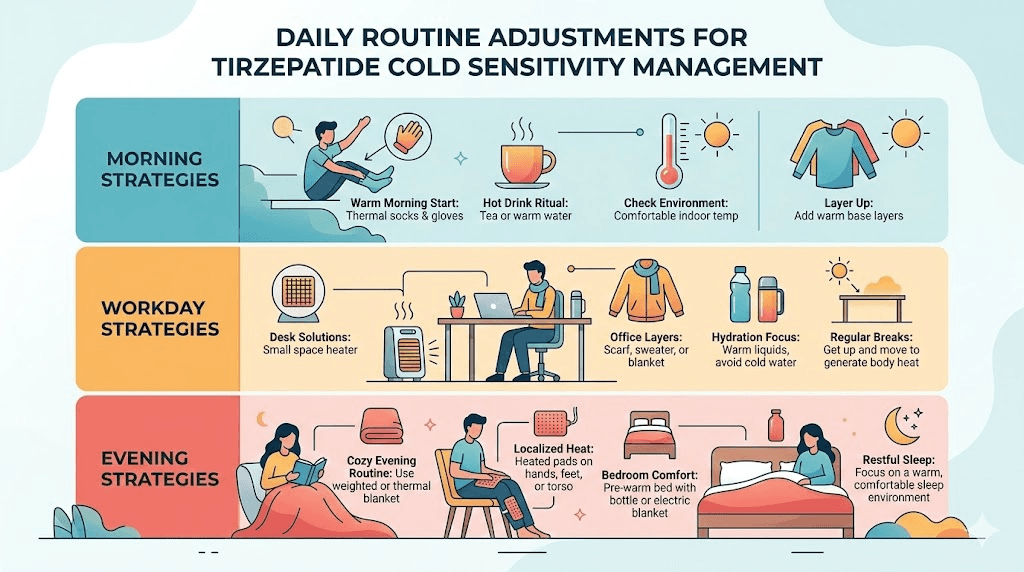
Complete protocol for managing tirzepatide cold sensitivity
Knowing why you feel cold is useful. Knowing what to do about it is essential. This section provides a systematic approach to managing cold sensitivity across every relevant domain, from clothing to nutrition to exercise to supplementation.
Clothing and environmental strategies
Start with the basics. They matter more than people think.
Layering system: Use three layers as your foundation. A moisture-wicking base layer keeps perspiration from cooling your skin. A middle insulating layer, fleece or merino wool, traps warm air. An outer layer blocks wind and elements. This system works better than one thick garment because you can adjust throughout the day as your body temperature fluctuates.
Extremity protection: Your hands and feet lose heat fastest due to vasoconstriction. Invest in quality thermal socks, ideally merino wool, and wear them consistently. Keep fingerless gloves at your desk for typing. Use warm slippers at home. A hat retains significant body heat since your head is a major heat-loss area. These small additions make a surprisingly large difference.
Home temperature: Set your thermostat to 68 to 72 degrees Fahrenheit (20 to 22 degrees Celsius). If you share a home with someone who does not need the extra warmth, a space heater in your primary living area is a reasonable compromise. Electric blankets and heated mattress pads transform sleep quality for cold-sensitive tirzepatide users.
Warm beverages: Keep a thermos of warm water, herbal tea, or bone broth nearby throughout the day. The internal warmth from hot liquids is modest but real, and the habit of sipping warm drinks creates a constant, low-level heat input. Bone broth adds the bonus of protein and electrolytes.
Workspace adjustments: A small desk heater, a heated keyboard pad, or even a hot water bottle on your lap can make office work comfortable when the office thermostat is set for people who are not losing weight rapidly. These tools seem minor but they address the specific problem, cold extremities during sedentary periods.
Nutrition protocol for maintaining body heat
What you eat, when you eat, and how much you eat all directly influence your body heat production. Optimizing nutrition is one of the most effective strategies for managing cold sensitivity.
Protein priority: Protein has the highest thermic effect of any macronutrient. Your body uses 20 to 30 percent of the calories from protein just to digest and process it, compared to 5 to 10 percent for carbohydrates and 0 to 3 percent for fat. This means protein literally generates more heat during digestion than other foods. Aim for 1.0 to 1.2 grams per kilogram of body weight daily during active weight loss. The tirzepatide nutrition guide covers meal planning strategies in detail.
Do not skip meals: Even when appetite is suppressed, eating regular meals maintains a baseline of diet-induced thermogenesis. Three moderate meals are better for temperature regulation than one large meal and two skipped meals. If large meals feel impossible due to appetite suppression, smaller frequent meals or protein shakes maintain caloric throughput and heat production.
Warm foods over cold foods: This seems obvious, but it is worth emphasizing. Warm soups, stews, cooked meals, and hot beverages contribute direct thermal energy. A bowl of warm bone broth with vegetables provides both heat and nutrition. Cold salads, smoothies, and chilled foods do the opposite. Structuring meals around warm preparations makes a noticeable difference.
Iron-rich foods: Iron is essential for hemoglobin production, and hemoglobin carries oxygen to tissues. Iron deficiency anemia reduces oxygen delivery and impairs thermoregulation. Women of reproductive age are at higher risk, especially during weight loss when dietary variety may decrease. Include red meat, spinach, legumes, and fortified grains. If your dietary restrictions limit iron sources, supplementation may be appropriate.
The complete tirzepatide meal plan provides structured approaches that address both weight management goals and temperature regulation needs. Balancing caloric restriction with adequate nutrition is the core challenge, and getting it right improves both cold tolerance and overall outcomes.
Exercise approach for metabolic heat generation
Exercise is the single most powerful tool for immediate and long-term cold sensitivity management. It addresses multiple mechanisms simultaneously.
Immediate heat generation: Physical activity produces heat directly. A 30-minute walk raises your core temperature and improves circulation for hours afterward. On days when cold sensitivity is worst, typically one to two days post-injection, even a brief walk or bodyweight exercise session can break the chill.
Resistance training for muscle preservation: This is critical. Maintaining and building muscle mass preserves your metabolic heat production capacity. Aim for two to three resistance training sessions per week, focusing on compound movements like squats, deadlifts, rows, and presses. These large muscle group exercises produce the most metabolic activity and the most heat. Losing weight without resistance training accelerates muscle loss and worsens cold sensitivity.
Cardiovascular exercise for circulation: Regular aerobic activity improves cardiovascular efficiency and peripheral blood flow. Better circulation means warmer extremities. The recommended target is 150 to 300 minutes of moderate-intensity aerobic exercise per week. Walking, cycling, swimming, and rowing all qualify. Understanding the broader benefits of exercise while on tirzepatide can help maintain motivation beyond the cold management aspect.
Morning exercise routine: Exercising in the morning raises metabolic rate for the rest of the day. This elevated metabolism produces more heat throughout your waking hours. If cold sensitivity is worst in the morning, a brief workout before starting your day, even 15 to 20 minutes, can set a warmer baseline for the hours that follow.
Avoid prolonged sedentary periods: Sitting still for hours allows body temperature to drop. Set reminders to stand and move every 30 to 60 minutes. A brief walk, some stretches, or a few bodyweight squats are enough to boost circulation and generate warmth.
Supplements that support temperature regulation
While no supplement directly eliminates tirzepatide cold sensitivity, several address underlying factors that contribute to it.
Vitamin B12: As discussed above, B12 supports red blood cell production and nerve function, both essential for proper thermoregulation. If your tirzepatide formulation does not include B12 in the compound, supplementing with 1000 mcg of methylcobalamin daily is a reasonable precaution. Sublingual forms bypass the gut absorption issues that GLP-1 agonists may create.
Iron: Supplement only if blood work confirms deficiency or low-normal levels. Excessive iron supplementation has its own risks. A standard dose of 18 to 27 mg daily from a multivitamin is generally sufficient for prevention. If deficiency is confirmed, your provider will recommend a therapeutic dose.
Vitamin D: Deficiency is common in the general population and may be more prevalent during weight loss. While vitamin D does not directly affect thermoregulation, it supports immune function, bone health, and muscle function, all of which interact with cold tolerance. A dose of 2000 to 4000 IU daily is commonly recommended.
Omega-3 fatty acids: Fish oil supports cardiovascular health and may improve peripheral blood flow. The anti-inflammatory properties can also help with body aches and joint pain that sometimes accompany weight loss. A dose of 1000 to 2000 mg of combined EPA and DHA daily is standard.
The comprehensive supplement guide for tirzepatide users covers additional options and dosing recommendations. Always discuss supplement additions with your healthcare provider, especially if you take other medications.
Timing strategies around injection day
Since cold sensitivity often peaks one to two days after injection, planning around this cycle can help manage the worst days.
Choose your injection day strategically: If weekends allow for more flexibility to dress warmly, control your environment, and exercise, injecting on Thursday or Friday means the peak cold period falls on days when you have more control over your comfort. The best time to take your tirzepatide shot involves considering multiple factors, and cold sensitivity management is a legitimate one.
Plan warm meals for post-injection days: Stock your refrigerator with ingredients for warm, protein-rich meals before your injection day. Soups, stews, and slow-cooker meals are ideal because they can be prepared in advance and reheated easily during the days when appetite is most suppressed and cold is most intense.
Schedule exercise on peak cold days: Counterintuitive as it sounds, light to moderate exercise on the days when you feel coldest provides the most relief. A warm shower after the workout extends the warming effect.
The science of brown adipose tissue and tirzepatide
Brown adipose tissue, commonly called brown fat, is your body natural furnace. It generates heat by burning calories through a process distinct from the way white fat stores energy. The relationship between tirzepatide and brown fat is one of the most fascinating and seemingly contradictory aspects of this side effect story.
What brown fat does
Unlike white adipose tissue which stores energy, brown adipose tissue exists specifically to produce heat. It does this through a protein called UCP-1 (uncoupling protein 1), which short-circuits the normal cellular energy production process and converts stored energy directly into warmth. This is called non-shivering thermogenesis.
Brown fat is activated by cold exposure and by sympathetic nervous system stimulation. When you step into cold air, your body activates brown fat to generate heat and maintain core temperature. It is concentrated in areas around the neck, upper back, and along the spine. Adults have varying amounts of brown fat, with leaner individuals typically having more active brown fat depots.
Brown fat is metabolically expensive in a good way. Active brown fat burns significant calories. Researchers have explored brown fat activation as a potential weight loss strategy, which is where the tirzepatide connection becomes interesting.
The tirzepatide thermogenic amino acid signature
A study published in Molecular Metabolism (Staresinic et al.) found that chronic tirzepatide administration in mice produced a thermogenic-like amino acid signature in brown adipose tissue. Specifically, tirzepatide increased the catabolism of branched-chain amino acids (BCAAs) within brown fat, a pattern that normally occurs during cold exposure.
The numbers were significant. Valine labeling in brown fat roughly doubled (19.05 nmol/g with tirzepatide versus 9.61 nmol/g with vehicle). The metabolite 3-HIB, a BCAA breakdown product, increased more than fourfold (11.19 nmol/g versus 2.62 nmol/g). TCA cycle intermediates including alpha-ketoglutarate, fumarate, malate, succinate, and citrate were all elevated, indicating increased metabolic activity in brown fat tissue.
A separate study published in Frontiers in Nutrition found that tirzepatide raised brown fat activity compared to pair-fed controls, with 1,053 differentially expressed genes identified. "Thermogenesis" and "oxidative phosphorylation" were among the most enriched pathways, suggesting that tirzepatide actively promotes heat-generating processes in brown fat.
What this means for cold sensitivity
Here is the paradox. Tirzepatide appears to activate brown fat thermogenesis, which should theoretically make you warmer. Yet people on tirzepatide report feeling colder. How do these observations coexist?
The answer likely involves balance. While tirzepatide may activate brown fat, the cumulative effects of reduced food intake, lost insulating white fat, decreased muscle mass, and adaptive thermogenesis overwhelm whatever additional heat brown fat produces. The brown fat activation represents one warming input. The cooling factors represent several simultaneous cooling inputs. The net result is still a temperature deficit for most people.
Additionally, the brown fat studies were conducted in mice, and direct translation to human experience is not straightforward. Mice have proportionally more brown fat than adult humans, and their thermoregulatory systems respond differently. A clinical trial called TABFAT is currently investigating tirzepatide effects on brown and beige adipose tissue in humans, which should provide more definitive data about whether the animal findings translate to meaningful brown fat activation in people.
The implications for understanding tirzepatide metabolic effects are significant. If tirzepatide does meaningfully activate human brown fat, it would mean the medication is not just reducing calories in, it is also modifying how the body processes energy and generates heat. This weight-independent metabolic effect could partially explain why tirzepatide produces greater weight loss than caloric restriction alone would predict.
Dose-dependent cold sensitivity patterns
Not all doses of tirzepatide produce the same degree of cold sensitivity. Understanding how dose relates to temperature regulation helps in making dosing decisions with your healthcare provider.
Low-dose vs. high-dose effects
At the starting dose of 2.5 mg, cold sensitivity is typically mild if present at all. The appetite suppression at this dose is moderate, weight loss is just beginning, and the metabolic shifts that drive cold sensitivity have not fully developed. Most people notice little to no temperature change at the starting dose.
As doses increase through the standard escalation schedule, cold sensitivity tends to increase in parallel. The 7.5 mg to 10 mg range is where many people first notice a meaningful difference. Appetite suppression becomes more aggressive, weight loss accelerates, and the combined physiological changes produce noticeable cold intolerance.
At 12.5 mg and 15 mg, the maximum approved doses, cold sensitivity can be significant for some individuals. These doses produce the most aggressive appetite suppression and the fastest weight loss, which amplifies every mechanism contributing to cold intolerance. However, individual variation is enormous. Some people tolerate 15 mg with minimal cold sensitivity while others struggle at 7.5 mg. Body composition, metabolic rate, genetic factors, and environmental conditions all influence the individual response.
Microdosing and temperature regulation
The growing interest in tirzepatide microdosing creates an interesting option for cold sensitivity management. Microdosing uses lower-than-standard doses, sometimes splitting standard doses across the week rather than taking them all at once.
From a cold sensitivity perspective, microdosing offers potential advantages. Lower individual doses produce less dramatic appetite suppression peaks, which means less severe drops in diet-induced thermogenesis. The more stable drug levels may reduce the cyclical cold intensity that peaks post-injection. And the gentler weight loss pace gives the body more time to adapt to composition changes.
The microdosing schedule and split dosing approaches are worth discussing with your provider if cold sensitivity is significantly impacting quality of life. The tradeoff is potentially slower weight loss in exchange for better tolerance of side effects including cold sensitivity.
Finding the right balance
Cold sensitivity should be part of the conversation when determining your optimal dose. If you are losing weight effectively at 7.5 mg and tolerating the side effects well, there may be no reason to escalate to 10 mg or higher. The goal is the minimum effective dose that produces the desired therapeutic outcome with manageable side effects.
Use the compounded tirzepatide dosage calculator to understand the dosing options available and discuss adjustments with your provider. Some people find that a moderate dose combined with good nutrition and exercise habits produces excellent results without the severe cold sensitivity that higher doses can trigger.
If you are on a higher dose and cold sensitivity becomes problematic, dose adjustment strategies include reducing to the previous dose, extending the interval between doses, or transitioning to a microdosing protocol. None of these decisions should be made without healthcare provider guidance.
Practical tips from experienced tirzepatide users
Beyond the clinical recommendations, people who have navigated months or years of tirzepatide cold sensitivity have developed practical strategies worth sharing.
Morning routines that help
The morning is typically when cold sensitivity is most noticeable. Your body temperature is at its daily low point, you have been fasting overnight, and metabolic rate has not ramped up from activity yet. Experienced users recommend:
Start with a warm beverage immediately upon waking. Coffee, tea, or warm lemon water raises internal temperature and provides a psychological boost. Follow it with a warm breakfast prioritizing protein. Warm oatmeal with protein powder, scrambled eggs, or warm bone broth with toast all work. The combination of warm liquid and protein-rich food maximizes diet-induced thermogenesis.
A brief morning exercise session, even 10 to 15 minutes, raises metabolic rate and generates heat that persists for hours. Bodyweight squats, jumping jacks, push-ups, or a brisk walk around the block are all sufficient. Some users combine this with a warm shower afterward, creating a warming cascade that carries through the first half of the day.
Dress warmly before you feel cold, not after. Layering preemptively is more effective than trying to warm up once the chill has set in. Keep warm clothing accessible, not stored away in closets.
Workspace and home adjustments
For people who work in offices where they do not control the thermostat, cold sensitivity on tirzepatide can be particularly challenging. Here are approaches that work:
USB-powered hand warmers and heated mouse pads keep your hands functional during desk work. A lap blanket or heated throw provides core warmth without looking conspicuous. If you have your own office, a small space heater under the desk warms your feet and lower legs, the areas most affected by vasoconstriction.
At home, electric blankets are universally praised by cold-sensitive tirzepatide users. A heated mattress pad transforms sleep quality. Smart thermostats that automatically raise the temperature during your typical cold-sensitive hours, usually early morning and evening, prevent the need to constantly adjust.
Hot water bottles are an old-fashioned solution that works remarkably well. Keep one in your lap during evening television time or at your feet while sleeping. They provide hours of consistent, gentle warmth without the electrical cost of heating an entire room.
Travel considerations
Traveling while on tirzepatide requires careful planning, and cold sensitivity adds another consideration. Pack more warm layers than you think you will need. Air conditioning on planes, in hotels, and in restaurants can make cold-sensitive people miserable. A packable down vest or compact fleece takes minimal luggage space but provides significant warmth.
Time zone changes may shift your injection schedule, which can affect the timing of peak cold sensitivity. Plan accordingly. If you know you will be in transit on your peak cold day, pack extra warm items and choose comfortable, warm clothing for travel.
Destination climate matters too. If you used to be comfortable in short sleeves at your destination, you may now need layers. Check forecasts and pack for temperatures 10 to 15 degrees Fahrenheit cooler than what you would have considered comfortable before starting tirzepatide.
Long-term outlook for tirzepatide cold sensitivity
Understanding the long-term trajectory helps maintain perspective during the uncomfortable early months.
The adaptation curve
Most people experience the worst cold sensitivity during the first 3 to 6 months of treatment, which coincides with the period of most rapid weight loss. As weight loss decelerates and the body composition stabilizes, cold sensitivity gradually improves. The body recalibrates its thermoregulatory processes, adaptive thermogenesis moderates, and the new metabolic baseline becomes normal.
By the 6 to 12 month mark, the majority of users report that cold sensitivity has improved significantly from its peak, though it may not return to pre-treatment levels. The remaining cold sensitivity is largely a function of having less insulating tissue, which is a permanent change as long as the lower weight is maintained.
Maintenance phase improvements
Once you transition from active weight loss to weight maintenance, cold sensitivity typically improves further. Caloric intake stabilizes at a higher level than during active loss, increasing diet-induced thermogenesis. Adaptive thermogenesis gradually resolves as the body stops perceiving a caloric emergency. Muscle mass may increase if resistance training continues, adding metabolic heat production.
Some people reduce their tirzepatide dose during maintenance, which also reduces the medication-related component of cold sensitivity. Others discontinue the medication entirely once their goals are met, though this requires careful planning to prevent weight regain. The decision about long-term GLP-1 use involves multiple factors, and cold sensitivity can be one consideration in the conversation.
Building cold tolerance over time
Interestingly, deliberate cold exposure practices, such as cold showers, cold water immersion, or spending time in cooler environments, can improve cold tolerance over time by activating and expanding brown adipose tissue. This is not about suffering. It is about gradual adaptation.
Start with ending your warm shower with 30 seconds of cool water. Over weeks, gradually extend the duration and lower the temperature. This practice has been shown to increase brown fat activity and improve cold tolerance independent of medication effects. Some tirzepatide users report that combining deliberate cold exposure with their treatment protocol made their overall cold sensitivity more manageable over time.
The approach requires patience. Cold adaptation takes weeks to months, and the benefits are cumulative. But it represents a proactive strategy that addresses the underlying physiology rather than just managing symptoms.
Frequently asked questions
Is feeling cold on tirzepatide dangerous?
For the vast majority of people, no. Cold sensitivity on tirzepatide is uncomfortable but not dangerous. It reflects the normal physiological consequences of weight loss and reduced caloric intake. However, if your core body temperature drops below 95 degrees Fahrenheit, or if cold sensitivity is accompanied by numbness, severe fatigue, significant hair loss, or cognitive changes, contact your healthcare provider for evaluation. These could indicate underlying issues beyond normal medication effects.
Does everyone on tirzepatide feel cold?
No. While cold sensitivity is commonly reported, not everyone experiences it, and the severity varies widely. People who lose more weight, lose it faster, have lower baseline muscle mass, or live in cooler climates tend to notice it more. Some people on tirzepatide report no noticeable temperature sensitivity changes at all. Individual metabolic differences, genetics, and environmental factors all influence whether and how intensely this side effect manifests.
Will switching from tirzepatide to semaglutide help with cold sensitivity?
Possibly, but not because one medication is inherently "warmer" than the other. Semaglutide typically produces less total weight loss than tirzepatide, which means less insulation reduction and potentially less cold sensitivity. However, if you are switching medications, the cold sensitivity will depend primarily on how much weight you continue to lose, not on which molecule you are using. Both medications produce cold sensitivity through the same fundamental mechanisms.
How long does tirzepatide cold sensitivity last?
Cold sensitivity typically peaks during the first 3 to 6 months of treatment, when weight loss is most rapid. It gradually improves as weight stabilizes and the body adapts. Most people report meaningful improvement by 6 to 12 months. Some degree of increased cold sensitivity may persist indefinitely if you maintain a significantly lower body weight, but this reflects your new body composition rather than an ongoing medication effect.
Can I take anything to stop feeling cold on tirzepatide?
There is no magic pill that eliminates tirzepatide cold sensitivity. However, a combination approach works well: adequate protein intake (1.0-1.2g/kg daily), regular exercise especially resistance training, B12 supplementation, layered warm clothing, environmental temperature management, and warm foods and beverages. Addressing the underlying mechanisms through nutrition and exercise is more effective than any single supplement or intervention.
Does the cold sensitivity get worse with higher doses?
Generally yes. Higher tirzepatide doses produce more aggressive appetite suppression and faster weight loss, both of which intensify cold sensitivity. Each dose escalation may temporarily worsen cold intolerance as the body adjusts. If cold sensitivity is severely affecting quality of life, discuss dose adjustment options with your healthcare provider, including microdosing protocols or maintaining a lower dose.
Should I stop taking tirzepatide because of cold sensitivity?
Cold sensitivity alone is rarely a sufficient reason to discontinue tirzepatide, especially if the medication is producing meaningful weight loss results and improving metabolic health markers. The management strategies outlined above can significantly reduce the impact of cold sensitivity. However, if cold intolerance is accompanied by concerning symptoms like numbness, extreme fatigue, or cognitive changes, or if it is severe enough to significantly impair daily functioning, discuss alternatives with your provider. Options include dose reduction, transitioning approaches, or investigating underlying causes.
Does cold sensitivity affect tirzepatide effectiveness?
No. Feeling cold does not reduce the therapeutic effectiveness of tirzepatide for weight loss or blood sugar management. In fact, cold sensitivity is often a sign that the medication is working as intended, producing the metabolic changes and weight loss that are its primary therapeutic goals. The cold is a side effect of the solution, not a separate problem.
External resources
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your thermostat stay comfortable, your layers stay warm, and your tirzepatide results stay worth every shiver.