Mar 8, 2026
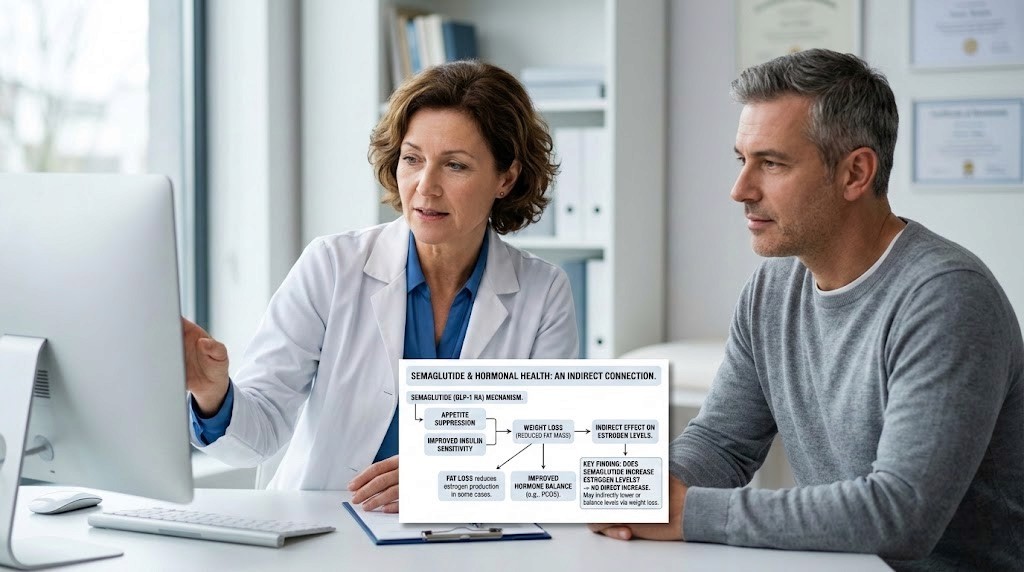
At the cellular level, semaglutide does something unexpected. It does not touch estrogen receptors. It does not stimulate the ovaries. It does not directly interfere with any hormone-producing gland in the body. And yet, women across the country report hormonal shifts after starting this GLP-1 receptor agonist, from changes in menstrual cycles to shifts in mood, energy, and even libido.
The confusion makes sense. When something changes your hormones, you want to know why. You want to know if the medication is safe. You want to know if these changes are temporary, permanent, or something to worry about.
Here is the short answer: semaglutide does not directly increase estrogen levels. But the full story is far more interesting, and far more important for anyone using this peptide for weight loss, blood sugar management, or metabolic health. The relationship between semaglutide and estrogen is indirect, running through fat tissue, insulin sensitivity, and a cascade of metabolic changes that reshape the entire hormonal landscape. Understanding this relationship is not optional for anyone serious about optimizing their semaglutide protocol. It is essential.
This guide covers everything: the mechanisms, the research, the timeline, and the practical steps to manage hormonal changes while using semaglutide. Whether you are premenopausal, postmenopausal, dealing with PCOS, or simply curious about how GLP-1 medications interact with your hormonal system, the answers are here.
How semaglutide actually works in the body
Before diving into estrogen, you need to understand what semaglutide does at a fundamental level. Semaglutide is a synthetic peptide that mimics GLP-1, a hormone your gut naturally produces after eating. It binds to GLP-1 receptors in the brain, pancreas, and gastrointestinal tract. The result is a powerful combination of reduced appetite, slower gastric emptying, improved insulin secretion, and decreased glucagon release.
None of these mechanisms directly involve estrogen production.
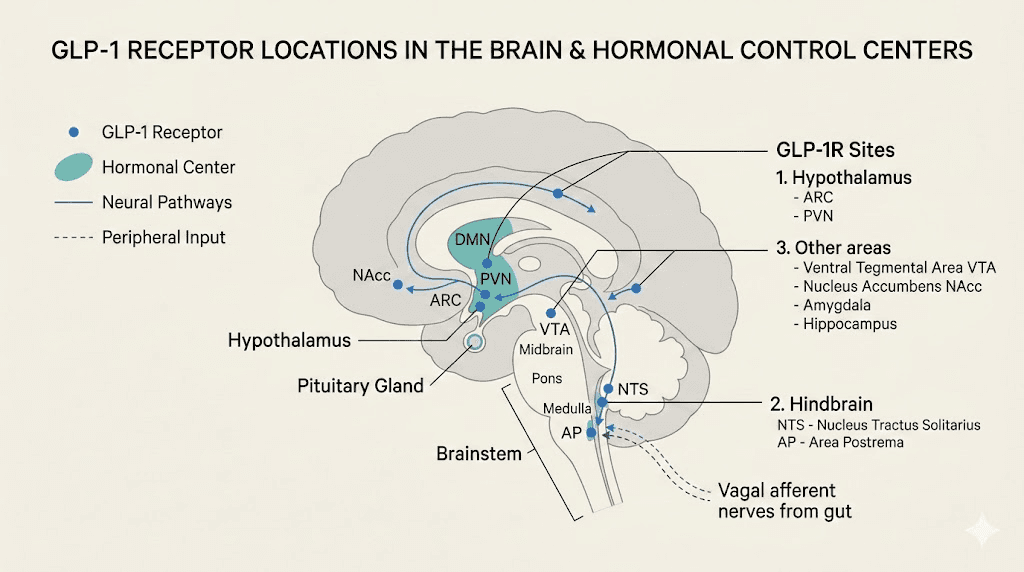
GLP-1 receptors exist in the hypothalamus, the brain region that controls both appetite and hormonal signaling. This is where things get interesting. While semaglutide targets appetite centers specifically, the hypothalamus also houses the command center for the hypothalamic-pituitary-ovarian (HPO) axis, the system that regulates estrogen, progesterone, and the entire menstrual cycle. The proximity of these pathways means that changes in one system can ripple into another, even without direct interaction.
Think of it like neighbors sharing a wall. Semaglutide is doing renovation work on one side. The hormonal system on the other side feels the vibrations.
The fat-estrogen connection: why weight loss changes everything
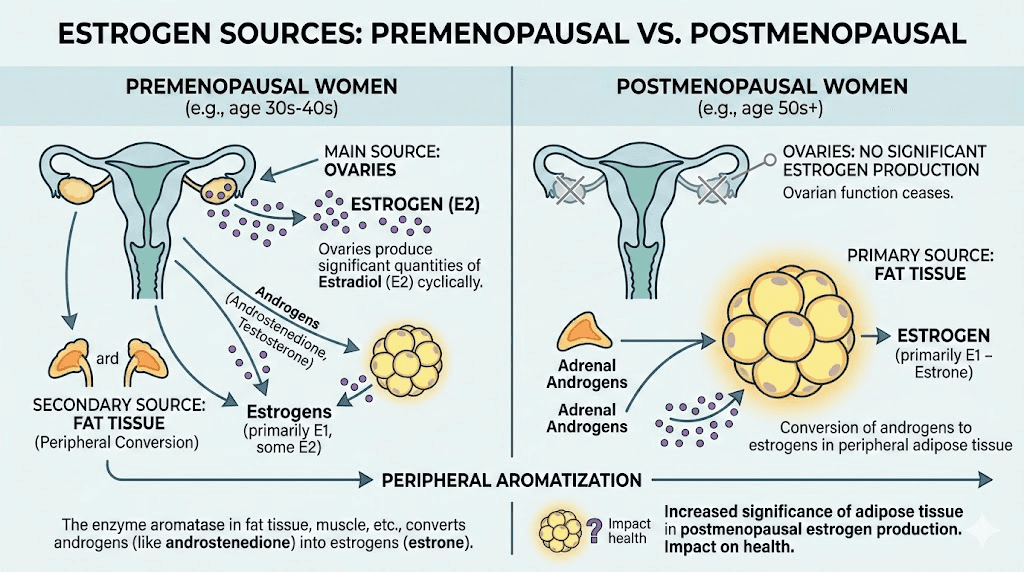
This is the single most important concept for understanding how semaglutide affects estrogen. Fat tissue is not just storage. It is an active endocrine organ that produces estrogen through a process called aromatization, where an enzyme called aromatase converts androgens (like testosterone) into estrogen.
The more fat tissue you carry, the more estrogen your body produces through this pathway.
When semaglutide drives significant weight loss, fat tissue decreases. As fat decreases, so does the aromatase activity within that tissue. The result is a measurable reduction in estrogen production from adipose sources. For premenopausal women, the ovaries remain the primary estrogen source, so this shift may be subtle. For postmenopausal women, where fat tissue is the primary estrogen source, the impact can be significant.
Research from the journal Menopause found that postmenopausal women on hormone therapy achieved approximately 30% greater weight loss with semaglutide compared to those not on HRT. This suggests that estrogen levels play an active role in how effectively semaglutide works, and vice versa.
What this means for different body compositions
The degree of estrogen change depends heavily on starting body composition. Someone with a BMI of 40 who loses 50 pounds will experience a more dramatic shift in adipose-derived estrogen than someone with a BMI of 30 who loses 20 pounds. The relationship is roughly proportional to fat mass lost, though individual genetics and metabolic factors play a role.
Women who carry more visceral fat (around the organs) tend to have higher aromatase activity than those who carry subcutaneous fat (under the skin). Since semaglutide preferentially reduces visceral fat in many users, the estrogen impact can be amplified in this population.
The estrogen paradox of obesity
Here is something most guides do not explain. In obesity, estrogen levels from fat tissue are often elevated, but this is not the "good" kind of estrogen dominance. Excess adipose-derived estrogen contributes to insulin resistance, irregular cycles, increased breast cancer risk, and a host of metabolic problems. When semaglutide reduces this excess estrogen production through fat loss, it is actually moving estrogen levels toward a healthier baseline.
The confusion arises because people associate "lower estrogen" with something negative. But lowering abnormally elevated estrogen is therapeutic. The goal is not maximum estrogen. The goal is balanced estrogen, and semaglutide-driven weight loss often helps achieve exactly that.
Semaglutide and menstrual cycle changes
Many women notice menstrual changes within the first few months of starting semaglutide. These can include heavier or lighter periods, shorter or longer cycles, spotting between periods, or temporary irregularity. The changes are real, documented, and usually temporary.
Three distinct mechanisms drive these changes.
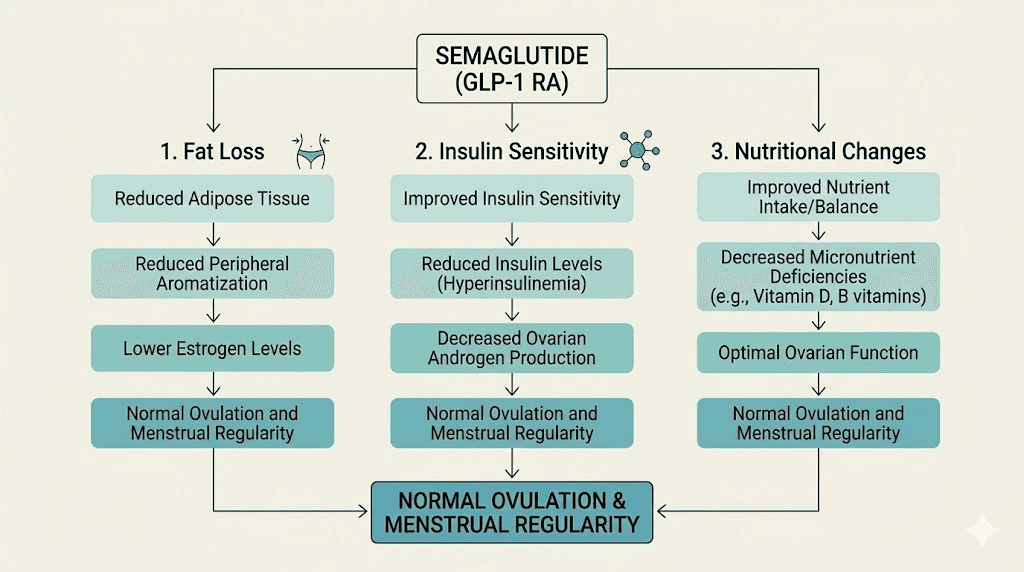
Mechanism one: estrogen shifts from fat loss. As discussed above, rapid weight loss reduces adipose-derived estrogen. The body needs time to recalibrate. During this adjustment period, cycles may become irregular as the hypothalamic-pituitary-ovarian axis adapts to new estrogen levels.
Mechanism two: improved insulin sensitivity. Semaglutide dramatically improves insulin sensitivity. Insulin and sex hormones are deeply connected. High insulin levels stimulate the ovaries to produce excess androgens and disrupt the normal estrogen-progesterone balance. When insulin drops, this disruption resolves, and cycles may temporarily shift before stabilizing in a healthier pattern.
Mechanism three: nutritional changes. Semaglutide significantly reduces caloric intake through appetite suppression. Dramatic caloric restriction, even when medically supervised, can signal the hypothalamus to reduce reproductive hormone output. This is the same mechanism behind exercise-induced amenorrhea in athletes. The body interprets significant energy deficit as a signal that conditions are not optimal for reproduction.
What the research shows about cycle changes
Clinical data from GLP-1 receptor agonist studies shows that menstrual irregularity is reported by approximately 5-10% of premenopausal women using these medications. The majority of cases resolve within 3-6 months as the body adapts. Some women actually report improved cycle regularity, particularly those who had irregular periods related to obesity or insulin resistance before starting treatment.
The key takeaway: cycle changes do not mean semaglutide is "increasing" or "decreasing" estrogen in a harmful way. The body is recalibrating. Monitoring these changes with your healthcare provider is wise, but they rarely indicate a serious problem.
Semaglutide, PCOS, and hormonal balance
Polycystic ovary syndrome affects roughly 10% of women of reproductive age, and it represents one of the most fascinating intersections between semaglutide and hormonal health. PCOS is fundamentally a metabolic disorder characterized by insulin resistance, elevated androgens, and irregular ovulation. The hormonal chaos of PCOS creates a vicious cycle: insulin resistance drives androgen production, elevated androgens disrupt estrogen-progesterone balance, and the resulting metabolic dysfunction makes weight management extremely difficult.
Semaglutide breaks this cycle at multiple points.
A meta-analysis published in the journal Reproductive Biology and Endocrinology found that GLP-1 receptor agonists reduced total testosterone levels by approximately 33% in women with PCOS. This is a massive hormonal shift. Lower testosterone means less disruption to the estrogen-progesterone balance, which means more regular ovulation, which means more normal menstrual cycles.
The insulin-androgen-estrogen triangle
In PCOS, high insulin levels stimulate the ovarian theca cells to produce excess testosterone. This testosterone converts to a potent form of estrogen called estrone (E1) in fat tissue, but the problem is that estrone without adequate progesterone (from regular ovulation) creates an "unopposed estrogen" state. This state increases the risk of endometrial hyperplasia and other complications.
When semaglutide improves insulin sensitivity and promotes weight loss, the entire triangle shifts. Insulin drops. Androgen production drops. Aromatization in fat tissue drops. And, critically, ovulation resumes in many women, providing the progesterone needed to properly balance estrogen.
Studies show that semaglutide-treated PCOS patients experience improved ovulatory cycles, reduced waist circumference, lower BMI, decreased serum triglycerides, and reduced total testosterone. For women with PCOS who have been struggling with weight loss resistance, this can feel like a breakthrough.
Fertility considerations
Here is something critical that not enough guides mention. Because semaglutide can restore ovulation in women with PCOS, it can increase fertility. If you are not planning pregnancy, this restored fertility means you need reliable contraception. There have been reports of unexpected pregnancies in women with PCOS who assumed they could not conceive, only to have semaglutide restore their ovulatory function.
Semaglutide is not approved for use during pregnancy and should be discontinued at least two months before a planned conception. If you have PCOS and are considering semaglutide, discuss family planning with your provider before starting.
Semaglutide and menopause: what postmenopausal women need to know
The postmenopausal body relies almost entirely on fat tissue for estrogen production. The ovaries have largely stopped producing estrogen, and adipose aromatase becomes the primary source. This makes the relationship between semaglutide-driven weight loss and estrogen levels particularly significant for postmenopausal women.
Significant weight loss in this population can measurably reduce already-low estrogen levels. The clinical implications include potential worsening of menopausal symptoms like hot flashes, vaginal dryness, bone density loss, and mood changes. This is not a reason to avoid semaglutide, but it is a reason to monitor and potentially adjust hormone therapy.
The HRT-semaglutide combination advantage
Research published in the journal Menopause in 2024 examined postmenopausal women using semaglutide with and without hormone replacement therapy (HRT). The findings were striking. Women on HRT lost approximately 30% more total body weight at 3, 6, 9, and 12 months compared to those not on HRT. This suggests a synergistic relationship where estrogen replacement supports the metabolic environment that makes semaglutide more effective.
Why does this happen? Estrogen influences leptin sensitivity, appetite regulation, fat distribution, and energy expenditure. When postmenopausal women supplement estrogen through HRT, they restore some of these metabolic advantages, giving semaglutide a better foundation to work from.
Additional research has shown that combining GLP-1 activation with estrogen provides stronger protection against diabetes than using either approach alone. The combination activates both GLP-1 and estrogen receptors, reducing food intake and promoting weight loss through effects on brain areas involved in feeding and reward.
Bone density considerations
Estrogen is essential for maintaining bone density. Rapid weight loss, regardless of the method, can accelerate bone loss. When semaglutide-driven weight loss also reduces adipose-derived estrogen in postmenopausal women, the bone density concern becomes more pressing.
Postmenopausal women using semaglutide should discuss bone density monitoring with their healthcare provider. Weight-bearing exercise, adequate calcium and vitamin D intake, and potentially HRT can help mitigate this risk. The combination of semaglutide with HRT appears to address both the weight loss goal and the bone protection need simultaneously.
Semaglutide and testosterone: the other side of the hormone equation
You cannot fully understand the estrogen question without understanding testosterone. The two hormones are directly connected through aromatase, the enzyme that converts testosterone into estrogen. Changes in one inevitably affect the other.
Effects on men
In men with obesity, excess fat tissue means excess aromatase activity, which means too much testosterone gets converted to estrogen. This creates a state of relative estrogen dominance and relative testosterone deficiency, contributing to fatigue, reduced muscle mass, low libido, and metabolic dysfunction.
When semaglutide drives weight loss in men, fat tissue decreases, aromatase activity drops, and less testosterone gets converted to estrogen. The net effect is typically an increase in available testosterone and a decrease in excess estrogen. Multiple studies confirm that significant weight loss in obese men raises testosterone levels, sometimes dramatically.
For men concerned about semaglutide and hormones, the research is generally reassuring. Weight loss from semaglutide tends to improve the testosterone-to-estrogen ratio, not worsen it.
Effects on women
In women, the testosterone story depends heavily on the starting condition. In women with PCOS, semaglutide reduces excess testosterone, which is therapeutic. In women without PCOS who have normal testosterone levels, the changes are usually minimal and clinically insignificant.
The testosterone reduction in PCOS can have visible effects: reduced acne, reduced hirsutism (excess hair growth), improved skin quality, and better libido balance. These are generally positive changes, though individual responses vary.
How semaglutide affects hormonal birth control
This section addresses a practical concern that many women have. Semaglutide slows gastric emptying, the speed at which food and medications move through the digestive system. For oral hormonal contraceptives, this could theoretically affect absorption.
The evidence here is nuanced. Studies on oral contraceptive absorption with GLP-1 receptor agonists show small decreases in peak drug concentration but no clinically significant changes in overall bioavailability. The FDA labeling for semaglutide notes that it may affect the absorption of concomitant oral medications but does not specifically warn against oral contraceptive use.
However, the nausea and vomiting that some women experience during early semaglutide treatment can interfere with oral contraceptive absorption. If you vomit within a few hours of taking your birth control pill, the dose may not be fully absorbed.
Practical recommendations include considering non-oral contraceptive methods (IUD, implant, injection, patch, ring) if you experience significant GI side effects with semaglutide. If you prefer oral contraceptives, taking them at a different time of day than your semaglutide injection can help minimize any absorption concerns.
The insulin-hormone connection: why metabolic health matters for estrogen
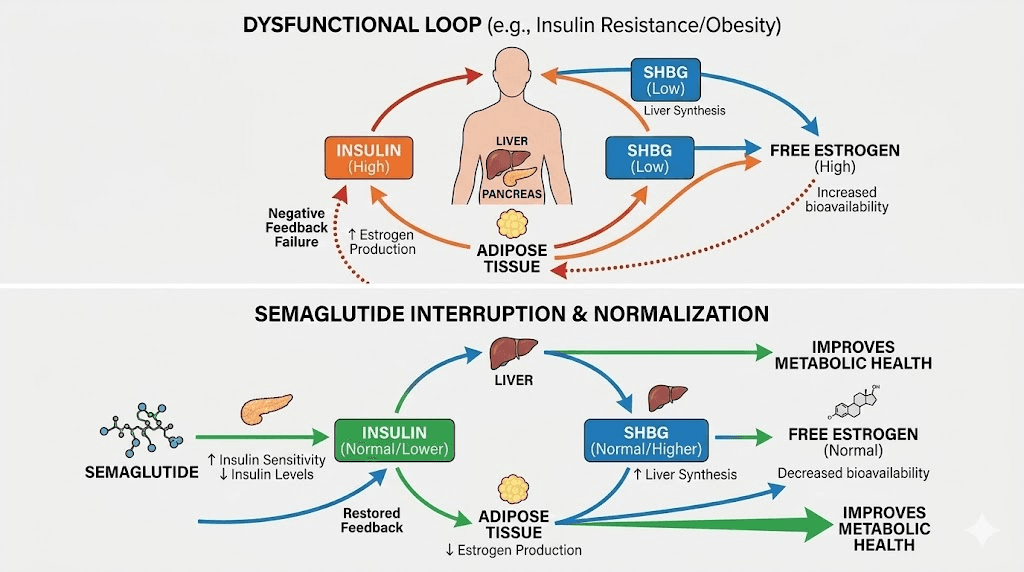
Insulin is the master regulator that nobody talks about in estrogen discussions. High insulin levels, a hallmark of metabolic syndrome and type 2 diabetes, directly stimulate estrogen production through multiple pathways. Insulin increases aromatase activity in fat tissue. It stimulates the ovaries to produce more androgens (which convert to estrogen). And it reduces sex hormone-binding globulin (SHBG), the protein that keeps sex hormones in check by binding them and making them inactive.
When SHBG drops, free (active) estrogen and testosterone levels rise, even if total production has not changed. This is why women with insulin resistance often show symptoms of both estrogen dominance (heavy periods, breast tenderness) and androgen excess (acne, hair growth) simultaneously.
Semaglutide addresses this at the root. By improving insulin sensitivity and reducing insulin levels, it allows SHBG to rise, which binds more free hormones, which brings the entire system closer to balance. This is not semaglutide directly changing estrogen. This is semaglutide fixing the metabolic dysfunction that was distorting estrogen levels in the first place.
The cortisol factor
Stress hormone cortisol also interacts with this system. Chronic stress elevates cortisol, which promotes fat storage (especially visceral fat), worsens insulin resistance, and disrupts the HPO axis. Some research suggests that the weight loss and metabolic improvement from semaglutide may indirectly lower cortisol levels, though this effect is not well-studied yet.
If cortisol drops, testosterone levels may improve naturally in men, and the overall hormonal environment becomes more favorable for balanced estrogen production in women. The entire system is interconnected, and semaglutide sits at a leverage point where metabolic improvement cascades into hormonal improvement.
Managing hormonal changes while taking semaglutide
Understanding the mechanisms is one thing. Knowing what to actually do about hormonal changes is another. Here are evidence-based strategies for managing the hormonal shifts that can accompany semaglutide use.
Monitor your baseline
Before starting semaglutide, get baseline bloodwork that includes estradiol (E2), total testosterone, free testosterone, SHBG, FSH, LH, DHEA-S, and a comprehensive metabolic panel including fasting insulin. This gives you a reference point for tracking changes. Without baseline numbers, you cannot know whether a symptom represents a new hormonal shift or a pre-existing imbalance that semaglutide is revealing.
Semaglutide does show up in certain blood tests, so make sure your provider knows you are taking it when interpreting results.
Nutrition strategies
Hormonal health requires adequate nutrition. When semaglutide suppresses appetite, it becomes easy to undereat critical nutrients. Focus on the following.
Healthy fats are essential for hormone production. Your body literally builds estrogen from cholesterol. Aim for adequate intake of olive oil, avocados, nuts, seeds, and fatty fish. Cutting fat too aggressively while on semaglutide can exacerbate hormonal disruption.
Protein is critical for maintaining muscle mass during weight loss, and muscle tissue influences metabolic rate and hormonal health. The semaglutide diet approach should prioritize 0.8-1g of protein per pound of lean body mass daily.
Cruciferous vegetables (broccoli, cauliflower, Brussels sprouts, kale) contain compounds like DIM and I3C that support healthy estrogen metabolism. These help the body process estrogen through favorable pathways, reducing the risk of estrogen dominance.
Fiber supports estrogen clearance through the digestive tract. Adequate fiber intake helps prevent reabsorption of estrogen that the body is trying to eliminate. Aim for 25-35g daily, which is achievable even with reduced appetite by choosing nutrient-dense foods.
Exercise for hormonal balance
Regular exercise has profound effects on hormonal balance during semaglutide use. Resistance training helps preserve muscle mass (which supports metabolic health and hormone production), while moderate cardiovascular exercise improves insulin sensitivity beyond what semaglutide achieves alone.
Avoid excessive high-intensity exercise, which can elevate cortisol and further disrupt the HPO axis, especially during the rapid weight loss phase. A balanced approach of 3-4 resistance training sessions and 2-3 moderate cardio sessions per week supports optimal hormonal health.
For those who struggle with exercise motivation or energy on semaglutide, even moderate walking provides meaningful hormonal benefits. The goal is consistency, not intensity. More about weight loss on semaglutide without exercise is available, though adding movement always improves outcomes.
Supplement considerations
Certain supplements may support hormonal balance during semaglutide use, though none replace proper medical care.
Vitamin D is essential for both estrogen metabolism and insulin sensitivity. Many people with obesity are vitamin D deficient, and weight loss can initially release stored vitamin D from fat tissue before levels drop as fat stores decrease. Test your levels and supplement accordingly.
Magnesium supports over 300 enzymatic reactions, including those involved in hormone production and insulin signaling. Glycinate or threonate forms are generally best tolerated, especially given the GI effects of semaglutide.
Omega-3 fatty acids support anti-inflammatory pathways that influence hormonal balance. They also support brain health and mood stability, which can be affected during hormonal transitions.
Probiotics support the estrobolome, the collection of gut bacteria that metabolize estrogen. A healthy estrobolome ensures proper estrogen clearance and recycling. Disrupted gut flora can lead to estrogen recirculation and relative dominance.
Semaglutide with hormone replacement therapy
The combination of semaglutide and HRT deserves special attention because the research shows genuine synergy. For postmenopausal women, this combination addresses two critical issues simultaneously: the metabolic dysfunction that drives weight gain after menopause and the hormonal deficiency that accelerates aging, bone loss, and cardiovascular risk.
Why the combination works
Estrogen replacement restores leptin sensitivity in the brain. Leptin is the satiety hormone that tells your brain you have enough energy stored. After menopause, declining estrogen impairs leptin signaling, making the brain think the body needs more fat reserves. This is one reason menopausal weight gain is so stubborn.
When HRT restores estrogen signaling and semaglutide adds powerful appetite suppression through GLP-1 pathways, the brain receives concordant signals from two different systems: you have enough energy, you do not need to store more. This dual signal appears to explain the enhanced weight loss seen in the research.
For women already on HRT considering adding compounded semaglutide, the existing evidence supports this combination. For women on semaglutide experiencing worsening menopausal symptoms, discussing HRT with a menopause-informed provider may address symptoms while also improving semaglutide effectiveness.
Practical protocol considerations
If using both semaglutide and HRT, timing matters. Semaglutide injection timing does not directly interact with transdermal HRT (patches, creams), but oral HRT may have absorption affected by the delayed gastric emptying that semaglutide causes. Discuss this with your prescriber if you use oral estrogen preparations.
Monitor symptoms regularly. Keep a simple log of hot flashes, sleep quality, mood, and cycle changes (if applicable). This data helps your provider adjust both medications optimally. Many women find that as they lose weight on semaglutide, their HRT dose may need adjustment since the fat tissue that was producing supplemental estrogen has decreased.
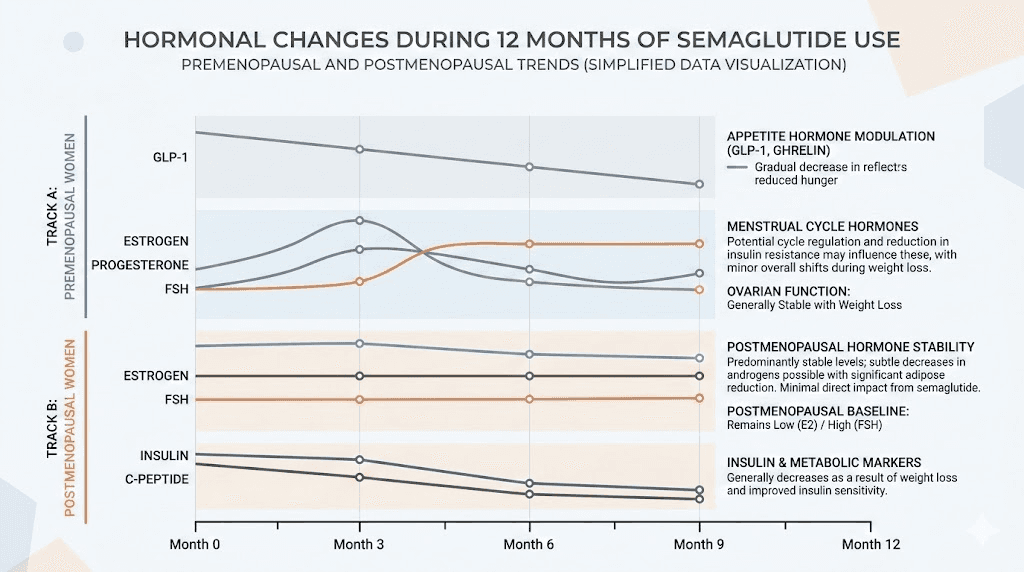
Timeline: when to expect hormonal changes on semaglutide
The hormonal effects of semaglutide follow a predictable pattern for most people, though individual variation is significant.
Weeks 1-4: initial adjustment
During the first week on semaglutide and the initial dose titration period, hormonal changes are minimal. The body is adjusting to the medication itself, and most people are on a low starting dose. GI side effects like nausea may dominate the experience. Weight loss is just beginning, so fat-mediated estrogen changes have not kicked in yet.
Some women may notice mild cycle changes even this early, likely related to the stress response of starting a new medication rather than actual hormonal shifts. Cortisol elevation from the novelty and anticipation can affect the cycle independently of any estrogen change.
Months 1-3: the transition zone
This is where hormonal changes become noticeable for many people. Weight loss is typically accelerating, appetite is significantly reduced, and the body is losing meaningful amounts of fat tissue. As fat decreases, adipose-derived estrogen production drops proportionally.
Women may notice cycle changes during this period. Some experience lighter periods. Others may skip a period entirely. A few report heavier bleeding as the body adjusts. These changes correlate with the rate of weight loss, faster loss generally means more hormonal disruption.
Insulin sensitivity is improving rapidly during this phase, which shifts the entire hormonal cascade described earlier. SHBG levels begin rising. Free hormone levels begin normalizing. Women with PCOS may notice their first regular cycle in months or years.
Months 3-6: recalibration
By this point, the body has had time to adapt to the new metabolic state. Hormonal disruption typically begins to stabilize. Cycles become more predictable. The initial chaos resolves into a new normal that often represents a healthier hormonal profile than before semaglutide.
Weight loss is still ongoing for most people, but the rate has usually moderated from the initial rapid phase. This slower pace of change gives the endocrine system more time to adjust. Week-by-week results show that the body finds its rhythm during this period.
Months 6-12: new equilibrium
Most hormonal changes have stabilized by this point. The body has established a new baseline for estrogen production based on the reduced fat mass. Cycles are typically regular (or the new pattern has become predictable). SHBG levels have normalized. The insulin-hormone axis is functioning more efficiently.
Some people reach a weight loss plateau during this phase. If weight stabilizes, hormonal levels also stabilize, since the driver of change (fat loss) has slowed. This is generally a good thing for hormonal balance, even if it feels frustrating from a weight loss perspective.
Beyond 12 months: maintenance phase
For those who continue long-term semaglutide use, hormonal levels should be stable and reflective of the new body composition. Regular monitoring (annually or as directed by your provider) ensures that estrogen, testosterone, and other hormones remain in healthy ranges.
If semaglutide is discontinued, withdrawal effects can include weight regain. If significant fat is regained, adipose-derived estrogen production increases again, potentially reversing the hormonal improvements achieved during treatment.
Signs that hormonal changes need medical attention
While most hormonal changes from semaglutide are benign and self-limiting, certain symptoms warrant medical evaluation.
See your provider promptly if you experience:
Absence of menstruation for three or more consecutive cycles (amenorrhea) without explanation
Extremely heavy bleeding that soaks through a pad or tampon every hour for several hours
Severe mood changes, depression, or anxiety that interfere with daily functioning
New or worsening hot flashes in premenopausal women
Significant hair loss beyond the normal shedding that can accompany rapid weight loss (see GLP-1 and hair loss)
Breast changes including lumps, persistent tenderness, or discharge
Vaginal dryness or pain that affects quality of life
Bone pain or fractures, especially in postmenopausal women
These symptoms do not necessarily mean semaglutide is the cause, but they warrant investigation. Hormonal bloodwork can identify whether estrogen levels have dropped below healthy ranges and whether intervention is needed.
How semaglutide compares to tirzepatide for hormonal effects
Since many people consider switching between semaglutide and tirzepatide, it is worth noting that the hormonal effects are broadly similar. Both medications cause weight loss through GLP-1 receptor agonism, both improve insulin sensitivity, and both reduce adipose-derived estrogen through the same fat-loss mechanism.
Tirzepatide additionally activates GIP receptors, which may provide slightly different metabolic effects, but the impact on estrogen through fat loss follows the same pathway. The side effect profiles differ somewhat, and tirzepatide may produce faster weight loss in some people, which could mean more rapid hormonal changes.
If you are considering switching, be aware that the transition itself can temporarily destabilize the hormonal equilibrium you have achieved on your current medication. Give the new medication 2-3 months before assessing its hormonal impact.
The thyroid connection
No discussion of semaglutide and hormones is complete without mentioning thyroid function. Semaglutide carries a black box warning about medullary thyroid carcinoma based on rodent studies (though this has not been observed in humans). Beyond this warning, weight loss itself affects thyroid function.
Rapid weight loss can temporarily reduce thyroid hormone levels (T3 and T4) as the body adapts to a lower metabolic rate. Since thyroid hormones interact with estrogen (hypothyroidism can increase estrogen levels by reducing SHBG), changes in thyroid function add another layer to the hormonal equation.
If you experience symptoms like unusual fatigue, cold intolerance, or constipation beyond what is expected from semaglutide, ask your provider to check thyroid function alongside hormonal panels. Conditions like Hashimoto thyroiditis interact with GLP-1 medications in ways that require careful monitoring.
Practical protocols for different populations
Protocol for premenopausal women
Goal: Maintain healthy estrogen balance while maximizing semaglutide benefits
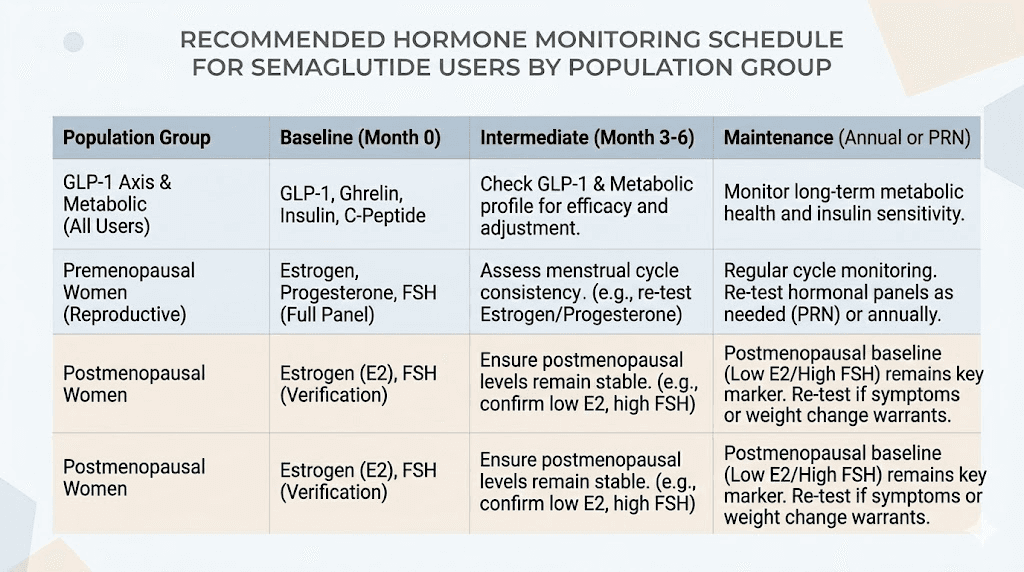
Monitoring schedule:
Baseline bloodwork before starting: estradiol, FSH, LH, testosterone, SHBG, fasting insulin, thyroid panel
Repeat at 3 months and 6 months, then annually
Track menstrual cycle (length, flow, symptoms) monthly
Nutritional targets:
Minimum 1,200-1,400 calories daily (undereating disrupts hormones)
30%+ calories from healthy fats
0.8-1g protein per pound of lean body mass
25-35g fiber daily
2-3 servings cruciferous vegetables weekly
Red flags requiring immediate evaluation: Three or more missed periods, sudden heavy bleeding, severe mood changes.
Use the semaglutide dosage calculator to ensure your dose is appropriate for your weight, and discuss any cycle changes with your prescriber during dose titration.
Protocol for postmenopausal women
Goal: Optimize weight loss while protecting bone density and managing menopausal symptoms
Monitoring schedule:
Baseline: estradiol, FSH, testosterone, SHBG, fasting insulin, thyroid panel, DEXA scan for bone density, vitamin D
Repeat hormones at 3 and 6 months
Repeat DEXA at 12 months or sooner if symptoms suggest bone loss
Special considerations:
Discuss HRT with provider, especially if menopausal symptoms worsen (research supports the combination)
Prioritize resistance training for bone and muscle preservation
Calcium: 1,000-1,200mg daily from food and supplements
Vitamin D: target 40-60 ng/mL blood levels
Consider bioidentical estrogen options if synthetic HRT is not tolerated
Red flags: New or worsening hot flashes, bone pain, mood depression, vaginal atrophy symptoms.
Protocol for women with PCOS
Goal: Reduce androgen excess, restore ovulatory cycles, improve insulin sensitivity
Monitoring schedule:
Baseline: estradiol, testosterone (total and free), DHEA-S, SHBG, fasting insulin, fasting glucose, HbA1c, AMH, thyroid panel
Repeat at 3 months (expect to see testosterone dropping and SHBG rising)
Repeat at 6 months and then every 6 months
Special considerations:
Use reliable contraception, as semaglutide may restore ovulation unexpectedly
Discontinue semaglutide at least 2 months before planned conception
Monitor for signs of improving PCOS: more regular cycles, reduced acne, reduced hirsutism
Consider combining with metformin if insulin resistance is severe (discuss with provider)
Some patients benefit from combining with berberine for additional insulin sensitization (research this carefully)
Red flags: Unexpected pregnancy symptoms, severe androgenic symptoms worsening, dramatic cycle changes after initial stabilization.
Protocol for men
Goal: Improve testosterone-to-estrogen ratio through fat loss
Monitoring schedule:
Baseline: total testosterone, free testosterone, estradiol, SHBG, fasting insulin, thyroid panel, PSA
Repeat at 3 months (expect rising testosterone, falling estrogen if significant fat loss occurring)
Repeat at 6 months and annually
Special considerations:
If on testosterone replacement therapy (TRT), discuss with provider as weight loss may allow dose reduction
Resistance training is especially important for maintaining muscle mass and supporting natural testosterone production
Adequate sleep (7-9 hours) supports testosterone production
Zinc and magnesium support testosterone synthesis
Red flags: Worsening libido, erectile dysfunction, gynecomastia (breast tissue development), persistent fatigue despite improving other metrics.
Common myths about semaglutide and estrogen
Misinformation about semaglutide and hormones is rampant online. Here are the most common myths and the reality behind them.
Myth: semaglutide directly increases estrogen
Reality: Semaglutide has no direct mechanism for increasing estrogen. It does not bind to estrogen receptors, does not stimulate the ovaries, and does not increase aromatase activity. Any estrogen changes are indirect, occurring through weight loss, insulin sensitivity changes, and metabolic improvement.
Myth: semaglutide causes estrogen dominance
Reality: The opposite is more likely. By reducing fat tissue and improving insulin sensitivity, semaglutide typically reduces excess estrogen in people who had elevated levels due to obesity. The hormonal shift moves toward balance, not toward dominance.
Myth: men should avoid semaglutide because it increases estrogen
Reality: In obese men, semaglutide-driven weight loss typically decreases estrogen and increases testosterone. The fat loss reduces aromatase activity, meaning less testosterone gets converted to estrogen. For most obese men, semaglutide improves the hormonal profile.
Myth: semaglutide makes menopause symptoms worse
Reality: It depends on context. Rapid weight loss can reduce adipose-derived estrogen, which may worsen some menopausal symptoms. But this can be managed with HRT, and the overall metabolic improvements from weight loss often outweigh the temporary hormonal disruption. The research showing better weight loss with the semaglutide-HRT combination suggests the two work well together.
Myth: you need to stop semaglutide if your hormones change
Reality: Hormonal changes are expected and usually temporary. Most women see their cycles stabilize within 3-6 months. Stopping semaglutide abruptly can cause its own set of problems, including rapid weight regain. Work with your provider to manage hormonal changes while continuing treatment, rather than stopping at the first sign of change.
The role of GLP-1 receptors in reproductive health
Emerging research is revealing that GLP-1 receptors exist not only in the brain, pancreas, and gut, but also in reproductive tissues including the ovaries, uterus, and testes. This discovery opens new questions about how GLP-1 receptor agonists like semaglutide might influence reproductive health beyond the indirect mechanisms already discussed.
In ovarian tissue, GLP-1 receptor activation appears to influence follicular development and steroid hormone production. Animal studies suggest that GLP-1 signaling plays a role in oocyte maturation and ovulation. While the clinical significance of these findings for human semaglutide users is not yet clear, it suggests that the relationship between GLP-1 medications and reproductive hormones may be more direct than previously thought.
In testicular tissue, GLP-1 receptors have been found in Leydig cells, which are responsible for testosterone production. This could partially explain why some men experience hormonal changes beyond what would be expected from weight loss alone. More research is needed to understand the magnitude and clinical relevance of these direct effects.
This is an evolving field. The indirect mechanisms (fat loss, insulin sensitivity, metabolic improvement) remain the primary drivers of hormonal change with semaglutide. But the direct pathways through reproductive tissue GLP-1 receptors may contribute, and future research will likely clarify their significance.
For the latest evidence-based protocols and guidance on navigating these complexities, SeekPeptides provides comprehensive resources that stay current with the research. Understanding the nuances of peptide-hormone interactions is exactly the kind of deep knowledge that separates effective protocols from guesswork.
Semaglutide dose and hormonal impact: does higher dose mean more change?
This is a question that comes up frequently. The relationship between semaglutide dose and hormonal impact is not directly proportional. Higher doses produce more appetite suppression and potentially more weight loss, which means more fat-mediated estrogen changes. But the dose itself does not independently drive hormonal changes.
During the dose titration process, starting low and increasing gradually allows the body more time to adapt both metabolically and hormonally. Rapid dose escalation that produces dramatic weight loss may create more hormonal disruption than a slower approach.
For those using split dosing, the hormonal impact should be similar to equivalent total weekly doses. The distribution of the dose does not change the overall metabolic and weight loss effect significantly enough to alter hormonal outcomes.
If you experience problematic hormonal symptoms, discuss with your provider whether a slower titration or temporary dose reduction might help while still maintaining therapeutic benefit. There is often a sweet spot where weight loss continues at a pace the body can adapt to hormonally.
Dietary phytoestrogens and semaglutide: do they interact?
Some people worry about dietary estrogen sources while taking semaglutide. Phytoestrogens, found in soy, flaxseed, legumes, and certain other foods, are plant compounds that weakly bind to estrogen receptors.
There is no evidence that phytoestrogens interact negatively with semaglutide. In fact, moderate phytoestrogen intake from whole food sources may support healthy estrogen metabolism. Soy foods, for example, contain isoflavones that can have mild estrogenic or anti-estrogenic effects depending on the body existing estrogen levels, acting more like modulators than pure estrogen boosters.
For people eating a healthy diet on semaglutide, including phytoestrogen-rich foods as part of a balanced approach is generally fine. Whole soy foods (tofu, tempeh, edamame) provide excellent protein, which is critical during semaglutide-driven weight loss. Flaxseed provides fiber and omega-3s. There is no need to avoid these foods specifically because of estrogen concerns.
The foods that actually disrupt hormonal balance are processed foods, excessive sugar, and alcohol. Avoiding these on semaglutide supports both weight loss and hormonal health far more than worrying about phytoestrogens.
Long-term hormonal outlook for semaglutide users
The long-term data on semaglutide and hormonal health is reassuring but incomplete. Studies extending 2-4 years show sustained metabolic improvements, continued weight maintenance (in those who remain on the medication), and stable hormonal profiles after the initial adjustment period.
What happens when people discontinue semaglutide? Restarting semaglutide after a break is common, and weight regain after discontinuation is well-documented. As weight returns, so does adipose-derived estrogen production, essentially reversing the hormonal changes that occurred during treatment. This is neither inherently good nor bad, it is simply the body responding to changes in fat mass.
For those who maintain their weight loss (whether through continued medication or lifestyle changes), the improved hormonal profile tends to persist. Lower insulin, higher SHBG, balanced estrogen, and improved testosterone ratios become the new normal as long as the metabolic improvements are maintained.
SeekPeptides members access comprehensive protocol guides that address long-term optimization, including hormonal monitoring schedules and adjustment strategies for sustained use. Navigating the long game requires more than a single article. It requires ongoing guidance adapted to changing circumstances.
Frequently asked questions
Does semaglutide directly increase estrogen levels?
No. Semaglutide does not directly interact with estrogen production or estrogen receptors. Any changes in estrogen levels are indirect, resulting from weight loss reducing fat tissue (which produces estrogen), improved insulin sensitivity affecting SHBG levels, and metabolic changes that cascade into the hormonal system.
Can semaglutide cause low estrogen?
Semaglutide-driven weight loss can reduce adipose-derived estrogen production. In premenopausal women with functioning ovaries, this reduction is usually minor. In postmenopausal women who rely on fat tissue for estrogen, significant weight loss can meaningfully lower estrogen levels. Monitoring and potentially combining with HRT can address this.
Will semaglutide affect my period?
Many women experience temporary menstrual changes during the first 3-6 months of semaglutide use. These can include lighter or heavier periods, shorter or longer cycles, or temporary irregularity. Most changes resolve as the body adapts to the new metabolic state.
Is semaglutide safe to take with hormone replacement therapy?
Research suggests the combination is not only safe but potentially synergistic. Postmenopausal women on HRT showed approximately 30% greater weight loss with semaglutide compared to those not on HRT. Always discuss the combination with your healthcare provider for personalized guidance.
Does semaglutide affect testosterone in men?
In obese men, semaglutide-driven weight loss typically improves testosterone levels by reducing fat tissue that converts testosterone to estrogen through aromatase. The result is usually higher testosterone and lower estrogen, an improved hormonal profile.
Can semaglutide help with PCOS symptoms?
Yes. Research shows that GLP-1 receptor agonists reduce testosterone levels by approximately 33% in women with PCOS, improve ovulatory cycles, reduce insulin resistance, and decrease androgen-related symptoms like acne and hirsutism. Semaglutide is increasingly used off-label for PCOS management.
Should I get hormone bloodwork before starting semaglutide?
Yes. Baseline bloodwork including estradiol, testosterone, SHBG, fasting insulin, and thyroid function provides a reference point for tracking any changes. Without baseline numbers, it is impossible to determine whether symptoms represent a new change or a pre-existing condition. Semaglutide can affect certain blood test results, so inform your provider about your use.
How long do hormonal side effects of semaglutide last?
Most hormonal disruption from semaglutide stabilizes within 3-6 months. The initial transition period, when weight loss is most rapid, produces the most noticeable changes. As the body adapts to its new metabolic state and weight loss pace moderates, hormonal levels typically find a new, often healthier, equilibrium.
Does semaglutide affect fertility?
Semaglutide can restore ovulatory function in women with PCOS, potentially increasing fertility. It is not approved for use during pregnancy and should be discontinued at least 2 months before planned conception. If you are not planning pregnancy and have PCOS, use reliable contraception while on semaglutide, as restored ovulation can lead to unexpected pregnancy.
Can semaglutide cause hormonal weight gain?
No. Semaglutide consistently produces weight loss, not weight gain. However, if hormonal changes (like reduced estrogen in postmenopausal women) cause symptoms that reduce activity levels or affect mood, this could indirectly slow weight loss progress. Addressing the hormonal component through HRT or lifestyle adjustments typically resolves this.
External resources
Semaglutide treatment of excessive body weight in obese PCOS patients (NIH/PMC)
Effects of GLP1RAs on pregnancy rate and menstrual cyclicity in women with PCOS (NIH/PMC)
Managing menopausal weight gain: the role estrogen plays with GLP-1 agonists (PCCA)
For researchers serious about understanding how their peptide protocols interact with hormonal health, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your hormones stay balanced, your protocols stay informed, and your progress stay consistent.