Mar 10, 2026

Everything you have read about semaglutide and feeling cold is probably half right. The forums say it is a side effect. The prescribing information does not mention it. And the actual reason you are reaching for a sweater three weeks into treatment has almost nothing to do with the medication itself.
Here is what is really happening. Semaglutide changes how your body feels in dozens of ways, but the cold sensation is not one of them. Not directly. The chill you feel comes from what the medication causes your body to do: eat less, burn fat, shift metabolic priorities. Those changes rewire your internal thermostat. And the science behind it is more fascinating than any Reddit thread gives it credit for. Your body ran a particular temperature for years. It had insulation. It had fuel. It had a metabolic rate calibrated to a specific weight. Now all of that is changing, sometimes faster than your hypothalamus can keep up with. This guide covers exactly why semaglutide treatment makes so many people feel cold, the five mechanisms driving the sensation, when it typically starts and stops, how it compares to tirzepatide cold sensitivity, and twelve proven strategies to stay warm without compromising your weight loss progress. SeekPeptides members have reported this as one of the most common surprises during treatment, and understanding the mechanisms makes it far easier to manage.
Why semaglutide makes you feel cold
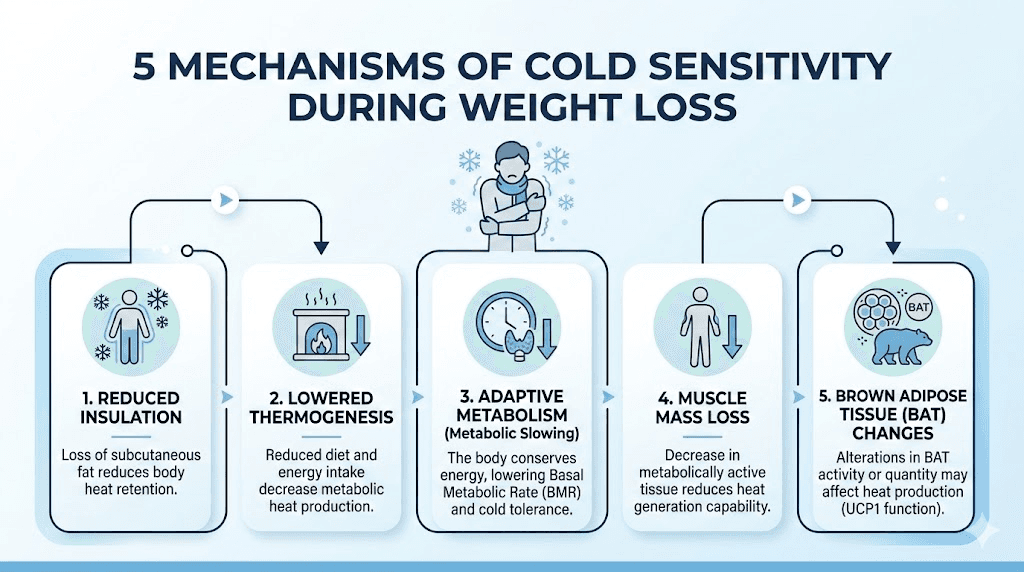
The cold sensation is real. Nobody is imagining it. But the path from semaglutide injection to shivering on the couch involves multiple physiological detours that most articles oversimplify. Five distinct mechanisms work together, and understanding each one separately is the key to managing all of them effectively.
Your body is losing its natural insulation
Fat is not just stored energy. It is a blanket. Subcutaneous fat, the layer sitting directly beneath your skin, acts as thermal insulation that prevents heat from escaping your body. When semaglutide starts working and you begin losing weight, that insulation thins out. The effect is measurable. Patients in the STEP clinical trials who lost 10 to 15 percent of their initial body weight reported significant changes in temperature perception. A person who weighed 220 pounds and drops to 190 has lost roughly 20 to 25 percent of their subcutaneous fat. That is a substantial reduction in insulation.
Think of it like removing a layer from a sleeping bag. The sleeping bag still works. You still produce heat. But more of that heat escapes into the environment instead of staying trapped against your skin. This is the most straightforward mechanism, and it is the one most people understand intuitively.
The effect is more pronounced in certain areas. Extremities like fingers and toes feel it first because they have less fat to begin with. People who carry most of their weight in their midsection may notice their torso feels colder sooner than expected. And the rate of fat loss matters too. Rapid early weight loss produces a more dramatic temperature shift than gradual loss over months.
Dietary thermogenesis drops when you eat less
Every time you eat, your body generates heat. This process, called dietary-induced thermogenesis or the thermic effect of food, accounts for roughly 10 percent of your total daily energy expenditure. Protein generates the most heat, around 20 to 30 percent of its caloric value. Carbohydrates produce 5 to 10 percent. Fats produce only 0 to 3 percent.
Semaglutide suppresses appetite significantly. Most people eat 20 to 40 percent fewer calories without even trying. That is a massive reduction in heat generation from digestion alone. If you were eating 2,500 calories daily and now consume 1,500, you have eliminated roughly 100 calories worth of pure heat production. That might sound small. It is not. Over the course of a day, that deficit in heat generation creates a noticeable difference in how warm you feel, especially during the first weeks of treatment when the appetite change is most dramatic.
The timing matters too. If you used to eat three large meals and now eat two small ones, the periods between meals become longer. During those gaps, your body produces less heat from digestion, and you feel colder. Many semaglutide users report feeling coldest in the late afternoon or evening, exactly when the gap between their last meal and the next is longest.
This is why choosing the right foods on semaglutide matters for more than just nutrition. Higher protein meals generate more digestive heat. Warm soups and cooked meals feel warming not just because of their temperature, but because of the metabolic processes they trigger. A well-planned semaglutide diet can meaningfully offset the cold sensation through strategic food choices alone.
Adaptive thermogenesis slows your internal furnace
This is the mechanism most articles miss entirely. Adaptive thermogenesis is your body intentionally reducing heat production in response to weight loss. It is not a malfunction. It is a survival mechanism that evolved over millions of years to prevent starvation.
When your body detects a sustained caloric deficit, it does not just burn stored fat to make up the difference. It also reduces energy expenditure across the board. Resting metabolic rate drops. Non-exercise activity thermogenesis decreases. You fidget less. You move more efficiently. And critically, your body produces less heat as a byproduct of cellular metabolism.
Research published in the American Journal of Physiology demonstrated that adaptive thermogenesis can reduce energy expenditure by 100 to 300 calories per day beyond what weight loss alone would predict. This metabolic slowdown is your body conserving fuel, and reduced heat production is a direct consequence. People who are not losing weight on semaglutide or experiencing weight loss plateaus are often dealing with this exact mechanism.
The frustrating part is that adaptive thermogenesis can persist even after weight stabilizes. Your body essentially recalibrates to a lower metabolic set point, and convincing it to produce more heat again requires specific interventions that we will cover in the strategies section below.
Muscle loss reduces your metabolic heat engine
Muscle tissue is metabolically expensive. It burns calories at rest, generates heat constantly, and acts as your body internal furnace. When you lose weight on semaglutide, you do not lose only fat. Without adequate protein intake and resistance exercise, a significant portion of weight loss comes from lean muscle mass.
Studies on GLP-1 receptor agonist treatment show that lean mass can account for 25 to 40 percent of total weight loss in patients who do not exercise or prioritize protein. That is a massive reduction in your body heat-generating capacity. Every pound of muscle you lose reduces your resting metabolic rate by approximately 6 to 10 calories per day. Lose 10 pounds of muscle and you are generating 60 to 100 fewer calories of heat daily.
This is why losing weight on semaglutide without exercise often produces more severe cold sensitivity than combining the medication with a structured training program. The people who supplement their GLP-1 treatment with resistance training and adequate protein maintain more muscle mass, maintain higher metabolic rates, and report less cold sensitivity.
Brown adipose tissue and metabolic signaling changes
Brown adipose tissue, or BAT, is your body dedicated heating system. Unlike white fat, which stores energy, brown fat burns energy specifically to generate heat. A clinical trial at UCLA (NCT05419726) is currently investigating how semaglutide affects BAT activity in obese subjects. Preliminary research suggests that GLP-1 receptor agonists may enhance BAT metabolic activity and promote the browning of white adipose tissue.
The relationship is complex. On one hand, semaglutide may increase BAT activity, which should theoretically produce more heat. On the other hand, the overall caloric deficit and adaptive thermogenesis may override this effect. The net result for most patients is still feeling colder, because the insulation loss and metabolic slowdown outweigh any BAT activation. Research in mice published in Frontiers in Nutrition showed distinct effects of semaglutide and tirzepatide on metabolic and inflammatory gene expression in brown adipose tissue, suggesting that the GLP-1 pathway interacts with thermogenesis in ways researchers are still untangling.
Is feeling cold an official side effect of semaglutide?
No. Feeling cold is not listed as an adverse effect in the FDA-approved prescribing information for Ozempic, Wegovy, or Rybelsus. The official side effect profile focuses on gastrointestinal effects like constipation, bloating, nausea, diarrhea, and dizziness. Cold sensitivity does not appear in the STEP trial adverse event data at all.
But absence of evidence is not evidence of absence.
The reason cold sensitivity does not show up in clinical trial data is straightforward. It is not caused by semaglutide pharmacology. GLP-1 receptor activation does not directly impair your thermoregulation centers in the hypothalamus. There is no robust evidence that the drug itself changes how your brain regulates body temperature. What the drug does is create the conditions, weight loss, caloric restriction, body composition changes, that produce cold sensitivity as a downstream effect.
This is an important distinction. Semaglutide side effects that appear in prescribing information are direct pharmacological effects. Nausea happens because GLP-1 receptors in the gut and brainstem are activated. Fatigue on semaglutide has multiple potential mechanisms. But cold sensitivity is an indirect consequence of what the medication achieves, not what it does at the receptor level.
That said, the anecdotal evidence is overwhelming. Online communities, patient forums, and clinical observations consistently report cold sensitivity as one of the most common unexpected experiences during semaglutide treatment. Some healthcare providers have started proactively counseling patients about it. The fact that it is not in the prescribing label does not mean it is not real or not worth addressing.
Anyone starting semaglutide should understand that this is a common experience, not a sign that something is wrong with the medication or with them. It simply means the treatment is working, and the body is adjusting to significant changes in composition and metabolism. Knowing how semaglutide makes you feel overall helps set realistic expectations for the journey.
When cold sensitivity starts and how long it lasts
Timing varies. But patterns exist.
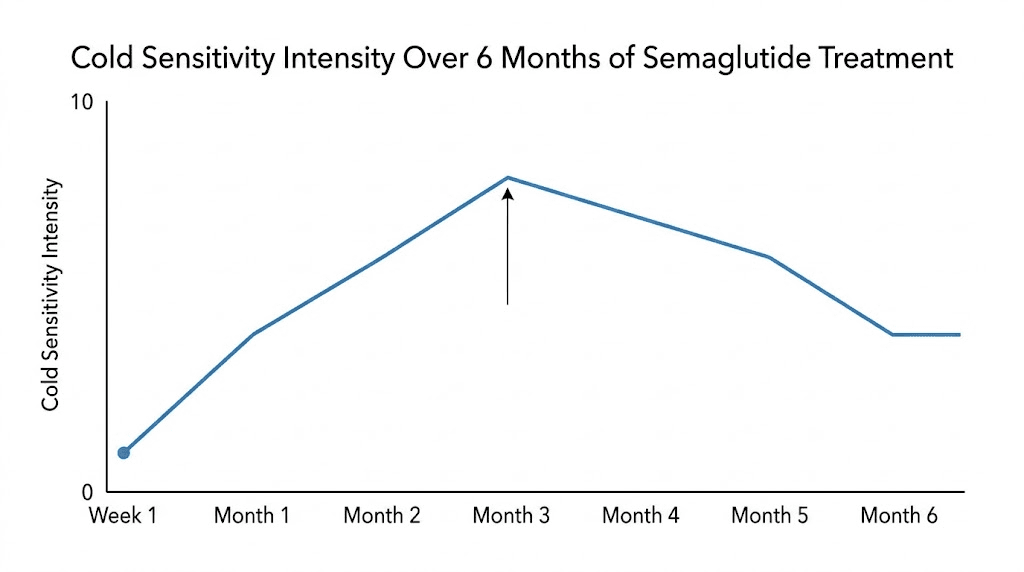
Most people begin noticing cold sensitivity within the first two to four weeks of treatment. This coincides with the initial appetite suppression phase, when caloric intake drops most dramatically. During the first week on semaglutide, the body is adjusting to GLP-1 receptor activation, and appetite changes are just beginning. By weeks two through four, the caloric deficit becomes substantial enough to affect heat production.
The dose escalation schedule plays a role. Semaglutide typically starts at 0.25 mg weekly and increases to 0.5 mg, then 1.0 mg, and potentially up to 2.4 mg for weight management. Each dose increase tends to suppress appetite further, creating a deeper caloric deficit. Many patients report that cold sensitivity worsens with each dose increase and then partially stabilizes before the next escalation. Understanding the semaglutide dosage schedule helps predict when these shifts may occur.
The peak of cold sensitivity typically occurs during months two through four. This is when the rate of weight loss is often fastest, the caloric deficit is deepest, and adaptive thermogenesis is actively ramping up. Patients who are losing weight rapidly during this window report the most intense cold sensitivity.
When does it get better?
Cold sensitivity generally improves in two phases. The first improvement comes when the body begins adapting to the new caloric intake, usually around months three to five. Even though weight loss continues, the body becomes somewhat accustomed to the reduced fuel supply and heat production partially recovers.
The second and more significant improvement comes when weight stabilizes. Once you reach a maintenance phase and the caloric deficit narrows, dietary thermogenesis increases, and adaptive thermogenesis begins to reverse. Most patients report meaningful improvement within several months of reaching a stable weight. However, some degree of increased cold sensitivity may persist long term, particularly in people who achieve substantial weight loss of 15 percent or more of initial body weight.
People restarting semaglutide after a break often experience the cold sensitivity cycle again, though typically less intensely than the first time. The body has some metabolic memory of the previous adaptation.
Cold sensitivity timeline by treatment phase
During weeks one through two, most people notice minimal cold sensitivity with initial appetite changes beginning. During weeks three through six, noticeable cold increases as caloric deficit deepens and appetite suppression strengthens. Months two through four represent the peak cold sensitivity period with the fastest weight loss and active adaptive thermogenesis. Months four through six bring partial adaptation where the body adjusts to new intake levels. And beyond month six, gradual improvement continues, especially as weight stabilizes and results become consistent.
The thyroid connection most people miss
When you feel cold constantly, thyroid function is the first thing to investigate. Not because semaglutide damages your thyroid, but because the metabolic changes during weight loss can unmask or exacerbate thyroid issues that were previously compensated.
Thyroid hormones, specifically T3 and T4, are central regulators of body temperature. T3 directly influences metabolic rate and heat production. When caloric intake drops significantly, the body reduces conversion of T4 to active T3 as an energy conservation strategy. This is not hypothyroidism in the clinical sense. It is a condition sometimes called low T3 syndrome or euthyroid sick syndrome, and it is a normal adaptive response to caloric restriction.
The practical effect is real though. Reduced T3 means reduced metabolic heat production. People who already had borderline thyroid function, subclinical hypothyroidism, or undiagnosed Hashimoto thyroiditis may find that semaglutide-induced weight loss pushes their temperature regulation past a threshold they were previously managing without symptoms.
This is why semaglutide and blood work monitoring matters. A complete thyroid panel, including TSH, free T3, free T4, and thyroid antibodies, should be part of baseline and follow-up labs for anyone on GLP-1 therapy. If cold sensitivity is severe, persistent, or accompanied by other symptoms like hair loss, extreme fatigue, or cognitive changes, thyroid testing becomes urgent rather than optional.
The relationship between thyroid hormones and brown adipose tissue adds another layer. BAT activation depends partly on thyroid hormone signaling. When T3 levels drop during caloric restriction, BAT becomes less efficient at generating heat. This creates a double penalty: less metabolic heat from reduced T3 and less thermogenic heat from impaired BAT function. People on semaglutide who also take thyroid medication should work with their provider to ensure dosing remains optimized as their weight and metabolism change.
How weight loss rewires your internal thermostat
Your hypothalamus regulates body temperature the same way a thermostat regulates a house. It has a set point, and it activates heating or cooling mechanisms to maintain it. But this thermostat is not fixed. It adapts to your body composition, your metabolic rate, and your energy availability.
When you lose significant weight, your hypothalamic set point does not immediately adjust downward. Instead, it continues trying to maintain the same temperature with fewer resources. Less insulation. Less metabolic heat. Less dietary thermogenesis. The result is that you feel cold even though your core body temperature has not actually dropped. Your body is working harder to maintain temperature, and the sensation of coldness reflects that increased effort.
The STEP trials demonstrated that patients losing 10 to 15 percent of initial body weight on semaglutide experienced significant metabolic adaptations. Before and after semaglutide results show dramatic physical changes, but the internal metabolic shifts are equally dramatic. Resting energy expenditure decreased beyond what would be predicted by the weight loss alone, consistent with adaptive thermogenesis.
Peripheral vasoconstriction is another factor. When heat production drops, your body prioritizes keeping vital organs warm by reducing blood flow to the extremities. This is why dizziness and cold hands and feet often appear together during rapid weight loss. The cardiovascular system is adapting to a smaller, lighter body with different thermal demands.
Understanding this rewriting process explains why cold sensitivity does not correlate perfectly with the amount of weight lost. Some people lose 30 pounds and feel fine. Others lose 15 pounds and are freezing. The difference often comes down to baseline metabolic rate, muscle mass, thyroid function, caloric intake, and individual variation in adaptive thermogenesis. People who maintain higher caloric intake through strategic meal planning while still losing weight tend to experience less severe cold sensitivity.
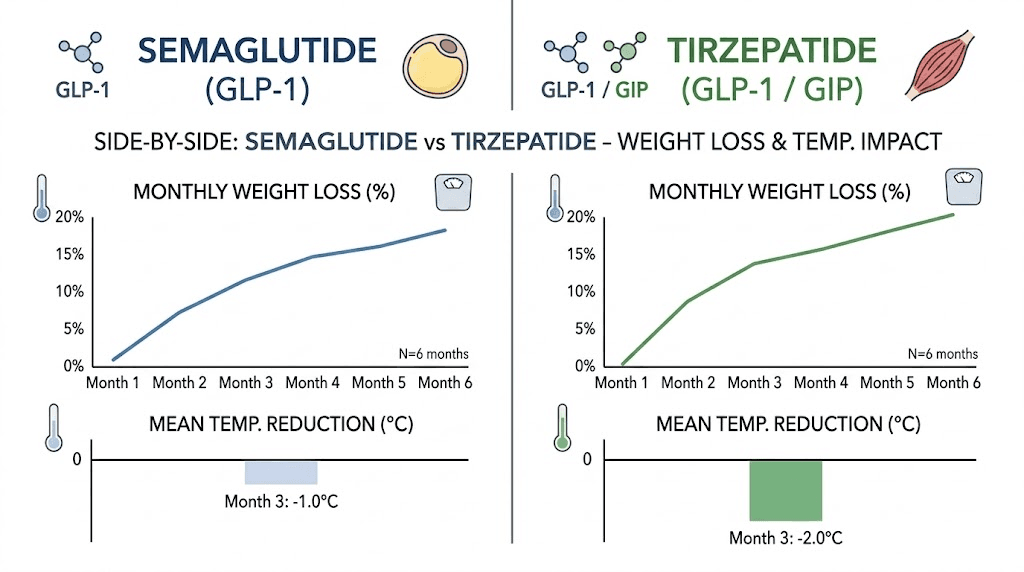
Semaglutide cold sensitivity compared to tirzepatide
Both GLP-1 receptor agonists cause weight loss. Both produce cold sensitivity. But there are meaningful differences.
Tirzepatide is a dual GIP/GLP-1 receptor agonist, meaning it activates two incretin pathways instead of one. The SURMOUNT trials showed that tirzepatide produces greater average weight loss than semaglutide at comparable treatment durations. More weight loss generally means more cold sensitivity, and tirzepatide cold sensitivity is reported at least as frequently as with semaglutide.
The GIP receptor activation adds a wrinkle. GIP receptors are present in adipose tissue, and GIP signaling may influence brown fat activity differently than GLP-1 alone. Some preliminary research suggests that the dual agonism could affect thermogenesis through pathways that semaglutide does not touch. Whether this increases or decreases cold sensitivity is still being investigated. A detailed comparison of semaglutide versus tirzepatide side effects shows that the overall side effect profiles share many similarities, with gastrointestinal effects being most common for both.
The rate of weight loss matters here too. Tirzepatide weight loss often occurs faster, particularly at higher doses. Faster weight loss produces more abrupt changes in insulation, dietary thermogenesis, and adaptive responses, which can make cold sensitivity feel more intense in the early months. People switching between the two medications sometimes notice differences in cold sensitivity that correlate with differences in appetite suppression intensity and weight loss rate.
Other side effects that overlap between the two medications include tiredness on tirzepatide, bloating, headaches, and constipation. The cold sensitivity mechanism is identical for both: it is a consequence of weight loss and metabolic adaptation, not a direct drug effect. Management strategies are the same regardless of which medication you are taking.
For those considering the broader landscape of weight loss peptides, comparing semaglutide, tirzepatide, and retatrutide provides a comprehensive look at how the newest options stack up. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, produces even greater weight loss in clinical trials and may produce correspondingly more intense cold sensitivity.
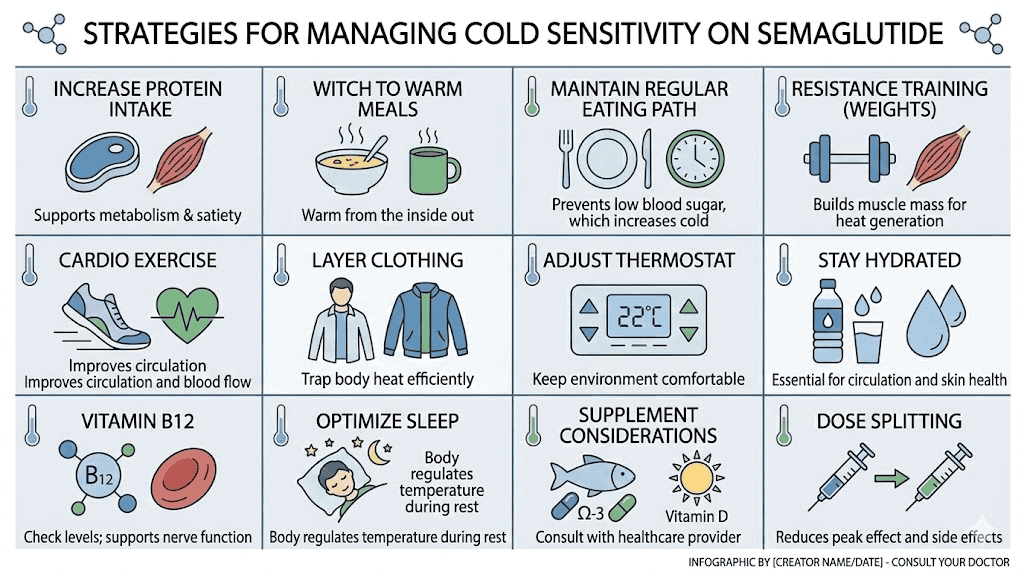
12 proven strategies to stop feeling cold on semaglutide
Cold sensitivity on semaglutide is manageable. The key is addressing multiple mechanisms simultaneously rather than relying on a single approach. These twelve strategies target the five root causes we covered above, and combining several of them produces the best results.
Strategy 1: Prioritize protein at every meal
Protein has the highest thermic effect of any macronutrient. Eating 30 to 40 grams of protein per meal generates measurably more heat than the same calories from carbohydrates or fat. The target for semaglutide users should be 1.0 to 1.5 grams of protein per kilogram of ideal body weight daily. For a person targeting 160 pounds, that is 73 to 109 grams of protein daily. Spreading this across three meals ensures consistent heat generation throughout the day. Protein-rich foods to eat on semaglutide include chicken, fish, eggs, Greek yogurt, and lean beef.
Strategy 2: Eat warm, cooked meals instead of cold food
This sounds obvious, but the science supports it beyond simple thermal transfer. Warm foods require less energy to bring to body temperature, and the spices commonly used in warm meals like ginger, cinnamon, cayenne, and turmeric have genuine thermogenic properties. A hot bowl of soup delivers heat directly while also triggering digestive thermogenesis. Planning your meals on semaglutide around warm, protein-rich options is one of the simplest ways to fight cold sensitivity.
Strategy 3: Do not skip meals
Extended fasting periods reduce dietary thermogenesis to zero. While intermittent fasting has benefits, combining it with semaglutide-induced appetite suppression can produce prolonged periods of very low heat generation. If cold sensitivity is a problem, eat smaller meals more frequently rather than one or two large meals. This keeps the metabolic furnace running throughout the day. Understanding the foods to avoid is important, but eating consistently matters just as much.
Strategy 4: Add resistance training two to three times per week
This is the single most impactful strategy for long-term cold management. Resistance training preserves and builds lean muscle mass, which increases your resting metabolic rate and heat production. Even moderate resistance training, two to three sessions of 30 to 45 minutes per week, can significantly offset the muscle loss that contributes to cold sensitivity. The heat generated during and after a resistance workout, through excess post-exercise oxygen consumption, keeps you warmer for hours. People exploring how to maintain weight loss results find that resistance training is essential for both temperature regulation and long-term metabolic health.
Strategy 5: Include 150 minutes of moderate aerobic activity weekly
Cardiovascular exercise increases blood flow, improves circulation to the extremities, and generates substantial heat during the activity itself. Walking, cycling, swimming, and other moderate-intensity activities for 150 minutes per week, about 30 minutes five days a week, improve the peripheral circulation that gets restricted during adaptive thermogenesis. The combination of resistance training and aerobic exercise addresses both the muscle loss and circulation components of cold sensitivity.
Strategy 6: Layer clothing strategically
Focus on core temperature first. A warm core sends more blood to the extremities. Thermal base layers made from merino wool or synthetic moisture-wicking fabrics work better than heavy outer layers. Keep extremities covered with warm socks and gloves indoors if needed. Many semaglutide users find that wearing a light thermal undershirt throughout the day, even at home, makes a significant difference without being cumbersome.
Strategy 7: Maintain indoor temperatures between 68 and 72 degrees Fahrenheit
This range provides enough ambient warmth to reduce the thermoregulatory burden on your body without being so warm that it interferes with sleep or comfort. If you previously kept your home at 65 degrees and felt fine, you may need to adjust upward by three to five degrees during active weight loss. Heated blankets for sleeping and a space heater for your workspace can provide targeted warmth where you spend the most time.
Strategy 8: Stay hydrated with warm beverages
Dehydration reduces blood volume, which impairs circulation and makes cold sensitivity worse. Semaglutide can reduce fluid intake along with food intake, since much of our daily water comes from food. Aim for at least 64 ounces of fluid daily, and prioritize warm options like herbal tea, warm water with lemon, and broth. Managing fluid intake on semaglutide supports both temperature regulation and overall treatment tolerance.
Strategy 9: Consider B12 and iron supplementation
Semaglutide can affect nutrient absorption, particularly vitamin B12. B12 deficiency causes its own cold sensitivity through impaired red blood cell production and peripheral neuropathy. Iron deficiency, which can worsen with reduced food intake, also contributes to feeling cold through reduced oxygen-carrying capacity. Semaglutide with B12 combinations exist for this reason. Some compounded formulations include methylcobalamin specifically to address this concern. Getting baseline blood work and monitoring levels ensures you catch deficiencies before they compound the cold sensitivity problem.
Strategy 10: Address sleep quality
Poor sleep impairs thermoregulation. Your body temperature naturally dips during sleep, and sleep deprivation disrupts the hormonal signals that regulate this cycle. Insomnia on semaglutide is reported by some users, and the combination of poor sleep and metabolic adaptation can make cold sensitivity significantly worse. Prioritize sleep hygiene: consistent bedtime, cool but not cold bedroom, warm blankets, and avoid stimulants in the evening. If injection timing affects your sleep, adjust accordingly.
Strategy 11: Use thermogenic supplements carefully
Certain supplements have mild thermogenic properties that can support heat production. Green tea extract, capsaicin from cayenne pepper, and ginger extract have research supporting their ability to slightly increase metabolic heat production. These are not dramatic interventions, but they contribute to the overall strategy. Glycine supplementation and L-carnitine with semaglutide are being explored for their metabolic benefits as well. Always discuss supplements with a healthcare provider to avoid interactions.
Strategy 12: Consider splitting your dose
Some patients find that splitting their semaglutide dose reduces the intensity of side effects, including cold sensitivity. Instead of one weekly injection, splitting into two smaller doses can smooth out the appetite suppression effect and prevent the dramatic caloric restriction swings that drive temperature changes. This approach should only be done under medical supervision, but it has helped some patients manage multiple side effects simultaneously.
Meal planning for warmth during semaglutide treatment
Food is your most accessible tool for managing cold sensitivity. The right meal plan addresses both the caloric deficit and the thermogenic shortfall simultaneously.
Thermogenic foods that generate internal heat
Certain foods increase metabolic heat production beyond their caloric content. Capsaicin in chili peppers activates thermogenic pathways through TRPV1 receptors. Ginger contains gingerols and shogaols that increase metabolic rate by 5 to 10 percent for several hours after consumption. Cinnamon improves insulin sensitivity and slightly raises metabolic rate. Black pepper contains piperine, which enhances both thermogenesis and nutrient absorption.
Incorporating these into daily meals is straightforward. Add ginger to morning tea. Use cayenne in lunch preparations. Season dinner with black pepper and cinnamon where appropriate. The effects are modest individually but cumulative over a full day of eating. A complete semaglutide diet plan should incorporate these thermogenic foods strategically.
Sample warming meal structure
Breakfast could include a warm protein bowl with eggs, sauteed vegetables, and a sprinkle of cayenne and turmeric. This delivers 25 to 35 grams of protein plus thermogenic spices plus warm temperature. Total thermic effect is significantly higher than a cold protein shake.
Lunch might feature a hearty bone broth soup with chicken, vegetables, and ginger. Bone broth provides collagen, electrolytes, and warmth. The protein from chicken drives dietary thermogenesis. The ginger adds a thermogenic bonus. This kind of meal keeps you warmer for two to three hours compared to a cold sandwich with the same calories.
Dinner could center around baked salmon with roasted vegetables and a side of warm quinoa seasoned with cinnamon and black pepper. Salmon provides protein and omega-3 fatty acids that support metabolic function. The roasted vegetables deliver warmth and micronutrients. The spiced quinoa adds complex carbohydrates that sustain energy for evening hours.
For those who need guidance on overall food choices while on treatment, detailed guides on what to eat during GLP-1 therapy and foods to avoid provide comprehensive frameworks. The GLP-1 breakfast ideas guide offers specific morning options designed to maximize both nutrition and satiety.
Protein targets for preserving muscle and heat
The protein target of 1.0 to 1.5 grams per kilogram of ideal body weight is not arbitrary. It is the range shown in research to minimize lean mass loss during caloric restriction. For a person with an ideal body weight of 70 kilograms (154 pounds), that means 70 to 105 grams of protein daily. Distribute this across at least three meals and one snack to maintain consistent dietary thermogenesis throughout the day.
Protein quality matters too. Complete proteins containing all essential amino acids, especially leucine, are most effective at preserving muscle mass and stimulating muscle protein synthesis. Animal sources like chicken, fish, eggs, and dairy provide complete amino acid profiles. Plant sources can work but require combining multiple sources to achieve completeness. Using a semaglutide dosage calculator helps ensure your medication dose is optimized, and applying the same precision to protein intake optimizes your body composition outcomes.
Exercise protocols that boost internal heat production
Exercise is heat generation. Every muscle contraction produces thermal energy. The right exercise program directly counteracts the cold sensitivity caused by semaglutide treatment.
Resistance training for metabolic heat
Compound exercises that engage multiple large muscle groups produce the most heat. Squats, deadlifts, bench press, rows, and overhead press recruit major muscle groups simultaneously, generating significant thermal output during the workout and for hours afterward through excess post-exercise oxygen consumption.
A simple but effective program for semaglutide users involves three sessions per week, each lasting 30 to 45 minutes. Focus on compound movements with moderate weight and 8 to 12 repetitions per set. This range is optimal for both muscle preservation and metabolic stimulation. Progressive overload, gradually increasing weight or volume over time, ensures continued muscle adaptation.
The post-exercise warmth effect is notable. After a resistance training session, metabolic rate can stay elevated for 24 to 48 hours. This extended metabolic boost translates directly to increased heat production during a period when semaglutide users most need it. People using their peptide calculator for dosing precision should apply similar discipline to their training progression.
Cardiovascular exercise for circulation
Moderate-intensity cardio improves blood flow to the extremities. Walking, cycling, swimming, or any activity that elevates heart rate to 60 to 70 percent of maximum for 30 minutes improves vasodilation and peripheral circulation. This directly addresses the vasoconstriction that makes hands and feet feel cold during weight loss.
Morning cardio may be particularly beneficial. Physical activity early in the day raises core body temperature and metabolic rate for several hours, providing a thermal boost during the period when many semaglutide users feel coldest. Even a 20-minute brisk walk after breakfast can meaningfully improve temperature comfort for the morning and early afternoon.
The counterintuitive case for mild cold exposure
Brief, controlled cold exposure, like ending a shower with 30 to 60 seconds of cold water, may actually help with long-term cold tolerance. Cold exposure activates brown adipose tissue and stimulates adaptive responses that improve thermogenesis over time. This is not about suffering through freezing temperatures. It is about gradually training your body to generate heat more efficiently.
Research on cold exposure and BAT activation shows that regular mild cold exposure can increase brown fat activity by 30 to 40 percent over several weeks. This enhanced BAT function improves baseline heat production and can partially offset the thermogenic deficit created by weight loss. However, this approach should be introduced gradually and is not appropriate for everyone. People who are already severely cold-sensitive should focus on the warming strategies first and consider cold exposure only after their baseline improves.
When feeling cold on semaglutide signals something more serious
Most cold sensitivity during semaglutide treatment is benign. It is uncomfortable but not dangerous. However, certain patterns and accompanying symptoms warrant medical evaluation because they may indicate underlying conditions that need treatment.
Red flags that require immediate attention
Severe fatigue combined with cold sensitivity may indicate hypothyroidism, anemia, or both. If you are not just cold but also exhausted, struggling to concentrate, and losing hair, get a thyroid panel and complete blood count immediately. These are not normal semaglutide side effects. Hair loss on GLP-1 therapy can have multiple causes, but combined with cold intolerance and fatigue, thyroid dysfunction becomes the primary suspect.
Numbness, tingling, or color changes in the extremities go beyond simple cold sensitivity. Blue or white fingertips or toes suggest Raynaud phenomenon or peripheral vascular issues that need evaluation. Nerve-related symptoms on semaglutide should always be reported to a healthcare provider. These symptoms may also indicate B12 deficiency, which can develop during prolonged GLP-1 therapy, especially at higher doses.
Chest pain, shortness of breath, or rapid heart rate combined with cold sensitivity suggest cardiovascular involvement and require urgent evaluation. While semaglutide has shown cardiovascular benefits in clinical trials, the rapid hemodynamic changes during significant weight loss can unmask pre-existing conditions. Vascular concerns on semaglutide should be taken seriously.
Conditions to investigate
Hypothyroidism is the most common medical cause of cold intolerance and should be ruled out early. As discussed, the relationship between weight loss and thyroid function is complex, and Hashimoto disease and GLP-1 therapy require careful monitoring. A complete thyroid panel, not just TSH, provides the full picture.
Iron deficiency anemia reduces the blood capacity to carry oxygen, which impairs both energy production and heat generation. Reduced food intake on semaglutide can decrease iron intake, particularly for people who eat less red meat. A ferritin level below 30 ng/mL warrants supplementation, even if hemoglobin is still in the normal range.
Vitamin B12 deficiency affects nerve function and red blood cell production. Symptoms include cold extremities, tingling, fatigue, and cognitive changes. B12 supplementation with semaglutide is increasingly recommended as a preventive measure. Compounded formulations that include B12 and glycine blends address this proactively.
Diabetes-related complications, including peripheral neuropathy and autonomic dysfunction, can cause cold extremities independent of semaglutide treatment. People using semaglutide for type 2 diabetes management should distinguish between medication-related cold sensitivity and diabetes complications that may need separate treatment.
When to contact your healthcare provider
Contact your provider if cold sensitivity is severe enough to interfere with daily activities, if it worsens rather than improves over time, if it is accompanied by any of the red flag symptoms listed above, or if it does not respond to the management strategies covered in this guide. Also contact your provider if you experience significant changes in menstrual patterns, unexplained weight gain despite continued medication use, or anxiety symptoms that could be related to metabolic changes.
In most cases, your provider will order blood work, adjust your dose, or provide targeted recommendations. Rarely is cold sensitivity a reason to discontinue semaglutide entirely. It is usually manageable with the strategies described above and resolves as the body adapts.
The psychological dimension of feeling cold on semaglutide
Cold sensitivity is a physical sensation, but it carries psychological weight that most guides ignore.
Feeling cold all the time affects mood. It disrupts sleep. It changes how you dress, where you sit, what activities you avoid. Some people report that constant cold sensitivity makes them question whether the medication is worth continuing. Others develop anxiety about going to air-conditioned environments or outdoor events. The psychological burden is real and valid.
Body image changes compound the issue. As weight drops, the body that used to feel warm and insulated now feels exposed and vulnerable. This is especially challenging for people who associated their previous body size with comfort and warmth. The cold becomes a physical reminder of change, and that change, even when desired, can feel unsettling.
Sleep disruption from cold sensitivity creates a cascade. Poor sleep increases cortisol, which can slow weight loss and increase anxiety. Increased anxiety makes cold sensitivity feel worse through heightened somatic awareness. Slower weight loss creates frustration, and the cycle continues. Breaking this pattern requires addressing the cold directly through the physical strategies above, while also acknowledging that adjustment takes time.
Support systems help. Connecting with others who share the experience normalizes it. SeekPeptides provides a community where members discuss these exact challenges, share solutions, and support each other through the adjustment period. Knowing that thousands of other people have felt the same thing and found it manageable makes a meaningful difference in persistence and treatment adherence.
Long-term outlook for cold sensitivity on semaglutide
The trajectory is encouraging. Cold sensitivity peaks during the most active weight loss phase and generally improves as the body reaches a new equilibrium. For most people, the worst of it lasts three to six months. The residual cold sensitivity that may persist long term is typically mild enough to manage with clothing choices and meal planning.
Maintenance strategies make the biggest difference. People who continue resistance training, maintain adequate protein intake, and prioritize weight maintenance protocols after reaching their goal weight report the best long-term temperature regulation. The muscle mass preserved or built during treatment continues generating heat indefinitely.
Metabolic adaptation does partially reverse. Research shows that resting metabolic rate recovers somewhat once weight stabilizes and caloric intake normalizes. The body eventually accepts its new set point and adjusts heat production accordingly. This process takes months to years, not weeks, but it does happen.
For people considering stopping semaglutide, cold sensitivity often improves quickly as appetite returns and caloric intake increases. However, if significant weight was lost and maintained, some degree of increased cold sensitivity relative to pre-treatment levels is expected. The insulation is not coming back unless the weight does.
The most important message is that cold sensitivity is a sign that the medication is working. Weight is being lost. Body composition is changing. Metabolism is adapting. These are all indicators of progress. Managing the cold is a practical challenge with practical solutions, not a reason to question the treatment itself.
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. Members access detailed dosing guides, compounded semaglutide information, and troubleshooting resources for every stage of treatment.
Frequently asked questions
Does semaglutide directly cause your body temperature to drop?
No. Semaglutide does not directly lower body temperature or impair thermoregulation at the receptor level. The cold sensation comes from indirect effects of weight loss, including reduced insulation from fat loss, decreased dietary thermogenesis from eating less, adaptive metabolic slowdown, and potential muscle mass loss. Your core body temperature typically remains normal. It is the perception of cold that changes as your body adapts to a new weight and metabolic state. Learn more about how semaglutide affects how you feel overall.
How long will I feel cold on semaglutide?
Most people experience the most intense cold sensitivity during months two through four of treatment, when weight loss is typically fastest. It generally begins improving around months four to six and continues to improve as weight stabilizes. Some residual cold sensitivity may persist long term, particularly for people who lose 15 percent or more of their initial body weight. Week-by-week semaglutide tracking helps identify your personal pattern.
Is feeling cold on semaglutide dangerous?
In most cases, no. Feeling cold is uncomfortable but not dangerous. However, it can signal underlying issues if accompanied by severe fatigue, hair loss, numbness or tingling in extremities, or cognitive changes. These symptoms warrant blood work to check thyroid function, B12 levels, and iron status. Fatigue on GLP-1 medications deserves investigation when it is persistent and severe.
Will taking a higher dose of semaglutide make cold sensitivity worse?
Potentially. Higher doses typically produce greater appetite suppression and faster weight loss, both of which contribute to cold sensitivity. The semaglutide dosage schedule escalates gradually for this reason, allowing the body time to adapt between increases. If cold sensitivity is severe at your current dose, discuss the escalation timeline with your provider before increasing.
Does the formulation of semaglutide affect cold sensitivity?
The cold sensitivity is driven by weight loss rather than the medication formulation. Whether you use branded Wegovy, branded Ozempic, compounded semaglutide, oral drops, or sublingual formulations, the cold sensitivity relates to the metabolic changes from weight loss. Compounded versions that include B12 or L-carnitine may provide minor benefits for energy and metabolism.
Can exercise really help with cold sensitivity on semaglutide?
Yes, significantly. Resistance training preserves muscle mass, which maintains metabolic heat production. Cardiovascular exercise improves peripheral circulation, which reduces cold extremities. The combination of both addresses two of the five mechanisms driving cold sensitivity. People who exercise regularly during GLP-1 therapy report meaningfully less cold sensitivity than those who do not.
Should I eat more to feel warmer on semaglutide?
Eating more can help with cold sensitivity by increasing dietary thermogenesis. However, this needs to be strategic rather than simply adding calories. Focus on increasing protein intake rather than total calories. Choose warm, thermogenic foods rather than calorie-dense but cold options. The goal is to optimize heat production per calorie consumed, not simply eat more. A structured diet plan for semaglutide balances warmth, nutrition, and continued weight loss.
Does feeling cold mean semaglutide is working?
Often, yes. Cold sensitivity correlates with active weight loss and metabolic adaptation. If you are feeling cold and also losing weight, the two are likely connected. However, feeling cold alone is not a reliable indicator of medication effectiveness. Some people lose weight without significant cold sensitivity, and some experience cold from other causes. Track your weight loss progress independently to assess medication effectiveness.
External resources
UCLA Clinical Trial: Brown Adipose Tissue Activity in Response to Semaglutide
Frontiers in Nutrition: Semaglutide and Tirzepatide Effects on Brown Adipose Tissue
The Role of Thyroid Hormone and Brown Adipose Tissue in Energy Homeostasis - PMC/NIH
Compensation for Cold-Induced Thermogenesis During Weight Loss - American Physiological Society
In case I do not see you, good afternoon, good evening, and good night. May your thermostat stay comfortable, your muscles stay warm, and your progress stay unstoppable.