Feb 27, 2026

The FDA reported dosing errors with compounded semaglutide that led to patients receiving five to ten times their intended dose. Five to ten times. That is not a rounding error. That is the difference between a therapeutic injection and a trip to the emergency room, and it happens because people confuse three simple numbers on their vial, their syringe, and their prescription.
You are staring at an insulin syringe right now, pulled back to the 25-unit mark, and you want to know one thing. How many milligrams is this? The answer is not a single number. It depends entirely on the concentration printed on your vial, and if you get that part wrong, every calculation that follows falls apart. A semaglutide units to mg conversion that works perfectly for one vial concentration will give you a completely wrong answer for another.
This guide breaks down exactly what 25 units of semaglutide equals in milligrams at every common concentration, walks through the math step by step, explains where 25 units falls in a standard dosing protocol, and covers the most dangerous mistakes people make with semaglutide dosage in units. Whether you are using a compounded semaglutide vial from a pharmacy or trying to understand how your prescribed dose translates to syringe markings, every answer you need is here.
SeekPeptides built this guide because dosing confusion is the single biggest safety issue in the GLP-1 space right now, and nobody should have to guess whether they are injecting the right amount.
The quick answer: what 25 units of semaglutide equals in milligrams
Here is the direct answer. But you need to know your vial concentration first.
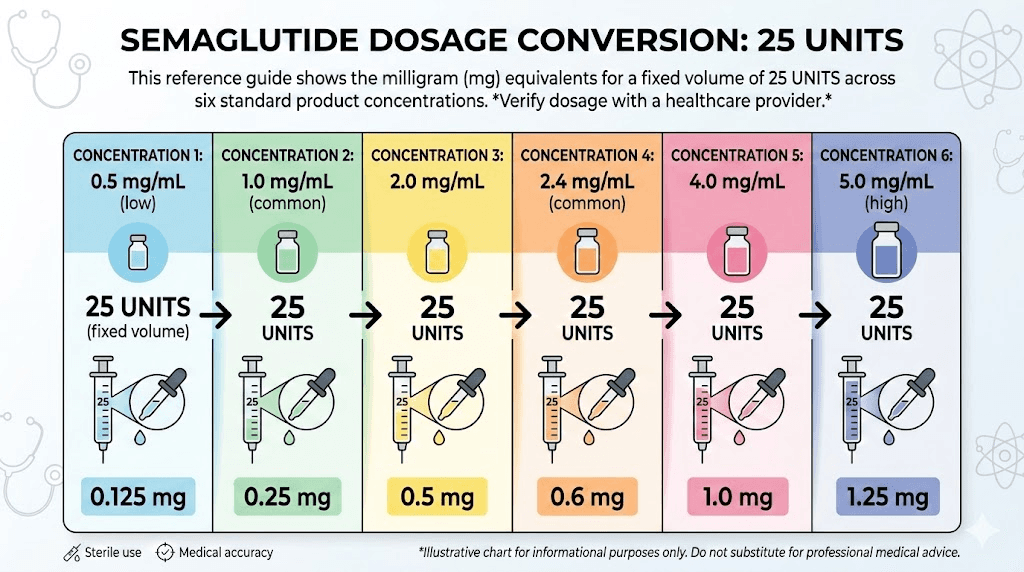
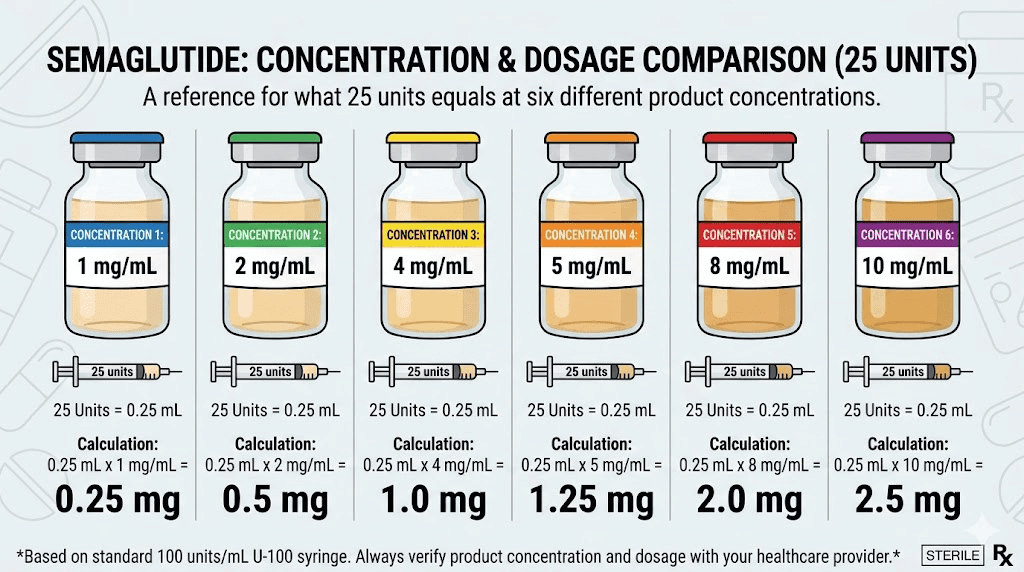
25 units on an insulin syringe always equals 0.25 mL of liquid. That part never changes. What changes is how many milligrams of semaglutide are dissolved in that 0.25 mL, and that depends entirely on the concentration written on your vial label.
Vial concentration | 25 units equals | Volume drawn |
|---|---|---|
1 mg/mL | 0.25 mg | 0.25 mL |
2 mg/mL | 0.50 mg | 0.25 mL |
2.5 mg/mL | 0.625 mg | 0.25 mL |
3 mg/mL | 0.75 mg | 0.25 mL |
5 mg/mL | 1.25 mg | 0.25 mL |
10 mg/mL | 2.50 mg | 0.25 mL |
Read that table carefully. At 1 mg/mL, 25 units delivers a gentle 0.25 mg starting dose. At 10 mg/mL, that same 25 units delivers 2.5 mg, which is the maximum maintenance dose for weight management. Same syringe marking. Ten times the medication. This is exactly why concentration matters more than anything else in your semaglutide dosage chart in units.
If you do not know your vial concentration, stop. Do not inject. Check the label on your vial or contact your pharmacy before drawing any medication.
Why the number on your syringe does not directly tell you your dose
Three different measurement systems collide every time someone draws semaglutide into a syringe. Understanding all three is the only way to dose safely.
Units: what the syringe measures
The numbers printed on an insulin syringe are units. Not milligrams. Not milliliters. Units. A standard U-100 insulin syringe holds 100 units per 1 mL of total volume. So when you pull the plunger to the 25-unit line, you are drawing exactly 0.25 mL of liquid into the barrel.
That is all the syringe tells you. Volume.
It does not know what is dissolved in that liquid. It does not know if the vial contains 1 mg per mL or 10 mg per mL. The syringe is simply a measuring device for liquid volume, and the semaglutide syringe dosage chart on your pharmacy instructions translates that volume into actual medication dose.
Milliliters: the volume of liquid
Milliliters measure how much liquid you are injecting. On a U-100 insulin syringe, the conversion is straightforward. 10 units equals 0.1 mL. 25 units equals 0.25 mL. 50 units equals 0.5 mL. 100 units equals 1.0 mL.
This relationship between units and milliliters stays constant regardless of what medication is in the syringe. Whether you are drawing semaglutide, insulin, or plain water, 25 units is always 0.25 mL. For a deeper breakdown of how semaglutide units convert to milliliters, our complete volume guide covers every common measurement.
Milligrams: the actual medication dose
Milligrams are what matter for your therapeutic effect. Your prescriber writes your dose in milligrams because that is the amount of active semaglutide entering your body. The challenge is that milligrams are invisible on the syringe. You cannot see them. You can only calculate them.
And the calculation requires one critical piece of information. The concentration of your vial.
This three-way relationship between units, milliliters, and milligrams is where nearly every dosing error originates. People see 25 units on the syringe and assume it means the same milligram dose regardless of concentration. It does not. A semaglutide conversion chart specific to your concentration is the only reliable way to translate syringe markings into actual dose.
The conversion formula explained step by step
The math behind converting 25 units to milligrams is simple once you understand it. One formula works for every concentration, every syringe size, and every dose.
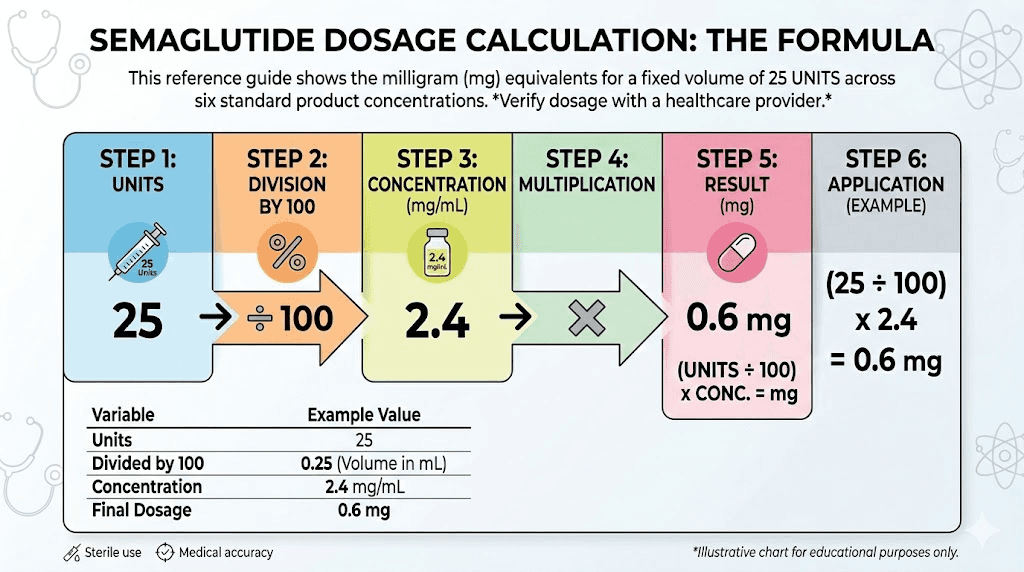
The universal formula
Dose in mg = (units on syringe / 100) x concentration in mg/mL
That is it. Divide your syringe units by 100 to get milliliters, then multiply by the concentration on your vial. The result is your dose in milligrams.
Worked example: 25 units at 5 mg/mL
Step 1. Divide 25 units by 100. That gives you 0.25 mL.
Step 2. Multiply 0.25 mL by 5 mg/mL. That gives you 1.25 mg.
So 25 units from a 5 mg/mL vial equals 1.25 mg of semaglutide. This is a common mid-range dose that falls between the 1 mg semaglutide dose and the 1.7 mg dose in standard titration schedules.
Worked example: 25 units at 2.5 mg/mL
Step 1. Divide 25 units by 100. That gives you 0.25 mL.
Step 2. Multiply 0.25 mL by 2.5 mg/mL. That gives you 0.625 mg.
At this concentration, 25 units delivers 0.625 mg. This falls between the standard 0.25 mg starting dose and the 1 mg escalation dose, which could represent a mid-point titration step for people who need a gentler increase.
Worked example: 25 units at 1 mg/mL
Step 1. Divide 25 units by 100. That gives you 0.25 mL.
Step 2. Multiply 0.25 mL by 1 mg/mL. That gives you 0.25 mg.
At 1 mg/mL, 25 units equals 0.25 mg, which is the standard starting dose for semaglutide weight loss protocols. Many pharmacies use this lower concentration specifically because it makes starting doses easier to measure on the syringe. Instead of drawing a tiny 5-unit dose from a 5 mg/mL vial, you draw a more visible and more accurate 25-unit dose from a 1 mg/mL vial. The 5 mg/mL semaglutide dosage chart and lower concentration charts handle these differences.
Worked example: 25 units at 10 mg/mL
Step 1. Divide 25 units by 100. That gives you 0.25 mL.
Step 2. Multiply 0.25 mL by 10 mg/mL. That gives you 2.5 mg.
This is the maximum dose. At 10 mg/mL concentration, 25 units delivers a full 2.5 mg maintenance dose. Some compounding pharmacies use this high concentration so that maintenance-dose patients inject smaller volumes. But the margin for error is enormous. Drawing just 5 extra units at this concentration adds 0.5 mg to your dose, which is the equivalent of jumping two full titration steps. For the complete breakdown of high-concentration dosing, see our 10 mg semaglutide dosage chart.
Complete conversion tables: 25 units compared to every common dose
Knowing what 25 units equals at your concentration is useful. But understanding how it compares to other unit measurements gives you the full picture of where your dose falls in the overall protocol.
At 5 mg/mL (the most common compounded concentration)
Units on syringe | Volume (mL) | Dose (mg) | Protocol stage |
|---|---|---|---|
5 units | 0.05 mL | 0.25 mg | Starting dose |
10 units | 0.10 mL | 0.50 mg | Month 2 dose |
20 units | 0.20 mL | 1.00 mg | Month 3 dose |
25 units | 0.25 mL | 1.25 mg | Between month 3 and 4 |
34 units | 0.34 mL | 1.70 mg | Month 4 dose |
48 units | 0.48 mL | 2.40 mg | Maintenance dose |
50 units | 0.50 mL | 2.50 mg | Maximum dose |
At 5 mg/mL, 10 units equals 0.5 mg and 20 units equals 1 mg. So 25 units at 1.25 mg sits right between the month 3 and month 4 escalation doses. Some providers prescribe this exact dose as an intermediate step for patients who tolerate 1 mg well but experience significant side effects at 1.7 mg. For context on higher doses, 40 units delivers 2 mg and 50 units delivers 2.5 mg.
At 2.5 mg/mL
Units on syringe | Volume (mL) | Dose (mg) | Protocol stage |
|---|---|---|---|
10 units | 0.10 mL | 0.25 mg | Starting dose |
20 units | 0.20 mL | 0.50 mg | Month 2 dose |
25 units | 0.25 mL | 0.625 mg | Between month 2 and 3 |
40 units | 0.40 mL | 1.00 mg | Month 3 dose |
68 units | 0.68 mL | 1.70 mg | Month 4 dose |
96 units | 0.96 mL | 2.40 mg | Maintenance dose |
Notice how dramatically different the picture looks at 2.5 mg/mL. The same 25 units that delivers 1.25 mg from a 5 mg/mL vial only delivers 0.625 mg here. This concentration is popular because it allows larger, easier-to-measure syringe draws at starting and low doses. The 5 mg in 2 mL dosage chart covers this concentration in full detail.
At 10 mg/mL
Units on syringe | Volume (mL) | Dose (mg) | Protocol stage |
|---|---|---|---|
2.5 units | 0.025 mL | 0.25 mg | Starting dose |
5 units | 0.05 mL | 0.50 mg | Month 2 dose |
10 units | 0.10 mL | 1.00 mg | Month 3 dose |
25 units | 0.25 mL | 2.50 mg | Maximum dose |
At 10 mg/mL, 25 units is the maximum therapeutic dose. Starting doses at this concentration require drawing just 2.5 units, which is nearly impossible to measure accurately on most insulin syringes. This is why higher concentrations are typically used only for patients on maintenance doses, not for people just beginning treatment. The 10 mg vial dosage chart explains why some pharmacies avoid shipping this concentration to new patients.
At 1 mg/mL
Units on syringe | Volume (mL) | Dose (mg) | Protocol stage |
|---|---|---|---|
25 units | 0.25 mL | 0.25 mg | Starting dose |
50 units | 0.50 mL | 0.50 mg | Month 2 dose |
100 units | 1.00 mL | 1.00 mg | Month 3 dose |
At 1 mg/mL, 25 units is the standard starting dose, and the syringe draws are large enough to measure precisely. But you run out of syringe capacity quickly. The 100-unit maximum on a standard syringe only gets you to 1 mg at this concentration, which means higher doses require either a larger syringe or a higher concentration vial.
Where 25 units falls in the standard semaglutide dosing schedule
The standard semaglutide titration protocol follows a step-up pattern over several months. Understanding where 25 units lands in that schedule helps you know whether your dose is appropriate for your treatment stage.
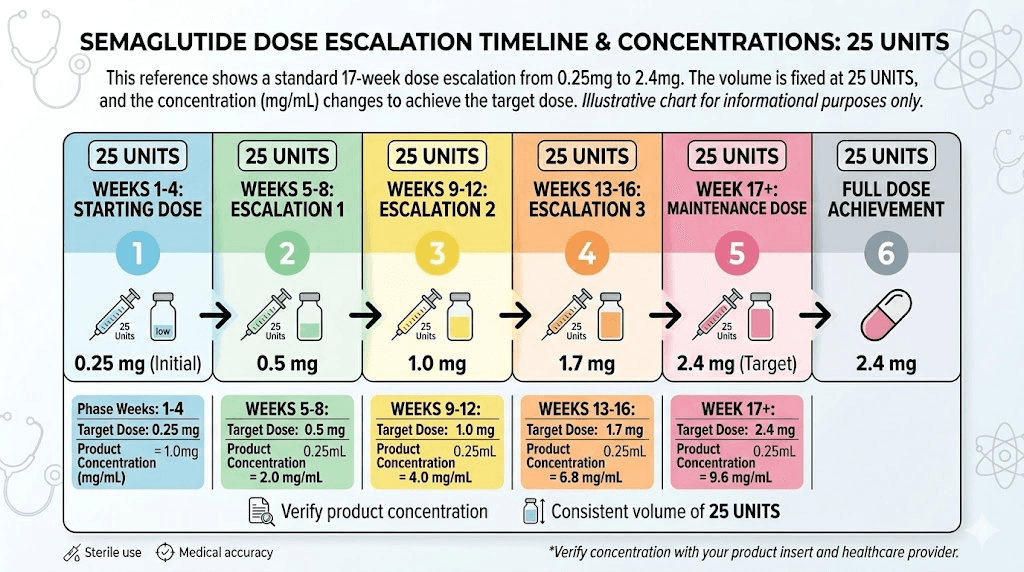
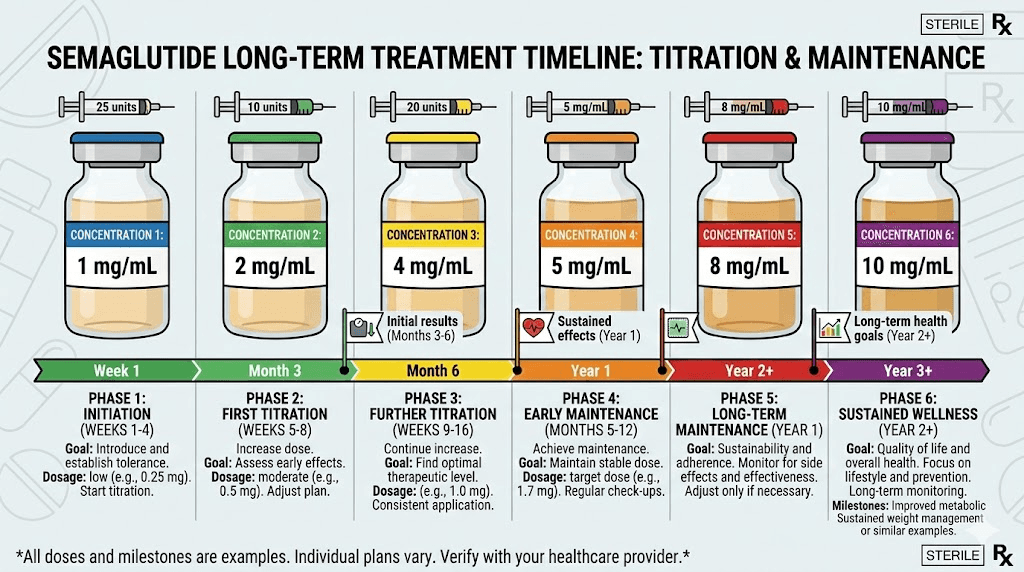
The standard titration protocol
Most providers follow this escalation schedule for weight management with semaglutide.
Weeks 1 through 4: 0.25 mg once weekly. This is the initial tolerance-building phase. Most people feel minimal appetite suppression at this dose but may experience some gastrointestinal adjustment. At 5 mg/mL concentration, this starting dose is just 5 units on the syringe, which is why some pharmacies provide lower-concentration vials for beginners. You can learn more about what to expect in the first week on semaglutide in our timeline guide.
Weeks 5 through 8: 0.50 mg once weekly. The first dose increase. Appetite suppression typically becomes noticeable during this phase, and most people begin to see measurable changes on the scale. Some experience semaglutide bloating or sulfur burping as the body adjusts to higher GLP-1 receptor activation.
Weeks 9 through 12: 1.0 mg once weekly. A significant step up. This is where many people find their effective dose, particularly those with moderate weight loss goals. Side effects tend to stabilize by this point for most users.
Weeks 13 through 16: 1.7 mg once weekly. The second-to-last escalation step. This dose provides strong appetite suppression and meaningful weight loss for the majority of users.
Week 17 onward: 2.4 mg once weekly. The standard maintenance dose for weight management, and the dose used in the major clinical trials. Some providers allow up to 2.5 mg for compounded formulations.
So where does 25 units fit?
It depends on your concentration.
At 5 mg/mL, 25 units gives you 1.25 mg, which falls between the week 9 and week 13 protocol doses. This is not a standard titration step in the FDA-approved Wegovy protocol, but many compounding pharmacies and telehealth providers use intermediate doses like 1.25 mg for patients who need a gentler escalation. If you jumped from 1 mg to 1.7 mg and experienced intolerable constipation, fatigue, or dizziness, stepping back to 1.25 mg might be exactly what your provider recommends.
At 2.5 mg/mL, 25 units gives you 0.625 mg, which falls between the starting dose and the second-month dose. Some microdosing protocols use this exact amount.
At 1 mg/mL, 25 units is simply the standard starting dose of 0.25 mg. Nothing unusual here.
At 10 mg/mL, 25 units is 2.5 mg, which is the maximum dose. If your vial is this concentration and you are drawing 25 units, you should be well into your maintenance phase and fully titrated up.
How to read 25 units on your insulin syringe
Drawing exactly 25 units sounds simple. Pull the plunger to the 25-unit mark. But syringe sizes vary, and the spacing between markings differs dramatically depending on the syringe capacity.
The 0.3 mL syringe (30-unit capacity)
This is the smallest common insulin syringe. It holds a maximum of 30 units, and each marking typically represents 0.5 or 1 unit. The 25-unit mark sits near the top of the barrel, leaving very little room above it. The advantage of this syringe for a 25-unit dose is precision. The markings are spread far apart, making it easy to see exactly where you are drawing to. The disadvantage is that you are using almost the entire syringe capacity for a single dose.
The 0.5 mL syringe (50-unit capacity)
This mid-size syringe is the most common choice for semaglutide injections. Each marking typically represents 1 unit, and 25 units falls exactly at the midpoint of the barrel. This gives you clear visibility, easy measurement, and room to draw slightly more if needed. For detailed guidance on how to give a semaglutide injection with a syringe, our step-by-step guide covers proper technique.
The 1.0 mL syringe (100-unit capacity)
The largest insulin syringe. Each marking typically represents 2 units, which means the 25-unit mark falls between two lines on many versions of this syringe. That introduces imprecision. If you need to draw exactly 25 units, you are estimating the halfway point between the 24-unit and 26-unit lines, and even small visual errors translate to measurable dose differences. Use a 0.5 mL syringe whenever possible for a 25-unit dose.
Syringe reading tips for accuracy
Hold the syringe at eye level. Tilting it up or down changes the apparent position of the plunger. Read the top edge of the rubber plunger, not the bottom. Make sure the syringe tip is submerged in the liquid before drawing to avoid air bubbles, which take up space and reduce your actual medication volume. And tap out any bubbles before injecting.
If you struggle with small markings, a magnifying glass helps. Accuracy matters here. At 5 mg/mL, each extra unit on the syringe adds 0.05 mg of semaglutide. At 10 mg/mL, each extra unit adds 0.1 mg. These small measurement variations compound over weeks and months of dosing. Our semaglutide dosage calculator eliminates the guesswork by calculating exact unit measurements for any concentration.
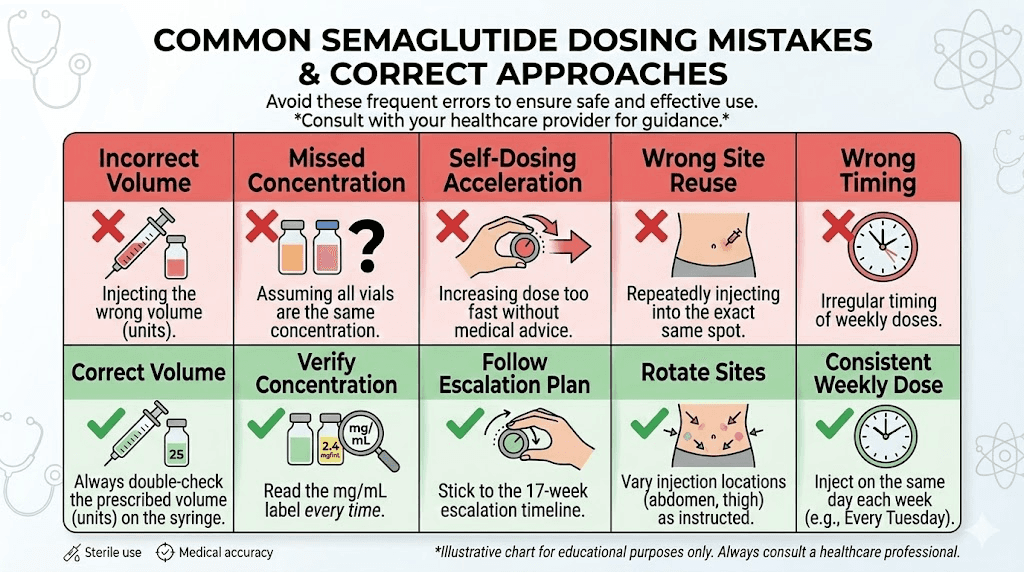
The most dangerous semaglutide dosing mistakes and how to avoid them
The FDA issued a formal safety alert about dosing errors with compounded injectable semaglutide. These are not theoretical risks. They are documented cases where real patients received doses far exceeding what their providers intended.
Mistake 1: using a dosage chart for the wrong concentration
This is the most common and most dangerous error. A patient receives a 2.5 mg/mL vial but follows a chart designed for 5 mg/mL. At 5 mg/mL, drawing 10 units gives you 0.5 mg. But at 2.5 mg/mL, drawing 10 units gives you only 0.25 mg, which is half the intended dose. The reverse is worse. Someone with a 5 mg/mL vial following a 2.5 mg/mL chart would draw twice what they intended.
Before every injection, check three things. The concentration on your vial label. The concentration that your dosage chart is designed for. Whether they match. If they do not match, contact your pharmacy immediately. For concentration-specific guides, we have detailed charts for 5 mg semaglutide, 5 mg vial dosing, and 10 mg vial dosing.
Mistake 2: confusing units with milligrams
Someone prescribed 2.5 mg of semaglutide draws 25 units thinking that 25 is close enough to 2.5. But 25 units is not 2.5 mg at most concentrations. At 5 mg/mL, 25 units equals 1.25 mg. At 1 mg/mL, 25 units equals only 0.25 mg. The only concentration where 25 units equals 2.5 mg is 10 mg/mL, and even that relationship is a coincidence of the math, not a general rule.
Units and milligrams are fundamentally different measurements. Never assume they correspond directly.
Mistake 3: using the wrong syringe type
Some patients use tuberculin syringes instead of insulin syringes. Tuberculin syringes are marked in milliliters rather than units, and the graduation markings are different. Drawing to the 0.25 mark on a tuberculin syringe gives you 0.25 mL (which is correct for 25 units), but the visual landmarks are different enough to cause errors. Always use a U-100 insulin syringe unless your provider specifically instructs otherwise. The semaglutide syringe dosage conversion chart is designed specifically for U-100 insulin syringes.
Mistake 4: not accounting for pharmacy changes
Compounding pharmacies sometimes change concentrations between refills without making it obvious. You might receive a 5 mg/mL vial one month and a 2.5 mg/mL vial the next. If you do not check the label each time, you could accidentally double or halve your dose. This is particularly common with compounded semaglutide because there is no standardized concentration across pharmacies.
Make it a habit. Every new vial, check the concentration. Every time.
Mistake 5: drawing from a vial that has been reconstituted incorrectly
If you are using lyophilized (freeze-dried) semaglutide that requires reconstitution, the amount of bacteriostatic water you add to 5 mg of semaglutide determines the final concentration. Add 1 mL and you get 5 mg/mL. Add 2 mL and you get 2.5 mg/mL. If you mixed incorrectly or lost track of how much water you added, every subsequent dose from that vial will be wrong.
Label your vials after reconstitution. Write the date, the total mg of semaglutide, the amount of water added, and the resulting concentration. For proper technique, follow our semaglutide reconstitution guide and cross-reference with the semaglutide reconstitution chart.
How 25 units compares to other common semaglutide doses
People search for specific unit-to-mg conversions constantly. If you landed on this page looking for 25 units, you might also want to know how neighboring doses compare. Here is the complete landscape at the most common 5 mg/mL concentration.
Units | mg at 5 mg/mL | Common protocol use | Detailed guide |
|---|---|---|---|
5 units | 0.25 mg | Starting dose (weeks 1-4) | |
10 units | 0.50 mg | Second-month dose | |
20 units | 1.00 mg | Third-month dose | |
25 units | 1.25 mg | Intermediate dose | You are here |
34 units | 1.70 mg | Fourth-month dose | |
40 units | 2.00 mg | Near-maintenance dose | |
48 units | 2.40 mg | Standard maintenance | |
50 units | 2.50 mg | Maximum dose | |
100 units | 5.00 mg | Full vial (do not inject this amount) |
At 5 mg/mL, the 25-unit dose of 1.25 mg is notably absent from the standard FDA-approved Wegovy titration schedule, which jumps from 1 mg directly to 1.7 mg. But many compounding pharmacy protocols include 1.25 mg as an intermediate step. And for good reason. The jump from 1 mg to 1.7 mg represents a 70% dose increase, which triggers more intense side effects than any other step in the protocol. Adding 1.25 mg as a bridge reduces the jump to just 25% followed by 36%, which many patients tolerate far better.
If you are wondering whether 20 units of semaglutide is too much or if 50 units is a lot, those guides break down the context for each dose level. The right dose depends on your treatment stage, body weight, tolerance, and therapeutic goals.
Compounded semaglutide concentrations and the 25-unit question
The compounded semaglutide market uses a wide range of concentrations, and that variety creates the bulk of dosing confusion. Unlike brand-name Ozempic or Wegovy, where the pen auto-delivers a preset dose, compounded semaglutide requires manual calculation every time you draw a dose.
Common compounding pharmacy concentrations
Pharmacy concentration choices vary. Here are the most common options and what 25 units delivers from each.
1 mg/mL. Used primarily for patients in early titration. Drawing 25 units delivers 0.25 mg, which is the standard starting dose. This concentration makes starting doses easy to measure but becomes impractical for maintenance doses because you would need to draw 240 units (2.4 mL) for a 2.4 mg dose, which exceeds the capacity of any standard insulin syringe. Pharmacies like Empower Pharmacy sometimes use this concentration for initial prescriptions.
2.5 mg/mL. A middle-ground concentration. Drawing 25 units delivers 0.625 mg. This concentration works for starting through mid-range doses on a single syringe but still runs into volume issues at maximum doses. The semaglutide dosage chart in mL covers volume calculations for this concentration.
3 mg/mL. Less common but used by some pharmacies. Drawing 25 units delivers 0.75 mg. This sits between common dose steps, making it useful for gradual titration.
5 mg/mL. The most widely used concentration for compounded semaglutide. Drawing 25 units delivers 1.25 mg. This concentration balances precision at low doses with practicality at high doses. All standard doses fit within a 50-unit (0.5 mL) syringe. Many of the most popular pharmacies, including Olympia Pharmacy and BPI Labs, use this concentration.
10 mg/mL. The highest commonly available concentration. Drawing 25 units delivers 2.5 mg. Only appropriate for patients on maintenance doses. The tiny volumes required for starting doses at this concentration make accurate measurement nearly impossible without specialized syringes.
How to verify your vial concentration
Check three places. First, the label on the vial itself. Second, the packaging insert or information sheet that came with the vial. Third, the pharmacy paperwork or online portal where your prescription details are listed. If any of these sources disagree, call the pharmacy before injecting.
The label should clearly state the concentration in mg/mL format. If it only lists total mg and total mL (for example, 5 mg in 2 mL), divide the total mg by the total mL to get the concentration. 5 mg divided by 2 mL equals 2.5 mg/mL.
B12 and other additives in compounded formulations
Many compounding pharmacies add supplemental ingredients to their semaglutide formulations. Semaglutide with B12 is the most common combination. Others include semaglutide with glycine, semaglutide with L-carnitine, and semaglutide with niacinamide. The semaglutide glycine B12 blend is particularly popular.
These additives do not change the semaglutide concentration calculation. If the vial label says 5 mg/mL of semaglutide, that is the number you use in your conversion formula regardless of what else is in the vial. But the additives can change the total volume of liquid in the vial, so always check the semaglutide-specific concentration rather than trying to calculate it from total vial volume. Our compounded semaglutide with B12 dosage chart has concentration-specific calculations for these combination formulations.
What to do if you drew or injected the wrong number of units
Mistakes happen. Here is what to do for each scenario.
If you drew too many units but have not injected yet
Simply push the plunger back to expel the excess medication into the vial. Then redraw to the correct 25-unit mark. Check for air bubbles after redrawing, tap them out, and push the plunger to the correct line again. No medication is wasted if you catch the error before injection.
If you already injected more than 25 units
Do not panic. But monitor yourself carefully. The most common side effects of an accidentally high semaglutide dose are nausea, vomiting, and diarrhea, which are intensified versions of the normal semaglutide side effects. If you injected significantly more than intended (for example, 50 units instead of 25 from a 5 mg/mL vial, giving you 2.5 mg instead of 1.25 mg), contact your healthcare provider. The appetite suppression may be immediate and intense, and you may need guidance on managing the next few days.
Keep hydrating. Eat small, bland meals. The best foods to eat on semaglutide during a period of increased nausea are the same ones recommended for any GI upset: plain crackers, toast, broth, and simple proteins. Avoid the foods to avoid on semaglutide, particularly greasy, fried, or heavy meals that worsen nausea.
For a true overdose (five to ten times the intended dose), seek medical attention immediately. The FDA warning specifically cited cases where patients received 5-10x their intended dose due to concentration confusion, resulting in severe adverse effects that required medical intervention.
If you injected fewer than 25 units
An underdose is less dangerous but still worth addressing. If you drew 20 units instead of 25 from a 5 mg/mL vial, you received 1.0 mg instead of 1.25 mg. That is not a medical emergency. It simply means your appetite suppression may be slightly less effective that week.
Do not give yourself a supplemental injection to make up the difference. Wait until your next scheduled dose and draw the correct amount. If underdosing happens repeatedly, it might indicate that you need a syringe with better markings for your dose range. Consider switching to a 0.3 mL or 0.5 mL syringe where the 25-unit mark is easier to identify precisely.
Practical tips for accurate 25-unit dosing
Getting exactly 25 units every time requires good technique and a few simple habits.
Choose the right syringe size
A 0.5 mL (50-unit) syringe is ideal for 25-unit doses. The 25-unit mark falls exactly at the halfway point, making it the easiest landmark to hit. The 0.3 mL (30-unit) syringe also works but leaves minimal room if you need to draw slightly more. Avoid the 1.0 mL (100-unit) syringe for this dose because the markings are compressed and harder to read at the 25-unit position.
Proper drawing technique
Wash your hands. Clean the vial stopper with an alcohol swab. Draw 25 units of air into the syringe. Insert the needle through the rubber stopper. Push the air into the vial (this replaces the liquid volume you are about to remove, preventing a vacuum). Invert the vial. Pull the plunger to the 30-unit mark to overdraw slightly. Tap out air bubbles. Slowly push the plunger back down to exactly 25 units. Remove the needle from the vial.
This overdraw-then-adjust technique is more accurate than trying to draw exactly 25 units in one pull, because air bubbles trapped during the initial draw would reduce your actual medication volume. For the full injection process, our guide on the best injection site for semaglutide covers site selection, rotation, and pain reduction techniques.
Storage matters for dose accuracy
Temperature affects semaglutide stability and potency. A vial that has degraded due to improper storage may not deliver the expected dose even if you draw the correct number of units, because some of the active compound may have broken down.
Keep your vial refrigerated between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius). If you need to know how long compounded semaglutide lasts in the fridge, most compounded formulations maintain potency for 28 to 90 days depending on the pharmacy and preservative used. Never freeze semaglutide. If your vial was left out warm or exposed to heat, check with your pharmacy before using it. And yes, compounded semaglutide must be refrigerated at all times.
If the liquid in your vial has changed color, become cloudy, or contains particles, do not use it. Our guides on what color semaglutide should be and semaglutide shelf life help you determine whether your medication is still safe to use.
Timing your injection
Semaglutide is a once-weekly injection. The best time of day to take semaglutide is whenever you can be consistent. Many people inject in the morning. Others prefer evening. The key is picking the same day each week and roughly the same time.
You can inject semaglutide in the abdomen, upper arm, or thigh. Rotate injection sites to prevent tissue irritation. Avoid injecting into areas that are bruised, tender, red, or hard. For step-by-step injection technique, see how to inject GLP-1 medications.
Understanding your results at the 25-unit dose level
What should you expect from 25 units of semaglutide? The answer depends on which milligram dose you are actually receiving.
At 0.25 mg (25 units from 1 mg/mL)
This is the lowest therapeutic dose. Expect minimal appetite changes in the first week or two. Some people feel slightly less hungry. Others notice nothing at all. This is normal and intentional. The starting dose exists to let your body adjust to the medication, not to produce dramatic weight loss. Our first week on semaglutide guide covers realistic expectations.
Weight loss at this dose is typically 1 to 3 pounds over four weeks, though some people lose nothing until the dose increases. If you are four weeks into semaglutide with no weight loss, the starting dose is almost certainly too low for your body to produce visible results. That is expected.
At 0.625 mg (25 units from 2.5 mg/mL)
This intermediate dose falls between the first and second standard titration steps. Appetite suppression is typically becoming noticeable at this range. Most people feel satisfied with smaller portions and experience fewer cravings, particularly for high-calorie, high-sugar foods. How long semaglutide takes to suppress appetite varies by individual, but most feel meaningful effects within two to three weeks at doses above 0.5 mg.
At 1.25 mg (25 units from 5 mg/mL)
This is a solid mid-range dose. Appetite suppression is typically significant at this level. Most people are eating noticeably less, losing weight consistently, and may be experiencing some manageable side effects. Common side effects include mild nausea (especially on injection day), occasional constipation, and fatigue.
How fast semaglutide works depends on the dose, and 1.25 mg typically produces measurable results within the first month at that dose. One-month results at this level often show 4 to 8 pounds of weight loss, with significant variation based on diet, activity, and starting weight.
At 2.5 mg (25 units from 10 mg/mL)
Maximum dose territory. Appetite suppression is at its strongest. Weight loss should be consistent and significant. Most clinical trial participants at this dose range lost 15 to 20 percent of their body weight over 68 weeks. Side effects are also at their peak intensity, though most people have acclimated to them through the titration process. Before and after semaglutide results at maintenance doses show transformative changes for many users.
If you have reached the maximum dose and are not losing weight on semaglutide, there are several factors to investigate. Diet quality, exercise habits, sleep, stress, and metabolic adaptation all play roles. Some people hit a semaglutide plateau that requires adjustments beyond simply increasing the dose.
When to consider switching from semaglutide to tirzepatide
If you are on 25 units of semaglutide and not seeing the results you want, switching medications is one option your provider might discuss.
Tirzepatide (the active ingredient in Mounjaro and Zepbound) differs from semaglutide in that it activates both GLP-1 and GIP receptors rather than GLP-1 alone. Clinical trials suggest tirzepatide produces greater average weight loss than semaglutide at comparable doses. The semaglutide vs tirzepatide dosage chart maps equivalent doses between the two medications.
The semaglutide to tirzepatide conversion chart helps providers determine the appropriate starting dose of tirzepatide for patients transitioning from semaglutide. Generally, if you are on 1.25 mg of semaglutide (25 units from a 5 mg/mL vial), you might start tirzepatide at 2.5 mg or 5 mg, depending on your provider preference and side effect history. For the full details on making this switch, see our guide on switching between semaglutide and tirzepatide.
Retatrutide is another option emerging in clinical trials, activating GLP-1, GIP, and glucagon receptors simultaneously. Early data suggests even greater weight loss than tirzepatide, though it is not yet commercially available. The side effect profiles differ between all three medications.
Combining semaglutide with other treatments
SeekPeptides members frequently ask about combining semaglutide with other compounds to enhance weight loss or manage side effects.
Combining phentermine and semaglutide is one approach some providers use, though the evidence base for this combination is limited. Phentermine vs semaglutide comparisons show they work through completely different mechanisms, which is why some clinicians believe they can complement each other.
Berberine and semaglutide is another combination that has gained attention, with berberine potentially supporting blood sugar regulation through mechanisms that differ from GLP-1 receptor activation.
For weight loss optimization while on semaglutide, following a structured semaglutide diet plan makes a measurable difference. The list of foods to eat while on semaglutide focuses on nutrient-dense options that keep you satisfied while supporting weight loss. And yes, people always ask about drinking alcohol on semaglutide, and the short answer is that alcohol tolerance typically decreases on GLP-1 medications.
Long-term considerations for semaglutide users
How long you stay on semaglutide is a question every user eventually asks. The current evidence suggests that weight regain occurs in most people who discontinue semaglutide, with studies showing roughly two-thirds of lost weight returning within a year of stopping. This has led many providers to recommend indefinite use for weight management.
Semaglutide withdrawal symptoms are not true pharmacological withdrawal like opioid or benzodiazepine withdrawal. But appetite and hunger signals return when the medication clears your system, typically within two to three weeks of the last injection. The psychological adjustment can be challenging for people who have become accustomed to reduced appetite.
If you do decide to discontinue, restarting semaglutide after a break generally requires retitrating from a lower dose rather than jumping back to your previous maintenance dose. This reduces the risk of severe side effects from sudden GLP-1 receptor activation.
For those exploring whether you can lose weight on semaglutide without exercise, the data says yes, but exercise significantly improves outcomes, preserves muscle mass, and supports metabolic health in ways that medication alone cannot replicate.
Using calculators to verify your 25-unit dose
Manual math works. But calculators eliminate the chance of arithmetic errors.
The SeekPeptides semaglutide dosage calculator takes your vial concentration and desired dose in milligrams, then tells you exactly how many units to draw. Enter your concentration, enter your target mg, and the calculator does the rest. No formulas to remember. No opportunities for decimal point errors.
If you are reconstituting semaglutide from a lyophilized powder, the peptide reconstitution calculator tells you exactly how much bacteriostatic water to add to achieve your desired concentration. And the general peptide calculator handles dosage calculations for any peptide, not just semaglutide.
These tools are free to use. No sign-up required. SeekPeptides built them specifically because dosing errors are preventable, and nobody should have to risk their health over a math mistake.
Related dosing questions you might have
If you are calculating 25-unit doses, you probably have related questions about the broader semaglutide dosing landscape. Here are quick answers with links to our detailed guides.
What is the right starting dose? Most protocols start at 0.25 mg once weekly, regardless of body weight. At 5 mg/mL, that is just 5 units on the syringe. See our full semaglutide dosing chart in units for every step in the standard protocol.
How do I know if my dose is working? Most people see noticeable appetite suppression within two to four weeks at effective doses. If semaglutide is not working yet, you may need a higher dose or more time. Patience during titration is essential.
Can I split my dose? Some providers prescribe twice-weekly semaglutide dosing at half the weekly amount. This is not standard protocol but is used by some clinicians to reduce side effects. Discuss this with your prescriber before making any changes.
What if I miss a dose? If you miss your weekly injection and it has been fewer than 5 days, take the dose as soon as you remember. If it has been 5 or more days, skip the missed dose and take the next one on your regular schedule. Do not double up.
How do I mix my own vial? If you received lyophilized semaglutide, follow the semaglutide mixing chart for your vial size. The 5 mg mixing chart and 10 mg mixing chart provide step-by-step instructions with exact water volumes.
For researchers serious about optimizing their protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Understanding GLP-1 medications beyond semaglutide
Semaglutide is one medication in a rapidly growing class of GLP-1 receptor agonists. Understanding the broader landscape helps you make informed decisions about your treatment.
GLP-1 and Ozempic are not the same thing. GLP-1 (glucagon-like peptide-1) is a natural hormone your body produces. Ozempic is a brand name for semaglutide, which mimics that hormone. Multiple medications now target GLP-1 receptors, each with different dosing, efficacy, and side effect profiles.
GLP-1 fatigue is a common side effect across the entire medication class, not just semaglutide. GLP-1 hair loss is another concern that patients frequently raise, though the evidence suggests rapid weight loss rather than the medication itself is the primary driver.
Other medications in the GLP-1 space include oral tirzepatide, which eliminates the need for injections, and GLP-1 patches, which deliver medication through the skin. The oral semaglutide drops offer yet another needle-free delivery method, though absorption and bioavailability differ from injectable forms.
Some people also explore whether certain supplements can provide GLP-1-like effects without prescription medication. Phentermine is not a GLP-1 despite sometimes being discussed in the same breath, as it works through an entirely different mechanism (sympathomimetic appetite suppression rather than incretin mimicry).
Semaglutide dosing for specific pharmacy brands
Different compounding pharmacies format their dosing instructions differently, which can add another layer of confusion to the 25-unit question.
Empower Pharmacy typically provides a dosage chart specific to the concentration they ship. Their vials usually come at 5 mg/mL or similar standard concentrations, and the included chart maps units to mg for that specific vial.
Olympia Pharmacy uses similar formatting. Their semaglutide products include concentration-specific dosing instructions, but you should still verify the concentration against the vial label before your first injection.
Direct Meds and BPI Labs each have their own documentation formats. The key across all pharmacies is the same. Find the concentration on the vial. Match it to the chart. Calculate your units.
Our pharmacy-specific guides include the Strive Pharmacy semaglutide dosage chart and the IVIM semaglutide dosing chart, which provide brand-specific unit-to-mg conversions for the exact concentrations those pharmacies use.
Reconstitution and its impact on 25-unit dosing
If you receive semaglutide as a lyophilized (freeze-dried) powder, you must reconstitute it before use. The amount of water you add directly determines the concentration, which in turn determines what 25 units equals in milligrams.
How reconstitution determines concentration
A 5 mg semaglutide vial reconstituted with 1 mL of bacteriostatic water produces a 5 mg/mL concentration. At this concentration, 25 units equals 1.25 mg.
The same 5 mg vial reconstituted with 2 mL of water produces a 2.5 mg/mL concentration. Now 25 units equals 0.625 mg.
And that same 5 mg vial reconstituted with 0.5 mL of water produces a 10 mg/mL concentration. At this concentration, 25 units equals 2.5 mg.
Same vial. Same powder. Same 25 units on the syringe. Wildly different doses depending on how much water you added. This is why proper semaglutide reconstitution technique is not optional. The 5 mg reconstitution chart and 10 mg reconstitution chart provide exact water volumes for every desired concentration.
Reconstitution best practices
Use a separate syringe for adding water, not the same one you inject with. Draw the exact amount of bacteriostatic water specified for your target concentration. Inject the water slowly down the side of the vial, never directly onto the powder. Swirl gently. Do not shake. Wait until the powder is completely dissolved before drawing any doses.
Once reconstituted, label the vial immediately with the date, total mg, water added, and resulting concentration. Store it in the refrigerator. For comprehensive mixing instructions, see our guide to mixing peptides with bacteriostatic water and the complete semaglutide reconstitution chart.
How long does a reconstituted vial last?
A reconstituted semaglutide vial typically lasts 28 to 90 days in the refrigerator, depending on the preservative (bacteriostatic water contains 0.9% benzyl alcohol as a preservative). How long semaglutide is good for after reconstitution varies by pharmacy recommendations, but most suggest using the vial within 28 days for maximum potency. After that, the semaglutide may begin to degrade, which could mean your 25-unit dose delivers less active medication than expected.
If you are unsure whether your vial is still viable, check the expired semaglutide safety guide and the compounded semaglutide expiration guide for detailed assessment criteria.
Side effect management at the 25-unit dose level
Side effects correlate strongly with dose. What you experience at 25 units depends on the milligram dose that those units represent and your individual sensitivity.
At lower mg doses (0.25 to 0.625 mg), side effects are typically mild or absent. Most people tolerate starting doses with minimal issues. Mild nausea on injection day is the most common report.
At mid-range doses (1.0 to 1.25 mg), side effects become more noticeable. Bloating, sulfur burps, and constipation are common. Most of these are manageable with dietary adjustments and over-the-counter remedies. Insomnia affects some users, while others report increased fatigue.
At maximum doses (2.4 to 2.5 mg), side effects are most pronounced. This is why the titration schedule exists, because gradual dose escalation gives your body time to adapt. Jumping straight to 2.5 mg (25 units from a 10 mg/mL vial) without titrating would produce severe nausea, vomiting, and diarrhea in most people.
Semaglutide can affect menstrual cycles in some women, and some users report changes in sex drive. These effects are more commonly reported at higher doses. Some people actually feel more energetic on semaglutide, potentially because reduced food intake and weight loss improve sleep quality and reduce metabolic burden.
Frequently asked questions
Is 25 units the same as 0.25 mL on the syringe?
Yes. On a U-100 insulin syringe, 25 units equals exactly 0.25 mL of liquid volume. This relationship is constant regardless of what medication is in the syringe. The semaglutide dosage chart in mL covers volume-based measurements in detail.
Does the brand of semaglutide change how many mg are in 25 units?
Not directly. What matters is the concentration (mg/mL), not the brand. However, different brands and compounding pharmacies use different concentrations, so a 25-unit draw from one pharmacy vial may deliver a different mg dose than a 25-unit draw from another. Always check the concentration on your specific vial.
Can I use the same conversion chart for tirzepatide?
No. Semaglutide and tirzepatide are different medications with different standard concentrations. A tirzepatide dosage chart in units uses tirzepatide-specific concentrations. If you are on both medications or switching between them, the semaglutide to tirzepatide conversion chart maps equivalent doses.
What if my pharmacy sends a different concentration than last time?
This happens more often than it should. Always check the label on every new vial before your first injection. If the concentration changed, your unit-to-mg conversion changes too, and you may need to draw a different number of units to maintain the same mg dose. Contact your pharmacy or provider to confirm the correct number of units for the new concentration.
Is 25 units of semaglutide a high dose?
It depends entirely on the concentration. At 1 mg/mL, 25 units (0.25 mg) is the lowest standard dose. At 10 mg/mL, 25 units (2.5 mg) is the highest. Context is everything. Our guide on whether 20 units is too much provides a framework for evaluating dose appropriateness at different concentrations.
Do I need to adjust my dose for body weight?
The standard semaglutide titration protocol does not adjust starting doses based on body weight. Everyone starts at 0.25 mg regardless of size. Higher-weight individuals may ultimately need higher maintenance doses for optimal effect, but the titration schedule remains the same. Your provider adjusts based on response and tolerability, not weight alone.
What happens if I take 25 units every day instead of once a week?
Do not do this. Semaglutide is formulated as a once-weekly injection because of its long half-life (approximately 7 days). Taking it daily would lead to dangerous accumulation in your body, potentially causing severe nausea, vomiting, pancreatitis, and other serious adverse effects. Always follow your prescribed dosing schedule.
Can I use a regular syringe instead of an insulin syringe?
Non-insulin syringes are marked in milliliters rather than units, and their graduation markings are different. While you could technically draw 0.25 mL with a regular syringe to get the equivalent of 25 units, the precision is usually lower, especially at small volumes. Insulin syringes are designed for subcutaneous injection and provide better accuracy for the volumes used in semaglutide dosing. See our peptide injection guide for syringe selection advice.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your calculations stay accurate, your concentrations stay verified, and your doses stay consistent.