Feb 18, 2026

You have been told your target dose is 2.4 mg of semaglutide per week. You are staring at an insulin syringe. And the numbers on that syringe say units, not milligrams. That gap between what your provider prescribed and what your syringe measures has caused more dosing errors than almost any other factor in compounded semaglutide administration. The FDA has documented cases where people accidentally injected five to twenty times their intended dose because they confused units with milligrams.
Here is the short answer. For a 2.4 mg dose of semaglutide, the number of units depends entirely on the concentration of your vial. At 5 mg/mL, 2.4 mg equals 48 units. At 3 mg/mL, it equals 80 units. At 2.5 mg/mL, it equals 96 units. Get the concentration wrong, and you could double or triple your dose without realizing it. This guide breaks down every concentration you are likely to encounter, gives you the exact formula, walks you through the math step by step, and shows you how to avoid the mistakes that send people to poison control centers. Whether you are using brand name Wegovy or a compounded semaglutide formulation, the conversion process follows the same logic. You just need to know your numbers.
SeekPeptides has built comprehensive dosing tools and educational resources specifically to help researchers navigate these calculations safely. Understanding the relationship between milligrams, milliliters, and units is not optional. It is the foundation of accurate dosing.
Why 2.4 mg matters: the maximum maintenance dose
The number 2.4 is not arbitrary. It is the FDA-approved maximum weekly maintenance dose of semaglutide for weight management under the brand name Wegovy. The STEP 1 clinical trial, published in the New England Journal of Medicine, enrolled 1,961 adults and found that participants receiving 2.4 mg of semaglutide weekly lost an average of 14.9% of their body weight over 68 weeks, compared to just 2.4% in the placebo group. One in three participants achieved at least 20% weight loss at this dose.
But you do not start at 2.4 mg. Nobody does.
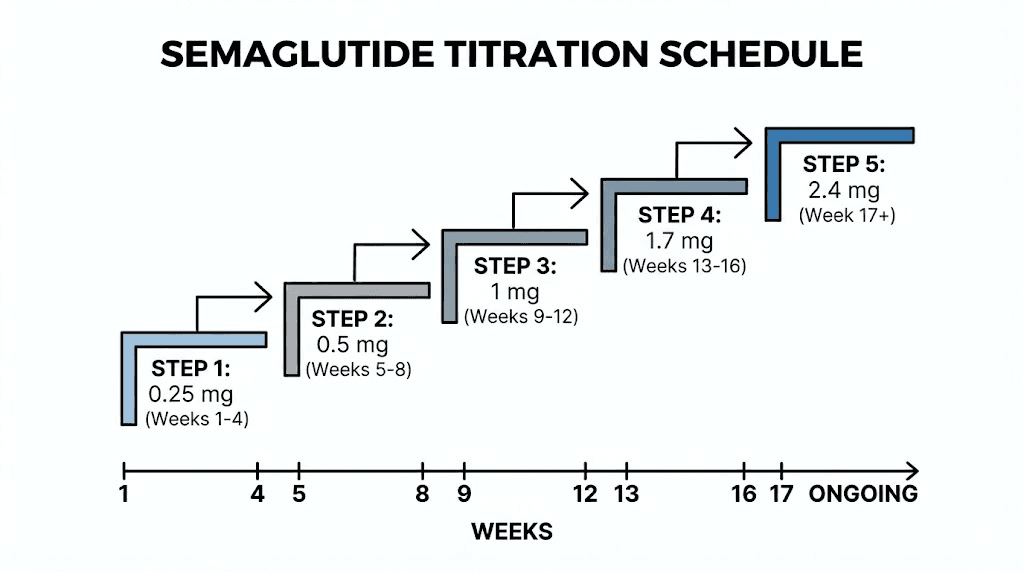
The standard semaglutide dosing protocol follows a five-step titration schedule designed to minimize gastrointestinal side effects. You increase the dose every four weeks until reaching the maintenance level. Here is the complete Wegovy titration schedule:
Weeks 1 through 4: 0.25 mg once weekly
Weeks 5 through 8: 0.5 mg once weekly
Weeks 9 through 12: 1.0 mg once weekly
Weeks 13 through 16: 1.7 mg once weekly
Week 17 onward: 2.4 mg once weekly (maintenance dose)
If you cannot tolerate 2.4 mg, your provider may keep you at 1.7 mg as the maintenance dose. The titration schedule exists because semaglutide activates GLP-1 receptors throughout the body, and your digestive system needs time to adjust. Jumping straight to 2.4 mg would cause severe nausea, vomiting, and diarrhea in most people. The slow escalation lets your body adapt while still moving toward the therapeutic target.
Understanding where 2.4 mg sits in the overall protocol helps you appreciate why getting the unit conversion right matters so much. At this dose level, an error that doubles your intake means you are suddenly receiving 4.8 mg, far beyond what any clinical trial has tested for standard weekly administration. The consequences of that kind of overdose include severe gastrointestinal distress, persistent nausea, vomiting that can last days, and in rare cases, extreme fatigue and dehydration requiring medical attention.
The conversion formula you need to memorize
Every semaglutide unit conversion uses the same formula. Once you understand it, you can calculate the correct number of units for any dose at any concentration. The formula is simple.
Units = (Dose in mg / Concentration in mg per mL) x 100
That is it. Three numbers. One division. One multiplication. But within that simplicity hides the most common source of dosing errors in compounded medications.
Let us break it apart. The dose in mg is what your provider prescribed, in this case 2.4 mg. The concentration in mg per mL is printed on your vial label. It tells you how many milligrams of semaglutide are dissolved in each milliliter of liquid. And the 100 at the end converts milliliters to units, because standard insulin syringes measure 100 units per milliliter. That last part is critical. An insulin syringe is not measuring medication strength. It is measuring volume. When you draw to the 48 unit mark on a U-100 insulin syringe, you are drawing 0.48 mL of liquid. The number of milligrams in that 0.48 mL depends entirely on how concentrated the solution is.
Think of it this way. Imagine you have a glass of lemonade and a glass of lemonade concentrate. Both glasses hold the same volume. But the concentrate delivers far more lemon per sip. Semaglutide concentration works the same way. A 5 mg/mL vial packs twice as much medication per unit as a 2.5 mg/mL vial. Draw the same number of units from both, and you get very different doses.
Here is the reverse formula if you need to go from units back to milligrams:
Dose in mg = (Units / 100) x Concentration in mg per mL
Both formulas are essential for cross-checking your work. Calculate your units, then verify by converting back to milligrams. If you do not get 2.4 mg when you plug your units back into the reverse formula, something went wrong. This double-check takes five seconds and could prevent a serious dosing error. Use the SeekPeptides semaglutide dosage calculator to verify your math every time.
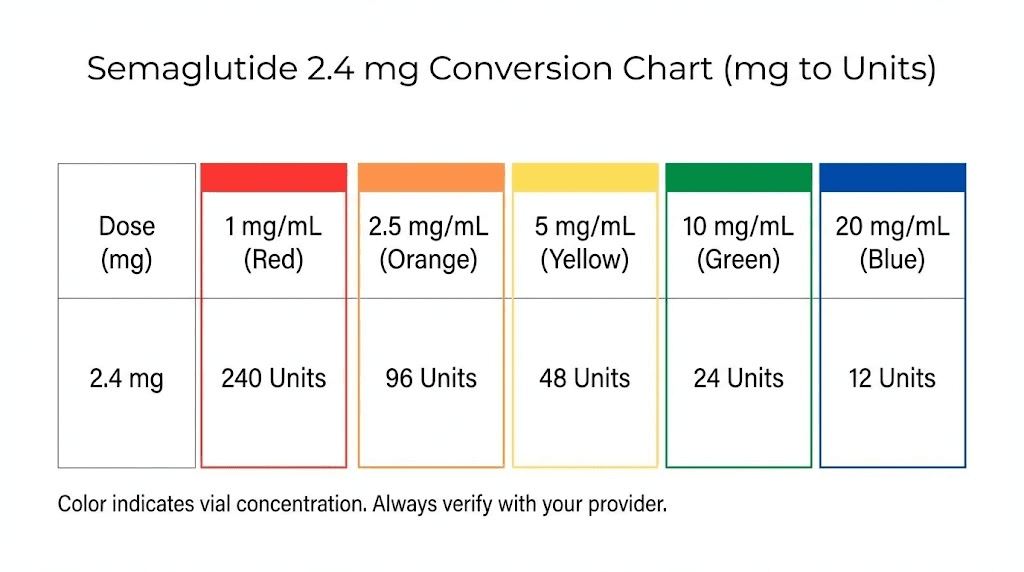
2.4 mg at every common concentration
Compounding pharmacies produce semaglutide at various concentrations. The concentration printed on your vial label determines how many units you need to draw. Here is the complete breakdown for a 2.4 mg dose across every concentration you are likely to encounter.
5 mg/mL concentration (most common)
This is the concentration you will see most frequently from compounding pharmacies. The math is straightforward.
2.4 mg divided by 5 mg/mL equals 0.48 mL. Multiply by 100, and you get 48 units.
On a standard 1 mL (100 unit) insulin syringe, 48 units falls just below the halfway mark. This is a comfortable volume to draw and inject. The 5 mg/mL concentration is popular precisely because it keeps injection volumes manageable even at higher doses. At the maximum maintenance dose of 2.4 mg, you are injecting less than half a milliliter. That means less discomfort at the injection site and less medication pooling under the skin. If your vial says 5 mg/mL, you can use the same 5 mg/mL dosage chart that covers the entire titration schedule.
Here is the complete titration in units at 5 mg/mL:
0.25 mg = 5 units
0.5 mg = 10 units
1.0 mg = 20 units
1.7 mg = 34 units
2.4 mg = 48 units
3 mg/mL concentration
Some pharmacies compound semaglutide at 3 mg/mL. This is less common but still widely available.
2.4 mg divided by 3 mg/mL equals 0.80 mL. Multiply by 100, and you get 80 units.
This is a significantly larger injection volume. At 80 units, you are drawing four-fifths of a full 1 mL syringe. Some people find this volume uncomfortable for subcutaneous injection. If you are using a 3 mg/mL concentration and working up to 2.4 mg, you may want to discuss splitting the dose across two injection sites with your provider. The higher volume also means your vial will run out faster. A 3 mL vial at 3 mg/mL contains 9 mg total, which gives you roughly 3.75 weeks of dosing at the 2.4 mg maintenance level.
Complete titration in units at 3 mg/mL:
0.25 mg = approximately 8 units
0.5 mg = approximately 17 units
1.0 mg = approximately 33 units
1.7 mg = approximately 57 units
2.4 mg = 80 units
2.5 mg/mL concentration
This concentration appears in some compounded formulations and is worth knowing about, especially since it can cause confusion with the 2.5 mg dose level in the titration schedule.
2.4 mg divided by 2.5 mg/mL equals 0.96 mL. Multiply by 100, and you get 96 units.
This is nearly a full syringe. At 96 units on a 100-unit syringe, you have almost no room for error. Drawing this dose accurately requires careful attention because even a small overshoot pushes you past the syringe capacity. For this reason, many providers recommend against using 2.5 mg/mL concentrations for patients on the 2.4 mg maintenance dose. If your pharmacy provides this concentration, ask whether a higher concentration option is available. Using the semaglutide dosage chart in units for your specific concentration eliminates guesswork.
2 mg/mL concentration
At 2 mg/mL, the math produces a number that exceeds a standard insulin syringe.
2.4 mg divided by 2 mg/mL equals 1.20 mL. That would be 120 units.
A standard U-100 insulin syringe only holds 100 units (1 mL). You physically cannot draw 120 units into a single syringe. This means the 2 mg/mL concentration is not practical for the 2.4 mg maintenance dose unless you split the injection across two syringes, drawing 60 units each. This is cumbersome and increases the potential for errors. If you are titrating toward 2.4 mg and your vial is 2 mg/mL, talk to your provider about switching to a higher concentration before reaching the maintenance dose.
1 mg/mL concentration
Some very dilute formulations exist at 1 mg/mL. At this concentration, 2.4 mg would require 2.4 mL, or 240 units. This is completely impractical for a single injection and not a concentration you should use at the 2.4 mg dose level. The 1 mg/mL concentration is really only suitable for the early titration stages at 0.25 mg (25 units) and 0.5 mg (50 units).
10 mg/mL concentration
Higher concentration vials exist at 10 mg/mL, though they are less common.
2.4 mg divided by 10 mg/mL equals 0.24 mL. Multiply by 100, and you get 24 units.
This is a very small volume, which sounds convenient but introduces its own problems. At 24 units, you are working with tiny increments where the difference between 24 and 25 units equals 0.1 mg of semaglutide. Small errors in drawing become proportionally larger. If your syringe markings are not precise, or if you have difficulty reading the small gradations, a 10 mg/mL concentration magnifies those issues. The benefit is a smaller injection volume, which can reduce site discomfort and injection anxiety.
Complete conversion table: every dose at every concentration
You will not stay at 2.4 mg forever without first passing through every earlier dose. And you may need to step back down if side effects become difficult to manage. Having a complete reference table for every dose at every common concentration saves time and prevents errors throughout the entire treatment journey. This table covers the standard semaglutide dosing schedule at each concentration level.
Dose (mg) | 1 mg/mL | 2 mg/mL | 2.5 mg/mL | 3 mg/mL | 5 mg/mL | 10 mg/mL |
|---|---|---|---|---|---|---|
0.25 mg | 25 units | 12.5 units | 10 units | 8.3 units | 5 units | 2.5 units |
0.5 mg | 50 units | 25 units | 20 units | 16.7 units | 10 units | 5 units |
1.0 mg | 100 units | 50 units | 40 units | 33.3 units | 20 units | 10 units |
1.7 mg | 170 units* | 85 units | 68 units | 56.7 units | 34 units | 17 units |
2.4 mg | 240 units* | 120 units* | 96 units | 80 units | 48 units | 24 units |
*Exceeds standard 100-unit syringe capacity. Split injection required or use a higher concentration.
This table should live next to your vial. Print it out or save it on your phone. Before every injection, check the concentration on your label, find the row for your current dose, and confirm the number of units. This takes ten seconds. The cost of skipping this step can be severe, everything from days of nausea to an emergency room visit. Cross-reference this with the semaglutide syringe dosage chart for visual guidance on where to draw on your syringe.
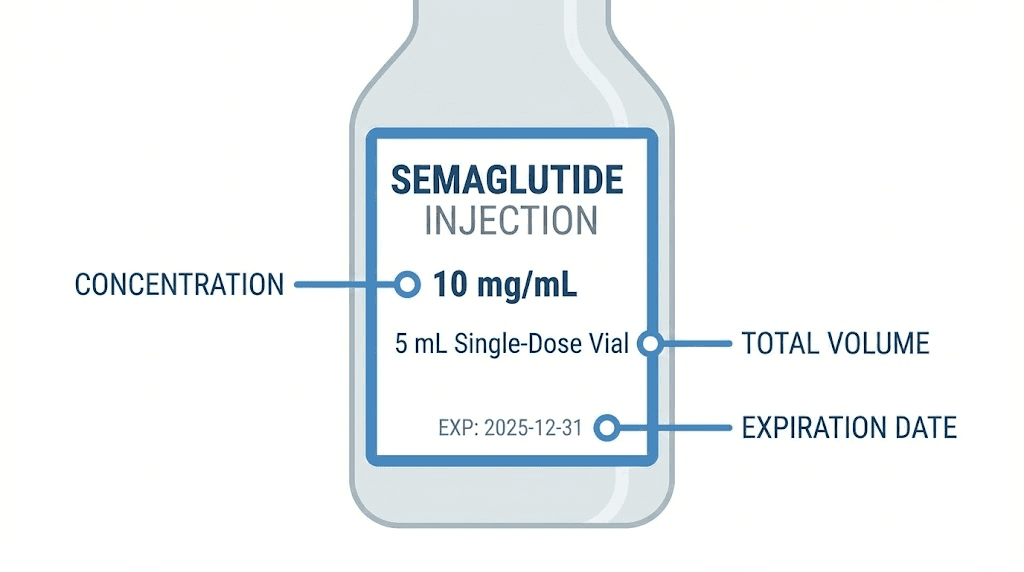
How to read your vial label correctly
The vial label contains every piece of information you need. But only if you know where to look and what matters.
Three numbers on the label determine your dosing. The concentration in mg/mL. The total volume of the vial. And the total amount of semaglutide in the vial. All three are related, but the concentration is the only one you need for your unit calculation.
Finding the concentration
Look for a number expressed as mg/mL. Common examples include 5 mg/mL, 2.5 mg/mL, or 3 mg/mL. This number tells you how many milligrams of semaglutide are dissolved in each milliliter of solution. Some labels write it differently. You might see "5mg/1mL" or "12.5 mg/2.5 mL" or "10mg per 2mL." These all mean the same thing, but you need to divide to find the per-milliliter concentration.
For example, a label that says 12.5 mg/2.5 mL. Divide 12.5 by 2.5, and you get 5 mg/mL. A label that says 10 mg per 2 mL. Divide 10 by 2, and you get 5 mg/mL. Both vials have the same concentration despite the labels looking different. Always reduce to a per-milliliter figure before using the conversion formula. Understanding semaglutide reconstitution helps you verify that the concentration on your vial matches what you expect.
Understanding total vial contents
The total amount tells you how many doses you can get from one vial. A common compounded semaglutide vial contains 5 mg total in 1 mL at 5 mg/mL. At the 2.4 mg maintenance dose, that vial gives you roughly two injections with a tiny amount left over, not enough for a full third dose.
Larger vials exist. A 2.5 mL vial at 5 mg/mL contains 12.5 mg total. That gives you about five weekly doses at 2.4 mg, which covers just over a month of treatment. Planning how many vials you need per month prevents gaps in your dosing schedule. Running out mid-titration and restarting after a break can increase side effects when you resume. The peptide cost calculator can help you plan your supply needs.
Expiration and storage
Your vial label also shows the expiration date and storage requirements. Compounded semaglutide typically needs refrigeration between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius). Leaving it out of the fridge for extended periods can degrade the medication, which means you might be injecting less active semaglutide than you think. If you are wondering about storage specifics, check the detailed guide on how long compounded semaglutide lasts in the fridge and whether compounded semaglutide needs refrigeration.
Step-by-step injection guide for the 2.4 mg dose
Knowing the math is one thing. Executing the injection correctly is another. Here is the complete process from vial to injection for a 2.4 mg dose using a 5 mg/mL concentration (48 units).
What you need
Gather everything before you start. You need your semaglutide vial (check the concentration on the label), an insulin syringe (U-100, typically 0.5 mL or 1 mL capacity), alcohol swabs, and a sharps disposal container. If you are using a 0.5 mL syringe (50 unit capacity), it works perfectly for 48 units at 5 mg/mL. A 1 mL syringe (100 unit capacity) also works but has wider spaces between markings, which can reduce accuracy for smaller doses during titration.
Preparation steps
Remove the vial from the refrigerator and let it sit for 10 to 15 minutes to approach room temperature. Cold injections can cause more discomfort and may affect absorption. Do not heat the vial. Do not shake it. Semaglutide is a peptide, and aggressive agitation can damage the molecular structure. A gentle swirl is fine if you see any separation, though properly compounded semaglutide should appear clear and uniform.
Clean the rubber stopper on the vial with an alcohol swab. Let it air dry completely. This takes about 30 seconds. Skipping this step introduces contamination risk, especially with multi-dose vials that you will be puncturing multiple times over several weeks. Following proper peptide injection protocols reduces infection risk significantly.
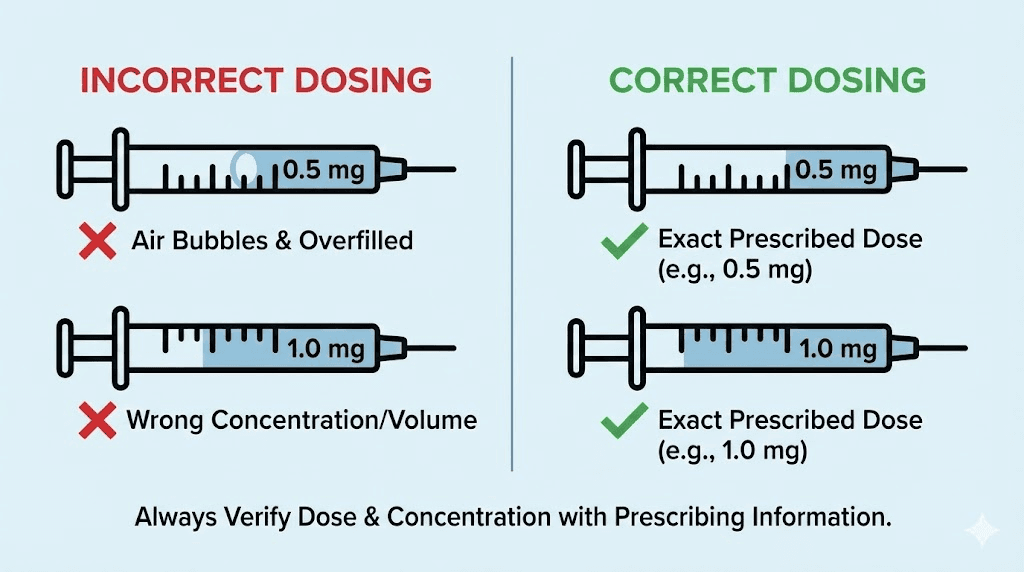
Drawing the correct dose
Pull back the syringe plunger to the 48-unit mark, filling it with air. Insert the needle through the rubber stopper and push the air into the vial. This equalizes pressure and makes drawing the liquid easier. With the needle still in the vial, turn the vial upside down. Slowly pull the plunger back to the 48-unit mark. Check for air bubbles.
Air bubbles matter. Not because a small bubble in a subcutaneous injection is dangerous, but because that bubble displaces medication. A visible air bubble at the 48-unit mark means you actually have less than 48 units of semaglutide in the syringe. Tap the syringe gently to move bubbles to the top near the needle, then push the plunger slightly to expel them. Pull back to 48 units again. Repeat until the syringe reads 48 units of clear, bubble-free liquid.
Double check. Look at the syringe at eye level. The flat edge of the plunger rubber should align exactly with the 48-unit marking. Not the dome of the rubber, not the top edge. The flat bottom edge. This distinction matters more than people realize, and it is a common source of small but consistent dosing errors. For detailed injection techniques, see the GLP-1 injection guide.
Choosing the injection site
Subcutaneous injection sites for semaglutide include the abdomen (at least two inches from the navel), the front of the thigh, and the upper arm. Rotate injection sites each week. Consistently injecting in the same spot can cause lipodystrophy, where the fat tissue under the skin becomes hardened or pitted. This affects absorption and appearance. Detailed guidance on where to inject GLP-1 medications can help you choose the best sites for consistent absorption.
The injection itself
Clean the injection site with an alcohol swab and let it dry. Pinch about an inch of skin between your thumb and forefinger. Insert the needle at a 45 to 90 degree angle (depending on the needle length and your body composition). Push the plunger slowly and steadily until all medication is delivered. Hold the needle in place for about 5 to 10 seconds after the plunger is fully depressed. This allows the medication to distribute and prevents leakback. Withdraw the needle and release the skin pinch. Do not rub the injection site. A small drop of blood or medication at the site is normal and does not indicate a problem.
Common dosing errors and how to avoid them
The FDA has reported that dosing errors with compounded semaglutide are alarmingly common. Some patients have accidentally administered five to twenty times their intended dose. Understanding these errors is the best way to prevent them.
Error 1: confusing units with milligrams
This is the single most dangerous mistake. A provider says "take 2.4 mg" and the patient draws to the 24-unit mark thinking that 24 is close enough to 2.4. But 24 units at 5 mg/mL is 1.2 mg, exactly half the intended dose. At 10 mg/mL, 24 units would actually be 2.4 mg. At 2.5 mg/mL, 24 units would only be 0.6 mg, one quarter of the dose. The same number of units delivers vastly different amounts depending on concentration.
The fix: never assume a relationship between the milligram dose and the unit number. Always calculate using the formula. Always verify against a concentration-specific chart. Tools like the semaglutide dosage calculator exist specifically to catch these errors before they reach the syringe.
Error 2: using the wrong concentration chart
A patient finds a dosing chart online that says 2.4 mg equals 48 units. They draw 48 units. But their vial is 2.5 mg/mL, not 5 mg/mL. At 2.5 mg/mL, 48 units delivers 1.2 mg instead of 2.4 mg. Or worse, someone with a 10 mg/mL vial uses the 5 mg/mL chart and draws 48 units, receiving 4.8 mg, double the intended dose.
The fix: always check YOUR vial concentration before looking at any chart. Charts are concentration-specific. A chart for 5 mg semaglutide does not apply to a 2.5 mg/mL or 10 mg/mL formulation. Match the chart to your vial. Every time.
Error 3: switching vials without recalculating
You have been drawing 48 units from your 5 mg/mL vial for weeks. Your pharmacy sends a refill, but this time the concentration is 3 mg/mL. You draw 48 units out of habit. Instead of 2.4 mg, you just injected 1.44 mg, about 60% of your intended dose. The reverse is even more dangerous. Going from a lower concentration to a higher one without recalculating means accidental overdose.
The fix: treat every new vial as a fresh calculation. Check the label. Run the formula. Verify against the chart. Especially when switching pharmacies or receiving a different batch. If the concentration changed, your units must change too. Document your current concentration and units in a visible spot, a note on the refrigerator, a phone reminder, or a log in your dosage tracking chart.
Error 4: misreading the syringe
Insulin syringes come in different sizes with different graduation markings. A 1 mL (100 unit) syringe typically has markings every 2 units. A 0.5 mL (50 unit) syringe may have markings every 1 unit. A 0.3 mL (30 unit) syringe has the finest markings but cannot hold enough for most 2.4 mg doses. Reading between the lines (literally) on a syringe you are unfamiliar with is a recipe for errors. Some people read the top of the plunger instead of the bottom edge, consistently overdosing by 1 to 2 units.
The fix: use the same syringe type every time. Learn exactly where your dose falls on that specific syringe. Practice drawing water before your first real injection. And always read the plunger at the flat bottom edge, not the dome.
Error 5: no pharmacist counseling
The FDA found that some compounding pharmacies ship semaglutide vials with syringes but provide zero guidance on how to measure or administer the dose. No dosing chart. No instruction sheet. No pharmacist consultation. Patients are left to figure it out on their own, which predictably leads to errors. This is also why comprehensive educational platforms like SeekPeptides exist, to fill the information gap that patients encounter when providers and pharmacies fall short on education.
Why concentration matters more than anything else
If you take one thing from this entire article, let it be this: the concentration on your vial label is the single most important number in your dosing protocol. Everything else, the formula, the charts, the syringe technique, all depends on knowing your concentration correctly.
Consider what happens when concentration is ignored. A person switches from a clinic that uses 5 mg/mL semaglutide to a different provider that uses 2.5 mg/mL. They have been drawing 48 units for months at 5 mg/mL (2.4 mg). They draw 48 units from the new vial without checking. They just received 1.2 mg instead of 2.4 mg. Their appetite suppression fades. They wonder why the medication stopped working. Some people in this situation double their units to compensate, then get a new vial at the original concentration and overdose.
Or the opposite. Someone who has been using 2.5 mg/mL gets a vial at 5 mg/mL. They draw their usual 96 units. They just injected 4.8 mg, double their intended dose. This is not hypothetical. The FDA and poison control centers have documented these exact scenarios playing out repeatedly with GLP-1 medications.
Different compounding pharmacies use different concentrations. The same pharmacy might change concentrations between batches. Your refill might not match your original vial. Never assume. Always check. The five seconds it takes to read the label could save you from days of misery or weeks of subtherapeutic dosing.
Using different syringe types
Not all insulin syringes are created equal, and choosing the right one for your dose and concentration makes a meaningful difference in accuracy.
U-100 syringes (most common)
Standard U-100 insulin syringes measure 100 units per 1 mL. These come in three main sizes:
1 mL (100 unit) syringe: Holds up to 100 units. Markings typically every 2 units. Good for larger doses but less precise for very small amounts. Suitable for the 2.4 mg dose at 5 mg/mL (48 units) and lower concentrations that require higher volumes.
0.5 mL (50 unit) syringe: Holds up to 50 units. Markings typically every 1 unit. More precise than the 1 mL syringe. Works perfectly for the 2.4 mg dose at 5 mg/mL (48 units) and is easier to read accurately. This is the optimal choice for most people at this dose and concentration.
0.3 mL (30 unit) syringe: Holds up to 30 units. Most precise markings. Only suitable for the 2.4 mg dose at 10 mg/mL (24 units) or the early titration doses at higher concentrations. Cannot hold enough for 2.4 mg at 5 mg/mL or lower concentrations.
Choosing the right syringe for your concentration
Match your syringe size to your calculated dose. Ideally, your dose should fall between 25% and 90% of the syringe capacity. Drawing at the extreme low or high end of a syringe reduces accuracy. For 48 units, a 0.5 mL (50 unit) syringe puts you at 96% capacity, close to the top but manageable. For 80 units (3 mg/mL), a 1 mL (100 unit) syringe works best. For 24 units (10 mg/mL), a 0.3 mL (30 unit) syringe gives the finest precision. Understanding peptide dosage calculations helps you choose the right tools every time.
Needle gauge considerations
Most insulin syringes come with 29, 30, or 31 gauge needles. Higher gauge numbers mean thinner needles. For subcutaneous semaglutide injection, a 30 or 31 gauge needle minimizes discomfort. The needle length should be 8mm (5/16 inch) for most body types or 12.7mm (1/2 inch) for those with more subcutaneous tissue. Shorter needles are generally more comfortable but must be long enough to reach the subcutaneous fat layer. Using a peptide injection pen can simplify administration if manual syringes feel challenging.
Comparing Wegovy pens vs compounded vials
The 2.4 mg dose conversion question comes up primarily with compounded semaglutide vials. Brand name Wegovy pens do not require unit calculations because the dose is pre-measured. Understanding the differences helps you navigate your options.
Wegovy pre-filled pens
Wegovy pens come in five dose strengths: 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, and 2.4 mg. Each pen delivers a single, fixed dose. You do not draw medication, calculate units, or choose a syringe. You click the button and the pen delivers exactly 2.4 mg. The concentration inside the pen is engineered by the manufacturer, and the delivery mechanism ensures accuracy.
The obvious advantage is simplicity. No math. No errors. No concentration confusion. The disadvantage is cost and availability. Wegovy pens carry significant expense, and supply shortages have been common. This is what drives many people toward compounded semaglutide alternatives.
Compounded semaglutide vials
Compounded semaglutide comes in multi-dose vials that require manual drawing with a syringe. The cost is typically a fraction of Wegovy. But the tradeoff is that you must understand concentrations, perform calculations, and draw accurately every time. The entire unit conversion topic exists because of compounded vials. If everyone used Wegovy pens, nobody would ever search "how many units is 2.4 mg of semaglutide."
Compounded formulations also vary between pharmacies. Some include additional ingredients like vitamin B12 (cyanocobalamin), methylcobalamin, or glycine. These additions do not change the semaglutide concentration itself (the mg/mL of semaglutide remains the same), but they do mean you should always verify the specific semaglutide concentration listed on your label rather than assuming based on total vial contents. The semaglutide vs tirzepatide comparison breaks down how these two GLP-1 medications differ in approach and dosing.
The full titration journey to 2.4 mg in units
Reaching 2.4 mg takes at least 16 weeks. Each step of the titration requires its own unit calculation. If you use the same concentration throughout (which you should, to avoid confusion), here is your complete weekly injection schedule in units.
At 5 mg/mL (recommended for simplicity)
Weeks 1 through 4 (0.25 mg): Draw to 5 units. This is a tiny volume, just 0.05 mL. Use a 0.3 mL or 0.5 mL syringe for better accuracy at this small amount.
Weeks 5 through 8 (0.5 mg): Draw to 10 units. Still small. Side effects typically begin emerging at this dose, primarily mild nausea in the first day or two after injection.
Weeks 9 through 12 (1.0 mg): Draw to 20 units. This is where most people notice significant appetite suppression. Appetite suppression onset varies, but many report noticeable changes within the first week at this dose.
Weeks 13 through 16 (1.7 mg): Draw to 34 units. A meaningful increase. Gastrointestinal side effects may return briefly as your body adjusts to the higher dose. Some providers extend this phase to six or eight weeks if side effects are significant.
Week 17 onward (2.4 mg): Draw to 48 units. This is your maintenance dose. Most people stay here long-term. The transition from 1.7 mg to 2.4 mg represents a 41% increase, which is the largest percentage jump in the entire titration. Monitor carefully for increased fatigue or constipation during the first two to three weeks at this new level.
What if you cannot tolerate 2.4 mg?
Not everyone reaches the full 2.4 mg maintenance dose. Some people experience persistent nausea, vomiting, or other gastrointestinal effects that do not resolve with time. In these cases, the FDA prescribing information for Wegovy allows staying at 1.7 mg as the maintenance dose.
If you have been at 2.4 mg and need to step back, drop to 1.7 mg (34 units at 5 mg/mL) and remain there for at least four weeks before attempting to increase again. Some people find that splitting the dose, injecting on two different days per week instead of one, helps with tolerability, though this is an off-label approach that should be discussed with your provider. If you are not losing weight on semaglutide, the dose may not be the only factor. Diet, activity level, sleep, and stress all influence outcomes.
For those experiencing persistent problems, understanding what to expect helps manage frustration. The guide on how long semaglutide takes to work provides realistic timelines, and the article on 4 weeks on semaglutide with no weight loss addresses early plateau concerns specifically.
What to do if you accidentally overdose
It happens. Despite all precautions, people sometimes inject more than intended. The response depends on how much over the target dose you went.
Mild overdose (up to 2x intended dose)
If you accidentally injected roughly 4 to 5 mg instead of 2.4 mg, expect amplified side effects. Nausea will likely be more intense. You may experience vomiting, diarrhea, or abdominal cramping. Stay hydrated. Eat small, bland meals. Avoid high-fat foods. These effects should resolve within 48 to 72 hours as the excess medication is processed. Skip your next scheduled dose and resume the following week at your regular 2.4 mg.
Significant overdose (3x or more)
If you believe you received three or more times your intended dose (7.2 mg or higher), contact your healthcare provider immediately or call Poison Control (1-800-222-1222 in the United States). At these levels, you are in territory with very limited clinical data. Severe nausea, persistent vomiting, and dehydration become real risks. You may need IV fluids and anti-nausea medication. Do not attempt to "wait it out" with a severe overdose.
Prevention protocol
Build these habits into every injection:
Check the vial concentration before drawing. Every time.
Calculate units using the formula. Every time.
Verify against a printed conversion chart. Every time.
Read the syringe at eye level before injecting. Every time.
Log your dose, units drawn, and vial concentration in a journal or app. Every time.
Repetitive? Yes. Necessary? Absolutely. The people who get this wrong are almost always the people who stopped checking because they "already knew" their dose. Use the SeekPeptides semaglutide calculator as a verification step. It takes seconds and eliminates math errors.
How 2.4 mg compares to other semaglutide doses in units
Context helps. Where does 2.4 mg sit relative to other common semaglutide doses, and what does that mean in practical syringe terms?
The Ozempic comparison
Ozempic (semaglutide for type 2 diabetes) maxes out at 2.0 mg per week. Wegovy (semaglutide for weight management) goes to 2.4 mg. The difference is 0.4 mg, which at 5 mg/mL concentration translates to 8 units. While Ozempic and GLP-1 medications are related, their dosing targets differ because weight management typically requires higher receptor activation than blood sugar control.
Microdosing context
Some people explore semaglutide at lower doses for maintenance after achieving their weight loss goals. A "microdose" might be 0.25 mg or 0.5 mg, just 5 to 10 units at 5 mg/mL. Compared to those amounts, the 48 units required for a 2.4 mg dose represents a substantial injection volume. The difference illustrates why the titration schedule exists and why you cannot jump from a microdose to the full maintenance dose.
The investigational 7.2 mg dose
Novo Nordisk has tested a 7.2 mg dose in the STEP UP trial, which showed 21% mean weight loss, significantly more than the 14.9% at 2.4 mg. At 5 mg/mL, 7.2 mg would require 144 units, more than a full 1 mL syringe can hold. This underscores why higher concentrations will become increasingly important as dosing paradigms evolve. If higher doses become standard, understanding concentration-based unit calculations will be even more critical.
For those considering their options between different GLP-1 medications, understanding dosing mechanics for each medication is essential. The tirzepatide dosing in units guide covers similar conversions for the other major GLP-1 medication.
Supporting your 2.4 mg protocol with diet and lifestyle
Getting the injection right is only part of the equation. At 2.4 mg, semaglutide provides powerful appetite suppression and metabolic benefits. But those benefits work best when paired with appropriate nutrition and activity.
Nutrition at the 2.4 mg dose
At full maintenance dose, appetite suppression is strong. Many people struggle to eat enough rather than eating too much. This creates a risk of inadequate protein intake, which accelerates muscle loss during weight loss. Aim for 0.8 to 1.0 grams of protein per pound of lean body mass. Prioritize protein at every meal.
The appetite suppression effect also means that the quality of every bite matters more. When you are only eating 1,200 to 1,500 calories per day, those calories need to deliver maximum nutrition. Lean proteins, vegetables, whole grains, healthy fats. Minimize empty calories from processed foods and sugar. The complete list of foods to eat while on semaglutide breaks down optimal choices, and the semaglutide diet plan provides a structured meal framework.
Hydration becomes critical
Semaglutide slows gastric emptying, which means food and liquid sit in your stomach longer. This can make people forget to drink enough water because they do not feel thirsty. Dehydration compounds the constipation that many experience at the 2.4 mg dose. Aim for at least 64 ounces of water daily, more if you exercise. Electrolyte supplements can help if plain water causes bloating or nausea.
Exercise considerations
Resistance training is particularly important during semaglutide-assisted weight loss. Studies show that approximately 30 to 40% of weight lost with GLP-1 medications comes from lean mass (muscle) rather than fat. Strength training helps preserve that muscle, which maintains metabolic rate, functional strength, and long-term weight maintenance.
Cardio remains important for cardiovascular health, but do not rely on it as the primary exercise modality. The reduced caloric intake at full maintenance dose may limit your energy for intensive workouts. Listen to your body. Some people find that exercising before their injection day (when appetite suppression is at its lowest) gives them more energy for training. Learning about how fast semaglutide works helps set realistic expectations for when you will notice both appetite changes and weight loss.
Supplements to consider
At the 2.4 mg dose, several supplements may support your protocol. A high-quality multivitamin covers potential nutrient gaps from reduced food intake. Vitamin B12 supports energy levels and is commonly combined with semaglutide in compounded formulations. Fiber supplements help with the constipation that frequently accompanies GLP-1 treatment. Protein powder fills the gap when appetite suppression makes eating full meals difficult. The article on whether semaglutide gives you energy addresses the relationship between dosing, nutrition, and energy levels in detail.
When to talk to your provider about your dose
The unit conversion math is straightforward once you understand it. But the clinical decision about whether 2.4 mg is the right dose for you requires medical judgment. Here are the situations where you should bring questions to your provider rather than adjusting on your own.
Persistent side effects beyond week 20
Some gastrointestinal effects are expected when you first reach 2.4 mg. Nausea, reduced appetite, occasional diarrhea. These should improve within two to four weeks. If you are still experiencing significant symptoms after a month at 2.4 mg, that is a conversation worth having. Your provider might recommend stepping back to 1.7 mg or adjusting injection timing. Detailed guidance on managing semaglutide-related symptoms is available if you need to modify your protocol.
Weight loss plateau
You have been at 2.4 mg for three months and the scale has stopped moving. Before asking for a higher dose, examine other factors. Sleep quality, stress levels, caloric intake, protein consumption, exercise consistency. Semaglutide amplifies good habits. It does not replace them. The article on why some people do not lose weight on semaglutide covers the ten most common plateau causes and their solutions.
Planning to discontinue
If you are considering stopping semaglutide after reaching your goal weight, discuss a tapering strategy with your provider. Abrupt discontinuation from 2.4 mg can lead to rapid weight regain and a rebound in appetite. A gradual reduction, stepping down through the titration doses in reverse, may ease the transition. The guide on how long to stay on semaglutide addresses duration of treatment and discontinuation planning.
Switching medications
Some people consider switching from semaglutide to tirzepatide or other GLP-1 medications. These switches involve different dosing calculations, different titration schedules, and different unit conversions. The semaglutide to tirzepatide conversion chart provides equivalent dosing guidance for those making this transition.
Reconstitution and concentration: what you need to know
Some researchers work with lyophilized (freeze-dried) semaglutide that requires reconstitution before use. In this scenario, YOU determine the concentration based on how much bacteriostatic water you add to the powder.
How reconstitution determines concentration
If you have a 10 mg vial of lyophilized semaglutide and add 2 mL of bacteriostatic water, you create a 5 mg/mL solution (10 mg divided by 2 mL). Add 4 mL instead, and you get 2.5 mg/mL. Add 1 mL, and you get 10 mg/mL. The amount of semaglutide does not change. Only the concentration changes based on the volume of water you add.
For a 2.4 mg dose:
10 mg reconstituted with 2 mL (5 mg/mL): draw 48 units
10 mg reconstituted with 4 mL (2.5 mg/mL): draw 96 units
10 mg reconstituted with 1 mL (10 mg/mL): draw 24 units
The peptide reconstitution calculator takes the guesswork out of this process. Enter your peptide amount and desired concentration, and it tells you exactly how much water to add. For a step-by-step walkthrough, the guide on reconstituting 5 mg semaglutide covers the full process with visual instructions.
Why 5 mg/mL is the sweet spot
At 5 mg/mL, the 2.4 mg dose requires 48 units. This volume is large enough to measure accurately on a standard insulin syringe and small enough to inject comfortably. Lower concentrations push you toward awkwardly large volumes. Higher concentrations make tiny measurement errors more impactful. Unless you have a specific reason to choose differently, reconstituting to 5 mg/mL provides the best balance of accuracy and comfort for the 2.4 mg maintenance dose. This matches the most common concentration used in compounded semaglutide preparations.
Handling and storage after reconstitution
Once reconstituted, semaglutide must be refrigerated. Most compounded or reconstituted semaglutide remains stable for four to six weeks when stored properly at 2 to 8 degrees Celsius. Write the reconstitution date on the vial. Discard any remaining solution after the recommended period, even if there is medication left. Using degraded semaglutide means you are injecting less active compound than your calculation assumes, leading to subtherapeutic dosing despite drawing the "correct" number of units. The storage guide on expired semaglutide explains what happens to the medication over time.
Quick reference card for the 2.4 mg dose
Save this reference for your injection days. It summarizes everything you need for accurate dosing at 2.4 mg.
Vial Concentration | Units to Draw | Volume (mL) | Recommended Syringe |
|---|---|---|---|
2.5 mg/mL | 96 units | 0.96 mL | 1 mL (100 unit) |
3 mg/mL | 80 units | 0.80 mL | 1 mL (100 unit) |
5 mg/mL | 48 units | 0.48 mL | 0.5 mL (50 unit) |
10 mg/mL | 24 units | 0.24 mL | 0.3 mL (30 unit) |
Pre-injection checklist:
Read vial label for concentration (mg/mL)
Calculate units: 2.4 divided by concentration times 100
Verify against the table above
Draw to the correct mark on your syringe
Read at eye level, flat edge of plunger
Log concentration, units, date, and injection site
For researchers who want automated verification, the SeekPeptides semaglutide dosage calculator handles all of this instantly. Input your concentration and target dose. It outputs the exact number of units. No math required.
Understanding the relationship between mg, mL, and units
The confusion around semaglutide dosing comes from three different measurement systems colliding. Each measures something different, and they only relate to each other through concentration. Understanding these fundamentals once eliminates the confusion forever.
Milligrams (mg) measure the amount of drug
When your provider prescribes 2.4 mg, they are specifying how much semaglutide you should receive by weight. One milligram is one thousandth of a gram. The 2.4 mg dose means 2.4 thousandths of a gram of the semaglutide molecule. This is an incredibly small amount. For perspective, a single grain of salt weighs about 60 mg, making your semaglutide dose roughly one twenty-fifth of a salt grain by weight.
Milliliters (mL) measure the volume of liquid
The semaglutide is dissolved in a liquid solution. Milliliters tell you how much liquid you need to draw to get your prescribed milligram amount. One milliliter is about twenty drops from an eyedropper. The volume you draw depends on how concentrated the solution is. More concentrated means less liquid needed for the same amount of drug.
Units measure markings on an insulin syringe
Units are a volume measurement specific to insulin syringes. On a U-100 syringe, 100 units equals 1 milliliter. That is all. Units do not inherently correspond to any specific amount of medication. 48 units means 0.48 mL of whatever liquid is in your syringe. The amount of semaglutide in that 0.48 mL depends entirely on the concentration.
Here is the relationship chain: Your provider prescribes mg. Your vial has a concentration in mg/mL. You convert to mL. Your syringe reads in units (where 100 units = 1 mL). The concentration is the bridge connecting what you need (mg) to what you measure (units). Without knowing the concentration, the other two numbers are meaningless in relation to each other. The 20 units semaglutide conversion guide demonstrates this same principle for another common dose level, and the 40 units to mg conversion extends the examples further.
Storing your syringe safety log
Keeping a simple injection log prevents errors, tracks your progress, and provides useful information if you need to discuss your protocol with a provider.
What to track each injection
Record these seven data points after every injection:
Date
Time
Dose (mg): 2.4 mg
Concentration (mg/mL): from your vial label
Units drawn: from your syringe
Injection site: abdomen left, abdomen right, thigh left, thigh right, arm left, arm right
Notes: any side effects, missed air bubbles, discomfort, etc.
This log takes 30 seconds to update. Over months, it becomes an invaluable record. You can see patterns: which injection sites cause less discomfort, whether side effects correlate with specific times of day, whether you have been rotating sites properly, and exactly how many doses remain in your current vial.
Tracking vial usage
A 5 mg/mL vial containing 2.5 mL holds 12.5 mg total. At 2.4 mg per week, that provides 5 full doses with 0.5 mg remaining, not enough for a sixth dose. Mark on your calendar when to order a refill. Running out mid-week means a skipped dose, which is not ideal but not dangerous. Resume at your regular 2.4 mg dose at the next scheduled time. Do not double up to compensate for a missed dose. Detailed information on timing your semaglutide doses helps you establish a consistent weekly schedule.
Combining semaglutide with other treatments
Many people at the 2.4 mg dose use other medications or supplements alongside their semaglutide protocol. Some combinations are straightforward. Others require careful consideration.
Semaglutide with B12
Vitamin B12 is commonly added to compounded semaglutide formulations or taken as a separate supplement. The rationale is that reduced food intake at the 2.4 mg dose can lead to B12 deficiency over time. The semaglutide with B12 guide covers the evidence and practical considerations for this combination.
Semaglutide with phentermine
Some providers prescribe phentermine alongside semaglutide for additional appetite suppression or to counter the fatigue that some people experience. This combination is off-label and requires medical supervision. The phentermine and semaglutide combination guide examines the research and safety considerations.
Alcohol on semaglutide
Semaglutide slows gastric emptying and alters how your body processes alcohol. Many people report dramatically increased sensitivity to alcohol at the 2.4 mg dose. One drink might feel like three. The drinking on semaglutide guide provides practical guidelines for those who choose to consume alcohol during treatment.
Frequently asked questions
Is 2.4 mg the highest dose of semaglutide available?
For FDA-approved formulations, 2.4 mg is the maximum weekly dose for weight management (Wegovy). Ozempic for diabetes maxes at 2.0 mg. Novo Nordisk has tested a 7.2 mg dose in clinical trials (STEP UP), showing 21% mean weight loss compared to 14.9% at 2.4 mg. That higher dose is not yet approved for standard use. For current protocols, 2.4 mg remains the target maintenance dose.
Can I just draw to the 2.4 mark on my syringe for 2.4 mg?
No. The markings on an insulin syringe indicate units of volume, not milligrams of medication. Drawing to the 24-unit mark would give you a different amount depending on your vial concentration. At 5 mg/mL, 24 units would deliver only 1.2 mg, half the intended dose. You must use the conversion formula: Units = (mg / concentration) x 100.
What happens if I skip a dose at 2.4 mg?
If you miss your weekly injection, take it as soon as possible within five days of the missed dose. If more than five days have passed, skip the missed dose and resume your regular schedule at the next planned injection day. Do not inject two doses to make up for a missed one. A single missed dose at 2.4 mg will not significantly impact your overall progress. Semaglutide has a long half-life of approximately one week, so some medication remains active even when you miss a dose.
Do I need to change my syringe size when I reach 2.4 mg?
It depends on your concentration and what syringe you have been using. At 5 mg/mL, 48 units fits in both a 0.5 mL (50 unit) and 1 mL (100 unit) syringe. If you were using a 0.3 mL (30 unit) syringe for the early titration doses, you will need to switch to a larger syringe by the time you reach 2.4 mg at most concentrations. The only exception is the 10 mg/mL concentration, where 2.4 mg requires just 24 units.
Why does my pharmacy keep changing the concentration?
Compounding pharmacies may adjust concentrations based on raw material availability, patient demand, or regulatory requirements. Some pharmacies standardized on one concentration and later switched to another. This is why you should never assume your new vial has the same concentration as the previous one. Always check the label and recalculate your units before every first injection from a new vial.
Can I mix my own semaglutide to a specific concentration?
If you are working with lyophilized semaglutide, you determine the concentration through reconstitution. Adding more water creates a lower concentration (more units needed per dose). Adding less water creates a higher concentration (fewer units needed). The reconstitution calculator tells you exactly how much water to add for your desired concentration.
Is 48 units at 5 mg/mL the most common way to get 2.4 mg?
Yes. The 5 mg/mL concentration is the most widely produced compounded semaglutide formulation, and 48 units is what most people at the maintenance dose draw each week. This combination offers the best balance of accuracy, injection comfort, and syringe compatibility.
Should I switch to Wegovy pens instead of calculating units?
Wegovy pens eliminate the need for unit calculations entirely. Each pen delivers a pre-measured dose. If unit conversion causes you anxiety or you have experienced dosing errors, Wegovy pens offer a simpler alternative. The tradeoff is typically higher cost and potential availability issues. Discuss both options with your provider to determine what works best for your situation.
External resources
For researchers serious about optimizing their semaglutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay accurate, your syringes stay precise, and your protocols stay consistent.