Feb 13, 2026

Before you draw 10 units into that syringe, stop. The number on the barrel means nothing without one critical piece of information. Your vial concentration. Get it wrong and you could inject five times your prescribed dose. Or one fifth. Both scenarios happen more often than anyone in the telehealth industry wants to admit, and the FDA has documented hospitalizations from exactly this type of error.
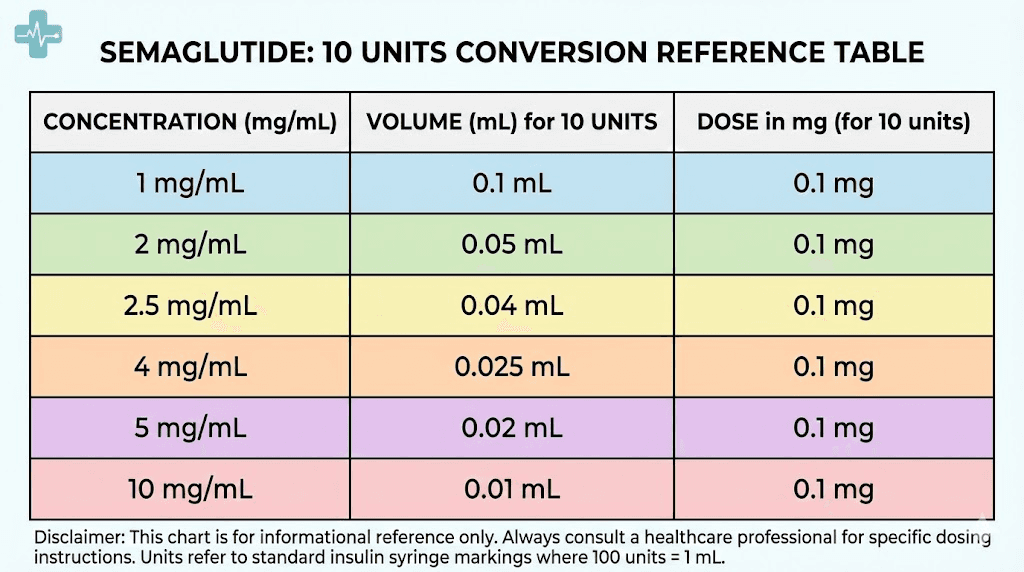
Here is the short answer. Ten units of semaglutide on an insulin syringe equals 0.1 mL of liquid. That is always true regardless of concentration. But 0.1 mL from a 5 mg/mL vial contains 0.5 mg of semaglutide. The same 0.1 mL from a 2.5 mg/mL vial contains only 0.25 mg. And from a 10 mg/mL vial, those 10 units deliver a full 1.0 mg. Same syringe reading. Wildly different doses.
This distinction is not academic. Poison control centers have seen a 1,500% increase in semaglutide-related calls since 2019, with the majority involving patients who mistakenly drew and administered five to twenty times their prescribed dose from multi-dose vials. The problem is almost always the same. Someone looked up a conversion chart online, applied it to a different concentration than the one they had, and injected a dose that sent them to the emergency room.
This guide exists to prevent that from happening to you. We cover every common compounded semaglutide concentration, provide exact conversion tables for each, explain the math behind the calculations so you can verify any number yourself, and walk through the most dangerous mistakes people make with semaglutide unit conversions. SeekPeptides built this resource because accurate dosing is the foundation of safe and effective GLP-1 therapy, and too many existing guides skip the details that actually keep people safe.
Why 10 units does not have a single answer
The confusion starts with a fundamental misunderstanding about what "units" mean on an insulin syringe. Units on a syringe measure volume, not drug quantity. One hundred units equals one milliliter. That is it. The syringe has no idea what medication is inside it, what concentration that medication has, or how many milligrams you are actually injecting.
Think of it like measuring cups in a kitchen. A measuring cup holds 250 mL whether you fill it with water or olive oil. The volume is identical. But the weight differs because the density differs. Semaglutide concentrations work the same way. The syringe measures how much liquid you draw. The concentration determines how much actual drug is dissolved in that liquid.
This is why you cannot simply Google "10 units of semaglutide in mg" and expect a universal answer. The answer depends entirely on your specific vial. And compounding pharmacies use at least six different concentrations for semaglutide, sometimes more.
The concentrations you will encounter
Compounded semaglutide arrives in multi-dose vials with the concentration printed on the label. The most common concentrations from compounding pharmacies include 1 mg/mL, 2 mg/mL, 2.5 mg/mL, 3 mg/mL, 5 mg/mL, and 10 mg/mL. Some pharmacies also compound at 4 mg/mL or custom concentrations based on provider specifications.
The 5 mg/mL concentration is the most widely used across telehealth platforms. But that does not mean yours is 5 mg/mL. If your provider uses a different compounding pharmacy, you might receive a 2.5 mg/mL vial or a 10 mg/mL vial. The compounded semaglutide landscape varies dramatically between providers and pharmacies.
Before doing any math, find your concentration. It is printed on the vial label, usually formatted as "X mg/mL" or "Xmg/1mL." If you cannot find it, call your pharmacy before injecting anything. This is not optional. This is the single most important safety step in the entire process.
Why brand-name semaglutide does not use units
If you have used Ozempic or Wegovy, you never dealt with unit conversions. Those products come in pre-filled pens with dose selectors calibrated in milligrams. You dial your dose, click, and inject. The pen handles all the math internally.
Compounded semaglutide is different. It arrives in a vial. You draw your dose with an insulin syringe. The syringe shows units. Your prescription says milligrams. Converting between them requires knowing your concentration. This disconnect is where the majority of dosing errors originate, and it is specific to compounded formulations that use multi-dose vials rather than pre-calibrated delivery systems.
The universal conversion formula
Every conversion in this entire guide comes from one formula. Learn it once and you can calculate any dose at any concentration forever.
Units = (Dose in mg / Concentration in mg per mL) x 100
That is it. Three numbers. One division. One multiplication. The result tells you exactly how many units to draw on your insulin syringe.
Let us work through the 10-unit question using this formula in reverse. If you already drew 10 units, how many milligrams did you get?
Dose in mg = (Units / 100) x Concentration in mg per mL
For a 5 mg/mL vial: (10 / 100) x 5 = 0.5 mg
For a 2.5 mg/mL vial: (10 / 100) x 2.5 = 0.25 mg
For a 10 mg/mL vial: (10 / 100) x 10 = 1.0 mg
Same 10 units. Three completely different doses. The difference between 0.25 mg and 1.0 mg is fourfold, which means using the wrong chart could quadruple your intended dose. Or quarter it.
Why 100 is in the formula
The number 100 appears because standard insulin syringes contain 100 units per milliliter. When you draw to the "10" mark on a 100-unit syringe, you have drawn 0.1 mL of liquid. When you draw to the "50" mark, you have drawn 0.5 mL. The relationship is always units divided by 100 equals milliliters.
Some syringes hold only 50 units total (0.5 mL) or 30 units total (0.3 mL). The individual unit markings still represent the same volume. Ten units on a 50-unit syringe equals the same 0.1 mL as 10 units on a 100-unit syringe. The formula works identically regardless of syringe capacity.
Understanding this relationship between syringe units and actual volume is essential for accurate dosing. If you use our semaglutide dosage calculator, it handles this conversion automatically based on your specific vial concentration.
Complete conversion tables: 10 units at every concentration
Here is what 10 units delivers at each common compounded semaglutide concentration. Bookmark this section. Reference it every time you prepare an injection until the conversion becomes second nature.
Quick reference: 10 units across all concentrations
Vial concentration | Volume drawn (10 units) | Semaglutide dose | Typical protocol phase |
|---|---|---|---|
1 mg/mL | 0.1 mL | 0.1 mg | Below standard starting dose |
2 mg/mL | 0.1 mL | 0.2 mg | Below standard starting dose |
2.5 mg/mL | 0.1 mL | 0.25 mg | Standard starting dose (weeks 1-4) |
3 mg/mL | 0.1 mL | 0.3 mg | Slightly above starting dose |
5 mg/mL | 0.1 mL | 0.5 mg | Second escalation dose (weeks 5-8) |
10 mg/mL | 0.1 mL | 1.0 mg | Mid-range therapeutic dose |
Notice the pattern. The dose in milligrams always equals the concentration divided by 10 when you draw 10 units. This makes mental math simple. Whatever your concentration is, move the decimal one place to the left, and that is your milligram dose for 10 units.
A 5 mg/mL vial at 10 units gives 0.5 mg. A 2.5 mg/mL vial at 10 units gives 0.25 mg. Quick. Clean. No calculator needed for this specific amount.
Full conversion charts by concentration
While you came here for the 10-unit answer, you will need the full chart for your entire dosing protocol. Semaglutide doses escalate over months, and each increase means drawing a different number of units. These tables cover every standard dose at the most common concentrations.
1 mg/mL concentration
This is the most dilute common concentration. You will draw larger volumes for each dose, which can be more precise for very low starting doses but requires larger syringes at higher doses.
Prescribed dose | Volume | Units on syringe |
|---|---|---|
0.25 mg | 0.25 mL | 25 units |
0.5 mg | 0.50 mL | 50 units |
1.0 mg | 1.00 mL | 100 units (full syringe) |
1.7 mg | 1.70 mL | Exceeds standard syringe |
2.4 mg | 2.40 mL | Exceeds standard syringe |
At 1 mg/mL, doses above 1.0 mg exceed the capacity of a standard 100-unit insulin syringe. This concentration is generally only practical for the early dose escalation phases. Higher therapeutic doses require a more concentrated formulation or multiple injections per session. Most providers who use this concentration transition patients to higher-concentration vials as doses increase. Check your semaglutide dosage chart for your specific protocol.
2.5 mg/mL concentration
This is one of the most popular concentrations, especially from pharmacies that add B12 (cyanocobalamin) to the formulation. The semaglutide with B12 combination frequently uses this concentration.
Prescribed dose | Volume | Units on syringe |
|---|---|---|
0.25 mg | 0.10 mL | 10 units |
0.5 mg | 0.20 mL | 20 units |
1.0 mg | 0.40 mL | 40 units |
1.7 mg | 0.68 mL | 68 units |
2.4 mg | 0.96 mL | 96 units |
At 2.5 mg/mL, every standard dose fits within a 100-unit syringe. The starting dose of 0.25 mg equals exactly 10 units, making this the concentration where "10 units" directly corresponds to the standard week-one dose. If your pharmacy uses this concentration, 10 units is your starting point. Clean and simple.
The semaglutide B12 dosage chart follows these same conversions since the B12 addition does not change the semaglutide concentration on the label. The concentration listed on your vial refers specifically to the semaglutide content.
5 mg/mL concentration
The most commonly prescribed concentration across major telehealth platforms. Compact volumes mean smaller injections, which most patients prefer.
Prescribed dose | Volume | Units on syringe |
|---|---|---|
0.25 mg | 0.05 mL | 5 units |
0.5 mg | 0.10 mL | 10 units |
1.0 mg | 0.20 mL | 20 units |
1.7 mg | 0.34 mL | 34 units |
2.4 mg | 0.48 mL | 48 units |
At 5 mg/mL, 10 units equals 0.5 mg, which is the second dose level in the standard escalation schedule. If you are on weeks 5 through 8 of a typical protocol, this is likely your dose. The 5 mg/mL semaglutide dosage chart covers the complete escalation schedule at this concentration.
Notice how compact the volumes are. Even the maximum dose of 2.4 mg requires only 48 units, less than half a syringe. The smaller injection volumes generally mean less discomfort at the injection site and faster absorption. This is why 5 mg/mL has become the industry standard for compounded semaglutide.
10 mg/mL concentration
Higher concentration vials are less common but increasingly used by pharmacies that want to minimize injection volumes, especially at higher doses.
Prescribed dose | Volume | Units on syringe |
|---|---|---|
0.25 mg | 0.025 mL | 2.5 units |
0.5 mg | 0.05 mL | 5 units |
1.0 mg | 0.10 mL | 10 units |
1.7 mg | 0.17 mL | 17 units |
2.4 mg | 0.24 mL | 24 units |
At 10 mg/mL, 10 units delivers a full 1.0 mg, which is a mid-range therapeutic dose in the standard escalation schedule. The starting dose of 0.25 mg requires only 2.5 units at this concentration, which is extremely difficult to measure accurately on most insulin syringes. The unit markings on a standard 100-unit syringe are spaced 1 unit apart, making 2.5 units a visual estimate between markings.
This precision challenge is the main drawback of high-concentration formulations for early dose levels. If you are starting semaglutide for the first time and your vial is 10 mg/mL, discuss with your provider whether a lower concentration might be more appropriate for the initial weeks. Accurate low-dose measurement matters because the titration phase is specifically designed to minimize side effects like fatigue, nausea, and gastrointestinal discomfort that are more likely when starting doses are too high.
The standard semaglutide dose escalation schedule
Understanding where 10 units falls in your overall protocol requires context about how semaglutide dosing works over time. The medication is not started at full strength. Instead, you follow a gradual escalation designed to let your body adjust and minimize side effects.
The Wegovy escalation model
Most compounded semaglutide protocols mirror the FDA-approved Wegovy escalation schedule, even though compounded versions are not FDA-approved themselves. The schedule looks like this.
Weeks 1-4: 0.25 mg once weekly. This is the acclimation phase. Your body adjusts to the medication. Weight loss is minimal. The goal is tolerability, not results.
Weeks 5-8: 0.5 mg once weekly. Appetite suppression becomes more noticeable. Most people start feeling reduced food interest during this phase. Some experience the first real weight loss.
Weeks 9-12: 1.0 mg once weekly. The therapeutic range begins. Significant appetite reduction for most users. Monthly weight loss of 4-8 pounds is typical.
Weeks 13-16: 1.7 mg once weekly. Approaching maximum dose. Strong appetite suppression. This is where many users find their optimal balance between effectiveness and side effect management.
Week 17 and beyond: 2.4 mg once weekly. Maximum recommended dose. Not everyone needs to reach this level. Some users achieve their goals at 1.0 or 1.7 mg and stay there.
Each escalation step requires a minimum of four weeks before moving up. Rushing the schedule increases the risk of nausea, vomiting, and other gastrointestinal side effects. If you experience persistent side effects at any dose, your provider may extend the time at that level before escalating. Understanding how fast semaglutide works helps set realistic expectations for each phase.
Where 10 units fits by concentration
Now you can see exactly where 10 units places you in the escalation schedule depending on your vial.
With a 2.5 mg/mL vial: 10 units = 0.25 mg = starting dose (weeks 1-4). You are at the very beginning of treatment.
With a 5 mg/mL vial: 10 units = 0.5 mg = second dose level (weeks 5-8). You have completed the initial acclimation and are stepping up.
With a 10 mg/mL vial: 10 units = 1.0 mg = third dose level (weeks 9-12). You are in the therapeutic range where significant results begin.
If someone tells you "I take 10 units of semaglutide" without mentioning their concentration, they could be on a starting dose, a mid-level dose, or a full therapeutic dose. The number is meaningless without context. This is why forums, Reddit threads, and social media discussions about semaglutide dosing can be confusing and potentially dangerous when people share unit numbers without specifying concentrations.
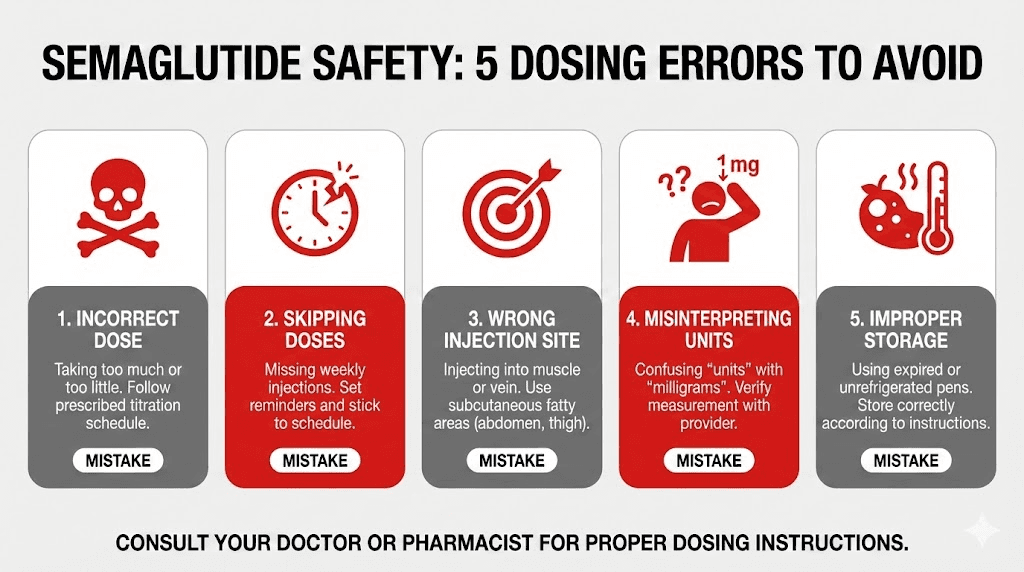
Real-world dosing errors and how to avoid them
This is not theoretical. The FDA has issued warnings about compounded semaglutide dosing errors. Poison control centers have documented a 1,500% increase in semaglutide-related calls since 2019. Most of these cases involve concentration confusion with compounded formulations.
The five most common mistakes
Mistake one: using a chart for the wrong concentration. This is the most dangerous and most frequent error. Someone receives a 2.5 mg/mL vial but follows a conversion chart designed for 5 mg/mL. They draw 20 units thinking they are getting 0.5 mg, but they actually get 0.5 mg from a 2.5 mg/mL vial when they only needed 10 units for that dose. The reverse is worse. If they have a 5 mg/mL vial and follow a 2.5 mg/mL chart, they draw 40 units thinking they need it for 1.0 mg, when 40 units from a 5 mg/mL vial actually delivers 2.0 mg, double what they intended.
The fix is simple. Always verify your vial concentration before consulting any chart. Match the chart to your exact concentration. If the chart does not specify a concentration, do not use it.
Mistake two: confusing units with milligrams. Units and milligrams are different measurements. A prescription for "0.5 mg" does not mean "0.5 units" on the syringe. Depending on concentration, 0.5 mg could be anywhere from 5 units to 50 units. If someone sees "0.5" on their prescription and draws to the 0.5 mark on a unit syringe, they have injected 0.5 units (0.005 mL), which is an unmeasurably tiny amount that would have zero therapeutic effect. The semaglutide dosage chart in mL clarifies these volume relationships.
Mistake three: switching pharmacies without checking concentrations. Your first pharmacy may compound at 5 mg/mL. When you refill, a different pharmacy might compound at 2.5 mg/mL or 10 mg/mL. If you continue drawing the same number of units, your dose has suddenly halved or doubled. Every time you receive a new vial, especially from a different source, check the concentration label before drawing your first dose.
Mistake four: relying on verbal instructions without written verification. A provider tells you "draw 10 units." You draw 10 units. But the provider was thinking of one concentration and your pharmacy sent a different one.
This happens frequently in telehealth environments where the prescribing provider and the dispensing pharmacy are separate entities. Always verify the math yourself. The formula is simple: dose in mg divided by concentration in mg/mL times 100 equals units.
Mistake five: ignoring partial unit markings. Some doses require drawing to marks between the printed lines on an insulin syringe. At a 10 mg/mL concentration, the starting dose of 0.25 mg requires 2.5 units, which falls between the 2 and 3 unit marks. Estimating this visually introduces imprecision. If your protocol requires fractional units consistently, discuss with your provider whether a different concentration or syringe type might improve accuracy. Our peptide calculator helps verify exact volumes for any concentration to eliminate guesswork.
What happens when you overdose semaglutide
Overdosing semaglutide is not immediately life-threatening in most cases, but it can cause serious complications that require medical attention. The symptoms escalate based on how far above the intended dose you go.
Mild overdose (1.5 to 2 times intended dose). Severe nausea, vomiting, diarrhea, and abdominal cramping. These symptoms can last 24-72 hours because semaglutide has a half-life of approximately one week, meaning the excess drug stays in your system for days. You cannot "wait it out" in a few hours.
Moderate overdose (2 to 5 times intended dose). Everything above plus dehydration from persistent vomiting and diarrhea, headaches, migraines, fainting, dizziness, and inability to keep food or liquids down. Dehydration can become dangerous quickly, potentially leading to acute kidney injury. Seek medical attention if you cannot maintain hydration.
Severe overdose (5 to 20 times intended dose). All of the above plus risk of acute pancreatitis (severe abdominal pain radiating to the back), gallbladder complications, and hospitalization. The FDA has documented cases where patients administered 5 to 20 times their prescribed dose from compounded multi-dose vials. These cases required emergency medical intervention.
If you suspect you have taken too much semaglutide, contact your healthcare provider immediately or call Poison Control at 1-800-222-1222. Do not wait for symptoms to appear. Early intervention can prevent dehydration and more serious complications.
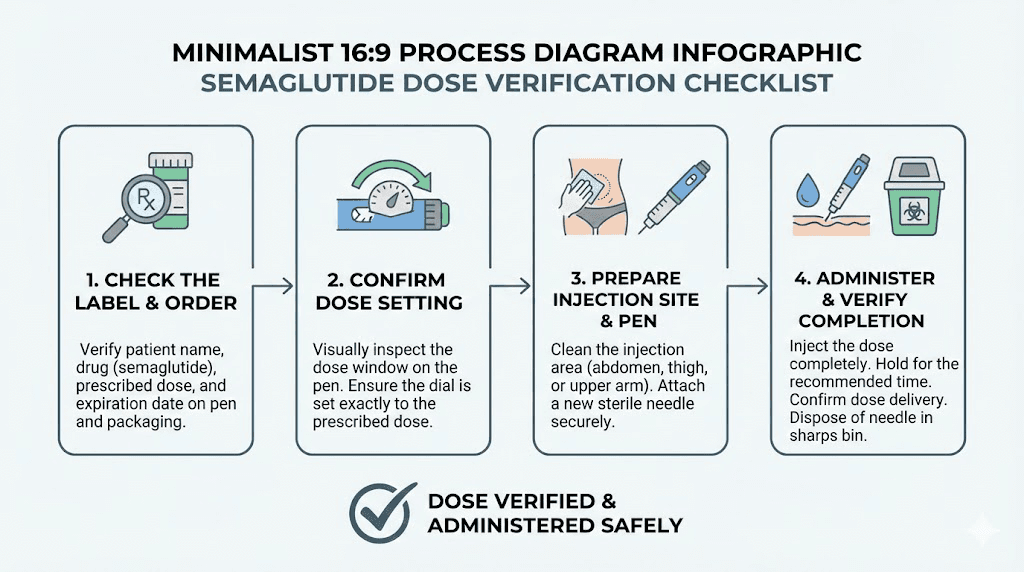
How to verify your dose every single time
Develop a pre-injection verification routine that takes thirty seconds and could save you from a dosing error. Do this before every injection until it becomes automatic muscle memory.
The four-step verification process
Step one: read the vial label. Find the concentration printed on the label. Say it out loud. "This is a five milligram per milliliter vial." Verbal confirmation engages a different cognitive process than visual scanning alone. It forces conscious acknowledgment rather than assumption.
Step two: confirm your prescribed dose. Check your provider instructions, patient portal, or written documentation. Your prescribed dose is in milligrams. "My dose is zero point five milligrams."
Step three: calculate or reference your units. Use the formula: (0.5 mg / 5 mg per mL) x 100 = 10 units. Or reference the chart specific to your concentration. Verify that the chart matches your vial concentration.
Step four: draw and double-check. Draw the calculated number of units into your syringe. Hold the syringe at eye level. Confirm the meniscus (the bottom curve of the liquid) aligns with your target mark. Remove any air bubbles by tapping the syringe and gently pushing the plunger until a tiny drop appears at the needle tip.
This process takes less time to perform than it does to read about. Once habituated, it happens in seconds. But it eliminates the most common category of dosing errors entirely.
When to use a calculator versus a chart
Charts are faster for standard doses at common concentrations. The semaglutide conversion chart covers every standard dose at every common concentration. Bookmark it. Print it. Keep it next to your supplies.
Calculators are better when you have an unusual concentration, a non-standard dose, or any situation where a pre-made chart does not cover your specific scenario. The SeekPeptides semaglutide dosage calculator accepts any concentration and any dose, computing the exact units and volume instantly. Use it whenever you are unsure, whenever you switch pharmacies, or whenever your dose changes.
Both approaches are valid. Using both together, calculating manually and then verifying against a chart or calculator, provides the highest confidence. Redundant verification catches errors that single-method approaches miss.
Understanding your insulin syringe
The syringe itself is a source of confusion for people unfamiliar with insulin delivery. Semaglutide users often come from a background of no injection experience, and the syringe markings are designed for insulin dosing, not peptide dosing. Understanding what you are looking at makes accurate dosing much easier.
Syringe types and their markings
100-unit (1 mL) syringe. The most common type for semaglutide. Markings run from 0 to 100 in increments of 2 units. Each small line represents 2 units. For a 10-unit dose, you count 5 small lines from zero. These syringes are appropriate for all standard semaglutide doses at concentrations of 2.5 mg/mL and above.
50-unit (0.5 mL) syringe. Markings run from 0 to 50 in increments of 1 unit. Each small line represents 1 unit, providing double the precision of a 100-unit syringe. These are excellent for low doses where precision matters, like 2.5 or 5 units. The tradeoff is that the maximum volume is 0.5 mL (50 units), so higher doses at lower concentrations may not fit.
30-unit (0.3 mL) syringe. Markings run from 0 to 30 in increments of 0.5 units. The finest precision available for insulin syringes. Ideal for very low-dose protocols like microdosing approaches, but the 0.3 mL maximum limits them to higher-concentration vials at standard doses.
Choosing the right syringe for your concentration and dose improves accuracy. As a general rule, use the smallest syringe that fits your dose. Smaller syringes have more detailed markings, which translates to more precise measurements.
Reading the meniscus correctly
Liquid in a syringe forms a slightly curved surface called a meniscus. When reading your dose, always align the bottom of the meniscus (the lowest point of the curve) with the target line. Not the top of the curve. Not the middle.
Hold the syringe at eye level, perpendicular to your line of sight. Looking up or down at the syringe creates parallax error, making the liquid appear higher or lower than it actually is. This matters because even a one-unit error at high concentrations translates to meaningful dose differences. At 10 mg/mL, a single unit represents 0.1 mg of semaglutide. Across a full treatment protocol, consistent small errors compound.
How 10 units compares to other common doses
Putting 10 units in context with the other dose levels you will encounter during treatment helps you understand where you are in your protocol and what comes next.
Dose comparison at 5 mg/mL (most common concentration)
Protocol phase | Weekly dose | Units on syringe | How it compares to 10 units |
|---|---|---|---|
Starting (weeks 1-4) | 0.25 mg | 5 units | Half of 10 units |
Level 2 (weeks 5-8) | 0.5 mg | 10 units | This is 10 units |
Level 3 (weeks 9-12) | 1.0 mg | 20 units | Double 10 units |
Level 4 (weeks 13-16) | 1.7 mg | 34 units | 3.4 times 10 units |
Maximum (week 17+) | 2.4 mg | 48 units | 4.8 times 10 units |
At 5 mg/mL, 10 units is a moderate early-phase dose. You have already completed the starting dose and are progressing into more effective territory. Appetite suppression should be noticeable by this point. If you have been on 10 units (0.5 mg from a 5 mg/mL vial) for four weeks and feel no difference in appetite, discuss with your provider whether escalation is appropriate. Our guide on semaglutide appetite suppression timeline covers what to expect at each dose level.
Dose comparison at 2.5 mg/mL
Protocol phase | Weekly dose | Units on syringe | How it compares to 10 units |
|---|---|---|---|
Starting (weeks 1-4) | 0.25 mg | 10 units | This is 10 units |
Level 2 (weeks 5-8) | 0.5 mg | 20 units | Double 10 units |
Level 3 (weeks 9-12) | 1.0 mg | 40 units | 4 times 10 units |
Level 4 (weeks 13-16) | 1.7 mg | 68 units | 6.8 times 10 units |
Maximum (week 17+) | 2.4 mg | 96 units | 9.6 times 10 units |
At 2.5 mg/mL, 10 units is your starting dose. The very beginning of treatment. You are in the acclimation phase where results are minimal but the groundwork for effective therapy is being established. The full protocol at this concentration uses almost the entire syringe by the maximum dose.
Special situations and edge cases
Standard charts handle standard situations. But treatment is not always standard. These common scenarios require additional thought beyond the basic conversion formula.
Vials with added ingredients
Many compounding pharmacies add ingredients to semaglutide formulations. The most common additions include cyanocobalamin (vitamin B12), L-carnitine, glycine, and niacinamide. These additions do not change the semaglutide concentration on the label. If your vial says 5 mg/mL semaglutide with B12, the semaglutide is still 5 mg/mL. The additional ingredients are dissolved in the same solution but do not affect your semaglutide dose calculation.
However, the total volume in the vial may differ. A vial labeled "5 mg/mL semaglutide with B12, 3 mL total" contains 15 mg of semaglutide dissolved in 3 mL of solution that also contains B12. You still use 5 mg/mL as your concentration for calculations. The semaglutide with glycine formulation and semaglutide with B12 dosage chart follow the same principle.
Reconstituted lyophilized semaglutide
Some compounded semaglutide arrives as a freeze-dried (lyophilized) powder that you reconstitute with bacteriostatic water before use. In this case, the concentration depends on how much water you add, which gives you control over the final concentration.
If you have a 5 mg vial of lyophilized semaglutide and add 1 mL of bacteriostatic water, the concentration is 5 mg/mL. If you add 2 mL, the concentration is 2.5 mg/mL. The amount of semaglutide is fixed. The concentration changes based on your dilution volume.
This flexibility is useful but introduces another potential error point. If you reconstitute with the wrong volume of water, your concentration will be different from what you expect, and every subsequent dose will be wrong. Always follow your pharmacy instructions exactly when reconstituting, and verify the math before your first draw. The semaglutide reconstitution guide walks through this process step by step. You can also verify calculations using the peptide reconstitution calculator.
Switching between concentrations mid-protocol
This happens more often than you might think. Your pharmacy runs out of your usual concentration. Your provider switches you to a different telehealth platform. You refill from a different source. Suddenly your 5 mg/mL vial is replaced by a 2.5 mg/mL vial, and every unit number you have memorized is wrong.
When switching concentrations, recalculate everything from scratch. Do not try to "adjust" your old numbers. Start fresh with the new concentration and the formula. If you were drawing 10 units from a 5 mg/mL vial (0.5 mg dose) and switch to 2.5 mg/mL, you now need 20 units for the same 0.5 mg dose. If you kept drawing 10 units from the new vial, you would only get 0.25 mg, cutting your dose in half. Underdosing can cause a return of appetite, withdrawal-like symptoms, and stalled progress.
What if your vial has no concentration label
This should not happen, but it does. Some compounding pharmacies send vials with incomplete labeling. If your vial does not clearly state the concentration in mg/mL, do not inject from it. Contact your pharmacy immediately and request the concentration in writing before using the medication.
Using medication with an unknown concentration is the single highest-risk scenario in compounded semaglutide dosing. It is not worth the gamble.
A one-week delay in treatment while you verify is vastly preferable to a five-fold overdose because you assumed the wrong concentration.
Semaglutide units versus tirzepatide units
If you are considering both medications, or if someone shares dosing information in a forum, understanding the differences between semaglutide and tirzepatide unit conversions prevents a separate category of confusion.
Tirzepatide also comes from compounding pharmacies in multi-dose vials with various concentrations. But tirzepatide concentrations are different from semaglutide concentrations, and the therapeutic dose ranges are different. Ten units of compounded tirzepatide delivers a different amount of drug than ten units of compounded semaglutide at the same concentration, because semaglutide and tirzepatide are different molecules with different potency profiles.
More importantly, semaglutide and tirzepatide are not interchangeable on a milligram-for-milligram basis. A dose of 0.5 mg semaglutide is not equivalent to 0.5 mg tirzepatide. If you switch between medications, your provider will determine the appropriate conversion, which is typically based on clinical guidelines rather than simple math. The semaglutide to tirzepatide conversion chart covers these equivalencies in detail.
Never apply semaglutide conversion charts to tirzepatide vials or vice versa. Different drug. Different concentrations. Different therapeutic targets. Different math entirely. The tirzepatide dosing chart in units exists specifically for tirzepatide conversions.
How to store your semaglutide for accurate dosing
Storage affects your medication, and compromised medication means unreliable dosing even with perfect unit calculations. If the active ingredient degrades because of improper storage, drawing exactly 10 units may deliver less than the expected milligram amount because some of the semaglutide molecules have broken down.
Temperature requirements
Compounded semaglutide should be stored in the refrigerator at 36-46 degrees Fahrenheit (2-8 degrees Celsius). The medication can tolerate room temperature excursions for limited periods, but prolonged exposure to temperatures above 77 degrees Fahrenheit (25 degrees Celsius) accelerates degradation.
Do not freeze semaglutide. Freezing can damage the protein structure of the molecule, potentially reducing potency without any visible change to the medication. A vial that has been frozen and thawed may look identical to a properly stored vial but deliver less active drug per unit drawn.
The compounded semaglutide refrigeration guide covers temperature management in detail, including what to do if your medication was exposed to heat during shipping or a power outage.
Vial handling best practices
Once a multi-dose vial is opened (the stopper has been punctured by a needle), it has a limited use window. Most compounding pharmacies recommend using opened vials within 28-30 days when stored in the refrigerator. After this period, bacterial contamination risk increases and drug stability decreases.
Mark the date you first pierce each vial. Discard vials that have been open longer than 28 days, even if medication remains. The cost of wasted medication is trivial compared to the cost of injecting a degraded or contaminated product.
Between uses, store vials upright with the stopper facing up. This keeps the rubber stopper dry and reduces the risk of leakage or contamination. Keep the vial in its original packaging or a clean, dry container to protect from light exposure.
Working with your provider for safe dosing
Your provider prescribed a specific dose in milligrams. The conversion to units is the implementation step. But several provider-related factors can introduce additional complexity that affects your dosing accuracy.
Questions to ask your provider
Before your first injection, get clear answers to these questions. Do not assume anything. Write the answers down.
What concentration is my vial? Your provider should know which pharmacy they use and what concentration that pharmacy prepares. If they cannot answer this, ask for the pharmacy contact information and call directly.
What is my dose in milligrams? Get the milligram dose, not just the unit number. If your provider says "draw 10 units" without specifying milligrams and concentration, ask for clarification. You need both pieces of information.
Which syringe should I use? A 100-unit, 50-unit, or 30-unit syringe. The provider should recommend based on your dose and concentration.
What is my escalation schedule? Know when your dose increases and to what level. Calculate the unit numbers for your next dose in advance so you are prepared when the escalation date arrives.
Who do I contact for dosing questions? Determine whether you reach out to the prescribing provider or the pharmacy for dosing clarification. Know the response time you can expect. If semaglutide is not working as expected, prompt communication with your provider enables faster dose adjustments.
Red flags in provider instructions
Be cautious if your provider gives unit-based instructions without specifying concentration. This happens frequently in high-volume telehealth practices where standardized instructions may not account for pharmacy variations.
Be cautious if your provider says "just take what feels right" or recommends adjusting doses without clear milligram targets. Semaglutide dosing is based on clinical protocols, not intuition.
Be cautious if you receive a vial with a concentration that does not match what your provider specified. Contact both your provider and pharmacy before using it. The discrepancy could be a labeling error, a pharmacy substitution, or a miscommunication in the supply chain.
Digital tools for dose verification
Technology can eliminate calculation errors if you use the right tools correctly.
Dosage calculators
The SeekPeptides semaglutide dosage calculator is purpose-built for this exact scenario. Enter your vial concentration and prescribed dose, and it returns the exact units and volume to draw. No manual math required. It also shows a visual syringe representation so you can see exactly where the liquid level should fall.
Always cross-reference calculator output with your own understanding. If the calculator says 20 units and you expected 10, stop and investigate. Either your concentration input is wrong, your dose expectation is wrong, or you need to verify your vial. Calculators eliminate arithmetic errors but cannot catch input errors.
Reconstitution calculators
If you are working with lyophilized semaglutide, the reconstitution calculator determines the correct amount of bacteriostatic water to add based on your desired concentration and the total semaglutide content. Getting the reconstitution right means every subsequent dose calculation starts from the correct baseline. Our guide on how much bacteriostatic water to mix with 10mg semaglutide and the 5mg mixing guide provide specific instructions for the most common vial sizes.
Phone apps and notes
Create a note on your phone with your verified conversion. Include your concentration, prescribed dose, and the exact units to draw. Update this note whenever your dose changes. Having a quick reference eliminates the need to recalculate before each injection and reduces the chance of memory-based errors.
Some users photograph their vial label and keep it alongside their dose note. This creates a visual reference that confirms the concentration even if the vial is stored in a separate location from where they prepare injections.
The broader context: why compounded semaglutide uses units
Understanding why this confusion exists in the first place helps frame the entire issue. Units are not a natural dosing measure for semaglutide. They are an artifact of the delivery system.
The pre-filled pen advantage
FDA-approved semaglutide products like Ozempic and Wegovy use pre-filled injection pens with dose selectors calibrated in milligrams. You dial to your prescribed dose, press the button, and the pen delivers the correct amount. There is no syringe. No vials. No concentration calculations. No conversion charts. The engineering of the pen eliminates the entire category of errors that compounded semaglutide users face.
This is one of the genuine advantages of brand-name over compounded semaglutide. The cost difference is enormous (brand-name can exceed $1,000 per month without insurance), but so is the dosing safety margin. Anyone who can turn a dial can use an Ozempic or Wegovy pen accurately. Compounded semaglutide from vials requires math, attention to detail, and verification habits that not everyone develops.
Why compounding pharmacies use vials
Compounding pharmacies cannot produce pre-filled autoinjector pens. Those delivery devices are proprietary technology protected by patents held by Novo Nordisk. Compounders are limited to preparing the medication in multi-dose vials, which requires patients to use insulin syringes and perform their own dose calculations.
This is not a flaw in the compounding model. It is a practical limitation. The medication itself may be therapeutically equivalent. But the delivery system requires significantly more patient education and diligence. This is why resources like conversion charts, calculators, and detailed guides exist, to bridge the gap between a multi-dose vial and the simplicity of a pre-filled pen.
The future of compounded GLP-1 delivery
Some compounding pharmacies have begun offering pre-measured dose syringes where each syringe contains exactly one dose, eliminating the need for patients to draw from vials. Others provide sublingual tablets and oral semaglutide drops that bypass injection entirely. These innovations address the dosing accuracy problem from different angles.
GLP-1 patches are also in development, promising needle-free delivery with pre-measured doses. The goal across the industry is to make accurate dosing easier and more accessible, reducing the reliance on patient-performed calculations.
What your 10 units should feel like
Beyond the math, understanding the expected clinical effects at each dose level helps you verify that your dosing is in the right ballpark. If your 10 units from a 5 mg/mL vial (0.5 mg) produces effects consistent with a much higher or much lower dose, it could indicate a concentration mismatch.
Expected effects at 0.25 mg (10 units from 2.5 mg/mL)
This is the lowest standard dose. Appetite suppression is typically mild to minimal. Most people notice a slight reduction in food interest, particularly in the 24-48 hours after injection. Some notice no change at all. Nausea is possible but usually mild. Weight loss is minimal, often 1-2 pounds over the first month, primarily from reduced food intake rather than dramatic appetite changes.
If you take 10 units from what you believe is a 2.5 mg/mL vial and experience severe nausea, dramatic appetite loss, or rapid weight changes, your concentration may be higher than labeled. Contact your provider and pharmacy to verify.
Expected effects at 0.5 mg (10 units from 5 mg/mL)
Appetite suppression becomes more noticeable. Most users describe a meaningful reduction in food noise, that persistent background awareness of food and eating. Portion sizes naturally decrease. Cravings diminish, particularly for high-calorie, high-sugar foods. Mild nausea is common, especially in the first week at this dose. Monthly weight loss of 3-5 pounds is typical.
This dose level is where many people first feel that semaglutide is "working." The appetite suppression timeline varies individually, but consistent effects at this dose are expected by weeks 5-8.
Expected effects at 1.0 mg (10 units from 10 mg/mL)
Strong appetite suppression. Significant reduction in food intake without conscious effort. Some users describe having to remind themselves to eat, which can actually become a nutritional concern if protein intake drops too low. Side effects are possible but should be manageable. Monthly weight loss of 5-8 pounds is common. This is a genuinely therapeutic dose where clinically meaningful outcomes begin.
If 10 units from what you believe is a 10 mg/mL vial produces no noticeable appetite change after four weeks, the concentration may be lower than expected. Alternatively, your individual response may require higher doses. Discuss with your provider. The guide on why semaglutide might not be working covers additional factors beyond dosing that affect results.
Supporting your semaglutide protocol
Accurate dosing is the foundation. But dosing alone does not determine outcomes. Several supporting strategies significantly improve results regardless of where you are in the escalation schedule.
Protein prioritization
GLP-1 medications reduce total food intake. When you eat less overall, protein intake often drops proportionally unless you deliberately prioritize it. Inadequate protein during rapid weight loss causes muscle loss, which reduces metabolic rate and increases the likelihood of weight regain after stopping medication.
Target 0.7 to 1.0 grams of protein per pound of goal body weight daily. If your goal weight is 170 pounds, aim for 119 to 170 grams of protein per day. This requires deliberate food choices: eggs, Greek yogurt, chicken breast, fish, cottage cheese, protein shakes, and legumes. On days when appetite is particularly suppressed, liquid protein sources like shakes become essential for meeting targets without requiring large meal volumes.
The semaglutide diet plan provides comprehensive nutrition guidance tailored specifically for users on GLP-1 medications.
Hydration management
Semaglutide slows gastric emptying. This means food and liquid spend more time in your stomach. Combined with reduced appetite making it harder to consume adequate fluids, dehydration is a real and common risk. The FDA has documented acute kidney injury secondary to dehydration as a serious adverse event with GLP-1 medications.
Aim for 80 to 100 ounces of water daily. More if you exercise regularly or live in a warm climate. Consider electrolyte supplementation, particularly sodium, potassium, and magnesium, to maintain proper hydration balance. Signs of dehydration include dark urine, dry mouth, headaches, dizziness, and decreased urine output.
Injection site rotation
Rotate injection sites with each weekly dose. The recommended areas are the abdomen (avoiding two inches around the navel), the front of the thigh, and the upper arm. Using the same spot repeatedly can cause lipodystrophy (changes in fat tissue under the skin) and may affect medication absorption consistency.
Develop a rotation pattern. Some people use a clockwise rotation around the abdomen. Others alternate between abdomen, right thigh, left thigh, and upper arm on a four-week cycle. The specific pattern matters less than the consistency of rotating. Our GLP-1 injection site guide covers optimal placement and technique.
Timing your injection
Semaglutide is administered once weekly on the same day each week. The specific day and time are flexible, but consistency matters for maintaining steady blood levels. Choose a day that works with your schedule and stick to it.
If you miss your injection day, take it as soon as you remember, as long as your next scheduled dose is at least two days away. If it is within two days, skip the missed dose and resume your normal schedule. Do not double up to "catch up." The semaglutide treatment duration guide covers long-term adherence strategies.
When to contact your provider about dosing
Certain situations require medical guidance rather than self-adjustment.
Contact your provider if: you discover a concentration mismatch after one or more injections, experience unexpected side effects that do not align with your dose level, receive a vial without clear concentration labeling, switch pharmacies and receive a different concentration than expected, suspect you administered too much or too little medication, or experience no therapeutic effects after four or more weeks at your current dose.
Seek emergency care if: you experience severe abdominal pain radiating to your back (possible pancreatitis), persistent vomiting that prevents hydration for more than 24 hours, signs of severe dehydration (fainting, confusion, dark concentrated urine), or if you suspect you administered five or more times your intended dose.
Do not attempt to self-correct dosing errors by taking less at your next injection. Semaglutide has a one-week half-life. The excess dose remains in your system for days regardless of what you do next. Medical guidance ensures proper monitoring during this period.
Frequently asked questions
Is 10 units of semaglutide the same as 10 mg?
No. Ten units is a volume measurement (0.1 mL), not a weight measurement. The milligram amount in 10 units depends entirely on your vial concentration. At 5 mg/mL, 10 units contains 0.5 mg. At 2.5 mg/mL, 10 units contains 0.25 mg. At 10 mg/mL, 10 units contains 1.0 mg. Always check your vial label to determine the correct conversion for your specific medication.
How many units of semaglutide should I inject per week?
The number of units depends on your prescribed milligram dose and your vial concentration. For a standard starting dose of 0.25 mg weekly, you would draw 5 units from a 5 mg/mL vial, 10 units from a 2.5 mg/mL vial, or 25 units from a 1 mg/mL vial. Always follow your provider specific instructions and verify conversions against your vial concentration. Use the semaglutide dosage calculator to confirm your exact unit measurement.
What happens if I accidentally inject 10 units instead of 5 units?
You have administered double your intended dose. The severity of consequences depends on the concentration and the resulting milligram dose. From a 5 mg/mL vial, 10 units instead of 5 units means you took 0.5 mg instead of 0.25 mg. This is not dangerous but may cause more nausea and appetite suppression than expected. From a 10 mg/mL vial, the same error means 1.0 mg instead of 0.5 mg, a more significant overdose. Contact your provider, monitor for severe nausea and vomiting, stay hydrated, and do not take additional doses until your next scheduled injection date.
Can I use the same conversion chart for compounded semaglutide and Ozempic?
No. Ozempic uses pre-filled pens with built-in dose selectors calibrated in milligrams. There are no "units" to convert with Ozempic. You dial your dose on the pen and inject. Conversion charts apply exclusively to compounded semaglutide in multi-dose vials where you draw the medication with an insulin syringe. If you are using Ozempic or Wegovy pens, you do not need any conversion calculations.
How do I know what concentration my compounded semaglutide is?
The concentration should be printed on the vial label, typically expressed as "X mg/mL" (for example, "5 mg/mL" or "2.5 mg/mL"). If the label is unclear, damaged, or missing concentration information, contact your compounding pharmacy before using the medication. Your prescribing provider should also have the concentration on file. Never inject from a vial with an unknown concentration.
Why do different pharmacies use different concentrations?
Compounding pharmacies have flexibility in formulation design. Some choose higher concentrations (like 10 mg/mL) to minimize injection volumes. Others choose lower concentrations (like 2.5 mg/mL) to allow more precise measurement of small doses. Cost factors, stability considerations, and pharmacy expertise also influence concentration choices. There is no single "correct" concentration for compounded semaglutide.
Is 10 units a good starting dose for semaglutide?
It depends on your concentration. If your vial is 2.5 mg/mL, then 10 units equals 0.25 mg, which is the standard starting dose. If your vial is 5 mg/mL, then 10 units equals 0.5 mg, which is the second dose level and not appropriate for someone who has never taken semaglutide before. Starting at the lowest dose and escalating gradually reduces side effects and improves tolerability. Always follow your provider prescribed escalation schedule.
Do I need a special syringe for semaglutide?
Standard insulin syringes work perfectly for compounded semaglutide. A 100-unit (1 mL) syringe is the most versatile choice. For very precise low-dose measurements, a 50-unit (0.5 mL) or 30-unit (0.3 mL) syringe provides finer graduation marks. Use syringes with attached needles (typically 29-31 gauge, 1/2 inch) for subcutaneous injection. Your pharmacy or provider should specify the recommended syringe type.
External resources
For researchers committed to accurate dosing and evidence-based protocols, SeekPeptides provides the most comprehensive GLP-1 resource available, with precision dosage calculators, verified conversion charts for every concentration, and a community of thousands who prioritize safe, effective medication management.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay verified, your conversions stay accurate, and your doses stay precisely where they belong.