Feb 13, 2026

One full syringe. That is what 100 units represents on a standard insulin syringe. But how many milligrams of semaglutide does that actually contain? The answer is not as simple as you might hope. It depends entirely on the concentration of your specific vial or pen, and getting this wrong can mean the difference between an effective dose and a trip to the emergency room.
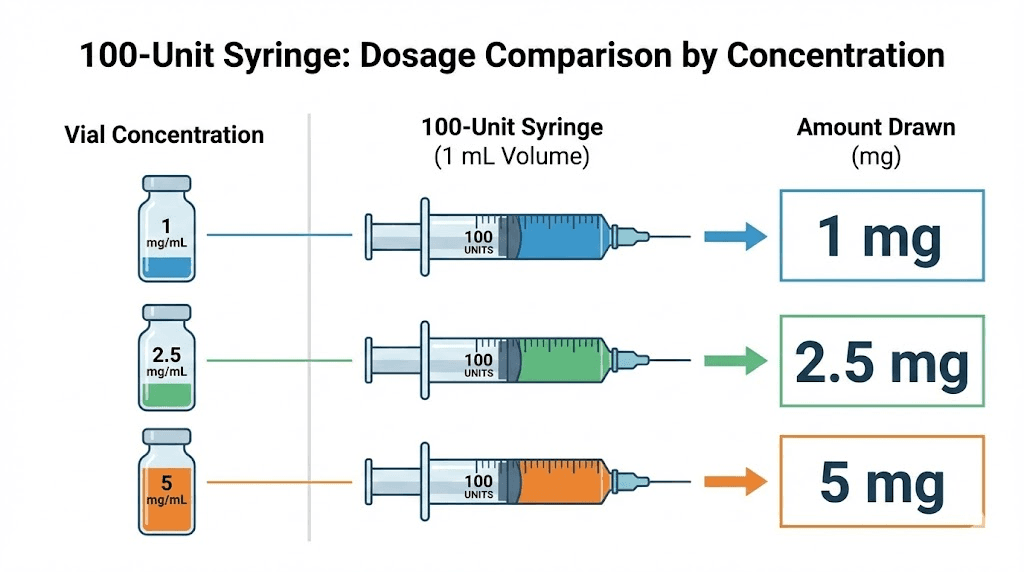
The FDA has reported a significant increase in semaglutide-related dosing errors, with some individuals injecting five to twenty times their prescribed dose. Many of these mistakes come down to one fundamental misunderstanding: confusing units with milligrams. A 100-unit insulin syringe always holds 1 mL of liquid. But the milligrams of semaglutide in that 1 mL? That changes based on concentration. At 1 mg/mL, 100 units equals 1 mg. At 5 mg/mL, 100 units equals 5 mg. Same syringe. Same markings. Wildly different doses.
This guide breaks down every concentration you will encounter, provides conversion charts you can reference in seconds, and walks through the exact math so you never have to guess. Whether you are working with a compounded semaglutide vial from a pharmacy, a branded Ozempic pen, or a 5 mg research vial, the formula is the same. You just need to know your concentration. SeekPeptides has helped thousands of researchers navigate exactly this kind of calculation, and by the end of this article, you will have the confidence to convert any semaglutide measurement with precision.
Why 100 units does not always equal the same number of milligrams
The confusion starts with the syringe itself. Insulin syringes measure volume in units. One hundred units equals 1 milliliter. Always. That part never changes regardless of what liquid fills the syringe.
But here is where people get lost.
The number of milligrams in that 1 mL depends on how concentrated the solution is. Think of it like coffee. A standard cup and an espresso cup both hold liquid. But the espresso has far more caffeine packed into a smaller volume because it is more concentrated. Semaglutide works the same way. A vial labeled 1 mg/mL contains 1 milligram in every milliliter of solution. A vial labeled 5 mg/mL contains five times as much active ingredient in the same volume. Drawing 100 units from a 1 mg/mL vial gives you 1 mg. Drawing 100 units from a 5 mg/mL vial gives you 5 mg. Same syringe reading. Five times the dose.
This distinction matters more than almost any other factor in semaglutide dosing. Researchers who have previously worked with medications where units have a fixed meaning, like insulin where 1 unit always equals 1 unit of insulin regardless of concentration, often carry that assumption into semaglutide dosing. That assumption can be dangerous. Semaglutide units on a syringe are purely a measurement of volume, not potency. The concentration printed on your vial label is the critical piece of information that translates volume into an actual dose.
Understanding semaglutide reconstitution principles helps clarify this further. When you reconstitute a lyophilized peptide with bacteriostatic water, you control the final concentration based on how much water you add. More water means a lower concentration per milliliter. Less water means a higher concentration. The same peptide powder produces completely different mg-per-unit values depending on your reconstitution volume.
The universal conversion formula
Every semaglutide unit-to-mg conversion uses one formula. Learn it once, and you can convert any concentration instantly.
Milligrams = (Units / 100) x Concentration (mg/mL)
That is it. Three variables. One multiplication.
Since 100 units always equals 1 mL on a standard insulin syringe, the formula simplifies even further for our specific question. When you draw 100 units, you are drawing exactly 1 mL. So the milligrams you get equals whatever the concentration says on the label. If the label reads 2.5 mg/mL, then 100 units gives you 2.5 mg. If it reads 5 mg/mL, you get 5 mg.
But most people do not inject a full 100 units at once. So let us look at how the formula works at any number of units. Say you need to draw 25 units from a 5 mg/mL vial. The math: (25 / 100) x 5 = 1.25 mg. Or 10 units from a 2.5 mg/mL vial: (10 / 100) x 2.5 = 0.25 mg. The semaglutide dosage calculator on our site does this math automatically, but knowing the formula means you can verify any result yourself.
For the reverse calculation, when you know the mg you want and need to find the units, flip the formula: Units = (Desired mg / Concentration) x 100. If your prescribed dose is 0.5 mg and your vial is 2.5 mg/mL: (0.5 / 2.5) x 100 = 20 units. This reverse formula is equally important because most prescriptions specify milligrams, not units. You need to translate that into something your syringe can measure.
100 units at every common semaglutide concentration
Here is the answer to the main question at every concentration you are likely to encounter. Bookmark this section.
Concentration (mg/mL) | 100 Units Equals | Common Source |
|---|---|---|
0.68 mg/mL | 0.68 mg | Ozempic 0.25/0.5 mg pen |
1 mg/mL | 1 mg | Some compounding pharmacies |
1.34 mg/mL | 1.34 mg | Ozempic 1 mg pen |
2 mg/mL | 2 mg | Some compounding pharmacies |
2.5 mg/mL | 2.5 mg | Common compounded concentration |
2.68 mg/mL | 2.68 mg | Ozempic 2 mg pen |
3 mg/mL | 3 mg | Some compounding pharmacies |
5 mg/mL | 5 mg | Common compounded/research vial |
10 mg/mL | 10 mg | High-concentration research vial |
Look at that range. The same 100 units on your syringe could deliver anywhere from 0.68 mg to 10 mg of semaglutide. That is nearly a 15x difference between the lowest and highest concentrations. Someone accustomed to a 1 mg/mL formulation who switches to 5 mg/mL without adjusting their unit measurement would inject five times their intended dose. The semaglutide conversion chart we have published covers even more concentration variations with detailed unit-by-unit breakdowns.
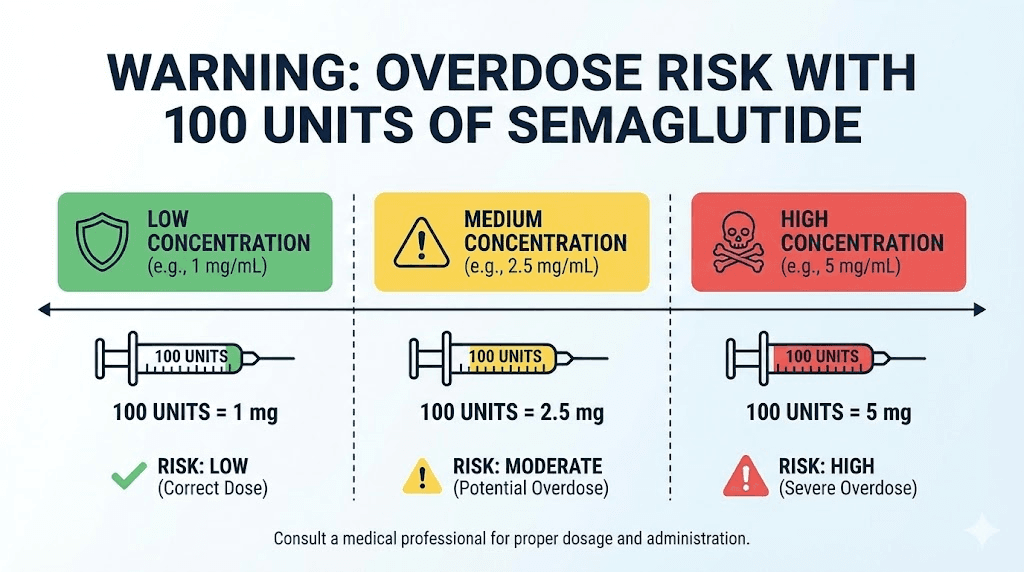
The most common compounded concentration is 2.5 mg/mL, which means 100 units delivers 2.5 mg of semaglutide. This is roughly equivalent to the maximum maintenance dose for diabetes management with Ozempic (2 mg weekly) but still below the maximum weight loss dose of Wegovy (2.4 mg weekly). For 5 mg/mL vials, 100 units would give you 5 mg, which is more than double the maximum FDA-approved weekly dose. Injecting this amount at once would be a significant overdose for most protocols.
Detailed conversion charts by concentration
The table above answers the headline question. But you probably need more than just the 100-unit conversion. Below are complete charts for the four most common semaglutide concentrations, showing every practical unit measurement and its corresponding mg value. Use the chart that matches your specific vial.
Conversion chart: 1 mg/mL concentration
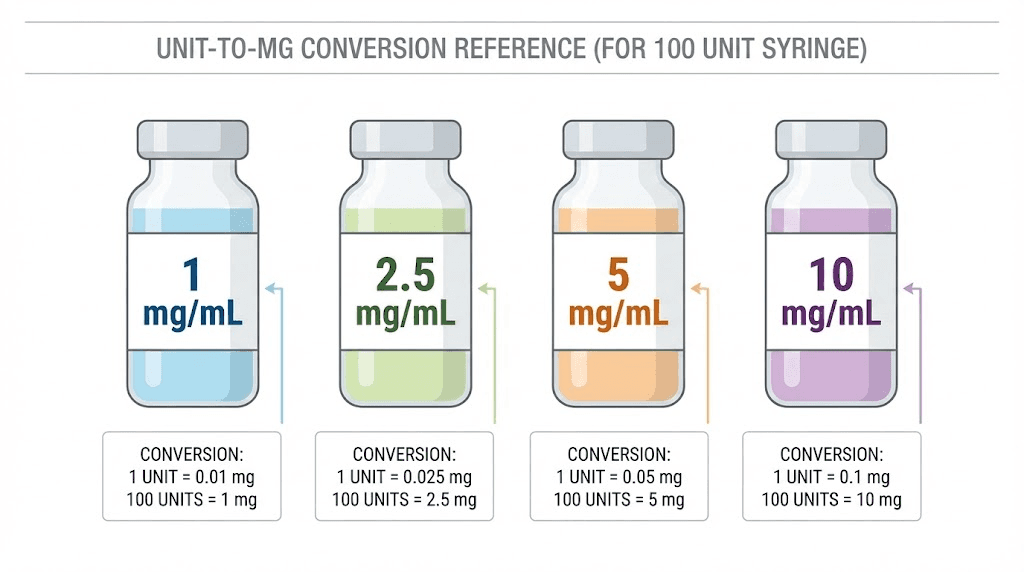
This concentration is the simplest to work with because units and volume have a straightforward relationship. Each unit on the syringe equals 0.01 mg. You will find this concentration at some compounding pharmacies, and it requires larger injection volumes to reach standard doses. That means more liquid under the skin per injection, which some researchers find uncomfortable at higher doses. The compounded semaglutide dose chart provides additional context for these lower concentrations.
Units | mL | mg |
|---|---|---|
5 | 0.05 | 0.05 |
10 | 0.10 | 0.10 |
15 | 0.15 | 0.15 |
20 | 0.20 | 0.20 |
25 | 0.25 | 0.25 |
30 | 0.30 | 0.30 |
40 | 0.40 | 0.40 |
50 | 0.50 | 0.50 |
60 | 0.60 | 0.60 |
70 | 0.70 | 0.70 |
80 | 0.80 | 0.80 |
100 | 1.00 | 1.00 |
At this concentration, reaching the standard starting dose of 0.25 mg requires drawing 25 units. The maintenance dose of 2.4 mg would require 240 units, which is more than two full syringes. This is why higher concentrations exist. They reduce injection volume.
Conversion chart: 2.5 mg/mL concentration
This is the most popular compounded semaglutide concentration. Many pharmacies default to 2.5 mg/mL because it balances manageable injection volumes with the ability to measure small dose increments accurately. If you received your semaglutide from a compounding pharmacy and are unsure of the concentration, 2.5 mg/mL is the most likely option, though you should always verify with the label. The semaglutide dosage chart in mL provides additional reference points for this concentration.
Units | mL | mg |
|---|---|---|
5 | 0.05 | 0.125 |
10 | 0.10 | 0.25 |
15 | 0.15 | 0.375 |
20 | 0.20 | 0.50 |
25 | 0.25 | 0.625 |
30 | 0.30 | 0.75 |
40 | 0.40 | 1.00 |
50 | 0.50 | 1.25 |
60 | 0.60 | 1.50 |
68 | 0.68 | 1.70 |
80 | 0.80 | 2.00 |
96 | 0.96 | 2.40 |
100 | 1.00 | 2.50 |
Notice how 10 units at this concentration delivers the standard starting dose of 0.25 mg. And 96 units gets you to the maximum Wegovy dose of 2.4 mg. This is why 2.5 mg/mL is so practical. The entire semaglutide dose escalation fits neatly within a single syringe.
Conversion chart: 5 mg/mL concentration
Higher concentration means smaller injection volumes, which many researchers prefer for comfort. But smaller volumes also mean smaller margins for error. A 2-unit mistake at 5 mg/mL equals 0.1 mg, double the error you would make at 2.5 mg/mL. Precision matters more as concentration increases. Our 5 mg/2 mL dosage chart covers this concentration in even greater detail.
Units | mL | mg |
|---|---|---|
5 | 0.05 | 0.25 |
10 | 0.10 | 0.50 |
15 | 0.15 | 0.75 |
20 | 0.20 | 1.00 |
25 | 0.25 | 1.25 |
30 | 0.30 | 1.50 |
34 | 0.34 | 1.70 |
40 | 0.40 | 2.00 |
48 | 0.48 | 2.40 |
50 | 0.50 | 2.50 |
60 | 0.60 | 3.00 |
80 | 0.80 | 4.00 |
100 | 1.00 | 5.00 |
At 5 mg/mL, only 5 units delivers the starting dose of 0.25 mg. The full escalation protocol from 0.25 mg to 2.4 mg spans just 5 to 48 units. And 100 units, a full syringe, would give you 5 mg, which is more than double the maximum approved weekly dose. Drawing a full syringe from a 5 mg/mL vial would be a serious dosing error for anyone following standard protocols.
Conversion chart: 10 mg/mL concentration
The highest concentration you will commonly encounter. Research vials and some compounding pharmacies use this concentration to maximize the number of doses per vial. At this concentration, even tiny measurement errors produce significant dose changes. A single unit on the syringe equals 0.1 mg of semaglutide. The semaglutide 10 mg dosage chart and the 10 mg vial dosage chart offer expanded reference tables for this concentration.
Units | mL | mg |
|---|---|---|
2.5 | 0.025 | 0.25 |
5 | 0.05 | 0.50 |
10 | 0.10 | 1.00 |
15 | 0.15 | 1.50 |
17 | 0.17 | 1.70 |
20 | 0.20 | 2.00 |
24 | 0.24 | 2.40 |
25 | 0.25 | 2.50 |
30 | 0.30 | 3.00 |
40 | 0.40 | 4.00 |
50 | 0.50 | 5.00 |
100 | 1.00 | 10.00 |
A full 100 units from a 10 mg/mL vial would deliver 10 mg of semaglutide. That is more than four times the maximum approved weekly dose. This concentration demands extreme precision. Most researchers use specialized syringe dosage charts and double-check every measurement when working at this concentration level.
Understanding insulin syringe markings and how they relate to semaglutide
If you have ever used an insulin syringe for semaglutide, you know the markings can be confusing. The syringe was designed for insulin, not semaglutide. And that difference matters.
Insulin syringes come in three standard sizes. The 30-unit syringe (0.3 mL) has markings every 1 unit and works well for very small, precise measurements. The 50-unit syringe (0.5 mL) marks every 1 unit and suits moderate doses. The 100-unit syringe (1 mL) marks every 2 units and handles the full range of doses but with slightly less precision at small volumes.
Here is the critical difference between insulin and semaglutide. With insulin, the units on the syringe directly correspond to international units (IU) of insulin activity. One unit of insulin is one unit, period, regardless of the insulin concentration you use (though most modern insulin is U-100, meaning 100 units per mL). With semaglutide, the unit markings only tell you volume. They say nothing about how much active medication you are drawing.
This distinction trips up even experienced researchers. If someone tells you to take "25 units of semaglutide," that instruction is meaningless without knowing the concentration. Twenty-five units from a 1 mg/mL vial is 0.25 mg. Twenty-five units from a 5 mg/mL vial is 1.25 mg. Five times the dose from the same syringe marking. The semaglutide syringe dosage conversion chart makes these differences visually clear for quick reference.
When selecting a syringe size, match it to your dose. If your typical dose falls between 5 and 15 units, a 30-unit syringe gives the best precision. If you routinely draw 20 to 50 units, the 50-unit syringe balances precision and capacity. Only use a 100-unit syringe when your dose requires more than 50 units, or when you need the full 1 mL capacity.
Branded Ozempic and Wegovy pens: a different system entirely
If you use a branded Ozempic or Wegovy pen, the unit conversation works differently than with vials and syringes. Understanding the distinction prevents dangerous crossover errors.
Ozempic pens come in three configurations. The starter pen delivers 0.25 mg or 0.5 mg doses and contains 2 mg total in 1.5 mL (concentration: approximately 1.34 mg/mL). The mid-range pen delivers 1 mg per dose and contains 4 mg total in 3 mL (same 1.34 mg/mL concentration). The high-dose pen delivers 2 mg per dose and contains 8 mg total in 3 mL (concentration: approximately 2.68 mg/mL).
Notice those concentrations: 1.34 mg/mL and 2.68 mg/mL. These do not match any common compounded vial concentration. This is critical. If you are used to a compounded vial at 2.5 mg/mL and someone hands you an Ozempic pen, you cannot apply the same math. The pen has a built-in dose selector that dials to specific milligram amounts, so you never need to think in units. But if you try to extract liquid from a pen with a syringe (some people do this for microdosing purposes), the concentration mismatch can cause major errors.
Wegovy pens follow a similar system but with fixed single-dose pens at 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, and 2.4 mg. Each pen is pre-loaded with one dose, so there is no measurement required. The concentration varies between pen strengths, and Novo Nordisk, the manufacturer, explicitly discourages any off-label dosing modifications to these pens.
The speed of semaglutide results depends partly on consistent, accurate dosing. Errors in conversion between pen and vial systems can create weeks of subtherapeutic or supratherapeutic dosing that disrupts the entire treatment timeline.
The semaglutide dose escalation protocol and where 100 units fits
Understanding where 100 units falls in the standard dose escalation schedule helps contextualize whether drawing 100 units makes sense for your protocol.
The standard semaglutide titration schedule looks like this:
Phase | Weekly Dose | Duration | Units at 2.5 mg/mL | Units at 5 mg/mL |
|---|---|---|---|---|
Month 1 | 0.25 mg | 4 weeks | 10 units | 5 units |
Month 2 | 0.50 mg | 4 weeks | 20 units | 10 units |
Month 3 | 1.00 mg | 4 weeks | 40 units | 20 units |
Month 4 | 1.70 mg | 4 weeks | 68 units | 34 units |
Month 5+ | 2.40 mg | Ongoing | 96 units | 48 units |
Look at the 2.5 mg/mL column. The maximum maintenance dose of 2.4 mg requires 96 units. Nearly a full syringe, but not quite 100. Drawing exactly 100 units from a 2.5 mg/mL vial would give you 2.5 mg, slightly above the maximum approved dose. At 5 mg/mL, the maximum dose requires only 48 units, less than half a syringe.
The escalation schedule exists for good reason. Semaglutide works by mimicking GLP-1, a hormone that slows gastric emptying and signals satiety to the brain. Starting at a low dose allows your body to adapt to these effects gradually. Jumping to a higher dose too quickly, or accidentally injecting 100 units from a concentrated vial, triggers severe gastrointestinal side effects that the semaglutide fatigue and nausea response can make genuinely debilitating.
Each dose increase should only happen after tolerating the previous dose for at least four weeks. Researchers who experience persistent nausea, vomiting, or other side effects should delay escalation rather than pushing through. The appetite suppression timeline varies between individuals, and some achieve their goals at 1 mg or 1.7 mg without ever reaching the maximum dose.
What happens if you accidentally inject 100 units from a high-concentration vial
Mistakes happen. And with semaglutide, a dosing error is not something you can simply reverse. The medication has a half-life of approximately one week, meaning it takes seven days for your body to clear just half of an administered dose. There is no antidote. No way to "undo" an injection.
Let us walk through the scenarios.
100 units from a 2.5 mg/mL vial (2.5 mg total): This is slightly above the maximum approved weekly dose of 2.4 mg. If you are already at maintenance dose, the overshoot is minimal, about 4% above target. You would likely experience some increased nausea but nothing dangerous for most people. If you are still in early escalation phases, though, jumping from 0.25 mg to 2.5 mg is a tenfold overdose that will almost certainly cause severe nausea, vomiting, and potentially dehydration.
100 units from a 5 mg/mL vial (5 mg total): This is more than double the maximum approved dose. Even for someone fully titrated to 2.4 mg weekly, this represents a significant overdose. Expect severe gastrointestinal symptoms lasting several days. The troubleshooting guide for semaglutide notes that overdosing paradoxically can stall weight loss due to the body stress response and inability to maintain adequate nutrition.
100 units from a 10 mg/mL vial (10 mg total): This is over four times the maximum dose. Seek emergency medical attention. Severe hypoglycemia, pancreatitis, and dangerous dehydration from persistent vomiting are real risks at this level. Emergency departments treat semaglutide overdoses with IV fluids and anti-nausea medications, but the long half-life means symptoms can persist for days.
CNN reported that poison control centers saw a nearly 1,500% increase in calls related to injectable weight loss drugs, many stemming from exactly this type of concentration confusion. The side effect comparison between semaglutide and tirzepatide shows that GI effects are dose-dependent for both medications, making accurate measurement essential for either compound.
How to verify your vial concentration before calculating
Every dosing calculation starts with one piece of information: the concentration printed on your vial or pen. Here is exactly where to find it and how to confirm it.
Step 1: Read the label
The concentration appears on the vial label, typically expressed as mg/mL. Common formats include:
"Semaglutide 5 mg/mL" (directly stated)
"Semaglutide 10 mg / 2 mL" (total content per total volume, meaning 5 mg/mL)
"Each mL contains 2.5 mg semaglutide" (stated per milliliter)
Watch for labels that state total content rather than concentration. A vial labeled "5 mg / 2 mL" has a concentration of 2.5 mg/mL, not 5 mg/mL. Dividing the total milligrams by the total milliliters gives you the concentration. The guide on mixing bacteriostatic water with 5 mg semaglutide explains how different reconstitution volumes create different concentrations from the same powder.
Step 2: Confirm with your pharmacy
If the label is unclear, damaged, or missing concentration information, call your pharmacy before using the vial. Never guess. A phone call takes two minutes. A dosing error can have consequences lasting a week or more.
Step 3: Check for additives
Many compounded semaglutide formulations include B12 (cyanocobalamin) or other additives. The label might read "Semaglutide 2.5 mg / Cyanocobalamin 1 mg per mL." The B12 does not change the semaglutide concentration. Your conversion math stays the same. But knowing about additives helps you understand exactly what you are injecting. The semaglutide with B12 guide and B12 dosage chart cover these combination formulations in detail.
Step 4: Document your concentration
Write the concentration on your dosing log or set it in your peptide calculator before each session. This prevents the scenario where you switch between vials of different concentrations and forget which one you are currently using. The peptide dosage calculation guide recommends labeling each syringe after drawing to add another layer of error prevention.
Reconstituted semaglutide: calculating your own concentration
When you reconstitute semaglutide from lyophilized powder, you create your own concentration. The math is straightforward, but mistakes here cascade through every subsequent dose.
The formula: Concentration (mg/mL) = Total peptide (mg) / Total water added (mL)
For a 5 mg vial of semaglutide powder:
Water Added (mL) | Resulting Concentration (mg/mL) | 100 Units Equals |
|---|---|---|
1 mL | 5.0 mg/mL | 5.0 mg |
2 mL | 2.5 mg/mL | 2.5 mg |
2.5 mL | 2.0 mg/mL | 2.0 mg |
5 mL | 1.0 mg/mL | 1.0 mg |
10 mL | 0.5 mg/mL | 0.5 mg |
See the pattern? More water means a lower concentration, which means each unit on the syringe represents less semaglutide. Adding 2 mL of bacteriostatic water to a 5 mg vial gives you 2.5 mg/mL, the most commonly used concentration. Adding 1 mL gives you 5 mg/mL, a higher concentration that requires smaller, more precise measurements.
The peptide reconstitution calculator automates this for you. Enter your peptide amount and desired concentration, and it tells you exactly how much water to add. But understanding the math behind it means you can verify the calculator output and catch any input errors before they become dosing errors.
One common mistake during reconstitution: not accounting for the volume of the peptide powder itself. Most lyophilized peptides occupy a negligible volume once dissolved, but some formulations include bulking agents that add measurable volume. If you add exactly 2 mL of water and the powder adds 0.1 mL of volume, your actual total volume is 2.1 mL, making the true concentration slightly lower than calculated. For most practical purposes this difference is clinically insignificant, but perfectionists should be aware of it.
The 5 mg semaglutide reconstitution guide walks through the complete process step by step, including proper water measurement techniques for achieving precise concentrations.
Common semaglutide unit conversion mistakes and how to avoid them
After analyzing the most common dosing questions across semaglutide communities, several patterns emerge. These are the mistakes people make again and again.
Mistake 1: Assuming all vials have the same concentration
Someone switches pharmacies or receives a new batch with a different concentration. They draw the same number of units they always have, not realizing the concentration changed. The fix is simple but essential: check the concentration label every single time you draw a dose. Even if you have been using the same pharmacy for months, verify. Formulations change.
Mistake 2: Confusing total vial content with concentration
A label says "5 mg." The researcher assumes 5 mg/mL. But the vial contains 2 mL of liquid, making the actual concentration 2.5 mg/mL. This error doubles the intended dose. Always divide total milligrams by total milliliters to find the true concentration. The bacteriostatic water mixing guide for 5 mg vials explains this distinction clearly.
Mistake 3: Using pen math for vial dosing
Ozempic pen concentrations (1.34 mg/mL and 2.68 mg/mL) do not match any common compounded vial concentration (1, 2.5, 5, or 10 mg/mL). Someone who reads that their Ozempic pen delivers 0.5 mg at a certain dial setting and then tries to replicate that with a syringe from a compounded vial will get the wrong dose unless they recalculate from scratch. Always base your calculations on your actual vial concentration, never on information from a different product.
Mistake 4: Not accounting for syringe dead space
Standard syringes have a small amount of dead space in the hub and needle where liquid remains after injection. This volume, typically 0.02 to 0.07 mL, never enters your body. For small doses like 5 units (0.05 mL), this dead space can represent a significant percentage of the intended dose. Low dead space syringes minimize this issue. Some researchers add a small air bubble behind the liquid to push medication through the dead space, though this technique requires practice to execute consistently.
Mistake 5: Drawing from a multi-dose vial after it has been stored too long
Semaglutide stability decreases over time after reconstitution. Using a vial past its recommended storage period does not change the concentration per se, but degraded semaglutide delivers less active medication than the label concentration suggests. The compounded semaglutide storage guide and refrigeration requirements detail proper storage protocols to maintain potency throughout the vial life.
The expired semaglutide guide addresses this concern directly, including signs of degradation and when to discard a vial.
Step-by-step conversion walkthrough: from prescription to syringe
Let us work through a complete real-world example. You have a prescription for 0.5 mg of semaglutide weekly. Your compounded vial is labeled 2.5 mg/mL. Here is exactly how to determine how many units to draw.
Step 1: Identify your prescribed dose. In this case, 0.5 mg.
Step 2: Identify your vial concentration. The label reads 2.5 mg/mL.
Step 3: Apply the formula. Units = (Desired mg / Concentration) x 100. So (0.5 / 2.5) x 100 = 20 units.
Step 4: Select the appropriate syringe. Twenty units is a comfortable measurement on either a 30-unit or 50-unit syringe. A 30-unit syringe provides the best precision at this volume.
Step 5: Draw to the 20-unit line on your syringe. Confirm visually. Inject.
Now let us do the same calculation for a 5 mg/mL vial. Same prescribed dose, 0.5 mg. Different concentration. Units = (0.5 / 5) x 100 = 10 units. Half the volume for the same dose, because the concentration is double.
And for a 1 mg/mL vial: Units = (0.5 / 1) x 100 = 50 units. Five times the volume, because the concentration is one-fifth. Same 0.5 mg of semaglutide in all three cases. Three very different syringe readings.
This walkthrough demonstrates why memorizing a single number of units is dangerous. The only safe approach is knowing your concentration and running the calculation each time. Or, even better, using the SeekPeptides semaglutide calculator that does this math instantly and correctly.
How 100 units compares to other common semaglutide conversions
People searching for the 100-unit conversion often need context for other common unit values too. Here is how 100 units sits relative to the most frequently searched conversions, all at the popular 2.5 mg/mL concentration.
Units | mg (at 2.5 mg/mL) | Escalation Phase | Related Guide |
|---|---|---|---|
10 | 0.25 mg | Month 1 starting dose | |
20 | 0.50 mg | Month 2 | |
40 | 1.00 mg | Month 3 | |
50 | 1.25 mg | Between escalation steps | |
68 | 1.70 mg | Month 4 | |
96 | 2.40 mg | Month 5+ maintenance | |
100 | 2.50 mg | Slightly above max dose | This article |
At 2.5 mg/mL, 100 units sits just above the maximum FDA-approved weekly dose for weight management. This means that if you find yourself drawing exactly 100 units from a 2.5 mg/mL vial each week, you are administering marginally more than the highest recommended dose. The long-term semaglutide use guide discusses maximum dosing protocols and when adjustments might be needed.
For the complete semaglutide dosage chart in units, including every increment from 1 to 100 units, visit our dedicated conversion page. It covers every concentration and includes printable reference charts you can keep near your supplies.
Semaglutide storage, handling, and how they affect your measurements
Accurate dosing is not just about math. It is about ensuring the semaglutide in your vial is still at the concentration the label claims. Improper storage degrades the peptide, reducing its effective concentration even though the label has not changed.
Temperature requirements
Semaglutide should be stored in the refrigerator at 36-46 degrees Fahrenheit (2-8 degrees Celsius) before first use. Once in use, most compounded formulations remain stable in the refrigerator for 28-42 days, depending on the pharmacy specifications. Never freeze semaglutide. Freezing can denature the peptide and destroy its biological activity entirely.
Room temperature storage is acceptable for brief periods, but prolonged exposure to temperatures above 77 degrees Fahrenheit (25 degrees Celsius) accelerates degradation. The peptide storage guide provides detailed stability data across temperature ranges and timeframes.
Light exposure
Semaglutide is light-sensitive. Store vials in their original packaging or wrap them in foil if the packaging has been discarded. Light exposure breaks down peptide bonds over time, reducing potency without any visible changes to the solution. You would not know the concentration has dropped until you notice reduced effectiveness.
Contamination prevention
Every time you puncture the rubber stopper of a multi-dose vial, you introduce a potential pathway for bacterial contamination. Bacteriostatic water contains a preservative (benzyl alcohol) that inhibits bacterial growth, but it does not make the solution immune to contamination. Always use an alcohol swab on the vial stopper before drawing. Always use a new, sterile needle for each draw. The guide on peptide mixing water explains why bacteriostatic water, not sterile water, should be used for multi-dose vials.
Visual inspection
Before drawing any dose, visually inspect the solution. Semaglutide solution should be clear and colorless. If you see cloudiness, particles, discoloration, or unusual viscosity, do not use the vial. These are signs of degradation or contamination. A degraded solution may have an actual concentration significantly lower than what the label states, which means your unit-to-mg conversion will overestimate the dose you are actually receiving. The expired semaglutide analysis covers degradation indicators in more detail.
Using calculators to verify your conversion
While understanding the math is essential, using a calculator as a verification tool adds a safety layer to every dose. SeekPeptides offers several free calculators specifically designed for peptide dosing.
The semaglutide dosage calculator
The semaglutide dosage calculator takes your vial concentration and desired dose in milligrams, then outputs the exact number of units to draw. It also shows the equivalent volume in milliliters and confirms whether your dose falls within standard protocol ranges. This tool is the fastest way to verify manual calculations and eliminates arithmetic errors entirely.
The peptide reconstitution calculator
If you are working with lyophilized semaglutide and need to determine how much bacteriostatic water to add for a specific target concentration, the reconstitution calculator handles this. Enter the total peptide amount (in mg) and your desired concentration, and it tells you exactly how many milliliters of water to add. You can also input the water volume first and see what concentration results.
The peptide cost calculator
The peptide cost calculator helps you understand how many doses you can get from each vial at your concentration. For a 5 mg vial reconstituted at 2.5 mg/mL (2 mL total), a weekly dose of 0.5 mg (20 units) gives you 10 doses per vial. At 2.4 mg weekly (96 units), you get just over 2 doses per vial. Knowing this helps with supply planning and cost management.
SeekPeptides members access additional calculation tools including personalized protocol builders that integrate dose tracking, escalation scheduling, and supply management into a single dashboard. These tools reduce the cognitive load of managing complex dosing protocols and provide built-in safety checks that flag unusual measurements before they become errors.
Switching between semaglutide concentrations safely
At some point, most semaglutide users switch concentrations. Maybe your pharmacy changes its formulation. Maybe you switch pharmacies. Maybe you graduate from a lower to higher concentration as your dose increases. Each switch is a potential error point.
The golden rule of concentration switches
When you switch concentrations, recalculate everything from scratch. Do not try to ratio your way from old units to new units. Start with your prescribed dose in milligrams, apply the conversion formula with the new concentration, and arrive at a fresh unit measurement. The semaglutide to tirzepatide conversion chart applies this same principle when switching between different medications entirely.
Practical example
You have been drawing 40 units weekly from a 2.5 mg/mL vial (1 mg dose). Your new vial is 5 mg/mL. If you draw 40 units from the new vial, you get 2 mg instead of 1 mg. Double your intended dose. The correct calculation for 1 mg from a 5 mg/mL vial: (1 / 5) x 100 = 20 units. Half the volume for the same dose.
Label your supplies
When transitioning between concentrations, label everything clearly. Write the concentration on the vial with a marker. Note the unit count for your current dose on your dosing log. Some researchers use color-coded tape, blue for 2.5 mg/mL, red for 5 mg/mL, to provide an instant visual cue about which concentration they are handling.
The switching medications guide covers the broader considerations when changing between GLP-1 formulations, including dose equivalency charts for cross-medication transitions.
Advanced considerations for semaglutide dosing precision
For researchers who demand maximum accuracy, several factors beyond basic concentration math influence your actual delivered dose.
Temperature and viscosity
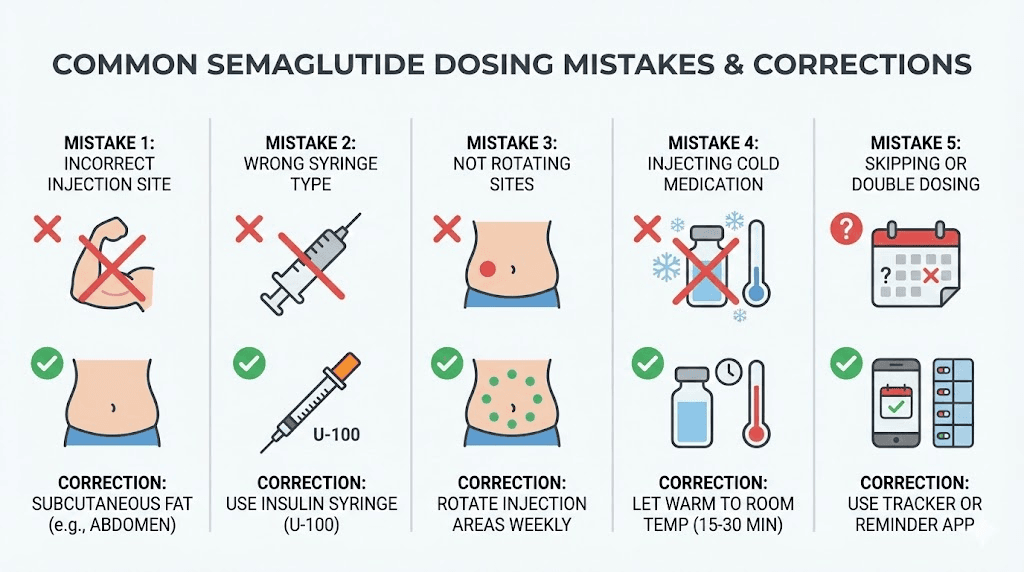
Cold semaglutide (straight from the refrigerator) is slightly more viscous than room-temperature semaglutide. This increased viscosity can make drawing the solution into the syringe more difficult and can lead to inaccurate measurements, especially at small volumes. Letting the vial warm to room temperature for 10-15 minutes before drawing improves accuracy and reduces injection discomfort. The semaglutide storage duration guide notes that brief room temperature warming does not affect stability.
Air bubbles
Air bubbles in the syringe reduce the actual volume of medication drawn. A syringe that appears to read 20 units but contains a 2-unit air bubble at the plunger only holds 18 units of medication. Flick the syringe firmly to move bubbles to the top, then push the plunger slightly to expel them. Re-check your measurement after removing bubbles.
Injection technique and absorption
Where and how you inject affects absorption, which indirectly affects the effective dose your body receives from a given number of units. Subcutaneous injection into the abdomen, upper arm, or thigh are standard sites. Each has slightly different absorption rates. Injecting into areas with more subcutaneous fat generally produces more consistent absorption. The GLP-1 injection site guide provides detailed instructions on optimal injection technique and site rotation.
Rotating injection sites prevents lipodystrophy, a localized change in fat tissue that can develop from repeated injections in the same spot. Lipodystrophy alters absorption characteristics, potentially causing inconsistent blood levels even with perfect dosing accuracy. The peptide injection fundamentals guide covers proper technique in comprehensive detail.
Syringe calibration
Not all insulin syringes are created equal. Cheaper syringes may have less precise markings or more dead space. BD (Becton Dickinson) and comparable medical-grade syringes offer the best precision for research applications. The investment in quality syringes pays for itself in dosing accuracy, especially when working with high-concentration formulations where small volume errors produce large dose variations.
Semaglutide with additives: does the conversion change?
Many compounded semaglutide formulations include additional ingredients. The most common additive is vitamin B12 (cyanocobalamin), but some pharmacies also add glycine, niacinamide, or other compounds. Does this change the unit-to-mg conversion for semaglutide?
No. The semaglutide concentration listed on the label already accounts for the presence of additives. If your vial reads "Semaglutide 2.5 mg / Cyanocobalamin 1 mg per mL," then 100 units still delivers 2.5 mg of semaglutide. The B12 comes along for the ride in that same volume, but it does not affect the semaglutide math.
The semaglutide with B12 comprehensive guide explains why B12 is commonly added (to help prevent the B12 deficiency that can accompany GLP-1 use) and what dosages are typical. The semaglutide with glycine guide covers another popular additive combination that some pharmacies offer.
The semaglutide B12 dosage chart provides unit-by-unit conversion tables specifically for combination formulations, so you can track both the semaglutide and B12 doses simultaneously. The methylcobalamin formulations page covers the alternative B12 form that some pharmacies use instead of cyanocobalamin.
Compounded vs. branded semaglutide: concentration differences that matter
The semaglutide market includes both FDA-approved branded products (Ozempic, Wegovy, Rybelsus) and compounded formulations from 503A and 503B pharmacies. Understanding the concentration differences between these categories prevents dangerous cross-calculation errors.
Branded product concentrations
Ozempic pens use concentrations of 1.34 mg/mL (for 0.25 mg, 0.5 mg, and 1 mg pens) and 2.68 mg/mL (for 2 mg pens). These concentrations are specific to the pen delivery system and are not found in any standard compounded vial. Wegovy uses single-dose pens where concentration is irrelevant to the user since each pen delivers one fixed dose.
Compounded concentrations
Compounding pharmacies typically produce semaglutide at 1 mg/mL, 2.5 mg/mL, or 5 mg/mL. Some specialty pharmacies offer 10 mg/mL for high-volume users who want to minimize injection volume. The Empower Pharmacy semaglutide guide, Olympia semaglutide guide, and Direct Meds semaglutide review each detail the specific concentrations and formulations offered by major compounding pharmacies.
Why this matters for 100-unit calculations
If a friend on a branded Ozempic pen tells you they take "1 mg weekly" and you try to replicate that from your compounded vial, you need YOUR vial concentration, not theirs. At 2.5 mg/mL, 1 mg requires 40 units. At 5 mg/mL, 1 mg requires 20 units. The prescribed dose in milligrams is transferable between products. The unit measurement is not.
Semaglutide vs. tirzepatide: do the conversions work the same way?
If you also use or are considering tirzepatide, you might wonder whether the same conversion math applies. The short answer is yes, the formula is identical. Units on an insulin syringe always measure volume. The concentration determines the mg per unit. The math works the same for any injectable peptide.
But the dosing protocols are completely different. Tirzepatide uses different mg targets (2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, 15 mg) and comes in different concentrations than semaglutide. The tirzepatide dosage in units guide covers the tirzepatide-specific conversions, and the semaglutide vs tirzepatide dosage chart provides a side-by-side comparison of both medications at various concentrations.
The switching from semaglutide to tirzepatide dosage chart and the semaglutide to tirzepatide conversion chart help researchers transition between these medications with accurate dose equivalencies. The tirzepatide 2.5 mg in units and tirzepatide 40 units to mg articles cover the most common tirzepatide conversion questions.
Building a safe dosing routine
Converting 100 units to milligrams is one calculation. Building a safe, repeatable dosing routine requires a system. Here is a protocol that experienced researchers follow to minimize errors.
Before each dose
Confirm your prescribed dose in milligrams. This is your anchor. Everything flows from here.
Verify your vial concentration. Read the label. Every time. Even if you think you know.
Calculate the units. Use the formula or a calculator. Write the number down.
Select the right syringe. Match syringe size to dose volume for optimal precision.
Inspect the solution. Clear and colorless means good. Anything else means stop.
During the draw
Swab the vial stopper with an alcohol pad. Let it dry.
Draw air equal to your dose volume into the syringe. Inject the air into the vial. This prevents a vacuum from forming.
Invert the vial and draw your calculated number of units.
Remove air bubbles. Flick, push, re-measure.
Verify the measurement one more time before withdrawing the needle from the vial.
After the injection
Record the dose in your log. Date, time, units drawn, concentration, milligrams administered, injection site.
Return the vial to the refrigerator immediately.
Dispose of the syringe in a proper sharps container.
This routine takes less than five minutes. It prevents the most common dosing errors. And it creates a record that helps you and your healthcare provider track your protocol over time. The complete peptide injections guide covers injection technique in greater detail, and the getting started with peptides article is an excellent resource for those new to injectable protocols.
When to contact your healthcare provider about dosing
Dose conversion math is something you can and should be able to do yourself. But certain situations require professional input.
Contact your healthcare provider if you suspect you have administered the wrong dose, if you experience symptoms that suggest overdose (severe nausea, persistent vomiting, abdominal pain, dizziness), if your vial concentration has changed and you are unsure about the new calculations, or if you have been prescribed a dose that seems unusually high or low compared to standard protocols.
Also reach out if you are not seeing expected results despite consistent dosing. The troubleshooting guide for weight loss stalls on semaglutide explores reasons beyond dosing errors that can affect outcomes, including diet, activity level, sleep, and metabolic factors. The semaglutide timeline guide sets realistic expectations for when results typically appear at each dose level.
For researchers navigating these questions independently, SeekPeptides provides comprehensive protocol resources, community support, and expert-reviewed dosing guides that cover the full spectrum of GLP-1 peptide use. Members access personalized protocol builders, detailed safety databases, and a community of experienced researchers who have navigated these exact situations.
Quick reference card: 100 units of semaglutide at every concentration
Print this. Keep it with your supplies. Reference it every time you have a question about what 100 units means for your specific vial.
Your Vial Concentration | 100 Units = | Is This a Normal Weekly Dose? |
|---|---|---|
0.68 mg/mL | 0.68 mg | Yes, within standard range |
1 mg/mL | 1.0 mg | Yes, month 3 dose |
1.34 mg/mL | 1.34 mg | Yes, within standard range |
2 mg/mL | 2.0 mg | Yes, near maintenance level |
2.5 mg/mL | 2.5 mg | Slightly above max (2.4 mg) |
2.68 mg/mL | 2.68 mg | Above max approved dose |
3 mg/mL | 3.0 mg | Above max approved dose |
5 mg/mL | 5.0 mg | SIGNIFICANT OVERDOSE |
10 mg/mL | 10.0 mg | DANGEROUS OVERDOSE |
The semaglutide reconstitution chart and 5 mg mixing chart complement this reference card with detailed reconstitution-specific tables. The 10 mg mixing chart covers the highest concentration formulations.
Frequently asked questions
Does 100 units always equal 1 mL on an insulin syringe?
Yes. On a standard U-100 insulin syringe, 100 units always equals 1 mL of liquid. This relationship between units and volume never changes. What changes is how many milligrams of semaglutide are dissolved in that 1 mL, which depends on the concentration of your specific vial.
Is 100 units of semaglutide safe to inject?
It depends entirely on your vial concentration and your current dose level. At 1 mg/mL, 100 units equals just 1 mg, a moderate dose within normal protocols. At 5 mg/mL, 100 units equals 5 mg, which is more than double the maximum approved weekly dose and would be considered an overdose. Always calculate the milligrams before determining if a dose is appropriate.
Why do different semaglutide vials have different concentrations?
Different concentrations serve different practical needs. Lower concentrations like 1 mg/mL allow for easier measurement of small doses but require larger injection volumes. Higher concentrations like 5 mg/mL reduce injection volume but require more precise measurements. Compounding pharmacies offer various concentrations to match different patient needs and dosing protocols. The compounded semaglutide guide explains the full range of available formulations.
Can I use an Ozempic pen conversion chart for my compounded semaglutide vial?
No. Ozempic pens use unique concentrations (1.34 mg/mL and 2.68 mg/mL) that do not match standard compounded vial concentrations. Using pen-specific conversion data for a vial will produce incorrect unit measurements. Always use a conversion chart that matches your exact vial concentration.
What if I accidentally injected 100 units from a 5 mg/mL vial?
Contact your healthcare provider or poison control (1-800-222-1222) immediately. A 5 mg dose is more than double the maximum approved weekly dose. Symptoms may include severe nausea, vomiting, and potentially dangerous hypoglycemia. Since semaglutide has a week-long half-life, there is no quick reversal, but medical professionals can manage symptoms with IV fluids and anti-nausea medications.
How do I know my compounded semaglutide concentration?
The concentration is printed on the vial label, typically expressed as mg/mL (e.g., "Semaglutide 2.5 mg/mL"). If the label shows total content (e.g., "5 mg / 2 mL"), divide the mg by the mL to get concentration (5 / 2 = 2.5 mg/mL). If you cannot find or read the concentration, contact your pharmacy before using the vial.
Does adding B12 to semaglutide change the unit conversion?
No. The semaglutide concentration on the label already accounts for any additives. A vial labeled "Semaglutide 2.5 mg / Cyanocobalamin 1 mg per mL" still delivers 2.5 mg of semaglutide per 100 units. The B12 is included in the same volume and does not affect semaglutide calculations. See the semaglutide with B12 guide for more details.
Is there a difference between semaglutide units and insulin units?
Yes, conceptually. Insulin units represent a standardized biological activity (1 unit of insulin has a specific glucose-lowering effect). Semaglutide "units" on an insulin syringe are purely a volume measurement (1 unit = 0.01 mL). The syringe itself does not know what liquid it contains. This is why you must always calculate the actual milligrams of semaglutide based on your vial concentration.
External resources
For researchers serious about optimizing their semaglutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, personalized dosing calculators, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay accurate, your conversions stay precise, and your protocols stay consistent.