Feb 22, 2026

Before you draw up your next dose, read this carefully. The FDA has documented cases of patients injecting five to twenty times more semaglutide than intended, all because of a simple unit conversion mistake. Hospitalizations followed. Some cases involved providers who miscalculated. Others involved patients who confused milligrams with units on an insulin syringe. The difference between getting your 1 mg dose right and getting it dangerously wrong comes down to one number: your vial concentration.
That is what this guide exists to solve.
The answer to "how many units is 1 mg of semaglutide" is not a single number. It changes based on the concentration of your specific vial. At a 5 mg/mL concentration, 1 mg equals 20 units. At 2.5 mg/mL, it equals 40 units. At 10 mg/mL, it equals just 10 units. Get the concentration wrong and you could inject two, four, or even ten times your intended dose. This guide walks through every concentration, the exact formula, step-by-step syringe measurement instructions, and the critical safety checks that prevent the dosing errors the FDA keeps warning about. Whether you are working with a compounded semaglutide vial or a branded product, the math matters more than most people realize. And getting it right is not optional.
The quick answer: 1 mg of semaglutide in units
Here is the direct answer. The number of units in 1 mg of semaglutide depends entirely on the concentration printed on your vial. There is no universal conversion. Every concentration produces a different unit count for the same milligram dose.
For the most common concentrations:
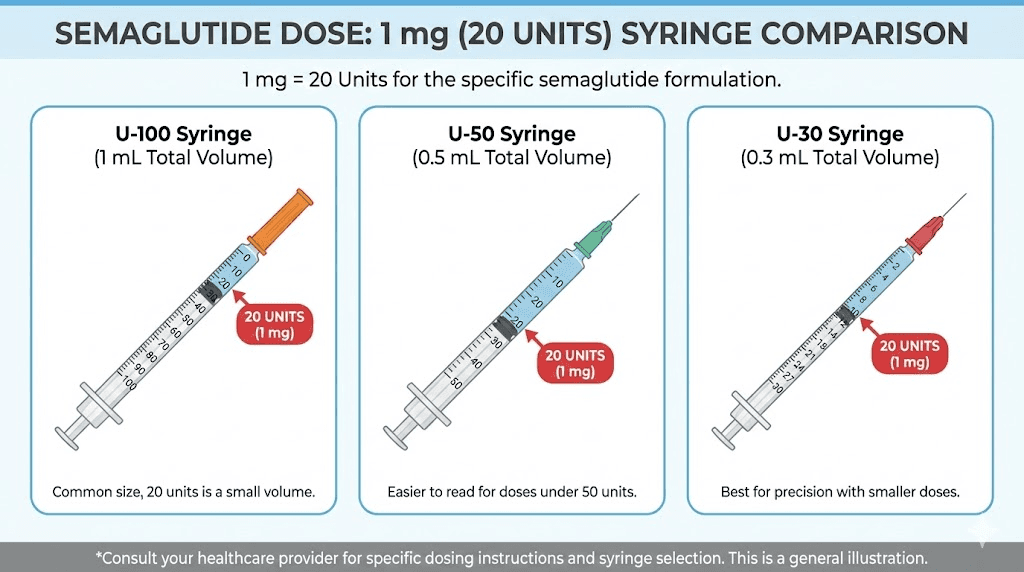
5 mg/mL concentration: 1 mg = 20 units
2.5 mg/mL concentration: 1 mg = 40 units
10 mg/mL concentration: 1 mg = 10 units
2 mg/mL concentration: 1 mg = 50 units
1 mg/mL concentration: 1 mg = 100 units
3 mg/mL concentration: 1 mg = approximately 33 units
That range, from 10 units to 100 units for the exact same dose, explains why dosing errors happen so frequently. Someone switching from a 5 mg/mL vial to a 2.5 mg/mL vial needs to double their unit count. Miss that adjustment and you get half the intended dose. Or worse, someone going the other direction gets double. This is why understanding the semaglutide dosage in units relationship to concentration is fundamental to safe dosing.
If you want to verify your conversion before drawing up any dose, the SeekPeptides semaglutide dosage calculator handles the math automatically. Enter your concentration and desired dose, and it returns the exact units to draw.
Why concentration is the only variable that matters
People search for "how many units is 1 mg of semaglutide" expecting a simple answer. One number. Done. But semaglutide does not work like insulin, where U-100 means 100 units always equals 1 mL. With semaglutide, the concentration of the solution determines everything about how you measure your dose.
Think of it this way. You have a cup of coffee. A weak brew might have 50 mg of caffeine per cup. A strong espresso might have 150 mg in the same volume. The cup size did not change. The concentration did. Semaglutide works the same way. A 5 mg/mL vial packs twice as much medication per milliliter as a 2.5 mg/mL vial. So you need half the volume to get the same dose.
Units on an insulin syringe measure volume, not drug content. Each unit on a U-100 syringe equals 0.01 mL. That never changes regardless of what medication fills the syringe. When you draw 20 units, you are drawing 0.2 mL of liquid. What varies is how much semaglutide sits inside that 0.2 mL, and that depends on the concentration. This concept trips up even experienced practitioners, which is why the semaglutide dosage conversion chart exists as a reference tool.
How concentration gets determined
If you receive an FDA-approved pen like Ozempic or Wegovy, concentration is predetermined. You do not need to think about it. The pen delivers the prescribed milligram dose automatically. The conversion question only matters when using a vial and syringe, which is the standard format for compounded semaglutide products.
Compounding pharmacies prepare semaglutide at various concentrations depending on their formulation. Some pharmacies standardize at 5 mg/mL. Others use 2.5 mg/mL, 2 mg/mL, or even custom concentrations. The concentration is always printed on the vial label, usually expressed as milligrams per milliliter (mg/mL). Before drawing any dose, you must identify this number. Without it, accurate dosing is impossible.
Your pharmacy should provide dosing instructions specific to your vial concentration. If they did not, contact them before your next injection. This is not something to guess about. The guide to semaglutide injection with a syringe covers the full administration process if you need a visual walkthrough.
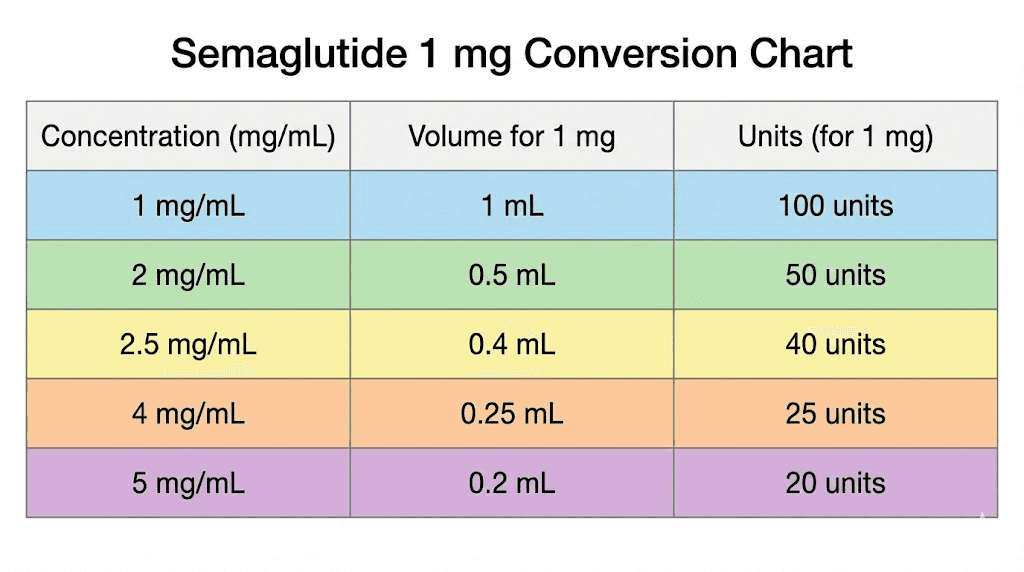
Complete conversion table: 1 mg at every common concentration
Here is the comprehensive reference table for converting 1 mg of semaglutide to insulin syringe units across all concentrations currently available from compounding pharmacies and reconstituted research vials. Keep this table accessible whenever you prepare a dose.
Concentration (mg/mL) | Volume for 1 mg | Units on U-100 syringe | Common source |
|---|---|---|---|
1 mg/mL | 1.0 mL | 100 units | Dilute reconstitution |
2 mg/mL | 0.5 mL | 50 units | Some compounding pharmacies |
2.5 mg/mL | 0.4 mL | 40 units | Common compounded format |
3 mg/mL | 0.33 mL | 33 units | Select compounding pharmacies |
5 mg/mL | 0.2 mL | 20 units | Most common compounded format |
10 mg/mL | 0.1 mL | 10 units | High concentration vials |
Notice the pattern. As the concentration doubles, the units needed get cut in half. A 10 mg/mL vial requires only 10 units for 1 mg, while a 1 mg/mL vial requires 100 units for the same milligram dose. The medication amount is identical. Only the volume changes.
For related dosage conversions at other milligram amounts, these references cover the math in detail: 20 units of semaglutide in mg, 10 units of semaglutide in mg, 100 units of semaglutide in mg, and 40 units of semaglutide in mg. Each one explains the conversion specific to common concentrations so you can cross-reference your own setup.
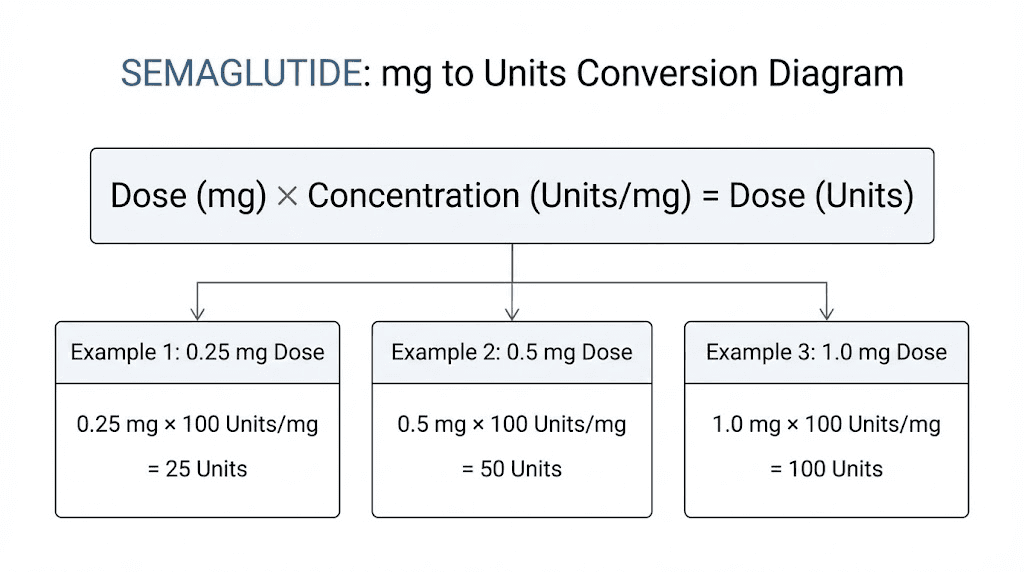
The universal formula for converting mg to units
Every conversion in this article comes from one formula. Memorize it and you can convert any semaglutide dose at any concentration without a chart.
Units = (desired dose in mg / concentration in mg/mL) x 100
That is it. Three numbers. One division. One multiplication. The result tells you exactly how many units to draw on your insulin syringe.
Breaking down the formula step by step
Let us walk through it with the 1 mg dose at a 5 mg/mL concentration.
Step 1: Identify your desired dose. In this case, 1 mg.
Step 2: Identify the concentration on your vial label. Here, 5 mg/mL.
Step 3: Divide the dose by the concentration. 1 mg divided by 5 mg/mL equals 0.2 mL.
Step 4: Multiply by 100 to convert milliliters to units. 0.2 mL times 100 equals 20 units.
So 1 mg from a 5 mg/mL vial equals 20 units on a U-100 insulin syringe. The peptide calculator performs this calculation automatically if you prefer a digital tool, and the reconstitution calculator helps if you are working with lyophilized powder that needs mixing first.
Why we multiply by 100
This step confuses some people. The multiplication by 100 exists because standard U-100 insulin syringes are calibrated so that 100 units equals 1 mL. That is their design specification. When you divide milligrams by concentration, you get milliliters. Multiplying by 100 converts those milliliters into the unit markings printed on the syringe.
If you were using a different syringe calibration, say a 0.5 mL syringe marked in 0.01 mL increments, you would skip the multiplication and work directly in milliliters. But since most semaglutide users rely on U-100 insulin syringes, the x100 conversion is standard practice.
Applying the formula to other doses
The formula works for every dose in the semaglutide dosage chart, not just 1 mg. Here is how it applies across the standard titration schedule at a 5 mg/mL concentration:
0.25 mg: 0.25 / 5 x 100 = 5 units (see 0.25 mg conversion guide)
0.5 mg: 0.5 / 5 x 100 = 10 units
1.0 mg: 1.0 / 5 x 100 = 20 units
1.7 mg: 1.7 / 5 x 100 = 34 units (see 1.7 mg conversion guide)
2.4 mg: 2.4 / 5 x 100 = 48 units (see 2.4 mg conversion guide)
The math stays consistent. Change the concentration and the numbers shift proportionally. For a 5 mg/mL dosage chart with all doses pre-calculated, or the 10 mg dosage chart for higher concentration vials, those guides lay everything out in table format.
How to identify your vial concentration
Your vial label contains every piece of information you need. But labels vary between pharmacies, and the critical number can sometimes blend into the surrounding text. Here is exactly what to look for.
Reading the vial label
The concentration appears in one of these formats:
"Semaglutide 5 mg/mL" printed directly on the label
"5 mg per mL" spelled out
"Total: 5 mg in 1 mL" showing total content and volume
"10 mg / 2 mL" showing total content per total volume (divide to get 5 mg/mL)
The last format requires a simple division. A vial labeled "10 mg / 2 mL" contains 5 mg per mL. A vial labeled "5 mg / 2 mL" contains 2.5 mg per mL. Always reduce the fraction to get the per-milliliter concentration before plugging it into the conversion formula. If you are working with a 5 mg vial, the concentration depends on the total volume of liquid in the vial.
Some compounding pharmacies also include the total number of doses per vial and the volume per dose. This can help you double-check your math. If the label says "20 doses at 0.25 mg each" from a vial with 2 mL total, you know the concentration is 5 mg / 2 mL = 2.5 mg/mL.
What if your label shows two concentrations
Vials containing semaglutide combined with B12 or semaglutide with methylcobalamin will list concentrations for both active ingredients. The semaglutide concentration is the one that matters for dosing. B12 concentration is secondary and does not affect how many units you draw for your semaglutide dose.
A typical label might read: "Semaglutide 5 mg/mL with Cyanocobalamin 1 mg/mL." Use 5 mg/mL for all your semaglutide calculations. The B12 comes along for the ride in whatever volume you draw.
Reconstituted vials from powder
If you reconstituted semaglutide from powder, your concentration depends on how much bacteriostatic water you added. A 5 mg vial reconstituted with 2 mL of bacteriostatic water gives you 2.5 mg/mL. The same vial reconstituted with 1 mL gives you 5 mg/mL. This is why tracking your reconstitution ratio is critical.
The semaglutide reconstitution chart maps out exact concentrations based on powder amount and water volume. For a 5 mg reconstitution chart or 10 mg reconstitution chart, those guides provide every combination you might encounter. And if you need to figure out how much water to add in the first place, the bacteriostatic water mixing guide for 10 mg and the 5 mg mixing guide walk through the process.
Common compounding pharmacy concentrations
Not all pharmacies prepare semaglutide the same way. The concentration you receive depends on which pharmacy fills your prescription, and sometimes on the specific formulation your provider orders. Here is what the major compounding pharmacies typically provide.
5 mg/mL (the most common)
This is the concentration you will encounter most frequently. It is the standard for many large compounding operations. At this concentration, 1 mg of semaglutide equals exactly 20 units. The math is clean and the injection volumes stay small, which is why pharmacies favor this concentration.
The 5 mg/2 mL dosage chart provides the complete dose escalation in units for this common vial format. If your pharmacy is Empower Pharmacy, they typically use formulations around this concentration range, sometimes combined with cyanocobalamin.
2.5 mg/mL
The second most common concentration. At 2.5 mg/mL, 1 mg equals 40 units. This concentration appears frequently in formulations that combine semaglutide with other compounds like glycine or B12, where the additional ingredients occupy volume in the solution.
Some providers prefer this concentration for patients on lower doses because it provides more precise measurement. Drawing 10 units for 0.25 mg is easier to be accurate with than drawing 5 units from a 5 mg/mL vial, where a small measurement error represents a larger percentage of the dose.
10 mg/mL and higher
High-concentration vials save space and reduce injection volume, but they demand extreme precision. At 10 mg/mL, 1 mg is only 10 units. A single unit of measurement error at this concentration means a 10% dose variation, compared to just 2.5% at a 2.5 mg/mL concentration. The 10 mg vial dosage chart details every dose step for this concentration.
If you are working with high-concentration vials, consider using a syringe with finer graduations. Half-unit syringes allow more precise measurement when the total unit count is low.
Custom concentrations
Some pharmacies like Olympia Pharmacy, Direct Meds, and BPI Labs may prepare formulations at non-standard concentrations. Always use the actual concentration listed on your specific vial, not a general chart you found online. The semaglutide syringe dosage chart covers the mathematics for any concentration you might encounter.
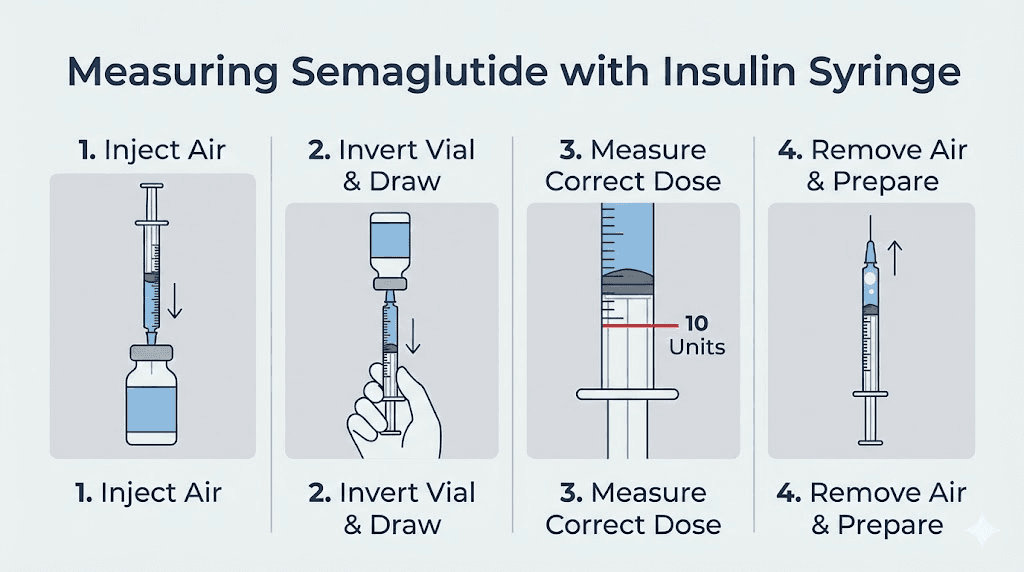
Step-by-step guide to measuring 1 mg with an insulin syringe
The conversion formula gives you the number. Now here is how to actually measure it accurately with a U-100 insulin syringe. Accuracy at this stage prevents the dosing errors that land people in emergency rooms.
What you need
Your semaglutide vial with known concentration
A U-100 insulin syringe (verify "U-100" on the packaging)
Alcohol swabs
Your calculated unit count for 1 mg
The measurement process
Step 1: Confirm your concentration. Read the vial label. Identify the mg/mL value. If the label shows total content and total volume (like "10 mg in 2 mL"), divide to get the per-mL concentration.
Step 2: Calculate your units. Use the formula: 1 mg divided by your concentration, multiplied by 100. For a 5 mg/mL vial, that is 1 / 5 x 100 = 20 units. Write this number down. Do not rely on memory.
Step 3: Clean the vial stopper. Wipe the rubber stopper with an alcohol swab and let it dry for a few seconds.
Step 4: Draw air into the syringe. Pull the plunger back to the same unit marking as your dose (20 units for our example). This air injection prevents a vacuum from forming in the vial.
Step 5: Insert the needle and inject air. Push the needle through the rubber stopper and inject the air into the vial.
Step 6: Invert the vial. Turn the vial upside down with the needle still inserted. The syringe should now point upward.
Step 7: Draw the medication. Pull the plunger back slowly to your target unit marking. For 1 mg at 5 mg/mL, pull to the 20-unit line.
Step 8: Check for air bubbles. Tap the syringe gently to move any bubbles to the top. Push the plunger slightly to expel the air, then readjust to your target units if needed.
Step 9: Verify the dose. Hold the syringe at eye level. Confirm the bottom of the plunger rubber stopper aligns exactly with your target unit marking. Not above. Not below. Exactly on the line.
For a full visual walkthrough of this entire process, the semaglutide injection guide covers each step with detailed explanations. And for choosing where to inject, the best injection sites guide covers optimal locations on the abdomen, thigh, and upper arm.
Critical accuracy tips
Small measurement errors at the syringe level can create meaningful dose variations. Here is how to stay precise.
Read the syringe at eye level. Looking down at the syringe creates parallax error. The fluid line appears different depending on your viewing angle. Hold it horizontal at eye height for accurate reading.
Use the right syringe size. If your dose is 20 units, a 0.3 mL (30-unit) syringe gives better precision than a 1 mL (100-unit) syringe because the graduation marks are more spread out. Match syringe capacity to dose size when possible.
Read the bottom of the plunger. The rubber stopper on the plunger has a dome shape. Always read the measurement from the flat bottom edge of the stopper, not the curved top edge. This distinction matters more than most people realize.
Temperature also plays a role in accurate dosing. If you just pulled your vial from the refrigerator, the solution may be slightly thicker and harder to draw. Let it sit at room temperature for 15 to 30 minutes before drawing your dose. For storage guidance, the semaglutide storage guide and refrigeration requirements explain proper handling.
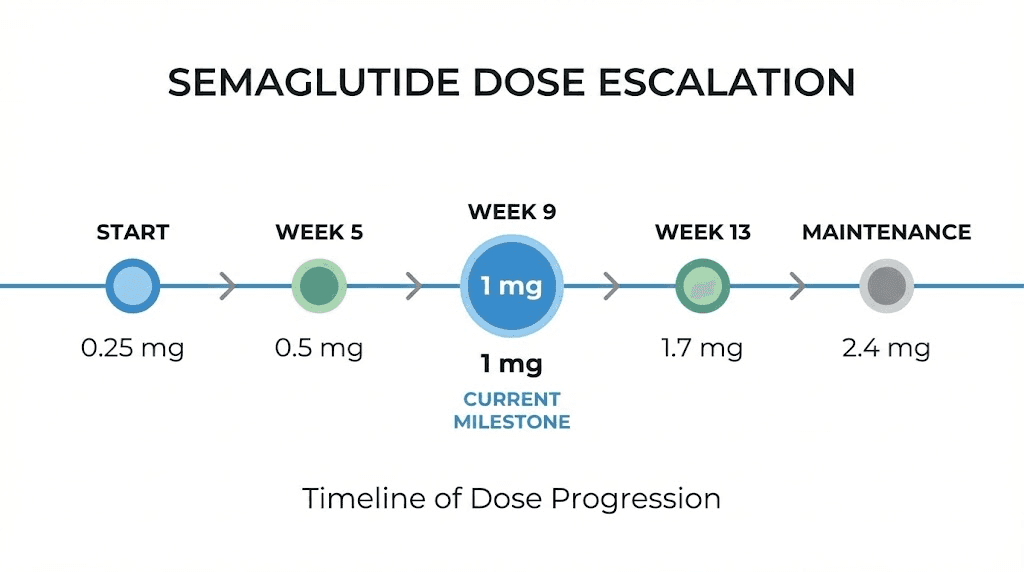
Where 1 mg falls in the standard dose escalation schedule
The 1 mg dose is not where you start. It sits at the midpoint of the standard semaglutide titration schedule, typically reached during weeks 9 through 12. Understanding where it falls in the full escalation helps you plan ahead and know what doses come before and after.
The standard Wegovy titration schedule
Weeks | Weekly dose | Units at 5 mg/mL | Units at 2.5 mg/mL | Phase |
|---|---|---|---|---|
1-4 | 0.25 mg | 5 units | 10 units | Starting dose |
5-8 | 0.5 mg | 10 units | 20 units | First escalation |
9-12 | 1.0 mg | 20 units | 40 units | Second escalation |
13-16 | 1.7 mg | 34 units | 68 units | Third escalation |
17+ | 2.4 mg | 48 units | 96 units | Maintenance dose |
At 1 mg, you have completed the initial loading phases and entered a dose level where most people begin noticing meaningful appetite suppression and early weight changes. The jump from 0.5 mg to 1 mg is a doubling of the dose, the largest percentage increase in the entire titration schedule. Some people experience increased side effects at this transition point. Others sail through it without noticing any difference.
For a deep dive into how fast semaglutide works at each dose level, that guide covers the timeline from first injection through maintenance. And if you are wondering how long it takes to see results, the answer varies significantly based on individual response and dose level.
The Ozempic schedule (for diabetes)
The Ozempic titration for type 2 diabetes management follows a slightly different pattern:
Weeks 1-4: 0.25 mg weekly
Weeks 5-8: 0.5 mg weekly
Week 9+: 1.0 mg weekly (may increase to 2.0 mg if needed)
Under this schedule, 1 mg serves as the primary maintenance dose for many patients. It represents the standard therapeutic level for glycemic control, with 2.0 mg reserved for those who need additional efficacy. The semaglutide dosing chart in units maps out both schedules side by side.
Compounded semaglutide escalation
Providers prescribing compounded semaglutide sometimes modify the standard escalation. Some start at lower doses, some extend time between increases, and some cap the maximum dose below 2.4 mg based on patient response. The 1 mg level remains a common milestone in most modified schedules because it represents a clinically meaningful dose where efficacy and tolerability typically balance well.
If you are curious about the compounded semaglutide with B12 dosage schedule, that chart accounts for the specific concentrations these combined formulations use.
What to expect when you reach the 1 mg dose level
Reaching 1 mg is a significant step in the semaglutide journey. This dose represents four times the starting amount and is where many people report the first substantial changes in appetite, cravings, and early weight loss. Here is what the research and clinical experience show.
Appetite suppression at 1 mg
Most users report noticeable appetite reduction by the 1 mg dose. The timeline for appetite suppression varies by individual, but many report that the jump from 0.5 mg to 1 mg is where food noise significantly decreases. Meals feel more satisfying with smaller portions. The constant background chatter about food quiets down.
Does this happen immediately at 1 mg? Not always. The appetite suppression timeline depends on individual GLP-1 receptor sensitivity, body composition, and metabolic factors. Some people feel it within days of their first 1 mg injection. Others need two or three weekly doses at this level before the full effect develops.
Common side effects at this dose
The transition to 1 mg triggers side effects in some people, particularly gastrointestinal symptoms. Nausea is the most frequently reported, usually mild and temporary. It tends to peak 24 to 72 hours after injection and resolve before the next weekly dose.
Other potential side effects at this dose level include constipation, fatigue, dizziness, excessive burping, and sleep disruption. These typically diminish over two to four weeks as the body adjusts. If side effects persist or become severe, your provider may recommend staying at 1 mg longer before escalating, or even temporarily reducing back to 0.5 mg.
The semaglutide vs tirzepatide side effects comparison provides context if you are weighing these medications against each other. And if you experience a plateau at this dose level, the semaglutide plateau guide covers strategies for breaking through.
Expected weight loss at 1 mg
Clinical trials show that even sub-maximal doses of semaglutide produce meaningful weight loss. The STEP trials demonstrated an average of 14.9% body weight loss at the full 2.4 mg maintenance dose over 68 weeks. At the 1 mg level, which patients typically pass through during weeks 9-12, early weight loss of 3-5% from baseline is common.
Individual results vary widely. The one-month results guide sets realistic expectations for the early stages, while the before and after overview shows what longer-term outcomes look like. If you are not seeing expected results, the troubleshooting guide for weight loss stalls and the four weeks without weight loss guide address the most common reasons and solutions.
Diet and lifestyle at the 1 mg level
Semaglutide works best alongside appropriate nutrition. At the 1 mg dose, you may find your food preferences shifting. Greasy and heavy foods become less appealing for many people. Lean proteins, vegetables, and lighter meals tend to sit better.
The semaglutide diet plan outlines a nutrition approach designed to complement the medication. For specific food guidance, the recommended foods list and the foods to avoid guide help optimize your results. Exercise is not strictly required for weight loss on semaglutide, as the guide on results without exercise explains, but it does improve body composition outcomes.
FDA warnings: dosing errors that put patients in the hospital
This is not hypothetical. The FDA has issued specific warnings about dosing errors with compounded semaglutide, and the numbers are alarming. Understanding what went wrong in these cases protects you from making the same mistakes.
The scope of the problem
In July 2024, the FDA documented cases where patients administered five to twenty times more than their intended semaglutide dose. A study published in the Journal of the American Pharmacists Association examined cases reported to a poison control center and found a pattern of administration errors specifically with compounded semaglutide products. The errors fell into several categories.
Provider miscalculation was one major source. In documented cases, a provider intending to prescribe 0.25 mg (5 units at 5 mg/mL) accidentally wrote 25 units, delivering 1.25 mg instead. A five-fold overdose from a single decimal error.
Patient confusion was equally common. Patients unfamiliar with insulin syringes drew the wrong number of units, either misreading the syringe markings or using the wrong syringe type entirely. Some patients confused milligrams with units directly, drawing 100 units when they meant 1 mg, resulting in massive overdoses at certain concentrations.
Why compounded semaglutide carries higher risk
FDA-approved pens like Ozempic and Wegovy have built-in safety mechanisms. The pen dial clicks to preset doses. You cannot physically set the wrong milligram amount because the device constrains your options. Compounded semaglutide in vials has none of these safeguards. The vial holds medication. The syringe has markings. The conversion happens entirely in your head or on paper.
This is precisely why getting the concentration-to-units conversion right matters so much. When someone asks "how many units is 1 mg of semaglutide," they are asking the exact question that, if answered incorrectly, leads to the errors the FDA documented. For safe dosing practices and a complete overview of peptide safety considerations, building a systematic approach to dose verification is essential.
How to protect yourself
Triple-check every dose conversion before drawing medication. Write the calculation on paper. Use the semaglutide dosage calculator to verify your math. Ask your pharmacist to confirm the unit count for each dose level at your specific concentration. Never assume. Never round. Never guess.
If you ever receive a new vial with a different concentration than your previous one, recalculate everything from scratch. Do not carry forward unit counts from an old vial. A different concentration means different units for every single dose level. SeekPeptides emphasizes this point in every dosing guide because concentration awareness is the single most important safety factor in semaglutide administration.
Converting every semaglutide dose to units at common concentrations
The 1 mg conversion is just one piece of the full picture. Here is the complete dose escalation converted to units for the three most common compounding concentrations. Bookmark this section or print it out for your reference.
Full conversion table: 5 mg/mL concentration
Dose (mg) | Volume (mL) | Units | Phase |
|---|---|---|---|
0.25 | 0.05 | 5 | Starting (Weeks 1-4) |
0.5 | 0.10 | 10 | Escalation 1 (Weeks 5-8) |
1.0 | 0.20 | 20 | Escalation 2 (Weeks 9-12) |
1.7 | 0.34 | 34 | Escalation 3 (Weeks 13-16) |
2.4 | 0.48 | 48 | Maintenance (Week 17+) |
At 5 mg/mL, unit counts stay low and manageable. Even the maximum 2.4 mg maintenance dose requires only 48 units, well within the range of a standard 0.5 mL insulin syringe. This concentration is the easiest to work with for most patients, which is why it is the most commonly prescribed. For a printable version of this chart, the syringe dosage conversion chart provides a clean reference format.
Full conversion table: 2.5 mg/mL concentration
Dose (mg) | Volume (mL) | Units | Phase |
|---|---|---|---|
0.25 | 0.10 | 10 | Starting (Weeks 1-4) |
0.5 | 0.20 | 20 | Escalation 1 (Weeks 5-8) |
1.0 | 0.40 | 40 | Escalation 2 (Weeks 9-12) |
1.7 | 0.68 | 68 | Escalation 3 (Weeks 13-16) |
2.4 | 0.96 | 96 | Maintenance (Week 17+) |
Notice how the 2.5 mg/mL concentration nearly maxes out a standard 1 mL (100-unit) insulin syringe at the 2.4 mg maintenance dose. At 96 units, you are close to the syringe capacity, which leaves very little room for error. If you are on the maintenance dose with this concentration, a 1 mL syringe is appropriate, but you need to be extremely precise. The dosage chart in mL provides an alternative way to think about these measurements.
Full conversion table: 10 mg/mL concentration
Dose (mg) | Volume (mL) | Units | Phase |
|---|---|---|---|
0.25 | 0.025 | 2.5 | Starting (Weeks 1-4) |
0.5 | 0.05 | 5 | Escalation 1 (Weeks 5-8) |
1.0 | 0.10 | 10 | Escalation 2 (Weeks 9-12) |
1.7 | 0.17 | 17 | Escalation 3 (Weeks 13-16) |
2.4 | 0.24 | 24 | Maintenance (Week 17+) |
The 10 mg/mL concentration creates a unique challenge. The starting dose of 0.25 mg requires only 2.5 units. Most insulin syringes do not have half-unit markings at every position, making this measurement difficult without a specialized syringe. For starting doses with high-concentration vials, ask your pharmacy about half-unit syringes. The 10 mg semaglutide dosage chart addresses these precision challenges in detail.
If you are also tracking tirzepatide dosage in units or comparing the two medications, the semaglutide vs tirzepatide dosage chart shows both conversion tables side by side for direct comparison. And the comprehensive comparison page covers efficacy, side effects, and dosing differences between the two.
Tips for accurate semaglutide dosing every time
Consistent dosing separates people who get reliable results from those who wonder why their progress stalls. These practical tips come from clinical experience and the most common errors documented in research settings.
Create a dosing reference card
Write your specific conversion on a card and keep it with your supplies. Include:
Your vial concentration
Your current dose in milligrams
The exact number of units to draw
Your injection day and preferred time
Update this card every time your dose changes or you receive a vial with a different concentration. This eliminates the need to recalculate from memory before each injection, which is when errors happen. The best time of day to take semaglutide guide can help you optimize your injection timing for minimal side effects.
Use the same syringe type consistently
Switching between syringe sizes creates confusion. A 0.3 mL syringe, a 0.5 mL syringe, and a 1 mL syringe all measure in units, but the physical spacing between markings differs. If you are used to drawing 20 units on a 0.3 mL syringe and switch to a 1 mL syringe, the 20-unit mark sits in a very different position. This visual change can cause measurement errors even when the mathematical conversion has not changed.
Pick one syringe size that works for your dose range and stick with it.
Verify before every injection
Even after months of consistent dosing, verify your unit count before drawing each dose. Complacency creates errors. The moment you stop checking is the moment a mistake slips through. This takes ten seconds and prevents the kind of errors that take days to recover from.
Check the vial label, confirm the concentration has not changed, run the quick mental calculation or glance at your reference card, and then draw. Every time. No exceptions. SeekPeptides members access detailed dosing protocols and verification checklists that build these safety habits into every administration routine.
Store your vials properly
Improper storage can affect semaglutide potency, which indirectly affects dosing accuracy. If the medication degrades, you may not receive the full intended dose even if your unit measurement is perfect.
Refrigerate your vials between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius). The semaglutide refrigerator storage guide covers optimal conditions, while the shelf life guide explains how long your vial remains effective. If your vial was accidentally left out, the temperature exposure guide explains whether it is still usable. And if you are uncertain about the expected appearance of your semaglutide, that reference helps you identify normal versus compromised solution.
For travel, the traveling with semaglutide guide covers cold chain maintenance during trips.
When to adjust from the 1 mg dose
Reaching 1 mg does not mean staying there forever. The standard protocol involves continued escalation toward the maintenance dose. But clinical reality often deviates from standard protocols. Here is how to think about dose adjustments around the 1 mg level.
When to move up from 1 mg
The standard schedule calls for escalation to 1.7 mg after four weeks at 1 mg. However, this timeline assumes you are tolerating the current dose well. If you are experiencing significant nausea, vomiting, or other gastrointestinal side effects at 1 mg, your provider may recommend staying at this dose for an additional two to four weeks before escalating.
Some patients find that 1 mg provides sufficient appetite suppression and weight loss without the need for higher doses. In these cases, providers may keep the dose at 1 mg indefinitely. The right dose is the lowest effective dose, not necessarily the maximum dose. The long-term semaglutide guide discusses treatment duration and dose optimization strategies.
When to step back from 1 mg
If side effects are unmanageable at 1 mg, dropping back to 0.5 mg for a few weeks and then reattempting the increase is a standard approach. This gives your GLP-1 receptors more time to adapt. The withdrawal symptoms guide is relevant if you need to pause treatment entirely, though temporary dose reduction does not typically produce withdrawal effects.
If 1 mg stops working
Some patients experience a plateau at the 1 mg dose where initial weight loss slows or stops. This does not necessarily mean the medication has stopped working. Metabolic adaptation, dietary changes, and fluid balance all influence the scale. Before concluding that the dose is insufficient, review the plateau troubleshooting guide and ensure nutritional and lifestyle factors are optimized.
If true efficacy reduction occurs, escalation to 1.7 mg typically restores progress. Some patients may consider switching medications entirely. The transition guide between medications and the conversion chart for switching cover that process.
Understanding insulin syringes and unit markings
Confusion about insulin syringe units is the root cause of most semaglutide dosing errors. Understanding how these syringes actually work eliminates an entire category of potential mistakes.
What "units" actually mean on an insulin syringe
On a U-100 insulin syringe, the term "units" originally referred to insulin units, where 100 units equals 100 international units of insulin in 1 mL. But when you use the same syringe for semaglutide, "units" become purely a volume measurement. Each unit equals 0.01 mL. That is all.
Semaglutide does not have "units" in the way insulin does. Semaglutide is dosed in milligrams. When people say "20 units of semaglutide," they mean 0.2 mL of solution drawn in a U-100 insulin syringe. The medication content of that 0.2 mL depends on the concentration.
This distinction is crucial. The semaglutide units to mg guide explains this relationship in depth, and the units to mL conversion guide makes the volume relationship explicit.
Common syringe sizes
Three insulin syringe sizes cover most semaglutide dosing needs:
0.3 mL syringe (30 units max): Best for doses up to 1.5 mg at 5 mg/mL concentration. The graduation marks are widely spaced, making precise measurement easier. Ideal for the 1 mg dose at 5 mg/mL (20 units).
0.5 mL syringe (50 units max): Covers the full dose escalation up to 2.5 mg at 5 mg/mL. Good all-purpose choice if you plan to escalate through the entire standard schedule.
1.0 mL syringe (100 units max): Necessary for lower concentrations at higher doses. Required for the 2.4 mg maintenance dose at 2.5 mg/mL (96 units). Graduation marks are more compressed, so extra care is needed for accuracy.
For more on understanding the relationship between 50 units and mg or checking whether 20 units is too much for your situation, those guides address specific unit count concerns.
Half-unit syringes
Some manufacturers produce insulin syringes with half-unit markings. These are valuable when your calculated dose falls between whole unit numbers. At a 10 mg/mL concentration, the starting dose of 0.25 mg requires 2.5 units, which is impossible to measure accurately on a standard syringe without half-unit marks.
Ask your pharmacy about half-unit syringe availability if your concentration requires fractional unit doses.
Other semaglutide dose conversions you should know
While this guide focuses on the 1 mg conversion, understanding the full spectrum of dose-to-unit relationships helps you manage your entire treatment course. Here is a quick reference for every standard dose, with links to dedicated guides for each.
Starting dose: 0.25 mg
At 5 mg/mL, 0.25 mg equals just 5 units. This is the smallest dose in the standard escalation and the one most prone to measurement error because a single unit off represents a 20% dose variation. The complete 0.25 mg conversion guide covers this dose at every concentration. Precision matters most here.
First escalation: 0.5 mg
At 5 mg/mL, 0.5 mg equals 10 units. Double the starting dose. Most people tolerate this increase without issues, and the additional 5 units on the syringe are easy to measure accurately. The dosage chart in units includes this and all other dose levels.
Third escalation: 1.7 mg
At 5 mg/mL, 1.7 mg equals 34 units. This is where some people first encounter the 1.7 mg unit conversion challenge. The 34-unit mark may not align perfectly with major graduation lines on all syringes, so counting individual unit marks carefully is important.
Maintenance dose: 2.4 mg
At 5 mg/mL, 2.4 mg equals 48 units. This is the full maintenance dose for weight management. The 2.4 mg conversion guide provides the complete breakdown and tips for measuring this dose accurately with different syringe sizes.
If you are tracking the semaglutide with B12 dosage chart, the conversion math remains the same. The B12 component does not change how many units you draw for your semaglutide dose.
Comparing semaglutide dosing to other GLP-1 medications
If you are considering or switching between GLP-1 receptor agonists, understanding how semaglutide dosing compares to alternatives helps contextualize where the 1 mg dose sits in the broader treatment landscape.
Semaglutide vs tirzepatide dosing
Tirzepatide follows its own dose escalation: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, and 15 mg. The milligram amounts are higher, but the receptor affinity and mechanism differ. Comparing 1 mg of semaglutide to 5 mg of tirzepatide is not a direct equivalence, but they sit at roughly comparable points in their respective escalation schedules.
For those exploring tirzepatide dosing in units, the conversion math uses the same formula. The semaglutide to tirzepatide conversion chart maps approximate therapeutic equivalence between the two medications. And if you are weighing the two options, the full comparison guide covers efficacy, cost, availability, and side effect profiles.
The role of GLP-1 receptor agonists
Semaglutide belongs to the GLP-1 receptor agonist class, a group of medications that mimic the incretin hormone GLP-1 to regulate blood sugar and reduce appetite. Understanding the relationship between GLP-1 and Ozempic helps clarify why these medications work the way they do. For general GLP-1 injection guidance and injection site recommendations, those resources apply to all medications in this class. The best time to take your GLP-1 shot can also help optimize your routine.
Some users explore whether combining GLP-1 medications with other treatments enhances results. The phentermine and semaglutide combination guide and the phentermine vs semaglutide comparison cover that topic. Similarly, the phentermine and GLP-1 classification guide clarifies how these medications differ mechanistically.
Reconstitution and its impact on unit conversion
If you are working with lyophilized (freeze-dried) semaglutide powder rather than a pre-mixed liquid, the reconstitution step directly determines your concentration. And your concentration determines your units. This makes the reconstitution step the foundation of accurate dosing.
How reconstitution creates your concentration
The formula is simple: concentration = total powder amount / total liquid volume.
For a 5 mg vial:
Add 1 mL of bacteriostatic water = 5 mg/mL concentration (1 mg = 20 units)
Add 2 mL of bacteriostatic water = 2.5 mg/mL concentration (1 mg = 40 units)
For a 10 mg vial:
Add 1 mL of bacteriostatic water = 10 mg/mL concentration (1 mg = 10 units)
Add 2 mL of bacteriostatic water = 5 mg/mL concentration (1 mg = 20 units)
The semaglutide mixing chart provides comprehensive tables for every powder amount and water volume combination. More specific guides exist for the 5 mg mixing chart and the 10 mg mixing chart.
Using bacteriostatic water
Bacteriostatic water is the standard diluent for reconstituting semaglutide. It contains 0.9% benzyl alcohol as a preservative, which allows the reconstituted solution to remain stable for multiple uses over several weeks. The bacteriostatic water guide explains proper handling and why it differs from sterile water or saline.
Measure the water volume carefully. Using a graduated syringe rather than eyeballing the amount ensures your final concentration matches your calculations. A 3 mL syringe with 0.1 mL gradations works well for this purpose. The general peptide reconstitution guide covers technique fundamentals that apply to semaglutide and all other peptides.
Recording your reconstitution details
Write down three things immediately after reconstituting:
The powder amount (e.g., 5 mg or 10 mg)
The exact volume of water added (e.g., 2 mL)
The resulting concentration (e.g., 2.5 mg/mL)
Label the vial with the concentration and the reconstitution date. The vial shelf life guide explains how long your reconstituted solution remains usable based on storage conditions. Most reconstituted semaglutide should be used within 28 days when stored properly. After that period, even if the solution looks clear, it should be discarded. The 28-day expiration guide explains why this timeline matters, and the expired semaglutide guide covers the risks of using medication past its recommended window.
Using the semaglutide dosage calculator
While the formula and charts in this guide let you calculate conversions manually, digital tools eliminate arithmetic errors entirely. SeekPeptides offers a free semaglutide dosage calculator that handles the conversion automatically.
How the calculator works
Enter two values: your desired dose in milligrams and your vial concentration in mg/mL. The calculator returns the exact number of units to draw on a U-100 insulin syringe. No formula needed. No room for arithmetic mistakes.
The general peptide calculator works for semaglutide and every other peptide. And the reconstitution calculator helps you determine the right water volume to achieve your target concentration before you even get to the dosing step. Together, these tools create a closed-loop system where every calculation gets verified before medication touches your syringe.
For those tracking costs across their treatment, the peptide cost calculator helps compare expenses between different vial sizes and concentrations, which can influence which concentration you choose to work with.
When to use the calculator vs manual calculation
Use the calculator for routine dose verification. Every time you draw a dose, a quick calculator check takes seconds and confirms your unit count. Use manual calculation when you want to understand the math, when you do not have internet access, or when teaching someone else how the conversion works.
Both methods should produce identical results. If they do not, something is wrong, and you need to identify the discrepancy before injecting anything.
Advanced considerations for the 1 mg dose
Beyond the basic conversion, several factors specific to the 1 mg dose level deserve attention.
Splitting doses
Some providers recommend splitting the weekly 1 mg dose into two 0.5 mg injections given three to four days apart. This approach can reduce side effects by avoiding the peak concentration spike that occurs with a single weekly injection. At 5 mg/mL, each split dose would be 10 units instead of one 20-unit injection.
Splitting does not change the total weekly milligram amount. It changes the pharmacokinetic profile. Discuss this option with your provider if side effects at the 1 mg level are interfering with your quality of life.
Timing considerations
The 1 mg dose, like all semaglutide doses, should be administered on the same day each week. You can change your injection day, but try to keep it consistent once established. If you miss a dose and more than five days remain until your next scheduled injection, take the missed dose as soon as possible. If fewer than five days remain, skip the missed dose and resume your regular schedule.
Research on semaglutide and energy levels suggests that some people experience fatigue in the first 24 to 48 hours after injection. Scheduling your dose for a day when mild fatigue would be least disruptive, such as a Friday evening, can make the transition period more manageable. The GLP-1 fatigue guide covers management strategies in detail.
Alcohol and the 1 mg dose
Alcohol consumption interacts with semaglutide in ways that become more noticeable at higher doses. At 1 mg, many users report reduced alcohol tolerance and altered taste preferences. The drinking on semaglutide guide explains the mechanisms and safety considerations.
Menstrual cycle considerations
Some women report menstrual changes when escalating to the 1 mg dose. Rapid weight loss and hormonal shifts can affect cycle regularity. The semaglutide and menstrual cycle guide addresses these concerns with evidence-based information.
Surgery and the 1 mg dose
If you have an upcoming surgery, your provider may recommend pausing semaglutide. The delayed gastric emptying effect can create anesthesia complications. The post-surgery resumption guide explains recommended timelines for stopping before and restarting after surgical procedures.
Alternative delivery methods for semaglutide
Vial and syringe is not the only way to receive semaglutide. Understanding alternative delivery methods provides context for why unit conversion is primarily a concern for compounded vial-based products.
Pre-filled pens (Ozempic, Wegovy)
FDA-approved pens eliminate the unit conversion question entirely. You select your dose in milligrams using the pen dial, and the device delivers the correct volume automatically. If unit conversion causes you anxiety, discussing pen options with your provider may be worthwhile. The tradeoff is typically cost, as branded pens are significantly more expensive than compounded vials.
Oral semaglutide
Oral formulations bypass injection entirely. The oral semaglutide drops guide and the sublingual semaglutide guide cover these alternatives. Oral dosing uses different milligram amounts than injectable due to reduced bioavailability, so the unit conversions in this article do not apply to oral products.
Alternative GLP-1 options
If semaglutide dosing complexity is a concern, other GLP-1 medications may offer simpler administration. Tirzepatide drops and tirzepatide tablets are emerging alternatives with different dosing formats. Newer options like the Onmorlo GLP-1 patches aim to simplify delivery even further.
Building a complete semaglutide dosing system
The most reliable approach to semaglutide dosing combines multiple verification steps into a system that catches errors before they happen. Here is what that system looks like in practice.
The verification triad
Step 1: Written reference. Keep a printed or handwritten card with your specific concentration and unit conversions for every dose level in your escalation schedule. Update it whenever anything changes.
Step 2: Calculator check. Before each injection, enter your dose and concentration into the semaglutide dosage calculator. Compare the result to your written reference. They should match.
Step 3: Syringe verification. After drawing the medication, hold the syringe at eye level and confirm the unit marking matches your calculated dose. If anything looks off, stop and recheck.
This three-step system catches mathematical errors, concentration changes, syringe misreads, and memory lapses. It takes under a minute and eliminates virtually all common dosing mistakes.
SeekPeptides members gain access to comprehensive protocol guides, community support, and expert resources that make building and maintaining these safety systems straightforward. For anyone navigating the complexities of peptide dosing, having a trusted resource base makes the difference between guesswork and confidence.
Track your doses
Maintain a simple log of each injection: date, time, dose in mg, units drawn, injection site, and any side effects. This log becomes invaluable if you ever need to troubleshoot results, discuss adjustments with your provider, or identify patterns in side effects relative to dose timing or injection location.
The peptide dosing guide provides a framework for systematic dose tracking that applies to semaglutide and other peptides. And for understanding the broader context of how peptides work in the body, that resource helps connect the dosing mechanics to the biological outcomes you are pursuing.
Frequently asked questions
Is 1 mg of semaglutide always 20 units?
No. The number 20 units only applies at a 5 mg/mL concentration. At 2.5 mg/mL, 1 mg equals 40 units. At 10 mg/mL, it equals 10 units. Always check your vial concentration before converting. The conversion chart for all concentrations provides the complete reference.
What happens if I accidentally take 2 mg instead of 1 mg?
Taking double your intended dose increases the risk of nausea, vomiting, diarrhea, and hypoglycemia. Contact your healthcare provider immediately. Do not take your next scheduled dose without medical guidance. The peptide safety guide covers overdose response protocols.
Can I use a regular syringe instead of an insulin syringe?
A regular syringe marked in milliliters will work if you skip the multiplication by 100 step and draw directly in mL. For 1 mg at 5 mg/mL, you would draw 0.2 mL. However, insulin syringes are preferred because their fine gauge needles reduce injection discomfort and their unit markings simplify small-volume measurement.
Does the 1 mg dose work better for diabetes or weight loss?
For diabetes (Ozempic), 1 mg is often the primary maintenance dose. For weight loss (Wegovy), 1 mg is a midpoint escalation dose, with the full maintenance being 2.4 mg. Clinical efficacy for weight management continues to improve at higher doses, which is why the weight loss protocol escalates beyond 1 mg.
How do I know if 1 mg is working?
Look for reduced appetite, decreased food noise (constant thoughts about eating), smaller portion satisfaction, and gradual weight change. Results typically become more noticeable after two to three weeks at a given dose. The semaglutide timeline guide sets realistic expectations for each phase.
Should I take 1 mg on the same day every week?
Yes. Consistency matters for maintaining steady blood levels. Choose a day that works for your schedule and stick with it. If you need to change your injection day, the dosing timing guide explains how to transition safely.
What if my pharmacy changes my vial concentration?
Recalculate your units immediately using the formula or the dosage calculator. Do not assume the units stay the same. A concentration change means every dose conversion changes. This is the most common source of dosing errors when patients refill prescriptions.
Is the 1 mg dose available as a pen?
Yes. Ozempic offers a 1 mg pen configuration, and the Wegovy escalation schedule passes through 1 mg during the dose-up phase. With pens, you do not need to convert to units because the pen dial handles the measurement automatically.
External resources
PubMed: Administration errors of compounded semaglutide reported to a poison control center
NEJM: Once-weekly semaglutide in adults with overweight or obesity (STEP 1 trial)
PMC: Once-weekly semaglutide for weight management clinical review
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your syringes stay precise, and your doses stay consistent.