Feb 20, 2026

What if the number on your syringe does not mean what you think it means? That single misunderstanding, confusing units with milligrams, has sent people to the emergency room. It has caused weeks of nausea that never needed to happen. And it has wasted hundreds of dollars in peptide that got drawn up wrong.
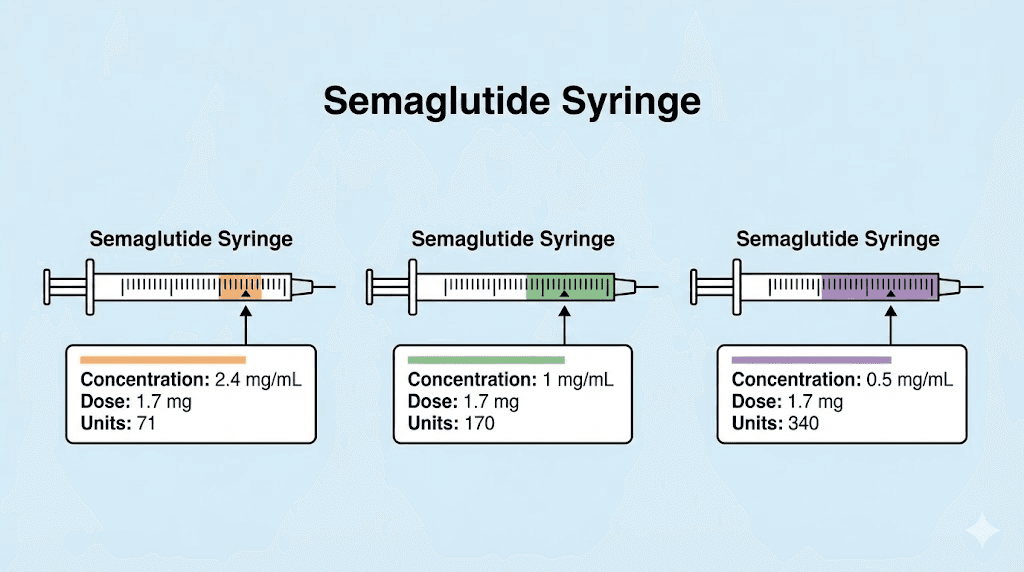
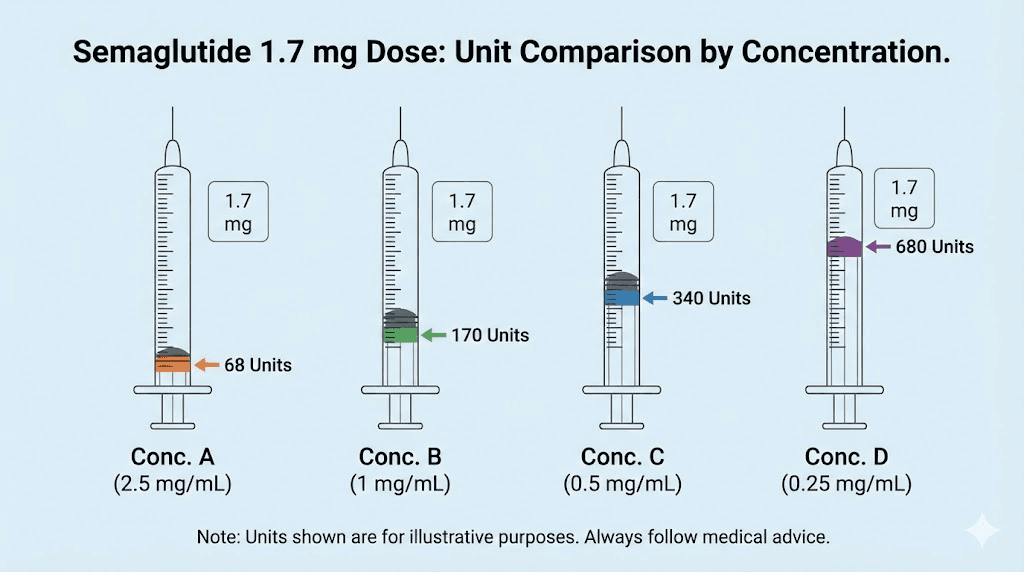
The question seems simple enough. How many units is 1.7 mg of semaglutide? But the answer changes completely depending on one variable that most dosing guides barely mention: the concentration of your vial. At 2.5 mg/mL, 1.7 mg equals 68 units. At 5 mg/mL, it equals 34 units. At 10 mg/mL, just 17 units. Same medication. Same dose. Wildly different numbers on your syringe.
The FDA has documented cases where patients using compounded semaglutide accidentally administered 5 to 20 times their intended dose because they confused these measurements. Some required hospitalization. Others experienced acute pancreatitis, severe dehydration, and gallstones. These were not reckless people. They were careful individuals who simply did not understand that semaglutide units and milligrams are not the same thing.
This guide covers everything about converting 1.7 mg of semaglutide to units on an insulin syringe. You will find complete conversion charts for every common concentration, the exact formula to calculate your dose, step-by-step measuring instructions, and the specific mistakes that lead to dangerous overdoses. Whether you are on compounded semaglutide from a pharmacy or using a brand-name pen, accurate dosing at 1.7 mg requires understanding what these numbers actually mean. SeekPeptides has built comprehensive dosing resources because getting this wrong is not a minor inconvenience. It is a safety issue.
The quick answer: 1.7 mg of semaglutide in units by concentration
Before diving into the math, here is the direct answer. The number of units you need to draw depends entirely on the concentration printed on your vial label.
Vial concentration | 1.7 mg equals | Volume (mL) | Common source |
|---|---|---|---|
2.5 mg/mL | 68 units | 0.68 mL | Many compounding pharmacies |
3 mg/mL | 56.7 units | 0.567 mL | Some compounding pharmacies |
5 mg/mL | 34 units | 0.34 mL | Common compounded vials |
10 mg/mL | 17 units | 0.17 mL | High-concentration compounded vials |
That table represents the four most common concentrations you will encounter. The differences are enormous. Drawing 68 units from a 5 mg/mL vial when you should have drawn 34 units means you just injected 3.4 mg instead of 1.7 mg. That is double your intended dose. If you are looking for a quick reference, our complete semaglutide dosage conversion chart covers every dose at every concentration.
One thing to understand immediately: these numbers only apply when using a standard U-100 insulin syringe. The U-100 designation means the syringe measures 100 units per milliliter. Almost every insulin syringe sold in pharmacies follows this standard, but you should always verify. If you are using a different syringe type, the markings will not align with these conversions and you could dramatically over or underdose.
For those on brand-name Wegovy or Ozempic pens, you do not need to worry about unit conversions at all. The pen delivers a pre-set milligram dose with each click. The unit conversion challenge applies specifically to people using compounded semaglutide drawn from vials with insulin syringes.
Understanding the conversion formula
The math behind semaglutide dosing is straightforward once you see the logic. Every confusion, every mistake, every dangerous overdose comes from not understanding this one simple relationship between three measurements.
The three measurements explained
Milligrams (mg) measure how much active semaglutide you want to inject. Your prescribed dose is always in milligrams. For the step 4 escalation dose, that number is 1.7 mg.
Milliliters (mL) measure the volume of liquid you need to draw. This is the physical amount of fluid in the syringe. The relationship between milligrams and milliliters depends on concentration.
Units are simply a way to read milliliters on an insulin syringe. On a standard U-100 syringe, 100 units equals 1 mL. So 50 units equals 0.5 mL. And 34 units equals 0.34 mL. Units are not a measurement of medication strength. They are a measurement of volume, just displayed in a format designed for insulin syringes. This distinction is critical, and our semaglutide dosage in units guide explains it in depth.
The formula
To convert any milligram dose to units, use this calculation:
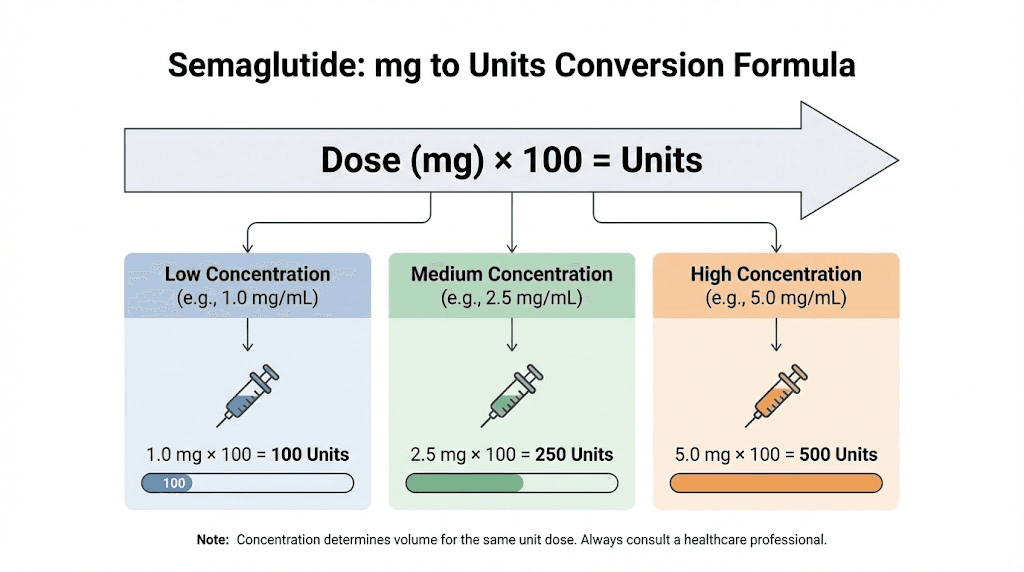
Units = (Dose in mg / Concentration in mg per mL) x 100
For 1.7 mg from a 2.5 mg/mL vial:
Units = (1.7 / 2.5) x 100 = 0.68 x 100 = 68 units
For 1.7 mg from a 5 mg/mL vial:
Units = (1.7 / 5) x 100 = 0.34 x 100 = 34 units
For 1.7 mg from a 10 mg/mL vial:
Units = (1.7 / 10) x 100 = 0.17 x 100 = 17 units
The formula works for any dose at any concentration. If you ever need to verify a different milligram amount, the SeekPeptides semaglutide dosage calculator handles the math automatically. Plug in your vial concentration, enter your dose, and it gives you the exact number of units to draw.
Why concentration changes everything
Think of it like this. A 2.5 mg/mL vial contains 2.5 milligrams of semaglutide dissolved in every milliliter of liquid. A 5 mg/mL vial packs twice as much medication into the same volume. So you need half the liquid to get the same dose.
This is exactly where mistakes happen. Someone switches from a 2.5 mg/mL vial to a 5 mg/mL vial but keeps drawing the same number of units. Instead of 1.7 mg, they inject 3.4 mg. Double the dose. The nausea hits hard. The vomiting starts. And they have no idea why their body is reacting so violently when they thought they were taking the same amount.
Every time you get a new vial, check the concentration on the label. Do not assume it matches your previous vial. Compounded semaglutide dosing charts vary between pharmacies, and even the same pharmacy may change concentrations between batches. Verifying the label takes five seconds. Recovering from a double dose takes days.
Why 1.7 mg matters in the semaglutide dose escalation schedule
The 1.7 mg dose is not arbitrary. It occupies a specific position in the FDA-approved titration protocol, and understanding where it fits helps explain why so many people search for this exact conversion.
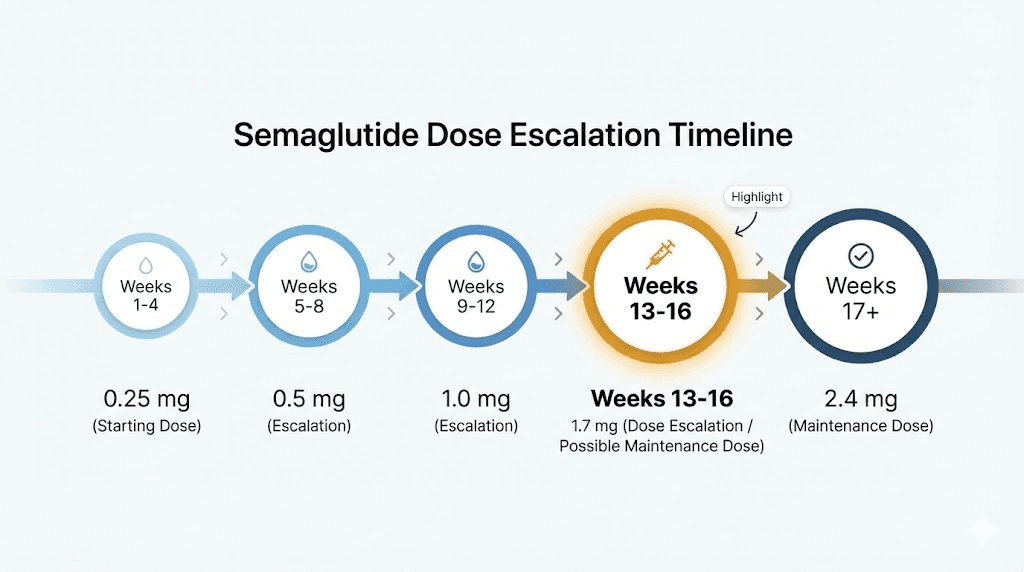
The standard dose escalation timeline
Semaglutide for weight management follows a 5-step escalation designed to minimize gastrointestinal side effects. Jumping straight to the full maintenance dose would cause severe nausea in most patients, so the protocol ramps up gradually over 16 to 20 weeks.
Step | Weeks | Dose | Units at 2.5 mg/mL | Units at 5 mg/mL |
|---|---|---|---|---|
Step 1 | Weeks 1 to 4 | 0.25 mg | 10 units | 5 units |
Step 2 | Weeks 5 to 8 | 0.5 mg | 20 units | 10 units |
Step 3 | Weeks 9 to 12 | 1.0 mg | 40 units | 20 units |
Step 4 | Weeks 13 to 16 | 1.7 mg | 68 units | 34 units |
Step 5 | Week 17 onward | 2.4 mg | 96 units | 48 units |
Step 4 represents the second-to-last escalation. By this point, most people have been on semaglutide for three months. Their body has adjusted to the GLP-1 receptor activation. The gastrointestinal side effects from the lower doses have typically stabilized. And the weight loss, which may have started noticeably around weeks 4 to 8, is beginning to accelerate.
The jump from 1.0 mg to 1.7 mg is the largest single increase in the protocol. You go from 40 units to 68 units on a 2.5 mg/mL concentration. That is a 70% dose increase. For comparison, the jump from 0.25 mg to 0.5 mg was a 100% increase, but at much lower absolute amounts. The 1.0 to 1.7 mg jump delivers more additional medication than any previous step.
What clinical trials show at 1.7 mg
The STEP 1 clinical trial, published in the New England Journal of Medicine, enrolled 1,961 adults with obesity. Participants who reached the full 2.4 mg maintenance dose lost an average of 14.9% of their body weight over 68 weeks, compared to 2.4% with placebo.
But not everyone needs to reach 2.4 mg. The FDA updated labeling for Wegovy to include 1.7 mg as an acceptable maintenance dose for patients who do not tolerate the higher amount. Research suggests that significant weight loss occurs even at this step 4 level, particularly when combined with proper dietary protocols and consistent physical activity.
Many people find that 1.7 mg provides the ideal balance. Enough appetite suppression to support meaningful weight loss. Manageable side effects that do not interfere with daily life. And a dose that feels sustainable for long-term use rather than something to white-knuckle through every week. For those tracking their early progress, our guide on semaglutide one-month results covers what to realistically expect at each stage.
The 1.7 mg dose as a maintenance option
Here is something most dosing guides overlook. The 1.7 mg dose is not just a stepping stone. It can be the destination.
If you reach 2.4 mg and experience intolerable side effects, the prescribing guidelines recommend stepping back to 1.7 mg for four weeks. If the 2.4 mg dose remains problematic after a second attempt, 1.7 mg can serve as your long-term maintenance dose.
This matters for people who experience persistent semaglutide fatigue, ongoing constipation, or excessive burping and nausea at the highest dose. Staying at 1.7 mg is not a failure. It is a clinically supported maintenance strategy that balances efficacy with tolerability. The weight loss may be slightly less dramatic than at 2.4 mg, but adherence improves when side effects are manageable, and adherence drives results more than any dose number ever will.
Complete conversion charts for every common concentration
Having one conversion memorized is not enough. Pharmacies change concentrations. Prescriptions get refilled with different vial strengths. And every switch requires recalculating your units. The charts below cover the four most common compounded semaglutide concentrations so you can quickly find your numbers regardless of what vial you receive.
2.5 mg/mL concentration chart
This is the most widely prescribed compounded semaglutide concentration. Many pharmacies default to 2.5 mg/mL because it provides a good balance between accuracy and vial size.
Dose (mg) | Volume (mL) | Units on U-100 syringe | Escalation step |
|---|---|---|---|
0.25 mg | 0.10 mL | 10 units | Step 1 |
0.5 mg | 0.20 mL | 20 units | Step 2 |
1.0 mg | 0.40 mL | 40 units | Step 3 |
1.7 mg | 0.68 mL | 68 units | Step 4 |
2.0 mg | 0.80 mL | 80 units | Custom |
2.4 mg | 0.96 mL | 96 units | Step 5 |
At 2.5 mg/mL, the 1.7 mg dose requires 68 units. This is a relatively large draw volume. You will need at least a 1 mL insulin syringe to measure this accurately. A 0.5 mL syringe simply does not have enough capacity. If your pharmacy provided a half-mL syringe, you may need to request a larger one or use our semaglutide syringe dosage chart to double-check your specific setup.
One advantage of the 2.5 mg/mL concentration at the 1.7 mg dose: the larger volume makes it easier to read the syringe markings. Each unit line is more spread apart compared to higher concentrations, reducing the chance of misreading. For someone new to drawing from vials, the semaglutide dosage chart in units provides visual references for every step.
5 mg/mL concentration chart
The 5 mg/mL concentration is common in compounded vials that contain more total medication per vial. Many 5 mg/mL semaglutide vials hold 2 mL of liquid, giving you 10 mg total per vial.
Dose (mg) | Volume (mL) | Units on U-100 syringe | Escalation step |
|---|---|---|---|
0.25 mg | 0.05 mL | 5 units | Step 1 |
0.5 mg | 0.10 mL | 10 units | Step 2 |
1.0 mg | 0.20 mL | 20 units | Step 3 |
1.7 mg | 0.34 mL | 34 units | Step 4 |
2.0 mg | 0.40 mL | 40 units | Custom |
2.4 mg | 0.48 mL | 48 units | Step 5 |
At 5 mg/mL, your 1.7 mg dose is just 34 units. This is half what you would draw from a 2.5 mg/mL vial. The smaller volume means each vial lasts longer, but accuracy becomes more critical. At this concentration, being off by just 2 units means a difference of 0.1 mg in your actual dose. If you are using a 5 mg vial for the first time, take extra care when lining up the plunger with the 34-unit mark.
A practical tip: at 5 mg/mL concentration, consider using a 0.5 mL (50-unit) insulin syringe instead of a 1 mL syringe. The half-mL syringe has larger markings between each unit line, making 34 units much easier to read accurately. This is the same principle behind our recommendation in the semaglutide dosing chart: match your syringe size to your draw volume for maximum precision.
10 mg/mL concentration chart
High-concentration vials pack 10 milligrams of semaglutide into every milliliter. These are less common but appear in some compounding pharmacies that prioritize compact vial sizes. The 10 mg semaglutide dosage chart covers this concentration in full detail.
Dose (mg) | Volume (mL) | Units on U-100 syringe | Escalation step |
|---|---|---|---|
0.25 mg | 0.025 mL | 2.5 units | Step 1 |
0.5 mg | 0.05 mL | 5 units | Step 2 |
1.0 mg | 0.10 mL | 10 units | Step 3 |
1.7 mg | 0.17 mL | 17 units | Step 4 |
2.0 mg | 0.20 mL | 20 units | Step 3 (adj.) |
2.4 mg | 0.24 mL | 24 units | Step 5 |
With 10 mg/mL, you only need 17 units for your 1.7 mg dose. This is an extremely small volume. A 0.3 mL (30-unit) insulin syringe is ideal here because the markings are the most spread apart, giving you the best precision. Using a 1 mL syringe at this concentration means squinting at tiny hash marks in the lower third of the barrel, where one slip of the plunger changes your dose significantly.
Be aware that 10 mg/mL vials require the most precision. Each unit on the syringe contains 0.1 mg of semaglutide. Overdrawing by just 5 units means taking an extra 0.5 mg, which is a nearly 30% overdose. This concentration is not recommended for people who are new to drawing from vials. If this is your first time with semaglutide, the reconstitution guide walks through the basics before you ever draw a dose.
3 mg/mL concentration chart
Some pharmacies use a 3 mg/mL concentration as a middle ground. This creates slightly awkward numbers but works perfectly well with the right syringe.
Dose (mg) | Volume (mL) | Units on U-100 syringe | Escalation step |
|---|---|---|---|
0.25 mg | 0.083 mL | 8.3 units | Step 1 |
0.5 mg | 0.167 mL | 16.7 units | Step 2 |
1.0 mg | 0.333 mL | 33.3 units | Step 3 |
1.7 mg | 0.567 mL | 56.7 units | Step 4 |
2.0 mg | 0.667 mL | 66.7 units | Custom |
2.4 mg | 0.800 mL | 80 units | Step 5 |
At 3 mg/mL, your 1.7 mg dose comes to 56.7 units. Round to 57 units on your syringe. The 0.3 unit difference represents less than 0.01 mg of semaglutide, which is clinically insignificant. Your pharmacy may provide specific rounding instructions with your vial. Always follow their guidance over general charts. If you want to explore how semaglutide doses convert to milliliters across concentrations, that reference guide covers the volume side of the equation.
How to measure 1.7 mg of semaglutide step by step
Knowing the number is one thing. Actually drawing it accurately from a vial requires technique. Here is the complete process, broken down for someone who may be doing this for the first time at the 1.7 mg dose.
Before you start
Gather everything you need. A clean workspace matters more than people realize. You need your semaglutide vial, an appropriately sized insulin syringe, an alcohol swab, and a sharps container for disposal. Having everything within reach prevents you from setting down a drawn syringe to search for a swab, which risks contamination or accidental needle sticks.
Check your vial label. Read the concentration. Then read it again. If it says 5 mg/mL, your target is 34 units. If it says 2.5 mg/mL, your target is 68 units. Write the number down. Put it where you can see it while drawing. This simple step prevents the most common dosing errors. For a visual walkthrough of finding the best injection site for semaglutide, check our dedicated guide.
Choose the right syringe size for your concentration. For 68 units (2.5 mg/mL), use a 1 mL syringe. For 34 units (5 mg/mL), use a 0.5 mL or 1 mL syringe. For 17 units (10 mg/mL), use a 0.3 mL syringe. The goal is always to use the smallest syringe that fits your dose, because smaller syringes have more precise markings.
The drawing process
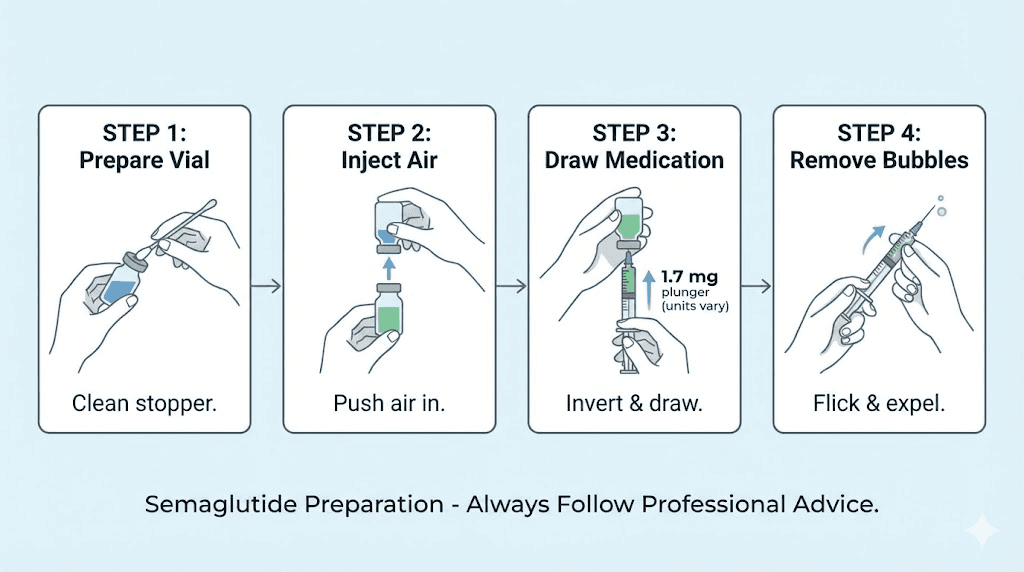
Wash your hands with soap and water. This is not optional. You are about to puncture your skin with a needle. Clean hands reduce infection risk at the injection site.
Clean the rubber stopper on your vial with an alcohol swab. Let it dry for about 10 seconds. This prevents introducing bacteria into the multi-use vial that you will be drawing from again next week.
Remove the cap from a new syringe. Never reuse syringes. Pull the plunger back to your target number of units to draw air into the barrel. For the 1.7 mg dose, that would be 68 units of air for a 2.5 mg/mL vial, or 34 units for a 5 mg/mL vial.
Insert the needle through the rubber stopper and push the air into the vial. This equalizes pressure inside the vial and makes drawing liquid much easier. Without this step, you will fight against a vacuum that makes accurate measuring difficult.
Turn the vial upside down with the needle still inserted. The tip of the needle should be submerged in the liquid. Slowly pull the plunger back to your target unit mark. Go slightly past it, then push forward to exactly the right number. This back-and-forth technique helps eliminate air bubbles that could affect your dose accuracy.
Check for air bubbles. If you see any in the barrel, flick the syringe gently with your finger to move them to the top near the needle. Then push the plunger up slightly to expel the air back into the vial. Re-draw to your exact target. Air bubbles in the syringe are not dangerous when injecting subcutaneously, but they do reduce the volume of medication you actually receive. A bubble that takes up 3 units of space means you are getting 3 fewer units of semaglutide than you measured.
Remove the needle from the vial. Your syringe should show your exact target units. Double-check one final time before proceeding to injection. If you are new to the injection process itself, the complete GLP-1 injection guide covers proper technique, and our article on where to inject GLP-1 explains optimal injection sites.
Injection tips specific to the 1.7 mg dose
At the step 4 dose, you may notice the injection volume is larger than what you have been used to at lower doses. If you were at 1.0 mg (40 units from a 2.5 mg/mL vial) and now you are injecting 68 units, that is 70% more liquid going under your skin.
A larger volume can occasionally cause more discomfort at the injection site. Some people report a slight stinging or a bump that takes longer to absorb. To minimize this, inject slowly over 5 to 10 seconds rather than pushing the plunger quickly. The slower pace gives the subcutaneous tissue time to accommodate the liquid and reduces that uncomfortable pressure feeling.
Rotate your injection sites. Abdomen, upper outer thigh, and back of the upper arm are all approved locations. Rotating prevents lipodystrophy, a condition where repeated injections in the same spot cause fat tissue changes that affect medication absorption. The best time of day to take semaglutide can also influence how you experience side effects at this higher dose.
Common dosing mistakes and FDA safety warnings
The FDA does not issue safety communications for minor concerns. When the agency specifically warned about dosing errors with compounded semaglutide, it reflected a pattern of serious adverse events that were entirely preventable.
The most dangerous mistake: concentration confusion
This is the big one. A patient gets a 5 mg/mL vial but uses the unit instructions from their previous 2.5 mg/mL prescription. Instead of drawing 34 units (which would deliver 1.7 mg from the 5 mg/mL vial), they draw 68 units, which delivers 3.4 mg. Double the intended dose.
The FDA documented cases where patients administered 5 to 20 times their intended dose through this type of error. Adverse events included severe nausea and vomiting, abdominal pain, fainting, headache, migraine, dehydration, acute pancreatitis, and gallstones. Some cases required emergency hospitalization.
This error happens most often at the 1.7 mg dose level because people have been escalating through lower doses where the consequences of a small error were less severe. At 0.25 mg, even doubling your dose produces relatively mild effects. At 1.7 mg, doubling to 3.4 mg can produce a medical emergency. The bacteriostatic water mixing guide covers proper dilution if you are reconstituting from lyophilized powder.
Syringe size errors
Not all insulin syringes are the same capacity. A U-100 syringe comes in 0.3 mL (30-unit), 0.5 mL (50-unit), and 1.0 mL (100-unit) sizes. The unit markings are identical in scale, but the total capacity differs.
If someone needs 68 units (1.7 mg from a 2.5 mg/mL vial) but only has a 50-unit syringe, they physically cannot draw enough. Some people have solved this by drawing two separate injections, which introduces additional error. Others have tried to eyeball beyond the syringe markings. Both approaches lead to inaccurate dosing.
The solution is simple. Always have the right syringe for your concentration and dose. If you are on a 2.5 mg/mL concentration at the 1.7 mg dose, you need a 1 mL (100-unit) syringe. Period.
Reading the syringe incorrectly
Insulin syringes have fine graduation marks. On a 1 mL syringe, each small line typically represents 2 units. On a 0.5 mL syringe, each small line represents 1 unit. On a 0.3 mL syringe, each line may represent 0.5 units.
Misreading these marks by even a few units matters more at higher concentrations. With a 10 mg/mL vial, misreading by 5 units means your dose is off by 0.5 mg, which is a 29% error at the 1.7 mg dose level. With a 2.5 mg/mL vial, the same 5-unit misread only changes your dose by 0.125 mg, which is about 7%.
Hold your syringe at eye level when reading. Do not look from above or below, as parallax error distorts the apparent position of the plunger. The bottom of the plunger rubber tip (the flat edge closest to the needle) is your measurement point. Our semaglutide syringe dosage conversion chart includes visual references for reading at different syringe sizes.
Skipping the air injection step
When drawing from a multi-dose vial, failing to inject air first creates a vacuum. The vacuum makes it harder to pull liquid, and people compensate by pulling harder, which often causes the plunger to jump past their target. Then they push back, then pull again, and each correction introduces more error and more air bubbles.
Inject air equal to your intended draw volume before pulling liquid. It takes two extra seconds and prevents five minutes of frustration.
Contaminating multi-dose vials
Each time you puncture the rubber stopper, there is a small risk of introducing bacteria. Cleaning the stopper with alcohol before every draw, using a new sterile needle each time, and storing the vial properly between uses prevents contamination that could cause infection. If you are wondering about vial longevity, our guides on how long semaglutide stays good and compounded semaglutide fridge storage cover proper handling in detail.
Compounded vs brand-name semaglutide at 1.7 mg
The unit conversion question almost exclusively applies to compounded semaglutide. Understanding why helps clarify the whole measurement challenge.
Brand-name pens: no conversion needed
Wegovy pens come in pre-set doses. The step 4 pen delivers exactly 1.7 mg with each injection. You do not draw from a vial. You do not calculate units. You attach a needle, select your dose, and inject. The pen mechanism handles all measurement internally.
Ozempic pens work similarly, though Ozempic dose options differ from Wegovy because it is approved for diabetes rather than weight management. Ozempic pens deliver 0.25 mg, 0.5 mg, 1 mg, or 2 mg, with no 1.7 mg option. If your provider prescribes 1.7 mg specifically, you are likely on Wegovy or a compounded formulation.
Compounded semaglutide: where conversions matter
Compounded semaglutide comes in vials rather than pens. You draw your dose using an insulin syringe, which means you must convert milligrams to units every single time. This is where every conversion chart, formula, and safety warning in this article becomes essential.
Compounding pharmacies produce semaglutide at various concentrations. Some pharmacies specialize in specific concentrations. Empower Pharmacy, for example, is one of the most well-known compounders. Olympia Pharmacy and Direct Meds are other popular options. Each may use different concentrations, which is why checking your vial label is non-negotiable.
Some compounded semaglutide also includes additional ingredients like vitamin B12, methylcobalamin, or glycine. These additions do not change the semaglutide concentration or your unit calculation, but they do add context to why different pharmacies produce different formulations.
Key differences in practice
Factor | Brand-name pen | Compounded vial |
|---|---|---|
Dose measurement | Pre-set by pen | Manual with syringe |
Error risk | Very low | Higher without training |
Concentration varies | No | Yes, by pharmacy |
Conversion needed | No | Yes, every dose |
Cost | Higher | Generally lower |
FDA oversight | Full FDA approval | State pharmacy board regulated |
Neither option is inherently better. Brand-name pens offer convenience and eliminate measurement error. Compounded semaglutide offers cost savings and concentration flexibility. The right choice depends on your comfort level with drawing from vials, your budget, and your provider recommendation. SeekPeptides members access detailed comparisons of compounding pharmacies and their specific formulations to make this decision easier.
Side effects at the 1.7 mg dose level
Side effects at step 4 follow a somewhat predictable pattern. Most people experience some increase in GI symptoms compared to the 1.0 mg dose they came from, but the severity varies widely between individuals.
What to expect when you first move to 1.7 mg
The first week at 1.7 mg is typically the hardest. Your body needs to adjust to the higher level of GLP-1 receptor activation. Common experiences include increased nausea, reduced appetite (sometimes to the point of food aversion), mild headache, and fatigue.
For most people, these effects peak around days 2 to 4 after the first 1.7 mg injection and gradually decrease over the following week. By the second or third injection at this dose, many report that side effects have settled to a manageable level. If you experienced a similar adjustment period when moving from 0.5 mg to 1.0 mg, expect a comparable timeline at this step.
The appetite suppression at 1.7 mg is typically stronger than anything experienced at lower doses. Some people describe it as having virtually no interest in food, particularly during the first few days after injection. Understanding how long it takes semaglutide to suppress appetite helps set realistic expectations for each dose increase.
Common side effects and their frequency
Side effect | Frequency at 1.7 mg | Typical duration | Management |
|---|---|---|---|
Nausea | Very common (40-50%) | 1 to 3 weeks | Small meals, ginger, hydration |
Decreased appetite | Very common (30-40%) | Ongoing (intended effect) | Eat protein-focused meals |
Diarrhea | Common (15-25%) | 1 to 2 weeks | Hydration, bland diet |
Constipation | Common (15-20%) | Ongoing for some | Fiber, water, magnesium |
Fatigue | Common (10-20%) | 1 to 2 weeks | Adequate sleep, electrolytes |
Headache | Moderate (10-15%) | Days | Hydration, OTC pain relief |
Injection site reactions | Uncommon (5-10%) | Hours to days | Rotate sites, ice pack |
Nausea is the most commonly reported side effect at every dose level, and it tends to increase with each escalation step before settling. The guides on GLP-1 fatigue and semaglutide constipation treatment offer specific protocols for managing these effects long-term.
When side effects signal a problem
Some side effects at 1.7 mg warrant medical attention. Contact your provider if you experience persistent vomiting lasting more than 24 hours, severe abdominal pain that does not respond to rest and OTC remedies, signs of dehydration (dark urine, dizziness, rapid heartbeat), or any sudden onset of severe symptoms.
The most serious concern at higher semaglutide doses is pancreatitis. While rare, the risk increases with dose. Symptoms include severe pain in the upper abdomen that radiates to the back, nausea and vomiting that do not improve, and tenderness when pressing on the abdomen. If you suspect pancreatitis, stop the medication and seek emergency care immediately.
For people who had no weight loss after 4 weeks on semaglutide at lower doses, the 1.7 mg step often represents a turning point. But weight loss plateaus can happen at any dose. Our guide on semaglutide plateaus explains why they occur and how to address them.
When to stay at 1.7 mg vs escalating to 2.4 mg
Not everyone should move to 2.4 mg. This is perhaps the most underappreciated aspect of semaglutide dosing, and it directly affects how long you will be drawing 1.7 mg worth of units from your vial.
Reasons to stay at 1.7 mg
You are losing weight consistently. If 1.7 mg produces steady, meaningful weight loss, there is a clinical argument for staying put. Higher doses do not always translate to more weight loss for every individual, and the marginal benefit of the extra 0.7 mg may not justify the additional side effects.
Your side effects are tolerable but present. If you experience mild nausea, occasional fatigue, or intermittent burping at 1.7 mg, these effects may intensify at 2.4 mg. For some people, the quality-of-life trade-off is not worth it.
You have a history of GI sensitivity. People with conditions like GERD, IBS, or gastroparesis may find that 1.7 mg is the maximum tolerable dose. Pushing beyond it can exacerbate underlying gastrointestinal conditions that make daily functioning difficult.
Your provider recommends it. Individual medical factors that you may not be aware of, including lab values, medication interactions, and personal risk factors, all inform dosing decisions. Follow your provider guidance over generic escalation schedules.
Reasons to escalate to 2.4 mg
Weight loss has stalled. If 1.7 mg produced initial results but you have hit a plateau, the higher dose may restart progress. The full maintenance dose provides maximum GLP-1 receptor activation, which can overcome adaptive mechanisms that reduce the drug effectiveness over time.
Side effects at 1.7 mg are minimal. If you tolerated the step 4 dose without significant issues, you are likely to handle 2.4 mg well. The escalation schedule exists specifically to identify people who can reach the full dose comfortably.
You have significant weight to lose. Clinical trials showed greater weight loss at 2.4 mg compared to lower maintenance doses. For people with higher starting BMI or those targeting larger total weight loss, the additional efficacy matters.
The decision is not permanent. You can always try 2.4 mg and step back to 1.7 mg if needed. The FDA guidelines explicitly support this approach. For people considering the comparison between semaglutide and alternatives, the semaglutide vs tirzepatide side effects comparison provides relevant context.
Other doses in the escalation and their unit conversions
While this article focuses on 1.7 mg, understanding how it relates to the other doses in the protocol helps you see the full picture. You may need to step down temporarily or reference other doses when discussing your protocol with a provider.
Step 1: 0.25 mg
The starting dose. At 2.5 mg/mL, it requires just 10 units. At 5 mg/mL, only 5 units. This is where everyone begins, and the small draw volume means errors at this stage have minimal clinical impact. Most people tolerate the starting dose well, with mild or no side effects. Detailed coverage in our guide to semaglutide appetite suppression explains what to expect at this initial level.
Step 2: 0.5 mg
The first doubling. At 2.5 mg/mL, 20 units. At 5 mg/mL, 10 units. This is where most people first notice appetite changes. Some experience their initial side effects here. Understanding conversion accuracy starts becoming more important as doses increase.
Step 3: 1.0 mg
At 2.5 mg/mL, 40 units. At 5 mg/mL, 20 units. The 1.0 mg dose is where weight loss typically becomes noticeable. It also tends to be where GI side effects first become bothersome for sensitive individuals. Many people who explored how long semaglutide takes to work found their answer during this step.
Step 5: 2.4 mg (full maintenance)
At 2.5 mg/mL, 96 units. At 5 mg/mL, 48 units. The maximum recommended dose for weight management. Nearly fills a 1 mL syringe at 2.5 mg/mL concentration. For a comprehensive breakdown, see our article on how many units is 2.4 mg of semaglutide.
Some people starting the journey wonder about specific amounts like what 10 units equals in milligrams, or they need to verify numbers in the middle of their escalation like 20 units in milligrams, 40 units in milligrams, or even 50 units in milligrams. Each of those guides addresses the specific conversion at that unit count, including context about which dose level that corresponds to.
Storing and handling your semaglutide vial
Proper storage directly affects dosing accuracy. Degraded semaglutide may not deliver the expected clinical effect even if you measure perfectly, and improper handling can change the solution properties in ways that affect drawing consistency.
Refrigeration requirements
Compounded semaglutide vials should be stored at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). This is standard refrigerator temperature. Place the vial in the body of the refrigerator, not in the door where temperature fluctuates with opening and closing, and not near the freezer compartment where it could accidentally freeze.
Freezing destroys semaglutide. If your vial freezes, discard it. The peptide structure denatures in ice formation, and thawed semaglutide may not work at all. For extended information on storage timelines, our guides on compounded semaglutide refrigeration and what happens if semaglutide gets warm cover the full spectrum of storage scenarios.
Room temperature exposure
Most compounded semaglutide vials can safely remain at room temperature (up to 77 degrees Fahrenheit) for short periods. The typical guideline is up to 28 days at room temperature, but this varies by compounder. Check your pharmacy specific instructions.
If you travel with semaglutide, use a small insulated cooler or a medication travel case with a cold pack. Do not leave vials in a hot car, in direct sunlight, or in checked luggage where temperature exposure is unpredictable.
Checking vial integrity before drawing
Before each draw, visually inspect your vial. The liquid should be clear and colorless. Any cloudiness, particles, discoloration, or visible debris means the medication has degraded and should not be used. This applies to every vial at every dose level but is especially important to emphasize at 1.7 mg, where the clinical stakes of an ineffective dose are higher than at the starting levels.
Also check the expiration status of your semaglutide. Using expired medication may result in reduced potency, meaning your measured 1.7 mg may not actually deliver the expected therapeutic effect.
Reconstitution and concentration: a deeper look
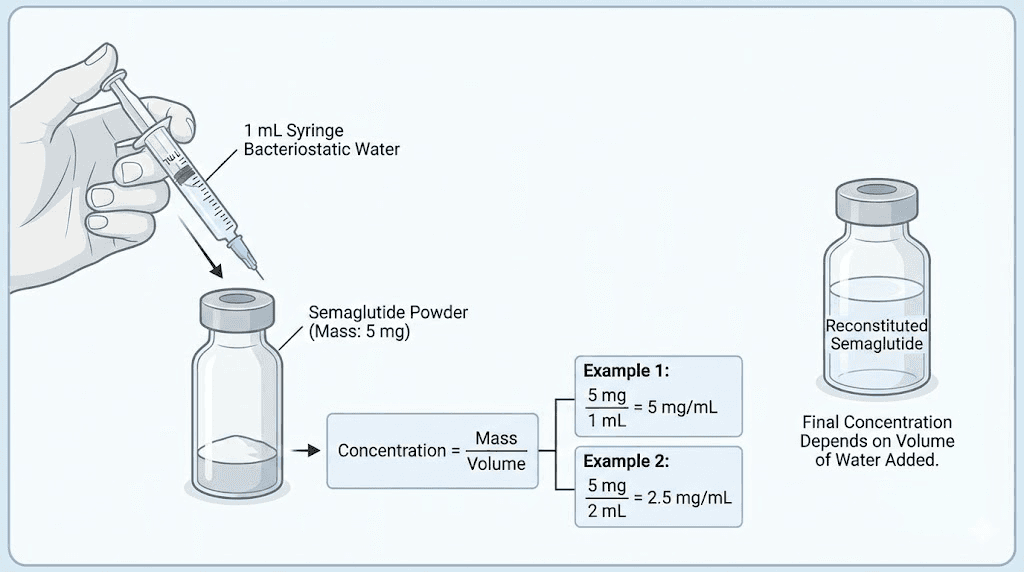
Some compounded semaglutide arrives as a lyophilized (freeze-dried) powder that requires reconstitution with bacteriostatic water before use. The amount of water you add determines the final concentration, which in turn determines how many units equal 1.7 mg.
How reconstitution affects your dose
If you receive a vial containing 5 mg of semaglutide powder and add 2 mL of bacteriostatic water, your concentration is 2.5 mg/mL. At that concentration, 1.7 mg equals 68 units.
If you add 1 mL of water to the same 5 mg vial, your concentration becomes 5 mg/mL. Now 1.7 mg equals 34 units.
The total amount of medication in the vial does not change. You still have 5 mg total. But the concentration, and therefore the units you need to draw, is completely different depending on how much water you added. This is why our guide to reconstituting 5 mg semaglutide and the bacteriostatic water mixing guide for 5 mg vials emphasize measuring water volumes precisely.
For 10 mg vials, the same principle applies at larger scale. Our 10 mg semaglutide mixing chart and 10 mg bacteriostatic water guide cover the specific volumes and resulting concentrations for the larger vial size.
Using the reconstitution calculator
The SeekPeptides peptide reconstitution calculator eliminates guesswork. Enter the total milligrams in your vial, the amount of bacteriostatic water you plan to add (or have already added), and it calculates the resulting concentration. From there, the semaglutide dosage calculator converts your 1.7 mg dose to the exact units for that concentration.
Using both calculators together creates a safety chain: vial contents plus water volume equals concentration, and concentration plus dose equals units. Each calculation cross-checks the other. If the numbers seem off at any step, something went wrong, and you should verify before injecting. For a complete set of reference charts, our semaglutide reconstitution chart provides visual guides for the most common vial sizes.
Comparing the 1.7 mg semaglutide dose to tirzepatide
Many people considering semaglutide at 1.7 mg also wonder how this dose compares to tirzepatide, the dual GIP/GLP-1 receptor agonist. The comparison is not straightforward because the two medications work through different mechanisms and use different dosing scales.
Dose equivalency is not one-to-one
There is no exact conversion between 1.7 mg of semaglutide and a specific tirzepatide dose. The medications target different receptors and have different pharmacokinetic profiles. However, in terms of clinical effect (weight loss and appetite suppression), 1.7 mg of semaglutide is roughly comparable to 5 to 7.5 mg of tirzepatide based on clinical trial outcomes.
The semaglutide to tirzepatide conversion chart provides a detailed comparison of equivalent doses. For a broader look at the differences between these two medications, the semaglutide vs tirzepatide comparison page covers mechanisms, efficacy, side effects, and cost.
Switching between medications
If you are considering switching from tirzepatide to semaglutide or vice versa, the 1.7 mg dose level is a common transition point. It provides enough GLP-1 activation to prevent significant rebound while your body adjusts to the new medication profile.
The dosage comparison chart maps equivalent doses between both medications across all escalation steps. Understanding these relationships helps prevent the common mistake of starting the new medication at too high or too low a dose.
For people specifically looking at tirzepatide dosing in units, the same concentration-dependent conversion principles apply. Tirzepatide also comes in various concentrations when compounded, and each requires its own unit calculation.
Practical tips for long-term success at 1.7 mg
Dosing accuracy matters, but it exists within a larger context of lifestyle, nutrition, and protocol adherence that collectively determine your results.
Nutrition at the 1.7 mg dose
Appetite suppression at step 4 is significant. Many people struggle to eat enough calories and protein. This is a real problem. Insufficient protein intake accelerates muscle loss during weight loss, which slows metabolism and can lead to the "skinny fat" outcome that nobody wants.
Aim for at least 0.7 to 1.0 grams of protein per pound of body weight daily. This is challenging when food holds no appeal. Protein shakes designed for GLP-1 users can help bridge the gap. High-protein, low-volume foods like Greek yogurt, eggs, and lean fish provide maximum nutrition in small portions that are easier to consume when appetite is suppressed.
For a structured approach, the semaglutide diet plan and our guide on best foods to eat while on semaglutide offer meal ideas tailored to reduced appetite at higher dose levels.
Timing your injection
The best time to take your GLP-1 shot becomes more relevant at higher doses where side effects are more noticeable. Many people prefer injecting in the evening so the peak side effects occur during sleep. Others prefer morning injections so the strongest appetite suppression aligns with daytime eating patterns.
Whatever time you choose, consistency matters more than the specific hour. Your body establishes a rhythm with weekly injections, and changing the timing frequently can lead to variable side effect profiles that make management harder.
Tracking your progress
At the 1.7 mg dose, you have been on semaglutide for at least 12 weeks. This is enough time to establish trends. Weigh yourself at the same time each week (morning, after using the bathroom, before eating). Track measurements, not just scale weight. And document how you feel, including energy levels, appetite, mood, and any side effects.
People who track outcomes make better dosing decisions because they have data to discuss with their provider. "I have been losing 1.5 pounds per week at 1.7 mg with mild nausea" is far more useful than "I think things are going okay." The guides on semaglutide before and after results and how long to stay on semaglutide provide benchmarks for what realistic progress looks like at each stage.
Managing the cost of semaglutide
At 1.7 mg weekly, your semaglutide consumption increases compared to lower doses. A vial that lasted 10 weeks at 0.5 mg may only last 3 weeks at 1.7 mg. Understanding your vial yield helps you plan refills and budget accordingly. The peptide cost calculator can help estimate your monthly costs based on your specific dose and concentration.
Some people switch to higher-concentration vials at this dose to reduce injection frequency (more medication per draw means fewer draws per vial). Others work with their pharmacy to find the most cost-effective concentration for their maintenance dose. SeekPeptides members gain access to detailed pharmacy comparisons and cost optimization strategies that can make a meaningful difference when you are committing to long-term therapy.
Understanding your syringe markings
Since getting 1.7 mg right depends entirely on reading your syringe correctly, let us look at each syringe type in detail.
1 mL (100-unit) syringe
This is the most common insulin syringe. It holds up to 1 mL of liquid, marked from 0 to 100 units. The large numbered markings typically appear at every 10 units (10, 20, 30, etc.). Between those, smaller lines mark every 2 units.
For 68 units (1.7 mg at 2.5 mg/mL), find the 60-unit line, then count 4 more small lines up. Each small line is 2 units: 62, 64, 66, 68. The plunger tip should align exactly with the 68-unit mark.
For 34 units (1.7 mg at 5 mg/mL), find the 30-unit line, then count 2 more small lines. That is 32, 34.
0.5 mL (50-unit) syringe
This syringe holds half the volume but has larger line spacing, making each unit easier to distinguish. Numbered markings typically appear at every 5 units, with individual lines marking each unit.
For 34 units on this syringe, find the 30-unit line and count 4 individual unit marks up. The precision advantage of this syringe makes it the preferred choice for 5 mg/mL concentrations at the 1.7 mg dose.
0.3 mL (30-unit) syringe
The smallest common insulin syringe. Perfect for high-concentration vials where you only need 17 units (1.7 mg at 10 mg/mL). The markings are the most spread apart, providing the best accuracy for small volumes. Each individual unit is clearly visible, and half-unit markings may also be present.
For 17 units, find the 15-unit line and count 2 more individual marks up. The small syringe size makes this measurement straightforward and nearly impossible to misread.
Our guide on converting units to milliliters provides additional clarity on how syringe readings translate to actual volumes.
Alcohol and semaglutide at 1.7 mg
Drinking alcohol while on semaglutide at any dose carries specific considerations, but these become more pronounced at higher doses like 1.7 mg.
Semaglutide slows gastric emptying. Alcohol in a stomach that empties slowly stays in contact with the stomach lining longer, potentially increasing irritation and nausea. At 1.7 mg, gastric emptying is significantly slower than at lower doses, which means alcohol effects may feel stronger, last longer, and cause more GI distress.
Alcohol also adds empty calories that work against weight loss goals. And it can lower inhibitions around food choices, potentially leading to high-calorie meals that negate the appetite-suppressive benefits of the medication.
The comprehensive guide on drinking on semaglutide covers all aspects of alcohol interaction, including which types of drinks tend to be better tolerated and how to minimize GI impact if you choose to drink occasionally.
Other medications and supplements with semaglutide at 1.7 mg
At this dose level, the question of what else you can safely take alongside semaglutide becomes more relevant. The slower gastric emptying at 1.7 mg affects the absorption of other oral medications, and some combinations deserve specific attention.
Phentermine and semaglutide is a combination some providers prescribe for additional appetite suppression. The phentermine vs semaglutide comparison explains the differences in mechanism and when combination therapy makes sense.
Supplements like B12 with semaglutide are popular because some users experience B12 deficiency symptoms at higher doses. Methylcobalamin, the active form of B12, can be taken separately or may already be included in your compounded formulation. The semaglutide methylcobalamin guide covers the rationale behind this combination.
Glycine is another supplement gaining attention among semaglutide users for its potential to reduce side effects and support joint health during rapid weight loss. Our semaglutide with glycine guide reviews the current evidence.
Always inform your provider about all supplements and medications before combining them with semaglutide at any dose. Drug interactions can affect both efficacy and safety, and the delayed gastric emptying at 1.7 mg may alter the timing and absorption of other oral medications you take.
What if you miss your 1.7 mg dose
Missing a weekly injection happens. Travel, illness, scheduling conflicts, and simple forgetfulness all contribute. The protocol for a missed dose at 1.7 mg follows the same general guidelines as any other dose level, but the specifics matter.
If fewer than 5 days have passed since your scheduled injection day, take the 1.7 mg dose as soon as you remember. Then resume your regular weekly schedule. Your next injection might be fewer than 7 days from this makeup dose, which is acceptable.
If more than 5 days have passed, skip the missed dose entirely and take your next scheduled 1.7 mg dose on your regular day. Do not double up. Taking 3.4 mg to "make up" for a missed dose creates the same overdose risks described in the safety section above.
Missed doses are also an opportunity to evaluate. If you have been on semaglutide long enough to reach the 1.7 mg step and suddenly missed a dose, pay attention to how you feel during the gap. Some people discover that their appetite returns aggressively within a few days of a missed dose, confirming the medication active role. Others barely notice, which may inform discussions with their provider about semaglutide withdrawal effects.
Using a semaglutide dosage calculator for verification
Mental math is fine. But when the consequences of an error include emergency hospitalization, verification tools are worth using.
The SeekPeptides semaglutide dosage calculator accepts your vial concentration and desired dose, then outputs the exact number of units. It works for every dose in the escalation schedule, including 1.7 mg, and covers all common concentrations.
A few ways to use the calculator for maximum safety. First, calculate your dose before your first draw at any new concentration. Second, cross-check your calculation against the chart in your pharmacy paperwork. Third, save or screenshot the result so you can reference it on injection day without recalculating. Fourth, recalculate whenever you receive a new vial, even from the same pharmacy, because concentrations can change between orders.
For those who also need to calculate reconstitution volumes, the peptide reconstitution calculator handles the water-to-powder math, and the general peptide calculator covers a broader range of peptide dosing scenarios beyond semaglutide.
SeekPeptides provides these tools free because dosing accuracy is too important to leave to rushed mental math or secondhand dosing charts from the internet. Getting the right number of units means getting the right dose, and getting the right dose means getting the results you are working toward.
Alternative delivery methods for semaglutide
While injectable semaglutide from vials is the most common form requiring unit calculations, alternative delivery methods exist and are worth understanding.
Oral semaglutide drops bypass the injection and syringe process entirely. These sublingual formulations absorb through the tissues under your tongue, and dosing is measured in milligrams directly rather than converted to units. Our semaglutide sublingual guide covers the differences in bioavailability and dosing between oral and injectable forms.
For people who are uncomfortable with injections or struggle with unit conversions, oral alternatives eliminate several categories of dosing error. However, oral semaglutide has different absorption characteristics and may require different dosing amounts to achieve equivalent blood levels. The choice between injectable vs oral peptides involves trade-offs in convenience, accuracy, bioavailability, and cost.
Double-checking your dose: a verification protocol
Experienced semaglutide users develop a pre-injection routine that catches errors before they happen. This is not excessive caution. It is the standard of care that prevents the hospitalization cases described throughout this article.
Step one: read your vial label and confirm the concentration. Write the number down or say it aloud. "My vial is 5 mg per mL."
Step two: state your intended dose. "I need 1.7 mg."
Step three: calculate or reference your units. "At 5 mg per mL, 1.7 mg equals 34 units."
Step four: confirm your syringe capacity. "My 0.5 mL syringe holds 50 units, so 34 units fits."
Step five: draw, verify at eye level, and inject.
This five-step verification takes under thirty seconds. It sounds redundant. It sounds like overkill. But every single serious dosing error reported to the FDA could have been prevented by any one of these five checkpoints. The cost of verification is half a minute. The cost of a dosing error is a trip to the emergency department, days of severe symptoms, and potentially serious complications that no one signed up for when they started a weight management protocol.
For people who want a permanent quick reference, the semaglutide dosage chart in units can be printed and kept with your supplies. Having a physical reference eliminates the need to recalculate from memory each week, especially on mornings when you are tired, distracted, or rushing through your routine.
SeekPeptides members get access to downloadable dosing reference cards, personalized to their specific vial concentration, that serve exactly this purpose. One glance, one number, zero guesswork.
Frequently asked questions
Is 68 units of semaglutide the same as 1.7 mg?
Only if your vial concentration is 2.5 mg/mL. At 5 mg/mL, 1.7 mg equals 34 units. At 10 mg/mL, it equals 17 units. The number of units always depends on the concentration. Check your vial label before every draw. Our semaglutide unit conversion chart covers all concentrations.
Can I use a 0.5 mL syringe for my 1.7 mg dose?
It depends on your concentration. At 5 mg/mL (34 units), a 0.5 mL syringe works perfectly. At 2.5 mg/mL (68 units), you need a 1 mL syringe because 68 units exceeds the 50-unit capacity of a half-mL syringe. At 10 mg/mL (17 units), a 0.3 mL syringe provides the most accurate reading.
What happens if I accidentally inject more than 1.7 mg?
Mild overdoses (up to about 2.4 mg) typically cause increased nausea, vomiting, and gastrointestinal discomfort. Larger overdoses can lead to severe dehydration, fainting, and in rare cases, acute pancreatitis. If you believe you have significantly overdosed, contact your healthcare provider or seek emergency care. Monitor for severe abdominal pain, persistent vomiting, and signs of dehydration.
How long does one vial last at the 1.7 mg dose?
For a 5 mg total vial: approximately 2.9 weekly doses (about 3 weeks). For a 10 mg total vial: approximately 5.9 weekly doses (about 6 weeks). For a 20 mg total vial: approximately 11.8 weekly doses (about 12 weeks). Calculate by dividing the total milligrams in the vial by 1.7. See our semaglutide shelf life guide to ensure your vial remains viable for its full use period.
Should I stay at 1.7 mg or go to 2.4 mg?
This is a clinical decision that depends on your weight loss progress, side effect tolerance, and provider recommendation. If 1.7 mg is producing consistent results with tolerable side effects, staying there is a valid option. The FDA approves 1.7 mg as a maintenance dose for those who do not tolerate 2.4 mg. Discuss the benefits and trade-offs with your provider based on your specific situation.
Is 1.7 mg the same as the step 4 Wegovy dose?
Yes. The Wegovy dose escalation schedule designates 1.7 mg as step 4, taken during weeks 13 to 16 before the final escalation to the 2.4 mg maintenance dose. Compounded semaglutide follows the same escalation protocol when prescribed for weight management.
Can I split my 1.7 mg dose into two injections per week?
Some providers do prescribe split dosing, typically 0.85 mg twice weekly instead of 1.7 mg once weekly, to reduce side effects. The total weekly amount remains the same, but the peak blood levels are lower, which can reduce nausea. However, this requires recalculating your units per injection. At 2.5 mg/mL, each split dose would be 34 units. Always get provider approval before changing your dosing schedule.
Why does my pharmacy use a different concentration than what this guide lists?
Compounding pharmacies have flexibility in choosing their formulation concentration. Some prefer 2.5 mg/mL for ease of measurement, others use 5 mg/mL to reduce injection volume, and some use custom concentrations based on their specific formulation process. The conversion formula works for any concentration: (Dose in mg / Concentration in mg per mL) x 100 = Units.
External resources
For researchers serious about optimizing their semaglutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, personalized dosing calculators, and a community of thousands who have navigated these exact questions about unit conversions, dose escalation, and long-term protocol management.
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your doses stay precise, and your results stay consistent.