Feb 5, 2026

Conflicting charts. Confusing labels. Three different answers from three different sources. If you have searched "20 units of semaglutide is how many mg" and gotten a different number every time, you are not alone. This is one of the most common and most dangerous points of confusion in the entire GLP-1 space.
Here is the short answer: it depends on your concentration.
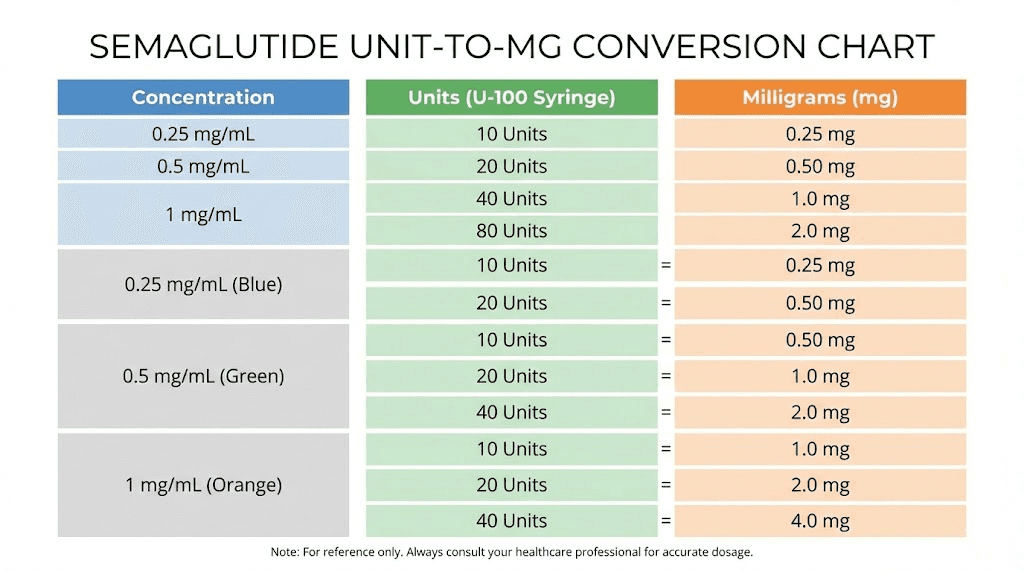
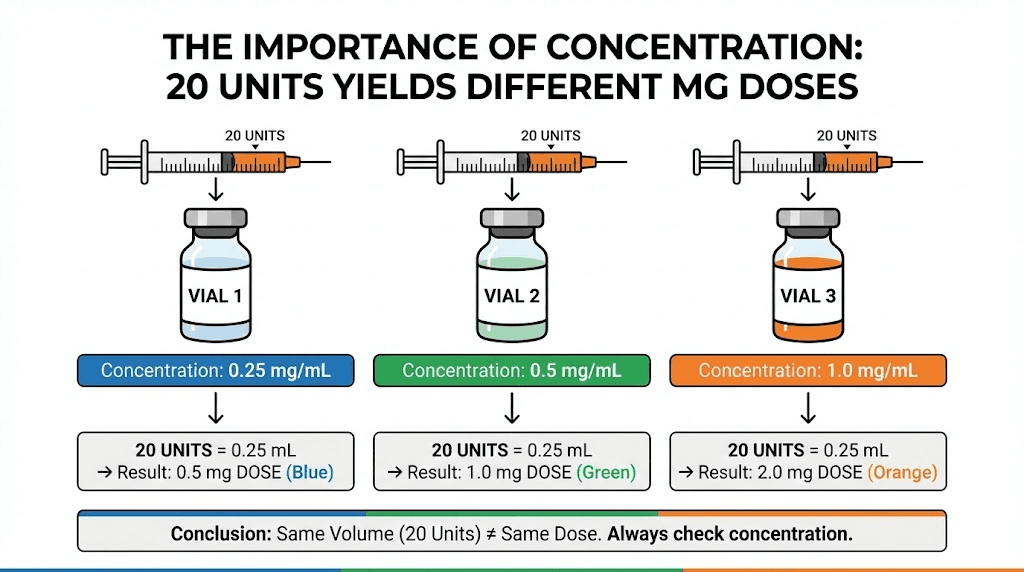
Twenty units drawn on an insulin syringe is not a fixed milligram amount. It changes based on how many milligrams of semaglutide are dissolved in each milliliter of solution. With a 5 mg/mL vial, 20 units equals 1 mg. With a 2.5 mg/mL vial, 20 units equals 0.5 mg. With a 1 mg/mL vial, 20 units equals only 0.2 mg. Same syringe marking. Wildly different doses. And the FDA has documented cases where this exact confusion led to overdoses five to twenty times higher than intended.
This guide will break down every concentration you might encounter, show you how to calculate the conversion yourself, provide complete reference charts for quick lookups, and explain the safety protocols that prevent dosing errors. Whether you are working with brand-name semaglutide products or compounded formulations, the math works the same way once you understand the underlying principle. SeekPeptides has helped thousands of researchers navigate exactly this kind of dosing confusion, and this guide covers everything you need to convert units to milligrams accurately every single time.
Why units and milligrams are not the same thing
This is where the confusion starts. And it is where most dosing errors originate.
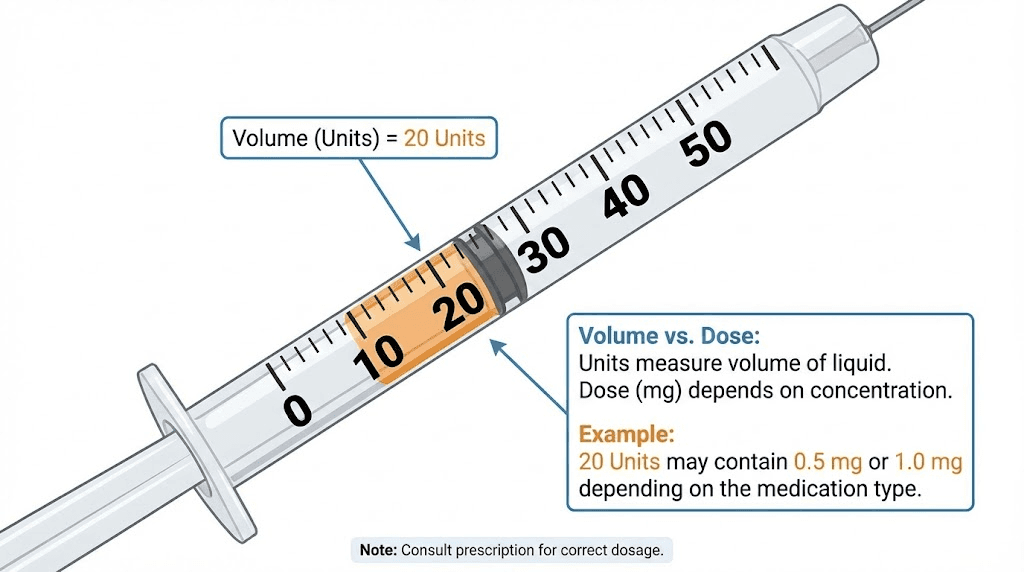
Units on an insulin syringe measure volume. Specifically, they measure hundredths of a milliliter. One unit equals 0.01 mL. Ten units equals 0.1 mL. Twenty units equals 0.2 mL. One hundred units equals a full 1 mL. The syringe does not know and does not care what is dissolved in the liquid. It only measures how much liquid you are drawing.
Milligrams measure the actual amount of active medication. This is the number your dosing protocol specifies. When a protocol says "take 0.5 mg of semaglutide," it means 0.5 milligrams of the active compound, regardless of how much liquid contains that amount.
The bridge between these two measurements is concentration.
Concentration tells you how many milligrams of semaglutide are dissolved in each milliliter of solution. A vial labeled "5 mg/mL" contains 5 milligrams of semaglutide in every milliliter. A vial labeled "2.5 mg/mL" contains half that amount per milliliter. Same volume of liquid, different amounts of medication.
Think of it like this. Two cups of coffee can look identical. Same amount of liquid. But one might have a single shot of espresso and the other might have a triple. The cup size (volume) stays the same. The caffeine content (concentration) changes everything. Your syringe is the cup. The concentration on your vial label tells you how strong that "coffee" is.
The formula that makes everything clear
Once you understand the relationship between units, volume, and concentration, one formula handles every conversion you will ever need:
Dose in mg = (Units / 100) x Concentration in mg/mL
That is it. Three numbers. One multiplication. And you have your milligram dose.
For 20 units with a 5 mg/mL concentration: (20 / 100) x 5 = 1 mg. For 20 units with a 2.5 mg/mL concentration: (20 / 100) x 2.5 = 0.5 mg. For 20 units with a 1 mg/mL concentration: (20 / 100) x 1 = 0.2 mg.
You can also reverse this formula when you know the milligram dose you want and need to figure out how many units to draw:
Units = (Desired dose in mg / Concentration in mg/mL) x 100
Want 0.25 mg from a 5 mg/mL vial? (0.25 / 5) x 100 = 5 units. Want 0.5 mg from a 2.5 mg/mL vial? (0.5 / 2.5) x 100 = 20 units. The semaglutide dosage calculator on SeekPeptides does this math automatically, but understanding the formula yourself adds an essential layer of safety verification.
Why insulin syringes use "units" instead of milliliters
Insulin syringes were designed for insulin, which is standardized at 100 units per milliliter (U-100). In that context, "units" made perfect sense because one unit of insulin always equaled one unit of biological activity. The markings on the syringe directly corresponded to the dose.
But semaglutide is not insulin. It has no standardized "unit" measurement. When you use an insulin syringe to draw semaglutide, the "unit" markings are simply measuring volume in hundredths of a milliliter. The word "units" on your syringe has nothing to do with semaglutide dosing units. This linguistic overlap is precisely why the FDA issued warnings about dosing errors with compounded semaglutide.
Complete conversion charts for every common concentration
Below are the reference charts for every semaglutide concentration you are likely to encounter. Find your vial concentration, then look up the unit marking to find your milligram dose. These charts eliminate the need for mental math during injection preparation.
1 mg/mL concentration
This is one of the lower concentrations available. You will need to draw more liquid for each dose, which some researchers prefer for accuracy with small doses.
Syringe units | Volume (mL) | Semaglutide dose (mg) |
|---|---|---|
5 units | 0.05 mL | 0.05 mg |
10 units | 0.10 mL | 0.10 mg |
15 units | 0.15 mL | 0.15 mg |
20 units | 0.20 mL | 0.20 mg |
25 units | 0.25 mL | 0.25 mg |
30 units | 0.30 mL | 0.30 mg |
40 units | 0.40 mL | 0.40 mg |
50 units | 0.50 mL | 0.50 mg |
100 units | 1.00 mL | 1.00 mg |
At 1 mg/mL, the math is the simplest. Units divided by 100 gives you both the volume in mL and the dose in mg. They are the same number. Twenty units is always 0.2 mg at this concentration. For researchers working with peptide dosage calculations for the first time, this concentration offers the most straightforward measurement experience.
2 mg/mL concentration
A mid-range concentration that balances accuracy with convenience. Common in some compounded formulations.
Syringe units | Volume (mL) | Semaglutide dose (mg) |
|---|---|---|
5 units | 0.05 mL | 0.10 mg |
10 units | 0.10 mL | 0.20 mg |
12.5 units | 0.125 mL | 0.25 mg |
15 units | 0.15 mL | 0.30 mg |
20 units | 0.20 mL | 0.40 mg |
25 units | 0.25 mL | 0.50 mg |
30 units | 0.30 mL | 0.60 mg |
40 units | 0.40 mL | 0.80 mg |
50 units | 0.50 mL | 1.00 mg |
100 units | 1.00 mL | 2.00 mg |
At this concentration, 20 units delivers 0.4 mg of semaglutide. Notice how the milligram dose is exactly double the volume in mL. If you are transitioning from a 1 mg/mL vial to a 2 mg/mL vial, you need to draw exactly half the volume to get the same dose. This is a common source of errors when researchers switch between different reconstitution concentrations.
2.5 mg/mL concentration
One of the most common concentrations for compounded semaglutide. Many pharmacies use this as their standard formulation.
Syringe units | Volume (mL) | Semaglutide dose (mg) |
|---|---|---|
5 units | 0.05 mL | 0.125 mg |
10 units | 0.10 mL | 0.25 mg |
15 units | 0.15 mL | 0.375 mg |
20 units | 0.20 mL | 0.50 mg |
25 units | 0.25 mL | 0.625 mg |
30 units | 0.30 mL | 0.75 mg |
40 units | 0.40 mL | 1.00 mg |
50 units | 0.50 mL | 1.25 mg |
60 units | 0.60 mL | 1.50 mg |
80 units | 0.80 mL | 2.00 mg |
100 units | 1.00 mL | 2.50 mg |
At 2.5 mg/mL, 20 units gives you 0.5 mg. This is a particularly convenient concentration because the standard starting dose of 0.25 mg falls on a clean 10-unit mark. The dose escalation steps also align reasonably well with standard syringe markings. Many peptide therapy clinics prefer this concentration for exactly that reason.
3 mg/mL concentration
Less common but still encountered, particularly in some compounded preparations.
Syringe units | Volume (mL) | Semaglutide dose (mg) |
|---|---|---|
5 units | 0.05 mL | 0.15 mg |
8.3 units | 0.083 mL | 0.25 mg |
10 units | 0.10 mL | 0.30 mg |
16.7 units | 0.167 mL | 0.50 mg |
20 units | 0.20 mL | 0.60 mg |
25 units | 0.25 mL | 0.75 mg |
33.3 units | 0.333 mL | 1.00 mg |
50 units | 0.50 mL | 1.50 mg |
100 units | 1.00 mL | 3.00 mg |
Notice how the standard dose increments (0.25 mg, 0.5 mg, 1.0 mg) fall on awkward syringe markings at this concentration. That is one reason this concentration is less popular. Drawing 8.3 units or 16.7 units precisely on a standard insulin syringe is difficult and introduces measurement error. If your pharmacy provided this concentration, consider using the peptide calculator for double-checking your volumes before each injection.
5 mg/mL concentration
This is the concentration used in brand-name Ozempic 1 mg pens and one of the most common concentrations in compounded vials. It is also the concentration most conversion charts reference online.
Syringe units | Volume (mL) | Semaglutide dose (mg) |
|---|---|---|
5 units | 0.05 mL | 0.25 mg |
10 units | 0.10 mL | 0.50 mg |
15 units | 0.15 mL | 0.75 mg |
20 units | 0.20 mL | 1.00 mg |
25 units | 0.25 mL | 1.25 mg |
30 units | 0.30 mL | 1.50 mg |
34 units | 0.34 mL | 1.70 mg |
40 units | 0.40 mL | 2.00 mg |
48 units | 0.48 mL | 2.40 mg |
50 units | 0.50 mL | 2.50 mg |
100 units | 1.00 mL | 5.00 mg |
At 5 mg/mL, 20 units equals exactly 1.0 mg. This is why many online sources simply state "20 units = 1 mg" without mentioning concentration. They are assuming 5 mg/mL. But if your vial is a different concentration, that answer is wrong and potentially dangerous. Always verify your concentration first. The 40-unit conversion guide covers the higher end of this chart in more detail.
10 mg/mL concentration
Higher concentrations like this appear in some compounded preparations, particularly for researchers on maintenance doses who want smaller injection volumes.
Syringe units | Volume (mL) | Semaglutide dose (mg) |
|---|---|---|
2.5 units | 0.025 mL | 0.25 mg |
5 units | 0.05 mL | 0.50 mg |
10 units | 0.10 mL | 1.00 mg |
15 units | 0.15 mL | 1.50 mg |
17 units | 0.17 mL | 1.70 mg |
20 units | 0.20 mL | 2.00 mg |
24 units | 0.24 mL | 2.40 mg |
25 units | 0.25 mL | 2.50 mg |
50 units | 0.50 mL | 5.00 mg |
At 10 mg/mL, 20 units delivers a full 2.0 mg. That is a significant dose, close to the maximum maintenance dose for weight management. At this concentration, even small measurement errors create large dose differences. Drawing 25 units instead of 20 units means taking 2.5 mg instead of 2.0 mg, a 25% overdose. Accuracy matters enormously at higher concentrations. Using a reconstitution calculator to verify your math is not optional with concentrations this high.
How to find your concentration
Before you can convert anything, you need to know your concentration. This sounds obvious, but it is the step most people skip, and the step where most errors begin.
Brand-name products
Ozempic pens come in three dosing tiers. The 0.25 mg and 0.5 mg pen uses a concentration of approximately 1.34 mg/mL. The 1 mg pen uses approximately 2.68 mg/mL. The 2 mg pen uses approximately 5.36 mg/mL. However, Ozempic pens have a built-in dose selector, so you rarely need to convert units manually. You dial your dose and the pen delivers it.
Wegovy pens come pre-filled at five dose levels: 0.25 mg, 0.5 mg, 1 mg, 1.7 mg, and 2.4 mg. Each pen delivers exactly one dose. There are no unit conversions needed because you are not drawing from a vial.
The conversion question, "20 units is how many mg," almost always applies to people using compounded semaglutide from multi-dose vials with insulin syringes.
Compounded semaglutide vials
Your vial label is your concentration source. Look for a number expressed as mg/mL. Common concentrations include 1 mg/mL, 2 mg/mL, 2.5 mg/mL, 3 mg/mL, 5 mg/mL, and 10 mg/mL. Some pharmacies also use unusual concentrations like 2.4 mg/mL or 3.33 mg/mL.
If your vial does not clearly state the concentration, do not guess. Contact the pharmacy that compounded it. Using the wrong concentration in your calculations can result in doses five to twenty times higher than intended. The safety implications are serious.
Lyophilized (freeze-dried) powder
If you received semaglutide as a lyophilized powder that you reconstitute yourself, then you determine the concentration based on how much bacteriostatic water you add.
The formula: Concentration (mg/mL) = Total mg of powder / Total mL of water added
A 5 mg vial reconstituted with 2 mL of bacteriostatic water gives you 2.5 mg/mL. The same 5 mg vial reconstituted with 1 mL gives you 5 mg/mL. And with 5 mL, you get 1 mg/mL. You choose your concentration by choosing how much water to add. Our peptide reconstitution calculator makes this straightforward.
Here are the most common reconstitution scenarios for a 5 mg vial:
Water added | Resulting concentration | 20 units equals |
|---|---|---|
1 mL | 5 mg/mL | 1.0 mg |
2 mL | 2.5 mg/mL | 0.5 mg |
2.5 mL | 2 mg/mL | 0.4 mg |
5 mL | 1 mg/mL | 0.2 mg |
And for a 10 mg vial:
Water added | Resulting concentration | 20 units equals |
|---|---|---|
1 mL | 10 mg/mL | 2.0 mg |
2 mL | 5 mg/mL | 1.0 mg |
3 mL | 3.33 mg/mL | 0.67 mg |
4 mL | 2.5 mg/mL | 0.5 mg |
5 mL | 2 mg/mL | 0.4 mg |
10 mL | 1 mg/mL | 0.2 mg |
Record your reconstitution details somewhere permanent. Write the concentration on the vial with a marker. Tape a note to the vial. Store it in a proper peptide storage container with the concentration clearly labeled. You will need this number every single time you draw a dose.
The standard semaglutide dosing schedule in units
Understanding how the standard dose escalation schedule translates into syringe units makes the practical application much clearer. The FDA-approved titration schedule for weight loss with semaglutide follows a gradual increase designed to minimize gastrointestinal side effects.
Dose escalation by concentration
Phase | Weekly dose | Duration | Units at 2.5 mg/mL | Units at 5 mg/mL |
|---|---|---|---|---|
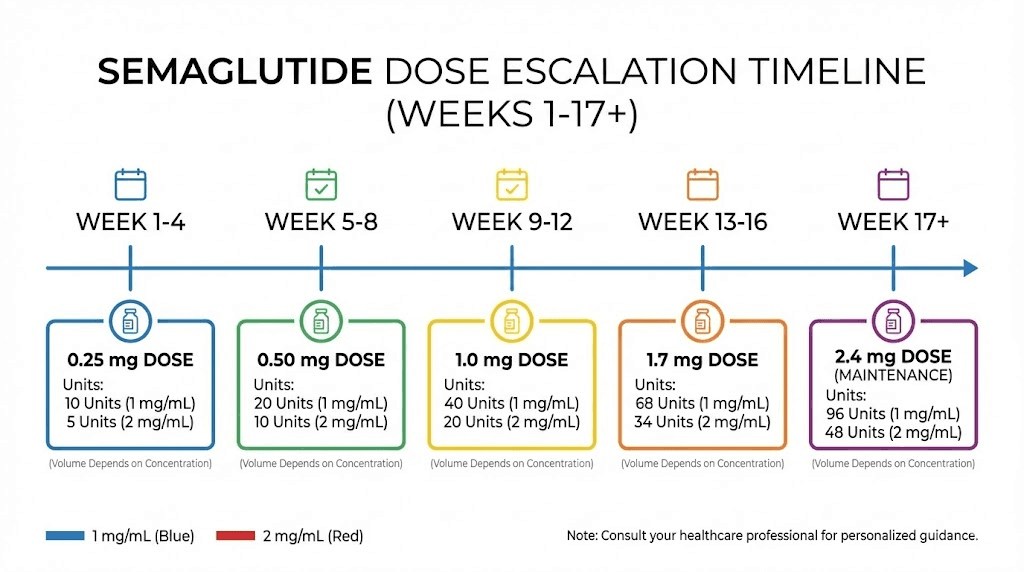
Loading | 0.25 mg | Weeks 1-4 | 10 units | 5 units |
Step 2 | 0.50 mg | Weeks 5-8 | 20 units | 10 units |
Step 3 | 1.00 mg | Weeks 9-12 | 40 units | 20 units |
Step 4 | 1.70 mg | Weeks 13-16 | 68 units | 34 units |
Maintenance | 2.40 mg | Week 17+ | 96 units | 48 units |
Look at how dramatically the unit amounts differ between concentrations. At 5 mg/mL, 20 units gives you 1 mg, your week 9-12 dose. At 2.5 mg/mL, 20 units gives you 0.5 mg, your week 5-8 dose. Same syringe reading, completely different point in your protocol. Getting this wrong means either underdosing by half or overdosing by double.
This is exactly why appetite suppression timelines vary so widely between users. Some of the discrepancy comes from individual biology. But some comes from people accidentally taking the wrong dose because they used the wrong concentration in their calculations.
Why the slow escalation matters
Semaglutide activates GLP-1 receptors in the gut, pancreas, and brain. The slow titration schedule exists because your body needs time to adapt to increased GLP-1 receptor activation. Jumping from 0.25 mg directly to 1 mg, which can happen with a single concentration mix-up, commonly causes severe nausea, vomiting, and in some cases, serious gastrointestinal distress.
The FDA documented over 520 adverse event reports related to compounded semaglutide as of April 2025. Many of these involved dosing errors where patients administered five to twenty times more than intended. The most common cause? Confusing units and milligrams. Not understanding concentration. Drawing 50 units when they meant 5 units because the syringe markings confused them.
If you are working with compounded semaglutide and using insulin syringes, you are responsible for accurate dosing. There is no built-in safety mechanism like a pre-filled pen provides. The semaglutide dosage calculator exists specifically to reduce this risk.
Common dosing errors and how to prevent them
The FDA and poison control centers have documented specific patterns of dosing errors with compounded semaglutide. Understanding these patterns is the best way to avoid repeating them.
Error 1: confusing units with the dose
A provider tells a patient to "take 5 units." The patient sees the number 5 on their syringe and draws to that line. But the syringe marking at "5" on some syringes actually indicates 50 units (0.5 mL), not 5 units (0.05 mL). The patient takes ten times the intended dose.
Prevention: Always confirm the actual volume in mL. Five units equals 0.05 mL. If you drew more than a tiny amount of liquid for a 5-unit dose, something is wrong. Stop. Verify. The amount of liquid for small semaglutide doses is surprisingly small.
Error 2: using the wrong concentration
A patient has been using a 2.5 mg/mL vial and drawing 10 units (0.25 mg) weekly. Their pharmacy switches them to a 5 mg/mL vial. They draw the same 10 units. Now they are taking 0.5 mg, double their intended dose.
Prevention: Every time you start a new vial, check the concentration on the label. Recalculate your units. Better yet, run the numbers through a calculator to verify. Never assume a new vial has the same concentration as the last one.
Error 3: not accounting for reconstitution volume
A researcher reconstitutes a 5 mg vial with 2 mL of bacteriostatic water (creating 2.5 mg/mL) but uses a 5 mg/mL conversion chart they found online. Every dose is double what they think it is.
Prevention: Calculate your concentration immediately after reconstitution. Write it on the vial. Use YOUR concentration for all calculations, not a generic chart from the internet. Generic charts assume a specific concentration that may not match yours.
Error 4: confusing mL with units
A patient is told to inject "0.25 mL" and draws to the 25-unit mark, thinking 25 units equals 0.25 mL. In reality, 25 units equals 0.25 mL, so this particular example happens to be correct. But a patient told to inject "0.5 mL" might draw to the "5" mark (5 units = 0.05 mL) instead of the "50" mark (50 units = 0.5 mL), getting one-tenth the intended dose.
Prevention: Always convert your dose to units before picking up the syringe. Know exactly which number on the syringe you are drawing to. Use the peptide dosage calculation guide if any step feels uncertain.
Error 5: using the wrong syringe type
Not all insulin syringes are created equal. U-100 syringes (100 units per mL) are the standard in the United States. But U-40 syringes (40 units per mL) exist for veterinary use, and U-50 syringes are used in some countries. Drawing "20 units" on a U-40 syringe delivers 0.5 mL, not 0.2 mL, a 2.5x overdose.
Prevention: Only use U-100 insulin syringes for semaglutide dosing. Check the packaging. The syringe should be marked "U-100" or "100 units/mL." If your syringe delivery device has different markings, do not use it.
Step-by-step guide to drawing your dose
Knowing the math is essential. But applying it correctly during the actual injection process requires a systematic approach. Follow these steps every time.
Before you begin
Gather your supplies. You need your semaglutide vial, a U-100 insulin syringe (typically 0.3 mL or 0.5 mL for semaglutide doses), alcohol swabs, and a sharps container. Check the vial label for concentration. Verify the expiration date. Make sure the solution is clear and colorless. If it is cloudy, discolored, or contains particles, do not use it. Review proper injection techniques if you are new to this process.
Step 1: calculate your dose in units
Use the formula: Units = (Desired mg dose / Concentration in mg/mL) x 100
Example: You want 0.5 mg from a 2.5 mg/mL vial. (0.5 / 2.5) x 100 = 20 units.
Write this number down. Do not rely on memory.
Step 2: prepare the vial
Remove the cap. Clean the rubber stopper with an alcohol swab. Let it dry for a few seconds. Do not blow on it or touch it after cleaning.
Step 3: prepare the syringe
Remove the needle cap. Pull back the plunger to draw air equal to the number of units you plan to withdraw. Push the needle through the rubber stopper. Inject the air into the vial. This prevents a vacuum from forming inside the vial.
Step 4: draw your dose
Turn the vial upside down with the needle still inserted. Slowly pull the plunger back to your target unit marking. Make sure the needle tip stays submerged in the liquid. If air bubbles appear, tap the syringe gently to move them to the top, push them back into the vial, and redraw.
Step 5: verify
Before removing the needle from the vial, check the syringe one more time. Is the plunger at the correct unit marking? Are there any air bubbles that could reduce your dose? Is the amount of liquid consistent with what you expect? For small doses (5-10 units), the liquid volume will be very small, barely visible in the syringe.
Step 6: inject
Clean the injection site with an alcohol swab. Pinch the skin. Insert the needle at a 45-90 degree angle. Slowly push the plunger all the way down. Hold for 5-10 seconds. Remove the needle. Do not rub the injection site. Apply light pressure if needed.
Step 7: record
Log your dose, the time, the date, the injection site, and the vial concentration. This record becomes invaluable for cycle planning and troubleshooting if you experience unexpected effects.
Special considerations for different syringe sizes
Insulin syringes come in three main sizes: 0.3 mL (30 units), 0.5 mL (50 units), and 1 mL (100 units). The size you choose affects your ability to measure accurately.
0.3 mL (30-unit) syringe
Best for small doses. Each unit marking represents a larger physical distance on the barrel, making it easier to draw precise small volumes. If your dose is under 30 units, this is the most accurate option. The downside: you cannot draw more than 30 units at a time. For higher maintenance doses, you will need a larger syringe.
0.5 mL (50-unit) syringe
The most versatile option. Handles both loading doses and most maintenance doses for concentrations of 2.5 mg/mL and above. Good accuracy for doses between 10 and 50 units. This is the syringe most researchers prefer for semaglutide.
1 mL (100-unit) syringe
Required for large volumes, such as lower concentration vials at higher doses. The trade-off: each unit marking represents a smaller physical distance, making small dose measurements less precise. If you are drawing less than 20 units on a 100-unit syringe, consider switching to a smaller syringe for better accuracy.
The syringe size does not change the math. Twenty units on a 30-unit syringe is the same volume as 20 units on a 100-unit syringe, both are 0.2 mL. The difference is purely in measurement precision and practical usability.
How 20 units compares across GLP-1 medications
Semaglutide is not the only GLP-1 receptor agonist available. If you are researching or have used other GLP-related peptides, understanding how 20 units translates across different medications provides helpful context.
Semaglutide vs tirzepatide at 20 units
Tirzepatide is a dual GIP/GLP-1 receptor agonist that uses different concentrations and dosing protocols than semaglutide. A direct unit-to-unit comparison is meaningless without accounting for concentration, potency, and receptor activity differences.
Tirzepatide concentrations in compounded forms commonly range from 10 mg/mL to 60 mg/mL. At 30 mg/mL, 20 units (0.2 mL) delivers 6 mg of tirzepatide. The tirzepatide dosing guide in units covers these conversions in full detail. The 2.5 mg tirzepatide conversion is another common starting point for comparison.
Other GLP-1 and weight management peptides
The same concentration-dependent conversion applies to every peptide you will encounter. Twenty units is always 0.2 mL of liquid. What changes is how much active compound is dissolved in that liquid. Whether you are researching retatrutide, cagrilintide, or any other weight loss peptide, the fundamental conversion formula remains the same: dose in mg equals units divided by 100 multiplied by concentration in mg/mL.
This universality is one of the most powerful concepts in peptide dosage calculation. Learn it once, apply it everywhere.
Reconstitution math for DIY researchers
If you are reconstituting semaglutide from lyophilized powder, you have the unique advantage of choosing your concentration. This section covers how to choose wisely and calculate everything correctly.
Choosing your target concentration
The ideal concentration depends on your dose and your preferred injection volume. Here are the considerations:
Higher concentrations (5-10 mg/mL) mean smaller injection volumes, which is more comfortable. But smaller volumes are harder to measure precisely. A half-unit error at 10 mg/mL changes your dose by 0.05 mg. That might not sound like much, but at the loading dose of 0.25 mg, that is a 20% error.
Lower concentrations (1-2 mg/mL) mean larger injection volumes, which is slightly less comfortable but significantly easier to measure accurately. A half-unit error at 1 mg/mL changes your dose by only 0.005 mg, a 2% error at the 0.25 mg loading dose.
For most researchers, 2.5 mg/mL represents the best balance between accuracy and convenience. It maps cleanly to the standard dosing protocol, and the injection volumes are manageable without sacrificing precision.
Reconstitution example: 5 mg vial
You have a 5 mg vial of lyophilized semaglutide and you want a 2.5 mg/mL concentration.
Water needed: 5 mg / 2.5 mg/mL = 2 mL
Add exactly 2 mL of bacteriostatic water to the vial. Swirl gently. Do not shake. Label the vial "2.5 mg/mL" with the date.
Now your dosing: the starting dose of 0.25 mg requires (0.25 / 2.5) x 100 = 10 units. Your step-two dose of 0.5 mg requires (0.5 / 2.5) x 100 = 20 units. Your step-three dose of 1.0 mg requires (1.0 / 2.5) x 100 = 40 units.
Total vial contents: 5 mg. At the starting dose of 0.25 mg per week, one vial lasts 20 weeks. At the maintenance dose of 2.4 mg per week, one vial lasts about two weeks. Factor in reconstituted peptide shelf life, typically 28-30 days refrigerated, when planning your reconstitution timing.
Reconstitution example: 10 mg vial
A 10 mg vial gives you more flexibility. For a 5 mg/mL concentration: add 2 mL of water. For 2.5 mg/mL: add 4 mL. For 2 mg/mL: add 5 mL.
The higher starting amount means a single vial can last through more of your dose escalation period, reducing the number of reconstitutions and minimizing the chance of concentration errors between vials. Store reconstituted vials properly refrigerated at 36-46 degrees Fahrenheit (2-8 degrees Celsius).
Troubleshooting common questions
Even with clear charts and formulas, specific situations create confusion. Here are the questions SeekPeptides researchers ask most frequently.
My pharmacy gave me a different concentration than last time
This happens regularly with compounded medications. You must recalculate your dose in units every time your concentration changes. Do not assume the new vial matches the old one. Write down the new concentration and run the math fresh. A dosage calculator simplifies this transition.
I accidentally drew too much. What do I do?
If you have not injected yet, simply push the excess back into the vial or dispose of the syringe and start over with a new one. If you already injected an overdose, monitor for symptoms: severe nausea, vomiting, dizziness, or low blood sugar. Seek medical attention for significant overdoses. The risk increases with the size of the excess, a 10% overdose is very different from a 500% overdose.
Can I split a larger dose into two injections?
Yes. If your calculated dose requires a volume larger than your syringe can hold, you can split it into two injections given at the same time in different sites. Each injection should contain the correct proportional amount. For example, if your total dose is 60 units, you can draw 30 units twice. The injection site rotation guide covers how to manage multiple injection sites.
My syringe has half-unit markings. Can I use them?
Some 0.3 mL syringes include half-unit markings (0.5, 1.5, 2.5 units, etc.). These are helpful for very precise small doses. At 5 mg/mL, a half-unit increment changes your dose by 0.025 mg. At 2.5 mg/mL, it changes by 0.0125 mg. Whether this precision matters depends on your protocol and how sensitive you are to small dose changes.
I am switching from a pen to a vial. How do I convert?
This is where most concentration confusion begins. Your pen delivers a specific milligram dose automatically. To replicate that dose with a vial and syringe, you need to know two things: the milligram dose you were taking and the concentration of your new vial. Then apply the formula: Units = (mg dose / concentration) x 100. The pen dose in mg is your target. The vial concentration determines how many units you draw.
How do I know if my semaglutide has gone bad?
Reconstituted semaglutide should be clear and colorless. Cloudiness, particles, unusual color, or a change in viscosity all indicate degradation. Exposure to heat, light, or freezing can damage the peptide. Improper storage is the most common reason for degradation. Expired peptides may lose potency even if they look normal.
Advanced dosing considerations
Beyond basic conversion, several factors affect how you should approach semaglutide dosing.
Weight-based dosing considerations
The standard semaglutide protocol uses fixed doses (0.25 mg, 0.5 mg, 1 mg, 1.7 mg, 2.4 mg) regardless of body weight. This differs from some other peptides that use weight-based protocols where dose scales with body mass.
Some researchers and clinicians advocate for weight-adjusted semaglutide dosing, particularly for individuals at the extremes of body weight. A 130-pound person may reach effective appetite suppression at lower absolute doses than a 300-pound person. Conversely, higher body weight may require the full dose escalation to achieve meaningful results.
This does not change the unit-to-mg conversion. It only affects which milligram dose you target. The math remains the same regardless of your protocol.
Microdosing semaglutide
Some researchers experiment with doses below the standard 0.25 mg starting point. At very small doses, concentration and syringe selection become critical. Drawing 2 units accurately on a 100-unit syringe is nearly impossible. Use a 0.3 mL (30-unit) syringe with half-unit markings. Choose a lower concentration so that your target dose falls on a readable syringe marking.
For example, if you want to try 0.125 mg: at 2.5 mg/mL, you would need 5 units, a comfortably readable marking. At 5 mg/mL, you would need 2.5 units, possible with half-unit markings but tricky. At 1 mg/mL, you would need 12.5 units, easy to read and draw. Similar precision matters with microdosing tirzepatide protocols.
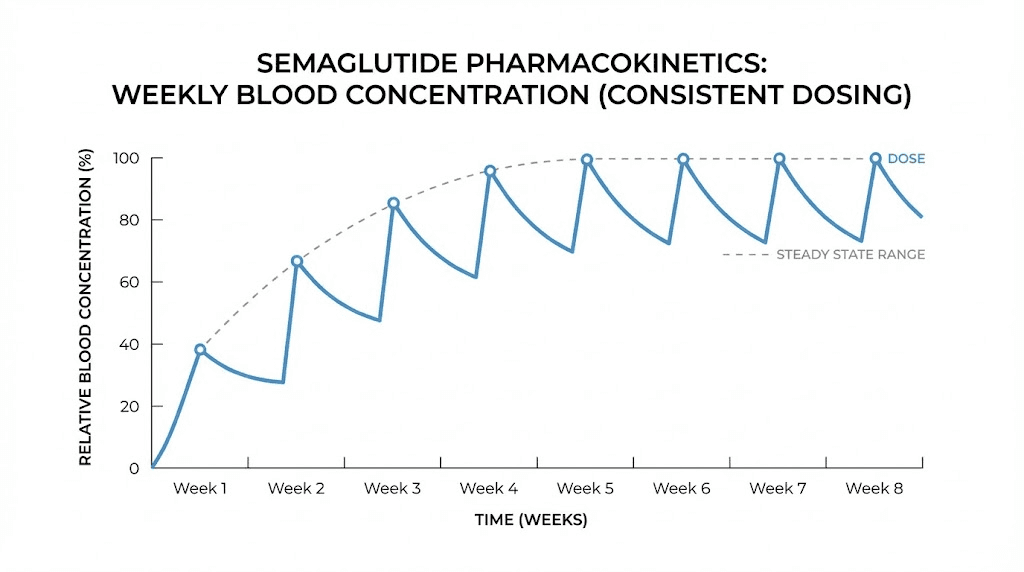
Dose timing and injection frequency
Semaglutide has a half-life of approximately seven days, which is why it is dosed once weekly. The unit amount you draw does not change based on what day you inject. However, consistent timing (same day each week, roughly the same time) helps maintain stable blood levels. If you miss a dose and it has been less than five days, take it as soon as you remember. If more than five days have passed, skip the missed dose and take the next one on your regular schedule.
Understanding the pharmacokinetics helps explain how long semaglutide takes to suppress appetite and why consistent weekly dosing matters for sustained results. Some researchers also wonder about why they are not losing weight on semaglutide, and dosing accuracy is often the first thing to investigate.
Quick reference: what does 20 units equal at every concentration
This is the master reference. Bookmark it. Print it. Tape it to your refrigerator next to your vial.
Concentration | 20 units (0.2 mL) equals | Context |
|---|---|---|
0.5 mg/mL | 0.10 mg | Very dilute, uncommon |
1 mg/mL | 0.20 mg | Low concentration, easy to measure |
1.34 mg/mL | 0.27 mg | Ozempic 0.5 mg pen concentration |
2 mg/mL | 0.40 mg | Common compounded concentration |
2.5 mg/mL | 0.50 mg | Most popular compounded concentration |
2.68 mg/mL | 0.54 mg | Ozempic 1 mg pen concentration |
3 mg/mL | 0.60 mg | Some compounded preparations |
3.33 mg/mL | 0.67 mg | 10 mg in 3 mL reconstitution |
5 mg/mL | 1.00 mg | Very common, most charts assume this |
5.36 mg/mL | 1.07 mg | Ozempic 2 mg pen concentration |
10 mg/mL | 2.00 mg | High concentration compounded |
The single most important takeaway from this entire article: there is no universal answer to "20 units is how many mg." The answer always depends on concentration. Anyone who gives you a flat number without asking about your concentration is giving you incomplete, potentially dangerous information.
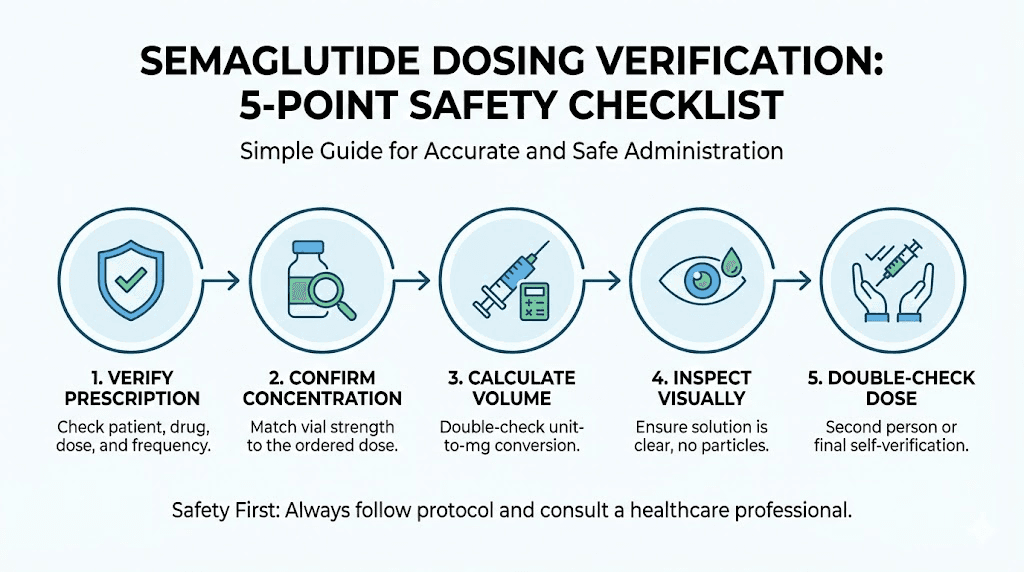
How to double-check your math before every injection
Accuracy is not a one-time calculation. It is a habit. Here is a five-point verification system to use before every dose.
Check 1: Verify your vial concentration. Read the label. Every time. Even if you used the same vial yesterday. Mistakes happen when people rush.
Check 2: Confirm your target dose in mg. Where are you in your escalation schedule? Has your provider changed your dose? Are you adjusting for side effects? Know your milligram target before touching a syringe.
Check 3: Calculate units. (Target mg / Concentration mg/mL) x 100 = units. Do this math. Every time. Write it down if it helps.
Check 4: Sanity check the volume. Does the calculated volume make sense? A 0.25 mg dose from a 5 mg/mL vial is only 5 units (0.05 mL), a tiny amount of liquid. If you calculated 50 units for a starting dose, something is wrong. Go back to step one.
Check 5: Verify the syringe reading. After drawing, confirm the plunger is at the correct marking. Count the lines on the syringe if needed. Better to take an extra thirty seconds than to inject the wrong dose.
SeekPeptides members have access to verification tools, protocol builders, and beginner mistake guides that make this process second nature. But even experienced researchers benefit from a systematic checking routine.
Understanding compounded semaglutide salt forms
Not all compounded semaglutide is the same at the molecular level. The FDA has flagged that some compounding pharmacies use semaglutide sodium or semaglutide acetate, which are different salt forms from the semaglutide base used in FDA-approved products like Ozempic and Wegovy.
Why does this matter for dosing? Because different salt forms have different molecular weights. A milligram of semaglutide sodium is not exactly the same as a milligram of semaglutide base. The active peptide component, the part that actually activates GLP-1 receptors, makes up a slightly different percentage of the total weight depending on the salt form.
In practical terms, this means your 20 units might deliver a slightly different amount of active semaglutide depending on which salt form your pharmacy used.
The difference is typically small, probably within 5-10%, but it adds another variable to an already complex dosing picture. This is one more reason why proper medical supervision matters when working with peptide compounds.
Vial life and dose planning
Understanding how many doses your vial contains helps you plan refills and avoid running out mid-protocol. Here is how to calculate it.
Total doses per vial
Number of doses = Total mg in vial / Your weekly dose in mg
For a 5 mg vial at various weekly doses:
Weekly dose | Doses per 5 mg vial | Vial lasts (weeks) |
|---|---|---|
0.25 mg | 20 doses | 20 weeks |
0.50 mg | 10 doses | 10 weeks |
1.00 mg | 5 doses | 5 weeks |
1.70 mg | ~3 doses | ~3 weeks |
2.40 mg | ~2 doses | ~2 weeks |
Remember that reconstituted semaglutide typically maintains potency for 28-30 days when stored properly in the fridge. If your vial contains more doses than you can use within that window, you either need to reconstitute with less water (higher concentration) to reduce the total volume, or accept that some of the vial will go unused.
For a 10 mg vial, double the dose counts above. At maintenance doses, a 10 mg vial lasts approximately four weeks, aligning well with the reconstituted shelf life. This is one reason researchers on higher doses often prefer 10 mg vials. The peptide cost calculator can help you compare the economics of different vial sizes.
When to consult a healthcare provider
Dosing calculations are mathematical. But dosing decisions are medical. Know the difference.
You should consult a healthcare provider if you are unsure about your current dose escalation step, experiencing persistent side effects, transitioning between different semaglutide products, combining semaglutide with other peptide stacks, or have underlying conditions that might affect how you metabolize the medication.
A provider can also verify your conversion calculations, confirm your concentration, and ensure your dosing protocol aligns with your health goals. The math in this guide is universally applicable. The medical decisions about which dose to target are individual.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact dosing questions.
Real-world dosing scenarios decoded
Theory is helpful. But real situations are messy. Here are actual dosing scenarios that researchers commonly encounter, broken down step by step with the math shown at every stage.
Scenario 1: starting your first semaglutide protocol
You receive a 5 mg vial of lyophilized semaglutide. Your protocol calls for the standard escalation starting at 0.25 mg weekly. You want to use a 2.5 mg/mL concentration because you read that it balances accuracy with convenience.
Step one: reconstitute. Add 2 mL of bacteriostatic water to the 5 mg vial. That gives you 5 mg / 2 mL = 2.5 mg/mL. Swirl gently. Never shake peptides.
Step two: calculate week 1-4 dose. (0.25 mg / 2.5 mg/mL) x 100 = 10 units. Draw 10 units on your insulin syringe. That is 0.1 mL of liquid, a very small amount. Use a 0.3 mL syringe for best accuracy.
Step three: plan ahead. Your vial contains 5 mg total. At 0.25 mg per week, you have 20 doses, which is 20 weeks. But reconstituted peptides last about 28-30 days in the refrigerator. You will use 4 doses (1 mg) in the first month. The remaining 4 mg will still be in the vial when it expires. You either need to escalate faster (not recommended without guidance) or accept some waste. Alternatively, reconstitute with less water to create a higher concentration, letting you store more of the total supply in powder form until needed.
A smarter approach: reconstitute only 2 mg worth at a time by adding 0.8 mL of water to a portion of the powder. But this requires careful measurement and is not practical with most vial sizes. The simplest solution is to use a 10 mg vial and reconstitute it all, since at escalating doses you will use it faster and the math stays clean. SeekPeptides members access protocol planners that calculate optimal reconstitution volumes for each stage of their escalation.
Scenario 2: switching pharmacies mid-protocol
You have been using a 2.5 mg/mL compounded vial. Drawing 40 units per week for your 1.0 mg dose. Your pharmacy closes. The new pharmacy sends a 5 mg/mL vial.
Old protocol: 40 units at 2.5 mg/mL = 1.0 mg. Correct.
If you draw 40 units from the new vial without recalculating: 40 units at 5 mg/mL = 2.0 mg. That is double your intended dose. A 100% overdose.
New protocol: (1.0 mg / 5 mg/mL) x 100 = 20 units. You now draw 20 units, not 40.
This exact scenario, switching concentrations without recalculating, is responsible for a significant percentage of the adverse events the FDA documented. It is also why experienced researchers always verify concentration before drawing. The getting started guide covers this transition process in detail.
Scenario 3: calculating doses for a non-standard concentration
Your pharmacy provides a 3.33 mg/mL vial (10 mg in 3 mL). The standard dose charts you find online do not cover this concentration. You need 1.7 mg for your week 13-16 dose.
Units = (1.7 mg / 3.33 mg/mL) x 100 = 51 units.
That is an awkward number. Most syringes have markings every 1 or 2 units, so hitting exactly 51 is possible but requires careful alignment. You could round to 50 units (1.67 mg) or 52 units (1.73 mg). The difference of 0.03 mg is clinically insignificant for most people. However, consistency matters, so pick one and stick with it throughout your protocol.
This is one reason why non-standard concentrations create ongoing headaches. If you have the option, request a concentration that aligns with clean syringe markings for your target doses. The reconstitution calculator lets you model different water volumes to find concentrations that map cleanly to your dose schedule.
Scenario 4: dose adjustment for side effects
You are at 1 mg weekly (20 units from a 5 mg/mL vial) but experiencing persistent nausea. Your provider suggests dropping to 0.75 mg for two weeks before trying 1 mg again.
New calculation: (0.75 mg / 5 mg/mL) x 100 = 15 units.
Simple. But here is where it gets interesting. Some providers suggest splitting the weekly dose into two smaller injections for better tolerability. Half of 0.75 mg is 0.375 mg, given twice weekly. That is (0.375 / 5) x 100 = 7.5 units per injection. You need a syringe with half-unit markings for this level of precision.
The weight loss peptide protocols section covers various dose adjustment strategies in depth. Managing side effects is normal and does not mean semaglutide is not working. It means your body needs more time to adapt to GLP-1 receptor activation in the gut.
Semaglutide concentration comparison with other common peptides
If you work with multiple peptides, understanding how semaglutide concentrations compare to other common research compounds provides useful context. The unit-to-mg conversion principle is universal, but typical concentrations differ significantly between peptides.
BPC-157
BPC-157 vials typically come in 5 mg. Reconstituted with 2 mL of bacteriostatic water, the concentration is 2.5 mg/mL, identical to common semaglutide concentrations. But BPC-157 doses are measured in micrograms (mcg), not milligrams (mg). A typical dose of 250 mcg equals 0.25 mg, which at 2.5 mg/mL is 10 units. The math is the same. The dose magnitude is different. Use the BPC-157 dosage calculator for precise calculations.
Tirzepatide
Tirzepatide uses much higher concentrations than semaglutide in its compounded forms. Where semaglutide commonly ranges from 2.5-5 mg/mL, tirzepatide concentrations often reach 30-60 mg/mL. This means dramatically different injection volumes for comparable biological effects. Twenty units of a 30 mg/mL tirzepatide solution delivers 6 mg, while 20 units of a 5 mg/mL semaglutide solution delivers 1 mg. The tirzepatide results guide contextualizes what these different doses mean for outcomes.
Retatrutide
Retatrutide is the newest triple agonist (GLP-1/GIP/glucagon). Research concentrations vary widely since the compound is still in clinical trials. The retatrutide pricing guide and dosage calculator help navigate the available options. The same conversion formula applies: dose in mg equals units divided by 100 multiplied by concentration.
TB-500 and other healing peptides
Healing peptides like TB-500 use the same conversion framework. A 5 mg vial reconstituted with 2 mL gives 2.5 mg/mL. The dose magnitudes differ (TB-500 protocols typically call for 2-5 mg per injection), but the math remains unchanged. This universality is why learning the formula once, for semaglutide, equips you for every peptide you will ever handle. The TB-500 dosage calculator automates these calculations.
Whether you are working with CJC-1295, ipamorelin, sermorelin, or any other injectable compound, the relationship between units, volume, and concentration is identical. Master it here and apply it everywhere.
How body weight and composition affect your semaglutide response
The standard dose escalation protocol is the same for everyone. But the response to any given dose varies substantially based on individual factors. Understanding these variables helps explain why someone taking the same 20 units from the same concentration might see dramatically different results than you.
Body weight
Larger bodies distribute semaglutide across more tissue. A 150-pound person achieves higher blood concentration per milligram than a 300-pound person. This is why some clinicians advocate for faster dose escalation in higher-weight individuals and slower escalation for those closer to goal weight. The optimal dose often correlates with body mass, though the relationship is not perfectly linear.
Body composition
Semaglutide distributes primarily through blood plasma and interstitial fluid, not fat tissue. This means that body fat percentage affects distribution volume less than total body weight. Two people at 200 pounds, one with 20% body fat and another with 40% body fat, will have somewhat different pharmacokinetic profiles. The leaner individual may experience stronger effects per milligram because they have proportionally more lean mass and blood volume relative to total weight.
Metabolism and genetics
Individual variations in GLP-1 receptor density and sensitivity affect how strongly any given dose activates the appetite suppression and glucose regulation pathways. Some people respond powerfully to 0.5 mg. Others need the full 2.4 mg to achieve comparable effects. This variability is normal and does not indicate that anyone is doing anything wrong.
If you have been on semaglutide for several weeks and are not seeing expected results, check your dosing accuracy first. Many cases of apparent treatment failure turn out to be dosing errors. Verify your concentration. Recalculate your units. Consider whether your weight management protocol needs adjustment based on your individual response.
Storing and handling semaglutide for maximum potency
Accurate dosing means nothing if your semaglutide has degraded. Storage conditions directly affect potency, and degraded semaglutide can deliver less active compound per milligram than the label states.
Before reconstitution
Lyophilized (freeze-dried) semaglutide is relatively stable. Store it at room temperature or refrigerated, away from direct light. Most lyophilized peptides maintain potency for months or even years when stored properly in powder form. Avoid extreme temperatures and humidity.
After reconstitution
Once you add bacteriostatic water, the clock starts ticking. Reconstituted semaglutide should be refrigerated at 36-46 degrees Fahrenheit (2-8 degrees Celsius). Do not freeze it. Freezing and thawing causes protein denaturation that destroys the peptide structure. The shelf life after reconstitution is typically 28-30 days, though some sources cite up to 56 days for semaglutide specifically.
Signs of degradation
Clear and colorless is what you want. Any of these signs mean you should discard the vial:
Cloudiness or turbidity. Visible particles or flakes. Yellow or brown discoloration. Unusual smell. Changed viscosity (thicker or thinner than normal).
Using degraded semaglutide does not just mean reduced potency. Degradation products can sometimes cause additional adverse reactions that the intact peptide would not. When in doubt, discard and reconstitute a fresh vial. The cost of wasted semaglutide is always less than the cost of injecting a compromised compound.
Temperature exposure tracking
One common mistake: leaving a vial out on the counter while preparing an injection and forgetting to put it back in the refrigerator. Brief temperature excursions (under 30 minutes at room temperature) are generally fine. Extended exposure to temperatures above 77 degrees Fahrenheit accelerates degradation. If your vial has been at room temperature for more than a few hours, its remaining shelf life is reduced. The exact impact depends on the temperature and duration, but erring on the side of caution with room temperature storage limits protects your investment.
Building a personal dosing reference card
The most practical thing you can do after reading this guide is create a personal dosing reference card. Write it on an index card, print it out, or save it on your phone. Here is what it should include:
Your current concentration: _____ mg/mL
Your current weekly dose: _____ mg
Your current unit amount: _____ units
Your syringe size: _____ mL (_____ unit capacity)
Your next dose increase: At week _____, increase to _____ mg = _____ units
Vial expiration: Reconstituted on _____, discard by _____
Update this card every time something changes. New vial, new concentration, dose adjustment, anything. The thirty seconds it takes to update your reference card can prevent the kind of dosing error that sends people to the emergency room.
For a more comprehensive tracking system, SeekPeptides offers digital protocol trackers, dose logging tools, and cycle planning guides that automate much of this record-keeping. But even a handwritten index card beats nothing.
Combining semaglutide with other peptides and the dosing implications
Many researchers eventually explore combining semaglutide with other compounds. Whether adding BPC-157 for gut support, cagrilintide for enhanced weight management, or healing peptides alongside GLP-1 therapy, each additional compound requires its own unit-to-mg conversion based on its own concentration.
Never assume that because two peptides have the same concentration, they share the same dose. BPC-157 at 2.5 mg/mL and semaglutide at 2.5 mg/mL use the same conversion math, yes. But BPC-157 protocols call for 250 mcg (0.25 mg) typically twice daily, while semaglutide uses 0.25-2.4 mg once weekly. Using the semaglutide dose for BPC-157 or vice versa would be a serious error. Each peptide in your stack needs its own calculated dose based on its own protocol and its own vial concentration.
Keep separate dosing cards for each compound. Label each syringe if preparing multiple injections. Never draw from the wrong vial. These sound like obvious precautions, but errors happen most often during routine tasks when attention wanders. The peptide stack calculator helps manage the complexity of multi-peptide protocols.
The bottom line on 20 units of semaglutide
Twenty units of semaglutide on an insulin syringe equals 0.2 mL of liquid. Always. Regardless of concentration, brand, or formulation. That never changes.
What does change is how many milligrams of semaglutide are dissolved in that 0.2 mL. At 1 mg/mL, it is 0.2 mg. At 2.5 mg/mL, it is 0.5 mg. At 5 mg/mL, it is 1.0 mg. At 10 mg/mL, it is 2.0 mg. The concentration printed on your vial label is the only variable you need. Once you have that number, one multiplication gives you your answer.
Most online sources that say "20 units equals 1 mg" are assuming a 5 mg/mL concentration. If that matches your vial, great. If it does not, their answer is wrong for you, and following it could mean taking two, four, or even ten times your intended dose.
Check your concentration. Do the math. Verify before you inject. Every single time. The five seconds it takes to confirm your calculation is the cheapest insurance against a dosing error you will ever find. And if the math ever feels confusing, tools like the semaglutide dosage calculator and the general peptide calculator exist specifically to remove the guesswork.
Frequently asked questions
Is 20 units of semaglutide the same as 1 mg?
Only if your vial concentration is 5 mg/mL. At 2.5 mg/mL, 20 units equals 0.5 mg. At 10 mg/mL, 20 units equals 2 mg. Always check your vial concentration before converting. Use the semaglutide dosage calculator for instant verification.
How do I convert semaglutide units to mg?
Use this formula: mg = (units / 100) x concentration in mg/mL. For example, 20 units from a 5 mg/mL vial: (20 / 100) x 5 = 1 mg. The formula works for any syringe unit amount and any concentration. Our peptide calculation guide covers this in detail.
Why do different sources give different answers for 20 units of semaglutide?
Because they are assuming different concentrations. Most generic charts assume 5 mg/mL (where 20 units = 1 mg). But compounded semaglutide comes in many concentrations, and each one produces a different mg dose from the same unit amount. This is the most common source of dosing errors.
What concentration does Ozempic use?
Ozempic pens use three different concentrations depending on the dose tier: approximately 1.34 mg/mL (for the 0.25/0.5 mg pen), 2.68 mg/mL (for the 1 mg pen), and 5.36 mg/mL (for the 2 mg pen). However, Ozempic pens have built-in dose selectors, so manual unit conversion is not necessary. Learn more about the differences between semaglutide products.
Can I use an insulin syringe for semaglutide?
Yes. U-100 insulin syringes are the standard for drawing semaglutide from multi-dose vials. The "units" on the syringe measure volume (hundredths of a mL), not drug units. Make sure you are using a U-100 syringe, not a U-40 or U-50. Read our injection device guide for more details.
How many units of semaglutide should I start with?
The standard starting dose is 0.25 mg weekly. At 5 mg/mL, that is 5 units. At 2.5 mg/mL, that is 10 units. At 1 mg/mL, that is 25 units. Always start with the lowest dose and escalate gradually every four weeks. The complete dosing protocol outlines each escalation step.
What happens if I accidentally take too many units?
An overdose of semaglutide can cause severe nausea, vomiting, dizziness, and hypoglycemia (low blood sugar). The FDA has documented cases of patients taking 5 to 20 times their intended dose due to unit confusion. If you suspect an overdose, seek immediate medical attention. Even moderate overdoses can cause significant gastrointestinal distress.
Does the concentration affect how well semaglutide works?
No. A 0.5 mg dose is a 0.5 mg dose regardless of whether it came from 20 units of a 2.5 mg/mL solution or 10 units of a 5 mg/mL solution. The total milligrams of active compound entering your body is what determines effectiveness. Concentration only affects how much liquid you inject. Results depend on consistent, accurate dosing over time, which is why understanding the timeline for semaglutide effects matters.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay verified, your calculations stay accurate, and your doses stay consistent.